VALIDITY OF DIETARY QUESTIONNAIRES IN SRI LANKAN ADULTS AND THE ASSOCIATION OF DIETARY INTAKE WITH OBESITY Ranil Jayawardena Mallika Arachchige MBBS (Colombo), HND (UK), MSc (Glasgow) Submitted in fulfilment of the requirements for the degree of Doctor of Philosophy Institute of Health and Biomedical Innovation School of Exercise and Nutrition Sciences, Faculty of Health, Queensland University of Technology April 2013
Transcript
VALIDITY OF DIETARY QUESTIONNAIRES IN SRI LANKAN ADULTS AND THE ASSOCIATION OF
DIETARY INTAKE WITH OBESITY
Ranil Jayawardena Mallika Arachchige
MBBS (Colombo), HND (UK), MSc (Glasgow)
Submitted in fulfilment of the requirements for the degree of
Doctor of Philosophy
Institute of Health and Biomedical Innovation
School of Exercise and Nutrition Sciences,
Faculty of Health,
Queensland University of Technology
April 2013
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity i
Keywords
Body Weight Perception, Diabetes, Diet, Dietary Diversity, Food Frequency
Questionnaire, Non-Communicable Diseases, Nutrition, Obesity, Sri Lanka.
ii Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
Abstract
Traditionally, infectious diseases and under-nutrition have been considered major
health problems in Sri Lanka with little attention paid to obesity and associated non-
communicable diseases (NCDs). However, the recent Sri Lanka Diabetes and
Cardiovascular Study (SLDCS) reported the epidemic level of obesity, diabetes and
metabolic syndrome. Moreover, obesity-associated NCDs is the leading cause of
death in Sri Lanka and there is an exponential increase in hospitalization due to
NCDs adversely affecting the development of the country. Despite Sri Lanka having
a very high prevalence of NCDs and associated mortality, little is known about the
causative factors for this burden. It is widely believed that the global NCD epidemic
is associated with recent lifestyle changes, especially dietary factors. In the absence
of sufficient data on dietary habits in Sri Lanka, successful interventions to manage
these serious health issues would not be possible. In view of the current situation the
dietary survey was undertaken to assess the intakes of energy, macro-nutrients and
selected other nutrients with respect to socio demographic characteristics and the
nutritional status of Sri Lankan adults especially focusing on obesity. Another aim of
this study was to develop and validate a culturally specific food frequency
questionnaire (FFQ) to assess dietary risk factors of NCDs in Sri Lankan adults.
Data were collected from a subset of the national SLDCS using a multi-stage,
stratified, random sampling procedure (n=500). However, data collection in the
SLDCS was affected by the prevailing civil war which resulted in no data being
collected from Northern and Eastern provinces. To obtain a nationally representative
sample, additional subjects (n=100) were later recruited from the two provinces
using similar selection criteria. Ethical Approval for this study was obtained from the
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity iii
Ethical Review Committee, Faculty of Medicine, University of Colombo, Sri Lanka
and informed consent was obtained from the subjects before data were collected.
Dietary data were obtained using the 24-h Dietary Recall (24HDR) method. Subjects
were asked to recall all foods and beverages, consumed over the previous 24-hour
period. Respondents were probed for the types of foods and food preparation
methods. For the FFQ validation study, a 7-day weight diet record (7-d WDR) was
used as the reference method. All foods recorded in the 24 HDR were converted into
grams and then intake of energy and nutrients were analysed using NutriSurvey 2007
(EBISpro, Germany) which was modified for Sri Lankan food recipes. Socio-
demographic details and body weight perception were collected from interviewer-
administrated questionnaire. BMI was calculated and overweight (BMI ≥23 kg.m-2),
Abstract .................................................................................................................................................. ii
The following papers have been published during my candidature ..................................................... vii Publications included in the thesis ............................................................................................ vii Relevant publications (with QUT affiliation) not included in the thesis .................................. viii Awards and grants during my candidature ................................................................................. xv Scholarly activities undertaken: ................................................................................................ xvi Conferences ............................................................................................................................ xvii
Table of Contents ................................................................................................................................. xix
List of Figures .................................................................................................................................... xxii
List of Tables .................................................................................................................................... xxiii
List of Abbreviations ........................................................................................................................... xxv Statement of Original Authorship ...................................................................................................... xxvi
Aims and objectives ................................................................................................................................ 6 Thesis orientation .................................................................................................................................... 7
Significance of the thesis......................................................................................................................... 9
Reference list ......................................................................................................................................... 12
Reference list ........................................................................................................................................ 83
Supplementary Materials, Part 1 ........................................................................................................... 89
Supplementary Materials, Part 2 ........................................................................................................... 96
CHAPTER 5: MANUSCRIPT 4 ....................................................................................................... 97 Title page .............................................................................................................................................. 98
Reference list ...................................................................................................................................... 131
Title page ............................................................................................................................................ 148
Reference list ...................................................................................................................................... 160
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xxi
Title page............................................................................................................................................. 168
Reference list ....................................................................................................................................... 199
CHAPTER 10: GENERAL DISCUSSION ................................................................................. 206 Comparison of different dietary assessment tools ............................................................................... 207
Nutritional issues in South Asia in relation to current diabetes epidemic ........................................... 212 Strengths of the study .......................................................................................................................... 216
Limitations of the study ...................................................................................................................... 216
Figure 2-2: Trends in prevalence in South Asia of a) diabetes mellitus and b) pre-diabetes (Data for individual countries were extracted from the following references; Bangladesh [18]; India [35-39]; Sri Lanka [27, 40, 41]) ...................................................... 43
Figure 2-3: Diabetes epidemicity index of South Asian countries (Ban – Bangladesh; Ind – India; Mal – Maldives; Nep – Nepal; Pak – Pakistan; SL – Sri Lanka; u – urban; r – rural; u+r – urban and rural; Diabetes [ ]; Diabetes Epidemicity Index [ ]) ...................... 44
Figure 2-4: Forest plot showing pooled odds ratios for a) Family history, b) Age, c) Male gender, d) Systolic Blood Pressure, e) Diastolic Blood Pressure, f) Body Mass Index and g) Waist-Hip ratio associated with diabetes (IV-Inverse variance; SE-Standard Error) .................................................................................................................................... 46
Figure 3-1: Trends in the prevalence of obesity (BMI ≥25 kg.m-2) in Sri Lanka, Bangladesh, Nepal, India and Pakistan in adult males ............................................................................. 68
Figure 3-2: Trends in the prevalence of obesity (BMI ≥25 kg.m-2) in Sri Lanka, Bangladesh, Nepal, India and Pakistan in adult females .......................................................................... 68
Figure 4-1: Study design of the Sri Lanka Diabetes and Cardiovascular Study. .................................. 73
Figure 4-2: Map of Sri Lanka with data collection (▀) sites ................................................................. 75
Figure 4-3. Example of a disaggregated recipe showing multiple levels (Chicken Koththu) ............... 88 Figure 4-4 : A typical Sri Lankan lunch ................................................................................................ 96
Figure 5-1: Example of a food photograph (200 g of rice) ................................................................. 115
Figure 12 Percentage energy contribution from macronutrients according to gender, ethnicity and area of residance,BMI,educational level and age groups. ........................................... 141
Figure 9-1: Bland and Altman plots for energy with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95% limits of agreements in red line. ................................................................... 204
Figure 9-2: Bland and Altman plots for protein with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95% limits of agreements in red line. ................................................................... 204
Figure 9-3: Bland and Altman plots for fat with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95% limits of agreements in red line. ......................................................................................... 205
Figure 9-4: Bland and Altman plots for carbohydrates with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95% limits of agreements in red line. ................................................................... 205
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xxiii
Table 2-1 Prevalence of diabetes and pre-diabetes in South Asian countries ....................................... 37
Table 2-2: Prevalence of diabetes according to area of residence ........................................................ 39
Table 2-3: Prevalence of diabetes in different regions .......................................................................... 41
Table 3-1: National prevalence of obesity (as percentage) in individual South Asian countries (BMI=Body mass index, WC=waist circumference) ........................................................... 65
Table 3-2: Socio-economic factors associated with the prevalence of obesity in the South Asian region. .................................................................................................................................. 67
Table 4-1: Demographic characteristics and BMI characteristics of the sample ................................... 85
Table 4-2: Average dietary intake of servings from different food group by Sri Lankan adults ........... 86
Table 4-3: Comparison of food intake of Sri Lankan adults with national and international recommendations. ................................................................................................................ 86
Table 4-4: Percentage distribution of the study sample according to their consumed foods portions from different food groups ..................................................................................... 87
Table 5-1: Demographic characteristics of the sample of the study population .................................. 112
Table 5-2: Nutrient intake of the study population.............................................................................. 113
Table 5-3: Elements of the food frequency questionnaire ................................................................... 114
Table 6-1: Socio-demographic characteristics of the survey population ............................................. 133 Table 6-2: Energy intake (kcal) of Sri Lankan adults by socio-demographic characteristics ............. 134
Table 6-3 Carbohydrate intake (g) of Sri Lankan adults by socio-demographic characteristics ......... 135
Table 6-4 Protein intake (g) of Sri Lankan adults by socio-demographic characteristics ................... 136
Table 6-5 Fat intake (g) of Sri Lankan adults by socio-demographic characteristics ......................... 137
Table 6-6 Dietary fiber intake (g) of Sri Lankan adults by socio demographic characteristics........... 138 Table 6-7 Sodium intake (mg) of Sri Lankan adults by socio-demographic characteristics ............... 139
Table 6-8: Mean Daily Micronutrient Intake by Sri Lankan Adults. .................................................. 140
Table 7-1. Mean and SD of dietary diversity score (DDS), dietary diversity score of portions (DDSP) and food variety score (FVS) ................................................................................ 163
Table 7-2 Percent consumption of different food groups by DDS for Sri Lankan adults (n=481) ..... 164
Table 7-3 Percent consumption of different food groups by DDSP for Sri Lankan adults (n=481) ............................................................................................................................... 165
Table 7-4 Mean BMI, Waist circumference and energy intake of the subjects according to DDS, DDSP and FVS. ........................................................................................................ 166
Table 8-2: Awareness of body weight and height ............................................................................... 185
Table 8-3: Percentage of adults in each category of weight perception, by BMI category calculated from measured height and weight. .................................................................... 186
Table 8-4: Percentage of adults in each category of waist circumference perception, according to WC cut-offs. ................................................................................................................... 186
Table 8-5: Logistic regression model of under perception, correct perception and over perception of body weight. ................................................................................................. 187
xxiv Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
Table 9-1: Comparison of consumption of nutrients estimated by 7DWR vs. FFQ. .......................... 201
Table 9-2: Percentage of subjects correctly classified by FFQ relative to the 7DWFR ...................... 202 Table 9-3 (Supplementary): Means, Standard Deviations Pearson’s Correlation Coefficients of
Nutrient intakes Based on FFQ 2 and FFQ 1 ..................................................................... 203
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xxv
List of Abbreviations
BMI Body Mass Index CVD Cardiovascular Disease
d Day
DDS Diet Diversity Score
DDSP Dietary Diversity Score with Portions
FFQ Food Frequency Questionnaire
FVS Food Variety Score
HDL High Density Lipoproteins
IV Inverse Variance
kg kilograms
LDL Low Density Lipoproteins
m meters
NCD Non-Communicable Diseases
NHS National Health Survey
OW Overweight
OR Odd Ratio
SD Standard Deviation
SE Standard Error
SLDCS Sri Lanka Diabetes and Cardiovascular study
TAG Triglycerides
TC Total Cholesterol
WC Waist Circumference
WHO World Health Organization
xxvi Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
Statement of Original Authorship
The work contained in this thesis has not been previously submitted to meet
requirements for an award at this or any other higher education institution. To the
best of my knowledge and belief, the thesis contains no material previously
published or written by another person except where due reference is made.
Signature:
Date: 7th November 2013
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xxvii
Acknowledgements
I greatly acknowledge the assistance I received from numerous individuals and
institutions for completing this research.
First and foremost, I would like to thank to my supervisory team, Prof. Andrew Hills,
Prof. Nuala Byrne, A/Prof. Mario Soares and Dr. Prasad Katulanda for their support,
advice, experience, and guidance throughout my candidature. I appreciate the
significant amount of time and assistance my supervisors have invested in the
development of my research and professional skills. Prof. Hills was a great mentor
and always provided me warm support and assistance over and above my
expectations. A/Prof. Soares expertise and critical perspectives were invaluable to
the development of this thesis. Dr. Katulanda provided a stimulating environment
with productive discussion through the research that helped make me a better
researcher. I am grateful to all of them for their invaluable support, wisdom and the
kind-hearted assistance extended to me during last three years.
I would like to express my gratitude to staff members of the university. I would like
to thank Queensland University of Technology for offering me a scholarship to
complete my PhD. The university has offered me many opportunities to attend and
present at seminars, trainings and conferences to further enhance my research skills
and disseminate my research findings. I must thank the Faculty of Health for
granting me the tuition fee waiver and living allowance scholarship, without which
my PhD study would not have been possible.
I would like to greatly acknowledge staff members from Diabetes Research Unit
(DRU), Faculty of Medicine, University of Colombo for support for field visits, data
collection, data analysis and data entering. I would like to thank my colleagues and
xxviii Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
and Upekha Ganegoda. I would also like to thank Connie Wishart for laboratory
analyses at IHBI and Martin Reese who helped me correct the English in this
dissertation.
I would like to thank all my family for their support, especially my mother Nalini,
brother Chathura and my mother-in-law Kusum who encouraged me to travel
overseas to further my studies. I am sure they are thrilled to see the end in sight. I am
deeply grateful to my wife, Kavindya, who accepted my decisions to undertake this
PhD journey, always believes in and stands by me, and continues to bring a smile to
my face. I could not have completed this research without your help.
Additionally, I would like to thank the participants in this study for their
contribution and cooperation. Their valuable input was a major factor in
accomplishing this study.
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xxix
Dedication
To my loving father, who passed away one month before I started my PhD.
1
Chapter 1: Introduction
BACKGROUND
Traditionally, infectious diseases and under-nutrition have been considered major health
problems in the developing world [1] with little attention paid to obesity and associated Non-
Communicable Diseases (NCDs). In the past, obesity was regarded as a sign of wealth in
developing settings and therefore has long been viewed as desirable. However, the prevalence of
obesity and NCDs are increasing at an alarming rate worldwide [2] and an increasing body of
evidence shows that people originating from the Indian sub-continent have a high risk for NCDs
including diabetes mellitus type 2 (DM), coronary heart disease (CHD) and stroke compared to
Europeans [3]. South Asia has the highest number of diabetics worldwide and 50% of the adult
disease burden in South Asia is attributable to NCDs [4]. Developing countries, particularly Sri
Lanka, have not been spared [5]. It has been identified that recent lifestyle changes, mainly
nutritional factors, may be associated with the increasing prevalence of NCDs globally.
Therefore, it is vital to be able to quantify existing dietary habits and associated health
conditions. Because eating habits vary significantly among ethnic groups, it is not possible to
predict dietary patterns without reliable country-specific information. In the absence of sufficient
and relevant data on diet and obesity levels in South Asian countries, successful interventions to
manage diet associated NCDs would not be possible.
The increasing prevalence of obesity, diabetes and associated NCDs is a major public health
problem in South Asia. The problem is exacerbated by the ethnic susceptibility of South Asians
to NCDs, a rapidly ageing population, socioeconomic changes and the lack of resources to
2 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
intervene. Sri Lanka recorded 524 deaths per 100,000 from cardiovascular and cerebrovascular
disease, considerably higher than in many affluent countries such as the UK (427), USA (397),
Australia (308) and France (205) [6]. Ischemic heart disease (10.6%) and cerebrovascular
diseases (9.0%) are reported as the leading causes of death in Sri Lanka [7]. According to
mortality data, from 1981 to 2000, there was an exponential increase in hospitalization due to
NCDs in Sri Lanka and it was previously estimated that by 2010 there would be a 40%, 36% and
29% increase in hypertension, diabetes mellitus and ischemic heart disease, respectively [8].
Despite Sri Lanka having a very high prevalence of NCDs and associated mortality, little is
known about the causative factors for this health burden. It is widely believed that the global
NCD epidemic is associated with recent lifestyle changes, especially increased intake of calorie-
dense foods, saturated fatty acids, sugary drinks, refined carbohydrates and lower intake of fruit
and vegetables [9].
In the UK, the National Diet and Nutrition Survey (NDNS) showed a very strong association
between diet and NCDs in adults [10]. The Sri Lankan Nutrition Survey was conducted in 1975,
however the main concern at that time was under-nutrition and protein-energy malnutrition in
children [11]. STEP survey findings noted a number of risk factors associated with NCDs in an
urban province in Sri Lanka, namely smoking, physical inactivity and low fruit and vegetable
intake [12]. The authors were unable to identify specific causes for NCD risk, possibly due to a
lack of comprehensive information on dietary habits. It is believed that the high prevalence and
incidence of NCDs is associated with the Sri Lankan population’s dietary practices. This is the
first diet and nutrition survey in Sri Lanka.
In Sri Lanka, diet-related chronic diseases currently account for 18.3% of all deaths and 16.7%
of hospital expenditure [13]. Despite consensus that diet plays a major role in the epidemic of
NCDs in Sri Lanka, nutritional interventions are far beyond the scope of the current capacity in
the country. Firstly, there are very few nutrition or dietetic experts in Sri Lanka and no dietetic
3
or clinical nutrition training available in the educational system therefore advice to the
population is minimal. Secondly, Sri Lanka has never conducted a food consumption survey due
to the absence of a validated dietary assessment tool and the necessary resources, and no cross-
sectional nutritional information is currently available on dietary habits and associated NCDs in
the country [14]. In addition, the cultural and ethnic diversity of the population may also affect
lifestyle considerably.
On the other hand, dietary diversity also affects disease status. All people need a variety of foods
to meet requirements for essential nutrients, and the value of a diverse diet has long been
recognized [15]. Traditionally, dietary diversity was linked to under-nutrition. There is very
limited evidence on the association between diet diversity and NCDs [16].
Different nutritional assessment tools are commonly used for dietary surveys in many countries,
including the 7-day weighed food approach widely used in the UK [10]. However, the approach
is costly and associated with significant participant burden. On the other hand, various Food
Frequency Questionnaires (FFQs) have been widely used and are recognized as reliable and
suitable for dietary assessment at the population level [17]. The FFQ is the most common dietary
assessment tool used in large epidemiologic studies of diet and health [18]. FFQs assess energy
and/or nutrient intake by determining how frequently a person consumes a limited number (100-
150) of foods which are the main sources of nutrients or of a particular dietary component in
question [19]. Respondents indicate how many times a day, week, month, or year they usually
consume the food items [20]. In some FFQs, standard portion sizes are used but not in all. For
example, an Australian FFQ included photographs of important portion sizes [21]. The strengths
of FFQs are: 1) a modest demand on time and energy of respondents; 2) relatively easy to
administer; 3) some are self-administered and machine readable and thus are relatively
economical to use in large-scale studies [18]. The main limitations of FFQs are that they limit
food lists to 100-150 items even though free-living individuals could be consuming more than
4 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
this number [22]. Similarly, limiting portion sizes may confuse some respondents. Another
limitation is reliance on the ability of respondents to explain their diet [23]. Despite these
limitations, the FFQ has been used in the US to collect nutritional intake and is considered the
method of choice for research on diet-disease relationships [24]. However, as foods vary by
culture and region, culture- or region-specific FFQs have been developed. The culture- or
region-specific FFQ consists of a list of foods eaten commonly in a particular country or by a
particular population, each food’s commonly eaten portion size and the reported intake
frequency. The FFQ food list typically explains 80–90% of the variability in the nutrients of
interest [18].
Developing a region-specific FFQ would be particularly helpful to identify high diet-related
disease status in Sri Lankan adults and would greatly assist in planning for the conduct of a
national level cross-sectional survey in 2014-2015. Developing the food item list from a
representative population is vital. A restricted food list may not be able to capture the full
variability of the Sri Lankan diet, which includes a variety of foods, ingredients, cooking
practices and brands. In this study, as energy, macro-nutrients and selected micro-nutrients will
be measured it is crucial to establish a comprehensive food list. To ensure that data are
representative of the population for whom the FFQ will be developed, large, representative,
randomly-selected samples are needed.
Public health promotion efforts aimed at overweight and obesity prevention often proceed from
the assumption that most individuals prefer to be thin, and that the first step in motivating
individuals to lose weight and associated health risk is to raise awareness of weight status among
those who are overweight [25]. This approach may be fitting for Western populations that value
thinness in women and lean, muscular physiques in men, and educated societies where
abdominal obesity may considered as a risk factor for metabolic problems such as diabetes.
However, this assumption may not be appropriate for South Asians where body size preference
5
may differ. In most non-Western cultures it is recognized that large bodies in both males and
females are associated with wealth and health [26]. That culture influences weight perception
preference has been the rationale for many studies researching the association between weight
perception and obesity among different ethnic groups. However, many of the studies have either
focused on minority immigrant populations in affluent countries [27] or primarily adolescent age
groups [26]. Results from these two groups may not represent the association between weight
perception and obesity in adults in South Asian countries where obesity has now reached an
epidemic level.
In summary, it is evident Sri Lanka is facing a significant health burden due to diet-related
NCDs. However, large nutritional interventions are far beyond the current capacity of the
country. Sri Lanka has never conducted a food consumption survey mainly due to the absence of
a validated dietary assessment tool and resources. Therefore, there are no available cross-
sectional nutritional data on dietary habits and associated NCDs in Sri Lanka. There is a
considerable cultural and ethnic diversity which may be associated with the dietary intake of the
population. Secondly, the associations between obesity, diet and behaviour, including weight
perception, is an unexplored area of interest.
6 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
AIMS AND OBJECTIVES
To address the research questions, this research project was separated into two parts. Part 1
comprised a cross-sectional study to obtain details of dietary habits of Sri Lankan adults. In
addition to nutritional data, anthropometric and behavioural data were collected. Validating a
dietary tool necessitated a separate study sample. Part 2 therefore, investigated the validity of the
dietary questionnaire against a reference method in a representative sample.
The aims and objectives for each phase are listed below. These aims and objectives are based on
gaps in existing knowledge identified from the literature which will be discussed in the
respective chapters.
Part 1
1. To identify food consumption according to servings in Sri Lankan adults.
2. To develop a FFQ for Sri Lankan adults to measure habitual dietary intake.
3. To assess the intakes of energy, macro-nutrients and selected other nutrients with respect
to socio-demographic characteristics and the nutritional status of Sri Lankan adults
focusing on diet-related metabolic chronic disease.
4. To explore the association of diet diversity with obesity in Sri Lankan adults.
5. To assess self-perception of body weight among Sri Lankan adults.
Part 2
1. To assess the validity of a newly developed FFQ to estimate nutrient intake compared
with a reference method.
7
THESIS ORIENTATION
This program of research is presented as a Thesis by Publication (Table 1 below). Nine
manuscripts (six published, two in press, one under review) are included as components of the
chapters in this thesis. All manuscripts have been accepted in, or submitted to, international
peer-reviewed journals. Each manuscript is written in the conventional style for the journal,
including reference style and spelling. As each manuscript is designed to stand alone, there is an
inevitable degree of overlap in their Introduction, Methods and Discussion sections.
The first two chapters incorporate the literature review for this thesis. South Asia is home to
almost one quarter of the world’s population. With the rapid emergence of obesity in the region,
an increasing body of evidence suggests that people originating from the Indian sub-continent,
including Sri Lanka, have a higher risk of type 2 diabetes, coronary heart disease and stroke
compared to Europeans. In addition, the socio-economic characteristics of the South-Asian
population are distinct from those seen in developed countries. South Asia has the highest
number of diabetes cases in the world. Therefore, the following section will further review the
current literature on obesity and diabetes in the region. Chapter 2 systematically evaluates the
scientific literature on the prevalence, trends and risk factors for diabetes in the South Asian
region. Manuscript 1 has been published (and tagged as “highly accessed”) in BMC Public
Health (2012). Similarly, Chapter 3 discusses the prevalence of overweight and obesity among
the adult population from individual countries in South Asia using the most recent representative
evidence and identifies and discusses the socio-economic factors associated with obesity in the
region. Chapter 3 is based on Manuscript 2, which has been accepted for publication (in press)
in Obesity Facts.
8 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
This research work is divided into two parts. Measurement of current food habits and obesity
among Sri Lankan adults comprises part 1, and the development and validation of a food
frequency questionnaire represents part 2. Chapter 4 includes a description of study design,
details methodology and presents the results. This chapter also includes Manuscript 3, based on
part 1, which has been published in the journal, Public Health Nutrition (2012). Importantly,
Chapter 4 provides additional methodological details due to the limited ability to describe
methodology in the published manuscripts. Manuscript 4 reports on the methods used in part 2,
the FFQ. Chapter 5 subsequently presents the methodological details of the development of
Food frequency Questionnaire. Manuscript 4 has been published in the Nutrition Journal
(2012).
Chapter 6 presents the results of part 1. National diet and nutrition surveys provide valuable
information on a possible partial explanation for the health status and disease risk of the
population studied. Manuscript 5 reports on a dietary survey undertaken to assess the intakes of
energy, macronutrients and selected other nutrients with respect to socio-demographic
characteristics and nutritional status of Sri Lankan adults focusing on diet-related metabolic
chronic disease. Manuscript 5 has been accepted in BMC Research Notes and is currently in
press.
Chapter 7 provides details of current obesity level in Sri Lanka and the association with dietary
factors. This chapter includes Manuscripts 6 and 7. Prevalence of obesity among Sri Lankan
adults is reported briefly in manuscript 6. This manuscript has been published in the Asia Pacific
Journal of Public Health (2012). Manuscript 7 provides further detailed information regarding
the association of obesity and dietary diversity. This manuscript has been published (tagged as
“highly accessed”) in the BMC Public Health (2013).
Chapter 8 presents the body weight perception and weight loss practices among Sri Lankan
adults. This chapter discusses the self-perception of body weight and weight loss approaches
9
among Sri Lankan adults. Manuscript 8 has been published in Obesity Research and Clinical
Practice.
Development of the Food Frequency Questionnaire is reported in Chapter 9. Study 2 is
described in detail in this chapter including a description of the methods and presentation of
results. This chapter also includes Manuscript 9, based on the results of part 2, and has been
submitted to the Nutrition Journal.
Finally, Chapter 10 provides a synthesis of the study findings across the three manuscripts, and
discusses the study limitations, directions for future research and the public health and clinical
significance of the research findings.
Table 1-1. Thesis orientation
Section Chapters Manuscripts
Introduction 1 N/A
Literature review 2, 3 1, 2
Methods 4, 5 3, 4
Results 6, 7, 8, 9 5,6,7,8,9
Discussion 10 N/A
N/A: not applicable
SIGNIFICANCE OF THE THESIS
The research and outcomes of this thesis are located within the priority field of nutrition and
obesity. Although the research was conducted among native Sri Lankan adults, many of the
findings can be generalized to native South Asians and South Asians living in other countries
such as Australia. Their significance is summarized in the following points.
10 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
1. This study was the first to develop and validate a FFQ for Sri Lankan adults using a
nationally representative sample. Dietary assessment of this population is invaluable to
understand the role of nutrition in chronic disease so that preventive strategies can be
implemented. The main weakness of the previous national level NCD survey in Sri
Lanka was the absence of nutritional data on the population and their relationship with
the high NCD risk in the country. One of the main objectives of the current work was to
develop a FFQ to administer in the next national level NCD survey. Moreover, this FFQ
could also be used to assess dietary habits of Sri Lankans living in other countries, as
they practice similar eating patterns to native Sri Lankans.
2. Most Sri Lankan meals are mixed dishes. We described a method to translate a mixed
meal to food group categories. Food which is a mixture of several food types was
systematically disaggregated before ingredients were categorized into appropriate food
groups. Decisions were then made about the point at which to stop the disaggregation
process so that foods or their ingredients could be tabulated in the appropriate food
groups. This study provided the first national estimate of energy and nutrient intake of
the Sri Lanka adult population. It is evident that consumption of high levels of
carbohydrate, fat mainly from saturated sources, low protein, low dietary fiber and high
levels of sodium may have detrimental effects on health and be related to the current
epidemic of NCDs.
3. This thesis is the first to report on dietary habits and nutrient intake of Sri Lankans.
Excess consumption of starchy foods but inadequate intake of dairy products, fruit and
vegetables may be associated with higher prevalence of diet associated NCDs. Dietary
diversity and variety have long been recognized as key elements of high quality diets.
Moreover, this thesis reports on a positive association between high dietary diversity and
11
obesity among Sri Lankan adults. Increased dietary diversity in health promotion may
not be appropriate for combating obesity epidemic in Sri Lanka.
4. The prevalence of obesity has reached epidemic levels in many parts of the world and Sri
Lanka is no exception. During the last two decades the level of obesity has increased
substantially in Sri Lanka. We found nearly a quarter of Sri Lankan adults are obese.
Although obesity levels have reached epidemic proportions, body weight misperception
was common among Sri Lankan adults. Two-thirds of overweight males and 45% of
females considered themselves as ‘about right weight’. Over one-third of both male and
female obese subjects perceived themselves as ‘about right weight’ or ‘underweight’.
12 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
REFERENCE LIST
1. Muller, O. and M. Krawinkel, Malnutrition and health in developing countries. Canadian
Medical Association Journal, 2005. 173(3): p. 279. 2. James, P.T., et al., The worldwide obesity epidemic. Obes Res, 2001. 9 Suppl 4: p. 228S-
233S. 3. Misra, A. and L. Khurana, Obesity-related non-communicable diseases: South Asians vs
White Caucasians. International Journal of Obesity, 2010. 4. Ghaffar, A., K. Reddy, and M. Singhi, Burden of non-communicable diseases in South
Asia. British Medical Journal, 2004. 328(7443): p. 807. 5. Misra, A. and L. Khurana, Obesity and the metabolic syndrome in developing countries.
Journal of Clinical Endocrinology & Metabolism, 2008. 93(11_Supplement_1): p. s9. 6. Abeywardena, M., Dietary fats, carbohydrates and vascular disease: Sri Lankan
perspectives. Atherosclerosis, 2003. 171(2): p. 157. 7. Jayasekara, R. and T. Schultz, Health status, trends, and issues in Sri Lanka. Nursing &
Health Sciences, 2007. 9(3): p. 228-233. 8. Premaratne, R., A. Amarasinghe, and A. Wickremasinghe, Hospitalisation trends due to
selected non-communicable diseases in Sri Lanka, 2005–2010. Ceylon Medical Journal, 2005. 50(2): p. 51.
9. WHO. Diet. Global Strategy on Diet, Physical Activity & Health 2010 2010 [cited 2010 9/10]; Available from: http://www.who.int/dietphysicalactivity/diet/en/index.html.
10. Henderson, L., J. Gregory, and G. Swan, The national diet & nutrition survey: Adults aged 19 to 64 years2003: Stationery Office.
11. Brink, E.W., et al., Sri Lanka Nutrition Status Survey, 1975. International Journal of Epidemiology, 1978. 7(1): p. 41-47.
12. Somatunga, L.C., NCD Risk Factor Survey in Sri Lanka (STEP Survey), 2004, WHO. 13. Popkin B.M., H.S., Kim S.,, The Nutritional Transition and Diet-Related Chronic
Diseases in Asia: Implications for Prevention. Washington, DC: International Food Policy Research Institute FCND Discussion Paper, 2001. 105.
14. FAO, FAO-Nutrition Country Profiles, 1999, Food and Agriculture organization of the United Nations Rome.
15. Ruel, M., Operationalizing dietary diversity: a review of micronutrient issues and research priorities. J Nutr, 2003. 133: p. 3911 - 3926.
16. Kennedy, G., M. Pedro, and C. Seghieri, Dietary diversity score is a useful indicator of micronutrient intake in Non-Breast-Feeding Filipino children. J Nut, 2007. 137: p. 472 - 477.
17. Cade, J., et al., Food-frequency questionnaires: a review of their design, validation and utilisation. Nutrition research reviews, 2004. 17(01): p. 5-22.
18. Willett, W., Nutrition Epidemiology. 2 ed1998, NEW YORK: Oxford University Press. 19. Subar, A.F., et al., Improving Food Frequency Questionnaires: A Qualitative Approach
Using Cognitive Interviewing. Journal of the American Dietetic Association, 1995. 95(7): p. 781-788.
20. Block, G., Human dietary assessment: methods and issues. Preventive Medicine, 1989. 18(5): p. 653-660.
21. Victoria, C.C. Dietary questionnaires. 2010; Available from: http://www.cancervic.org.au/about-our-research/epidemiology/nutritional_assessment_services.
22. Iqbal, R., et al., Refinement and validation of an FFQ developed to estimate macro-and micronutrient intakes in a south Indian population. Public Health Nutrition, 2009. 12(01): p. 12-18.
23. Mullen, B., et al., Validity of a food frequency questionnaire for the determination of individual food intake. American Journal of Clinical Nutrition, 1984. 39(1): p. 136.
24. Centers for Disease Control and Prevention. NHANES III. 2010; Available from: http://www.cdc.gov/nchs/nhanes/nh3data.htm.
25. Wammes, B., et al., The impact of a national mass media campaign in The Netherlands on the prevention of weight gain. Public Health Nutrition, 2005. 8(08): p. 1250-1257.
26. Becker, A.E., S.E. Gilman, and R.A. Burwell, Changes in Prevalence of Overweight and in Body Image among Fijian Women between 1989 and 1998**. Obesity Research, 2005. 13(1): p. 110-117.
27. Brener, N.D., et al., The Association between Weight Perception and BMI among High School Students. Obesity, 2004. 12(11): p. 1866-1874.
14 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
Chapter 2: Manuscript 1
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or publisher of
journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the Australasian
Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Prevalence and trends of the diabetes epidemic in South Asia: a systematic review and meta-analysis Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Priyanga Ranasinghe Study design and data collection. Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying
authorship.
Nuala Byrne 18/04/2013
Name signature Date
15
TITLE PAGE
Prevalence and trends of the diabetes epidemic in South Asia: a systematic
review and meta-analysis
Ranil Jayawardena1,2*, Priyanga Ranasinghe2,3, Nuala M. Byrne1, Mario J. Soares4, Prasad
Katulanda2, Andrew P. Hills5
1- Institute of Health and Biomedical Innovation, Queensland University of Technology,
Brisbane, Queensland, Australia
2- Diabetes Research Unit, Department of Clinical Medicine, Faculty of Medicine, University of
Colombo, Colombo, Sri Lanka
3- Department of Pharmacology, Faculty of Medicine, University of Colombo, Colombo, Sri
Lanka
4- Curtin Health Innovation Research Institute, School of Public Health, Curtin University,
Perth, Australia
5- Mater Mothers’ Hospital, Mater Medical Research Institute and Griffith Health Institute,
† calculated from available data; NR – Not reported; a - publication year
Chapter 2: Manuscript 1 41
Table 2-3: Prevalence of diabetes in different regions Region Year Prevalence of Diabetes
South Asia* 1995-2005/2006 4.5%-10.3%
Global† 2011 8.5%
Middle-East† 2011 11.0%
North America† 2011 10.7%
South America† 2011 9.2%
South-East Asia† 2011 9.2%
Western Pacific† 2011 8.3%
Europe† 2011 6.7%
Africa† 2011 4.5%
* based on most recent national surveys in regional countries
† IDF 2011 [10]
42 Chapter 2: Manuscript 1
Figure 2-1: Summarized search protocol
Chapter 2: Manuscript 1 43
Figure 2-2: Trends in prevalence in South Asia of a) diabetes mellitus and b) pre-diabetes (Data for individual countries were extracted from the following references; Bangladesh [18]; India
[35-39]; Sri Lanka [27, 40, 41])
44 Chapter 2: Manuscript 1
Figure 2-3: Diabetes epidemicity index of South Asian countries. (Ban – Bangladesh; Ind – India; Mal – Maldives; Nep – Nepal; Pak – Pakistan; SL – Sri Lanka; u – urban; r – rural; u+r – urban and rural; Diabetes [ ]; Diabetes Epidemicity Index [ ])
Chapter 2: Manuscript 1 45
Continue to page 46.
46 Chapter 2: Manuscript 1
Figure 2-4: Forest plot showing pooled odds ratios for a) Family history, b) Age, c) Male gender, d) Systolic Blood Pressure, e) Diastolic Blood Pressure, f) Body Mass Index and g)
Waist-Hip ratio associated with diabetes (IV-Inverse variance; SE-Standard Error)
Chapter 3: Manuscript 2 47
Chapter 3: Manuscript 2
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Prevalence, trends and associated socio-economic factors of obesity in South Asia Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
48 Chapter 3: Manuscript 2
TITLE PAGE
Prevalence, trends and associated socio-economic factors of obesity in South Asia Ranil Jayawardena1,2, Nuala M. Byrne1, Mario J. Soares3, Prasad Katulanda2, Andrew P. Hills4 1Institute of Health and Biomedical Innovation, Queensland University of Technology, Brisbane, Queensland, Australia 2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka 3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health Sciences, Curtin University, Perth, WA, Australia 4Mater Mother’s Hospital, Mater Medical Research Institute and Griffith Health Institute, Griffith University, Brisbane, Queensland, Australia
Citation
R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills (2013). Prevalence, Trends and
Associated Socio-Economic Factors of Obesity in South Asia. Obesity Facts (in press) Ms No.:
201202017
Chapter 3: Manuscript 2 49
SUMMARY
Worldwide obesity levels have increased unprecedentedly over the past couple of decades.
Although the prevalence, trends and associated socio-economic factors of the condition have
been extensively reported in Western populations, less is known regarding South Asian
populations. A review of articles using MEDLINE with combinations of the MeSH terms:
Obesity, Overweight, and “Abdominal Obesity” limiting to epidemiology and south Asian
counties. Although the methodological heterogeneity and variation according to country, area of
residence, gender exist, the most recent nationally representative and large regional data show a
clear epidemic of obesity, overweight and abdominal obesity. Prevalence estimates of
overweight and obesity [based on Asian cut-offs; Overweight ≥23 kg/m2, Obesity ≥25 kg/m2]
ranged from 3.5% in rural Bangladesh to over 65% in the Maldives. Abdominal obesity was
more prevalent than general obesity in both sexes in this ethnic group. Countries with the lowest
prevalence had the highest upward trend of obesity. Socio-economic factors associated with
greater obesity in the region included female gender, middle age, urban residence, higher
educational and economic status. In conclusion, South Asia is significantly affected by the
obesity epidemic. Collaborative public health interventions to reverse these trends need to be
mindful of many socioeconomic constraints in order to provide long term solutions.
50 Chapter 3: Manuscript 2
INTRODUCTION
Worldwide obesity levels have increased unprecedentedly over the past couple of decades.
Indeed, according to the World Health Organization’s (WHO) recent global estimates, over one
billion and nearly 300 million adults are overweight and obese, respectively [1]. In many
affluent countries, obesity has reached epidemic levels and is associated with non-communicable
diseases (NCDs) including diabetes, hypertension, dyslipidemia and coronary heart disease, all
major public health issues [2]. In affluent countries, socio-economic status and education level
are negatively associated with the prevalence of obesity, a situation which contrasts to that in
South Asia [3]. Traditionally, infectious diseases [4] and under-nutrition [5] were considered
major health problems in South Asia and little attention was paid to obesity by healthcare
workers, policy makers or researchers. However, with the rapid emergence of the obesity
epidemic in South Asian countries, and an increasing body of evidence that people originating
from the Indian sub-continent have a high risk for NCDs including diabetes mellitus type 2
(DM), coronary heart disease (CHD) and stroke compared to Europeans [6], greater attention is
being paid. Alarmingly, South Asia has the highest number of patients with diabetes worldwide
and 50% of the adult disease burden in South Asia is attributable to NCDs [7].
It is estimated that the total population living in South Asia now exceeds 1.56 billion with India
(2nd), Pakistan (6th) and Bangladesh (7th) among the ten most populated countries in the world
[8]. Moreover, people who originated from the Indian sub-continent are also widespread in most
countries of the world, predominantly in affluent nations. The disease burden in South Asians is
invariably a high priority as a global health issue. Although there have been a few in-depth
reviews on obesity and associated disease in Asia [6,9], none has discussed obesity prevalence
and trends for individual countries in the region. Therefore, the main aim of this study was to
Chapter 3: Manuscript 2 51
discuss the prevalence of overweight and obesity among the adult population from individual
countries in South Asia using the most recent representative evidence. Associated aims were to
plot obesity trends over time across the last few decades, and identify and discuss the socio-
economic factors associated with obesity in the region.
METHODS
In this review, South Asians are defined as people living in the Indian subcontinent which
consists of the following countries: India, Pakistan, Sri Lanka, Bangladesh, Nepal, Bhutan and
the Maldives. Countries from the Far East (Japan, China etc.) and South East Asia (Malaysia,
Thailand, Singapore etc.) were excluded [10]. There is an active collaboration and mutual
assistance (South Asian Association for Regional Cooperation - SAARC) among these countries
in economic, social, cultural, technical and scientific fields [11]. Despite the existence of
considerable heterogeneity among the inhabitants of South Asia, there are several similarities in
the biological and socio-cultural aspects of the people from this region that allows this group to
be considered as a single unit for the purpose of examination of health issues [12].
Overweight and obesity prevalence data among adults in the South Asian countries studied were
obtained by searching Medline with combinations of the MeSH terms: Obesity and Overweight
as separate main key words for papers published in English between 1 January 1980 and 31
December 2011. Secondly, each key word was divided into subheadings and Epidemiology/EP
included for searching with main key words. Thirdly, the conjunction of the above results was
narrowed down by adding the name of each country (India, Pakistan, Bangladesh, Sri Lanka,
Nepal, Bhutan and Maldives) as key words. A manual search was performed for future evidence
using the reference lists of selected articles and corresponding authors were contacted to obtain
additional data. Furthermore, relevant governmental health and WHO websites were browsed.
52 Chapter 3: Manuscript 2
The primary search was focused on research investigating the prevalence of overweight, obesity
or abdominal obesity in each country. Priority was given to larger (n>2000), nationally
representative samples.
Studies done in the clinical settings and patients with especial medical conditions and limited to
especial groups (e.g. doctors) or age category (e.g. age >65 y) were excluded. Studies of South
Asians living in the non-South Asian countries were excluded.
Initial screening of articles was carried out using abstracts. Unless it was clear from the abstract
that this strategy met the inclusion criteria for the review, the article was rejected. For prevalence
data, the most recent, well-designed and nationally representative or large studies were included.
Trends were plotted by available prevalence data from each country according to gender.
RESULTS
National prevalence of obesity in individual countries (Table 1)
No data were found from Bhutan. Limited nationwide surveys were found in the region and most
recent studies were completed between 2004 and 2006. The STEPS survey in the Maldives [13]
and SLDC study [14] in Sri Lanka reported on prevalence of overweight, obesity and abdominal
obesity using similar anthropometric cut-offs and in a similar period of time. The study in the
Maldives reported the highest prevalence of overweight, obesity and abdominal obesity in the
region with 60.8% of males and 65.5% of females overweight and obese. The overall prevalence
of obesity and abdominal obesity were 43.5% and 40.0% with half the women being obese
(48.1%) and abdominally obese (54.1%) [13]. Sharma et al. recently reported a very high
prevalence of overweight among both Nepalese men (59.1%) and women (61.8%), however they
have reported lower BMI cut-offs to define overweight (≥22 kg/m2) [15]. As per the WHO
definition for overweight in Asian adults (BMI ≥23 kg/m2) a quarter of Sri Lankan adults (M:
22.6%, F: 28.0%) were overweight [14]. In Bangladesh, a large survey undertaken on
reproductive age woman reported levels of overweight of 9.6% and 18.9% among rural and poor
Chapter 3: Manuscript 2 53
urban areas [16]. No nationally representative data are available on men, however data from four
sites in Bangladesh showed around 10% of men have BMI scores above 25 kg/m2 [17]. Results
from the National Health Survey of Pakistan showed a high prevalence of overweight (M: 22.0%
F: 27.9%) and obesity (M: 12.5% F: 18.6) in the early 1990s [18] moreover, authors noted a 2.5
times greater prevalence of obesity among urban than among rural residents [18]. In 2007, a
study on a rural population showed 19.5% and 24.7% obesity levels (BMI ≥25 kg/m2) in men
and women, respectively [19].
Prevalence data in India is more complex. For example, the Indian National Family Health
Survey-3 reported prevalence data on obesity in a large sample (n=111781) across 26 states [20]
with moderate levels of obesity; 9.3% for men and 12.6% for women. However in contrast,
Deepa et al. [21] reported 46.1% and 50.2% overweight and obesity in a study in South India. In
addition, using the Asian waist circumference cut–offs, the same study reported that 35.1% of
men and 56.2% of women had abdominal obesity, a higher level than any other national values
for countries in the region [21]. A study undertaken in six different geographical locations in
India (East, South, North, West/Central) showed different levels of obesity according to rural or
urban residence. In urban areas, obesity levels were as high as 30.7% in men and 38.8% in
women; whilst in rural areas values were 9.4% in men and 14.1% in women. In contrast, obesity
levels in slums were intermediate, 16.7% and 26.1%, for men and women respectively [22].
Similar patterns were reported for abdominal obesity.
Time trends in the prevalence of obesity
No well-designed nationally representative studies were found for the Maldives or Bhutan.
Limited time series information is available for other countries. Prevalence data were plotted in
the time trends according to the methodological similarities of the studies. BMI ≥25 kg/m2 was
used as it was the commonly used cut-off for most of the recent and earlier studies, which allows
54 Chapter 3: Manuscript 2
conclusions to be drawn on weight trends. An obvious upward trend was seen in all countries in
the region (figure 1a and 1b). In Sri Lanka, the age-adjusted prevalence of obesity in both men
and women increased from 7.0% (male) and 13.4% (female) in 1990 to 9.9% (male) and 19.2%
(female) in 2000. A further increase in obesity can be seen in 2005 (M: 16.4%; F: 20.7%)
[23,24] [14]. As obesity data in 1990 and 2000 were taken from an urban area (Colombo,
Maharagama) [23,24], the comparison in 2005 was taken from obesity prevalence in the urban
area [14]. Obesity prevalence in males may have be under-reported in 2000 and 1995 as the
authors used a BMI level of >27 kg/m2 as the obesity cut-off for males but >25 kg/m2 for female
counterparts [23,24].
Although the absolute prevalence of overweight and obesity in Nepal and Bangladesh are
currently the lowest in the region, the relative increases over the last two decades are the highest
in the region. A series of national or regional obesity datasets on ever-married, non-pregnant
women in Bangladesh show a clear positive trend in both urban and rural populations [25]. In
1996, only 2.7% of women had a BMI >25 kg/m2 and within three years the proportion had
reached 4.4%. By 2004, a value three times higher than in 1996 (8.9%) [25] was seen. In Nepal,
the prevalence of obesity among women was 1.6% which increased to 6.4% in 2001, then to
10.1% in 2006. This level of change over such a short period is the highest in the region. Despite
the absence of trend data on the prevalence of overweight and obesity in Pakistan, Shah et al.
[19] conducted two independent cross-sectional population surveys in rural Pakistan in 1995 and
2007. The age-adjusted prevalence of overweight and obesity (BMI >25 kg/m2) increased from
13.9% in 1995 to 19.4% in 2007. In men, the increase was from 15.4% to 19.5%; and in women
from 12.5% to 24.7%.
There are a few nationwide and several regional studies in India over the last few decades,
however, there is no series of national level study to cover all parts of the country. This may be
due to the size of the population and lack of resources. The National Nutrition Monitoring
Chapter 3: Manuscript 2 55
Bureau of India conducted a couple of large studies in nine rural states in India in 2000 [26] and
2005 [27]. The obesity prevalence was 5.7% and 8.2% in men and women respectively in 2000,
which increased to 7.8% and 10.9% in 2005. Although values are low in both circumstances,
obesity levels had increased by 37% and 32% in both men and women respectively over the
five-year period. Some regional studies reported very high levels of obesity, in particular in
urban areas [21,22,28]. However, in India, there is a considerable disparity in the prevalence and
in the time trends in the prevalence of obesity by different geographical regions and residents in
different areas of the same geographical location. A recent review noted the complexity of over
and under-nutrition problems in India [29].
Socio-economic factors associated with prevalence of obesity in the South Asian region
Several similar socio-economic factors are associated with the increase in obesity in the region.
*Sub-ethnicity – minor ethnicity groups; Healthy dietary habits (high fruits and vegetable intake,
low fat meals)
68 Chapter 3: Manuscript 2
Figure 3-1: Trends in the prevalence of obesity (BMI ≥25 kg.m-2) in Sri Lanka [14,23,24], Bangladesh [25], Nepal [25], India [26,27,28] and Pakistan [19] in adult males
Figure 3-2: Trends in the prevalence of obesity (BMI ≥25 kg.m-2) in Sri Lanka [14,23,24], Bangladesh [25], Nepal [25], India [26, 27,28]and Pakistan [19] in adult females
Prev
alen
ce
Prev
alen
ce
Years
Years
Chapter 4: Manuscript 3 69
Chapter 4: Manuscript 3
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Food consumption of Sri Lankan adults: an appraisal of serving characteristics Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
70 Chapter 4: Manuscript 3
TITLE PAGE
Food consumption of Sri Lankan adults: an appraisal of serving characteristics Ranil Jayawardena1,2, Nuala M. Byrne1, Mario J. Soares3, Prasad Katulanda2, Andrew P. Hills4 1Institute of Health and Biomedical Innovation, Queensland University of Technology, Brisbane, Queensland, Australia 2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka 3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health Sciences, Curtin University, Perth, WA, Australia 4Mater Mothers’ Hospital, Mater Medical Research Institute and Griffith Health Institute, Griffith University, Brisbane, Queensland, Australia
Citation
R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. (2012) Food consumption of Sri
Lankan adults: an appraisal of serving characteristics Public Health Nutrition: 16 (4); 653-658
Chapter 4: Manuscript 3 71
ABSTRACT
Objective
The main aim of this study was to identify food consumption in Sri Lankan adults based on
serving characteristics.
Design
This is a cross-sectional study. Fruits, vegetables, starch, meat, pulses, dairy products and sugar
were assessed in the diet with portion sizes estimated using standard methods.
Setting
Randomly selected twelve clusters from Sri Lanka Diabetes Cardiovascular Study.
Subjects
Six hundred non-institutional adults.
Results
The daily intake of fruits (0.4), vegetables (1.7) and dairy (0.4) portions were well below
national recommendations. Only 3.5% of adults consumed the recommended five fruits and
vegetables per day and over one third of the population consumed no dairy products, and less
than 1% of adults consumed 2 portions per day. In contrast, Sri Lankan adults consumed over 14
portions of starch, and 3.5 portions of added sugars daily. Almost 70% of those studied exceeded
the upper limit of the recommendations for starch intake. The total number of meat and pulse
portions was 2.78 per day.
Conclusion
Dietary guidelines emphasize the importance of a balanced and varied diet however a substantial
proportion of the Sri Lankan population studied failed to achieve such a recommendation. Health
promotion should be focused on improving healthier dietary habits among this population.
72 Chapter 4: Manuscript 3
INTRODUCTION
Sri Lanka is a developing country in South Asia undergoing rapid socioeconomic transition and
both over- and under-nutrition are serious health concerns. In 2005, the prevalence of
hypertension, diabetes and dysglycaemia in Sri Lanka was nearly 20%, 11% and 20%,
respectively [1,2]. Although Sri Lanka is a developing country, it has recorded 524 deaths per
100,000 for mortality from cardiovascular and cerebrovascular disease, a figure which is
considerably higher than the rate in many affluent countries such as the UK (427), USA (397),
Australia (308) and France (205) [3]. Despite Sri Lanka having a very high prevalence of NCDs
and associated mortality, little is known about its causative factors. It is widely believed that the
NCD epidemic in the country is partially associated with unhealthy dietary habits [3].
Food intake patterns play an essential role in the maintenance of health and wellbeing at both
individual and population levels. Food products supply energy, essential macro- and micro-
nutrients, however, over- or under-nutrition have the potential to cause serious health
consequences [4]. A national level dietary survey has several important functions and provides
valuable information. Survey data are also helpful to monitor nutritional status, observe dietary
practices and study the relationships between diet and disease. The main objective of this study
was to identify food consumption according to servings in Sri Lankan adults. In addition, the
present study aimed to derive serving sizes and food exchange information not presently
available for some food groups in Sri Lanka.
METHODOLOGY
Subjects
Participants for the present study were recruited based on the sample from the Sri Lanka
Diabetes and Cardiovascular study (SLDCS), a national study conducted between 2005 and
Chapter 4: Manuscript 3 73
2006. Detailed sampling procedures used in the SLDCS have been previously reported (figure
4.1) [2].
Figure 4-1: Subject selection process of the Sri Lanka Diabetes and Cardiovascular Study.
The current study was conducted between January and March 2011 during which time the
researchers were able to collect data from the previously missing North and Eastern provinces in
the SLDCS because of the improved security situation. In the original study, researchers
randomly selected 100 clusters consisting of 50 subjects according to the probability-
proportional-to-size method, to gain a representative sample from seven of the nine provinces.
74 Chapter 4: Manuscript 3
From the 100 clusters, ten were randomly selected stratifying to the area of residence and
ethnicity. To address the gap in national data from the remaining two provinces, we selected one
cluster of 50 participants from the North and East by using ‘Village Office Units’ voter lists to
randomly select one household. The remaining 49 households were selected applying the
uniform method used in the SLDCS. In summary, the total sample in the present study
comprised 600 subjects (500 from previous SLDCS areas and 100 additional from the Northern
and Eastern provinces). Figure 2 shows the data collecting sites. Those who were pregnant,
lactating, acutely ill or on a therapeutic diet were excluded. The present study was approved by
the Ethics Review Committee, Faculty of Medicine, University of Colombo, Sri Lanka.
Measurements
The selected households were initially contacted via telephone by the study team who provided
information regarding the study and verbal consent was taken. Where telephone facilities or
contact phone numbers were unavailable, households were visited by the study team with prior
postal notice. Subsequently, households were visited on a random day to minimize bias for food
selection. Dietary and demographic details were obtained after final written informed consent
was obtained. An interviewer-administered questionnaire was used for data collection.
Information regarding socio-demographic factors, timing of daily routines and meals were
obtained.
Chapter 4: Manuscript 3 75
Figure 4-2: Map of Sri Lanka with data collection (▀) sites
24-hour Dietary Recall
Two interviewers obtained dietary data by asking the participants what they ate in the previous
24-hours in direct chronological order. To minimize the inter-personal variation at the end of the
day two interviewers reviewed each other’s work and maintained homogeneity of the recording
procedure. Where there was a disparity in the dietary recalls, participants were re-contacted or
the 24-hour recall repeated on a different day. Food portion sizes were obtained using standard
household measurements such as plate, bowl, cup, glass, and different spoons; and these were
clarified by demonstration using real utensils and series of food portion size photographs and
food atlas [5, 6]. When participants recalled the amount of food consumed by weight this value
was entered.
76 Chapter 4: Manuscript 3
Data entry and analysis
The daily food intake was divided into seven food groups, namely 1) Cereal or equivalents
(starchy food); 2) Vegetables; 3) Fruits; 4) Meat or alternatives; 5) Pulses; 6) Dairy, and 7)
Added sugar. Detailed methodology regarding the translation of food eaten into the respective
food groups is provided in Appendix 1 (after this manuscript).
Method for translating food consumed into food group servings
All food recorded in 24-hour recall by each participant was assigned to one of the seven major
food groups defined above. Food was recorded either in household measures (cups, spoons etc.)
or by weight in the 24 hour recall and was translated into serving size for of each food
consumed. Thus, weight of food in grams or amount of household measure of food was divided
by weight of one serving or amount of household measure for one serving and summed to derive
servings of each food group. Food which was a mixture of several food types was disaggregated
before ingredients were categorized into appropriate food groups. An example of disaggregation
is illustrated in figure 4-3. A similar method was used for the US population for food grouping
when food mixtures required disaggregation [7]. The servings of food consumed in mixed foods
were calculated by modifying existing recipe files to develop a cascaded recipe file with multiple
levels of breakdown. Common recipes were accepted after checking for face validity by
consulting nutritionists and when in doubt, respective households were contacted [8]. For
uncommon food items, detailed recipes were collected at the time of the 24-hour dietary recall
from participants or other responsible person from each household.
Statistics
Average daily portion sizes were calculated as the total portion size divided by the number of
participants. The sum of vegetable and fruit portions were divided to obtain average daily fruit
Chapter 4: Manuscript 3 77
and vegetable consumption, and the same method was used to calculate average daily meat and
pulse intake. We analyzed the mean daily consumption of each food group according to gender.
Two sample t-tests were used to determine whether the mean values differed between the
genders. Data were analyzed using SPSS version 14 (SPSS Inc., Chicago,IL, USA) statistical
package. In all analyses a p value <0.05 was considered statistically significant.
RESULTS
Sample size was 490 (with a response rate of 82%), of which 34.5% (n=169) were males. The
socio-demographic profile of the study population is shown in Table 4.1.
The estimated mean daily servings from the five major pyramid food groups from the random
24-hour dietary recall, according to gender is shown in Table 2. In addition, sub-categories of
protein types, namely pulses and meat and alternatives, and added sugar are also reported. Mean
intake of fruits (0.43 portions/day) and vegetables (1.73 portions/day) were well below minimum
recommendations (fruits >2 portions; vegetables >3 portions). The total of fruit and vegetable
intake was 2.16 portions per day. Daily consumption of meat or alternatives was 1.75 portions
and the sum of meat alternatives and pulses was 2.78 portions per day. On average, Sri Lankan
adults consumed over 14 portions of starch daily, moreover males consumed five more cereal
portions compared to females. Sri Lankan adults consumed on average, 3.5 portions of added
sugars per day. Table 3 compares food consumption of Sri Lankan adults with national [9] and
international (US) recommendations [10].
We identified considerable variations in consumption frequency for each food type and their
portion size in the study population. Table 4 illustrates that participants reported an intake of
different portion sizes for main food groups and their combinations. Starchy foods were
consumed by everybody; and over 88% met the minimum daily recommendations. Importantly,
nearly 70% of adults exceeded the maximum daily recommendation for starch portions per day
78 Chapter 4: Manuscript 3
(11/day). More than 12% of men consumed ≥25 starch servings per day. In contrast to their
starch consumption, participants reported a very low intake of other food groups (Table 4). Only
11.6%, 2.1% and 3.5% of adults consume the minimum daily recommended servings of
vegetables, fruits and, combined fruit and vegetable servings, respectively. Six out of ten adult
Sri Lankans sampled did not consume any fruit. Milk and dairy consumption was extremely low,
over one third of the population did not have any dairy products and less than 1% of adults
consumed 2 portions per day. A quarter of Sri Lankans did not report consumption of meat and
pulses. Regarding protein consumption, 36.2% attained the minimum Sri Lankan
recommendation of protein; and significantly more men achieved the recommendation of ≥3
meat or alternative servings per day (M:42.6%; F:32.8%, p<0.05).
DISCUSSION
Recently, the WHO STEP survey reported on some dietary aspects from one health area in the
Western Province [11] but apart from this the present study represents the first national level
dietary survey undertaken in Sri Lanka to obtain habitual dietary intake data of the general
population. As the UK National Nutrition and Dietary Survey (NDNS) collected dietary details
from 1724 participants from a population of 60 million; we believe that the sample size of 600
used in the current study is within adequate limits.
During the last 5 years, Sri Lanka has faced significant urbanization and this has resulted in
some previous study clusters changing from rural to urban status. Whilst the present study
population is reasonably representative of all major ethnic groups in the country, there was a
higher proportion of urban living, mean age and participants with a higher mean BMI compared
to previous surveys [12]. Our results showed a low mean daily intake of fruit and vegetables
amongst Sri Lankan adults (2.16 portions) compared to the US (3.0) and France (3.6) [13]. The
Chapter 4: Manuscript 3 79
low intake of fruits and vegetables may be a contributing factor to the high prevalence of diet-
associated NCDs such as diabetes, non-alcoholic fatty liver and cardiovascular diseases in Sri
Lanka compared to other countries [3]. The specific reason for the low intake of fruit and
vegetables is unclear; studies from developed countries suggest a lack of perceived social
pressure to increase fruits and vegetable intake and suggest that increased public health efforts
require stronger health messages that incorporate consumer awareness of the low consumption
levels [14]. Moreover, peoples’ low purchasing ability and seasonal variation of fruits and
vegetables prices may adversely affect consumption. Despite five servings of fruits and
vegetables per day being considered the minimum daily intake by national dietary guidelines [9]
nearly half of the population eats less than 2 portions of fruits and vegetables, with less than 4%
reaching the minimum recommendation. Somathunga reported that 96.9% of Sri Lankan adults
did not consume five fruits and vegetables daily in the WHO Step Survey (2004) undertaken in
the Western province of Sri Lanka, comparable with our findings [11].
Pulses were the main source of protein, mainly dhal, the most common curry in the local
context, and boiled pulses eaten for breakfast. Although pulses are grouped in the protein
category, the main nutrient is carbohydrate, and thus invariably, consumption of pulses masks
significant amounts of carbohydrate. There is no conclusive evidence regarding protein intake
and disease risk in Sri Lanka. The MASALA study reported that higher levels of protein
consumption are associated with increased odds of diabetes in South Asians independent of age,
sex, waist circumference and hypertension [15]. A significant proportion of Sri Lankan males
(data not shown) consume over 5 servings of meat per day.
Sri Lankans consumed large numbers of starch servings; nearly 65% consumed well above the
upper cut-offs of the food pyramid guidelines and a considerable proportion of males consumed
very high levels of starch. This is mainly due to the average person’s meal being comprised of
three of quarters rice with a small amount of vegetable curry (averaging 15 g), a small piece of
80 Chapter 4: Manuscript 3
meat or fish (15 g) and some starchy curry such as potato or dhal (supplementary file 1).
Relatively low levels of starch portions were consumed by females mainly due to low absolute
food intake. A high carbohydrate meal leads to negative metabolic consequences such as
hyperinsulinaemia, high serum TAG and low HDL-cholesterol levels [16]. Most Sri Lankans
consume the largest starch portion for lunch or dinner and limit themselves to three meals per
day (data not shown); which may cause postprandial hyperglycaemia and
hypertriacylglycerolaemia [16]. More than one fifth of Sri Lankan adults are dysglycaemic and
the prevalence of diabetes is alarmingly high [2]; the high consumption of carbohydrate may be
associated with the diabetes epidemic in the country.
Dairy products provide valuable nutrients such as calcium, which is important for building and
maintaining strong bones. In addition, milk products provide several essential nutrients such as
proteins, vitamins and minerals. Lekamwasam and colleagues reported a 45% prevalence of
osteoporosis among postmenopausal women in Sri Lanka [8]. The CARDIA study revealed that
dairy consumption was inversely associated with the incidence of all individual components of
insulin resistance syndrome among individuals with a BMI ≥25 kg/m2 and increased dairy
consumption may reduce risk of type 2 diabetes and cardiovascular disease. Dairy intake is
substantially lower than Sri Lankan recommendations; over 1/3 of the population did not have
any dairy products and only 5% reached minimum levels. The main reason behind the low dairy
consumption could be the price of dairy products is unaffordable mainly due to the lack of local
production of dairy products and the consumption of dairy products largely depends on imported
milk powder [17];
This first national level dietary survey provides a sound basis for future food policy as it affects
Sri Lankan adults, and for the development of relevant nutrition education programs.
Furthermore, the rational assessment of food portion exchange tables will offer health
Chapter 4: Manuscript 3 81
professionals such as nutritionists, general practitioners, and nurses, valuable insights into Sri
Lankan meals and the development and prescription of meal plans in clinical and community
settings. A major strength of our study was the recruitment of a representative group from all
ethnic, education, areas of residence and age groups. Despite the relatively low participation of
male participants, women’s diet composition is similar to that of their male counterparts as most
Sri Lankan men eat at home. Second, the use of a random 24-hour dietary recall method helped
to obtain accurate results regarding dietary habits. Thirdly, disaggregation of food in Sri Lankan
dishes to guideline-based food groups leads to the more accurate counting of small portions of
foods in respective groups (as shown in figure 4-4). The main limitation of our data collection
and analysis was lack of data on oil consumption. Unlike meals in Western countries, coconut
oil, coconut milk or scraped coconuts are included in most mixed dishes which lead to
significant methodological challenges in obtaining accurate measurements of fat intake [18].
Secondly, portion sizes were estimated by recalling commonly used utensils and demonstrating
standard spoons, cups and plates, in addition to series of food photographs.
CONCLUSION
Dietary guidelines have emphasized the importance of a balanced and varied diet. Meals that
include no servings or very few servings of different food groups such as fruits and vegetables,
dairy products, fish and meat and pulses, lack both balance and variety. It is evident that a
substantial proportion of the Sri Lankan population does not consume a varied and balanced diet
which is suggestive of a close association between the nutrition-related NCDs in the country and
these unhealthy eating habits. We recommend that the government, health institutions and
organizations conduct larger national level dietary and nutrition surveys periodically to identify
associated disease conditions. This would allow practical public health initiatives to improve the
quality of the Sri Lankan diet.
82 Chapter 4: Manuscript 3
Chapter 4: Manuscript 3 83
REFERENCE LIST
1. Wijewardene, K., et al., Prevalence of hypertension, diabetes and obesity: baseline
findings of a population based survey in four provinces in Sri Lanka. The Ceylon
medical journal, 2005. 50(2): p. 62-70.
2. Katulanda, P., et al., Prevalence and projections of diabetes and pre-diabetes in adults in
Sri Lanka—Sri Lanka Diabetes, Cardiovascular Study (SLDCS). Diabetic Medicine,
2008. 25(9): p. 1062-1069.
3. Abeywardena, M., Dietary fats, carbohydrates and vascular disease: Sri Lankan
perspectives. Atherosclerosis, 2003. 171(2): p. 157.
4. Krebs-Smith, S., et al., Characterizing food intake patterns of American adults. The
American Journal Of Clinical Nutrition, 1997. 65(4): p. 1264S-1268S.
5. Michael Nelson et al, A Photographic Atlas of Food Portion Sizes. 1997, UK: MAFF
publications.
6. Suzana Shahar et al. Atlas of Food Exchanges & Portion Sizes. 2009, MDC Publishers:
Kuala Lampur.
7. Cleveland, L., et al., Method for assessing food intakes in terms of servings based on
food guidance. The American Journal Of Clinical Nutrition, 1997. 65(4): p. 1254S-
1263S.
8. Dissanayake, C., Ceylon Cookery. 9 ed. 2010, Sri Lanka: Stamford Lake (pvt) Ltd.
9. U.M.M. Samaranayake et al., Food Base Dietary Guidelines for Sri Lanka. 2011,
Colombo: Nutrition Devision, Ministry of Healthcare and Nutrition, Sri Lanka.
10. United States Department of Agriculture, The Food Guide Pyramid in Home and Garden
Bulletin Number 252 Center for Nutrition policy and Promotion, Editor. 1992. p. 17.
11. Somatunga, L.C., NCD Risk Factor Survey in Sri Lanka (STEP Survey). 2004, WHO.
84 Chapter 4: Manuscript 3
12. Katulanda, P., et al., Prevalence of overweight and obesity in Sri Lankan adults. Obes
Rev, 2010.
13. Tamers, S.L., et al., US and France adult fruit and vegetable consumption patterns: an
international comparison. Eur J Clin Nutr, 2009. 63(1): p. 11-7.
14. Levin, A., Nutrition and Policy. 5: Who Should Teach Patients about Nutrition? Annals
of Internal Medicine, 1999. 131(4): p. 317-318.
15. Wang, E.T., L. de Koning, and A.M. Kanaya, Higher Protein Intake Is Associated with
Diabetes Risk in South Asian Indians: The Metabolic Syndrome and Atherosclerosis in
South Asians Living in America (MASALA) Study. Journal of the American College of
Nutrition, 2010. 29(2): p. 130-135.
16. Misra, A., et al., South Asian diets and insulin resistance. Br J Nutr, 2009. 101(4): p.
465-73.
17. FAO, Sri Lanka –dairy products, in FAO Briefs on Import Surges. 2007, Trade and
Markets Division (EST), Food and Agriculture Organization of the United Nations
(FAO): Rome.
18. Amarasiri, W.A. and A.S. Dissanayake, Coconut fats. Ceylon Med J, 2006. 51(2): p. 47-
51.
Chapter 4: Manuscript 3 85
Table 4-1: Demographic characteristics and BMI characteristics of the sample Variables Males (N=169) Female (N=321)
Age (y) (mean±SD) 48.4±15.6 48.1±14.1
Area of residence % (n)
• Urban
• Rural
• Estate †
27.8 (47)
60.4 (102)
11.8 (20)
36.1 (116)
57.6 (185)
6.2 (20)
Ethnicity % (n)
• Sinhalese
• Muslim
• Sri Lankan Tamil
• Indian Tamil
71.0 (120)
4.7 (8)
11.8 (20)
12.4 (21)
80.1(257)
7.2(23)
7.2(23)
5.6(18)
Education level % (n)
• No Schooling
• Up to 5 years
• Up to 11 years
• Up to 13 years
• Graduate
6.5 (11) 6.5 (21)
27.2 (46) 25.2(81)
34.9(59) 40.5(130)
27.2(46) 22.7(73)
4.1(7) 5.0(16)
BMI (kg/m2) (mean±SD) 21.97±3.45 23.73±4.29
† Tea and rubber plantation zones
86 Chapter 4: Manuscript 3
Table 4-2: Average dietary intake of servings from different food group by Sri Lankan adults Food group Mean portions (SD)
All adults SD Males SD Females SD
Starch 14.06 5.59 17.17 6.17 12.39 4.45
Fruits 0.43 0.62 0.44 0.77 0.43 0.65
Vegetables 1.73 1.25 1.95 1.42 1.61 1.13
Meat or alternatives 1.75 1.63 1.92 1.88 1.65 1.48
Pulses 1.04 1.01 1.29 1.24 0.90 0.83
Dairy 0.39 0.46 0.40 0.48 0.39 0.45
Sugar 3.56 3.10 3.64 3.34 3.51 2.97
Fruit and vegetable 2.16 1.46 2.39 1.65 2.04 1.34
Pulses and meats 2.78 1.87 3.22 2.14 2.55 1.66
Table 4-3: Comparison of food intake of Sri Lankan adults with national and international recommendations.
Food groups Average intake of portions
National recommendations [9]
US recommendations[10]
Starch 14 6-11 6-11
Fruits 0.4 2-3 2-4
Vegetables 1.7 3-4 3-5
Fruits and vegetables 2.1 ≥ 5 ≥ 5
Meat and pulses 2.8 1-2 2-3
Dairy 0.4 1-2 2-3
Sugar 3.6 low Sparingly
Chapter 4: Manuscript 3 87
Table 4-4: Percentage distribution of the study sample according to their consumed foods portions from different food groups
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Development of a food frequency questionnaire for Sri Lankan adults. Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Sumathi Swaminathan Study design and statistics analysis Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
98 Chapter 5: Manuscript 4
TITLE PAGE
Development of a food frequency questionnaire for Sri Lankan
adults.
Ranil Jayawardena1,2*, Sumathi Swaminathan3, Nuala M. Byrne1, Mario J. Soares 3,4,
Prasad Katulanda2, Andrew P. Hills5
1Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of
Technology, Brisbane, Queensland, Australia.
2Diabetes Research Unit, Department of Clinical Medicine, Faculty of Medicine, University of
Colombo, Colombo, Sri Lanka.
3St John's Research Institute, St John’s National Academy of Health Sciences, Bangalore, India.
4Curtin Health Innovation Research Institute, School of Public Health, Curtin University, Perth,
Western Australia.
5Mater Mothers’ Hospital, Mater Medical Research Institute and Griffith Health Institute,
beverages (n=7), miscellaneous (n=14), and alcohol (n=5).
The paper describes the process of development of a FFQ for Sri Lankan adults using a
nationally representative sample. Dietary assessment of this population is invaluable to
understand the role of nutrition in chronic disease so that preventive strategies can be
implemented. The aim of dietary assessment of populations is to rank people by a measure of
usual rather than current diet. The strengths of this study include a nationally representative
sample of Sri Lankan adults and the creation of a comprehensive new database for nutrient
analysis. However, males are under-represented in this study which stems from data collection
being on a random day when most males were engaged in active occupations away from home.
However, in Sri Lanka family members consume similar foods; therefore, obtaining dietary data
from females did not significantly affect the food list in our study. The number of food items in a
FFQ is a crucial factor in determining the accuracy of the data and the practicability of the
questionnaire. Many FFQs have between 100–150 items [25] and the risk of over-reporting
through increased subject burden increases with the large number of items [22, 25]. In our FFQ,
106 Chapter 5: Manuscript 4
we have 90 items and 12 photos of food items to enable an accurate estimation of dietary
exposure.
Sri Lanka as a tropical island has no clear four seasons but two monsoons influence cultivation.
Hence, additional seasonal fruits and vegetables are also included in our FFQ. Over 55% of adult
males are current alcohol drinkers [26]; however in our data collection alcohol consumption was
under-reported (0.5% of participants) with no women reporting the consumption of alcohol. In
Sri Lanka, drinking alcohol has negative social and religious stigma. Thus, common alcoholic
beverages were added to the FFQ. Dietary recalls indicated differences between the ethnic
groups in the type of nutrients derived from different food sources. The main carbohydrate
source varied among ethnic groups; Indian Tamils reported consuming wheat flower (as Roti)
whereas Sinhalese eat rice as the main staple food and Sri Lankan Tamils consume Dose, Itale
and Wade frequently. Ethnicity was an important factor in the selection of foods containing
protein, not surprisingly; pork and beef consumption was not reported by Moors (Muslims) and
Tamils, respectively.
A variety of methods are available to collect food consumption data but a common challenge for
individual-based dietary assessment methods is portion size estimation. Although weighing
served portions is often considered the gold standard; for practical reasons, portion estimation
using photographs are used among both adults and children [27]. A study conducted in Burkina
Faso showed that food photographs are valuable for the quantification of food portion size
among rural and less educated middle-aged women [28]. Men usually consume larger portions
than women [29] and the use of photographs helps to categorize gender variation in portion sizes
more precisely. This is crucial to obtaining reliable estimates of macronutrient and micronutrient
intakes. Several countries use FFQs with photo series and scoring systems [30, 31].
Chapter 5: Manuscript 4 107
The main weakness of the previous national level NCD survey (SLDCS) was the absence of
nutritional data on the population and their relationship with the high NCD risk in the country.
One of the main objectives of the current work was to develop a FFQ to administer in the next
national level NCD survey. Moreover, this FFQ could also be used to assess dietary habits of Sri
Lankans living in other countries, as they practice similar eating patterns to native Sri Lankans.
There is no updated nutrient database in the country. Sri Lankan food composition tables were
published in 1979, and since then many chemical analysis techniques have changed. Newer
processed food items have been introduced into the market. We used the USDA food
composition tables as the backbone of our nutrient database. This is arguably the most
comprehensive, standardized, largest and continuously updated database that has used to develop
population-specific food composition tables in other countries [25]. Mixed dishes were not listed
in the USDA database, and for such items we followed calculated values from traditional
recipes. The recipes vary according to ethnic groups in Sri Lanka and were therefore modified to
allow generalization to the whole country.
Limitations
Coconut oil is the main cooking oil in Sri Lanka [32], however, other types of cooking oils are
used in different communities. Our FFQ does not enable us to differentiate the types of cooking
oil consumed which may have important health implications for NCDs. However, we used
additional questions to obtain details of oil consumption. Another limitation is the lack of data
on micronutrients on Sri Lankan mixed dishes, prolonged cooking time and addition of various
spicies and herbs which could alter the nutritional values of the raw ingredients [33].
108 Chapter 5: Manuscript 4
CONCLUSION
This study highlights the development of a FFQ and the related nutrient composition database
for Sri Lankan adults. Culturally specific dietary tools are central to capturing the role of diet in
risk for chronic disease in Sri Lanka. While the reproducibility and validity of this FFQ needs to
be determined, an important ongoing program would be the regular updating of the new nutrient
database we have also developed.
Acknowledgements
The authors would like to acknowledge Miss Fathima Shakira and other members in the
Diabetes Research Unit, Colombo, for their contribution in arranging logistics for the study.
Chapter 5: Manuscript 4 109
REFERENCE LIST
1. Somatunga, L.C., NCD Risk Factor Survey in Sri Lanka (STEP Survey). 2004, WHO.
2. Stamler, J., Assessing diets to improve world health: nutritional research on disease causation in populations. American Journal of Clinical Nutrition, 1994. 59(1): p. 146S.
3. Lee R.D., N.D.C., National Dietary and Nutrition Surveys, in Nutritional Assessments, D.C.N. Robert D. Lee, Editor. 2002, McGraw-Hill Science Engineering. p. 111-143.
4. Willett, W., Nutrition Epidermiology. 2 ed. 1998, NEW YORK: Oxford University Press.
5. FAO, FAO-Nutrition Country Profiles. 1999, Food and Agriculture organization of the United Nations Rome.
6. Popkin B.M., H.S., Kim S.,, The Nutritional Transition and Diet-Related Chronic Diseases in Asia: Implications for Prevention. Washington, DC: International Food Policy Research Institute FCND Discussion Paper, 2001. 105.
7. Meera Shekar, A.S., Lidan Du, , Malnutrition in Sri Lanka: Scale, Scope, Causes, and Potential Response, W. Bank, Editor. 2007, Human Development Unit, South Asia Region.
8. Katulanda, P., et al., Prevalence and projections of diabetes and pre-diabetes in adults in Sri Lanka—Sri Lanka Diabetes, Cardiovascular Study (SLDCS). Diabetic Medicine, 2008. 25(9): p. 1062-1069.
9. Wijewardene, K., et al., Prevalence of hypertension, diabetes and obesity: baseline findings of a population based survey in four provinces in Sri Lanka. The Ceylon medical journal, 2005. 50(2): p. 62-70.
10. Katulanda, P., et al., Prevalence of overweight and obesity in Sri Lankan adults. Obes Rev, 2010.
11. Katulanda, P., et al., Metabolic syndrome among Sri Lankan adults: prevalence, patterns and correlates. Diabetology & Metabolic Syndrome, 2012. 4(1): p. 24.
12. Samaranayake U.M.M. et al., Food Base Dietary Guidelines for Sri Lanka. 2011, Colombo: Nutrition Devision, Ministry of Healthcare and Nutrition, Sri Lanka.
13. Jayawardena R., B.N.M., Soares M.J., Katulanda P., Hills A.P.,, Consumption of Sri Lankan adults: an appraisal of serving characteristics Public Health Nutrition, 2012. FirstView:1-6.
14. Nelson M., A.M., Meyer J.,, A Photographic Atlas of Food Portion Sizes. 1997, UK: MAFF publications.
110 Chapter 5: Manuscript 4
15. Shahar S., Y.N.A.M., Safii N.S., Ghazau R., Ahmad R., , Atlas of Food Exchanges & Portion Sizes. 2009, MDC Publishers: Kuala Lampur.
16. Perera W.D.A., J.P.M., Thaha S.Z., , Tables of food composition for use in Sri Lanka. 1979.
17. USDA. Foods List. National Nutrient Database for Standard Reference 2012 3/30/2012; 24:[Available from: http://ndb.nal.usda.gov/ndb/foods/list.
18. Gopalan C., R.B.V., Balasubramanian S.C.,, Nutritive value of Indian foods, ed. N.I.o. Nutrition. 1989, Hyderabad.
19. Welch A.A., U.I.D., Buss D.H., Paul A.A., Southgate D.A.T., , McCance and Widdowson’s The Composition of Foods. 5th ed. 1995, Cambridge: Royal Society of Chemistry.
20. Dissanayake, C., Ceylon Cookery. 9 ed. 2010, Sri Lanka: Stamford Lake (pvt) Ltd.
21. Hodge A., P.A.J., Brown W.J., Ireland P., Giles G., , The Anti Cancer Council of Victoria FFQ: relative validity of nutrient intakes compared with weighed food records in young to middle-aged women in a study of iron supplementation. Australian and New Zealand Journal of Public Health 2000. 24(6): p. 576-586.
22. Kobayashi, T., et al., Development of a food frequency questionnaire to estimate habitual dietary intake in Japanese children. Nutrition Journal, 2010. 9(1): p. 17.
23. Ireland P., J.D., Giles G., O'Dea K., Powles J., Rutishauser I., Wahlqvist M.L., Williams J.,, Development of the Melbourne FFQ: a food frequency questionnaire for use in an Australian prospective study involving an ethnically diverse cohort. Asia Pacific J Clin Nutr, 1994. 3: p. 19-31.
24. Bharathi, A., et al., Development of food frequency questionnaires and a nutrient database for the Prospective Urban and Rural Epidemiological (PURE) pilot study in South India: Methodological issues. Asia Pacific Journal of Clinical Nutrition, 2008. 17(1): p. 178-185.
25. Dehghan, M., et al., Development of a semi-quantitative food frequency questionnaire for use in United Arab Emirates and Kuwait based on local foods. Nutrition Journal, 2005. 4(1): p. 18.
26. Rahav, G., et al., The influence of societal level factors on men's and women's alcohol consumption and alcohol problems. Alcohol and alcoholism (Oxford, Oxfordshire). Supplement, 2006. 41(1): p. i47-55.
27. Frobisher C., M.S.M., The estimation of food portion sizes: a comparison between using descriptions of portion sizes and a photographic food atlas by children and adults. Journal of Human Nutrition and Dietetics, 2003. 16(3): p. 181-188.
28. Huybregts, L., et al., Validity of photographs for food portion estimation in a rural West African setting. Public Health Nutrition, 2008. 11(06): p. 581-587.
29. Caster, W.O., Systematic estimation of food intakes from food frequency data. Nutrition Research, 1986. 6(4): p. 469-472.
30. Victoria, C.C. Dietary questionnaires. 2010; Available from: http://www.cancervic.org.au/about-our-research/epidemiology/nutritional_assessment_services.
31. Ocké, M.C., et al., The Dutch EPIC food frequency questionnaire. I. Description of the questionnaire, and relative validity and reproducibility for food groups. International Journal of Epidemiology, 1997. 26(suppl 1): p. S37.
32. Amarasiri, W., Coconut fats. Ceylon Med J, 2009. 51(2).
33. Khokhar S., R.M., Swan G.,, Carotenoid and retinol composition of South Asian foods commonly consumed in the UK. Journal of Food Composition and Analysis, 2012. 25(2): p. 166-172.
Table 5-3: Elements of the food frequency questionnaire
* Dairy, sweets, desserts, nuts
Cereals or
equivalents
Vegetables Pulses Meat or
alternatives
Fruits Beverages Miscellaneous* Alcohol
Total food items and mixed dishes
36 48 11 17 19 13 29 2
Contribution of 90%
28 21 5 9 9 7 12 2
Grouping of food items
19 18 5 9 9 7 12 2
Inclusion of foods 0 2 1 1 1 0 2 3
Final food items 19 20 6 10 9 7 14 5
Chapter 5: Manuscript 4 115
Supplementary file 1
Figure 5-1: Example of a food photograph (200 g of rice)
116 Chapter 6: Manuscript 5
Chapter 6: Manuscript 5
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Energy and Nutrient Intakes among Sri Lankan Adults
Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Shalika Tennakoon data collection and data analysis Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
Chapter 6: Manuscript 5 117
TITLE PAGE
Energy and Nutrient Intakes among Sri Lankan Adults
R. Jayawardena1,2*, S.N. Thennakoon2, N.M. Byrne1, M.J. Soares3, P. Katulanda2, A.P.
Hills4
1Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of
Technology, Brisbane, Queensland, Australia.
2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka.
3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health
R Jayawardena, SN Thennakoon, NM Byrne, MJ Soares, P Katulanda, AP Hills. Energy and
Nutrient Intakes among Sri Lankan Adults. BMC Research Notes (in press) MS:
1400644043847201
118 Chapter 6: Manuscript 5
ABSTRACT
Introduction
Dietary practices are a key factor related to health status at both individual and population levels.
Over- and under-nutrition both have the potential to contribute to serious health consequences.
Sri Lanka is undergoing a rapid socioeconomic transition which is related to a significant health
burden related to under-nutrition and an epidemic of non-communicable diseases. However, to
date, detailed data on food consumption in the Sri Lankan population is limited. The aim of this
study was to identify energy and major nutrient intake among Sri Lankan adults.
Methods
A nationally-representative sample of adults was selected using a multi-stage random cluster
sampling technique. An interviewer-administered 24-h dietary recall was used to obtain data
concerning the nutritional intake of the population. NutriSurvey® software was used to analyze
the nutritional composition of typical meals.
Results
Data from 463 participants (166 Males, 297 Females) were analyzed. Total energy intake was
significantly higher in males (1913±567 kcal/d) than females (1514±458 kcal/d). However, there
was no significant gender differences in the percentage of energy from carbohydrate
(Male:72.8±6.4%, Female:73.9±6.7%), fat (Male:19.9±6.1%, Female:18.5±5.7%) and protein
(Male:10.6±2.1%, Female:10.9±5.6%). The average intake of dietary fiber was 21.3 g/day and
16.3g/day for males and females, respectively. There was a significant difference in nutritional
intake related to ethnicities, areas of residence, education levels and BMI categories.
Discussion
The present study provides the first national estimates of energy and nutrient intake of the Sri
Lankan adult population. Regular nutrition surveys are needed at the national level to obtain
valuable information on diet and associated diseases.
Chapter 6: Manuscript 5 119
INTRODUCTION
The epidemic of nutrition related non-communicable diseases (NCDs) such as type 2 diabetes
mellitus, obesity, cardiovascular diseases (CVDs) and certain cancers are continuing to
challenge the health sectors in Asia [1]. Sri Lanka is a low-middle income South Asian country
with a population of approximately 20 million. Despite most Sri Lankans having relatively good
health status, during the last two decades NCDs have become a more prominent health issue in
the country [2]. A quarter of Sri Lankan adults suffer from metabolic syndrome [3]. According
to results from the Sri Lanka Diabetes and Cardiovascular Study (SLDCS), the prevalence of
diabetes among Sri Lankan adults was nearly 11% and one-fifth of adults have diabetes or pre-
diabetes while one third of those with diabetes are un-diagnosed [4]. Premarathna et al. have
also reported that there was an increase in the incidence of hospitalization of Sri Lankan adults
by 36%, 40% and 29% due to diabetes mellitus, hypertensive disease and ischemic heart disease,
respectively, in 2010 compared to 2005 [5]. Diet-related chronic diseases currently account for
18.3% of all deaths and 16.7% of hospital expenditure in the country [1]. There is a significant
health burden due to NCDs and this will be a challenge to the health sector in a developing
country like Sri Lanka.
Some methods to assess the quantity and quality of dietary intake include prospective food
records (with weighed or estimated food portions), retrospective 24-h recalls (24 HDR), and
food frequency questionnaires (FFQs) [6]. The 24HDR which is less time-consuming and has a
low respondent burden, is the method used to gather the quantitative estimate of all foods and
beverages an individual has consumed in the previous 24 hours at a population level. Several
national dietary surveys have used 24 HDR and it is known to be acceptable for gathering
dietary information on a given day at the population level [7,8].
120 Chapter 6: Manuscript 5
National diet and nutrition surveys provide valuable information on a possible partial
explanation for the people’s health status and disease risk [9]. Assessment of the dietary and
nutritional status of the population is also essential to monitor the ongoing nutrition transition in
a country [6]. As a developing country, no studies have been carried out to investigate the
information on the diet of Sri Lankans and their nutritional status at a national level. Since Sri
Lanka is a multi-cultural country, peoples’ foods and dietary habits at a national level should be
assessed with a representative sample of Sri Lankan adults, which will be more useful to
implement health policies and to initiate many interventions. By keeping this view in mind, the
current dietary survey was carried out to assess the intakes of energy, macro-nutrients and
selected other nutrients with respect to socio-demographic characteristics and the nutritional
status of Sri Lankan adults focusing on diet-related metabolic chronic disease.
METHODOLOGY
Study sampling and the subjects
The eligible respondents of this study were healthy Sri Lankan adults aged >18 years recruited
from a sub-sample of the Sri Lanka Diabetes and Cardiovascular Study [4]. In this study, a total
of 600 subjects were randomly selected representing all nine provinces. This sample population
was then stratified for area of residence and ethnicity. Description of sample selection is
published elsewhere [10]. Ethical approval for this study was obtained from the Ethical Review
Committee, Faculty of Medicine, University of Colombo, Sri Lanka.
Measurements
Socio-demographic variables
The selected subjects were initially contacted via telephone or a postal notice by the study team
and the information regarding the study was provided in order to obtain their willingness to
participate in the study. On the study day, the purpose of the study was briefly explained to the
subjects and information sheets related to the study were also given out. Written consent was
Chapter 6: Manuscript 5 121
obtained from each volunteer prior to data collection. Socio-demographic details and diabetes
status were obtained by using an interviewer-administered questionnaire and body weight and
height were measured using a standard method. Areas of residence, ethnicities, and education
levels were categorized according to Sri Lankan governmental standards [11]. Body mass index
(BMI) was calculated by weight (in kilograms) divided by height squared (in meters) and several
cut-offs were presented as recommended by WHO experts for Asian populations [12].
Dietary assessment
Dietary data were obtained from a 24 HDR method. Subjects were asked to recall all foods and
beverages consumed over the previous 24-hour period. Respondents were probed for the types of
foods and food preparation methods. For uncommon mixed meals, the details of recipes and
preparation methods were collected at the time of taking the 24 HDR. Dietary recalls were
collected by two trained nutritionists who had received uniform training and adhered to the
standard operating procedure (SOP). As dietary assessment aids, the standard household
measurements such as plate, bowl, cup, glass, and different spoons etc. and food photograph
atlases were used to facilitate the quantification of portion sizes. One medium-sized coconut
spoon of rice was taken as 100 g, a full plate as 400 g, one cup of liquid as 150 ml, one glass of
liquid as 200 ml, a table spoon as 15 g and a tea spoon was taken as 5 g. For different curries,
weights of average respective amounts were taken. Household measurements were clarified by
demonstration of the real utensils and the food portion size photographs. When subjects recalled
some food amount in grams, that information was directly entered. Further details of dietary
assessment were published previously [10].
Data analysis
All foods recorded in 24 HDR were converted into grams and then, the intake of total energy,
macro nutrients (Carbohydrate, Protein and Fat), sodium and dietary fiber were analyzed using
122 Chapter 6: Manuscript 5
NutriSurvey 2007 (EBISpro, Germany) which was modified for Sri Lankan food recipes. As no
updated nutritional database has been gathered for some Sri Lankan food, we used the US
Department of Agriculture (USDA) nutrient database [13] as our standard to estimate nutrient
content in addition to local and regional food composition databases [14, 15]. Due to the absence
of energy and nutrient information on local mixed cooked dishes, we used a cookery book [16].
All the recipes were accepted after checking for face validity by consulting local housewives and
nutritionists. According to recipes, ingredients were weighed to the nearest 1 g for edible
portions of the foods. Then food items were cooked accordingly and the end product was
weighed. Nutritional composition of the final meal was calculated by entering nutritional values
and the weight of individual ingredients to the spreadsheet. The sum of each nutrient was
computed and standardized to 100 g of final product. We also excluded participants whose
reported daily energy intake was not between 800 and 4200 kcal to identify under- and over-
reporters of food intake [17].
Statistical Analysis
All data were doubly entered and rechecked in Microsoft Excel 2007. Data sorting and cleaning
were carried out before data analysis. Data on energy, macro-nutrients and some selected
nutrient intakes were transferred from the NutriSurvey 2007 to the Minitab version 15.0 for
statistical analysis. Nutrient intake distributions are presented as mean ±SE, median, 25th and
75th percentiles to characterize population intake levels for socio-demographic characteristics
(gender, ethnicity, age groups, and educational levels) and BMI categories. One-way ANOVA
and t-test were used to examine the differences in mean intakes energy and nutrients intakes. P
value < 0.05 was considered statistically significant.
Chapter 6: Manuscript 5 123
RESULTS
Socio-demographic profile
From 600 subjects, 491 (81.8%) participated and 28 under-reported their energy intake.
Accordingly, a total of 463 (77.2%) were included for the analysis. Socio-demographic profiles
and BMI categories of subjects are presented in Table 6.1. The majority of subjects were from
rural areas (59.7%) with 33% of the population from urban areas and the balance from the estate
sector (tea plantation area) 7.3%. The majority were women (n=297). By ethnic group, the
following were represented: Sinhalese (78%), Sri Lankan Tamil (9%), Indian Tamil (7%), and
Muslim (6%). Adults between the age of 41 and 50 years formed the biggest group (25.27%)
while the smallest group was the youngest adults aged between 18-30 yrs (13.17%). It was
significant that a majority of the study population (39%) had received formal education up to
Ordinary Level. The next largest group was adults (25%) who had studied up to Advanced
Level.
Energy intake
Table 6.2 represents the distribution of energy intake of Sri Lankan adults. The mean energy
intake of men was significantly higher (1912.7 kcal/d) than that of women (1513.6 kcal/d)
(p<0.05). People living in the estate sector had a significantly lower energy intake compared to
both the urban and rural subjects (p<0.05). Muslims had the highest intake of daily energy
(1748.8 kcal) while Indian Tamils had the lowest (1437.7 kcal/d) a statistically significant
difference for both men and women (p<0.05). Calorie consumption of both gender groups
declined gradually with age. Energy intake increased gradually with educational level.
According to BMI categories, lower energy levels were reported in both extremes and no distinct
pattern was seen.
124 Chapter 6: Manuscript 5
Carbohydrate intake
The mean daily carbohydrate intake is shown in Table 6.3. The total mean carbohydrate intake
of Sri Lankan adults was approximately 304.4 g (71.2% of total energy from carbohydrates as
shown in Figure 1). By strata, rural adults had a higher intake of carbohydrate (307.7 g) than
their estate counterparts (270.3 g). Mean carbohydrate intake was highest in Sinhalese (308.7 g)
and lowest in Indian Tamils (269.9 g). Male adults’ carbohydrate intake (352.4 g/day) was
significantly higher than that of women (277.5 g/day) and carbohydrate intake declined with age.
Protein intake
Sri Lankan adults recorded a mean daily protein intake of 44.6 g with men’s intake (52.8 g)
significantly higher than that of women (40.0 g). As shown in Table 6.4, rural (42.9 g/day) and
estate (43.7g/day) adults had similar daily intakes of protein. However, by ethnicity, mean
protein intake was significantly higher in Muslims (52.2 g) compared others. The youngest age
group also consumed significantly more protein than others, but only in men.
Fat intake
Estimated daily mean fat intake of Sri Lankan adults was 35 g. A more or less similar fat
consumption was noted for rural and urban residents (Table 6.5) whereas estate people had
significantly lower intake of fat (24.76 g; p>0.05). The youngest age group recorded the highest
fat intake (37.7 g) while the lowest intake was observed in the oldest age group (30.8 g). By
ethnic group, Muslims had the highest fat intake (44.7 g) whilst the Indian Tamils had the lowest
(24 g), being significantly lower than Muslims (p<0.05). With education level, fat consumption
increased, particularly among men. Adults with a normal BMI and BMI >25 - < 27.5 kgm-2 had
a higher fat intake than other BMI categories.
Chapter 6: Manuscript 5 125
Energy contribution from macro nutrients
As a whole, 71.2% of total calories came from carbohydrates, 10.8% from protein and 18.9%
from fat. Comparisons of the percentage of total calories derived from macronutrients according
to socio-demographic profile and BMI categories are shown in Figure 6.1. By ethnic group,
Muslims consumed more energy from fat (22.3%) while Indian Tamils had the lowest amount of
fat (15.5%) and highest intake of carbohydrates (75%). The percentage of calories from protein
was relatively higher among the graduates. In contrast, adults who did not receive a formal
education had a higher percentage of calories from carbohydrates compared to other groups.
There was no difference in energy distribution between diabetic and non-diabetic subjects.
Dietary fiber
The daily mean dietary fiber intake of Sri Lankan adults was 18.1 g (men: 21.3 g; women: 16.3
g; p<0.05). By area of residence, estate adults had a higher dietary fiber intake (20.6 g) than their
urban and rural counterparts (Table 6.6). Mean dietary fiber intake was highest in Indian Tamils
(20.6 g) and lowest in Sinhalese (17.6 g) (p<0.05). Dietary fiber intake increased with
educational level and a similar trend was observed for women as men. Daily dietary fiber intake
was always higher among men than women from different socio-demographic backgrounds.
Adults aged >60 years had the lowest intake of fiber.
Sodium
Daily mean sodium intake was 3.26 g and 2.51 g for men and women, respectively (p<0.05).
Dietary sodium intake of Sri Lankan adults according to demographic and BMI categories is
shown in Table 6.7. Mean sodium intake of rural adults was 2.89 g, followed by urban adults
(2.73 g). The Estate sector had the lowest intake (2.48 g). Muslims and Sri Lankan Tamils had a
higher intake of sodium than Sinhalese and Indian Tamils. With aging, sodium intake declined
and the youngest age group recorded the highest intake (3.04 g).
126 Chapter 6: Manuscript 5
DISCUSSION
Although national dietary and nutrition surveys have a number of important functions and can
provide much valuable information, Sri Lanka had never conducted a national food consumption
survey, probably due to lack of human and financial resources. This is the first attempt to report
energy and macronutrient intakes in a fairly representative sample over the island using updated
food composition data. Subject distribution of ethnic groups, area of residence and educational
levels closely mirror the national statistics [11].
Differences in calorie consumption were seen according to demographic and BMI categories.
Men typically consume larger portions of foods and are expected to derive a higher amount of
energy than their female counterparts [18]. The daily intake of energy by Sri Lankan men was
found to be higher than that of women by about 350 kcal. Similar differences were reported
among Malaysian adults [19] and in Britain where the difference was nearly 700 kcal [20].
When compared to people living in urban and rural areas, estate workers consume fewer
calories. Lower mean energy intake was also reported among Malaysian estate workers [21].
The decline in calorie consumption with age was probably due to a reduction in physical activity
levels and poor appetite, particularly in older adults. Different energy intakes in ethnic groups
may represent their cultural eating habits. For instance, Muslim people tend to have a higher
energy intake and eat more fat rich food items compared to Indian Tamils. Up to A/L (12 years
education) by education level, energy consumption gradually increased, which is probably
associated with increased purchasing power with higher education status; however, graduate
groups may be also aware of health issues associated with excess caloric intake. In developed
countries, calorie consumption is inversely associated with education levels [22]. Except for the
very obese category, consumption of total energy intake rose steadily with BMI category.
Under-reporting of food intake by obese subjects is well documented [23].
Chapter 6: Manuscript 5 127
The total daily intake of protein in Sri Lankan adults is almost half that of US adults and, among
Americans, two-thirds of all protein is derived from animal sources [24]. In contrast, plant
sources (rice and pulses) are the main contributors of protein among Sri Lankan adults [10,25].
American men consume over 100 g of fat daily and for women, 65 g [26]. Corresponding values
for Sri Lankans are 40.5 g and 31.9 g, respectively. In addition to the amount of fat, the type of
fat is crucial for the development of diet-related chronic diseases such as cardiovascular disease.
Although sub-types of fat are not reported in this analysis, the main lipid source in the Sri
Lankan diet is coconut milk/oil which is high in saturated fatty acids [27]. Therefore, it is
important to conduct further studies to explore the coconut consumption and associated
cardiovascular disease risk in this population.
According to the ranges of population nutrient intake goals recommended by WHO, the
percentage of energy from total carbohydrates, fats and proteins should be 15-30%, 55-75% and
10-15%, respectively [28]. British adults consume less than fifty percent of calories (men:
47.7%; women: 48.5%) from carbohydrates, whilst fat intake contributes 35.8% and 34.9% of
total calories for men and women, respectively. The contribution of protein as an energy source
is 16.5% for both sexes [20]. In contrast to Western countries, Malaysians derive nearly 60% of
their energy from carbohydrates, 14% of energy from protein and the rest from fats [19]. In
contrast to Western countries and some Asian countries, Sri Lankan adults consume
proportionally more carbohydrates (>71% of calories) and less fat (<19% of calories) and
proteins (<11%). The prevalence of diabetes in Sri Lanka is 11% and one-fifth of adults are
suffering from diabetes despite low levels of obesity (BMI >30 kg/m2 = 3.7%) [4]. Since the
study is cross-sectional in nature, we cannot conclude that the association between the relatively
larger contribution of energy from carbohydrate and higher prevalence of diabetes/dysglycemia
among Sri Lankan adults, in spite of carbohydrates contributing over 70% of energy for both
128 Chapter 6: Manuscript 5
diabetics and non-diabetics. Longitudinal studies assessing the prospective risk of developing
diabetes and the proportion of energy derived from macronutrients are needed to fully elucidate
an association. A high intake of carbohydrate may lead to hyperinsulinaemia, high serum TAG
and low HDL-cholesterol levels and chronic consumption of large carbohydrate meals may
cause postprandial hyperglycaemia and hypertriacylglycerolaemia and eventually develop
insulin resistance and diabetes [29].
A generous intake of dietary fiber reduces risk of developing many diseases including coronary
heart disease, stroke, hypertension, diabetes, obesity, and certain gastrointestinal disorders as
well as improving metabolic parameters and immune functions [30]. The definition, method of
measuring fiber and recommendations varies in different countries. The backbone of our food
composition data is based on Food Composition Databases USDA. According to US guidelines,
the current recommendation is to consume 14 g fiber per every 1000 kcal, therefore using the
energy guideline of 2000 kcal/day for women and 2600 kcal/day for men, the recommended
daily dietary fiber intake is 28 g/day for adult women and 36 g/day for adult men [31]. Although
Sri Lankan adults consume fewer calories compared to US adults, their dietary fiber intake is
insufficient according to their calorie intake.
Epidemiological, clinical and animal experimental evidence showed a direct relationship
between dietary electrolyte consumption and blood pressure [32]. Furthermore, clinical trials
show that a reduction in salt (NaCl) intake reduces BP levels in normotensive and hypertensive
populations and prevents the development of hypertension [32]. Recommended Na intake is a
maximum of 2.3 g/day [32]. Our findings showed that most Sri Lankan adults exceed current
recommendations. The high consumption of sodium may be associated with the epidemic of
hypertension (Men: 18.8%; Women: 19.3%) among Sri Lankan adults [33].
Chapter 6: Manuscript 5 129
This study has several limitations. Sri Lanka has over 20 million inhabitants. Therefore, diet
records of a sample of 463 subjects may not represent the eating patterns of the whole
population. However, a well-conducted UK NDNS [20] measured the dietary records of 1724
respondents and achieved a lower response rate of 47%. Considering available resources, the
high response rate and satisfactory representation of demographic parameters, we believe this is
a practical sample size. Secondly, 24 HDR may not be the best tool to determine habitual diet,
however, random 24 HDR in a large sample has been used in other national surveys [7]. Thirdly,
our findings were limited to energy and selected major macronutrients due to sub-quality
nutritional information on sub-categories of macronutrients and micronutrients of Sri Lankan
mixed dishes (Table 6.8). Another limitation is that despite reports of high alcohol consumption
among Sri Lankan men [34], alcohol intake was under-reported in our study (<0.5%). In this
survey, low energy reporters (<800 kcal/day) were excluded, therefore exclusion will have
biased the data towards higher intakes. Lastly, we did not attempt to correlate energy intake and
its adequacy to this population as calorie recommendations may vary with several factors such as
gender, age, body weight, body composition and physical activity level.
Acknowledging the limitations of the survey, the present study provides the first national
estimates of energy and nutrient intake of the Sri Lankan adult population. It is evident that
consumption of high levels of carbohydrate, fat mainly from saturated sources, low protein, low
dietary fiber and high levels of sodium may have detrimental effects on health and be related to
the current epidemic of NCDs. Unfortunately, current food-based dietary guidelines are based on
limited research [25]. Therefore, well-designed and nationally representative studies are needed
to explore the association between diet and chronic disease among Sri Lankan adults. Moreover,
regular diet and nutrition surveys should be carried out to obtain information on dietary patterns
130 Chapter 6: Manuscript 5
and nutrient intakes and, ideally, periodical monitoring is needed to identify the changing trends
in food intake and to assess public responses to dietary recommendations.
Chapter 6: Manuscript 5 131
REFERENCE LIST
1. Popkin B.M. HS, Kim S.,: The Nutritional Transition and Diet-Related Chronic Diseases in Asia: Implications for Prevention. Washington, DC: International Food Policy Research Institute FCND Discussion Paper 2001, 105.
2. Jayasekara R, Schultz T: Health status, trends, and issues in Sri Lanka. Nursing & Health Sciences 2007, 9:228-233.
3. Katulanda P, Ranasinghe P, Jayawardena R, Sheriff R, Matthews D: Metabolic syndrome among Sri Lankan adults: prevalence, patterns and correlates. Diabetology & Metabolic Syndrome 2012, 4:24.
4. Katulanda P, Constantine GR, Mahesh JG, Sheriff R, Seneviratne RD, Wijeratne S, Wijesuriya M, McCarthy MI, Adler AI, Matthews DR: Prevalence and projections of diabetes and pre-diabetes in adults in Sri Lanka--Sri Lanka Diabetes, Cardiovascular Study (SLDCS). Diabet Med 2008, 25:1062-1069.
5. Premaratne R, Amarasinghe A, Wickremasinghe AR: Hospitalisation trends due to selected non-communicable diseases in Sri Lanka, 2005-2010. Ceylon Med J 2005, 50:51-54.
6. Walter Willett EL: Nutritional epidemiology. In Monographs in Epidemiology and Biostatistics. Edited by Willett W: Oxford University Press; 1998: 101-147
7. University of Otago and Ministry of Health: A Focus on Nutrition: Key findings of the 2008/09 New Zealand Adult Nutrition Survey. In Book A Focus on Nutrition: Key findings of the 2008/09 New Zealand Adult Nutrition Survey. (Editor ed.^eds.). City: Ministry of Health; 2011.
8. Giskes K, Turrell G, Patterson C, Newman B: Socio-economic differences in fruit and vegetable consumption among Australian adolescents and adults. Public Health Nutr 2002, 5:663-669.
9. Sasaki S: The value of the National Health and Nutrition Survey in Japan. Lancet 2011, 378:1205-1206.
10. Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Hills AP: Consumption of Sri Lankan adults: an appraisal of serving characteristics Public Health Nutrition 2012, FirstView Article : pp 1-6.
11. Statistical Abstract [http://www.statistics.gov.lk/abstract2010/Pages/index.htm] 12. WHO expert consultation: Appropriate body-mass index for Asian populations and
its implications for policy and intervention strategies. The Lancet 2004, 363:157-163. 13. USDA: Foods List. In Book Foods List (Editor ed.^eds.), 24 edition. City; 2012. 14. Perera W.D.A. JPM, Thaha S.Z., : Tables of food composition for use in Sri Lanka. 1979. 15. Gopalan C. RBV, Balasubramanian S.C.,: Nutritive value of Indian foods. Hyderabad;
1989. 16. Dissanayake C: Ceylon Cookery. 9 edn. Sri Lanka: Stamford Lake (pvt) Ltd; 2010. 17. Azadbakht L, Mirmiran P, Esmaillzadeh A, Azizi F: Dietary diversity score and
cardiovascular risk factors in Tehranian adults. Public Health Nutrition 2006, 9:728-736.
18. Caster WO: Systematic estimation of food intakes from food frequency data. Nutrition Research 1986, 6:469-472.
19. Mirnalini K ZM, Safiah MY, Tahir A, Siti Haslinda MD, Siti Rohana D, Khairul Zarina MY, Mohd Hasyami S & Normah H,: Energy and Nutrient Intakes: Findings from the Malaysian Adult Nutrition Survey (MANS). Mal J Nutr 2008, 14:1-24.
20. Swan G: Findings from the latest National Diet and Nutrition Survey. Proc Nutr Soc 2004, 63:505-512.
21. Chee SS ZH, Ismail MN, and Ng KK,: Anthropometry, dietary patterns and nutrient intakes of Malaysian estate workers. Mal J Nutr 1996, 2:112-126.
22. Rennie KL, Jebb SA: Prevalence of obesity in Great Britain. Obes Rev 2005, 6:11-12. 23. Heitmann BL, Lissner L: Dietary underreporting by obese individuals--is it specific
or non-specific? BMJ 1995, 311:986-989. 24. Smit E, Nieto FJ, Crespo CJ, Mitchell P: Estimates of animal and plant protein intake
in US adults: results from the Third National Health and Nutrition Examination Survey, 1988-1991. J Am Diet Assoc 1999, 99:813-820.
25. Samaranayake U.M.M. et al.: Food Base Dietary Guidelines for Sri Lanka. Colombo: Nutrition Devision, Ministry of Healthcare and Nutrition, Sri Lanka; 2011.
26. Kennedy ET, Bowman SA, Powell R: Dietary-fat intake in the US population. J Am Coll Nutr 1999, 18:207-212.
27. Amarasiri W: Coconut fats. Ceylon Med J 2009, 51. 28. Report of a Joint WHO/FAO Expert Consultation: Diet, Nutrition and the prevention
of Chronic Diseases. In Book Diet, Nutrition and the prevention of Chronic Diseases (Editor ed.^eds.). City; 2003.
29. Misra A, Khurana L, Isharwal S, Bhardwaj S: South Asian diets and insulin resistance. Br J Nutr 2009, 101:465-473.
30. Anderson JW, Baird P, Davis RH, Jr., Ferreri S, Knudtson M, Koraym A, Waters V, Williams CL: Health benefits of dietary fiber. Nutr Rev 2009, 67:188-205.
31. USDA: The Food Supply and Dietary Fiber: Its Availability and Effect on Health. In Book The Food Supply and Dietary Fiber: Its Availability and Effect on Health (Editor ed.^eds.), vol. 36. City: U.S. Department of Agriculture; 2007.
32. Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D, Obarzanek E, Conlin PR, Miller ER, 3rd, Simons-Morton DG, et al: Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med 2001, 344:3-10.
33. Wijewardene K, Mohideen MR, Mendis S, Fernando DS, Kulathilaka T, Weerasekara D, Uluwitta P: Prevalence of hypertension, diabetes and obesity: baseline findings of a population based survey in four provinces in Sri Lanka. The Ceylon medical journal 2005, 50:62-70.
34. Rahav G, Wilsnack R, Bloomfield K, Gmel G, Kuntsche S: The influence of societal level factors on men's and women's alcohol consumption and alcohol problems. Alcohol and alcoholism (Oxford, Oxfordshire) Supplement 2006, 41:i47-55.
.
Chapter 6: Manuscript 5 133
Table 6-1: Socio-demographic characteristics of the survey population
Characteristics Total (n = 463) Men (n = 166) Women (n = 297) n % n % n %
Area of Residence Urban Rural Estate
153 276 34
33.04 59.61 7.34
45 102 19
26.51 61.45 11.45
108 174 15
36.36 58.58 5.05
Age group (yrs) 18-29 30-39 40-49 50-59 >60
61 84 117 106 95
13.17 18.14 25.27 22.89 20.52
27 23 38 40 38
16.26 13.85 22.89 20.10 22.89
34 61 79 66 57
12.73 22.85 29.59 24.72 21.35
Ethnicity Sinhala Muslim Sri Lankan Tamil Indian Tamil
360 27 42 34
77.75 5.83 9.07 7.34
118 8 20 20
71.08 4.82 12.05 12.05
242 19 22 14
8.15 6.40 7.41 4.71
Educational Level No Schooling Up to 5 years Up to O/L Up to A/L Graduate
27 113 182 116 25
58.31 24.41 39.31 25.05 5.39
11 43 59 46 07
6.62 25.90 35.54 27.71 4.22
16 70 123 70 18
5.39 23.57 41.41 23.57 6.06
BMI Category < 18.5 kg.m-2
> 18.5 - < 22.9 kg.m-2 > 23 - < 24.99 kg.m-2
> 25 - < 27.5 kg.m-2 > 27.5 kg.m-2
64 163 76 95 65
13.82 35.21 16.41 20.52 14.04
29 75 21 32 09
17.47 45.18 12.65 19.28 5.42
35 88 55 63 56
11.78 29.63 18.52 21.12 18.86
134 Chapter 6: Manuscript 5
Table 6-2: Energy intake (kcal) of Sri Lankan adults by socio-demographic characteristics
Chapter 6: Manuscript 5 135
Table 6-3 Carbohydrate intake (g) of Sri Lankan adults by socio-demographic characteristics
136 Chapter 6: Manuscript 5
Table 6-4 Protein intake (g) of Sri Lankan adults by socio-demographic characteristics
Chapter 6: Manuscript 5 137
Table 6-5 Fat intake (g) of Sri Lankan adults by socio-demographic characteristics
138 Chapter 6: Manuscript 5
Table 6-6 Dietary fiber intake (g) of Sri Lankan adults by socio demographic characteristics.
Chapter 6: Manuscript 5 139
Table 6-7 Sodium intake (mg) of Sri Lankan adults by socio-demographic characteristics
140 Chapter 6: Manuscript 5
Table 6-8: Mean Daily Micronutrient Intake by Sri Lankan Adults.
Figure 6.2 Percentage energy contribution from macronutrients according to gender, ethnicity and area of residance,BMI,educational level and age groups
.
Chapter 7: Manuscript 6 and 7 142
Chapter 7: Manuscript 6 and 7
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: The obesity epidemic in Sri Lanka revisited Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
Chapter 7: Manuscript 6 and 7 143
CHAPTER 7A: MANUSCRIPT 6
Letter to the editor
The obesity epidemic in Sri Lanka revisited.
Ranil Jayawardena MBBS, MSc1,2, Nuala M. Byrne MSc PhD1, Mario J. Soares MBBS
MSc PhD3, Prasad Katulanda MD DPhil2, Andrew P. Hills MSc PhD4
1Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of
Technology, Brisbane, Queensland, Australia.
2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka.
3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health
among Sri Lankan adults: prevalence, patterns and correlates. Diabetology & Metabolic
Syndrome. 2012;4(1):24.
Chapter 7: Manuscript 6 and 7 147
CHAPTER 7B: MANUSCRIPT 7
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: The obesity epidemic in Sri Lanka revisited and High dietary diversity is associated with obesity in Sri Lankan adults: an evaluation of three dietary scores Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Bijesh Yadav statistical analysis Andrew Hills Study design, data interpretation and revision
of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
148 Chapter 7: Manuscript 6 and 7
TITLE PAGE
High dietary diversity is associated with obesity in Sri Lankan adults: an
evaluation of three dietary scores
Ranil Jayawardena1,2*, Nuala M. Byrne1, Mario J. Soares3, Prasad Katulanda2, Bijesh Yadav4,
Andrew P. Hills5
1Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of
Technology, Brisbane, Queensland, Australia.
2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka.
3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Body weight perception and weight loss practices among Sri Lankan adults Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
168 Chapter 8: Manuscript 8
TITLE PAGE
Body weight perception and weight loss practices among Sri Lankan adults
Ranil Jayawardena 1,2*, Nuala M. Byrne 1, Mario J. Soares 3, Prasad Katulanda 2, Andrew P.
Hills 4
1Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of
Technology, Brisbane, Queensland, Australia.
2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka.
3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Validation of a Food Frequency Questionnaire to assess nutritional intake among
Sri Lankan adults.
Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
Chapter 9: Manuscript 9 189
TITLE PAGE
Ranil Jayawardena1,2*, Nuala M. Byrne1, Mario J. Soares3, Prasad Katulanda2, Andrew P. Hills4
1Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of
Technology, Brisbane, Queensland, Australia.
2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka.
3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health
Figure 9-1: Bland and Altman plots for energy with the mean difference and limits of
agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95% limits of agreements in red line.
807060504030
50
40
30
20
10
0
-10
-20
-30
Averages
Diff
eren
ces
LLA = -24.95
ULA = 32.06
Mean = 3.55
Bland-Altman Plot
Figure 9-2: Bland and Altman plots for protein with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95%
limits of agreements in red line.
Chapter 9: Manuscript 9 205
706050403020
30
20
10
0
-10
-20
-30
-40
-50
Averages
Diff
eren
ces
LLA = -35.34
ULA = 22.42
Mean = -6.46
Bland-Altman Plot
Figure 9-3: Bland and Altman plots for fat with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95% limits of
agreements in red line.
450400350300250200150
200
100
0
-100
-200
Averages
Diff
eren
ces
LLA = -180.09
ULA = 98.25
Mean = -40.92
Bland-Altman Plot
Figure 9-4: Bland and Altman plots for carbohydrates with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95%
limits of agreements in red line.
206 Chapter 10: General discussion
Chapter 10: General discussion
Chapters two to nine have incorporated separate discussion sections in which a specific
commentary of respective research findings in relation to the local, regional and global literature
have been provided. Further, each chapter has provided an interpretation of factors that may
have contributed to the research findings, the strengths and limitations of each study, and the
implications of the results for health promotion, education and further research. This final
chapter provides an overall discussion of the findings of the three major studies and the nine
manuscripts which collectively address the applicability of different nutritional assessment tools
and nutritional issues in South Asia in relation to current diabetic epidemic. The significance of
the research is discussed in light of its contribution to the current body of knowledge. Moreover,
this chapter discusses the strengths and limitations of the project as a whole. Finally, an overall
conclusion is provided along with a discussion of the application of findings for both clinical and
public health settings, and recommendations for future research.
Chapter 10: General discussion 207
COMPARISON OF DIFFERENT DIETARY ASSESSMENT TOOLS
Many different methods have been developed for the purpose of assessing dietary intake (1).
These range from detailed individual weighed records collected over a certain time period to
food frequency questionnaires, dietary recalls, household survey methods and dietary histories.
The most appropriate dietary assessment tool will depend on the purpose for which it is needed
e.g. to measure nutrients, foods or eating habits and diet-related health risks. It is important to
understand that each method has merits, associated errors and practical difficulties to be
considered when making a choice (2). While the 7-day weighed record is widely considered as
the reference method (3) for large epidemiological surveys, the FFQ is a more appropriate
method (1).
Dietary records
The respondent records the identity and amounts of all foods and beverages at the time of
consumption for a period of time (usually 1-7 days). Food and beverages are quantified by
estimating portion sizes using household measurements, or weighing the food or beverage on
scales. There are two types of food records 1) estimated food records and 2) weighed food
records (2).
For the estimated food record approach, the respondent records the foods and beverages and the
amounts of each consumed over one or more days. The amounts consumed may be measured,
using a scale or household measure (such as cups, tablespoons), or estimated, using models,
pictures, or no particular aid (2). Typically, if multiple days are recorded, they are consecutive
and no more than 3 or 4 days are included. Recording periods of more than 4 consecutive days
are usually unsatisfactory, as reported intakes decrease because of respondent fatigue (4).
The weighed record involves an individual or an investigator weighing every item of food and
drink prior to consumption. A detailed description of the food and its weight is recorded in a
specially designed booklet. Usually a space is left to record any leftovers so that the precise
weight of food eaten can be calculated. The 7-day weighed record has often been referred to as
the ‘gold standard’ against which less detailed and demanding methods can be compared (3). In
208 Chapter 10: General discussion
this thesis, a 7-day weighed record was used to validate the newly developed food frequency
questionnaire. However for collecting the food list, a 24-hour dietary recall was administrated.
24-hour dietary recall
For the 24-hour dietary recall, the respondent is asked to remember and report all the foods and
beverages consumed in the preceding 24 hours or in the preceding day. The recall is typically
conducted by interview, in person or by telephone - either computer-assisted or using a paper-
and-pencil form (5). Well-trained interviewers are crucial to administer a 24-hour recall as much
of the information is collected by asking probe questions. Ideally, the interviewer should be a
nutritionist; however, non-nutritionists who have been trained in the use of a standardized
instrument can also be effective. All interviewers should be knowledgeable about foods
available in the marketplace and about preparation practices, including prevalent regional and
ethnic foods or need to perform face validity (1). The interview is often structured, usually with
specific probes to help the respondent remember all foods consumed throughout the day.
Probing is especially useful in collecting necessary details, such as how foods were prepared. It
is also useful in recovering many items not originally reported, such as common additions to
foods (e.g., curry on rice) and eating occasions not originally reported (e.g., snacks and beverage
breaks). This is particularly important for elderly groups (2). However, interviewers should be
provided with standardized neutral probing questions so as to avoid leading the respondent to
specific answers when the respondent really does not know or remember (1).
Dietary history
Particularly in clinical settings a dietary history is used to assess eating habits and nutrition
levels. A dietary history is a structured interview method consisting of questions about habitual
intake of foods from the core (e.g., meat and alternatives, cereals, fruit and vegetables, dairy and
‘extras’) food groups in the last seven days (1). This is followed by a ‘cross check’ to clarify
information about usual intake in the past 3, 6, or 12 months, depending on the aims of the
assessment. This can be used as an alternative to the 24-hour dietary history or food recall. Usual
portion sizes are generally obtained in household measures and/or with the use of photographic
aids (5).
Chapter 10: General discussion 209
Food Frequency Questionnaire (FFQ)
The FFQ is one of the most commonly used methods in epidemiological studies to assess
individual long-term dietary intake of foods and nutrients (2). The questionnaires are typically
self-administered, asking the respondents to report the usual frequency of consumption of items
from a list of foods for a specified time period. The method is sufficiently simple to be used in
large epidemiological studies. Even though the absolute intake is an estimate, using this method
can rank individuals by levels of past nutrient intake in epidemiological studies (1). The
questionnaire is able to rank the population into levels of exposure which are used in the
calculation of relative risk for the development of the disease in question. Therefore, the FFQ is
the most suitable method for measuring dietary factors for nutrition-related NCDs in a large
survey. Moreover, the FFQ can be used to represent different ethnic groups as well as to
discriminate between people’s intake for nutrients known to be associated with the nutritional
related disease (6). For example, Liu et al. found a FFQ was able to assess dietary glycaemic
load in relation to metabolic risk factors (7).
At its simplest, the FFQ consists of a list of foods and a selection of options relating to the
frequency of consumption of each of the foods listed (e.g., times per day, daily, weekly,
monthly)(1). FFQs are designed to collect dietary information from large numbers of individuals
and are normally self-administered, though interviewer-administered and telephone interview are
possible modifications. Levels of education and facilities will determine the mode of
administration. For example, interviewer-administrated methods have been used in India where a
considerable proportion of the population is illiterate whereas in developed countries, an
internet-based FFQ is widely used (8). FFQs normally ask about intake within a given time
frame (e.g., in the past 1-2 months or 1 year) and therefore aim to capture habitual intake. The
length of the food list can vary depending on the nutrients or foods of interest. The number of
food items varies from few to several hundred (1). Many FFQs also attempt to collect
information about portion size in addition to frequency of consumption (9). These may be
referred to as semi-quantitative FFQs. Although there are difficulties implicit in calculating the
absolute nutrient intake of individuals from food frequency questionnaires, they are useful for
gathering information on groups of individuals as well as for looking at habitual intake of a
range of foods.
210 Chapter 10: General discussion
The appropriateness of the food list is crucial in the food frequency method (10). The full
variability of an individual’s diet, which includes many foods, brands, and preparation practices,
cannot be fully captured with a finite food list. Obtaining accurate reports for foods eaten both as
single items and in mixtures is particularly problematic especially in Asian countries where
many mixed dishes and curries eaten. FFQs can ask the respondent to report either a combined
frequency for a particular food eaten both alone and in mixtures or separate frequencies for each
food used. All FFQs must be associated with a food database to allow for the estimation of
nutrient intakes for an assumed or reported portion size of each food queried (8).
In pursuit of improving the validity of the FFQ, investigators have addressed a variety of
frequency questionnaire design issues such as length, closed versus open-ended response
categories, portion size, seasonality, and time frame (1,10). Frequency instruments designed to
assess total diet generally list more than 100 individual line items, many with additional portion
size questions, requiring 30 to 60 minutes to complete. This raises concern about length and its
effect on response rates.
Accuracy of nutrient estimates
Accuracy of energy and nutrient is extremely important in any nutrition survey. The accuracy of
nutrient estimates depends on two factors: the accuracy of dietary information provided by the
participants and the accuracy of the food composition data. Key considerations related to these
two potential sources of error are outlined below.
Any technique used to measure food intake should not interfere with the subject's dietary habits
as this may alter the parameter being measured. Both under-reporting and over-reporting of food
intake are well-known problems in all types of dietary surveys, regardless of the dietary
assessment method used. If food intake is under-reported, energy and nutrient intakes may also
be underestimated, and estimates of inadequate intake may be overestimated. It is difficult to
quantify under-reporting, but research shows that the degree of under-reporting varies according
to personal characteristics and across types of foods (11,12). For example, under-reporting is
more common in those with a high BMI, and in females. Certain foods are more likely to be
under-reported, especially those perceived as less healthy (e.g., cakes, biscuits, desserts, fats).
On the other hand, over-reporting of fruit and vegetable intake can be seen amongst more
educated groups (11). Moreover, it is widely observed that culturally preferred foods tend to be
over-reported and vice versa (13). Apart from the type of foods, an accurate detail of the amount
of food is equally important. In all dietary assessment methods where food is not weighed,
Chapter 10: General discussion 211
portion sizes must be determined before nutrient output can be calculated. There are a number of
methods by which portion sizes may be obtained. These may include field workers weighing
certain food items on the individual’s behalf, the use of photographic atlases (14, 15) showing
portion sizes of commonly eaten foods to an individual, using data from manufacturers, portion
sizes collected from previous weighed food records, and household measures.
Unlike most developed countries, there is no centrally managed nutrient database in Sri Lanka.
We therefore compiled information from the food composition tables of Sri Lanka (16), the
United States Department of Agriculture nutrient database (USDA) (17), the Indian Food
Composition Tables (18), and McCance and Widdowson’s food composition tables (19) to
develop a comprehensive and new nutrient composition database as follows. a) Nutrition values
for single food items were taken mainly from the USDA nutrient database; b) Nutrition
information leaflets or details from direct contact with producers were used for locally available
food products (e.g., biscuits); c) For mixed dishes and cooked foods, local recipes were taken
from popular cookery books (20), and by interviewing participants. All recipes were accepted
after checking for face validity by consulting local housewives and nutritionists. According to
the recipes, ingredients were weighed to the nearest 1 g for edible portions of the foods, and the
food items were cooked and weighed. Nutritional composition of the final recipe was calculated
by entering nutritional values and weights of individual ingredients into a spreadsheet. The sum
of each nutrient was computed and standardized to 100 g of the final product. Data on weight
loss associated with cooking (e.g., due to water evaporation) was recorded to ensure accurate
nutrient density of the portion size consumed. However, nutrient losses (e.g., vitamins) during
food preparation were not considered. However in ideal circumstances, all food items should be
chemically analysis for their nutrient ingredients.
212 Chapter 10: General discussion
NUTRITIONAL ISSUES IN SOUTH ASIA IN RELATION TO THE CURRENT DIABETES EPIDEMIC
Diet is an important factor in preventing diabetes, managing existing diabetes, and preventing, or
delaying the development of its complications (21). Eating habits are one of the main
determinants of diabetes among South Asians. Although the published data on dietary habits and
development of diabetes in this region is limited, it is believed that dietary habits play an
important role in the epidemic of diabetes among South Asians.
Carbohydrates
Compared to Europeans, the diet of South Asians is predominantly based on starchy foods (22).
Similarly, Indian vegetarians have a higher percentage of carbohydrates in their diet when
compared to American vegetarians and non-vegetarians (23). Our data shows a majority of Sri
Lankan adults consume starchy foods above the upper limit of recommendations (24). Elevated
2-h insulin concentrations have been shown to be positively associated with the proportion of
energy intake from carbohydrate (22). Others have shown that compared with a low-
carbohydrate diet (35% of total energy from carbohydrates), an iso-caloric high-carbohydrate
diet (60% of total energy from carbohydrates) caused a 27.5% increase in plasma triglycerides, a
similar increase in VLDL-cholesterol levels, and an 11% reduction in HDL cholesterol levels
(25). A typical South Asian diet consists of over 60% of carbohydrates which may lead to
undesirable glycaemic and lipid changes. The quality of carbohydrates is also an important
factor in diabetes and a diet with high glycaemic index foods has been shown to increase
postprandial plasma glucose levels in subjects with impaired glucose tolerance (26). Mohan et
al. argued that increased consumption of refined cereals may be more detrimental than the
amount of carbohydrates among Indians (27). Higher intake of white rice was associated with an
increased risk of type 2 diabetes (28). Added sugar consumption is also high in India (29). Sri
Lankans consume over 3.5 portions of sugar day (24) and as sugary foods and refined starch
digest rapidly and are converted to glucose, this increases insulin demand and may lead to
pancreatic b-cell exhaustion in the long run (30).
Dietary fats
In a 14-year follow-up of 84,204 non-diabetic women, total fat and SFA and MUFA intake were
not associated with risk of type 2 diabetes (31). Similarly, another large prospective study on
Chapter 10: General discussion 213
men (n=42,504) found total fat and SFA were not associated with type 2 diabetes incidence
when adjusted for BMI (32). According to the National Sample Survey Organization (2004-
2005), the consumption of fat among Indians was 44 g/d in rural areas and 58.2 g/d in urban
areas (33). In the studies conducted in this thesis, we found that fat intake among men and
women in Sri Lanka was 40.5 g/d and 31.9 g/d, respectively (34). Most South Asians are getting
less than 20% of total calories from fat. According to the ranges of population nutrient intake
goals recommended by WHO, the percentage of energy from total carbohydrates, fats and
proteins should be 55-75%, 15-30% and 10-15%, respectively (35). Total fat consumption as an
energy source is under the safe limits among South Asians. However, type of fats may be
significant in this population. India and other South Asian countries often use ghee for cooking
which contains high TFA (36) whereas Sri Lankans and South Indians often consume coconut
products which contain SFA (37). Full cream milk and dairy products also provide SFA and
cholesterols. Although there is no evidence to suggest fat consumption and diabetes are
associated among South Asians, unhealthy fat consumption might increase the complications of
diabetes, especially cardiovascular complications. Ghee and dairy products also provide SFA
and cholesterols. On the other hand, MUFA and PUFA consumption is low among this
population (38).
Dietary fiber
Large prospective studies support a protective role of dietary fiber for the development of
diabetes (39, 40). A randomized, cross-over study showed that a high fiber diet (total, 50 g; 25 g
of soluble fiber and 25 g of insoluble fiber) compared to the recommended amount (total, 24 g; 8
g of soluble fiber and 16 g of insoluble fiber), significantly improved glycaemic control,
decreased hyperinsulinaemia, and lowered plasma lipid concentrations in patients with type 2
diabetes (41). These benefits most likely occur by slowing the digestion and absorption of food
and by regulating several metabolic hormones (40). Limited available data showed that daily
intake of dietary fiber is low among South Asians (34, 38).
Vitamin and minerals
Zinc is an important structural and functional molecule for insulin. Zinc supplementation in
patients with diabetes demonstrates that zinc supplementation has beneficial effects on
glycaemic control and promotes healthy lipid parameters (42). A meta-analysis of randomized
double-blind controlled trials regarding the effect of magnesium supplementation on glycaemic
control in type 2 DM showed significant reduction of fasting glucose level in the treatment
214 Chapter 10: General discussion
group (43). Mean daily intake of manganese and zinc is lower in Indian vegetarians (23). A
systematic review and meta-analysis of observational studies and clinical trials in adults with
outcomes related to glucose homeostasis showed vitamin D and calcium insufficiency may
negatively influence glycaemia (44). Several studies reported a high prevalence of
hypovitaminosis D and low dietary calcium level among Indians (45, 46). Our data showed low
calcium and vitamin D intakes among Sri Lanka adults. Indians consumed high amounts of salt,
Indian (Ladakh) men showed >200 mmol/day sodium excretion (47). In a Finnish prospective
study, the hazard ratio for diabetes for the highest (>200 mmol/24 h) versus combined lower
quartiles of 24-h urinary sodium excretion was 2.05 (95% CI, 1.43-2.96) after adjusting several
known risk factors. In contrast, potassium may have a protective effect against diabetes (48).
Fruit and vegetables are good sources of potassium.
Fruit and vegetables
Fruit and vegetables contain several nutrients, which may have a number of health benefits. The
effect is beyond the cumulative effects of individual nutrients such as dietary fiber, vitamins and
antioxidants. Although fruit and vegetables are not nutrients, we elaborate separately. Fruit and
vegetable intake is inversely associated with diabetes incidence (49). The EPIC-Norfolk Study
reported that subjects with unknown diabetes that consumed higher intakes of fruits and
vegetables had significantly lower levels of HbA1c (50). In a multivariate analysis, a significant
inverse trend was observed between fruit intake and the probability of having the glycaemic
component (plasma glucose ≥110 mg/dl) of metabolic syndrome features (51). Fruit and
vegetables reduce diabetes-associated complications, especially heart disease and stroke (52).
Fruit and vegetables are widely available in the South Asian countries but consumption is very
low. Average fruit consumption of four cities from Bangladesh was 1.7 servings/day and 1.6
servings/day among men and women, respectively. Corresponding values for vegetable
consumption were 3.4 and 3.0, for men and women (53). Fruit and vegetable intake among
Indian men and women were 1.2 servings/day for fruit and 1.3 servings/day for vegetables.
According to the World Health Survey 2002-2003, Pakistan and Nepal have the highest
prevalence of low fruit and vegetable consumption among 52 countries. Less than 1% of
Pakistani and less than 2% of Nepalese consume a minimum of five fruits and vegetables daily
(54). In Sri Lanka, we found that mean dietary intake of fruit and vegetables was 2.16
portions/day and only 3.5% of adults consumed according to the recommendations (24).
Similarly, only 2.7% of Maldives adults had five or more portions of fruits and vegetables daily
Chapter 10: General discussion 215
(55). The vegetable consumption pattern is very unique among South Asians. Although there is a
considerable variation among different ethnic groups, most of the vegetables are consumed in
the form of a curry, with cooking oils, curd, coconut milk and dairy fats. Moreover, adding
strong spices prevents consumption of vegetables in a large quantity. The cooking methods used
are boiling, steaming, grilling, baking and roasting as opposed to the South Asian countries
where frying is mostly the preferred method.
Occurrence and progression of diabetes and other metabolic diseases are associated with dietary
habits however assessment of dietary factors for chronic diseases is inherently difficult due to
several confounding factors. There is limited published data available on nutrient composition
and dietary habits of native South Asians. Lifestyle factors of immigrant South Asians could also
be different to their native counterparts. Furthermore, dietary habits are considerably
heterogeneous among ethnic groups. Culturally specific and sensitive dietary interventions are
required to identify nutritional risk factors for diabetes among South Asians.
216 Chapter 10: General discussion
STRENGTHS OF THE STUDY
There are several strengths of this research work including the sampling, data collection and
reporting methods. Firstly, studies were based on a sub-sample of the Sri Lanka Diabetes and
Cardiovascular Study (SLDCS). The SLDCS included a nationally representative sample of
5000 adults aged ≥18 years selected using a multi-stage random cluster sampling technique. The
response rate for the first study was over 80% and for the validation study approached 70%.
Having a representative sample is a key strength for any population-based study.
Secondly, although data collection was undertaken in different community settings, all
anthropometric data were collected using standardised equipment and techniques. Similarly, as
discussed in Chapter 2, robust data collection techniques were applied to collect the 24-hour
recall data. The seven-day weighed intake (7DWI) is considered the “gold standard” method to
retrieve dietary data. A satisfactory validation against 7DWI demonstrated the appropriateness of
the FFQ for this population.
Finally, it is extremely difficult to categorize mixed dishes to food groups therefore complex
dishes were disaggregated before ingredients were categorized into appropriate food groups.
This scientifically sound method helped to categorize dishes into the main food groups.
Moreover, defining portion sizes for many local fruit and vegetable, protein and starch items is
based on sound nutrition concepts.
LIMITATIONS OF THE STUDY
Due to the scope and various constraints such as time and funding associated with the
completion of the PhD project within a three-year period, several limitations of this research
Chapter 10: General discussion 217
project must be acknowledged. These relate to sampling, selection and confounding bias, and
limitations of some of the measurement tools used.
The accuracy of cross-sectional studies is based on the selection of a representative sample.
However, participation rate is a significant factor to assess the quality of the sampling. Study 1
had an 82% response rate but male participation was considerably lower. Moreover,
participation of young adults was limited. Although data collection was undertaken with prior
notice, few men and young working people participated due to other commitments. Having a
large proportion of over 40 year-old adults may limit the interpretation for young adults with
diverse eating patterns. Similarly, Study 2 was dominated by middle-aged women. Weighing
their own food was also not practical for many busy individuals.
Sri Lanka is a multi-cultural country with four sub-ethnic groups, namely Sinhalese, Indian
Tamil, Sri Lankan Tamils and Muslims. Each sub-ethnic group has different dietary and
behaviour patterns. Due to the small sample size, the representation of dietary intakes of
minority ethnic groups may not be adequate. The lower number of subjects in minority groups
may have affected an accurate determination of the prevalence of obesity. For example, there
was a high non-response rate from Sri Lankan Tamils in the previously war-affected areas.
Another shortcoming of this study was the limited accuracy of the nutrient values of some of the
food items. Due to highly diverse food items, many local food items were not available in any of
the food composition databases. Furthermore, there is a significant difference in the list of
ingredients in the ‘same’ dishes due to differences in cultural background. Therefore, due to the
absence of accurate nutritional composition of the food items, energy and nutrient values of
similar food items were used.
218 Chapter 10: General discussion
Obesity perception is very subjective. Measurement of obesity using an objective scale is not the
ideal. Self-perception of body weight is associated with additional parameters such as perception
of body shape and associated health risk. Qualitative details of misperception of body weight
would provide a more complete picture and help to better understand misperception of body
weight among this population. Lack of qualitative data with regards to obesity perception may
therefore be a limitation of the studies presented in this thesis.
RECOMMENDATIONS
Recommendations for future research
It is evident that Sri Lanka has a serious diet-related non-communicable diseases burden. A lack
of local data on eating habits and nutrient intake are evident. Our findings showed high intakes
of starchy foods and low fruit and vegetable intake. However, we collected only quantitative
data therefore we do not know the reasons for these less healthy eating habits which may be
associated with several cultural, economic and behavioural factors. Therefore, qualitative studies
among a representative group of adults would be essential to determine the underlying reasons
and causes at the grass root level. Similarly, qualitative data are necessary for a better
understanding of the misperception of body weight among many Sri Lankan adults.
Analytical research is important to obtain accurate nutrient values of local fruits, vegetables,
green leaves and locally made sweets. These foods play an important role in the Sri Lankan diet
but a lack of nutrition composition data hinders the provision of culturally acceptable nutritional
advice. In particular, research on micronutrients such as vitamin, mineral and anti-oxidant levels
is essential. Moreover, as Sri Lankans often consume foods which are cooked under extreme
heat and for a long time, it is hard to predict the nutrient composition of the end meal. Food
science research is therefore important to accurately document nutrient values of Sri Lankan
meals.
Chapter 10: General discussion 219
Children’s dietary patterns are equally important in the prevention of diet-related NCDs.
However, currently there is no country-specific FFQ for children. Dietary habits and portion
sizes in children are very different to adults. In particular, take-away foods are the main choices
in schools. Adolescents also have distinctive eating habits during a life transition period that can
be both physically and mentally taxing. Further research is therefore important to document the
food habits of children and adolescents and associated health risks in Sri Lanka.
Recommendations for public health and clinical initiatives and interventions
Translation of theory to practice is essential in health-related studies. This thesis is the first
nutritional survey undertaken in Sri Lanka and reports several unhealthy eating habits among
adults. However, cross-sectional studies are not adequate to establish the causative relationship
between dietary habits and high NCD levels. With the current findings, it is possible to start
public health intervention studies to encourage the reduction of high starchy food consumption
and increase intake of fruit and vegetables. Furthermore, dairy consumption of Sri Lankans is
also extremely low which may be due to the unavailability of fresh milk. Government policies
should give higher priority to increased milk and dairy food production and consumption.
The number of people suffering from obesity and diabetes has reached epidemic levels.
However, dietary changes and weight reduction are challenging for clinicians. Our data showed
an association between dietary habits and obesity level among Sri Lankan adults. A significant
amount of nutrition knowledge is important to provide a balanced diet with limited food items.
One of the main objectives of this thesis was to develop and validate a country-specific FFQ for
Sri Lankan adults. Researchers and government bodies should utilize this FFQ for the next
national health survey and other dietary intervention studies. The Sri Lankan government should
provide the technical support to improve the practicality of this FFQ for large-scale studies.
220 Chapter 10: General discussion
Firstly, optical scanning facilities are needed to obtain selected food items and secondly,
software development for the analysis of nutrients values and reporting is needed.
Chapter 10: General discussion 221
CONCLUSIONS
This thesis fills the significant research gap regarding dietary habits and obesity in Sri Lankan
adults. Findings from the nutrition survey showed on average, Sri Lankan adults consumed over
14 portions of starch/d; moreover, males consumed 5 more portions of cereal than females. Sri
Lankan adults consumed on average of 3.56 portions of added sugars/d with mean daily intake
of fruits and vegetables well below minimum dietary recommendations. As expected, over 70%
of energy was derived from carbohydrates. Moreover, high dietary diversity was associated with
high obesity levels among Sri Lankan adults. The success of a weight reduction intervention is
dependent upon an individual’s awareness of their own body weight and their motivation to
change. Self-perception of body weight is a strong determinant of nutritional habits and weight
management and misperception of body weight may be a barrier to successful weight loss and
healthy weight management in this population. The development and validation of this country-
specific FFQ will boost nutritional research in the country however more effective collaborations
of clinicians, public health experts and policy makers are needed to improve the health and
wellbeing of Sri Lankan adults.
222 Chapter 10: General discussion
REFERENCE LIST
1. Walter Willett EL. Nutritional epidemiology. In: Willett W, editor. Monographs in
Epidemiology and Biostatistics: Oxford University Press; 1998. p. 101-47.
2. Wendy Wrieden. A short review of dietary assessment methods used in National and
Scottish Research Studies. Dundee2003.
3. Henderson L, Gregory J, Swan G. The national diet & nutrition survey: Adults aged 19 to
64 years: Stationery Office; 2003.
4. Gersovitz M, Madden JP, Smiciklas-Wright H. Validity of the 24-hr. dietary recall and
seven-day record for group comparisons. Journal of the American Dietetic Association.
1978;73(1):48.
5. Buzzard I, Faucett CL, Jeffery RW, McBANE L, McGOVERN P, Baxter JS, et al.
Monitoring Dietary Change in a Low-Fat Diet Intervention Study:: Advantages of Using 24-
Hour Dietary Recalls vs Food Records. Journal of the American Dietetic Association.
1996;96(6):574-9.
6. Shahar D, Shai I, Vardi H, Brener-Azrad A, Fraser D. Development of a semi-
quantitative Food Frequency Questionnaire (FFQ) to assess dietary intake of multiethnic
populations. European journal of epidemiology. 2003;18(9):855-61.
7. Liu S, Manson JE, Stampfer MJ, Holmes MD, Hu FB, Hankinson SE, et al. Dietary
glycemic load assessed by food-frequency questionnaire in relation to plasma high-density-
lipoprotein cholesterol and fasting plasma triacylglycerols in postmenopausal women. Am J Clin
Nutr. 2001 Mar;73(3):560-6.
8. Bharathi AV, Kurpad AV, Thomas T, Yusuf S, Saraswathi G, Vaz M. Development of
food frequency questionnaires and a nutrient database for the Prospective Urban and Rural
Epidemiological (PURE) pilot study in South India: methodological issues. Asia Pac J Clin Nutr.
2008;17(1):178-85.
9. Victoria CC. Dietary questionnaires. 2010; Available from:










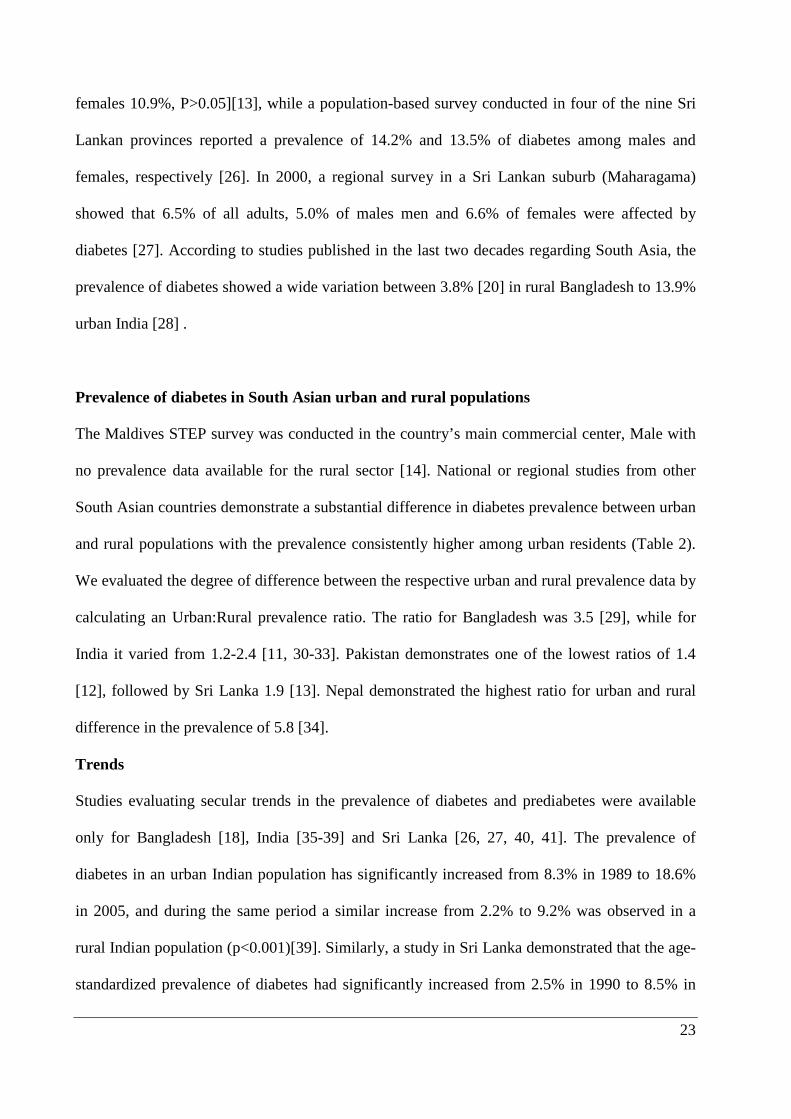
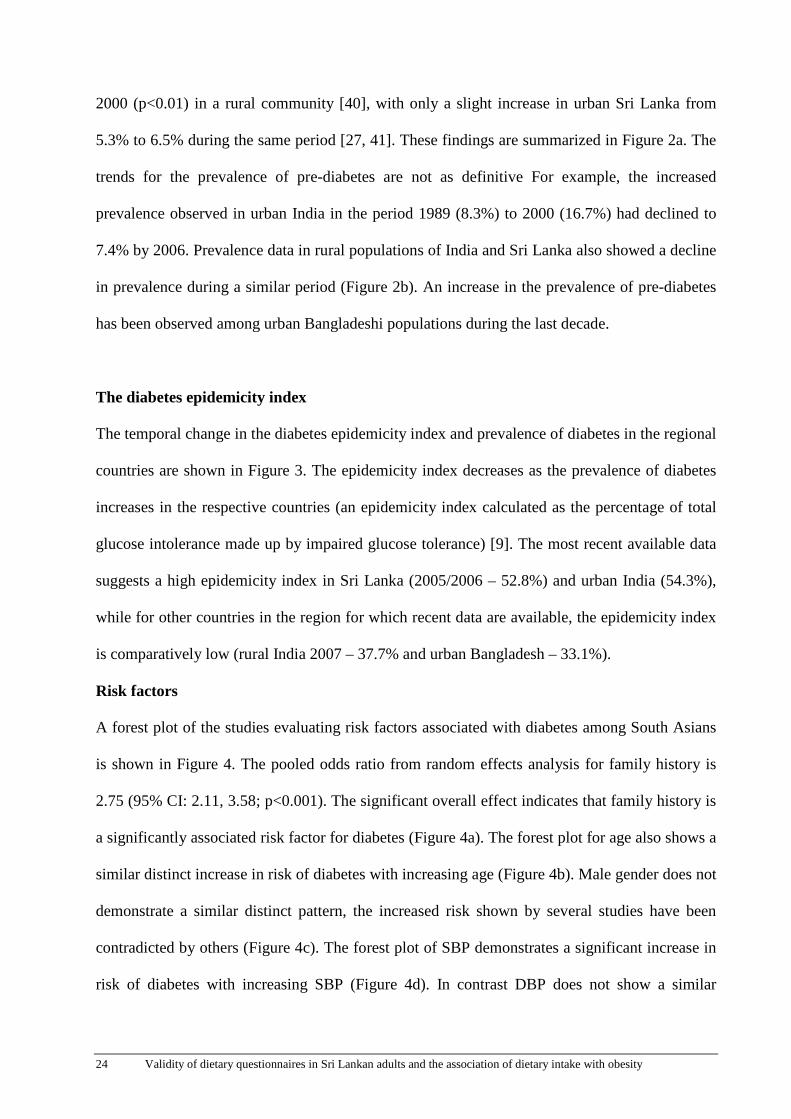

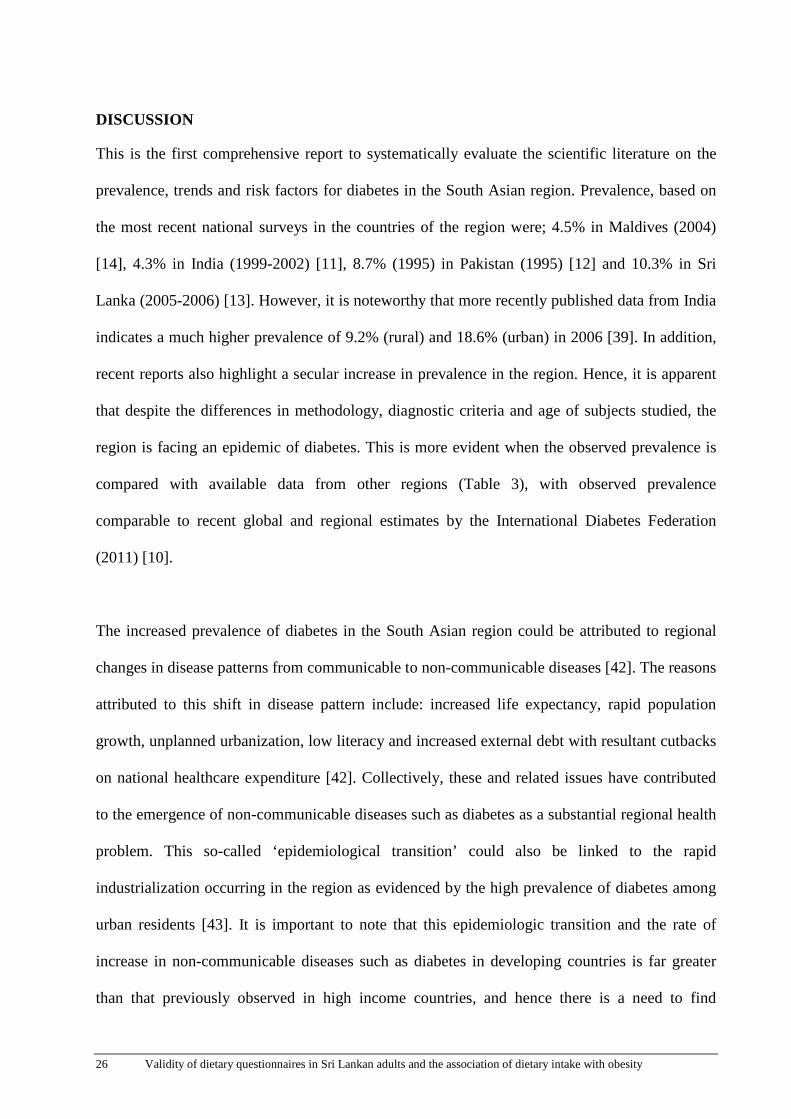

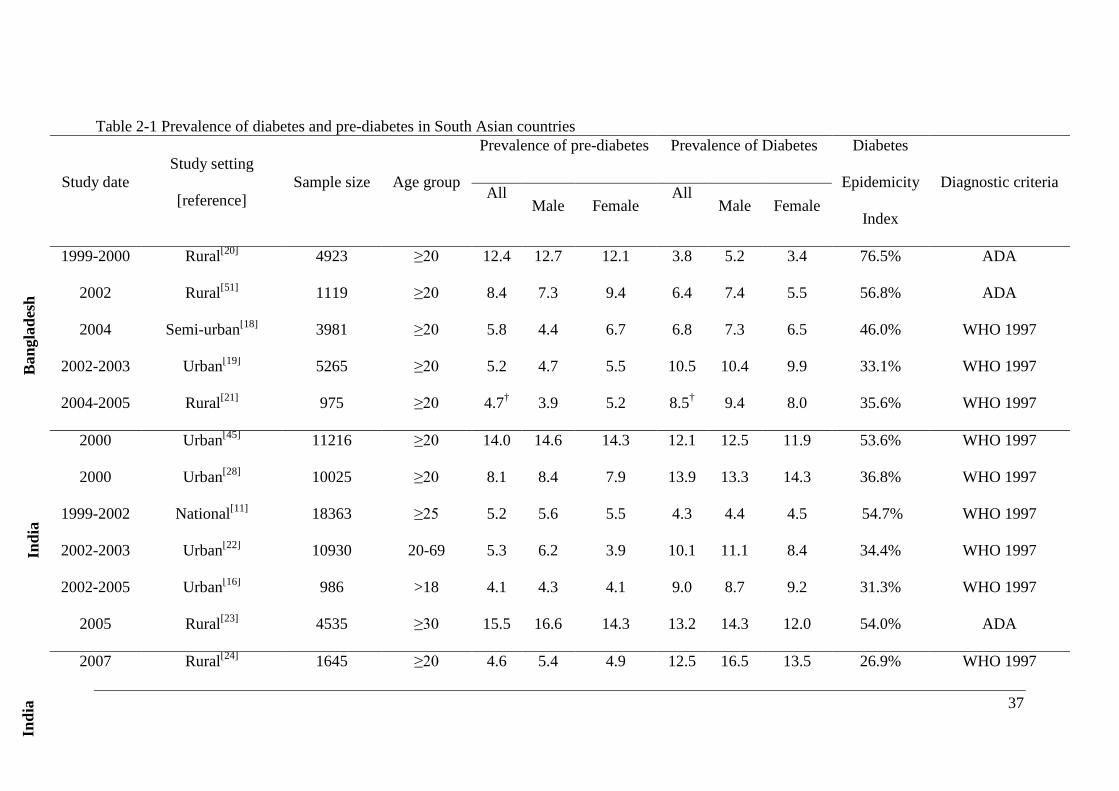
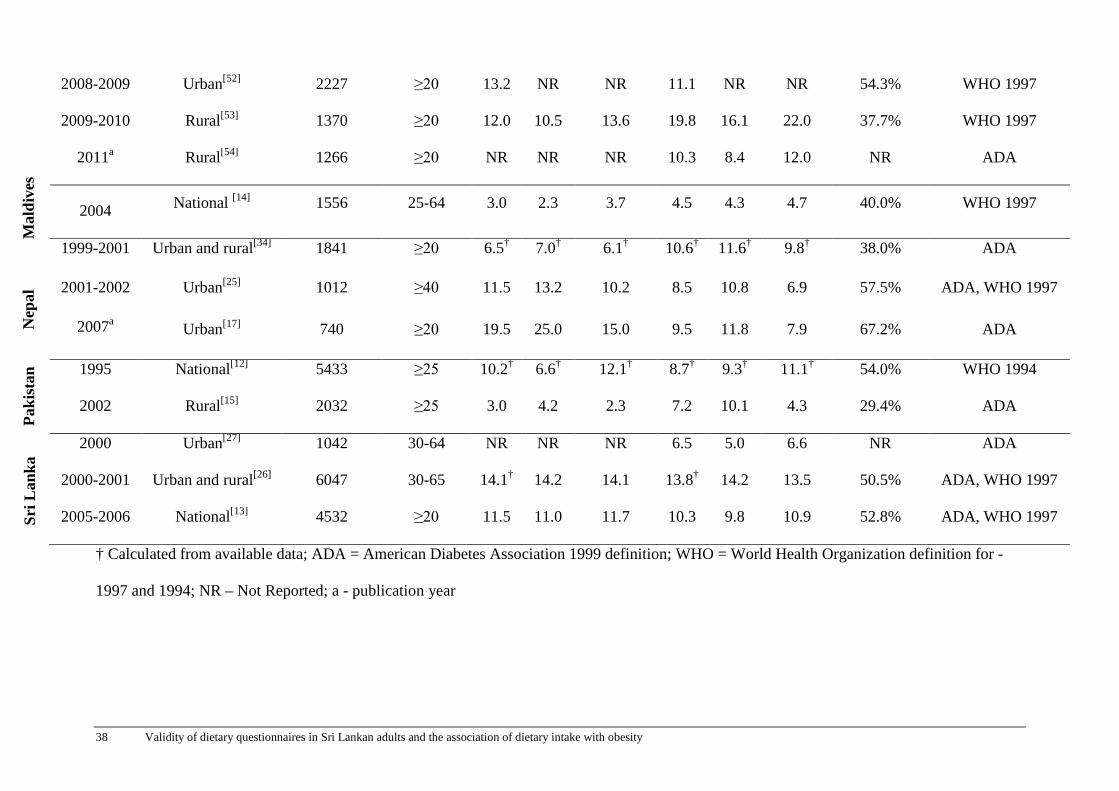
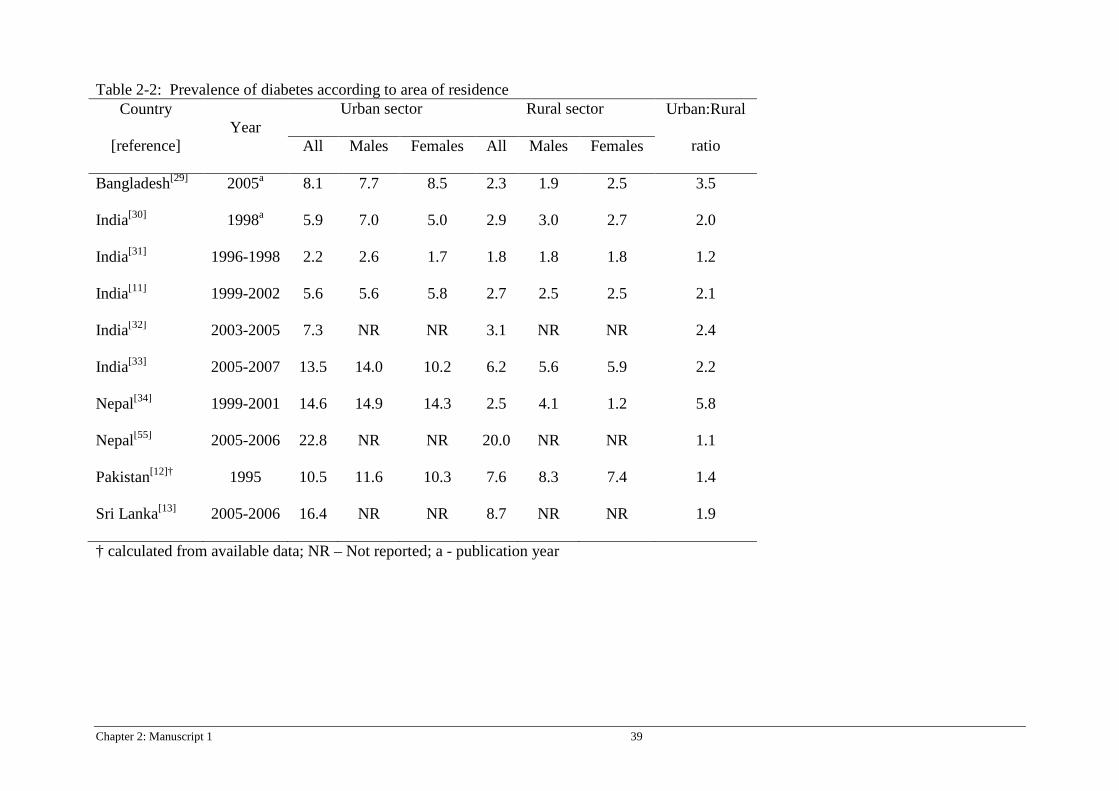

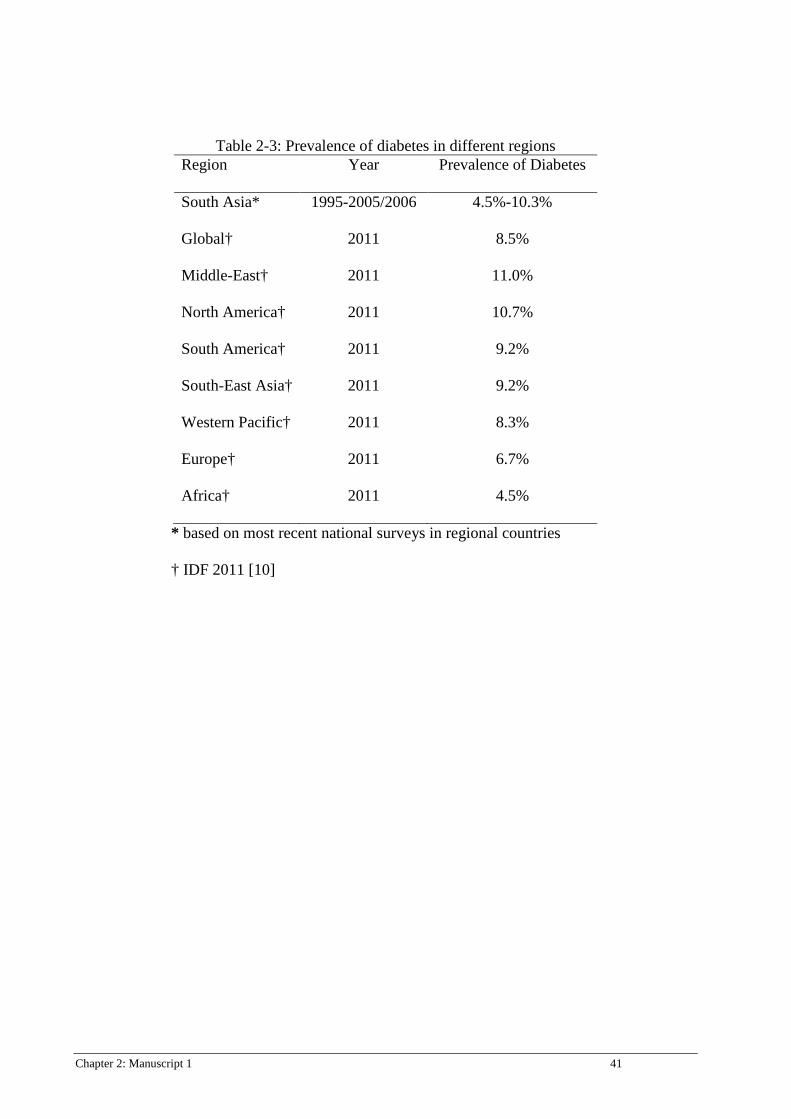
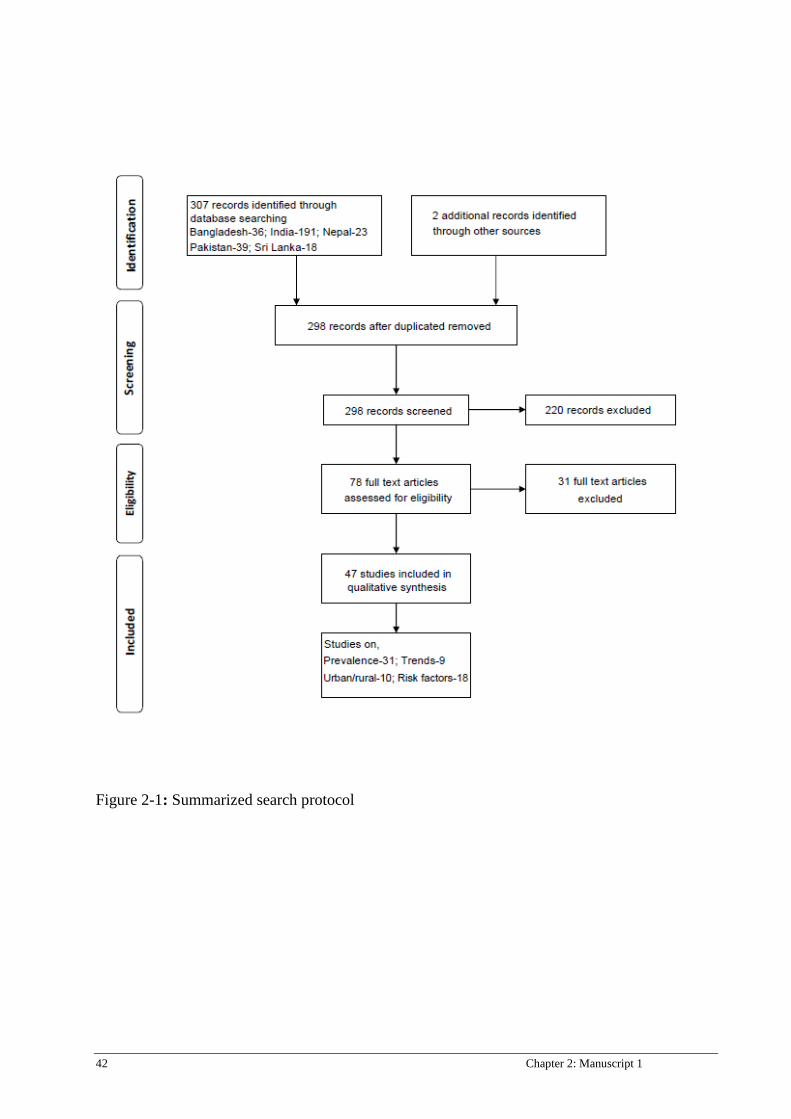
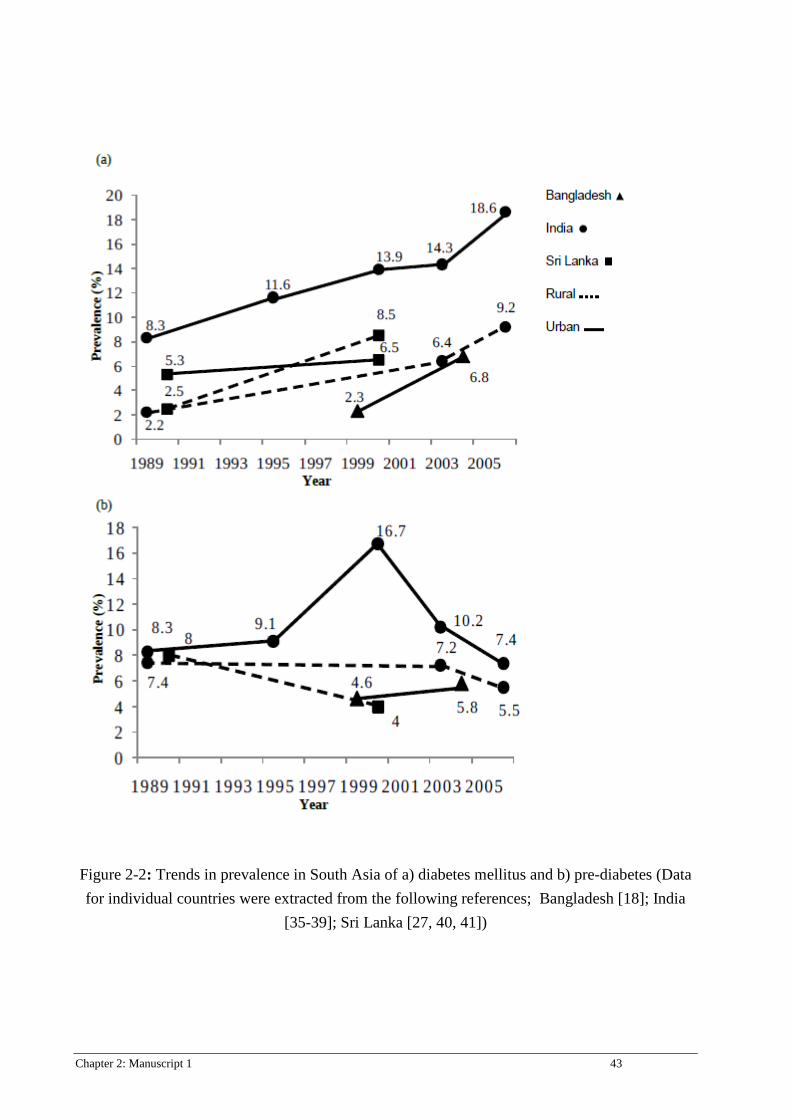
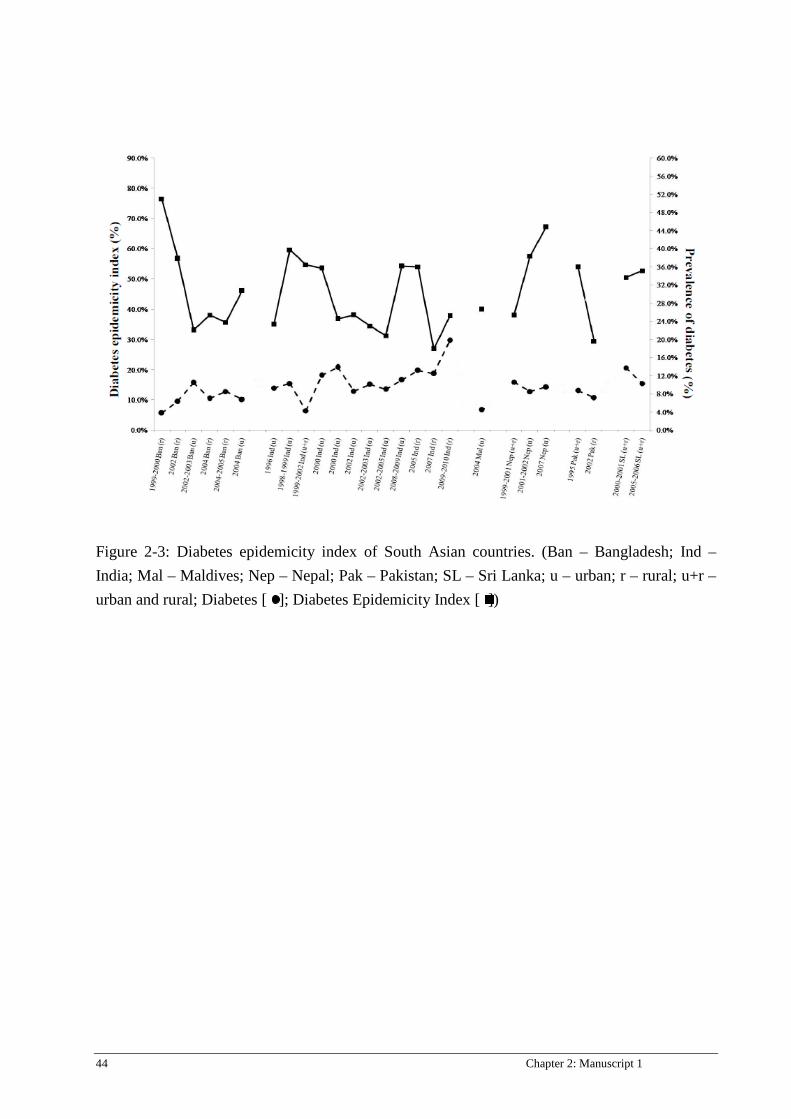
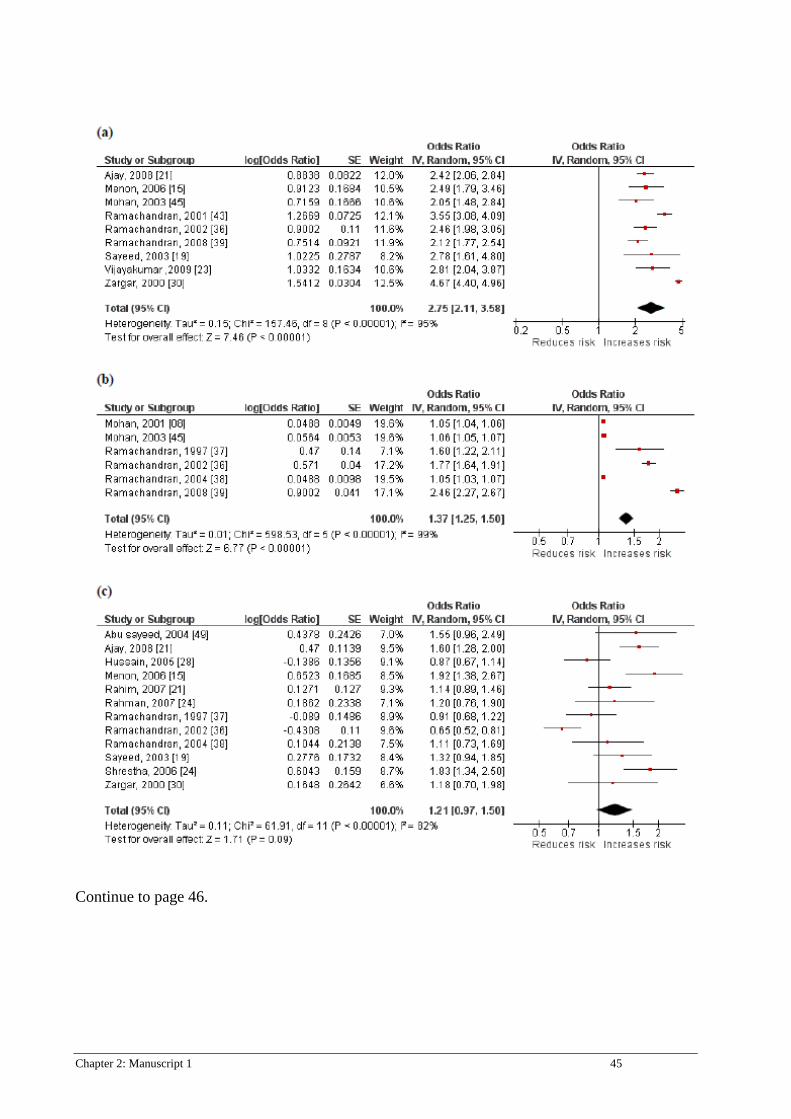
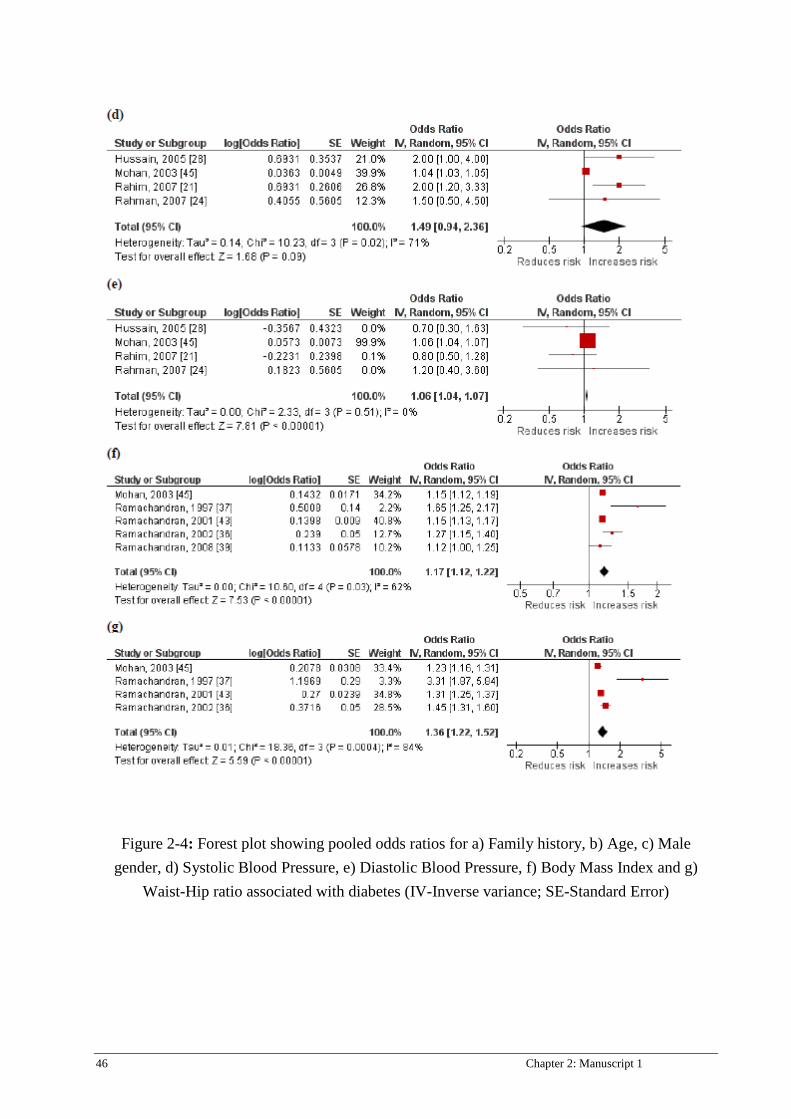



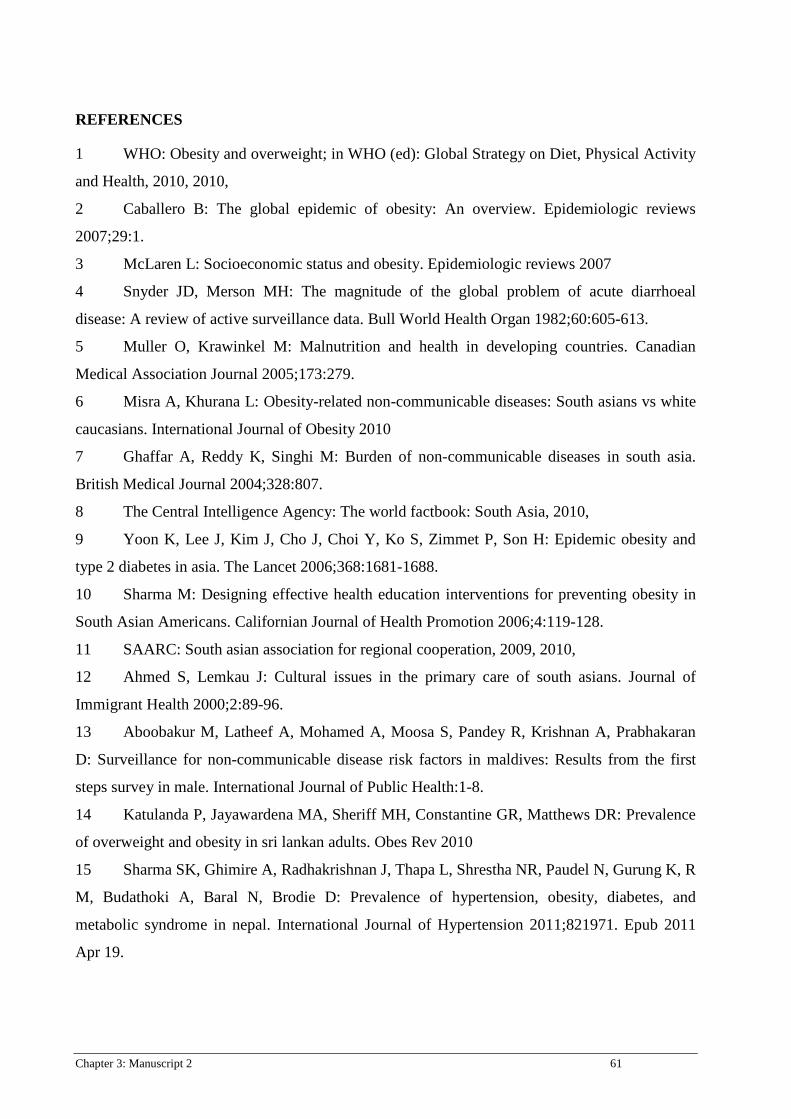
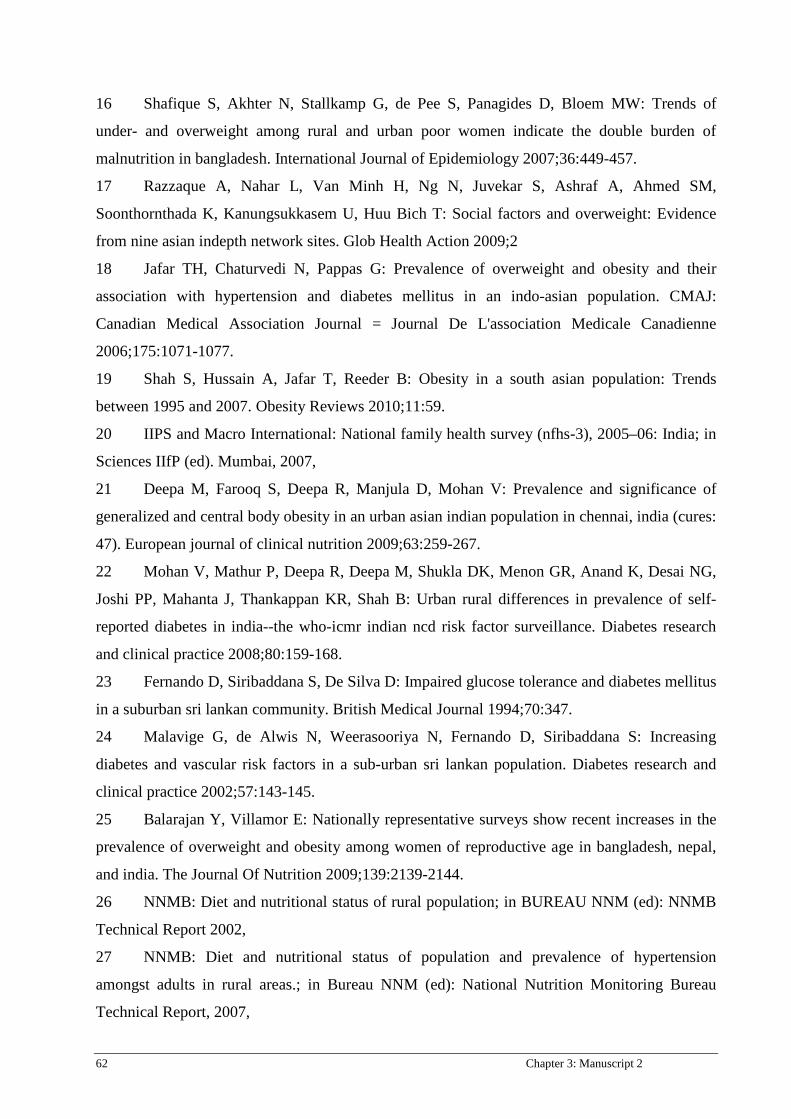
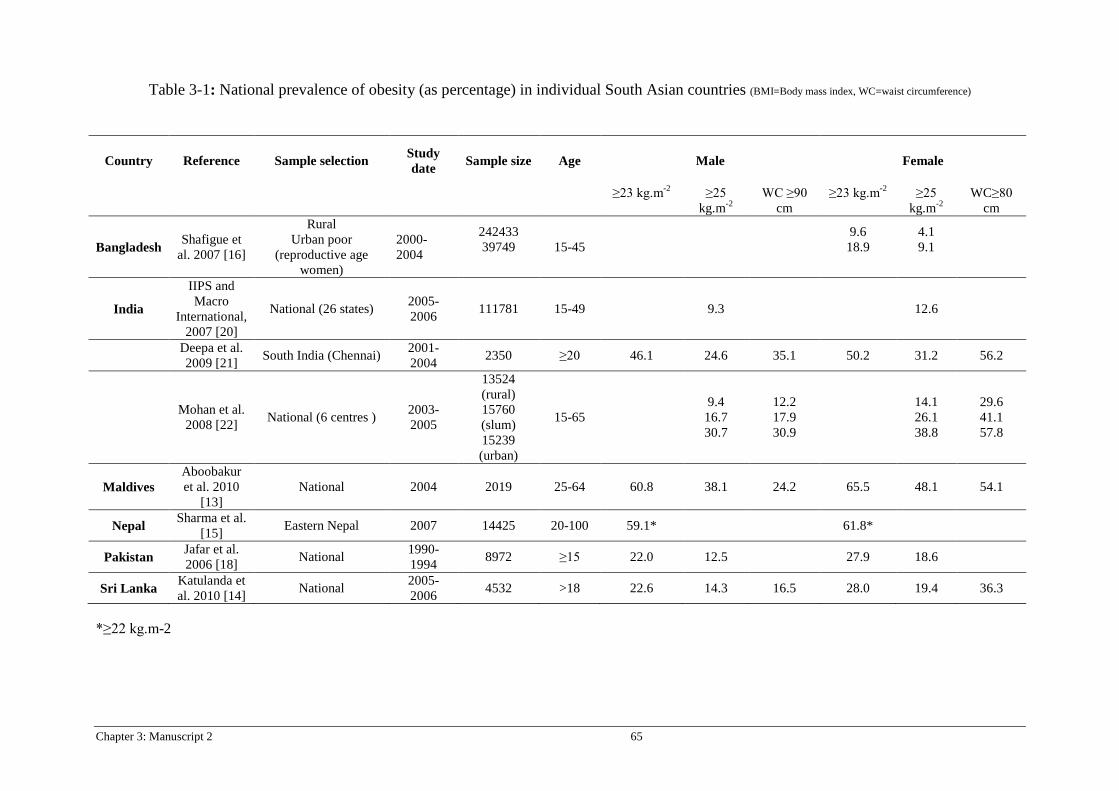
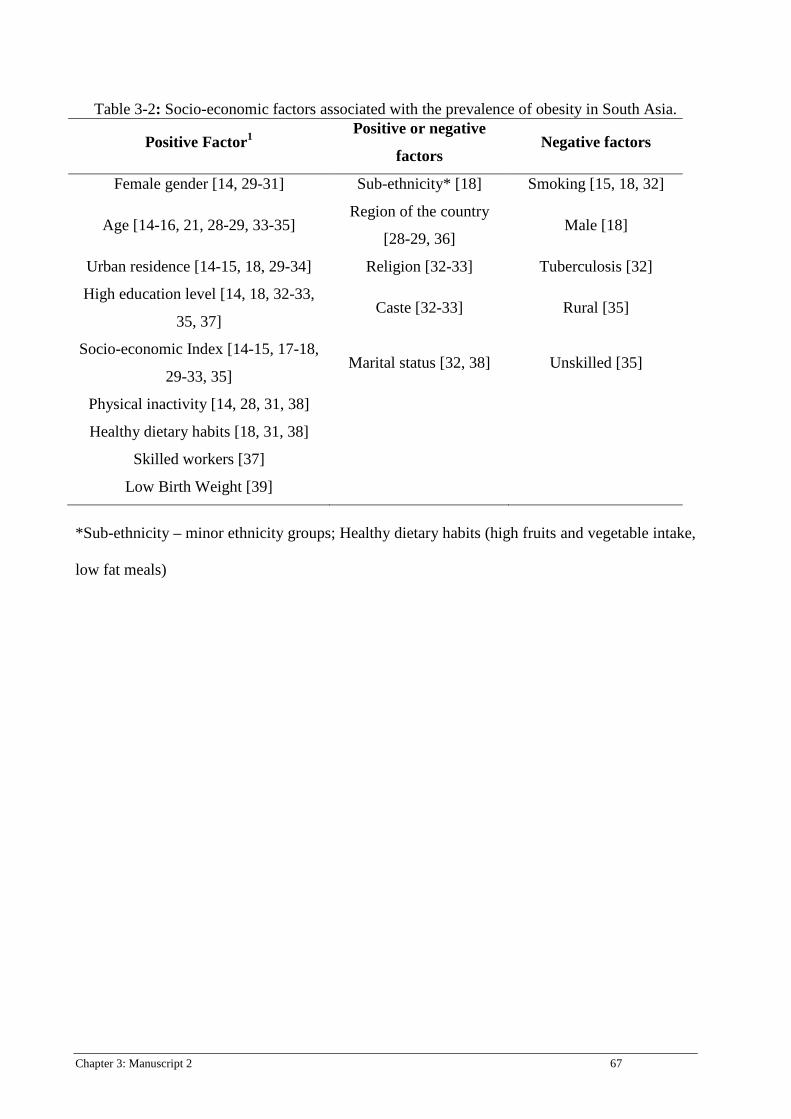
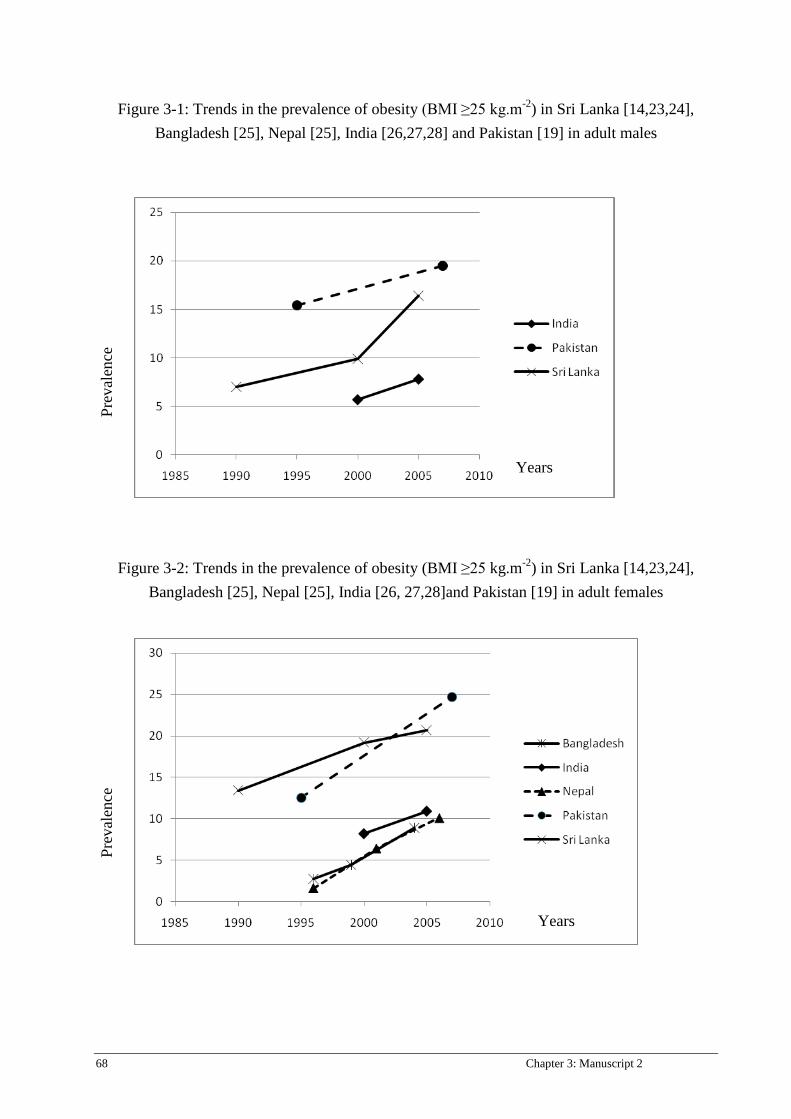
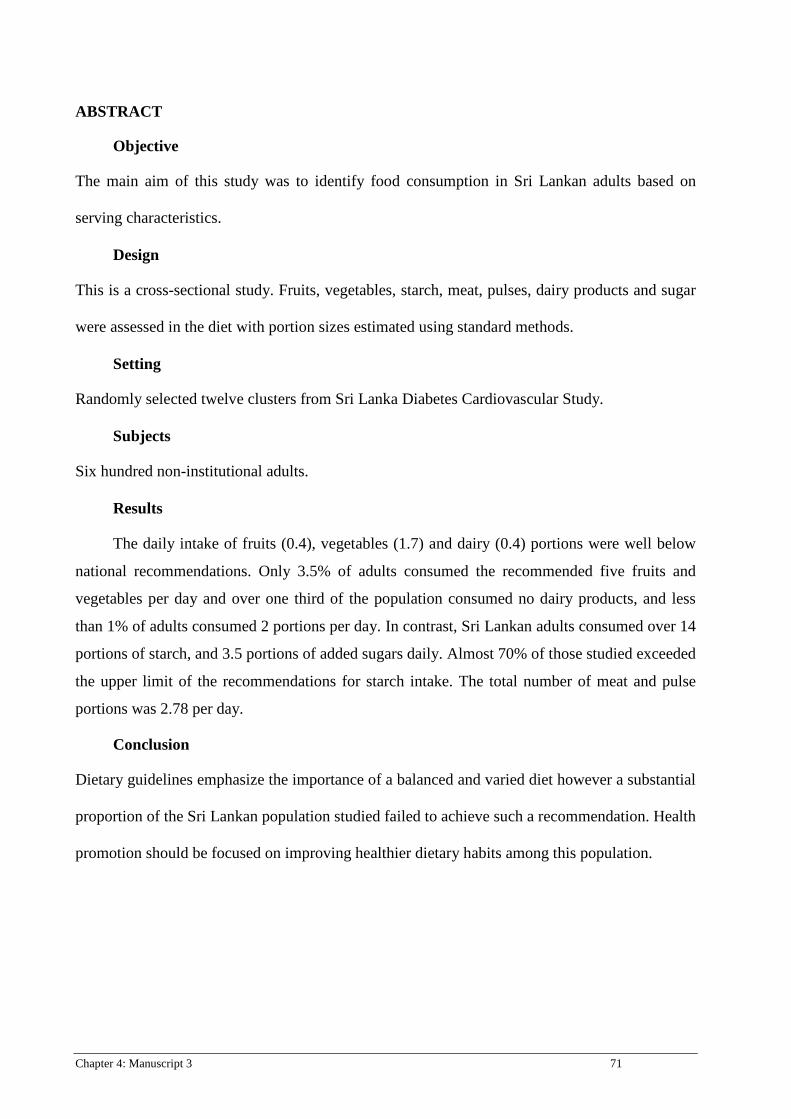
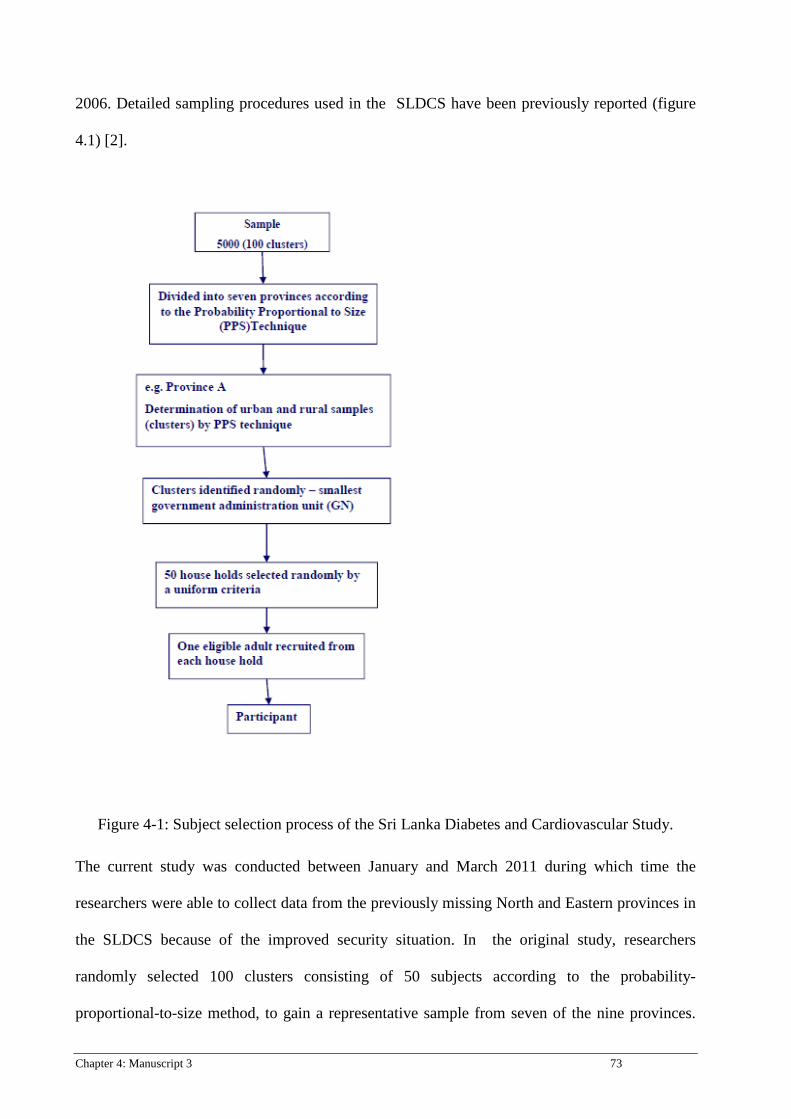
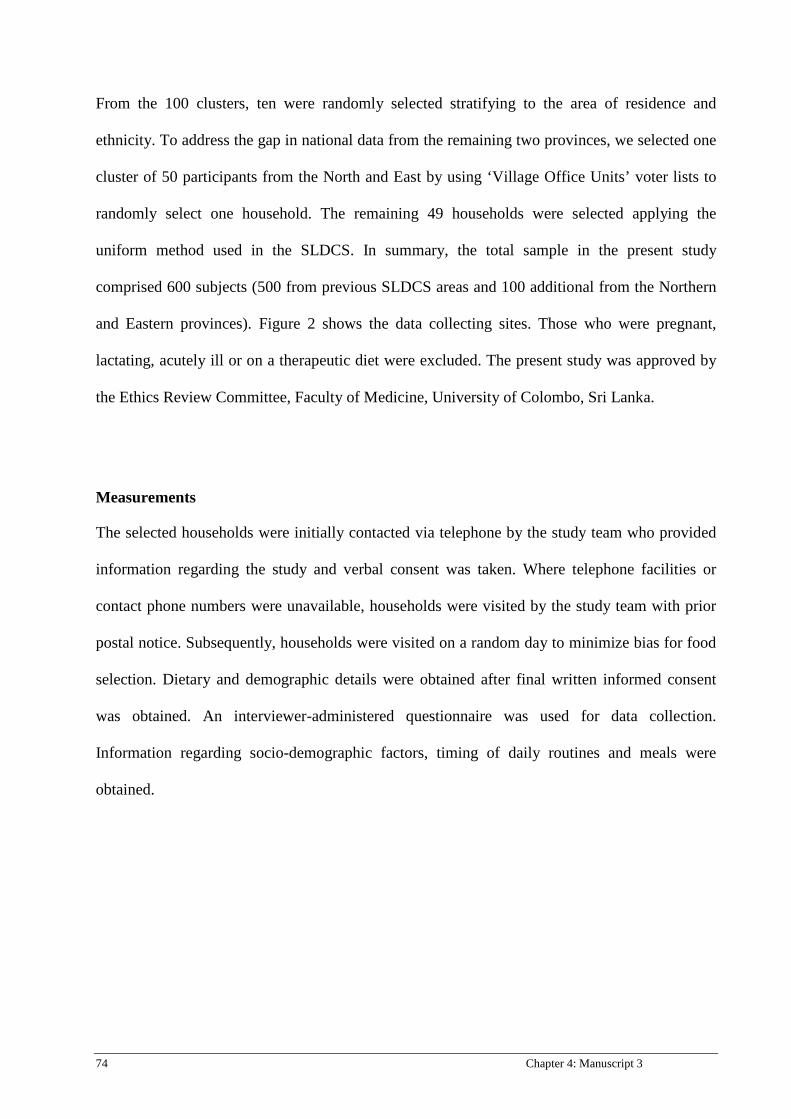
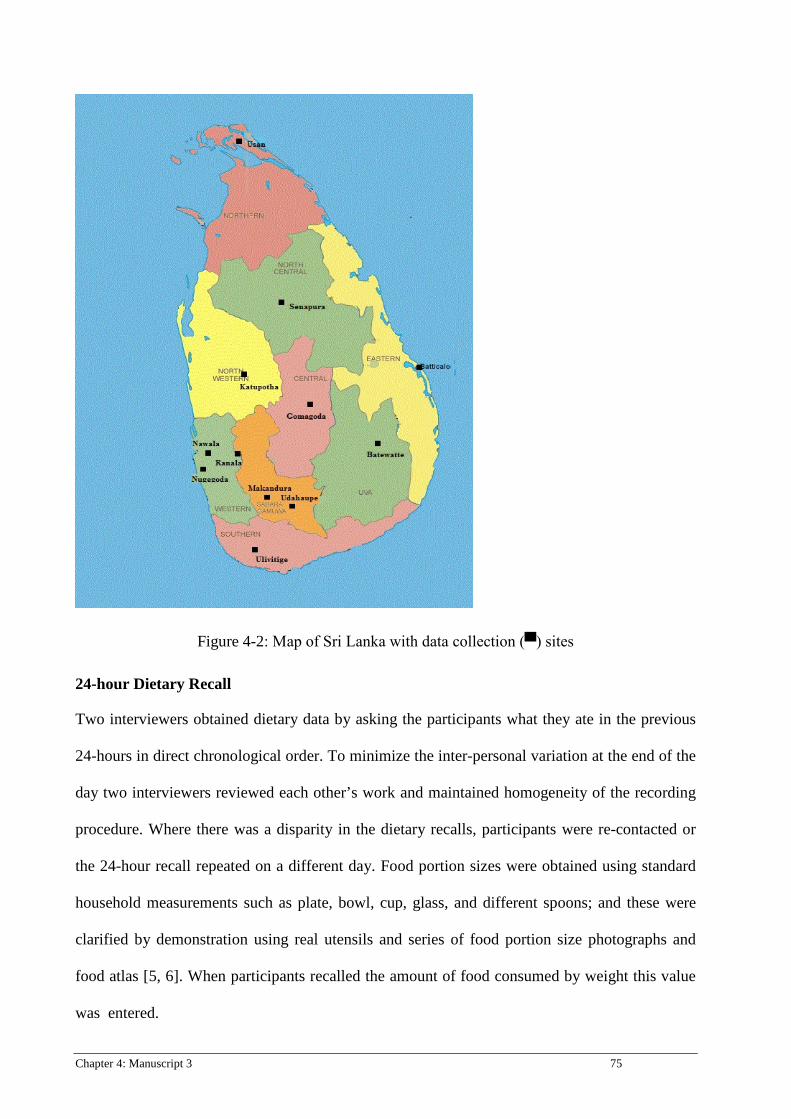
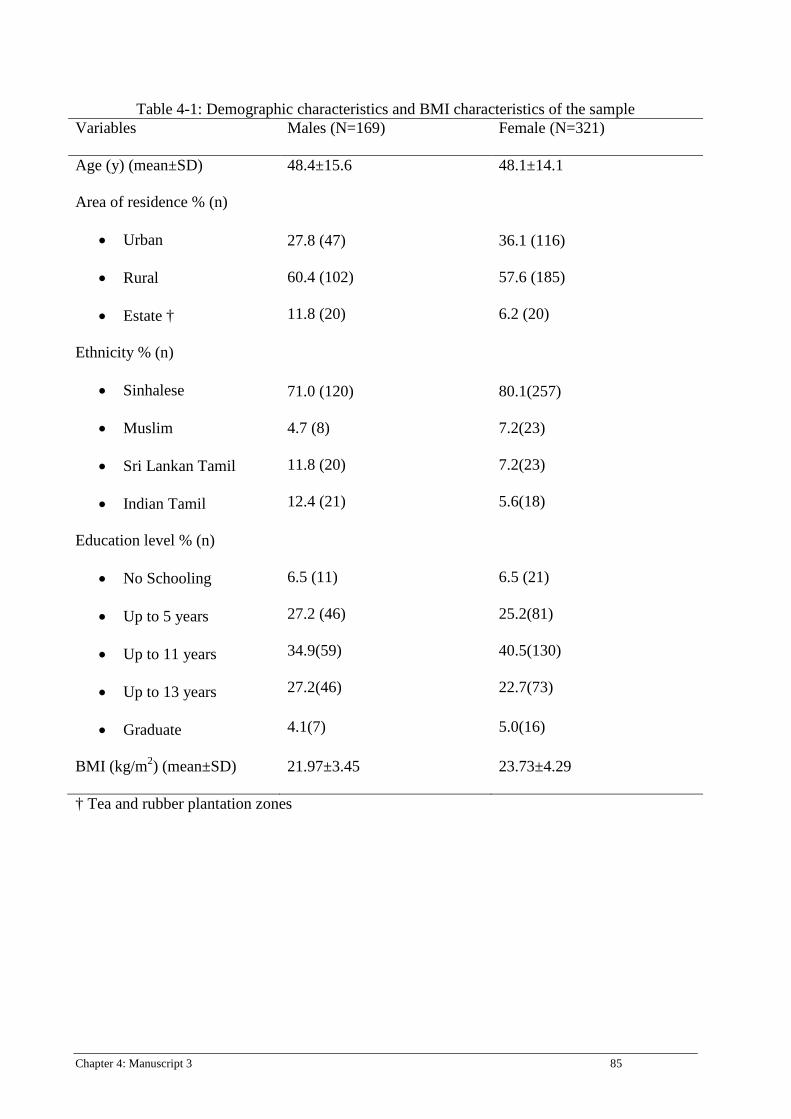
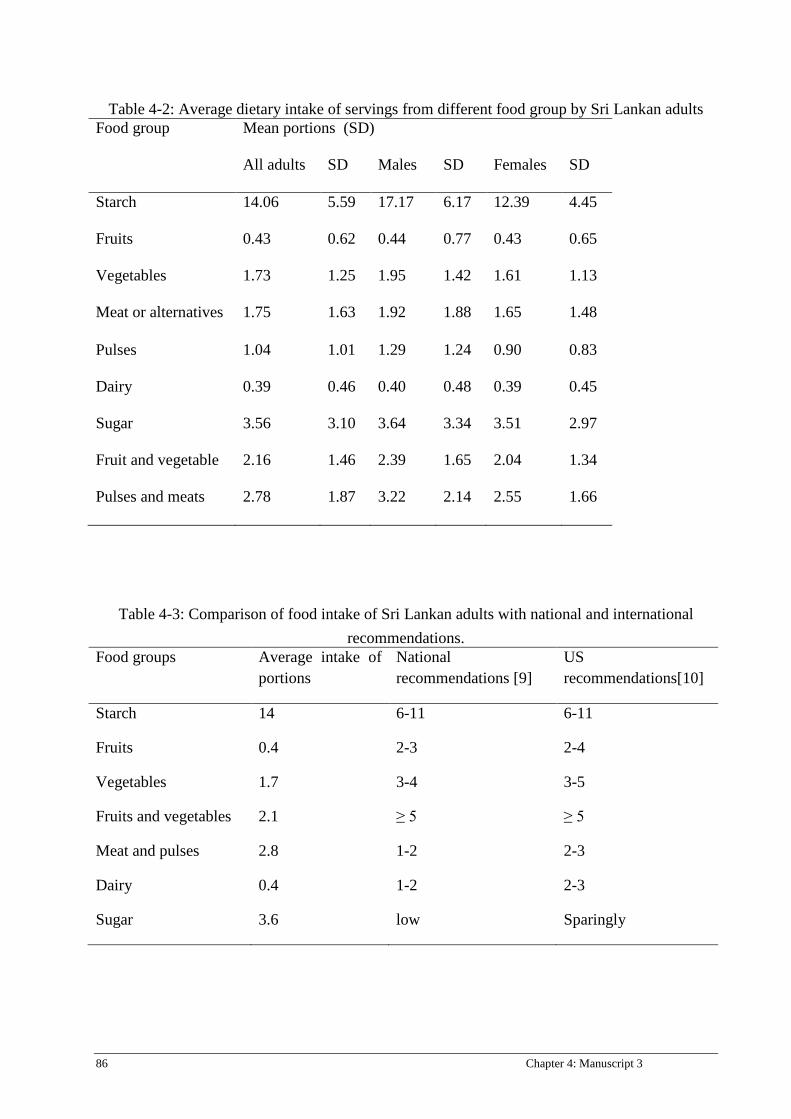
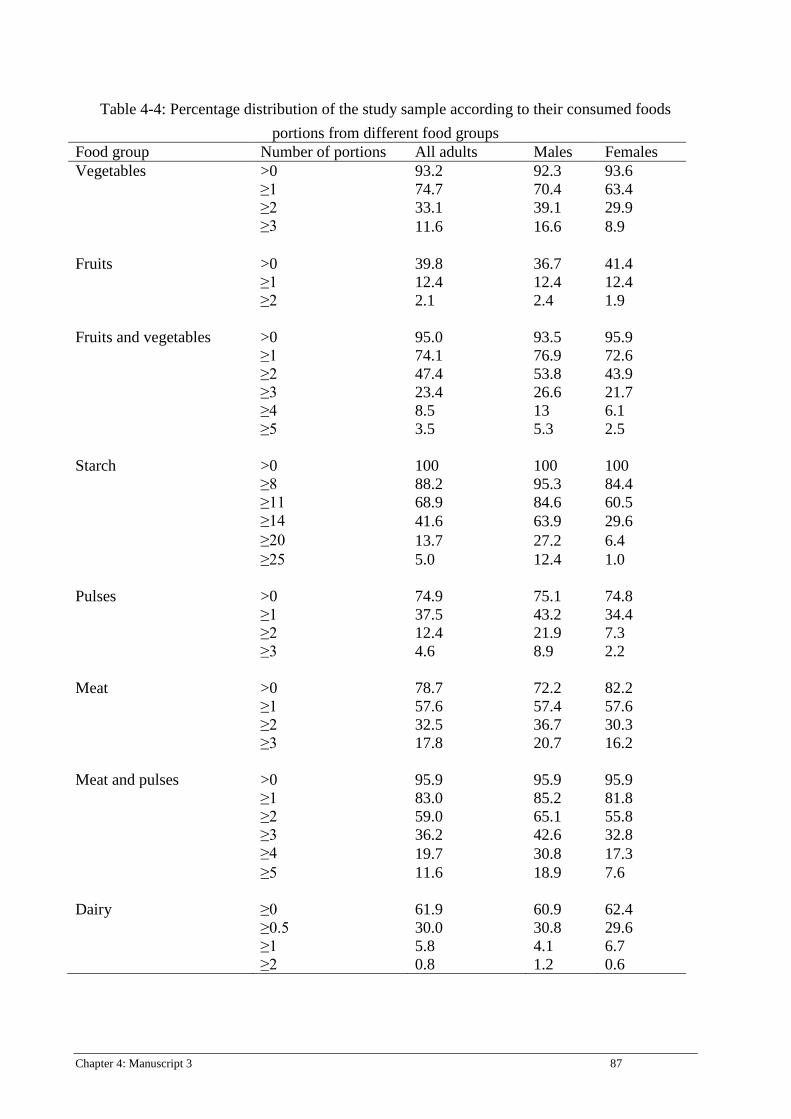
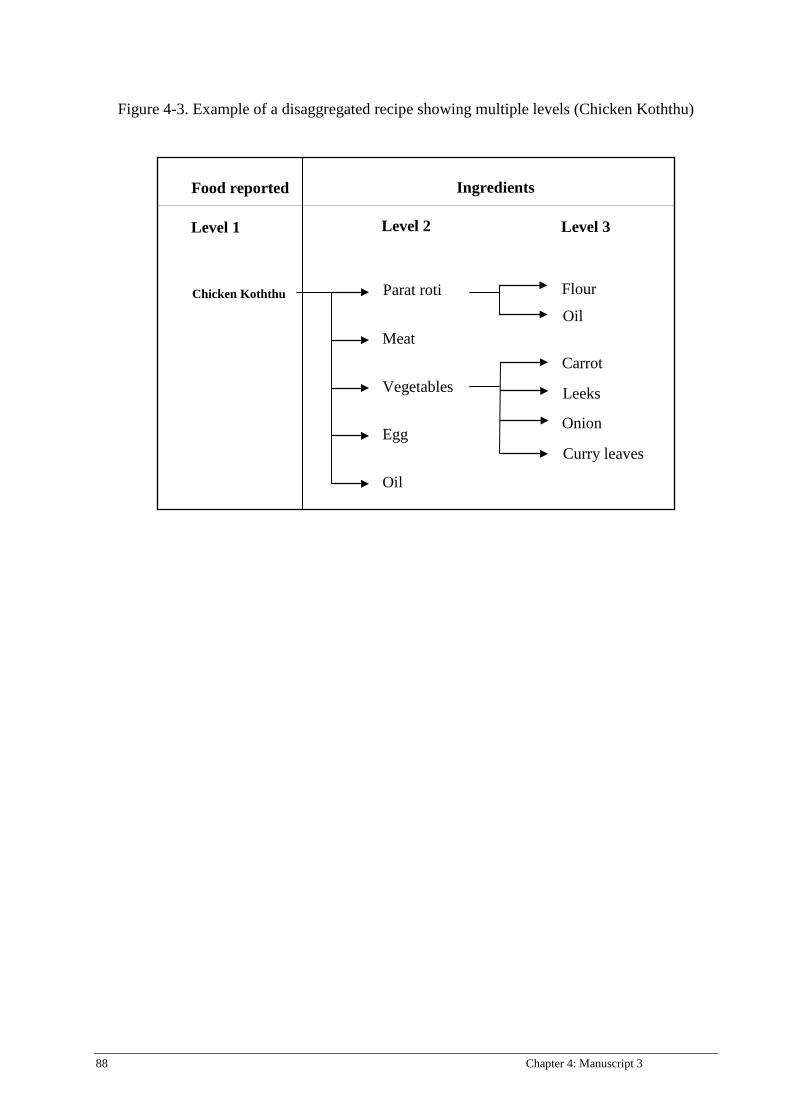

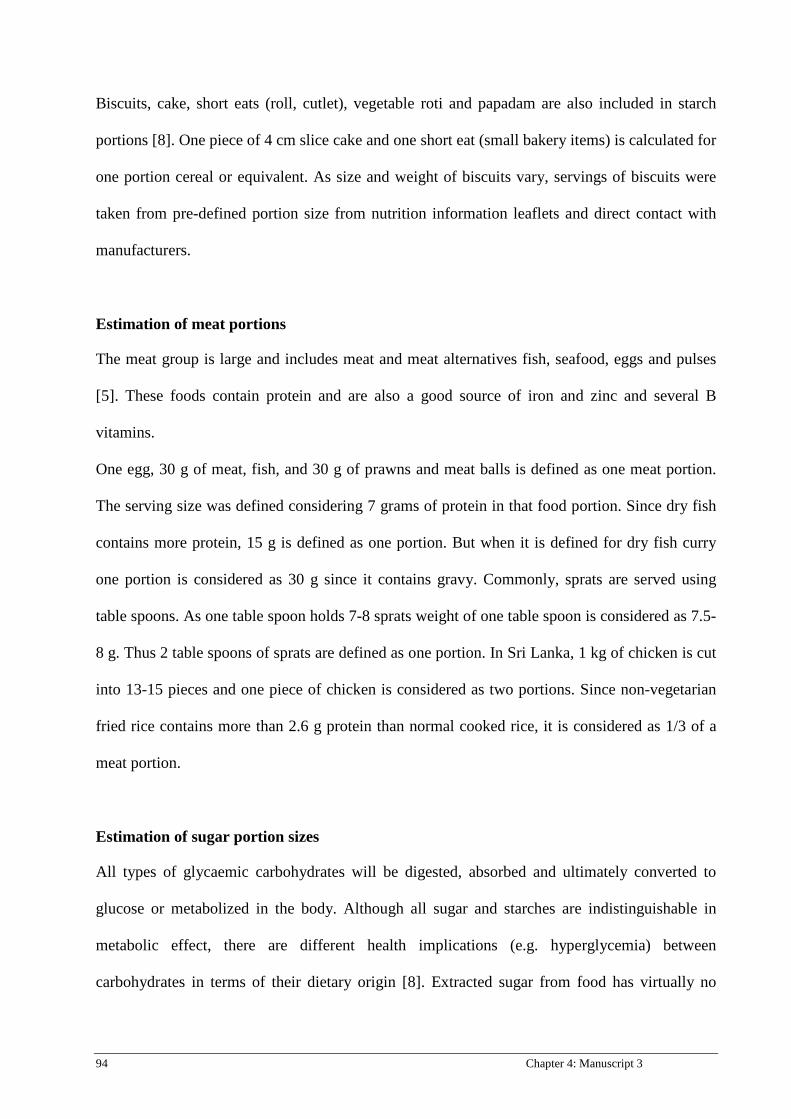

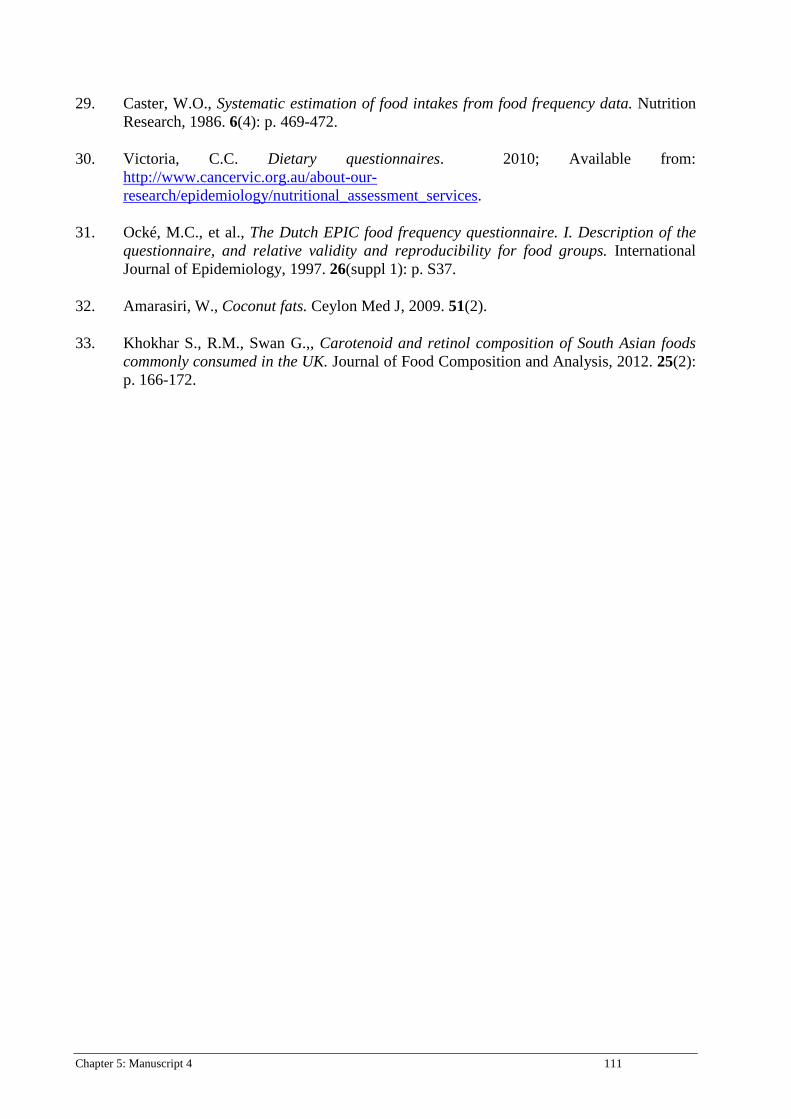
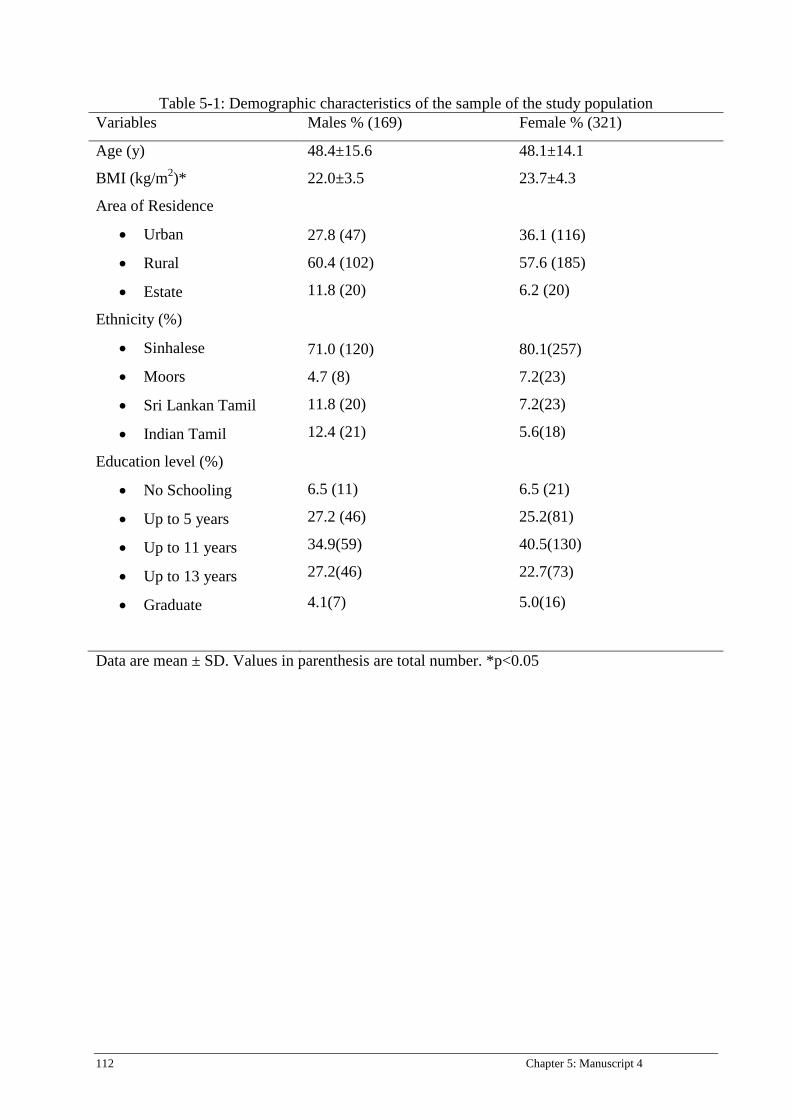
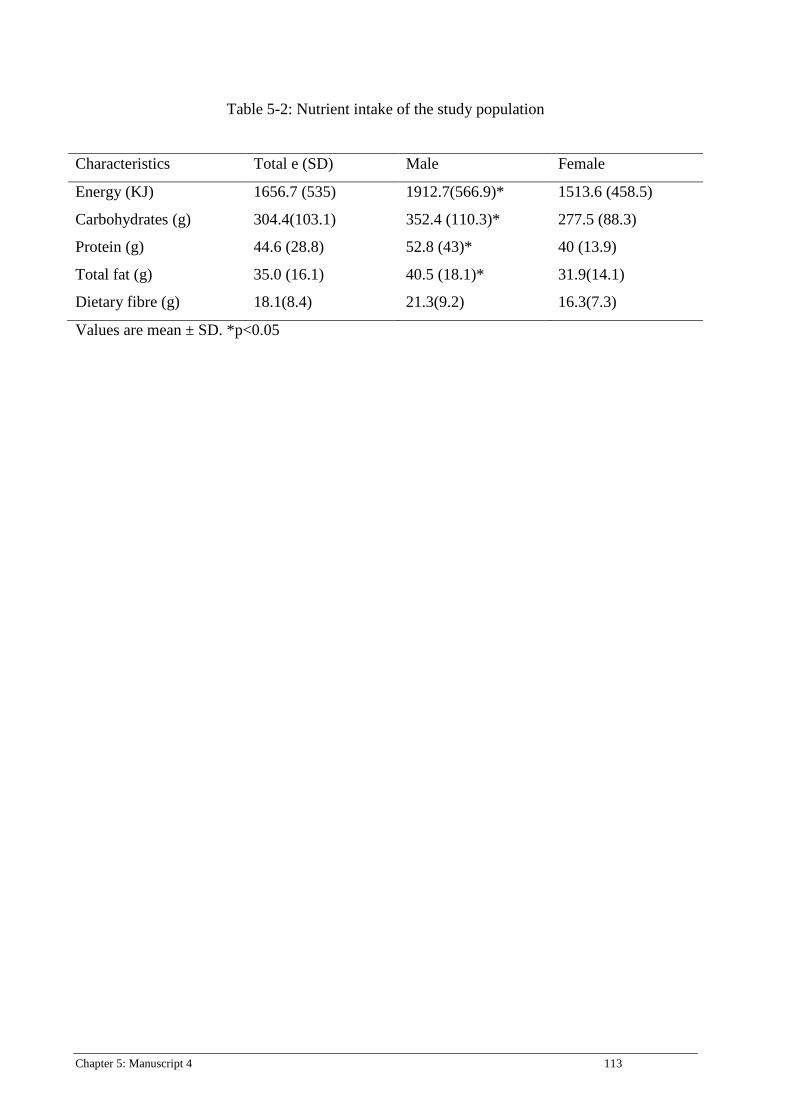
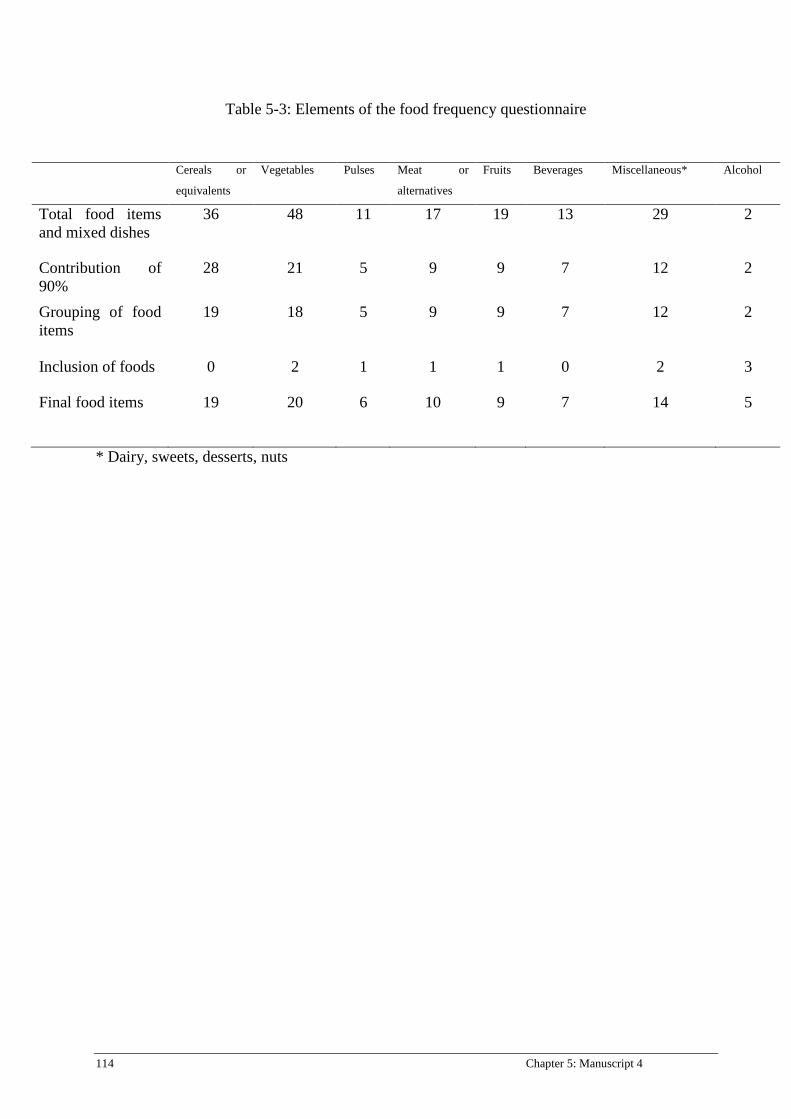


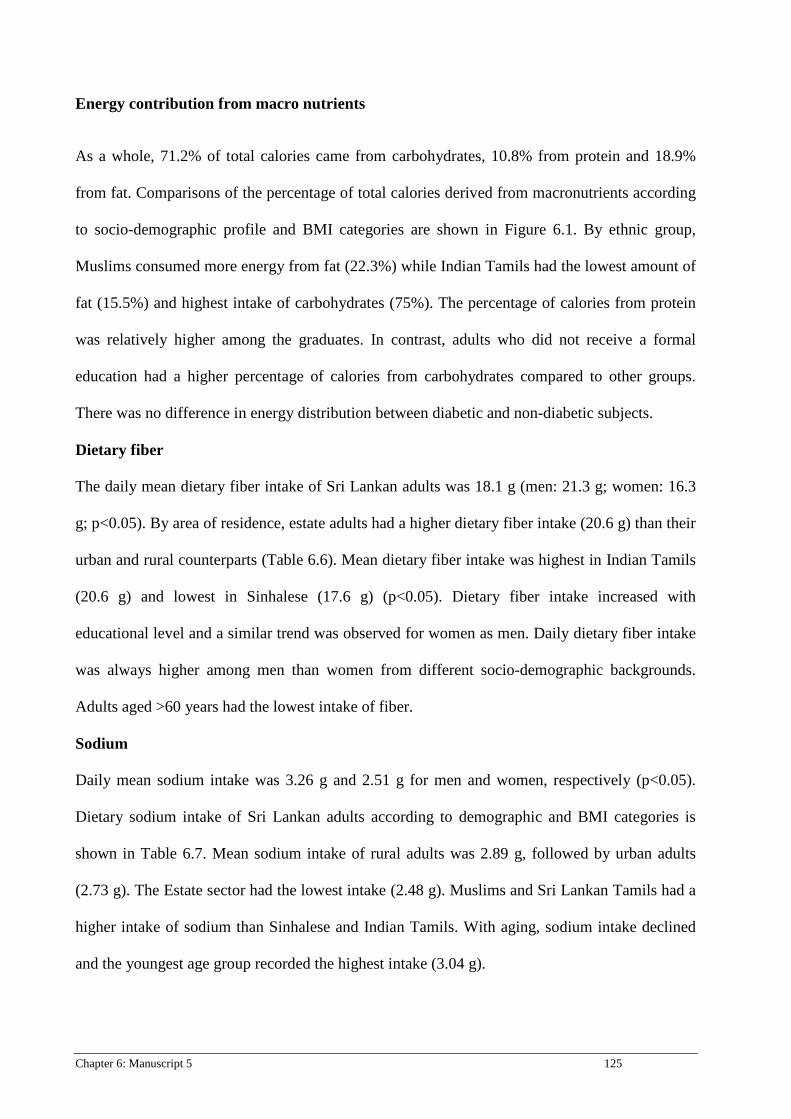
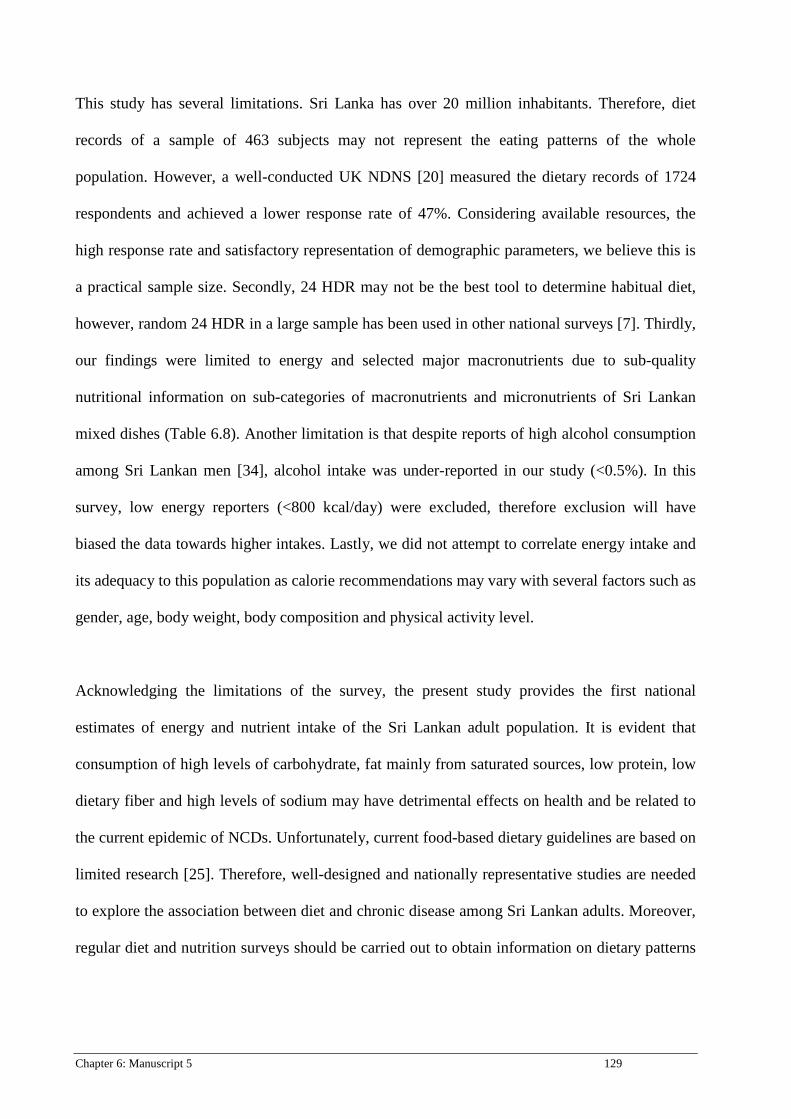

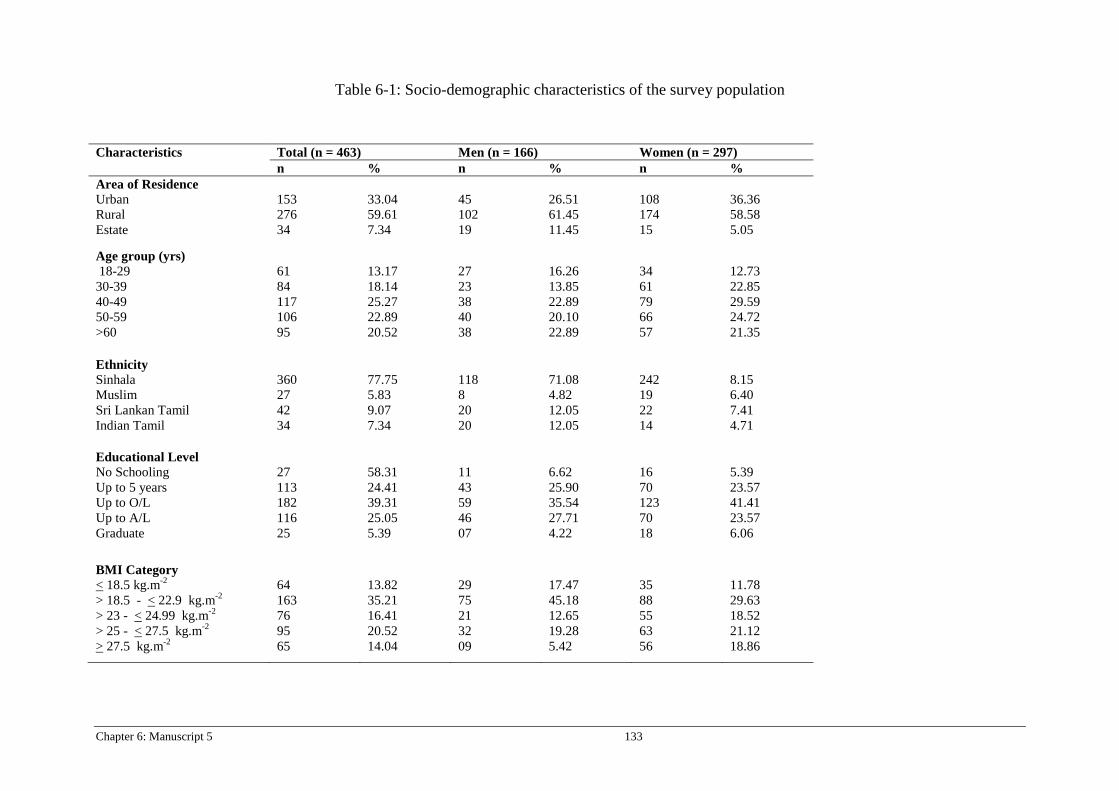
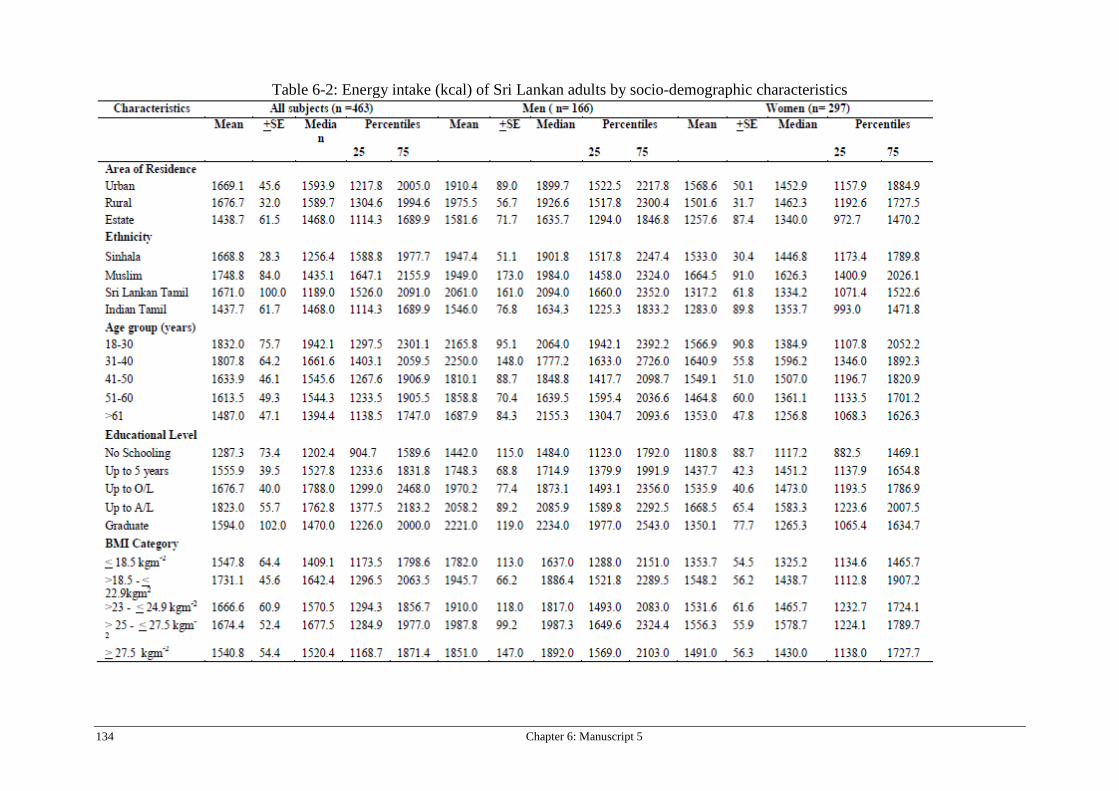
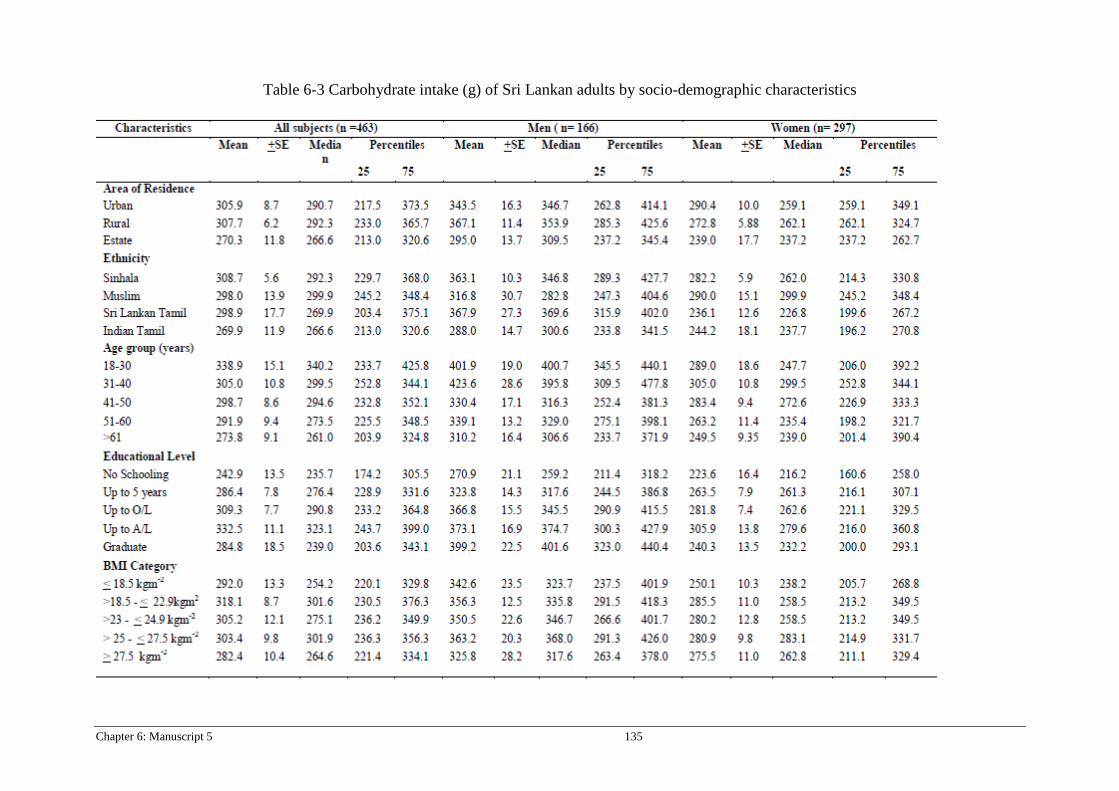
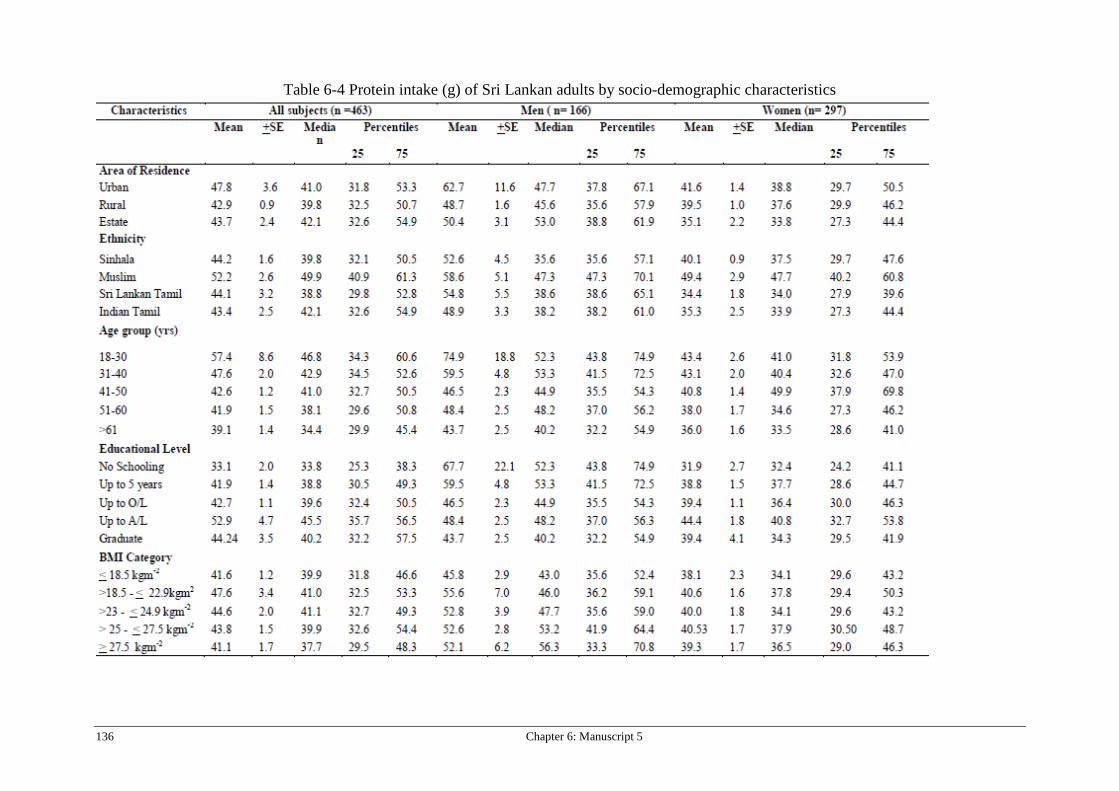
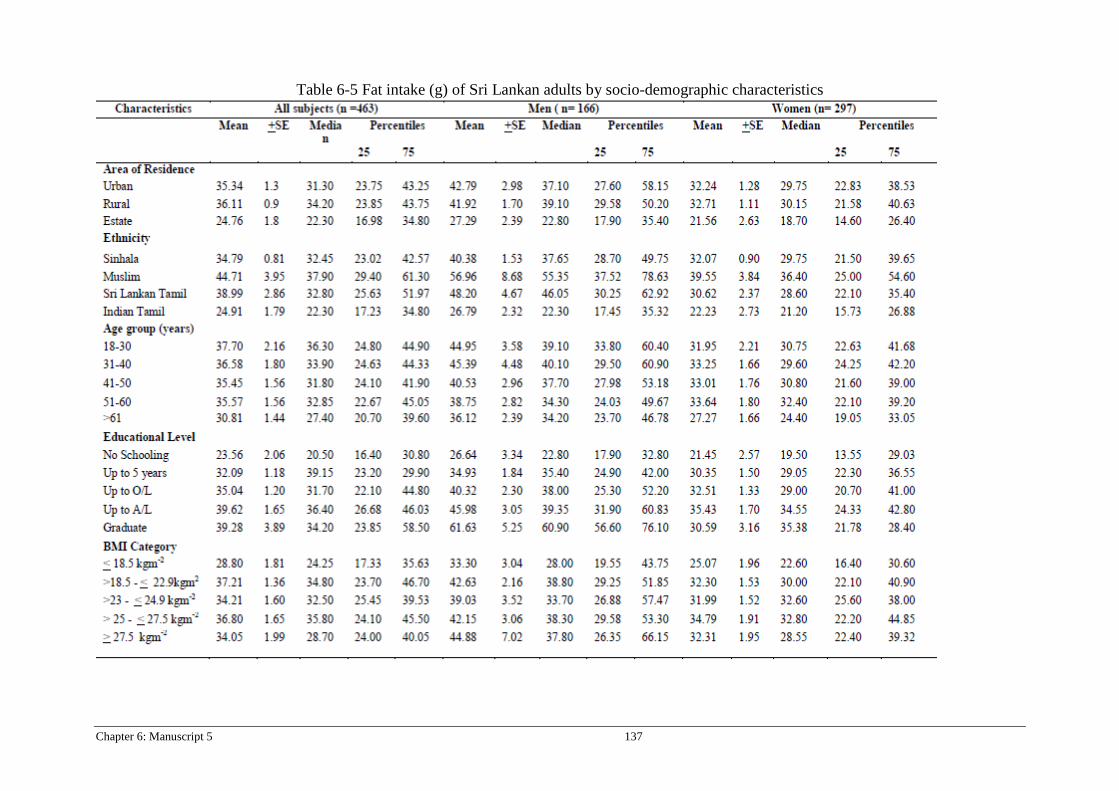
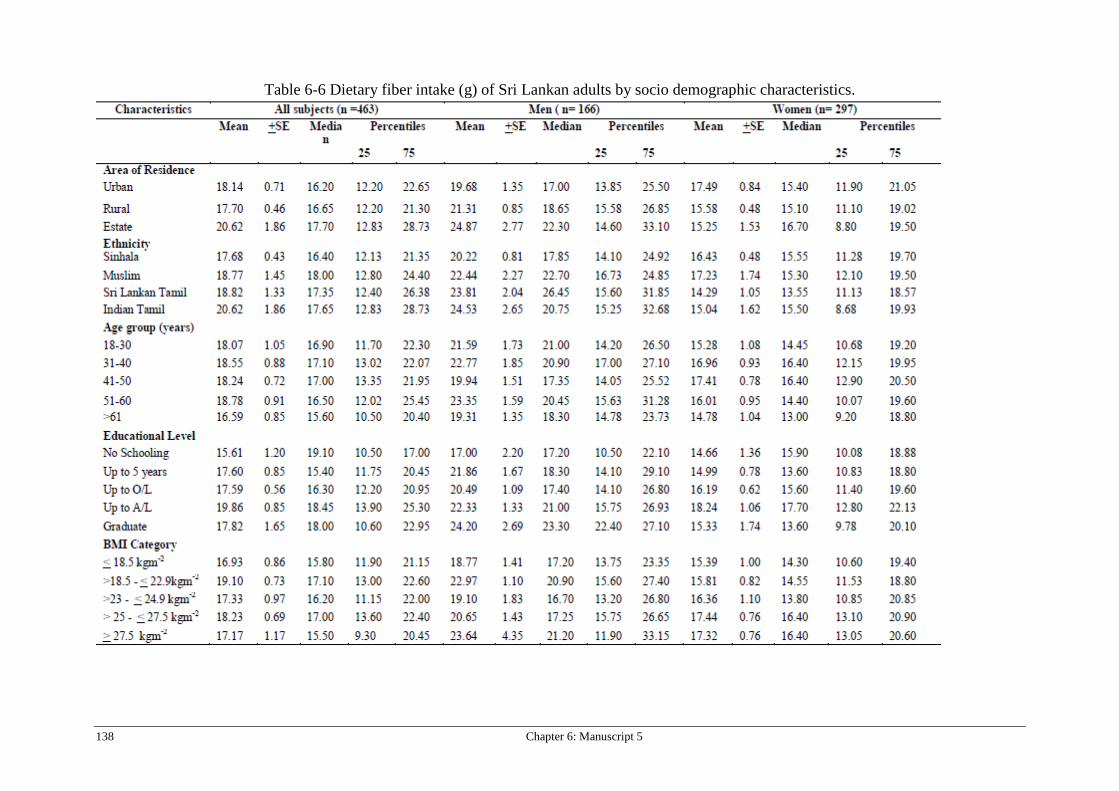
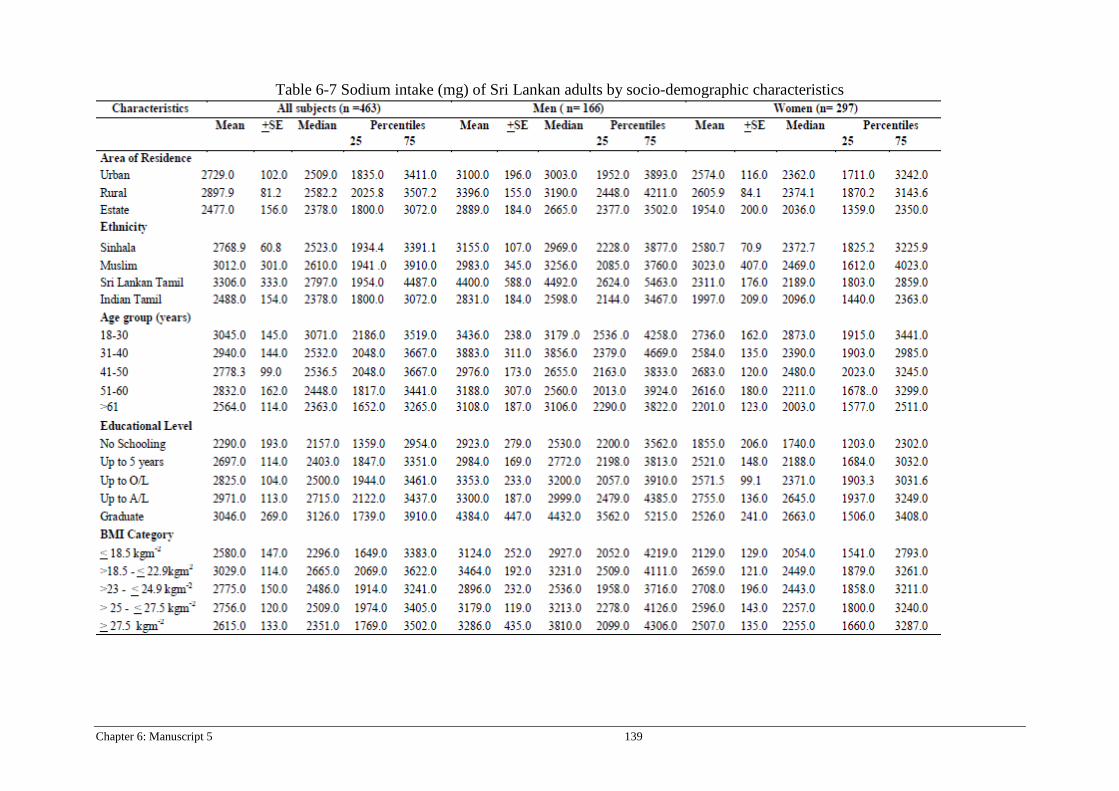
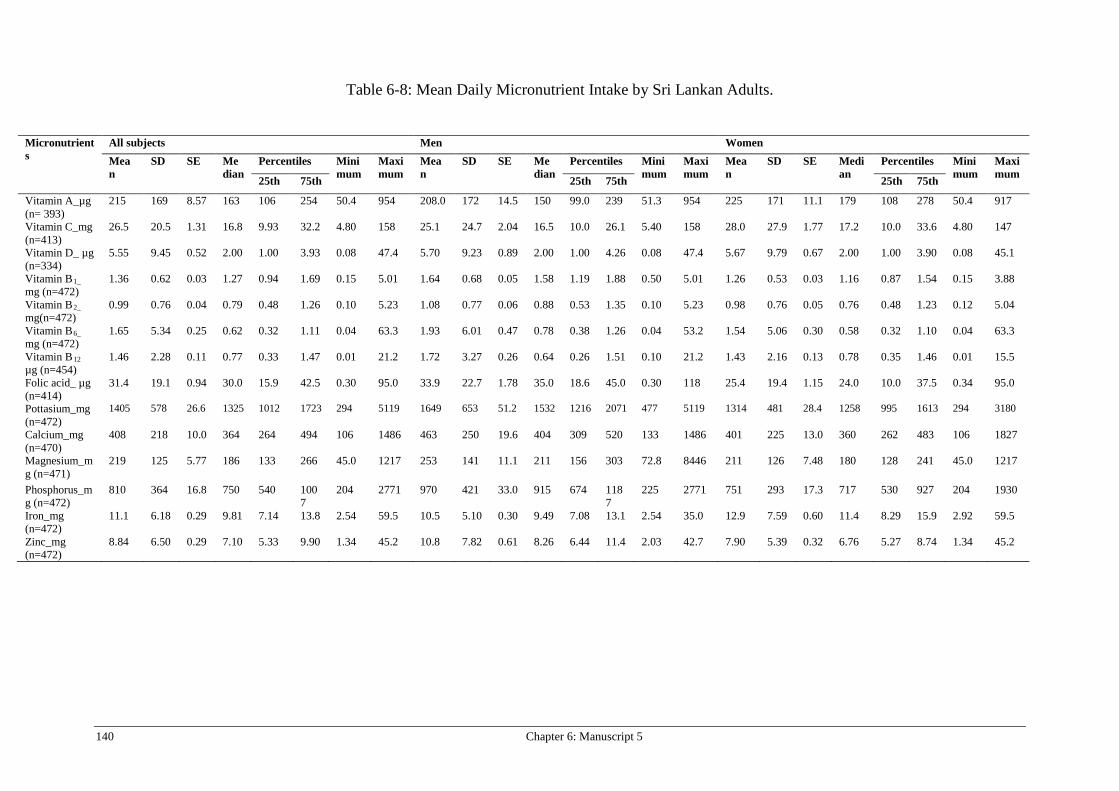
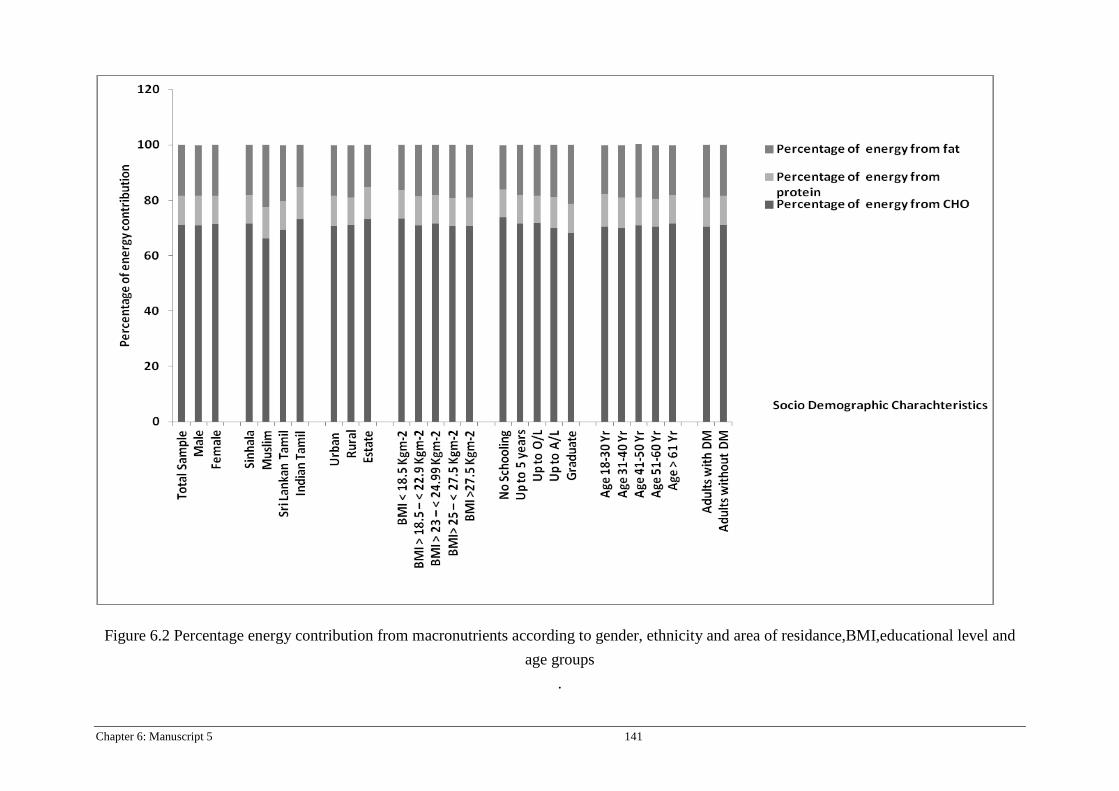
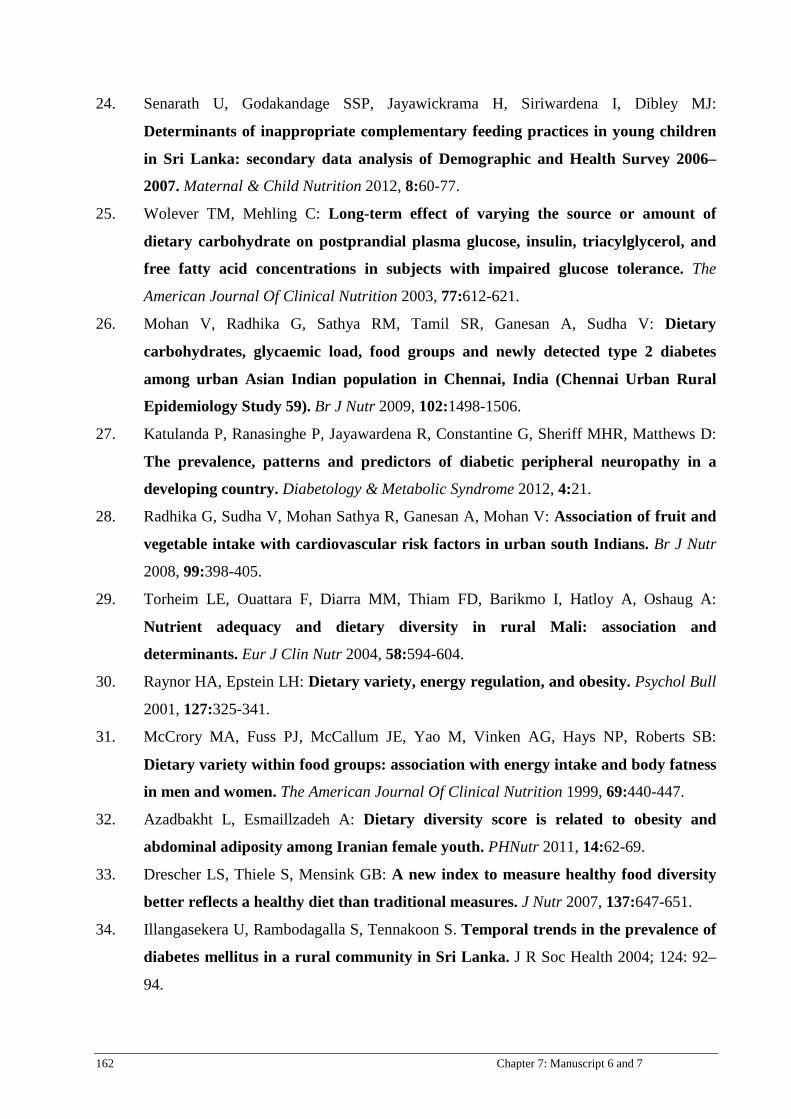
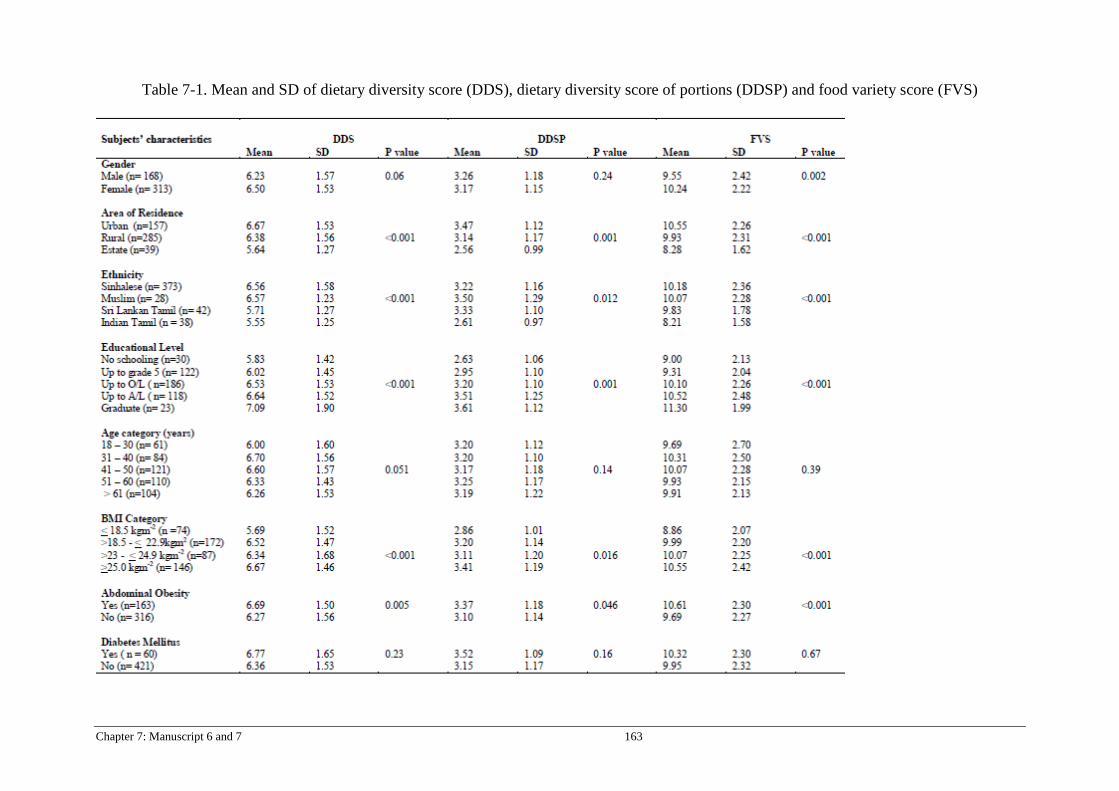
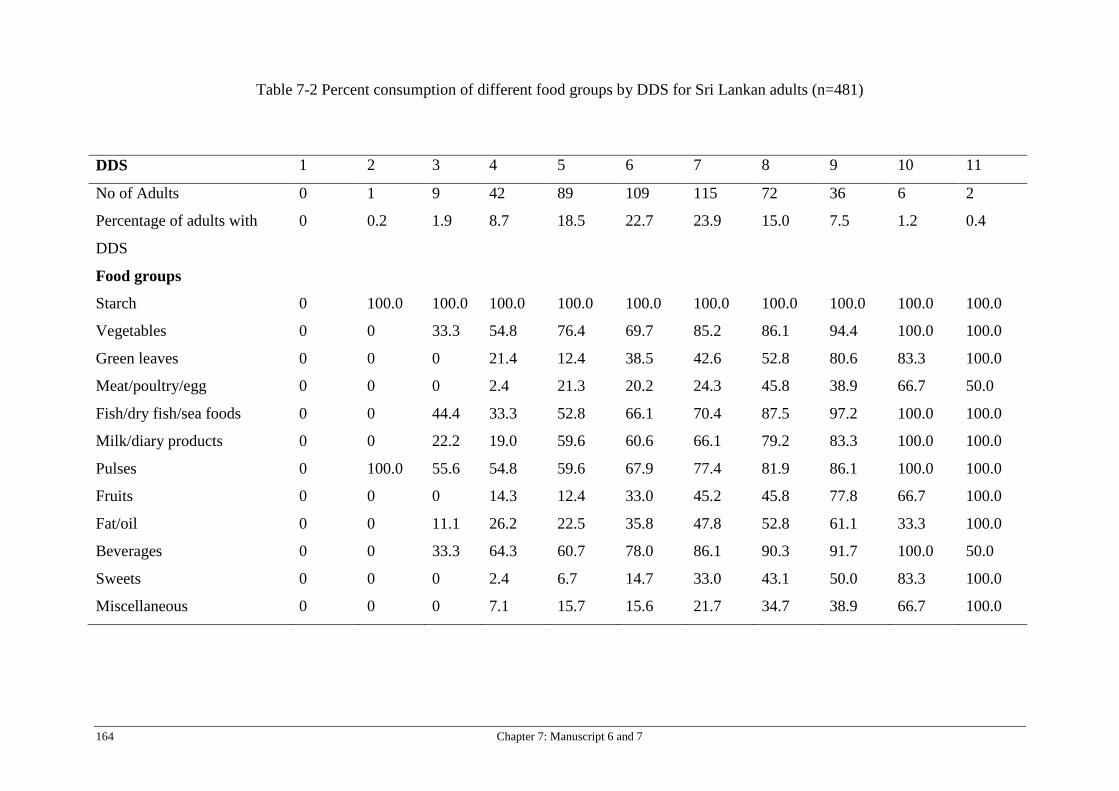
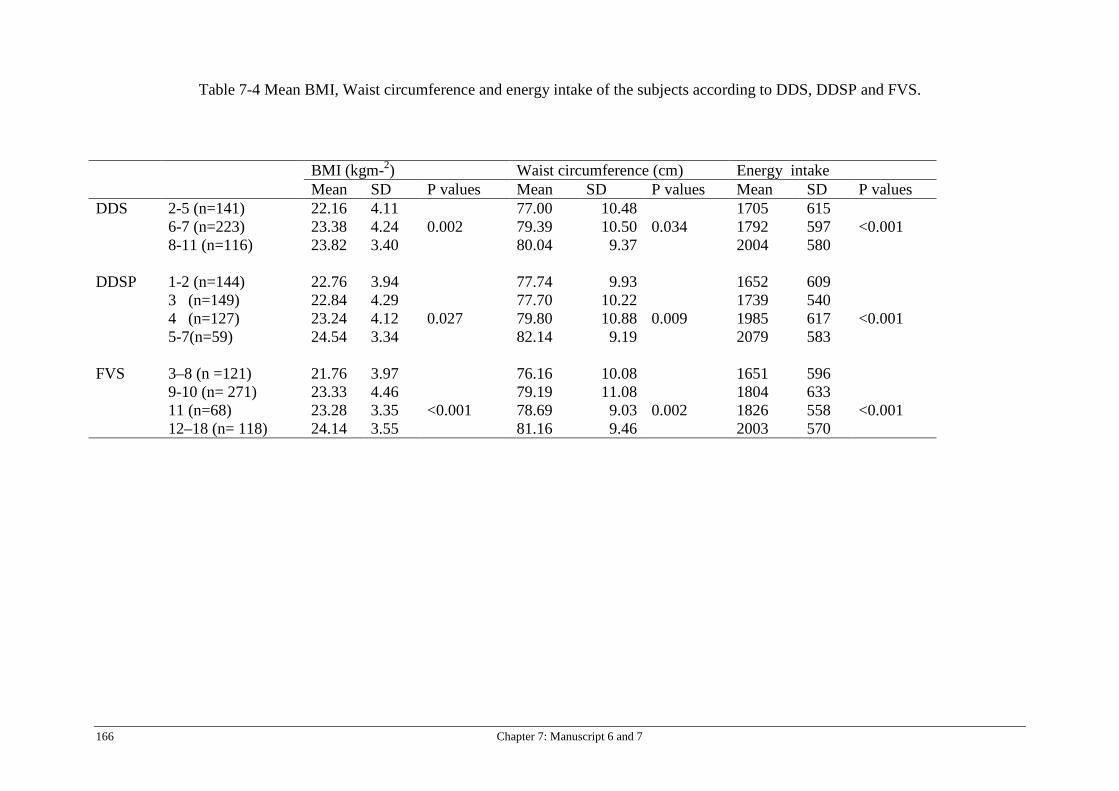


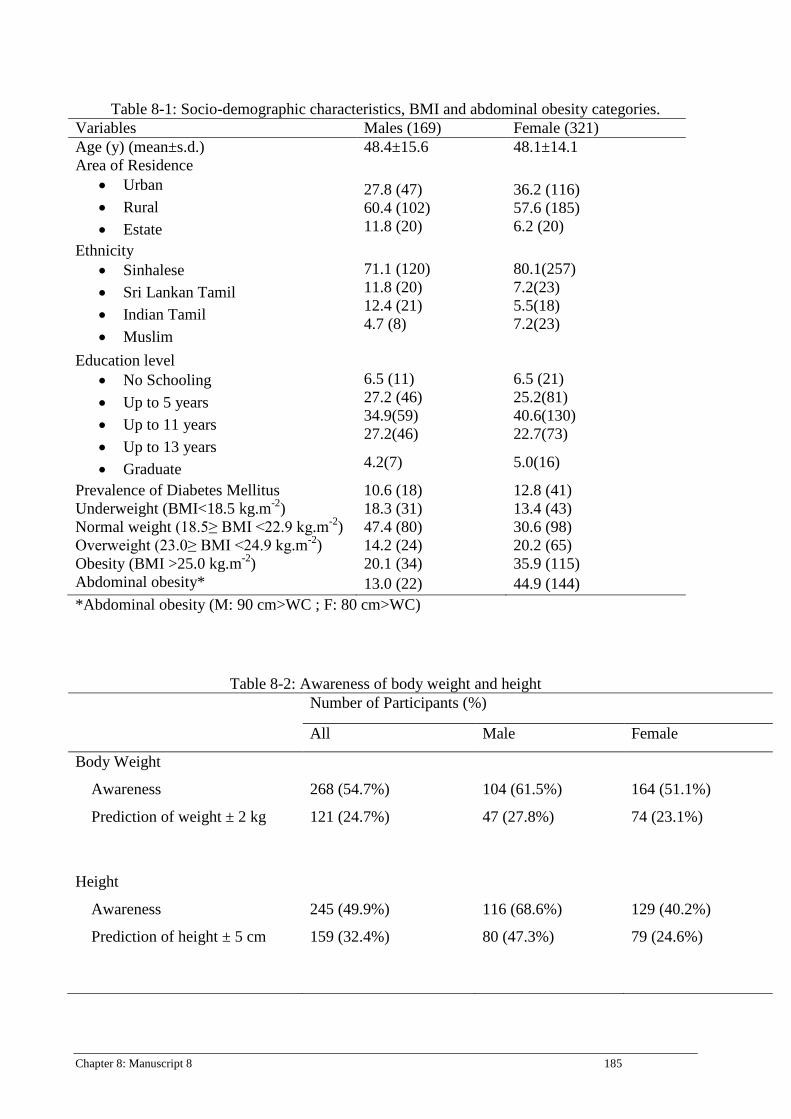
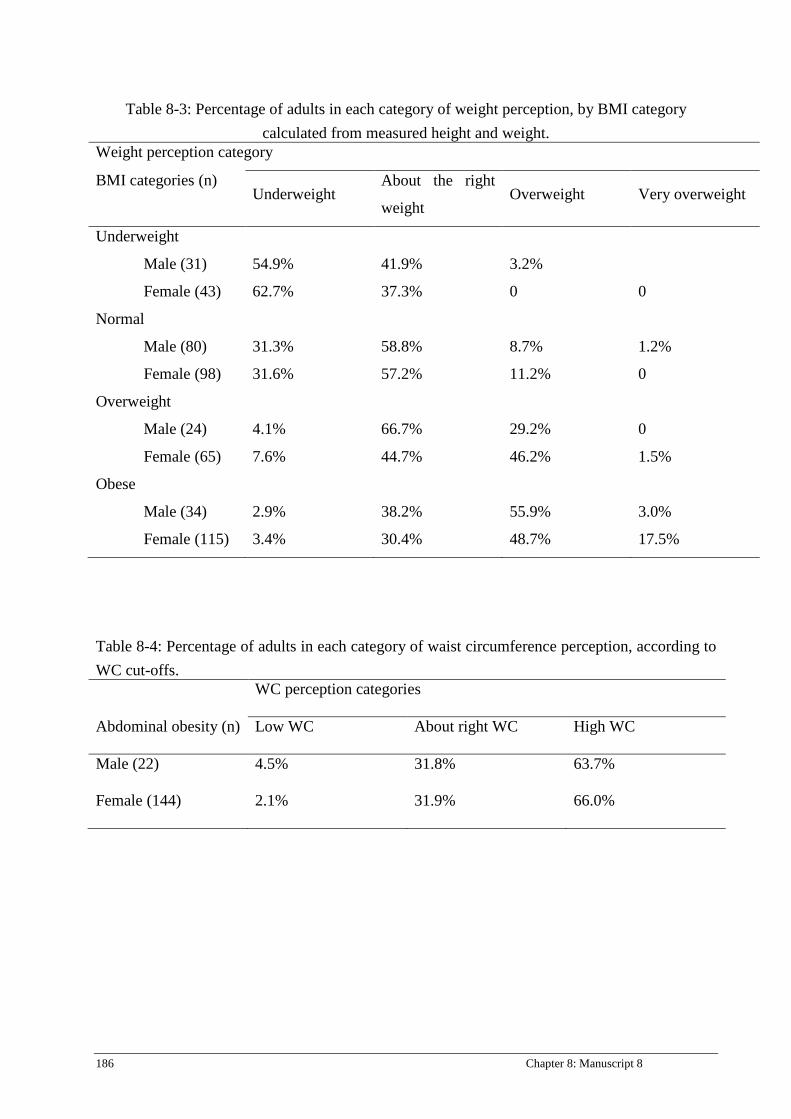


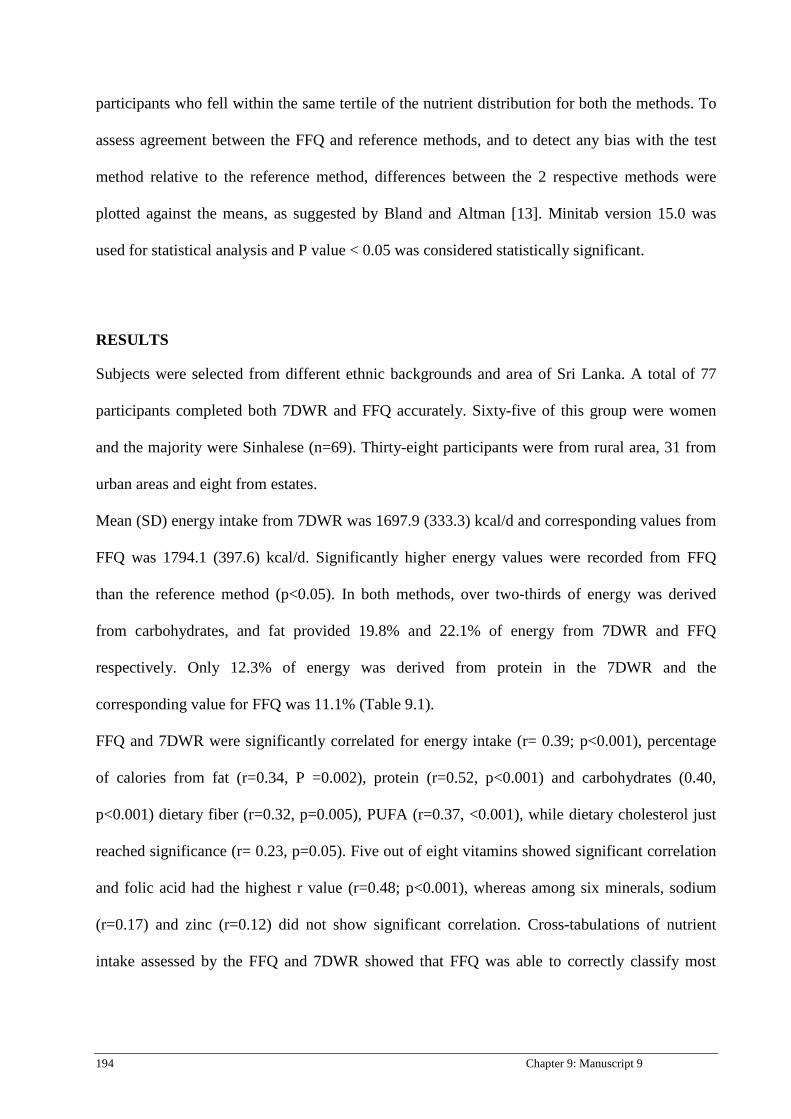
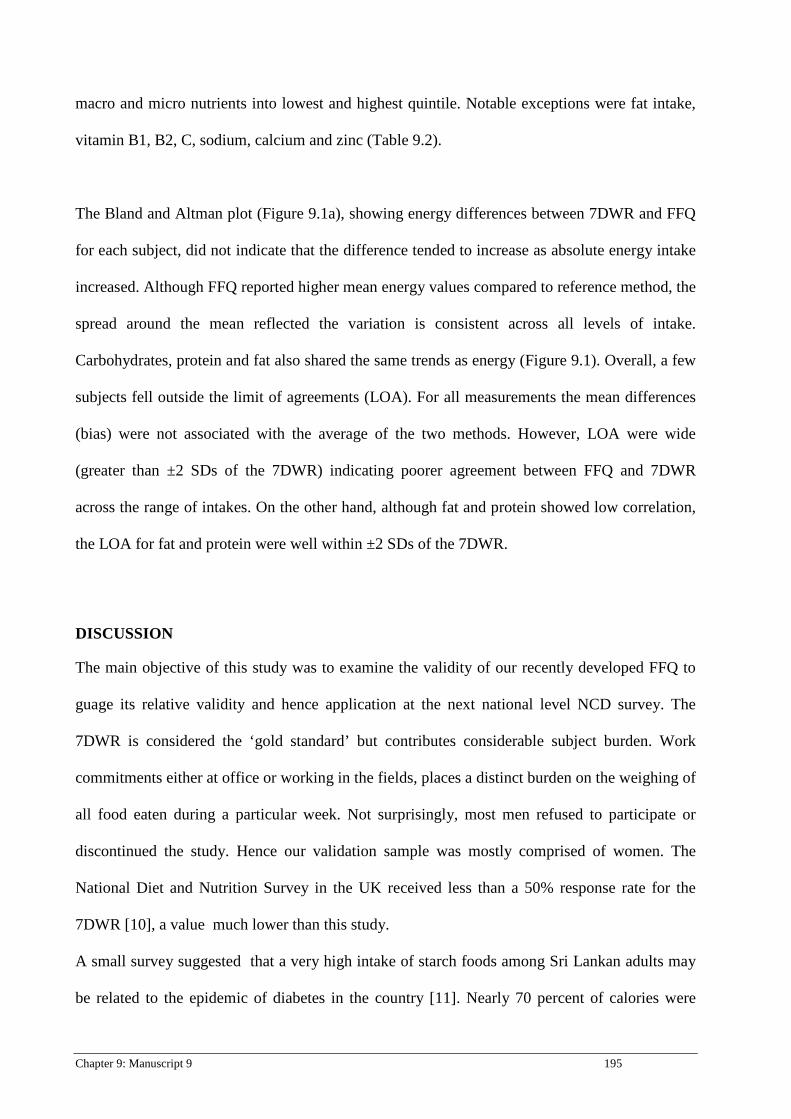
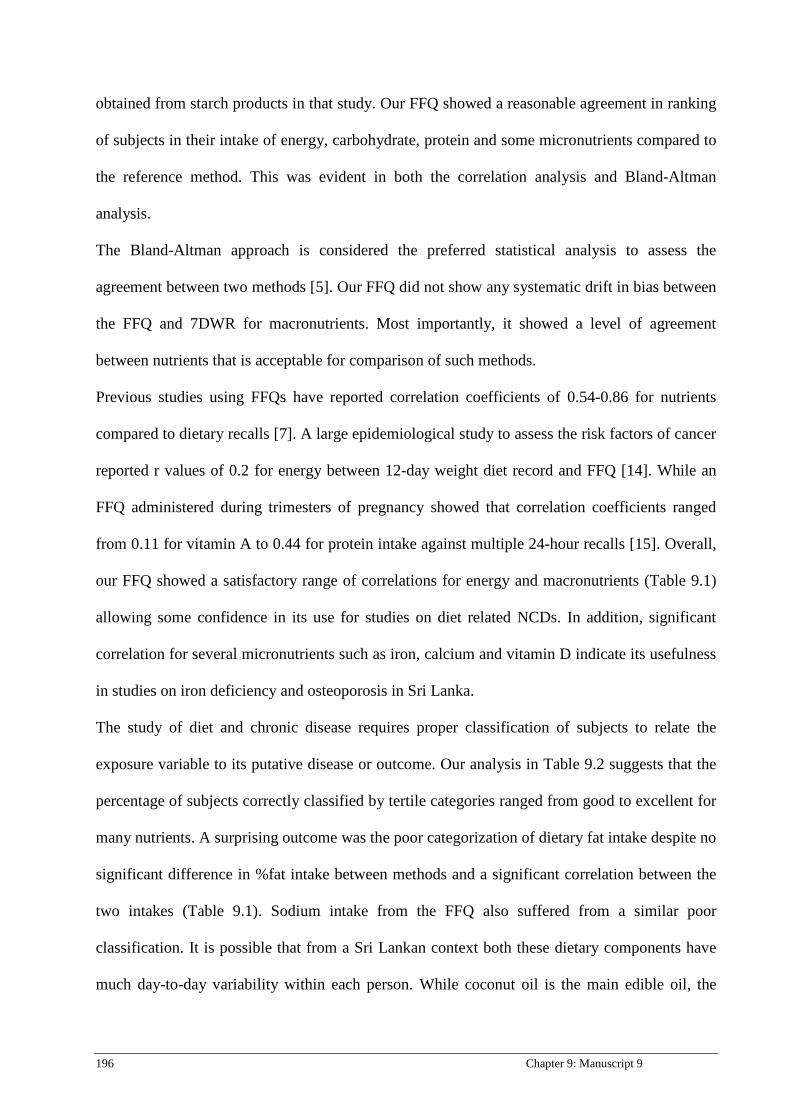
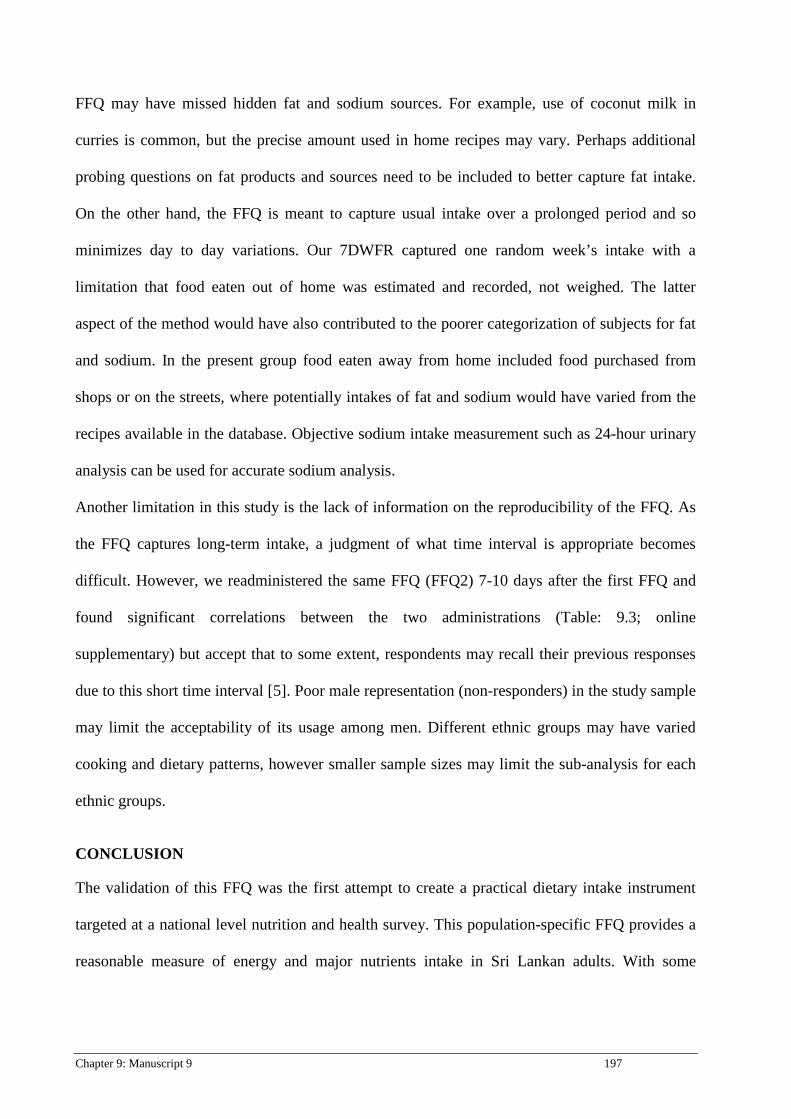


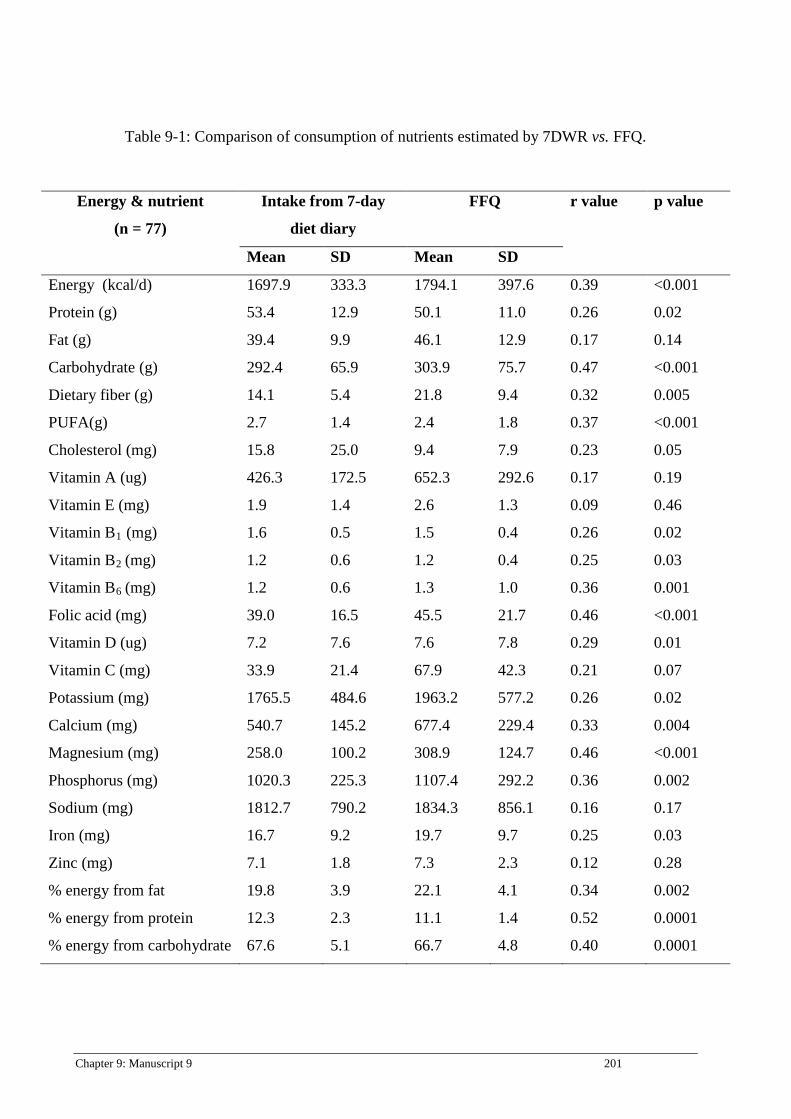
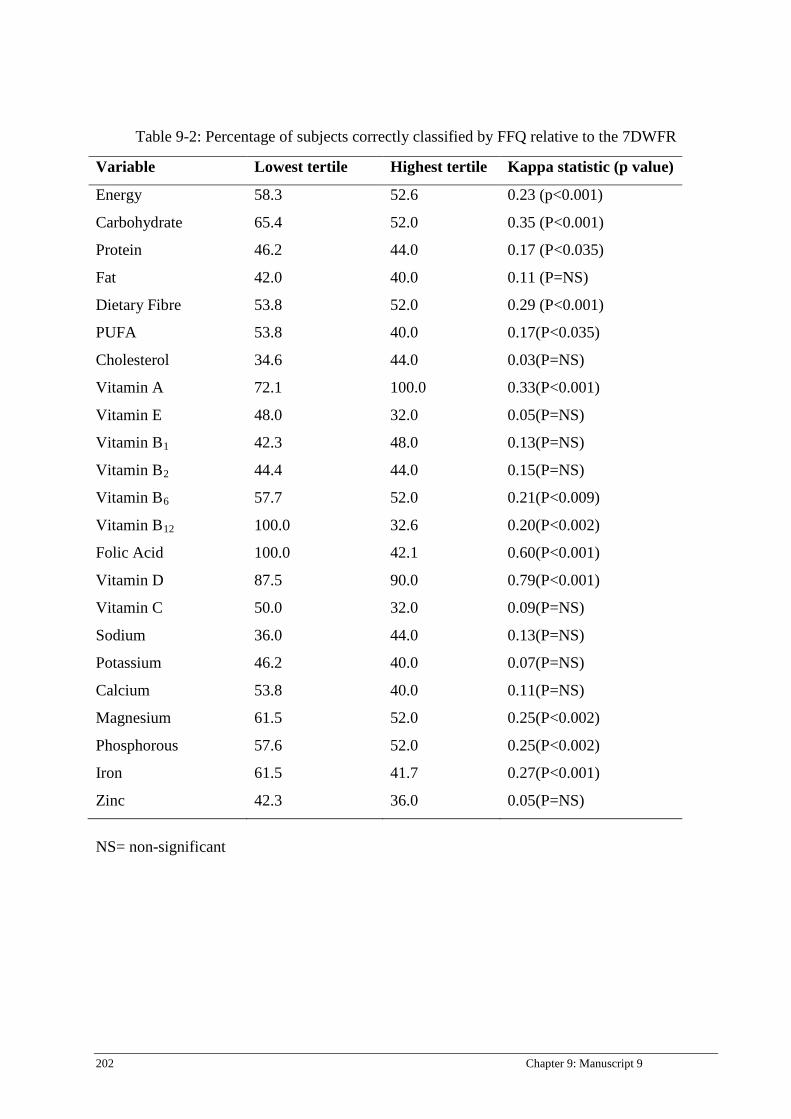
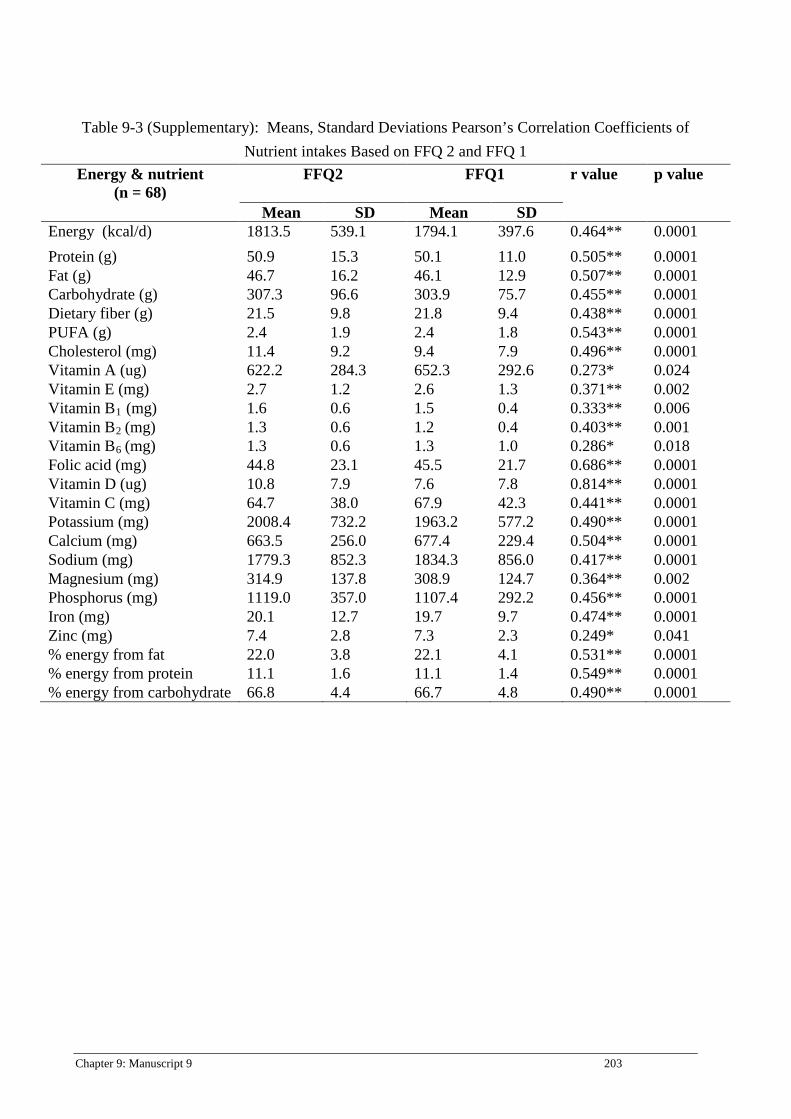
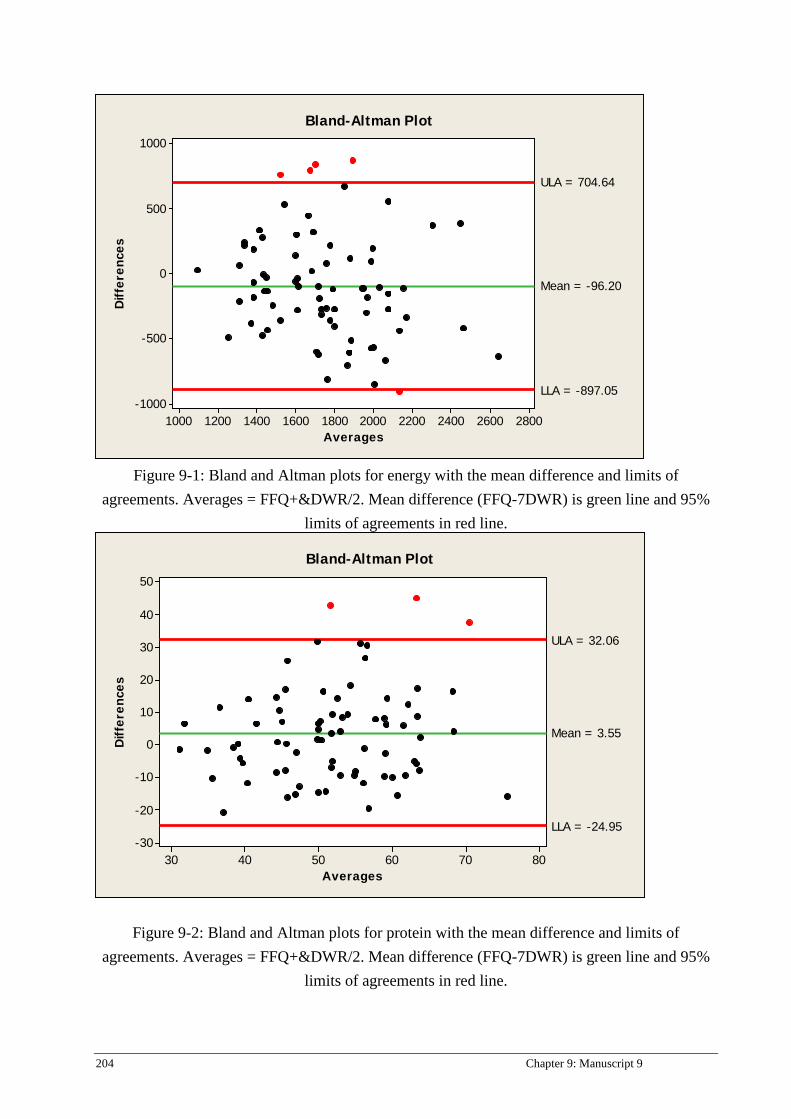
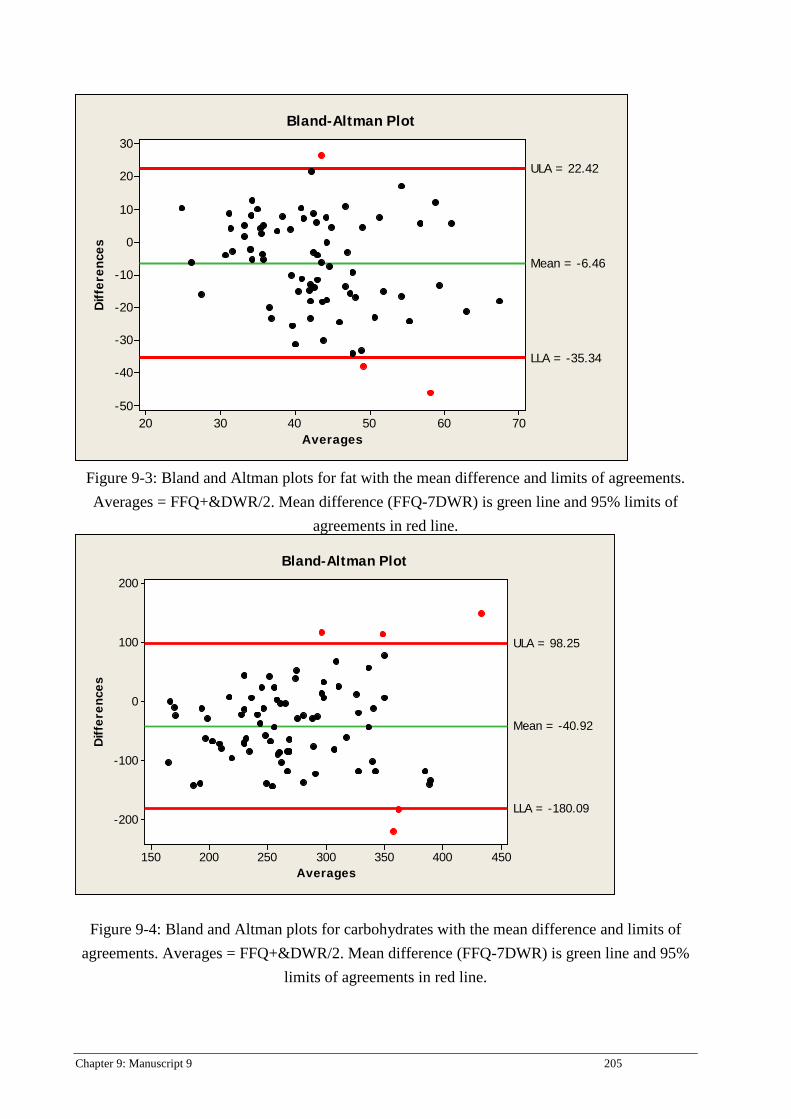



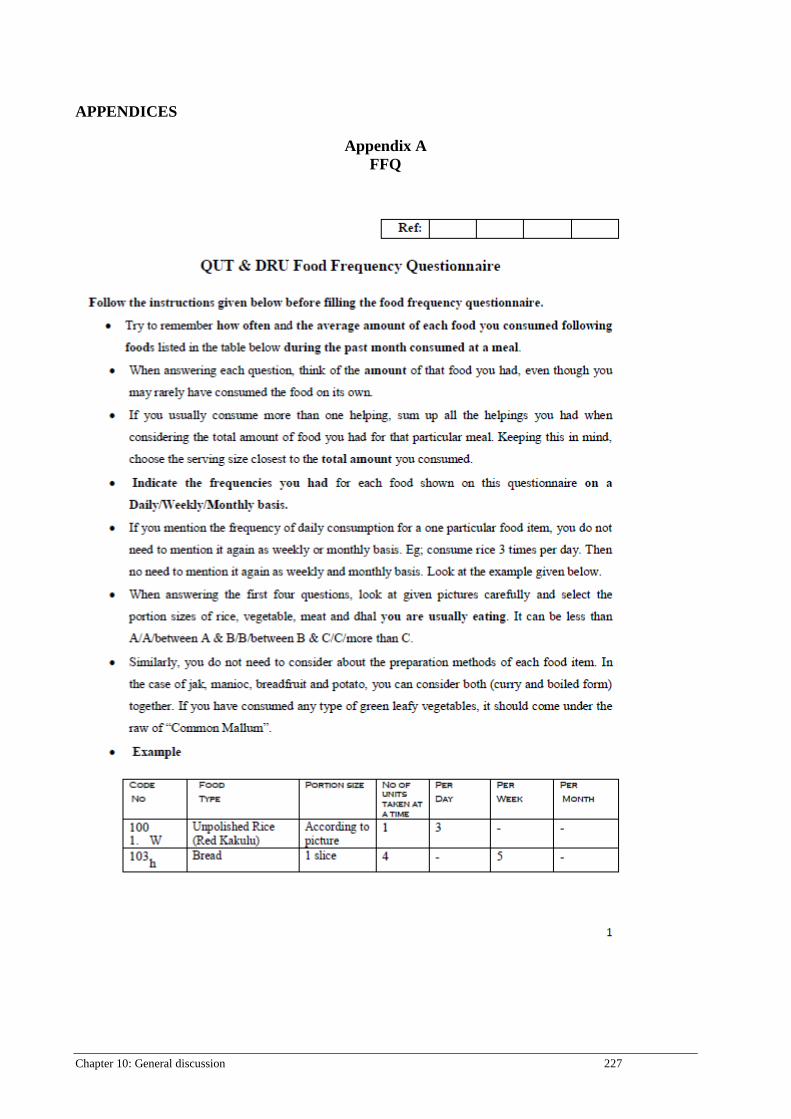
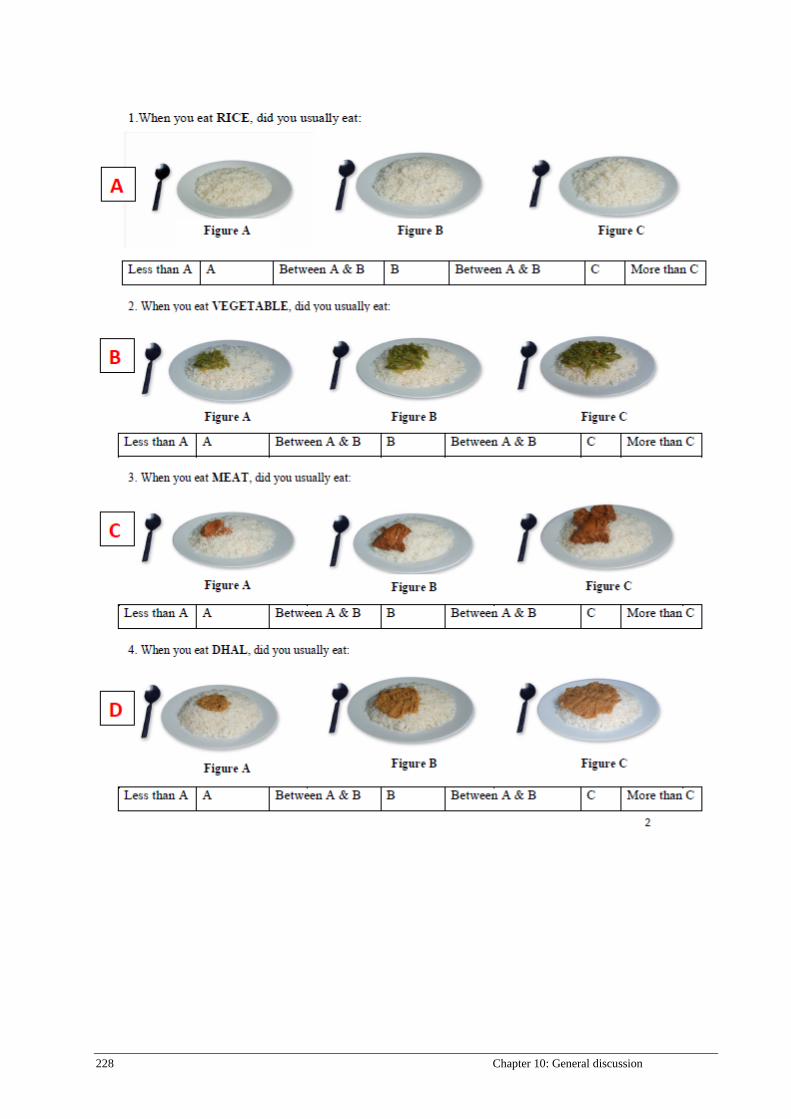
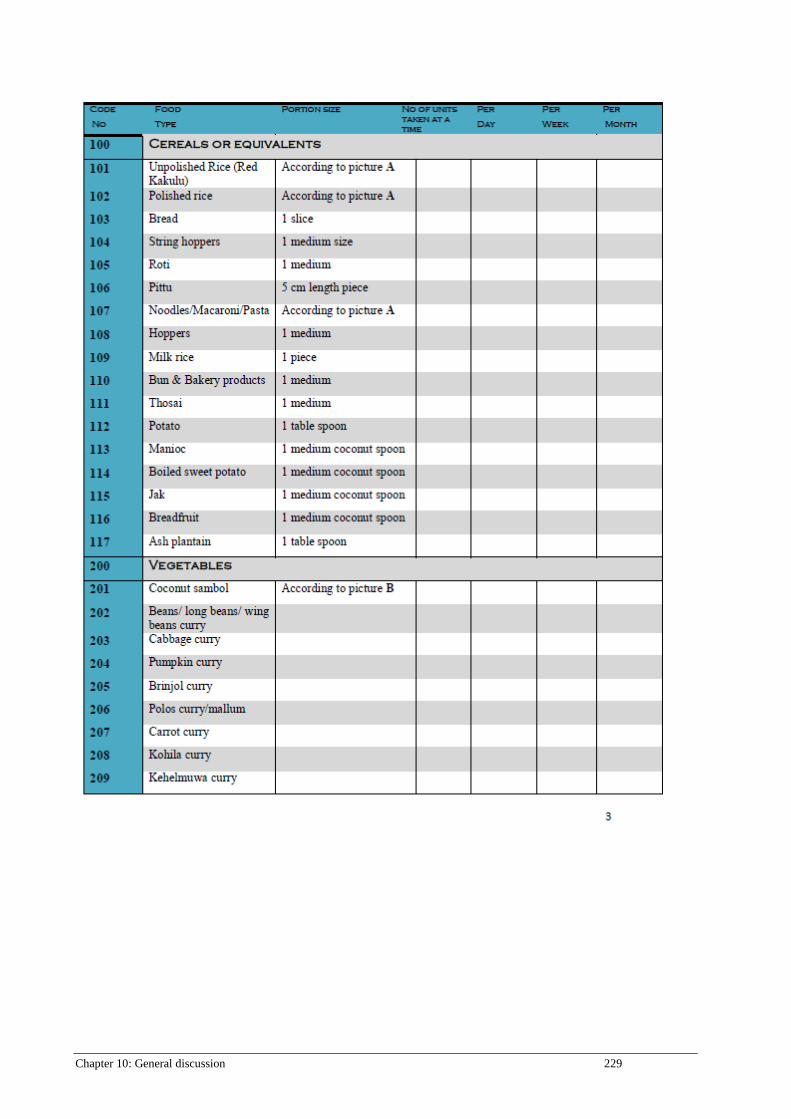
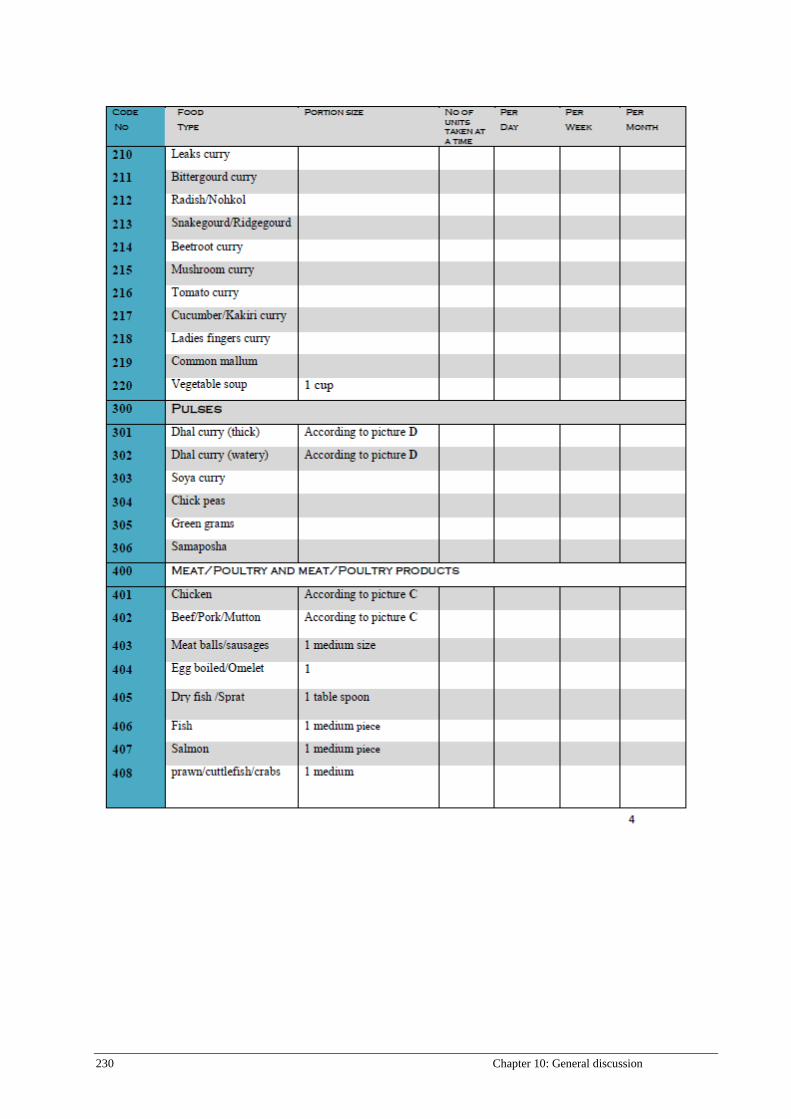
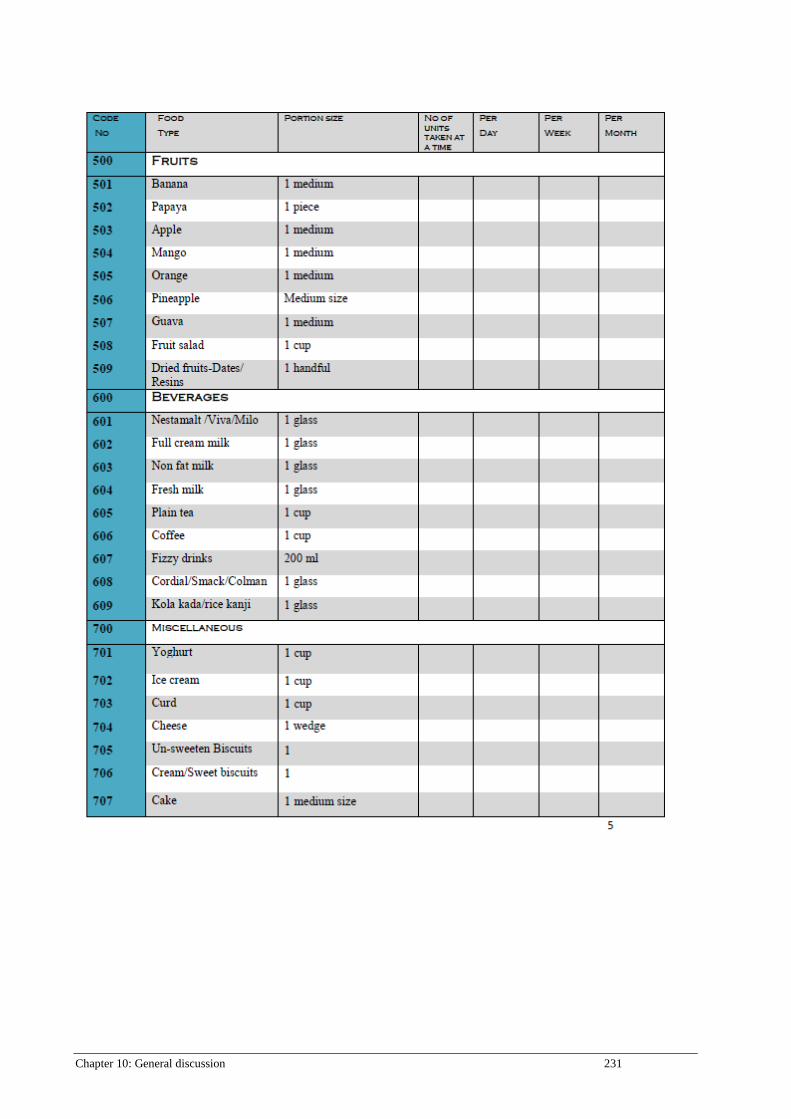
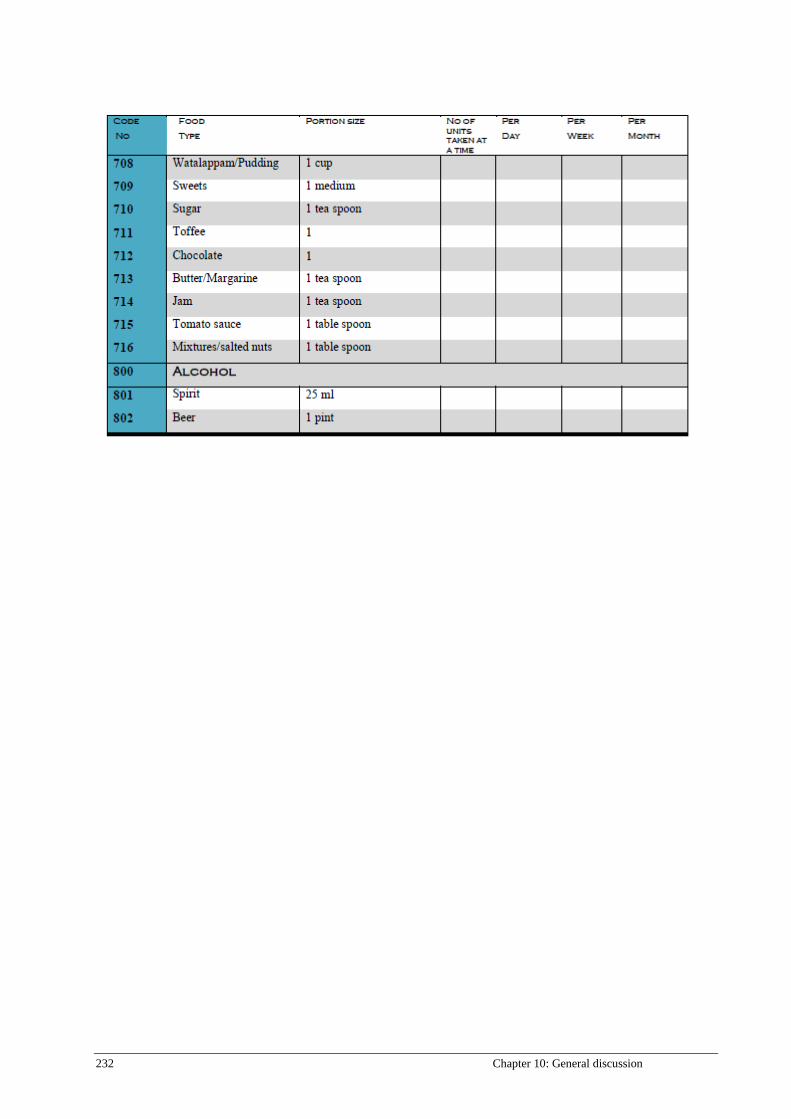


![[Guest Editor, Chandana Jayawardena.] Tourism and (BookFi.org)](https://static.documents.pub/doc/80x56/55cf8e8b550346703b933cde/guest-editor-chandana-jayawardena-tourism-and-bookfiorg.jpg)














