Thorax, 1978, 33, 603-607 Pulmonary manifestations of hypogammaglobulinaemia RUSSELL J DUKES, EDWARD C ROSENOW III, AND PAUL E HERMANS From the Division of Thoracic Diseases and Internal Medicine and the Division of Infectious Diseases and Internal Medicine, Mayo Clinic and Mayo Foundation, Rochester, Minnesota, USA Dukes, R J, Rosenow, E C III, and Hermans, P E (1978). Thorax, 33, 603-607. Pulmonary manifestations of hypogammaglobulinaemia. Fifty-five patients with late-onset idiopathic immunoglobulin deficiency were studied and upper or lower respiratory tract infections were encountered in about 90%. Cylindrical bronchiectasis was shown in all of the 21 patients in whom bronchograms were done. A thymoma was found in four patients. Three patients had diffuse interstitial pulmonary disease-two with proved and one with presumed lymphocytic interstitial pneumonitis. Five patients had no evidence of pulmonary disease, including two patients with long-standing late-onset immunoglobulin deficiency who had essentially no serum immunoglobulins. This small subgroup of patients with immunoglobulin deficiency without severe pulmonary infections cannot be explained in the context of current understanding of immunoglobulin deficiency. Thirty-two patients were followed up for long enough for the response to treatment to be assessed. Idiopathic late-onset immunoglobulin deficiency or variable immune deficiency was defined by an expert committee of the World Health Organisa- tion in 1971. Patients with this disorder acquire abnormally low concentrations of serum immuno- globulins and experience recurrent infections starting several years after birth but have no underlying demonstrable disease to which the immunoglobulin deficiency can be attributed (Fundenberg et al, 1971). Because respiratory symptoms are the most common presenting com- plaint in late-onset immunoglobulin deficiency, we undertook a review of our clinical experience and chest radiographs. We studied 55 patients with this disorder to evaluate the spectrum of chest disease. Material and methods In this retrospective study, data on 55 patients (29 male and 26 female) were analysed. The earliest onset of symptoms was at the age of 7 years and the latest at age 67, the mean being 30 years (male 27, female 35). The mean age at which a definite diagnosis was made, however, was 41-9 years (male 38-6, female 45 7). All patients save one were white; this distribution reflects a bias introduced by our patient population. The specific criteria used in diagnosing late-onset im- munoglobulin deficiency and the methods used for quantitative measurement of the serum immuno- globulins and for serum protein electrophoresis have been reported (Hermans et al, 1976). The lower limit of normal for y-globulin at our insti- tution is 0-8 g/dl. The lower limits of normal for IgA, IgG, and IgM are 0-3, 6-4, and 0-2 mg/ml respectively. Since almost all of these patients were seen by one of us, the treatment was fairly consistent and included y-globulin injections and antibiotics. Commercial pooled human y-globulin was given by intramuscular injections as a loading dose of 60 ml and then either 20 or 30 ml intramuscularly, according to the patient's weight, once a month thereafter. The antibiotic regimen usually con- sisted of tetracycline or ampicillin, 500 mg four times a day for one week in alternating fashion with a rest period of one week in between. It must be emphasised that each patient's treatment was somewhat different, depending on the severity of his disease. Specifically, patients who had only minor respiratory infections received only anti- biotics initially until the severity of the infection warranted the use of y-globulin. Most patients were instructed in the techniques 603 on 16 June 2019 by guest. Protected by copyright. http://thorax.bmj.com/ Thorax: first published as 10.1136/thx.33.5.603 on 1 October 1978. Downloaded from
Transcript
Thorax, 1978, 33, 603-607
Pulmonary manifestations ofhypogammaglobulinaemiaRUSSELL J DUKES, EDWARD C ROSENOW III, AND PAUL E HERMANS
From the Division of Thoracic Diseases and Internal Medicine and the Division of Infectious Diseasesand Internal Medicine, Mayo Clinic and Mayo Foundation, Rochester, Minnesota, USA
Dukes, R J, Rosenow, E C III, and Hermans, P E (1978). Thorax, 33, 603-607. Pulmonarymanifestations of hypogammaglobulinaemia. Fifty-five patients with late-onset idiopathicimmunoglobulin deficiency were studied and upper or lower respiratory tract infections wereencountered in about 90%. Cylindrical bronchiectasis was shown in all of the 21 patients inwhom bronchograms were done. A thymoma was found in four patients. Three patients haddiffuse interstitial pulmonary disease-two with proved and one with presumed lymphocyticinterstitial pneumonitis. Five patients had no evidence of pulmonary disease, including twopatients with long-standing late-onset immunoglobulin deficiency who had essentially noserum immunoglobulins. This small subgroup of patients with immunoglobulin deficiencywithout severe pulmonary infections cannot be explained in the context of currentunderstanding of immunoglobulin deficiency. Thirty-two patients were followed up for longenough for the response to treatment to be assessed.
Idiopathic late-onset immunoglobulin deficiencyor variable immune deficiency was defined by anexpert committee of the World Health Organisa-tion in 1971. Patients with this disorder acquireabnormally low concentrations of serum immuno-globulins and experience recurrent infectionsstarting several years after birth but have nounderlying demonstrable disease to which theimmunoglobulin deficiency can be attributed(Fundenberg et al, 1971). Because respiratorysymptoms are the most common presenting com-plaint in late-onset immunoglobulin deficiency, weundertook a review of our clinical experience andchest radiographs. We studied 55 patients with thisdisorder to evaluate the spectrum of chest disease.
Material and methods
In this retrospective study, data on 55 patients (29male and 26 female) were analysed. The earliestonset of symptoms was at the age of 7 years andthe latest at age 67, the mean being 30 years(male 27, female 35). The mean age at which adefinite diagnosis was made, however, was 41-9years (male 38-6, female 45 7). All patients saveone were white; this distribution reflects a biasintroduced by our patient population. The
specific criteria used in diagnosing late-onset im-munoglobulin deficiency and the methods used forquantitative measurement of the serum immuno-globulins and for serum protein electrophoresishave been reported (Hermans et al, 1976). Thelower limit of normal for y-globulin at our insti-tution is 0-8 g/dl. The lower limits of normal forIgA, IgG, and IgM are 0-3, 6-4, and 0-2 mg/mlrespectively.
Since almost all of these patients were seen byone of us, the treatment was fairly consistent andincluded y-globulin injections and antibiotics.Commercial pooled human y-globulin was givenby intramuscular injections as a loading dose of60 ml and then either 20 or 30 ml intramuscularly,according to the patient's weight, once a monththereafter. The antibiotic regimen usually con-sisted of tetracycline or ampicillin, 500 mg fourtimes a day for one week in alternating fashionwith a rest period of one week in between. It mustbe emphasised that each patient's treatment wassomewhat different, depending on the severity ofhis disease. Specifically, patients who had onlyminor respiratory infections received only anti-biotics initially until the severity of the infectionwarranted the use of y-globulin.Most patients were instructed in the techniques
603
on 16 June 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.33.5.603 on 1 October 1978. D
Russell J Dukes, Edward C Rosenow Ill, and Paul E Hermans
of postural drainage and physiotherapy to thechest. The presence of cough, sputum production,and documented episodes of pneumonia were re-corded. Each symptom was described as none,mild, moderate, or severe. Cough and sputum pro-duction were called moderate if the patient com-plained of them spontaneously, as severe if thepatient woke with them at night, and mild if theywere simply elicited during the review of systems.Susceptibility to pneumonia was graded as fol-lows: none, when there were no recurrent episodesof pneumonia in one year; mild, one episode ayear; moderate, two to four episodes a year; andsevere, five or more episodes a year.
Result
RESPIRATORY SYMPTOMSThe severity of cough and sputum production andthe number of episodes of pneumonia a year atthe time of diagnosis are summarised in table 1.Forty-one (75%) of our patients had an initialcomplaint of cough, 39 (71%) had sputum pro-duction, and 41 (75%) had a history of recurrentpneumonia. Other presenting symptoms includeddyspnoea on exertion in 13 (24%), haemoptysis ineight (15%), and asthmatic bronchitis in one (2%).Five patients (9%) denied that they had ever hadany respiratory symptoms or episodes of pneu-monia; three of these patients had symptoms ofchronic sinusitis.
Table 1 Signs and symptoms at time of diagnosis in55 patients
Of 33 patients available for follow-up, 32 weretreated according to the above regimen. Thefollow-up period ranged from four months to 19years, with an average of two years. No com-
parison can be made between treated and un-treated groups, but the effect of treatment was
evaluated on the basis of complaints by comparingthe severity of complaints before and during treat-ment. Table 2 shows that patients tended to im-
*Results are measured by evaluation of symptoms before and duringtreatment.
prove with treatment. Of the 16 patients whocomplained of five or more episodes of pneumoniaa year before treatment, only one patient had thismany episodes of pneumonia during treatment.A total of 15 patients had complete pulmonary
function tests. The results usually showed a pat-tern of airways obstruction and did not correlatewell with other indicators of the severity of thedisease.
CHEST RADIOGRAPHSWe reviewed all chest radiographs (table 3). Sevenpatients (13%) had normal and 48 (87%) had ab-normal chest films. Thymoma was present in fourpatients (two were spindle cell, one was lympho-cytic, and one was of unknown type). Diffuseinterstitial pulmonary disease was noted in threepatients; in two of these lymphocytic interstitialpneumonitis was proved by biopsy, and in theother this diagnosis was thought possible on thebasis of radiographic findings only. Bronchogramswere done on most patients who expectoratedcopious amounts of purulent sputum. Bronchi-ectasis was found in all 21 so examined. Thebronchiectasis was all of the cylindrical type, andin most of these cases it affected both lower lobes.No saccular bronchiectasis was seen. Changes suchas localised fibrosis, focal areas of atelectasis, orapical thickening were present on the chest filmsof the other patients. One patient had squamouscell carcinoma of the lung. No case of pleuraleffusion, lung abscess, or pneumothorax was foundbut four patients had a history of empyema.
Table 3 Chest radiographic findings in 55 patients (%)
Pulmonary manifestations of hypogammaglobulinaemia
LYMPHOCYTIC INTERSTITIAL PNEUMONITIS ANDHYPOGAMMAGLOBULINAEMIATwo patients had diffuse pulmonary disease withthe finding of lymphocytic interstitial pneumonitison open lung biopsy. A third patient had similarfindings on the chest radiograph, but no biopsywas performed.
Case IA 38-year-old white woman with a long history ofsinusitis and frequent upper respiratory infectionscame for evaluation of lymphadenopathy; biopsyof a lymph node showed only hyperplasia. Thechest film, which had been normal two yearsbefore, showed diffuse bilateral infiltration. Anopen lung biopsy showed interstitial pneumonitiswith scattered interstitial lymphoid follicles. Re-sults of all cultures were negative. Serum proteinelectrophoresis showed the following (normalrange in parentheses): albumin 4-10 g/dl (3 5 to4 7); a,-globulin 0 37 g/dl (0-2 to 0-5); a2-globulin054 g/dl (05 to 08); B-globulin 0171 g/dl (0-7to 1-3); y-globulin 0-20 g/dl (0-8 to 1-6); andtotal proteins 5-92 g/dl. Immunoglobulinsmeasured: IgM 00 mg/ml (0-2 to 1-4); IgA 00mg/ml (013 to 3 0); IgG 017 mg/ml (6-4 to 14-3);and IgE less than 5 ng/ml (6 to 780).The patient was treated with monthly injections
of 30 ml of y-globulin, alternating courses of anti-biotics, and prednisone-initially 40 mg/day andtapered over a few months to a maintenancedosage of 5 mg twice daily. When last seen 14years later in 1977 she was still on this regimen,and the chest radiograph was normal. The fre-
quency of respiratory infections was less. Pul-monary function is compared below (normal inparentheses).
Case 2A 38-year-old white woman had a long history of
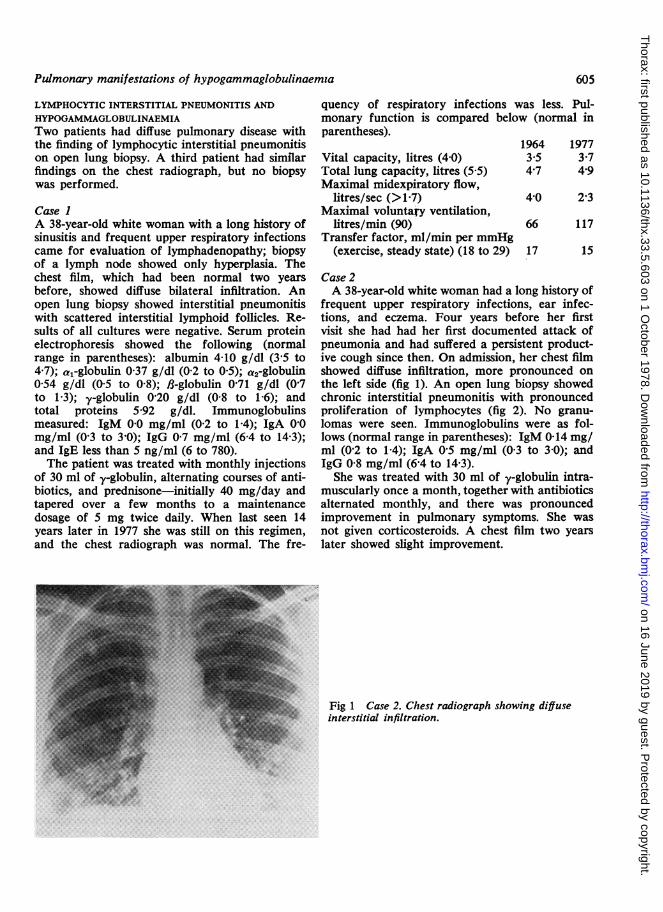
frequent upper respiratory infections, ear infec-tions, and eczema. Four years before her firstvisit she had had her first documented attack ofpneumonia and had suffered a persistent product-ive cough since then. On admission, her chest filmshowed diffuse infiltration, more pronounced onthe left side (fig 1). An open lung biopsy showedchronic interstitial pneumonitis with pronouncedproliferation of lymphocytes (fig 2). No granu-lomas were seen. Immunoglobulins were as fol-lows (normal range in parentheses): IgM 0-14 mg/ml (0-2 to 1-4); IgA 05 mg/ml (0-3 to 3 0); andIgG 0-8 mg/ml (6-4 to 14-3).She was treated with 30 ml of y-globulin intra-
muscularly once a month, together with antibioticsalternated monthly, and there was pronouncedimprovement in pulmonary symptoms. She wasnot given corticosteroids. A chest film two yearslater showed slight improvement.
Fig 1 Case 2. Chest radiograph showing diffuseinterstitial infiltration.
605
on 16 June 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.33.5.603 on 1 October 1978. D
Russell J Dukes, Edward C Rosenow III, and Paul E Hermans
Fig 2 Case 2. Open lung biopsyspecimen showing chronicinterstitial pneumonitis withpronounced lymphocyticproliferation (Haematoxylin andeosin X400).
....-qiii
Discussion
Late-onset idiopathic immunoglobulin deficiencyis diagnosed after exclusion of conditions that maylead to secondarily low immunoglobulin concentra-tions. Lymphocytic lymphoma, chronic lympho-cytic leukaemia, multiple myeloma, nephroticsyndrome, and protein-losing enteropathy (Asher-son, 1975) must be ruled out.
In addition to recurrent infections, individualswith late-onset hypogammaglobulinaemia arepredisposed to other diseases. These includelymphoreticular neoplasms, carcinomas, atrophicgastritis, diarrhoea with or without malabsorption,nodular lymphoid hyperplasia of the small bowel,cholelithiasis, giardiasis, lymphocytic interstitialpneumonia, thymomas, and thyroid abnormalities(Gafni et al, 1960; Hermans et al, 1976).Of our patients with hypogammaglobulinaemia
91% had respiratory symptoms, and 87% hadabnormal chest radiographs. Treatment with anti-biotics and y-globulin injections resulted in sub-jective improvement in respiratory symptoms inmost patients. A loading dose of 60 ml of .y-globu-lin was injected intramuscularly over a period ofthree days followed by a maintenance dosage of20 to 30 ml once a month. Since Haemophilusinfluenzae, Streptococcus (Diplococcus) pneu-
moniae, and Streptococcus pyogenes are the pre-dominant pathogens in immunoglobulin-deficientpatients, ampicillin is the antibiotic of first choice.Ampicillin-resistant strains of H influenzae requirechloramphenicol.
The absence of necrotising pulmonary infectionsleading to abscess formation suggested that anaero-bic micro-organisms and the Enterobacteria donot play an important part in the respiratory in-fections of patients with hypogammaglobulin-aemia. Apparently, host defence mechanismsother than immunoglobulins offer adequate pro-tection against these infectious agents. Of specialinterest were the five patients who had markedlylow -y-globulin concentrations but no recurrentrespiratory tract infections.Immune defences of the lung have recently
been reviewed (Kaltreider, 1976). Why some ex-ceptional patients can have extremely low serumconcentrations of immunoglobulins without anincreased susceptibility to infection while mostpatients with a similar degree of immunoglobulindeficiency are severely affected by recurrent in-fections remains an enigma. Several mechanismsshould be considered to explain the paradox en-countered in two of our patients. Some patientswith serum immunoglobulin deficiency may havea relatively intact secretory immunoglobulinsystem. One patient with an intact secretorysystem dissociated from systemic immunoglobulindeficiency has been reported (Spitler et al, 1973).Alternatively, a compensatory mechanism involv-ing other components of the immune system mayprotect such patients. A third hypothesis is thatpatients with significantly lowered immunoglobu-lins and recurrent infection also lack another, asyet undefined, essential component of host defencemechanisms. Preliminary studies in one of our
606
on 16 June 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.33.5.603 on 1 October 1978. D
Pulmonary manifestations of hypogammaglobulinaemia
two patients with severe immunoglobulin defici-ency but without increased susceptibility to infec-tion have shown that the secretory system of thispatient also lacks the ability to produce IgA (bycourtesy of Dr Tomasi, Department of Im-munology).
Also of interest are the two patients withdocumented and a third with suspected lympho-cytic interstitial pneumonitis. Liebow and Carring-ton (1973) have also noted this association. Littleis known about this disorder. It would be ofspecial interest to know whether these lympho-cytes are of B-cell or T-cell origin. We arecurrently reviewing our experience with alllymphocytic interstitial pneumonitis unrelated toimmunoglobulin deficiency. The clinical course ofthe interstitial pneumonitis in the two patients re-ported here is less progressive than that of theothers we have seen. In fact, the clearing of thediffuse infiltration on the chest film in case 1 ismost unusual.
Several mechanisms of pathogenesis for late-onset immune deficiency have been proposed.Most recently, Waldmann et al (1974) have foundthat some patients have a population of "suppres-sor" T cells that appear to interfere with thematuration of B cells into immunoglobulin-secreting plasma cells. Other reports have em-phasised that the defect may reside at variousstages of B-cell development, the common de-nominator being decreased immunoglobulin pro-duction (Choi et al, 1972; Geha et al, 1974).
peripheral-blood lymphocytes in severe hypogamma-globulinaemia. Lancet, 1, 1149-1151.
Fudenberg, H, Good, R A, Goodman, H C, Hitzig,W, Kunkel, H G, Roitt, I M, Rosen, F S, Rowe,D S, Seligmann, M, and Soothill, J R (1971).Primary immunodeficiencies: report of a WorldHealth Organisation committee. Pediatrics, 47, 927-946.
Gafni, J, Michaeli, D, and Heller, H (1960). Idio-pathic acquired agammaglobulinemia associatedwith thymoma: report of two cases and review ofthe literature. New England Journal of Medicine,263, 536-541.
Geha, R S, Schneeberger, E, Merler, E, and Rosen,F S (1974). Heterogeneity of "acquired" or com-mon variable agammaglobulinemia. New EnglandJournal of Medicine, 291, 1-6.
Hermans, P E, Diaz-Buxo, J A, and Stobo, J D(1976). Idiopathic late-onset immunoglobulin de-ficiency: clinical observations in 50 patients. Ameri-can Journal of Medicine, 61, 221-237.
Kaltreider, H B (1976). Expression of immune mech-anisms in the lung. American Review of Respira-tory Disease, 113, 347-379.
Liebow, A A, and Carrington, C B (1973). Diffusepulmonary lymphoreticular infiltrations associatedwith dysproteinemia. Medical Clinics of NorthAmerica, 57, 809-843.
Spitler, L E, Levin, A S, and Fudenberg, H H (1973).Agammaglobulinemia, absent delayed sensitivityand lymphopenia without infections: a demonstra-tion of immunologic unknowns. American Journalof Medicine, 54, 371-377.
Waldmann, T A, Durm, M, Broder, S, Blackman, M,Blaese, R M, and Strober, W (1974). Role of sup-pressor T cells in pathogenesis of common variablehypogammaglobulinaemia. Lancet, 2, 609-613.
References
Asherson, G L (1975). Immunodeficiency disorders.Practitioner, 214, 494-501.
Choi, Y S, Biggar, W D, and Good, R A (1972).Biosynthesis and secretion of immunoglobulins by
Requests for reprints to: Dr E C Rosenow III, MayoClinic, 200 First Street SW, Rochester, MN 55901,USA.
607
on 16 June 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.33.5.603 on 1 October 1978. D