Public procurement of innovations, diffusion and endogenous institutions Max Rolfstam Sønderborg Participatory Innovation Research Centre, University of Southern Denmark, Sønderborg, Denmark Wendy Phillips Bristol Business School, University of the West of England, Bristol, UK, and Elmer Bakker Tandridge District Council, Oxted, UK Abstract Purpose – Public procurement has been increasingly seen as an important innovation policy tool. One neglected aspect of the public procurement of innovation is, however, diffusion. The purpose of this paper is to counter this neglect by exploring how institutional coordination may affect the diffusion of innovations procured by a public agency. Design/methodology/approach – A case study including semi-structured interviews and the consulting of different documents were used to study how institutions and institutional coordination affect the adoption and diffusion of innovation. Findings – Several endogenous institutions were identified that act as barriers to the diffusion of innovation throughout an organisation. Attempts to re-design and negate these barriers were also identified. Research limitations/implications – Institutional analysis of innovation has a tendency to be limited to formal and exogenous institutions. The paper underscores the importance of taking into account the endogenous institutional set-up. The results are drawn on a single case study. Practical implications – The understanding of public procurement of innovation needs to be expanded beyond the formal procurement process. Special attention needs to be given to diffusion processes where institutional coordination and re-design should be considered an important component. Originality/value – The paper considers diffusion as an important component of public procurement of innovation, and emphasises the importance of the endogenous institutional level both for understanding and for coordinating diffusion, which are two aspects commonly neglected in the literature. Keywords Public procurement, Innovation, Institutions, Diffusion, Adaption Paper type Case study Introduction This paper concerns the role of public procurement as a means to stimulate innovation, which has, over the last decade, been emphasised increasingly (Edler et al., 2005). At the European level, public agencies have been described as “big market players” which “have powerful means to stimulate private investment in research and innovation” (European Commission, 2005, p. 8). In the UK, initiatives are under way to make The current issue and full text archive of this journal is available at www.emeraldinsight.com/0951-3558.htm IJPSM 24,5 452 Received 15 February 2010 Revised 16 September 2010 Accepted 21 September 2010 International Journal of Public Sector Management Vol. 24 No. 5, 2011 pp. 452-468 q Emerald Group Publishing Limited 0951-3558 DOI 10.1108/09513551111147178
Transcript
Public procurement ofinnovations, diffusion andendogenous institutions
Max RolfstamSønderborg Participatory Innovation Research Centre,
University of Southern Denmark, Sønderborg, Denmark
Wendy PhillipsBristol Business School, University of the West of England, Bristol, UK, and
Elmer BakkerTandridge District Council, Oxted, UK
Abstract
Purpose – Public procurement has been increasingly seen as an important innovation policy tool.One neglected aspect of the public procurement of innovation is, however, diffusion. The purpose ofthis paper is to counter this neglect by exploring how institutional coordination may affect thediffusion of innovations procured by a public agency.
Design/methodology/approach – A case study including semi-structured interviews and theconsulting of different documents were used to study how institutions and institutional coordinationaffect the adoption and diffusion of innovation.
Findings – Several endogenous institutions were identified that act as barriers to the diffusion ofinnovation throughout an organisation. Attempts to re-design and negate these barriers were alsoidentified.
Research limitations/implications – Institutional analysis of innovation has a tendency to belimited to formal and exogenous institutions. The paper underscores the importance of taking intoaccount the endogenous institutional set-up. The results are drawn on a single case study.
Practical implications – The understanding of public procurement of innovation needs to beexpanded beyond the formal procurement process. Special attention needs to be given to diffusionprocesses where institutional coordination and re-design should be considered an importantcomponent.
Originality/value – The paper considers diffusion as an important component of publicprocurement of innovation, and emphasises the importance of the endogenous institutional levelboth for understanding and for coordinating diffusion, which are two aspects commonly neglected inthe literature.
Keywords Public procurement, Innovation, Institutions, Diffusion, Adaption
Paper type Case study
IntroductionThis paper concerns the role of public procurement as a means to stimulate innovation,which has, over the last decade, been emphasised increasingly (Edler et al., 2005). Atthe European level, public agencies have been described as “big market players” which“have powerful means to stimulate private investment in research and innovation”(European Commission, 2005, p. 8). In the UK, initiatives are under way to make
The current issue and full text archive of this journal is available at
www.emeraldinsight.com/0951-3558.htm
IJPSM24,5
452
Received 15 February 2010Revised 16 September 2010Accepted 21 September2010
International Journal of Public SectorManagementVol. 24 No. 5, 2011pp. 452-468q Emerald Group Publishing Limited0951-3558DOI 10.1108/09513551111147178
government “a smarter customer”, with stimulation of private sector innovation as acentral theme (Department of Trade and Industry, 2004, p. 11). Similar developmentsare also emerging elsewhere. Public procurement contributes to around 16 per cent ofEuropean GDP (EC, 2004) and in some countries, e.g. the UK and in some market areas,e.g. medical equipment, the share is even bigger. Consequently, the public sectorcommands a strong purchasing power that, if managed appropriately, could promoteinnovation.
The demand-side influence of public agencies to shape and drive innovation hasbeen well researched (see, e.g. Rolfstam, 2005; Edler and Georghiou, 2007) with anemphasis on developmental technology procurement (Edquist et al., 2000, p. 21). Theaim of this paper is to focus on the supply-side and adaptive public technologyprocurement: the role of public agencies in the adoption of emerging private sectorinnovations., innovations being developed by the private sector that are new to thepublic sector. Building on the notion that, “without diffusion, innovations have littlesocial or economic impact” (Hall, 2005, p. 459) the paper adopts an institutionalapproach on innovation studies, to explore how institutions affect diffusion processeswithin organisations. Thus, by emphasising this other aspect of public procurement,this paper sets out to further explore and essentially expand the understanding ofpublic procurement in relation to innovation.
The paper will commence with an overview of the literature, it will then present anexplorative case study of an attempt by the English National Health Service (NHS) toprocure and diffuse a new catheter throughout its Trusts. It will then conclude with adiscussion of the role of public sector agencies in promoting the uptake of emerginginnovations from the private sector.
Public procurement, innovation and diffusionPublic procurement occurs when a public agency purchases goods and/or servicesfrom an outside body (Arrowsmith, 2005, p. 1). The goods and services may be eitherregular, off-the-shelf-products, which serve the general needs of the user, or innovativeproducts which have been delivered as a result of development carried out by thesupplier to meet further requirements that are not fulfilled by existing products(Edquist et al., 2000). A public agency can influence demand for innovation by directprocurement, acting as a proxy customer (e.g. by creating standards) or as a linkagecreator between suppliers and users (Rothwell, 1994). The demand-side approachwhere “a public agency places an order for a product or system which does not exist atthe time, but which could probably be developed within a reasonable period” (Edquistet al., 2000, p. 5) also suggests that public technology procurement may be a useful toolto stimulate innovation.
The definition of innovation applied in this paper is derived from the intersection ofdefinitions made by two authorities on the topic (Freeman, 1982; Rogers, 1995).Freeman defines innovation as “the introduction of a new product, process, system ordevice – to be distinguished from invention which is a new idea, a sketch, or model fora new improved device, product, process or system” (Freeman, 1982, p. 7). Aninnovative product does however not remain an innovation but eventually matures (seeUtterback, 1994), corresponding to what Edquist et al. (2000) refer to as ‘regular’products as presented above. Rogers (1995, p. 5) defines innovation as “an idea,
Publicprocurement of
innovations
453
practice, or object that is perceived as new by an individual or other unit of adoption”(Rogers, 1995, p. 11).
Diffusion then, is this idea, practice or object “communicated through certainchannels over time among the members of a social system” (Rogers, 1995, p. 5.). A basicrequirement for diffusion in any social system is that the innovation has to be known.It is also likely that the innovation has “at least some degree of benefit for its potentialadopters” (Rogers, 1995, p. 13). This means an innovation can be developed in onesocial system and then be exposed to another social system. Also, what has become amature, off-the-shelf product in one social system might be considered an innovation inanother. In this light the dichotomy distinguishing regular from innovative publicprocurement suggested by Edquist et al. (2000) becomes ambiguous. A procurement of,what these authors would call “regular” goods, i.e. already existing products developedelsewhere might actually be perceived as “new” when introduced into another socialsystem. This means that, from the potential adopter’s perspective,some off-the-shelfproducts may be considered as public procurement of innovations.
Thus, the position taken here, as argued by Uyarra and Flanagan (2010), is that theapplication of public procurement as a means to stimulate innovation involves not onlypublic technology procurement where a public agency formulate demand for productsthat do not currently exist. There is also a need to acknowledge the supply-side, forexample, when private sector suppliers approach public procurers with unsolicitedoffers of new innovative products. In order to fund future innovations, suppliers needto secure returns of investment in research and development. In sectors dominated bythe public sector, suppliers offering unsolicited innovative products or services may bedependent on public agencies’ ability to adopt innovation. What further makes this animportant issue is the common use of framework agreements in public procurement.Although centrally negotiated contracts may exist, diffusion will not take place untilcall-offs (i.e. actual purchase) are made from these contracts by departments within theorganisation. Thus, understanding public sector adoption of innovations may becritical for stimulation of innovation in a long-term perspective.
The decision to adopt an innovation is generally determined by how it is perceivedby adopters. It may sometimes be hard to conceptually distinguish between diffusionand adoption as both these concepts try to capture how an innovation is received. Oneway of attaining such a distinction is to think of diffusion as something that takesplace in a population, e.g. a sample of firms or adopting units among which adoptionwould take place. Adoption studies understood in this perspective focus on theindividual unit, e.g. a person and try to further understand the individual adoptionbehaviour (Lissoni and Metcalfe, 1996).
The characteristic features of diffusion and adoption processes occurring withinorganisations may be considered through employing a social systems approach.Rogers defines a social system as “a set of interrelated units that are engaged in jointproblem solving to accomplish a common goal” (Rogers, 1995, p. 23). Units of such asystem may be individuals, informal groups, organisations, and/or subsystems(Rogers, 1995, p. 23). There are some fundamental differences between individualconsumers’ adoption of an innovative end-consumer product and an innovationadopted by an organisation. Following Rogers (1995), individuals within anorganisation may sometimes not be able to adopt an innovation before theorganisation, i.e. somebody with authority over the organisation, has decided to do so.
IJPSM24,5
454
Also, the decision made by an organisation to adopt a certain innovation does not bynecessity mean that an individual within the organisation will do so directly. Thus,within an organisational context, the decision to reject or adopt an innovation is not asstraight-forward as it might be elsewhere (Rogers, 1995).
The role of institutions and institutional co-ordinationThe focus of this paper is not so much on the decisions per se as the determinants ofdiffusion and adoption of an innovation in a social system, as emphasised by systemicapproaches to innovation studies (Dosi et al., 1988; Lundvall, 1992; Edquist andJohnson, 1997; Hollingsworth, 2000), which acknowledge the role that institutions playduring the process of innovation. Institutions are perceived as “the rules of the game ina society. . . that shape interaction” (North, 1990, p. 3) or as “sets of habits, routines,rules, norms and laws, which regulate the relations between people and shape humaninteraction” ( Johnson, 1992, p. 26). Institutions manifest on different levels in society.Super-national law such as the EC Directives on Public Procurement, transpositions ofthese laws into national public procurement law, specific directives and policies forspecific public agencies, endogenous institutions or rationalities (see Gregersen, 1992)among potential suppliers or collaborators, individual habits and values are allexamples of institutions relevant for analysis of public procurement of innovation.
Current institutional analysis of innovation tends however to be limited to formalinstitutions, i.e. the legal and regulatory framework associated with a given innovationprocess. Although some authors acknowledge that the concept is much broader inscope (Edquist and Johnson, 1997; Hollingsworth, 2000), empirical innovation researchtaking into account that institutions may exist on different levels are rather scarce. Forinstance, within research interested in how institutions may affect possibilities forpublic procurement of innovation, the main focus has been on the legal frameworks asstipulated by the European Directives on Public Procurement (Edquist et al., 2000;Nyholm et al., 2001). The argument brought forward in this paper is that it is veryproblematic to make any general statements based on formal institutions only.Empirical research also suggests that in order to provide an adequate understanding,other institutional levels need to be taken into account (Rolfstam, 2009).
Cases in point are given, e.g. by Coriat and Weinstein (2002) who distinguishbetween Type 1 and Type 2 institutions. The former type “is based on the criteria ofauthority and enforcement and posed on all the agents” (Coriat and Weinstein, 2002, p.283). These are typically formal laws that apply to everyone and cannot be waived(Coriat and Weinstein, 2002, p. 282), i.e. institutions that traditionally have beenemphasised in the innovation literature. Type 1 institutions also include anenforcement system that punishes any violation of the institutions. Type 2 institutionsare the rules that individual agents decide to give themselves; they are “‘private’collective agreements between groups of agents” (Coriat and Weinstein, 2002, p. 283).The other dimension these authors take into account is institutional lifetime. Theydistinguish between Type A and Type B institutions where the former refers to longlasting institutions regulating reproduction of the society as a whole, whereas type Binstitutions are fixed in time. One example of a Type A institution would be a hospitaland its role to provide health services for citizens. The hospital as an institutionremains relatively unchanged over time. One example of a type B institution would bea contract between a public procurer and a supplier where the contract would regulate
Publicprocurement of
innovations
455
certain behaviour from the actors towards each other over a relatively short definedtimespan.
Another distinction is made between exogenous and endogenous institutions( Jacoby, 1990). Exogenous institutions affect organisations from the outside and areimposed on organisations with little or no control from the organisation itself.Endogenous institutions typically develop within organisations, and may also changeas a result of learning within the organisation. A certain institutional set-up in anorganisation may prevent the adoption of a specific item and its diffusion throughoutthe organisation. An innovation new to an organisation may or may not beinstitutionally matching with, for example, existing technology, current and existingstandards, established ways of working, perceived values, strategic decisions,rationalities, or established budgets. Thus certain endogenous institutions may act asbarriers to the adoption of innovations into an organisation and their subsequentdiffusion.
The literature also discusses the difference between formal and informalinstitutions (Borras, 2004). This is a dichotomy that may or may not converge withthe exogenous – endogenous dichotomy discussed previously. Although exogenousinstitutions such as laws are formal, not all exogenous institutions are. Certain culturaltraditions might be exogenous but still informal. Similarly, endogenous institutionsmay be formal or informal. An example of a formal endogenous institution would be awritten work instruction used by an organisation. What is perhaps the most significantdifference is that the exogenous – endogenous dichotomy takes into account thatinstitutions are relative and may have a different “range” ( Jepperson, 1991, p. 146).They may manifest as formal national law only when applied in a particular countryand not in other countries; a manager may have authority over his or her employeesbut not over other managers’ employees, etc. This is an aspect that is not captured wellby the informal-formal dichotomy.
Institutions typically evolve slowly and reactively and therefore tend to lag behindtechnical change. This may lead to mismatch problems “which prevent the fullrealization of the productivity potentials of technical innovations, which forestall thereallocation of resources and efforts from mature to emerging technologies, and whichgenerally favour established technological trajectories to new ones” (Edquist andJohnson, 1997, p. 55), which suggests that institutions may also sometimes act asbarriers, preventing the diffusion of innovation throughout an organisation. This lineof thinking raises a need to also consider the institutional aspect of introducing aninnovation into an organisation – i.e. what some authors refer to as institutionalcoordination.
Innovation theory based on institutional perspectives brings coordination and thecoordinative functions of institutions to the fore. Research on innovation processes andsystems points to “tension or mismatch between different kinds of designedinstitutions that often represent different levels of policy-making” (Edquist et al., 1998,p. 38). Also Lundvall and Borras (2005, p. 627) raise a concern regarding theco-ordination of policies affecting innovation. Thus, understanding how theinstitutional set-up affects innovation processes involves detailed analysis of theinterplay between different kinds of institutions conceived as coordinationmechanisms or governance structures (Hollingsworth, 2000). Coordination mightalso be necessary if public procurement of innovation is to be sustained. In other
IJPSM24,5
456
words, if institutional barriers are not negotiated, projects involving publicprocurement of innovation may have to be terminated without rendering theintended result (Rolfstam, 2007). Institutional coordination for public procurement ofinnovation may involve “developing, mobilizing, and coordinating competence amongmultiple buyers” (Hommen and Rolfstam, 2009, p. 27).
The literature surveyed in the previous sections supports an understanding ofinnovation as a social process characterised by interactive learning guided byinstitutions. Developing such a perspective will also contribute towards understandingthe level of institutional coordination required to overcome prevailing institutionalbarriers that may prevent the diffusion of innovations. In the past, innovation literaturehas tended to focus on formal or exogenous institutions such as national law, failing totake into account other institutional levels which may have negative consequences forinstitutional coordination – if an exogenous template is employed, endogenousinstitutional barriers may be ignored.
In responding to this oversight, the paper will explore how institutional interplayaffects innovation diffusion by addressing the following research question: How maycoordination (or the lack thereof) among different kinds of institutions affectperformance in public procurement of innovations?
MethodThe case discussed in this paper was identified within the context of a study conductedin England and Sweden in 2006 involving multiple cases of public procurement.Included in the study were two categories of public procurement projects, those that ledto innovation, and those that could have led to innovation should some factors havebeen in place (Rolfstam, 2009). Innovation is not an isolated event and building on theunderstanding that the process of innovation is supported by a series of activities,including diffusion (Maidique, 1980), the current case falls into the latter category, andwas thus chosen through purposeful or theoretical sampling to fill a theoreticalcategory (Eisenhardt, 1989, p. 537). Unlike “best-practice” studies, cases like the onereported here, might offer greater possibilities to identifying barriers that managersand policy makers can eventually deal with in order to increase innovation anddiffusion throughout their organisations.
One strength associated with case studies is that it allows the use of a variety ofsources (Denscombe, 1998). Yin (1994) lists six sources of evidence that might be usedin case studies, documentation, archival records, interviews, direct observations,participant observations and physical artefacts; the case study employed the first threesources. Examples of documentation and archival records consulted were policyreports from, e.g. Department of Health, or different agencies within NHS, andacademic literature such as reviews of research on the effects of silver coated catheters.
Data and informants were selected by means of conceptually-driven sequentialsampling (Miles and Huberman, 1994, p. 27). This means that the selection ofinterviewees was purposive, rather than random. Interviewed people wereprocurement practitioners involved in the process to procure the new catheter,representatives for the supplier, Bard Ltd in England and staff at the Department ofHealth. Six persons were involved; all interviews were recorded and transcribed.Semi-structured interviews were carried out. By doing so, additional information maybe provided that may be of interest and relevance to the case. The research was carried
Publicprocurement of
innovations
457
out following a case study protocol developed at the early stages of the project (Yin,1994).
The case of the silver coated catheterThe National Health Service (NHS) was established after the Second World War toprovide healthcare for everyone resident in the UK and is today one of the largestorganisations in the word employing roughly 1.3 million people (Lister, 2004). The costof running the NHS is estimated to £100 billion and financed entirely by tax money.The NHS consists of an array of different healthcare providers and administrativefunctions. The healthcare providers are organised in different types of trusts; e.g.Primary Care Trusts, NHS Hospital Trusts (or Acute Trusts), or NHS Hospitals. TheNHS falls under the jurisdiction of the Department of Health within which resides theNHS Purchasing and Supply Agency (PASA), a central procurement agency. NHSPASA’s role is “to ensure that the NHS in England makes the most effective use of itsresources by getting the best possible value for money when purchasing goods andservices” (NHS PASA, 2008). There are several channels which suppliers can use todiffuse their products into the NHS organisation. These different supply routes alsohave different institutional characteristics that may affect diffusion within theorganisation and will be discussed in more detail in the following sections.
Public procurement of a solutionThis case concerns the problems with Catheter Associated Urinary Tract Infections(CAUTIs) and can be seen as a special chapter of the general issue of combatinginfectious deceases, which has been a challenge for healthcare agencies globallythrough out history. In the last decades of the twentieth century one specific areaemerged as particularly problematic in UK – the increasing problems withhealthcare-associated infections i.e. those infections transmitted to patients seekingcare at NHS facilities. Four major problematic areas are: infections of the urinary tract,surgical-wound infections, lower-respiratory tract, and skin infections (Emmerson et al.,1996) where the most common of these are urinary infections (see also Department ofHealth, 2003). Thus, in 2002, healthcare-associated infections were identified as “amajor problem for the NHS” (Department of Health, 2002, p. 62) and therefore listed asone of the key areas that should be prioritised in order “to combat the present as well asthe possible future threat posed by infectious diseases” (Department of Health, 2002, p.22). Apart from the suffering imposed on individual patients, healthcare-associatedinfections are also costly for the healthcare system. Costs for these infections have beenestimated to £930 million per annum in England, where £124 million are imposed byurinary tract infections (Plowman et al., 2001).
Many factors drive the increase of healthcare-associated infections. Factors are forinstance the increased number of patients with severe illnesses in the healthcaresystem as patients in a serious condition become more vulnerable to infections; but itcan also be therapeutic factors, i.e. that indwelling catheters need to be used to helpcuring patients; organisational factors, e.g. poor staff to patient ratio; or behaviouralfactors such as poor compliance with hygiene standards (Department of Health, 2003).Guidelines have also been developed to address these areas (Pratt et al., 2007). Theseguidelines are also made accessible to NHS employees through an award-winninge-learning project (Pratt and O’Malley, 2007). The interest in this paper concerns
IJPSM24,5
458
another element that may contribute in the battle against healthcare-associatedinfections, namely adoption of new technology. In general, promoting the adoption ofinnovation within organisations appears to be a rather underdeveloped area and in theguidelines for healthcare-associated infections, is still listed under “Areas for furtherresearch” (Pratt et al., 2007).
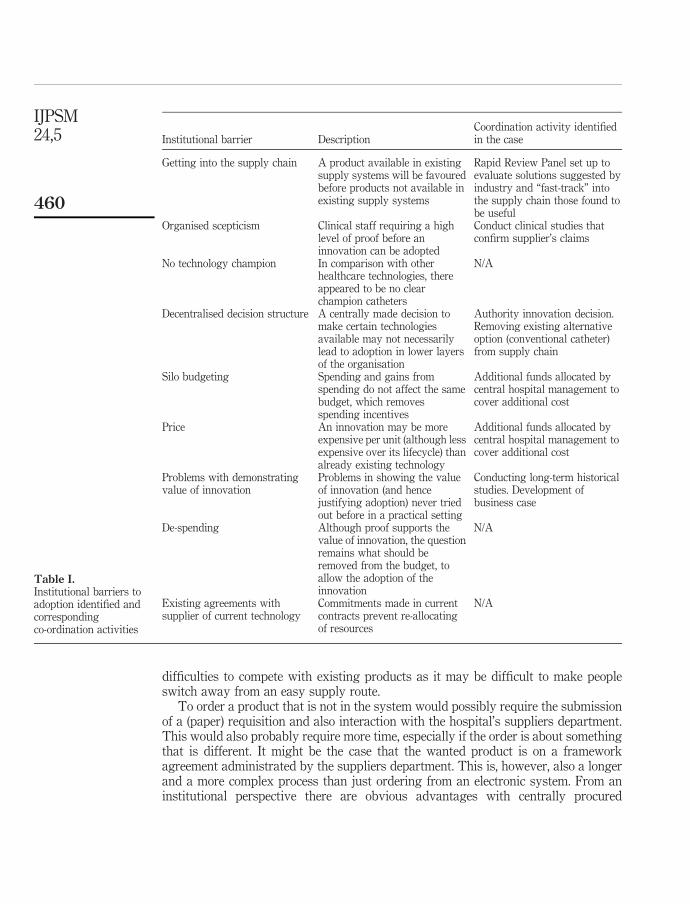
The role of endogenous institutionsIn undertaking this case study a route of a new technology into the English NHS wasinvestigated in order to identify the role of endogenous institutions during the uptakeof innovations. With a focus on catheter associated urinary tract infections, this studycharts the progress of the Bardex catheter a catheter that, on account of theantibacterial properties of its silver counting, claims to reduce healthcare-associatedinfections. Several endogenous barriers were identified as well as some measures thatwere designed to overcome them. These are discussed in the following sections andsummarised in Table I.
Supplying to the NHSWithin the NHS there is no stipulated route for the supply of consumables. Any singleNHS trust may utilise supply routes as they find most appropriate. In principle (for thepurposes here) there are three routes for supply of consumables to a NHS hospital.Products can be ordered through an electronic ordering system, Logistics On-Line(LOL). The products that are in this electronic catalogue are supplied from one of thesix regional stores managed by the NHS Supply Chain (formerly NHS Logistics). Asecond option is to order directly from a supplier through a framework agreementnegotiated centrally. These products are available online through the NHS E-Cat.These orders are placed directly to the suppliers with a reference to the frameworkcontract number, and the supplier will deliver directly to the specified address andinvoice the Trust directly. It is also possible to order from contracts set up throughpublic procurement on the local level. Similar to ordering from framework agreementsprovided centrally (managed earlier by NHS PASA and nowadays by the NHS SupplyChain), the supplier delivers to a specified address and invoice directly the Trust.
These three supply routes differ in terms of the administrative complexity.Procurement through the NHS Supply Chain is the most straightforward as it is simplyabout ordering from the LOL. Buying products included in the NHS PASA frameworkagreements as published in the E-Cat requires awareness of the specific contracts aswell as interaction with the supplier and is therefore slightly more demanding and timeconsuming. The third option, to manage the complete procurement process locally, isthe most complex, as it requires development of contract specification, going throughaward procedures to find suppliers, and in the case of framework agreements orderingproducts.
The default supply route for catheters into a NHS ward is managed in a ratheroperational manner. For a nurse with responsibility for replenishing the stock ofcatheters on a ward, ordering a new catheter would be a routine task accomplishedthrough the use of an electronic system. Deliveries come once a week in appropriatepackages and the invoice will typically be handled by the supplies department at thehospital. A new alternative product that is not in the LOL system may face some
Publicprocurement of
innovations
459
difficulties to compete with existing products as it may be difficult to make peopleswitch away from an easy supply route.
To order a product that is not in the system would possibly require the submissionof a (paper) requisition and also interaction with the hospital’s suppliers department.This would also probably require more time, especially if the order is about somethingthat is different. It might be the case that the wanted product is on a frameworkagreement administrated by the suppliers department. This is, however, also a longerand a more complex process than just ordering from an electronic system. From aninstitutional perspective there are obvious advantages with centrally procured
Institutional barrier DescriptionCoordination activity identifiedin the case
Getting into the supply chain A product available in existingsupply systems will be favouredbefore products not available inexisting supply systems
Rapid Review Panel set up toevaluate solutions suggested byindustry and “fast-track” intothe supply chain those found tobe useful
Organised scepticism Clinical staff requiring a highlevel of proof before aninnovation can be adopted
No technology champion In comparison with otherhealthcare technologies, thereappeared to be no clearchampion catheters
N/A
Decentralised decision structure A centrally made decision tomake certain technologiesavailable may not necessarilylead to adoption in lower layersof the organisation
Problems in showing the valueof innovation (and hencejustifying adoption) never triedout before in a practical setting
Conducting long-term historicalstudies. Development ofbusiness case
De-spending Although proof supports thevalue of innovation, the questionremains what should beremoved from the budget, toallow the adoption of theinnovation
N/A
Existing agreements withsupplier of current technology
Commitments made in currentcontracts prevent re-allocatingof resources
framework agreements. From the perspective of the daily operations on a hospitalward for instance, supply of catheters would preferably take place as straight rebuys.These are routine transactions requiring a minimum of new information andconsideration of new alternatives (Robinson et al., 1967). On the other hand, for a newproduct not in the systems and therefore more difficult to access, the same routinesbecome an institutional barrier as they may reduce both trialability and observabilityfor an innovation.
In August 2004 the Rapid Review Panel was set up. Run by the Health ProtectionAgency on behalf of the Department of Health, the purpose of the panel was toencourage industry to come with ideas that would tackle the problems related tohealthcare-associated infection. The panel’s task was to “assess new and novelequipment, materials, and other products or protocols that may be of value to the NHSin improving hospital infection control and reducing hospital acquired infections”(Health Protection Agency, 2006). One of the first products submitted to the RapidReview Panel was the Bardex catheter. The suppliers claimed that the risks ofacquiring an infection with the Bardex catheter would be much less then conventionalcatheters. The Rapid Review Panel agreed that it was a good product, it was new, ithad antibacterial activity and that there were evidence that it would reduce the numberof catheter associated infections if used in patents needing catheterisation for morethan 48 hours. As one of very few products, the Bardex catheter received the top mark,i.e. the judgment was that it had “shown benefits that should be [made] available toNHS” (Health Protection Agency, 2006).
As a response to the result of the Rapid Review Panel, NHS PASA “fast tracked” theBardex catheter into the NHS Supply Chain. When the Bardex catheter was introducedin England 2002, initially the only supply route available was the most complex one,i.e. it was neither available on contract and neither was it in stock. When it becameavailable from the NHS Supply Chain, in September 2005, roughly a year after theRapid Review Panel had published their results, the use of the product increased. In2006, about 30 NHS hospitals were using the Bardex catheter. The estimated markedshare for products in its range was at the time 2-3 per cent. In USA the same catheterhad a market share around 40 per cent.
It should be noted that from a clinical point of view, the Rapid Review Panel had astrictly indicative function. The pane makes statements based on evidence taken intoaccount whether or not a product does what is says it does, as reported from otherstudies. The panel does neither recommend nor provide mandatory directives whetheror not to use a certain product. In this case, the decision to use the Bardex catheter ismade by clinicians. What did happen as a result of the panel’s judgement was that theBardex catheter was brought into the NHS supply chain by NHS PASA more quickly,which meant that any clinician in a hospital championing the Bardex catheter couldjust order it from the system rather than going through a complete procurementprocess.
Organised scepticismIn the first years of the diffusion process of the Bardex catheter, scepticism regardingthe evidence-base prevailed among NHS clinicians, infection control staff andcontinence advisors. NHS staff did not necessarily subscribe to the view that the silvercoating used on the Bardex catheter would help reducing healthcare-associated
Publicprocurement of
innovations
461
infections. Although no studies appear to challenge the assertions made by thesuppliers of the Bardex catheter, concerns have been raised regarding the limitations ofthe referred studies. Within the time-frame of this study, the Rapid Review Panel’sgrading of the Bardex catheter did not lead to an increased rate of diffusion. Theorganised scepticism illustrates well the double aspect of institutions discussed byCoriat and Weinstein (2002). An institution works both as a constraint or as a resource(Coriat and Weinstein, 2002, p. 283). The requirement for evidence of an innovativeproduct’s claimed properties is central to any organisation providing healthcare. Froma diffusion perspective these requirements tend to work as a barrier for diffusion.
Technology championsWhat is often emphasised as a significant element in the diffusion processes is the roleof innovation champions. These are typically “powerful individuals” (Rogers, 1995, p.398) who promote the innovation within an organisation, or implementing leadersenabling collective learning (Edmondson et al., 2001). What has been suggested aproblem in the case of catheters in general relates to the way catheters are used withinhealthcare organisations. As different from, e.g. wound infections which much clearerfalls under the responsibility of surgical units, the problems related to catheters are notas easily connected to a specific unit. Catheters are used in operating departments, inaccident emergency services, post operatively, in any medical unit or ward. This meansthat ownership of the problem becomes less clear and the emergence of innovationchampions specifically devoted to catheters is not promoted.
Decentralised decision-structureAs was discussed above, the need for an innovation is central to its diffusion. Whatseems to be common among the early adopters of the Bardex catheter is that withinthese hospitals a clear perception of the need to prevent and controlhealthcare-associated infections prevailed. Comprehensible business cases weredeveloped displaying the current level of catheter associated infections, their cost, andthe expected benefit from introducing the Bardex catheter. What also seems to be acommon theme is that the decision to introduce the Bardex catheter for a hospital wasoften made centrally, perhaps by the overall financial budget holder for the wholeorganisation. Some of the hospitals that were among the first in England to introducethe Bardex catheter did that through an authority innovation-decision (Rogers, 1995, p.372). While introducing the order codes for the Bardex catheter in the ordering system,they excluded the possibility to order traditional catheters.
Silo budgetingOne issue related to the diffusion of the Bardex catheter was also the problem ofevaluating the economic benefits of using the product. Compared with traditionalcatheters, the Bardex catheter was more expensive. Studies indicated, however, thatalthough the Bardex catheter would be more expensive per unit, it would still savemoney in the end, as it would reduce the risk for patients of contractinghealthcare-associated infections, and avoid unnecessary hospitalisation. Arguing forusing a new catheter that is more expensive than the ones currently in use also toucheson a generic problem of public healthcare and the nature of “saving” by improvinghealthcare. Although the use of the Bardex catheter might mean that unnecessary
IJPSM24,5
462
hospitalisation can be avoided, the savings are not clearly visible. The reason for this isbecause it is hard to measure the value of what is not spent. Also, what is unavoidablefor new products is that independent studies of economic benefits are not available(Williams and Bryan, 2007). One way of attaining evidence of economical benefits isthrough historical studies of the same care unit, where comparison between usage ofconventional catheters and Bardex catheters is possible (Rupp et al., 2004). It ishowever in the nature of such studies that they take time.
Another problem relates to the way budgets are organised. In some cases thepotential benefits of the introduction of the Bardex catheter would not be visible in thebudget affected by the increased spending on a more expensive catheter. Althoughtotal cost would be lower for the hospital, the incentives for a financial managerresponsible for a budget to accept a cost without gaining anything would be low.Similar experiences have been made by other companies attempting to introduceinnovations to the NHS. “[T]here is a major problem in gaining acceptance into theNHS due to budget silos – where the purchasing department bears the brunt of the costwhile the savings are passed onto another department” (Levinson, 2006, p. 10). Theseproblems related to the “separation of appraisal and resource allocation functions”have also been brought up by researchers (Williams and Bryan, 2007, p. 2127). Even ifit would be possible to establish the economic benefits (supported in, e.g. Rupp et al.,2004) from using Bardex catheters, it would still be impossible for a procurementdepartment which has not been provided with the means to cover the excess costassociated with the adoption of Bardex catheter. One way of removing this barrier, asreported in the interviews, was to internally fund the increased cost. This means thatresources were put aside to cover the extra cost associated with procuring the Bardexcatheter with a higher per-unit price in order to save money due to reduction in totalhospitalisation time.
Pricing, de-spending, and existing contractsIn one sense existing framework agreements also work as institutional barriers and,using Coriat and Weinstein’s (2002) classification, could be called a Type 2/Type B (i.e.endogenous, fixed-term) institutional barriers, i.e. the time delay imposed on adoptiondecisions as resources are tied in current contracts. Even if an adopting unit would liketo change catheter, they would generally wait until current contracts are about to bere-negotiated. One interviewee highlighted that the evaluation is not only about theBardex catheter versus traditional catheters. In an economic organisation there mightalso be other priorities or potentially beneficial activities to consider that wouldimprove the health service. This issue, more generally formulated, concerns theimportance of de-spending. Even in situations where there are sufficient levels ofevidence verifying that a new product is beneficial, the questions remains, what otheritem should be removed from the budget in order to allow for the introduction of thenew (Williams and Bryan, 2007, pp. 2125-2126). In that sense, diffusion has its ownversion of creative destruction.
Endogenous institutions and coordinationTable I summarises institutional barriers to the diffusion of the Bardex catheter intothe NHS, as found in the case study. The rightmost column in Table I lists suggestionsof coordination activities to negotiate the institutional barriers identified. These
Publicprocurement of
innovations
463
suggestions came out of the study, either through the interviews or through furtherconsultation of related literature. The list includes three institutional barriers where noclear-cut corresponding coordination activity was found. The fact that catheters ingeneral lack a natural champion is not easily remedied. De-spending is also a problemthat is not easily resolved. Although the third barrier might prompt attention to howcontracts are written, to deal with existing contracts suddenly becoming barriers fornew emerging products, is probably a very complex task. These are all aspects thatmay be addressed in future research.
Wards primarily provide care for patients – other tasks, such as procuring supplies,are given relatively less attention and are conducted in a routinised way. Procurementactivities leading to innovation, although possible, would in practice be exceptional.This makes perfectly sense if a ward is considered as a provider of health services only.Understanding a ward as an adopter of innovation gives reason to some furtherreflection (see Rolfstam, 2010). Routinisation of the procurement activities means thatproducts already in the digital order system, i.e. regular products, will benefit fromsome kind of de facto preference in comparison to products not included in the system.Unless some event occurs, e.g. that a contract expires, or that a new item is entered intothe system after a procurement process has been carried out, the range of availableproducts for wards is in principle static. Thus, unless something happen, the chancesof adopting new products are low.
From an institutional perspective, the setting up of the Rapid Review Panel was anattempt to create the necessary change, i.e. to re-design the institutional set-up definedby the NHS supply chain. Making the Bardex catheter available in the digital ordersystem was necessary, but not fully sufficient for diffusion as other institutions werealso at play. For instance, the organised scepticism among physicians is one suchinstitution. The benefits from organised scepticism are obvious for patient safety inrelation to introduction of new untried technology. Assuming that a certain technologyis actually safe and good, organised scepticism does work as an institutional barrier. Aclear technology champion had could have helped to negate such negativity but, due tothe way catheters are used in the organisation, such champions are unlikely to occurspontaneously.
The case provides lots of examples on institutions with different range (Jepperson,1991, p. 146). The institutional range of the Rapid Review Panel was for instancerelatively limited, as any hospital or trust could choose themselves whether or not tofollow the advice given by the panel. Apart from the decentralised decision-structure,other institutions in the organisations also contribute to the institutional set-up. Manyof these institutions stem from a general concern from public agencies to beaccountable for spending taxpayers’ money. The prevailing incentives structure thatcomes with that concern do not encourage managers to break their budgets or buyproducts with higher per unit price than existing options. It could also be seen thatinstitutional re-design by central management, either in the form of authorityinnovation decisions, or additional allocating of funds were common among the earlieradopters of the Bardex catheter.
Although some examples of institutional coordination and re-design identified herewere rather concrete, the case also includes institutional barriers that do not have aclear-cut countermeasure. Organised scepticism, for example, regarded above as aninstitutional barrier for innovation, is in general a good institution that should not be
IJPSM24,5
464
destroyed. The way forward for public procurers of innovation is probably anegotiation game, where one potential move would be to allocate resources for clinicaltests of new products. De-spending and the problem of getting out of existing contractsare other examples that appear problematic. How should managers know whatproducts they should exclude from the digital order system? And is it at all possible tobreak earlier made commitments just because a new competing product emerges? Howcan you know that an untried product is actually better than existing products? Toovercome these problems, the most promising way forward for public agencies is toengage in long term innovation planning and technology forecasting. This requires arather fundamental shift in how to look at public agencies in general. Public agenciesmust take on the role of competent buyers and drivers of innovation. In other words,they need to see public procurement of innovation as a way towards improvedperformance of the public services they are set up to deliver.
Concluding remarksThe paper focuses on a relatively neglected area, namely adoption and diffusion ofinnovations in public procurement. There are two main justifications forcountervailing that tendency. First, a better understanding of diffusion processes inrelation to public procurement of innovation may help to stimulate innovation,especially in those markets operated by innovative suppliers mainly addressing publicneeds. Second, a better understanding of diffusion processes may help managers tosustain a more efficient service by adopting new and better products.
The empirical findings underscore the importance of adopting a more holistic viewof public procurement of innovation. The case study revealed an array of institutionalbarriers that had an inhibiting affect on the diffusion of the procured item. These werebarriers that had to be dealt with in order for the procured item to diffuse into theorganisation. One basic implication of the case concerns the understanding of thepractice of procuring innovation as different from procurement of well-known regulargoods. The understanding of public procurement of innovation cannot be limited tosetting up the tender-procedure and awarding a winner. Resources must also be addedto coordinate and negotiate the institutional set-up in which the procured innovation isdiffused into. The value of an innovation may be considerably underutilised if noattention is paid to the diffusion of the innovation into the organisation.
Theoretically, this paper deals with innovation and diffusion as essentially a socialand interactive process, determined by institutions, which my or may not enablediffusion. Therefore, institutional coordination may at times be necessary in order toachieve diffusion. Although the perception of institutions as elements working ondifferent societal levels is well established in the literature, the paper also attempts tocounteract the tendency to limit institutional analysis of innovation to exogenouslevels. Often this means that the institutional analysis of public procurement ofinnovation boils down to analysis of the procurement law. By pinpointing barriershindering innovation and diffusion on other institutional levels, the limitations of suchnarrowly focused approaches becomes evident. In principle, all the institutionalbarriers discussed in this case belong to the endogenous level. This in turn justifies theclaim that institutional coordination and re-design should also take into accountendogenous levels.
Publicprocurement of
innovations
465
References
Arrowsmith, S. (2005), The Law of Public and Utilities Procurement, Sweet & Maxwell, London.
Borras, S. (2004), “System of innovation theory and the European Union”, Science and PublicPolicy, Vol. 31 No. 6, pp. 425-33.
Coriat, B. and Weinstein, O. (2002), “Organizations, firms and institutions in the generation ofinnovation”, Research Policy, Vol. 312, pp. 273-90.
Denscombe, M. (1998), The Good Research Guide for Small-scale Social Research Projects, OpenUniversity Press, Buckingham.
Department of Health (2002), “Getting ahead of the curve: a strategy for combating infectiousdiseases”, available at: http://image.guardian.co.uk/sys-files/Society/documents/2003/12/05/idstrategy2002.pdf (accessed 13 February 2007).
Department of Health (2003), “Winning ways. Working together to reduce healthcare-associatedinfection in England”, available at: www.dh.gov.uk/assetRoot/04/06/46/89/04064689.pdf(accessed 13 February 2007).
Department of Trade and Industry (2004), Department of Trade and Industry Five Year Program– Creating Wealth from Knowledge, DTI/Pub 7613/0.5k/11/04/NP, URN 04/1871.
Dosi, G., Freeman, C., Nelson, R., Silverberg, G. and Soete, L. (1988), Technical Change andEconomic Theory, Pinter Publishers, London and New York, NY.
EC (2004), A Report on the Functioning of Public Procurement Markets in the EU: Benefits fromthe Application of EU Directives and Challenges for the Future 03/02/2004, available at:http://ec.europa.eu/internal_market/publicprocurement/docs/public-proc-market-final-report_en.pdf (accessed 16 February 2007).
Edler, J. and Georghiou, L. (2007), “Public procurement and innovation – resurrecting thedemand side”, Research Policy, Vol. 36 No. 9, pp. 949-63.
Edler, J., Ruhland, S., Hafner, S., Rigby, J., Georghiou, L., Hommen, L., Rolfstam, M., Edquist, C.,Tsipouri, L. and Papadakou, M. (2005), Review of Issues at Stake: Study for the EuropeanCommission, Fraunhofer ISI, Karlsruhe.
Edmondson, A.C., Bohmer, R.M. and Pisano, G.P. (2001), “Disrupted routines: team learning andnew technology implementation in hospitals”, Administrative Science Quarterly, Vol. 46No. 4, pp. 685-716.
Edquist, C. and Johnson, B. (1997), “Institutions and organizations in systems of innovation”,in Edquist et al. (1997).
Edquist, C., Hommen, L. and Tsipouri, L. (Eds) (2000), Public Technology Procurement andInnovation, Kluwer Academic, Dordrecht.
Edquist, C., Hommen, L., Johnson, B., Lemola, T., Malerba, F., Reiss, T. and Smith, K. (1998), TheISE Policy Statement: The Innovation Policy Implications of the ‘Innovation Systems andEuropean Integration’ Research Project, Unitryck, University of Linkoping Press,Linkoping.
Eisenhardt, K.M. (1989), “Building theories from case study research”, The Academy ofManagement Review, Vol. 14 No. 4, pp. 532-50.
Emmerson, A.M., Enstone, J.E., Griffin, M., Kelsey, M.C. and Smyth, E.T.M. (1996), “The secondnational prevalence survey of infection in hospitals – overview of the results”, Journal ofHospital Infection, Vol. 32, pp. 175-90.
European Commission (2005), Implementing the Community Lisbon Programme: More Research andInnovation – Investing for Growth and Employment: A Common Approach, COM 2005: 488.
Freeman, C. (1982), The Economics of Industrial Innovation, MIT Press, Cambridge, MA.
IJPSM24,5
466
Gregersen, B. (1992), “The public sector as a pacer in national systems of innovation”,in Lundvall, B.-A. (Ed.), National Systems of Innovation. Towards a Theory of Innovationand Interactive Learning, Pinter Publishers, London.
Hall, B. (2005), “Innovation and diffusion”, in Fagerberg, J., Mowery, D. and Nelson, R. (Eds),The Oxford Handbook of Innovation, Oxford University Press, Oxford.
Health Protection Agency (2006), Rapid Review Panel, available at: www.hpa.org.uk/infections/topics_az/rapid_review/default.htm (accessed 17 October 2006).
Hollingsworth, J.R. (2000), “Doing institutional analysis: implications for the study ofinnovations”, Review of International Political Economy, Vol. 7 No. 4, pp. 595-644.
Hommen, L. and Rolfstam, M. (2009), “Public procurement and innovation: towards a taxonomy”,Journal of Public Procurement, Vol. 9 No. 1.
Jacoby, S.M. (1990), “The new institutionalism: what can it learn from the old?”, IndustrialRelations, Vol. 29, p. 2.
Jepperson, R.J. (1991), “Institutions, institutional effects, and institutionalism”, in Powell, W.W.and DiMaggio, P.J. (Eds), The New Institutionalism in Organizational Analysis, TheUniversity of Chicago Press, Chicago, IL and London, pp. 1-38.
Johnson, B. (1992), “Institutional learning”, in Lundvall, B.-A. (Ed.), National Systems of Innovation.Towards a Theory of Innovation and Interactive Learning, Pinter Publishers, London.
Levinson, O. (2006), “The whiz clean catch the rocky road to marketing an innovative product intothe NHS. Procuring for Healthcare 2006 Investing in Innovation”, HES Magazine, June.
Lissoni, F. and Metcalfe, S. (1996), “Diffusion of innovation ancient and modern: a review of themain themes”, in Dodgson, M. and Rothwell, R. (Eds), Handbook of Industrial Innovation,Edward Elgar, London.
Lister, S. (2004), “NHS is world’s biggest employer after Indian Rail and Chinese Army”,Timesonline, 20 March, available at: www.timesonline.co.uk/tol/news/uk/health/article1050197.ece (accessed 25 February 2008).
Lundvall, B.-A. (Ed.) (1992), National Systems of Innovation. Towards a Theory of Innovation andInteractive Learning, Pinter Publishers, London.
Lundvall, B.-A. and Borras, S. (2005), “Science, technology and innovation policy”,in Fagerberg, J., Mowery, D. and Nelson, R. (Eds), The Oxford Handbook of Innovation,Oxford University Press, Oxford.
Maidique, M.A. (1980), “Entrepreneurs, champions and technological innovation”, SloanManagement Review, Winter.
Miles, M.B. and Huberman, M.A. (1994), Qualitative Data Analysis: An Expanded Sourcebook,2nd ed., Sage, Thousand Oaks, London, New Delhi.
NHS PASA (2008), NHS Procurement, available at: www.pasa.nhs.uk/PASAWeb/NHSprocurement/AboutNHSPASA/LandingPage.htm (accessed 25 February 2008).
Nyholm, J., Lars, N., Frelle-Petersen, C., Riis, M. and Torstensen, P. (2001), “Innovation policy in theknowledge-based economy – can theory guide policy making?”, in Archibugi, D. andLundvall, B.-A. (Eds), The Globalizing Learning Economy, Oxford University Press, Oxford.
Plowman, R., Graves, N., Griffin, M.A., Roberts, J.A., Swan, A.V., Cookson, B. and Taylor, L.(2001), “The rate and cost of hospital-acquired infections occurring in patients admitted toselected specialities of a district general hospital in England and the national burdenimposed”, Journal of Hospital Infection, Vol. 47, pp. 198-209.
Publicprocurement of
innovations
467
Pratt, R.J. and O’Malley, B.O. (2007), “Supporting evidence-based infection prevention andcontrol practice in the National Health Service in England. The NHS/TVU/intuitionapproach”, Journal of Hospital Infection, Vol. 65 No. 52, pp. 142-7.
Pratt, R.J., Pellowe, C.M., Wilson, J.A., Loveday, H.P., Harper, P.J., Jones, S.R.L.J., McDougall, C.and Wilcox, M.H. (2007), “epic2: National Evidence-Based Guidelines for PreventingHealthcare-Associated Infections in NHS Hospitals in England”, Journal of HospitalInfection, Vol. 65 No. 52, pp. S1-S64.
Robinson, P.J., Faris, C.W. and Wind, Y. (1967), Industrial Buying and Creative Marketing, Allyn& Bacon, Boston, MA.
Rogers, E.M. (1995), Diffusion of Innovations, 4th ed., The Free Press, New York, London,Toronto, Sydney, Tokyo, Singapore.
Rolfstam, M. (2005), “Public technology as a demand-side innovation policy instrument –an overview of recent literature and events”, paper presented at DRUID WinterConference, Skoerping/ Aalborg, Denmark.
Rolfstam, M. (2007), “Organisations and institutions in public procurement of innovations:the case of the Energy Centre in Bracknell Forest”, paper presented at UK DRUID WinterConference, Skoerping, Aalborg, Denmark.
Rolfstam, M. (2009), “Public procurement as an innovation policy tool: the role of institutions”,Science and Public Policy, Vol. 36 No. 5, June.
Rolfstam, M. (2010), “A tentative model of a demand system for public procurement ofinnovation”, Proceedings of the International Public Procurement Conference, Seoul, SouthKorea, 26-28 August 2010.
Rothwell, R. (1994), “Issues in user-producer relations in the innovation process: the role ofgovernment”, Int. J. Technology Management, Vol. 9 Nos 5-7.
Rupp, M.E., Fitzgerald, T., Marion, N., Helget, V., Puumala, S., Anderson, J.R. and Fey, P.D.(2004), “Effect of silver-coated urinary catheters: efficiency, cost-effectiveness, andantimicrobial resistance”, American Journal of Infection Control, Vol. 32 No. 8.
Utterback, J.M. (1994), Mastering the Dynamics of Innovation: How Companies Can SeizeOpportunities in the Face of Technological Change, MIT Press, Boston, MA.
Uyarra, E. and Flanagan, K. (2010), “Understanding the innovation impacts of publicprocurement”, European Planning Studies, Vol. 18, pp. 123-43.
Williams, I.P. and Bryan, S. (2007), “Cost-effectiveness analysis and formulary decision makingin England: findings from research”, Social Science and Medicine, Vol. 65, pp. 2116-29.
Yin, R.K. (1994), Case Study Research, Design and Methods, 2nd ed., Sage Publications, NewburyPark, CA.
Further reading
Edquist, C. (Ed.) (1997), Systems of Innovation – Technologies, Institutions and Organizations,Pinter, London and Washington, DC.
Fagerberg, J., Mowery, D. and Nelson, R. (Eds) (2005), The Oxford Handbook of Innovation,Oxford University Press, Oxford.
Corresponding authorMax Rolfstam can be contacted at: [email protected]
IJPSM24,5
468
To purchase reprints of this article please e-mail: [email protected] visit our web site for further details: www.emeraldinsight.com/reprints