Pulsatile tinnitus Aristides Sismanis, MD, FACS Department of Otolaryngology—Head and Neck Surgery, Medical College of Virginia/Virginia Commonwealth University, PO Box 980146, 1201 East Marshall Street, Suite 402, Richmond, VA 23298, USA Pulsatile tinnitus (PT) usually originates from vascular structures within the cranial cavity, head, and neck region, and the thoracic cavity either by increased blood flow or lumen stenosis. Pulsatile tinnitus can be classified either as arterial or venous according to the vessel of origin, and dif- ferentiation between these two types can be made easily by applying light digital pressure over the ipsilateral internal jugular vein (IJV). This ma- neuver has no effect on the intensity of the arterial type, whereas it makes the venous type subside immediately. Venous PT can originate not only from primary venous anomalies, but also from conditions causing increased intracranial pressure and transmission of arterial pulsations to the dural venous sinuses [1]. Classification of PT as objective or subjective is based on whether it is audible by both patient and examiner or only by the patient. Nonvascular PT is very rare and originates from sources other than vascular. Arterial etiologies Atherosclerotic carotid artery disease Atherosclerotic carotid artery disease (ACAD) is a common cause of PT in patients older than 50 years of age, especially when associated with certain risk factors, such as atherosclerosis, hypertension, angina, hyperlipidemia, diabetes mellitus, or smoking. Objective PT can be the first manifestation of ACAD in these patients [2]. PT in such cases is secondary to bruits produced by turbulent blood flow at stenotic segments of the carotid artery. In a series of 12 patients with PT secondary to ACAD, an ipsilateral carotid bruit was present in all of them [2]. Diagnosis can be established by Otolaryngol Clin N Am 36 (2003) 389–402 E-mail address: [email protected]0030-6665/03/$ - see front matter Ó 2003, Elsevier Science (USA). All rights reserved. doi:10.1016/S0030-6665(02)00169-X
Transcript
Pulsatile tinnitus
Aristides Sismanis, MD, FACSDepartment of Otolaryngology—Head and Neck Surgery,
Medical College of Virginia/Virginia Commonwealth University, PO Box 980146,
1201 East Marshall Street, Suite 402, Richmond, VA 23298, USA
Pulsatile tinnitus (PT) usually originates from vascular structures withinthe cranial cavity, head, and neck region, and the thoracic cavity either byincreased blood flow or lumen stenosis. Pulsatile tinnitus can be classifiedeither as arterial or venous according to the vessel of origin, and dif-ferentiation between these two types can be made easily by applying lightdigital pressure over the ipsilateral internal jugular vein (IJV). This ma-neuver has no effect on the intensity of the arterial type, whereas it makesthe venous type subside immediately. Venous PT can originate not onlyfrom primary venous anomalies, but also from conditions causingincreased intracranial pressure and transmission of arterial pulsations tothe dural venous sinuses [1].
Classification of PT as objective or subjective is based on whether it isaudible by both patient and examiner or only by the patient. NonvascularPT is very rare and originates from sources other than vascular.
Arterial etiologies
Atherosclerotic carotid artery disease
Atherosclerotic carotid artery disease (ACAD) is a common cause of PT inpatients older than 50 years of age, especiallywhen associatedwith certain riskfactors, such as atherosclerosis, hypertension, angina, hyperlipidemia,diabetes mellitus, or smoking. Objective PT can be the first manifestation ofACAD in these patients [2]. PT in such cases is secondary to bruits producedby turbulent blood flow at stenotic segments of the carotid artery.
In a series of 12 patients with PT secondary to ACAD, an ipsilateralcarotid bruit was present in all of them [2]. Diagnosis can be established by
0030-6665/03/$ - see front matter � 2003, Elsevier Science (USA). All rights reserved.
doi:10.1016/S0030-6665(02)00169-X
duplex ultrasound studies [2]. In cases suspected of intracranial atheroscle-rotic vascular disease, head MR angiography (MRA) can be very useful.Another common cause of arterial PT in middle-aged individuals is atortuous internal carotid artery or intracranial vessels.
Intracranial vascular abnormalities
Intracranial vascular abnormalities are uncommon etiologies of tinnitus;however, misdiagnosis may lead to catastrophic consequences for the pa-tient. In the author’s experience, the most common abnormality has beendural arteriovenous fistulae (AVFs). Aneurysms, with the exception ofdissecting aneurysms of the internal carotid and vertebral arteries, do notpresent with PT.
Dural AVFs comprise approximately 15% of intracranial arteriovenousmalformations (AVMs) and usually become symptomatic during the fifth orsixth decades of life [3,4]. The transverse and sigmoid dural sinuses are themost common sites involved, followed by the cavernous sinus. In contrast toAVMs, AVFs are usually acquired and thought to result from dural venoussinus thrombosis. Thrombosis may be spontaneous or secondary to trauma,obstructing neoplasm, surgery, and infection. As the thrombosed segmentrecanalizes, ingrowth of dural arteries takes place and artery-to-sinusanastomoses are formed [3]. PT in these patients is of the arterial type and isassociated with a bruit over the involved dural sinus and objective PT.
The mortality from hemorrhage of dural AVFs has been reportedbetween 10% and 20% [3]. In cases with retrograde drainage into the corti-cal veins, the chance of subarachnoid or parenchymal hemorrhage is muchhigher [3].
Dissecting aneurysms are rare and more often involve the internalauditory canal (ICA) and less often the vertebral artery. Manifestationsinclude PT, pain, transient ischemic attacks, cranial neuropathies, Horner’ssyndrome, and subarachnoid hemorrhage [3]. Sudden head rotation,especially when accompanied by extension (ie, the tennis ‘‘ace serve’’), isthe most likely precipitating event [5]. Fibromuscular dysplasia, variousarteriopathies, such as Marfan syndrome, and osteogenesis imperfecta arepredisposing factors. The various arterial PT etiologies are as follows:
1. ACAD [2]2. Intracranial and extracranial arteriovenous malformations [6–8]3. Dural arteriovenous fistulas and aneurysms [7–10]4. Atherosclerotic subclavian artery disease [11]5. Atherosclerotic occlusion of the contralateral common carotid artery
390 A. Sismanis / Otolaryngol Clin N Am 36 (2003) 389–402
10. External carotid artery stenosis [19]11. Ectopic intratympanic carotid artery [20–22]12. Persistent stapedial artery [23]13. Aberrant artery in the stria vascularis [24]14. Vascular compression of the eighth nerve [25]15. Increased cardiac output (anemia, thyrotoxicosis, or pregnancy) [26,27]16. Aortic murmurs [28]17. Paget’s disease [9,29,30]18. Otosclerosis [31]19. Hypertension, antihypertensive agents [31]20. Vascular neoplasms of skull base and temporal bone [32–35]21. Tortuous carotid and vertebral arteries [36]
Venous etiologies
Pseudotumor cerebri syndrome
Pseudotumor cerebri syndrome has been in the author’s experience themost common etiology of venous PT in young and obese female patients.This syndrome is characterized by increased intracranial pressure withoutany focal signs of neurologic dysfunction with the exception of occasionalfifth, sixth, and seventh cranial nerve palsies [37]. Synonyms of this entityinclude benign intracranial hypertension syndrome and idiopathic intra-cranial hypertension.
Diagnosis is made by exclusion of lesions producing intracranial hyper-tension, such as mass lesions, obstructive hydrocephalus, and venous sinusocclusion. Pseudotumor cerebri syndrome is of unknown etiology; however,it has been associated with various medical conditions and intake of certainmedications. Conditions associated with pseudotumor cerebri syndromeinclude the following [38]:
In most patients, this syndrome has a benign and self-limiting course;however, in 25% of patients it may become chronic [37].
The exact pathophysiology of this syndrome remains unclear; however,increased resistance to cerebrospinal fluid (CSF) absorption resulting ininterstitial brain edema is suspected [38]. Increased intracranial venouspressure secondary to elevated intra-abdominal, pleural, and cardiac fillingpressures has been documented in patients with central obesity and asso-ciated pseudotumor cerebri [39–41]. These findings are in accordance withthe concept of increased resistance to CSF absorption as etiology of pseudo-tumor cerebri syndrome.
Although the classic presentation of pseudotumor cerebri syndromeconsists of headaches or visual disturbances, PT alone or in association withhearing loss, dizziness, and aural fullness has been recognized as the mainmanifestation of this syndrome [1,42–46]. Many of these patients aremorbidly obese (body weight more than 100 lb above ideal weight) and haveassociated papilledema. It has been well documented that absence ofpapilledema does not exclude this entity [34,47,48]. This is very importantinformation because some neurologists may decline lumbar puncture andCSF pressure measurement in PT patients suspicious for pseudotumorcerebri who have no associated papilledema.
Head CT or MRI is normal in most of these patients, although an emptysella or small ventricles and cortical sulci may be present [31]. Diagnosis isestablished by lumbar puncture and confirmation of CSF pressure of more
392 A. Sismanis / Otolaryngol Clin N Am 36 (2003) 389–402
than 200 mm of water with normal constituents. The modified Dandy diag-nostic criteria for pseudotumor cerebri syndrome are summarized as fol-lows [49]:
1. Symptoms and signs of increased intracranial pressure2. Absence of localizing neurologic findings except for occasional sixth and
seventh nerve palsies3. Awake and alert patient4. Absence of deformity, displacement, and obstruction of the ventricular
system and otherwise normal neurodiagnostic studies except for in-creased CSF pressure
5. No other cause of increased intracranial pressure
Pulsatile tinnitus in these patients is thought to have the followingpathophysiology. Arterial CSF pulsations are transmitted to the exposedand compressible medial aspects of the dural venous sinuses resulting inperiodic compression of their walls and lumen narrowing with conversion ofthe normal laminar blood flow to turbulent [1,50].
The low-frequency sensorineural hearing loss, present in many of thesepatients, should not be confused with the hearing loss seen in patients withMeniere’s disease. This is a pseudosensorineural hearing loss secondary tothe masking effect of the PT, and light digital compression over theipsilateral IJV results in immediate cessation of PT and improvement ornormalization of hearing [1]. Stretching or compression of the cochlearnerve and brainstem caused by the intracranial hypertension or possibleedema could also play a role in the hearing loss and dizziness encountered inthese patients. This is supported by the abnormal auditory evoked responsespresent in one third of these patients [45].
Venous hum
Venous hum, idiopathic, or essential PT are synonyms used interchange-ably in the literature to describe patients with PT of unclear etiology[6,51,52]. The most common age group of patients with idiopathic PT isbetween 20 and 40 years and there is a marked female preponderance [53].
A possible cause of idiopathic PT is believed to be turbulent blood flowproduced in the IJV as it curves around the lateral process of the atlas [53].Other anatomic abnormalities of the IJV and dural venous sinuses can alsobe responsible for this entity.
Diagnosis of venous hum should be made only after appropriateevaluation and elimination of other disorders, such as pseudotumor cerebrisyndrome. Because many of the idiopathic PT patients reported in theliterature have not had an adequate work-up to rule out increased intra-cranial pressure, it is suspected that in at least some of these cases undiag-nosed pseudotumor cerebri syndromewas the underlying etiology.Associatedsymptoms of headaches and blurred vision, especially in morbidly obese
393A. Sismanis / Otolaryngol Clin N Am 36 (2003) 389–402
female patients, should alert the physician to pseudotumor cerebri syn-drome. The venous etiologies of PT are summarized as follows:
Pseudotumor cerebri syndrome [1]Jugular bulb abnormalities [54–57]Hydrocephalus associated with stenosis of the sylvian aqueduct [58]Increased intracranial pressure associated with Arnold-Chiari malforma-
tion [58]Abnormal condylar and mastoid emissary veins [59,60]Idiopathic or essential tinnitus [6,51–53]
Nonvascular etiologies
Palatal, stapedial, and tensor tympani muscle myoclonus
Myoclonic contractions of the tensor veli palatini, levator veli palatini,salpingopharyngeus, and superior constrictor muscles can result in objectivePT. These contractions can range between 10 and 240 per minute andshould not be confused with the arterial pulse. This disorder is seen in youngpatients, usually within the first three decades of life, although it also maybe encountered in older individuals [61,62]. Neurologic disorders, such asbrainstem infarctions, multiple sclerosis, trauma, and syphilis, have alsobeen reported in association with this entity. Involvement of the olivarytracts, posterior longitudinal bundle, dentate nucleus, and reticular for-mation has been identified in these patients [62,63]. Myoclonic con-tractions of the stapedial muscle have also been reported as a cause of PT[51,64].
Evaluation
History
The history is very important in evaluating these patients. Most patientsdescribe their symptom as hearing their ‘‘own heartbeat’’ or as a ‘‘thumpingnoise,’’ making diagnosis of PT apparent. Occasionally, however, patientsmay not volunteer the pulsatile component of their tinnitus and this maylead to overlooking this very important information.
Associated symptoms of hearing loss, aural fullness, dizziness, headaches,and visual disturbances, such as visual loss, transient visual obscurations,retrobulbar pain, and diplopia are highly suggestive of associated pseudo-tumor cerebri syndrome [1]. Older patients with a history of cerebrovas-cular accident, transient ischemic attacks, hyperlipidemia, hypertension,diabetes mellitus, and smoking should be suspected of having ACAD [2].Women with associated headaches, dizzy spells, syncope, fatigue, andlateralizing neurologic deficits should be evaluated for fibromuscular
394 A. Sismanis / Otolaryngol Clin N Am 36 (2003) 389–402
dysplasia [13–15]. Patients with sudden onset of PT in association withcervical or facial pain, headache, and symptoms of cerebral ischemia shouldbe highly suspicious of extracranial or intrapetrous carotid artery dissection[16,17].
Examination
Young and morbidly obese women with PT should be highly suspectedfor pseudotumor cerebri syndrome [1,65]. Otoscopy is essential for detectingmiddle ear pathology, such as a high or exposed jugular bulb, aberrantcarotid artery, glomus tumor, and Schwartze’s sign. Rhythmic movementsof the tympanic membrane can be present in patients with tensor tympanimyoclonus.
Complete head and neck examination is very important. A palpable thrillmay be present with cervical arteriovenous malformations [7]. Myocloniccontractions of the soft palate can be identified in patients with palatalmyoclonus. Wide opening of the oral cavity during examination may resultin elimination of the soft palate contractions [8]. For this reason fiberopticexamination through the nose is a more revealing method of examination.
Auscultation of the ear canal, periauricular region, orbits, neck, and chestshould be performed for detection of objective PT, bruits, and heartmurmurs. In particular, special attention should be paid when auscultatingthe postauricular and upper neck regions, because most of dural AVFsoccur in this area. Presence of a bruit in this area should be considered asan intracranial vascular abnormality until proved otherwise. Preferablyauscultation should be performed in a very quiet area, such as an audiologybooth, using a modified electronic stethoscope. Auscultation with anelectronic stethoscope has been found to be more sensitive than traditionalauscultation techniques [66,67]. The Litmann electronic stethoscope model2000 can be used for this purpose. When objective PT is detected, its rateshould be compared with the patient’s arterial pulse and the effect of lightdigital pressure over the ipsilateral IJV should be checked. PT of venousorigin, such as in patients with pseudotumor cerebri syndrome, decreases orcompletely subsides with this maneuver [1]. In patients with an arterial-type of PT this maneuver is ineffective. The effect of head rotation ontinnitus intensity should also be evaluated because venous PT often de-creases or completely subsides on head rotation toward the side of the PT.This is probably caused by compression of the IJV between the contract-ing sternocleidomastoid muscle and the transverse process of the atlas [1].Finally, in cases with a bruit, digital pressure should be applied in the post-auricular area and if decrease of the PT intensity is reported, an AVF shouldbe suspected.
A complete neurologic examination, including cranial nerve examination,should be performed. Consultation with neurology or neuro-ophthalmologyshould be obtained for patients suspected of pseudotumor cerebri syndrome.
395A. Sismanis / Otolaryngol Clin N Am 36 (2003) 389–402
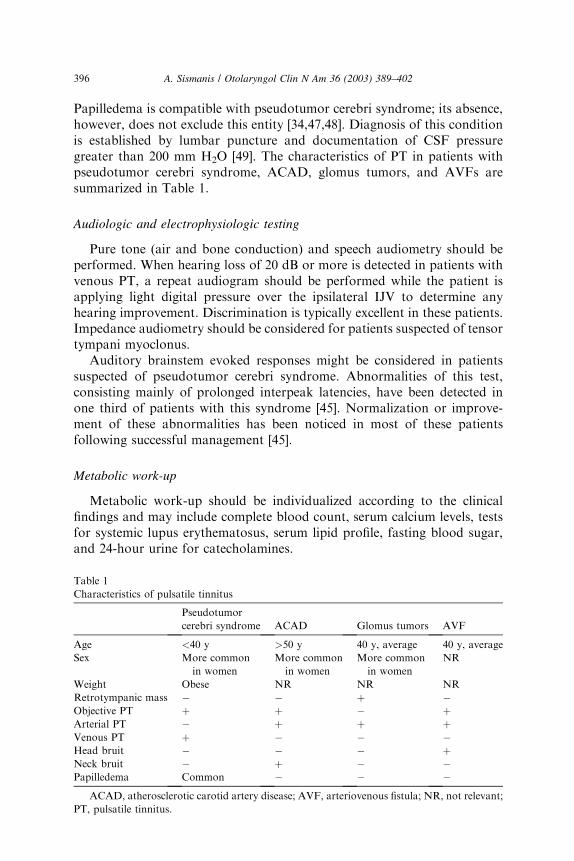
Papilledema is compatible with pseudotumor cerebri syndrome; its absence,however, does not exclude this entity [34,47,48]. Diagnosis of this conditionis established by lumbar puncture and documentation of CSF pressuregreater than 200 mm H2O [49]. The characteristics of PT in patients withpseudotumor cerebri syndrome, ACAD, glomus tumors, and AVFs aresummarized in Table 1.
Audiologic and electrophysiologic testing
Pure tone (air and bone conduction) and speech audiometry should beperformed. When hearing loss of 20 dB or more is detected in patients withvenous PT, a repeat audiogram should be performed while the patient isapplying light digital pressure over the ipsilateral IJV to determine anyhearing improvement. Discrimination is typically excellent in these patients.Impedance audiometry should be considered for patients suspected of tensortympani myoclonus.
Auditory brainstem evoked responses might be considered in patientssuspected of pseudotumor cerebri syndrome. Abnormalities of this test,consisting mainly of prolonged interpeak latencies, have been detected inone third of patients with this syndrome [45]. Normalization or improve-ment of these abnormalities has been noticed in most of these patientsfollowing successful management [45].
Metabolic work-up
Metabolic work-up should be individualized according to the clinicalfindings and may include complete blood count, serum calcium levels, testsfor systemic lupus erythematosus, serum lipid profile, fasting blood sugar,and 24-hour urine for catecholamines.
396 A. Sismanis / Otolaryngol Clin N Am 36 (2003) 389–402
Ultrasound studies
Duplex carotid ultrasound (including the subclavian arteries) or echo-cardiogram studies are very helpful in patients suspected of ACAD, athero-sclerotic subclavian artery disease, or valvular disease [31]. In particular,patients with carotid bruits should have a carotid ultrasound study beforeany extensive radiologic evaluation because if diagnosis of ACAD is estab-lished, the need for such an evaluation may be obviated.
Radiologic evaluation
Radiologic evaluation should be individualized according to the historyand physical examination findings, such as presence of retrotympanic mass,objective PT, bruit, and papilledema. The following represents the author’scurrent radiologic evaluation algorithm:
1. For patients with normal otoscopy, screening with high-quality MRAand MR venography (MRV) in conjunction with brain MRI should beinitially obtained. Small ventricles or empty sella are findings occa-sionally seen in patients with pseudotumor cerebri syndrome [31]. MRIdemonstration of dilated cortical veins is suggestive of an AVM; how-ever, neither the arterial supply nor the nidus of an AVM may bedetectable on MRI [68]. In 12 patients with angiographic diagnosis ofAVMs, 8 patients had dilated cortical veins on MRI [69]. Dural venoussinus thrombosis also can be diagnosed with MRV. In patients with nor-mal MRI-MRA-MRV associated with objective-arterial PT or a headbruit, carotid angiography should be strongly considered to exclude duralAVFs and fibromuscular dysplasia [23,69].
2. Patients with a retrotympanic mass should have a high-resolution,temporal bone CT as their initial evaluation [31]. If glomus tympan-icum, aberrant internal carotid artery, or jugular bulb abnormalities arediagnosed, no other imaging studies are needed. For patients withglomus jugulare tumors, CT examination of the neck should also beobtained to assess for additional chemodectomas along the carotidarteries. Carotid angiography is indicated only for prospective surgicalcases to evaluate the collateral circulation of the brain (arterial andvenous) in anticipation of possible vessel ligation or preoperative tumorembolization [28].
A diagnostic algorithm for patients with PT is shown in Fig. 1.
Management
Management that should be directed toward treating any underlyingetiology is summarized next. Most patients with PT secondary topseudotumor cerebri syndrome are overweight and weight loss is probably
397A. Sismanis / Otolaryngol Clin N Am 36 (2003) 389–402
the most important aspect of their management. PT in these patients mayrespond to medical management with acetazolamide (Diamox), 250 mg threetimes a day, or furosemide (Lasix), 20 mg twice a day [1,34]. Both of thesemedications are thought to reduce CSF production. Lumbar-peritonealshunt may be considered for patients with progressive deterioration ofvision, persistent headaches, and disabling PT [1,31,46]. In morbidly obesepatients, however, this procedure is often complicated by shunt occlusionbecause of the increased intra-abdominal pressure [70]. Weight reductionsurgery has been found effective in relieving PT in morbidly obese patientsand pseudotumor cerebri syndrome. This procedure should be consideredwhen conservative management with dietetic measures has failed. Thirteenout of 16 patients who underwent weight reduction surgery experiencedcomplete resolution of their PT [71]. Optic nerve sheath fenestration has beenreported to be beneficial for patients with progressive visual loss andheadaches [72].
Fig. 1. Pulsatile tinnitus diagnostic algorithm. (A) Retrotympanic mass present. (B) Normal
otoscopy.
398 A. Sismanis / Otolaryngol Clin N Am 36 (2003) 389–402
Repair of a symptomatic high-dehisced jugular bulb has been reported byusing pieces of mastoid cortical bone; septal, conchal, or tragal cartilage;and surgical wax [21,73–75]. The author does not have any personal ex-perience with these surgical techniques and remains skeptical regarding theirsuccess. PT secondary to otosclerosis usually subsides following a successfulstapedectomy [31]. Tensor tympani and stapedial myoclonus may respondto sectioning of the respective muscles by tympanotomy [76]. Botulinumtoxin has been reported for the management of palatal myoclonus [77].
Patients with ACAD benefit from carotid endarterectomy when carotidobstruction is more than 60% [78]. Angioplasty has relieved PT secondaryto atherosclerotic obstruction of the subclavian and intracranial carotidarteries [79,80]. PT secondary to antihypertensive medication, such asenalapril maleate or verapamil hydrochloride, usually subsides soon afterdiscontinuation of these agents [24].
Dural AVFs can be treated with selective embolization, radiosurgery, orselective embolization followed by radiosurgery [81–84]. Vascular neo-plasms, such as glomus jugulare tumors, are usually treated surgically.Stereotactic surgery may be considered for patients who are poor surgicalcandidates [85].
Finally, in patients with idiopathic PT, tinnitus typically subsides with lightpressure over the ipsilateral IJV making ligation of this structure a verytempting procedure. The results of this procedure, however, have been veryinconsistent andpoor overall. In a series of 13 patientswith essential tinnitus, 3underwent ligation of the ipsilateral IJV and only 1 benefited permanently.The other two patients experienced return of their PT within a few days [55].Furthermore, over the past several years the author has become aware ofa significant number of cases fromdifferent parts of the countrywhere patientsunderwent this procedure anddeveloped intracranial hypertension.Diagnosisof pseudotumor cerebri was made in some of these cases and at least in severalmalpractice litigation followed. There is rarely, if ever, an indication for thisprocedure solely for the purpose of alleviating PT [86].
References
[1] Sismanis A. Otologic manifestations of benign intracranial hypertension syndrome:
diagnosis and management. Laryngoscope 1987;97(suppl 42):1–17.
[2] Sismanis A, Stamm MA, Sobel M. Objective tinnitus in patients with atherosclerotic