28
- Report No. 135 A Survey of Dishwashing Behaviour in the Northeast:
-
Report No. 135
A Survey of Dishwashing Behaviour
in the Northeast:

THAI-AUSTRALIAN NORTHEAST VILLAGE WATER RESOURCE PROJECT
A SURVEY OF DISHWASHING BEHAVIOUR IN THE NORTHEAST:
THE POTENTIAL FOR HYGIENE EDUCATION
Report No. 135
June 1989
Kevin Hewison Sociologist
Contents
1.0 Summary
2.0 Introduction and Background
3.0 The Study
4.0 Dishwashing Behaviour
4.1 Characteristics of Dishwashers
4.2 Dishwashing Patterns
4.2.1 4.2.2 4.2.3 4.2.4
Times per day Place Washing-up receptacle Washing water source
4.3 Purchase and Use of Soaps and Detergents
4.4 Soaking of Dishes
4.5 Rinsing
4.6 Drying and Storage
5.0 Health and Hygiene Education
5.1 Health and Hygiene Education in Thailand
5 .1.1 5.1.2 5.1.3
Background Health and hygiene education Considerations on increasing the effectiveness of health and hygiene education
a. b. c. d. e. f.
Selection of behaviours Implementati<m Target groups Training Educational materials Evaluation
6.0 Dishwashing and Hygiene Education
7.0 Further Investigation Requirements
8.0 References
Page
1
3
5
6
6
7
7 7 7 8
8
10
12
12
14
14
14 16 17
18 18 19 19 20 20
21
22
23
1.0 SUMMARY
1. This report examines the behaviour of people in Northeastern villages concerning dishwashing, and draws some guidelines for health and hygiene education.
2. The study, based on a small sample, has a number of shortcomings the most important being that it was conducted by survey rather than observation. The results, therefore, are a first-stage in an assessment of dishwashing behaviour and the potential for hygiene education in this area.
3. In examining dishwashing, it was found that it is a task for .women of child-bearing age who have a primary school education this means they are probably basically literate. School-age children seem not to be involved with dishwashing. Most people say that they wash dishes two or three times a day, using groundwater or water from surface supplies. Dishwasing is usually done in the household kitchen area.
4. About half of the respondents reported_that they regularly soaked dishes and other kitchen utensils prior to washing them. Most also reported rinsing their dishes more than once after washing. About half of the respondents stored dishes wet and their dishes were not always dry when used for the next meal. One-third of respondents stored their dishes in conditions which are not necessarily hygienic.
5. When asked about their use of soap for dishwashing, all said they used soap powder, but none use dishwashing detergents Breeze brand soap powder is used by more than half of the respondents, and most buy their soap powder at a village store. The average monthly amount spent on soap for dishwashing is 6.2 baht.
6. A survey of key documents on water supply and sanitation reveals that the 1985 AIT Masterplan gave health and hygiene _education a high priority. This priority has not, however, been conv~rted into either budget or field activities.
7. A number of considerations for increasing the effectiveness of health and hygiene education are then listed under the following headings: selection of behaviour; implementation; target groups; training; educational materials; and evaluation. Recommendations for further investigation are also noted.
1
'-' I
1 • 0 U'\11 fl 'ilt:l f)
1 •
2.
3.
4.
5.
6.
7.
1 1tl'l1umYu~ L Dun 1 1u 1 L ciua Ntln 11m 1"!ciau"Wq~n 1 5:W'llfl 'llh ~ ~1 ~u'l 'UVI~ii'lu'l um fll'l~ 1umm I ~
L Utl'l L wua L nt~1nun11~1'l"l1'U m'1~ L tlun11ri1Vl'U'ilLL'UTV11'lll~~rl1wfun15~mt1Yi'1u~'ll~mt1. ·
LLtl ~ci'll1'VIt11 , I I I I
<f ~ v o ''l o V ~ .e:i '1.1 ~ I 'lJ tJ ~,.3 v .q .o::!i .o::::!VJ i1
L 'Ufl 'l "11 n n 1 5 1'JnH1 tl 'l'VI1fl tl 'U 1 'l"l1n 'il"l 'lfl1"l:W'llfl N'il'Wtl1 'ilfl tJU 1 'l LLtl ~ 'llfl'VIei 1 flUfl!IC'i'ilflfl n 1 5'111 b 'il \J 'lJ 'l1 ,
~1 L tiun 111 'iltl'l il'LLuurl1 1 1"1 LL'VI'U~"l ~ 'l il'n 1 1t1' 'l L n vm 1 1dl 11 .:JtTu Nt:~n 11 ~nH1 ~ 'l L tlu ~u vlfl'U LL 1 n
'llfl .:Jn 1 11..1 1 ~ L ~u L ~ t11nu'Wq ~n 1 1 :wn 1 1~ 1 'l"l1'U LLt:~ ~ il'n tJJ11'W'llfl 'l n 1 1 ~nH1Yl1'Uci'll1'VI til , 'l un 1 1 ~nH1 Yi'1u n 1 1~ 1 'l "11'U 1 Yi'"Wu -i1n 1 1 ~ 1 'l"ll'U L tlu 'l1'U 'llfl 'l N'VlruA .:Ja ~'l u 1 t1 L "'~ ~ruW'u fi ut:~ ~
1J v 1.1 v ,
<i '-'~II. <'j ~ I I J{ ,_, v .o!j <i I G 'l v <i ~ :Wfl11:W1TI'UU5~~:W1'lnH1 ~'l'Vl:W1tlfl11:W11fl'ULV1~1'U5Vl'U'l~fl'il'Wflci:Wfl15 C'f1'UL'iln 'U1tJLjtJ'U'U'U
~ y
'ilLVI~a'U11"1~1~~rl1'UL~t11~fl'lL'Un1j~1'l"l1'U "11nn1jrl1j1"J'WU11'W1nL'll1~1'l"l1'U1''Ut:~~cia'l y
ii .:Jci1:Wflf .:J1 'iltl'l il'J 1u 1'il1t:~Vl~aJ 1"11n LLVI~ 'lJ 1 N 1~u~1 'l ~ LLt:~ ~ 1 'iltJll j n~"l ~~1 'l"ll'U'l uu ~ L 1ru I
~Ltlu~a'lflf1n1t~'luu1u I I I
~ .ct tr!VJ 'iJV VJ 'lJ I ')" .q V I
1..1 1 ~:W1rufl HVI'U 'l 'llfl 'l I\! 'VI b 'il1Un 1 5cifJU~ 1:1-1 b 'il 51 tl 'l1'U 11 b 'iltllln 1l LLtn'W1 n L 'll1"' ~ LL~"l1'U ~1 :W LLtl ~ I 'l ~ 1~'¥') V I q o V 'lJ I 'U
L fljfl.:J ·ll b'Um1nfl'U'VI"l~'VI1n11t:~1'l LLt:~~rl1'ULVI~"l~~1'l"l1'U~1JJYl1tiU1 L 1..1~1mnn11VIU'lflf'l I I I I
v .., G ~ ~ ..,<i G v <i<i.., d 'i "' I 'l" v Vltl'l"l1ntl1'lLC'i1"! 1..15~:W1CUflj'JVI'U'l'llfl'lN'VI~nciaU~1:WLnU"l1'U'VI'U'VI'VItl1'lLC'ij"Jb'iltlb:W5fl VIL~'l
y "
L ~ m1au LLt:~ ~ 'l uu 1 'l flf 'l"l1'U~ 1 :w~ ti' 'l fl 'l L J t~na ~ L ~au 1:1-11 'l iil un 1 j full 1 ~'VI1'Ufl1Vl1 j ~a ~a111 " I I
1..1 j ~JJ1ru'VIU 'lL 'Uci1:W'llfl 'l N~nciaU~1JJ L flU"l1'U~1:W'llfl 'l'W1n L 'll1 'l 'ULLUu~1~~nci'll~nHru~ U\J \J 1
L~fl~1JJL~tl1nun11'lil'ciu'lun15~1'l"l1'U 'VInfluuan11'lil'N'l~n~an'lun1j~1'l"l1'U 1~~'lfl1'lil' " , 'lJ I I I I
u1tJ1Vl;aN~1lKru1m'lil'rl1Vlfu~1'l"l1'ULt:~tl N'l~n~an~~au~ci~flu'lil'Lnun11fl~'l'Vlu'l'lla'l~1u1u I
Ni1~ nciau ~ 1 :w LLtl ~rl1'U:IJ1 n n"' ~~f) 1\1 'l ~m1anm tiL 'U f 1'U 'll1 tl 'llfl 'l 'l 'UVI~U 1'U ~1 'l il'~ 1 tJ'C11Vl fu ~f) " y "
N'l~n~an L ~a'liilun11~1'l"l1'U~1JJ'lln L ~aut:~~1..lj~JJ1ru 6. 2 U1'VI I , I I I I 11
<f _q,j u ~ I 4 <f .c:f u V o "'=\ d I 'l 4 L:Wfl1Jj1"JC'iflULflnC'f1j'V1~1flill~'lntl11~'JLjfl'JLntl1nUn15"l'il'Vl1'U1LLtl~n15C'i'll1J1U1tln'WU11 'UU
~ , 2524 1 mJ LLN'ULL~U'VI~'l~'il'l'h 1 'ilti'C'I~ 1U'U L 'VIfl1 'U 1 tl~ LLll 'l L fl L ~tl ~'11 YlL ~m 1:W'C11rlqJa'UYlU LL 1n LLfl
n 11 ~nH1 Yl1'U~'ll~nH1 LLt:~~~'ll1'VIm a~1 '11 1n111:Wm 1:wrl1rl'~'l ~1 Y1 fun 1 j~"J1 1ru1..Y'ilci1 11111 'l
Yi'1un11 L 1u'Vl;arl'l L ci~:w'l~n"lnn:w'luciu1JJLL~a~1'l'l'il
Yl'ltTtl~'l~n15Lci'Ufl~flfl1j~"J15ru1an'Vlt:~1tlllj~L~tl L~flL~:IJ1..lj~~'VITINtl'llfl'ln11~nH1Yl1'UC'i'll~nH1 '
n11L~an~nH1'Wq~nj5:W n11~1Luun1j n~:w <\ 'l tJV V I t.1 I VJ ~~ LLt:~~C'i'll1'VIt11J11tl 1l'Vl1'llfl1l1'l ~ 'il'l'llfltll'Urlfl , L u 1Vl:w1 t1 n 1 j Nnau jJJ 1'ci'ila1..ln j(ifln 'l Yi'1un 1 1~nH1 LLt~~n 1 jU j ~ L ~tiNt:~ j 1:w« .:J1 rul.zJm ciumm~ , ,
2
2.0 INTRODUCTION AND BACKGROUND
The Thai-Australian Northeast Village Water Resources Project (NEVWRP) has, for some time, been conducting activities directed toward gaining an understanding of water user behaviour within the village household. The small survey reported here was carried out as a part of this wider agenda.
Dishwashing behaviour may appear, at first glance, to be a rather mundane matter, with but a marginal impact on health. Studies in Thailand and elsewhere have suggested, however, that household activities such as personal hygiene (e.g.· handwashing) and dishwashing are significant for health.
Feachem (1984: 46 7) argues that "all of the pathogens that are known to be major causes of diarrhoea in many countries, are transmitted primarily or exclusively by faecal-oral route". This indicates the potential significance of hygiene education and behaviour programmes in reducing the chances for infection by direct faecal-oral transmission of pathogens. Any attempt to interrupt this route must, however, be based on reliable and adequate supplies of water and improved sanitation facilities.
Faecal-oral transmission can be either water-borne, direct, or food-borne. Studies which have targeted various hygienic behaviours with education programmes are designed to reduce, directly or indirectly, faecal-oral transmission of pathogens (e.g. Stanton and Clemens, 1987; and S.tanton, Clemens, Khair, et. al., 1987). These studies have tended to focus on handwashing, food preparation, and rubbish and faeces removal.
While these areas are also seen to be important for Northeastern Thailand, a recent study by Pinfold (1988), conducted with NEVWRP, has also indicated the potential importance of dishwashing in the faecal-oral transmission of pathogens. Pinfold's intensive observations of ten households not only identified water user behaviour patterns, but also asaessed the levels of bacteriological, contamination of the various containers of water kept in the household. His findings are summarised in Table 1:
3
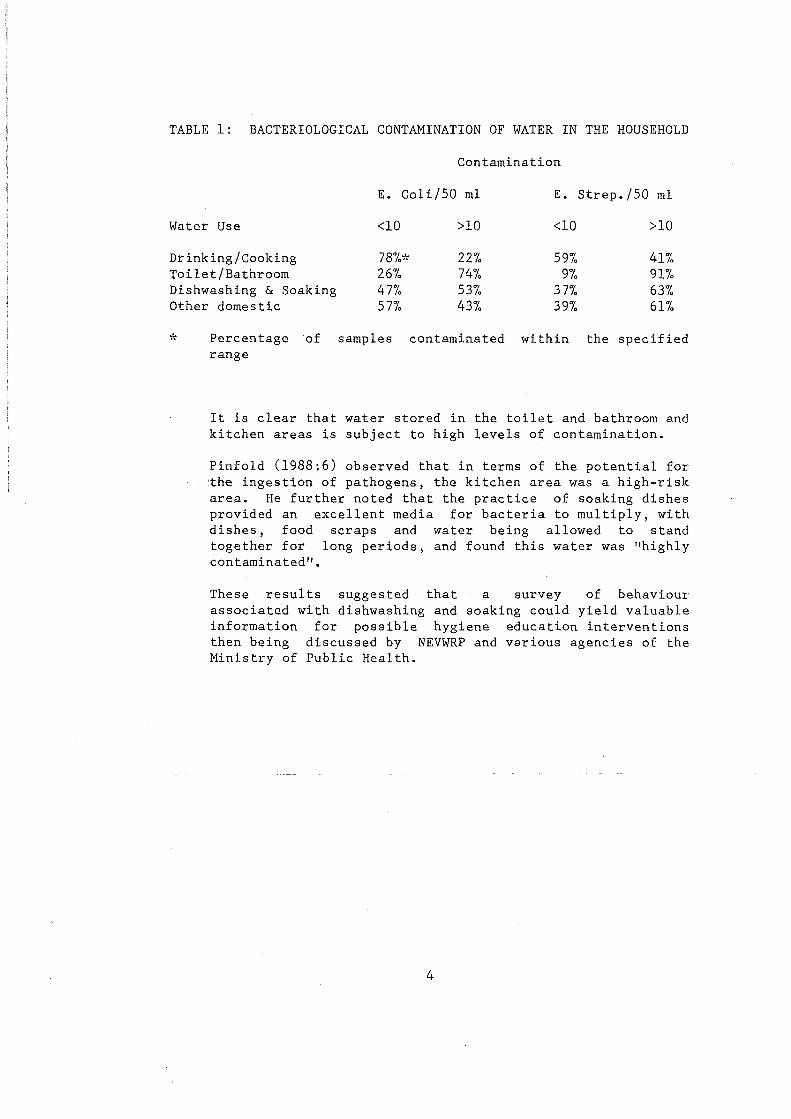
TABLE 1: BACTERIOLOGICAL CONTAMINATION OF WATER IN THE HOUSEHOLD
Contamination
E. Coli/50 ml E. Strep./50 ml
Water Use <10 >10 <10 >10
Drinking/Cooking 78%* 22% 59io 41io Toilet/Bathroom 26% 74% 9io 91io Dishwashing & Soaking 47% 53io 37% 63io Other domestic 57% 43% 39io 61%
* Percentage of samples contaminated within the specified range
It is clear that water stored in the toilet and bathroom and kitchen areas is subject to high levels of contamination.
Pinfold (1988:6) observed that in terms of the potential for the ingestion of pathogens, the kitchen area was a high-risk are~. He further noted that the practice of soaking dishes provided an excellent media for bacteria to multiply, with dishes, food scraps and water being allowed to stand together for long periods, and found this water was "highly contaminated".
These results suggested that a survey of behaviour associated with dishwashing and soaking could yield valuable information for possible hygiene education interventions then being discussed by NEVWRP and various agencies of the Ministry of Public Health.
4
3.0 THE STUDY
The selected study instrument was a questionnaire survey. While it is recognised that direct observation can provide better results (Stanton, Clemens, Aziz and Rahman, 1987), it was felt that for initial NEVWRP purposes, a questionnaire was sufficient. NEVWRP wished to have data for the following:
(i) To collect some basic information on dishwashing behaviour from a range of locations in the Northeast.
(ii) To gather data relating to detergent marketing potential for possible discussions with advertising agencies and detergent manufacturers.
In other words, the Project information to allow for basic knowledge.
was attempting to gather enough discussions from a position of
In total, 55 questionnaires were completed, representing approximately five percent of households in each of ten selected villages in ten provinces of the Northeast. The provinces selected were: Loei, Khon Kaen, Sakol Nakhon, Surin, Udorn Thani, Srisaket, Nongkhai, Nakhon Ratchasima, Mukdahan and Chaiyaphum.
The reasons for selecting these provinces, and the particular villages in each, was not based on any statistical methodology. Rather, using Project experience, an attempt was made to get a geographic spread of provinces, and to have a range of ethnic groups represented. Thus, provinces were chosen . from the upper, central and lower Northeast, and with ethnic groups of Khmer, So, Lao, and Thai-Korat represented. It was hoped that such a range would provide an "average" of practices across the Northeast and its different ethnic groups. No attempt was made to draw differences between them on cultural grounds, however (with one exception, noted below). The villages chosen were all reasonably small, so that the survey could be completed by one field assistant. This field assistant was a male, while the respondents were mainly women. The survey was completed during the wet season.
The data presented below, then, represents an to understand the behaviour patterns for significant yet mundane household activity.
5
initial effort a potentially
4.0 DISHWASHING BEHAVIOUR
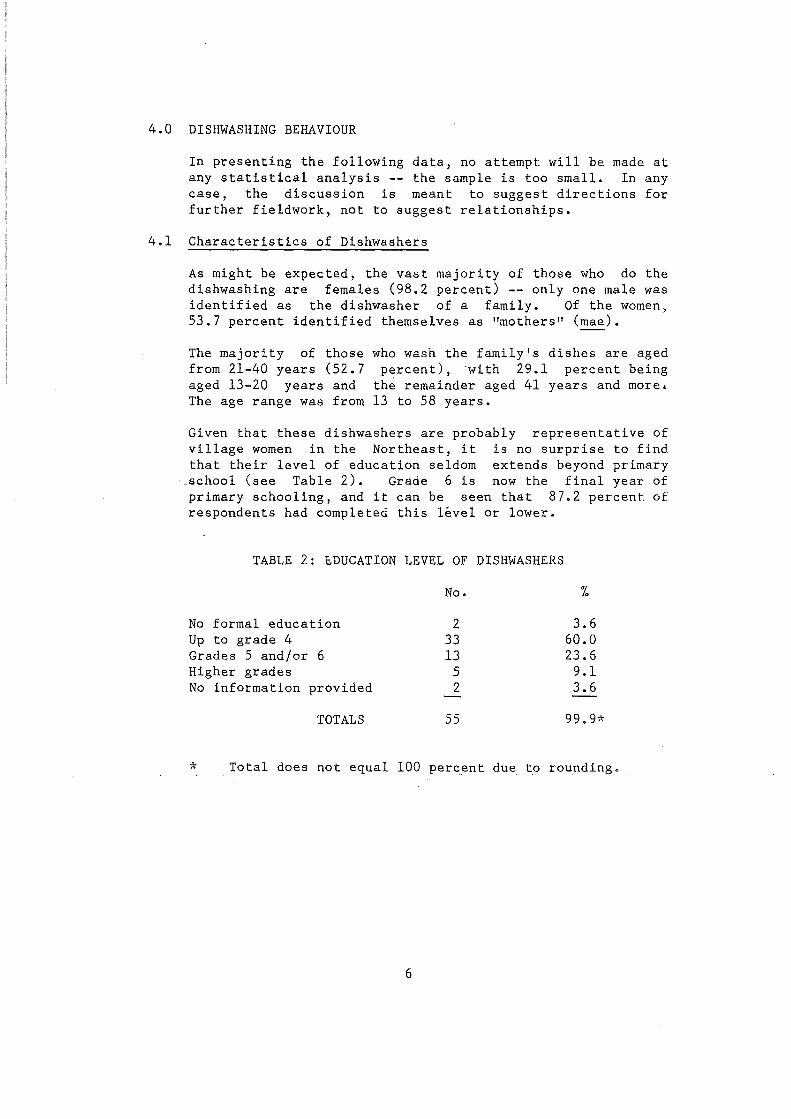
In presenting the following data, no attempt will be made at any statistical analysis -- the sample is too small. In any case, the discussion is meant to suggest directions for further fieldwork, not to suggest relationships.
4.1 Characteristics of Dishwashers
As might be expected, the vast majority of those who do the dishwashing are females (98.2 percent) -- only one male was identified as the dishwasher of a family. Of the women, 53.7 percent identified themselves as "mothers" (mae).
The majority of those from 21-40 years (52.7 aged 13-20 years and The age range was from
who wash the family's dishes are aged percent), with 29.1 percent being
the remainder aged 41 years and more. 13 to 58 years.
Given that these dishwashers are probably representative of village women in the Northeast, it is no surprise to find that their level of education seldom extends beyond primary
.school (see Table 2). Grade 6 is now the final year of primary schooling, and it can be seen that 87.2 percent of respondents had completed this level or lower.
TABLE 2: BDUCATION LEVEL OF DISHWASHERS
No formal education Up to grade 4 Grades 5 and/or 6 Higher grades No information provided
TOTALS
No.
2 33 13
5 2
55
3.6 60.0 23.6 9.1 3.6
99.9*
* Total does not equal 100 percent due to rounding.
6
4.2 Dishwashing Patterns
4.2.1 Times per day
4.2.2
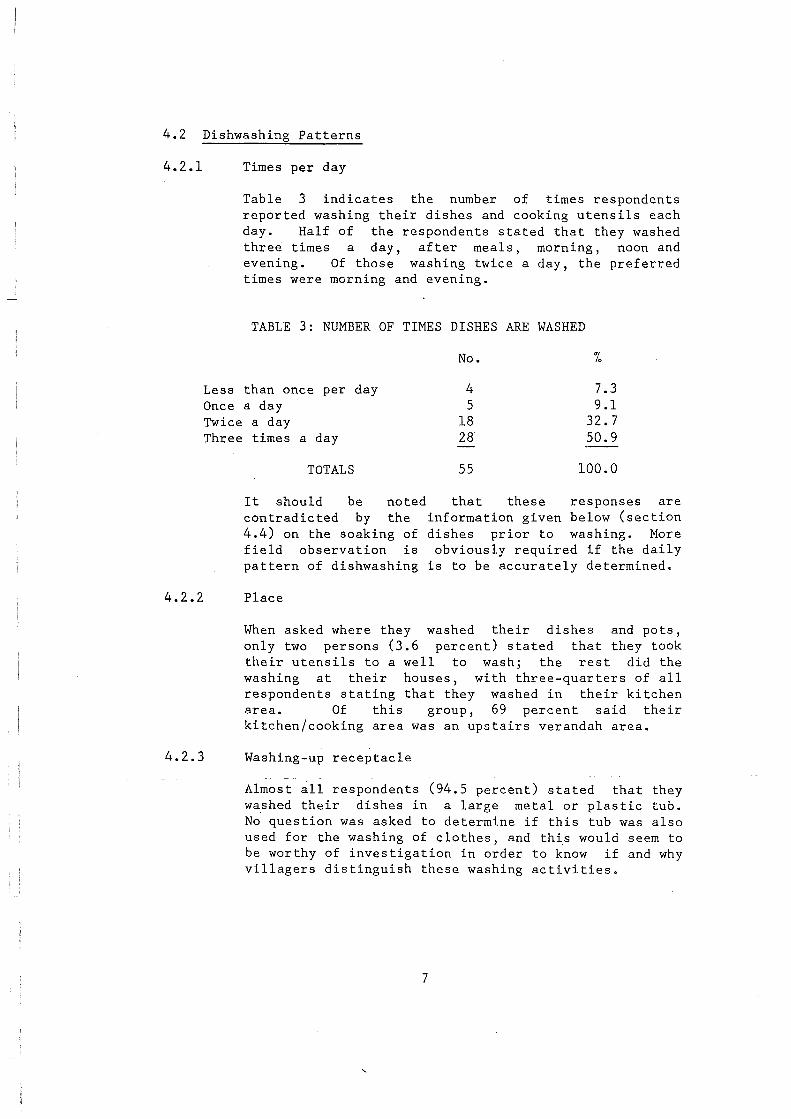
Table 3 indicates the number of times respondents reported washing their dishes and cooking utensils each day. Half of the respondents stated that they washed three times a day, after meals, morning, noon and evening. Of those washing twice a day, the preferred times were morning and evening.
TABLE 3: NUMBER OF TIMES DISHES ARE WASHED
Less than once per day Once a day Twice a day Three times a day
TOTALS
It should be noted contradicted by the 4.4) on the soaking of field observation is pattern of dishwashing
Place
No.
4 5
18 28
55
7.3 9.1
32.7 50.9
100.0
that these responses are information given below (section dishes prior to washing. More obviously required if the daily
is to be accurately determined.
When asked where they washed their dishes and pots, only two persons (3.6 percent) stated that they took their utensils to a well to wash; the rest did the washing at their houses, with three-quarters of all respondents stating that they washed in their kitchen area. Of this group, 69 percent said their kitchen/cooking area was an upstairs verandah area.
4.2.3 Washing-up receptacle
Almost ~11 respondents (94.5 percent) stated that they washed their dishes in a large metal or plastic tub. No question was asked to determine if this tub was also used for the washing of clothes, and th~s would seem to be worthy of investigation in order to know if and why villagers distinguish these washing activities.
7
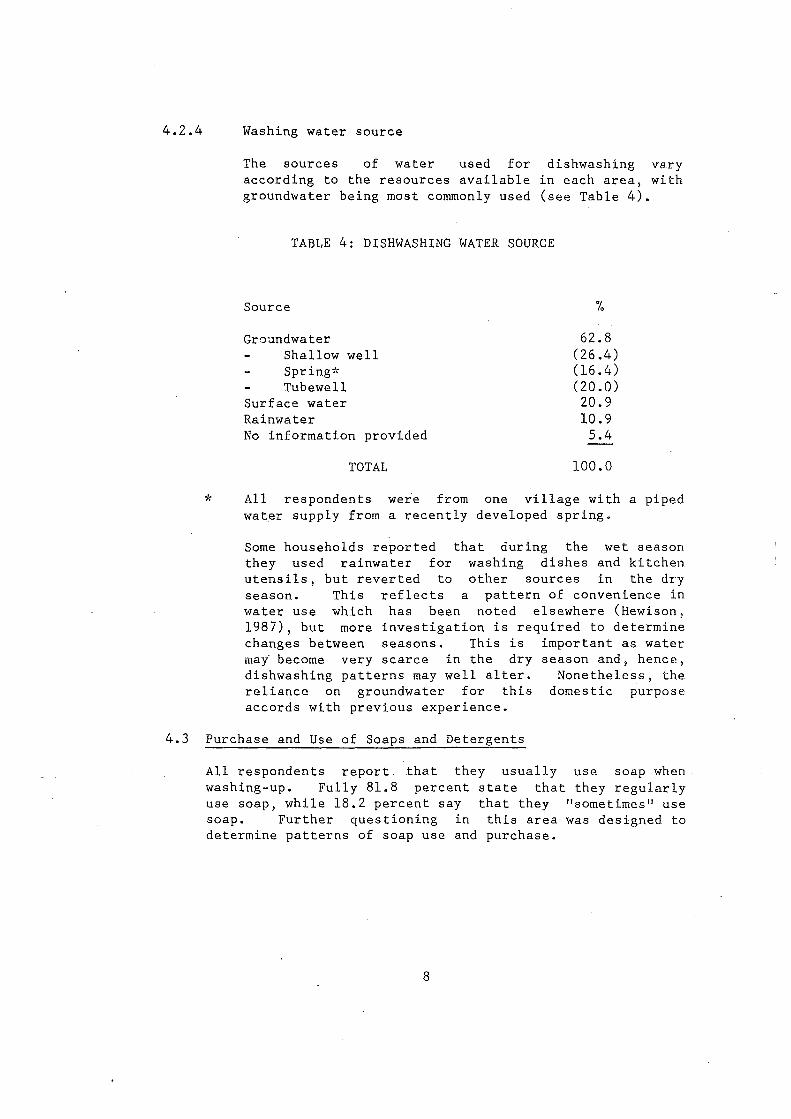
4.2.4 Washing water source
The sources of water used for dishwashing vary according to the resources available in each area, with groundwater being most commonly used (see Table 4).
TABLE 4: DISHWASHING WATER SOURCE
Source
Groundwater Shallow well Spring* Tub ewell
Surface water Rainwater No information provided
TOTAL
%
62.8 (26.4) (16. 4) (20.0) 20.9 10.9
5.4
100.0
* All respondents were from one village with a piped water supply from a recently developed spring.
Some households reported that during the wet season they used rainwater for washing dishes and kitchen utensils, but reverted to other sources in the dry season. This reflects a pattern of convenience in water use which has been noted elsewhere (Hewison, 1987), but more investigation is required to determine changes between seasons. This is important as water mai become very scarce in the dry season and, hence, dishwashing patterns may well alter. Nonetheless, the reliance on groundwater for this domestic purpose accords with previous experience.
4.3 Purchase and Use of Soaps and Detergents
All respondents report that they usually washing-up. Fully 81.8 percent state that use soap, while 18.2 percent say that they soap. Further questioning in this area determine patterns of soap use and purchase.
8
use soap when. they regularly
"sometimes" use was designed to
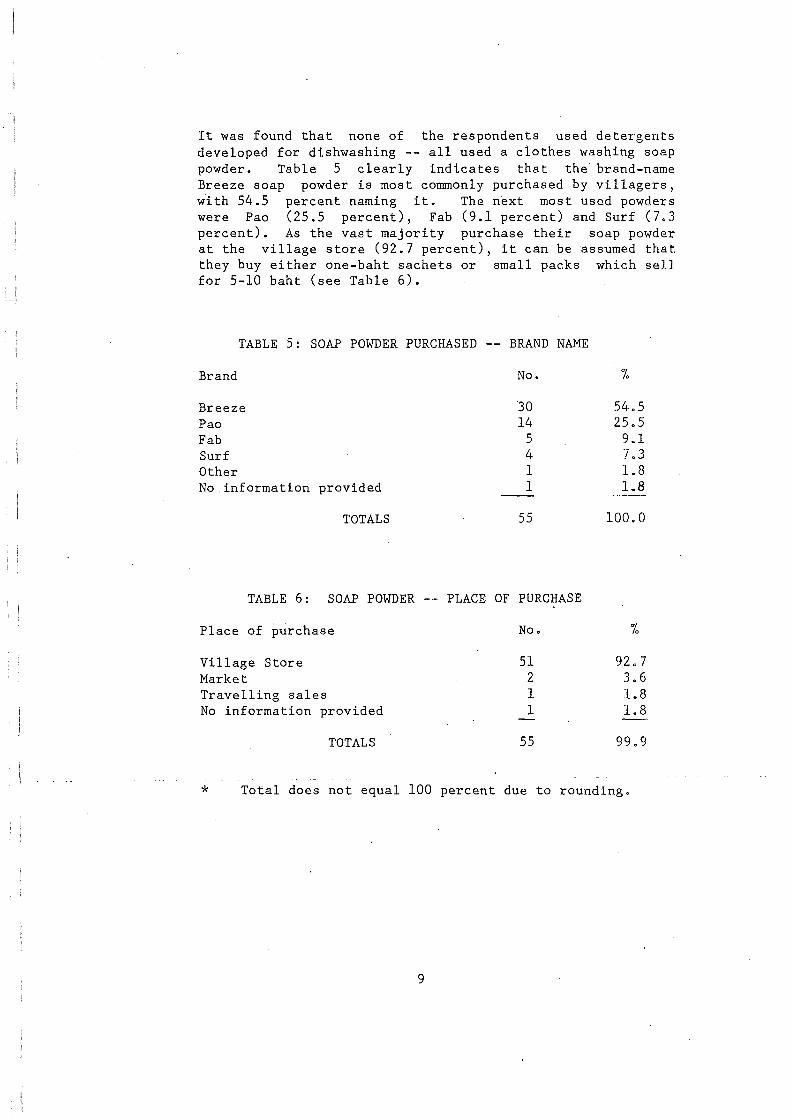
It was found that none of the respondents used detergents developed for dishwashing -- all used a clothes washing soap powder. Table 5 clearly indicates that the' brand-name Breeze soap powder is most commonly purchased by villagers, with 54.5 percent naming it. The next most used powders were Pao (25.5 percent), Fab (9.1 percent) and Surf (7.3 percent). As the vast majority purchase their soap powder at the village store (92.7 percent), it can be ~ssumed that they buy either one-baht sachets or small packs which sell for 5-10 baht (see Table 6).
TABLE 5: SOAP POWDER PURCHASED -- BRAND NAME
Brand No. "/o
Breeze '30 54.5 Pao 14 25.5 Fab 5 9.1 Surf 4 7.3 Other 1 1.8 No.information provided 1 l.B
TOTALS 55 100.0
TABLE 6: SOAP POWDER -- PLACE OF PURCHASE
Place of purchase No. %
Village Store 51 92.7 Market 2 3.6 Travelling sales 1 1.8 No information provided 1 1.8
TOTALS 55 99.9
* Total does not equal 100 percent due to rounding.
9
The person· who made the purchase of soap powder was most often a female (84.5 percent), and of these, 74.2 percent were identified as "housewives". Other purchasers were usually children of the family. An attempt was also made to assess the amount of money spent on soap purchases (see Table 7). The data should, however, be treated with caution as it is difficult for people to accurately delineate how much soap powder they use for washing dishes and for washing clothes (given that they use the same powder). Nevertheless, from the survey, it was found that the average monthly family expenditure was 6.2 baht.
TABLE 7: MONTHLY EXPENDITURES ON SOAP POWDER FOR DISHWASHING
Amount No. "/o
Less than 3 baht 1 1.8 3-5 baht 38 69.1 6-10 baht 11 20.0 More than 10 baht 3 5.5 No information provided 2 3.6
TOTALS 55 100.0
More investigation of expenditure patterns is required, but it would appear that a significant rural market for detergents exists, and that people see a value to the use of washing powder for dishwashing. It would be useful if marketing of dishwashing detergents could include hygiene "messages".
4.4 Soaking of Dishes
Given that Pinfold dishes, prior to number of questions
(1988) had identified the soaking of washing, as a potential problem area, a were asked concerning this practice.
When asked if they regularly soaked dishes, pots and other kitchen utensils prior to washing them 58.2 percent of people stated that they did. Two main reasons were given for this practice there was no time to wash-up immediately (46.9 percent), or washing was easier after soaking (21.9 percent). The details are presented in Table 8 below. Soaking was most often done without soap (65.6 percent of respondents).
10
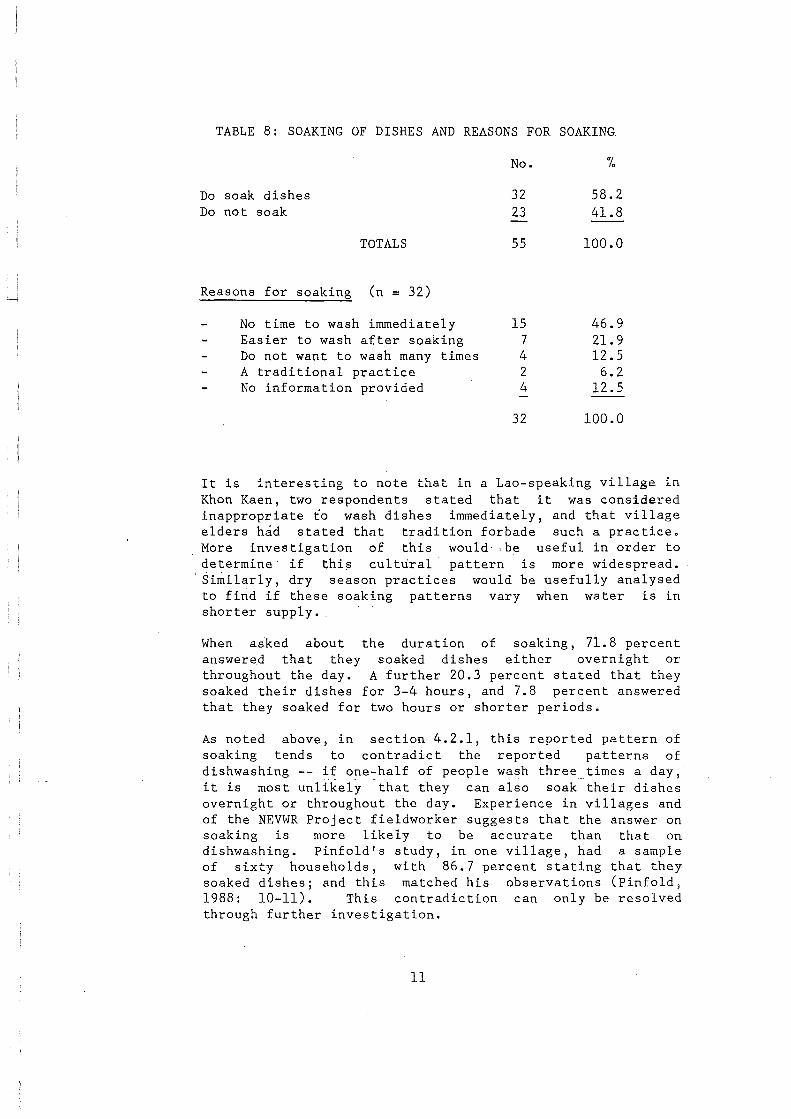
TABLE 8: SOAKING OF DISHES AND REASONS FOR SOAKING.
No. fo
Do soak dishes 32 58.2 Do not soak 23 41.8
TOTALS 55 100.0
Reasons for soaking (n = 32)
No time to wash immediately 15 46.9 Easier to wash after soaking 7 21.9 Do not want to wash many times 4 12.5 A traditional practice 2 6.2 No information provided 4 12.5
32 100.0
It is interesting to note that in a Lao-speaking village in Khon Kaen, two respondents stated that it was considered inappropriate to wash dishes immediately, and that village elders had stated that tradition forbade such a practice. More investigation of this would· . be useful in order to determine if thi~ cultural· pattern is more widespread.
·Similarly, dry ·season practices would be usefully analysed to find if these soaking patterns vary when water is in shorter supply •.
When asked about the duration of soaking, 71.8 percent answered that they soaked dishes either overnight or throughout the day. A further 20.3 percent stated that they soaked their dishes for 3-4 hours, and 7.8 percent answered that they soaked for two hours or shorter periods.
As noted above, in section 4.2.1, this reported pattern of soaking tends to contradict the reported patterns of dishwashing -- if one-half of pe()ple wash three times a day, it is most unlikely that they can also soak their dishes overnight or throughout the day. Experience in villages and of the NEVWR Project fieldworker suggests that the answer on soaking is more likely to be accurate than that on dishwashing. Pinfold's study, in one village, had a sample of sixty households, with 86.7 percent stating that they soaked dishes; and this matched his observations (Pinfold, 1988: 10-11). This contradiction can only be resolved through further investigation.
ll
4.5 Rinsing
It was noted above (section 2.0) that Pinfold (1988) had mentioned the potential for faecal-oral transmission of pathogens related to dishwashing behaviour. However, it is not clear if the "high-risk" he suggests is associated with the soaking water itself, the soaked dishes, or both --he notes both aspects in his paper. If, however, the use of dishes which have been soaked is considered a potential risk, then rubbing and rinsing of dishes in water after soaking and washing may well reduce contamination.* Interestingly, all respondents stated that they rinsed dishes after washing. Indeed, 93.7 percent stated that they rinsed twice or more each time they washed. It would be useful to know why villagers. do-- this, and what bacteriological impact this ptactice has.
4.6 Drying and Storage
Drying of dishes and utensils may be considered a useful practice, as a lack of moisture means that bacteria will die. A small number of respondents (15.5 percent) stated that they wiped dishes dry. The majority either stored dishes to dry (43.6 percent) or stored them wet (40o9 percent). This was confirmed by 54.5 percent respondents who noted that their dishes were "sometimes" dry when they used them for the next meal, while 45.5 percent stated that they were usually dry.
The method of storing dishes, cutlery, and kitchen utensils is generally considered significant for health in environmental sanitation programmes in Thailand (Department of Health, 1987). In examining this question, sixty percent of respondents answered that they stored their washed dishes in a food cupboard; 36.4 percent stored them around the kitchen or in the washing tub; and only 3.6 percent used a rack (see Table 9).
* Feachem (1984:471) does not examine dishwashing and rinsing, but notes that in some studies the rapid hand-washing with water was useful in removing coliforms. ·
12
TABLE 9: STORAGE OF WASHED DISHES AND UTENSILS
No. '1.
Food cupboard 33 60.0 Kitchen area 16 29.1 Washing-up tub 4 7.3 Rack 2 3.6
TOTALS 55 100.0
An area for possible research which emerges from this is in the area of drying of dishes. If this is done with a cloth -- and this is not noted in the survey -- then there is a potential for contamination. Stanton and Clemens (1986a, 1986b) note that in Bangladesh, cloth could be an element in spreading diarrhoeal disease. It would be useful to observe the other uses of cloth also used for drying dishes.
13
5.0 HEALTH AND HYGIENE EDUCATION
As noted above in section 2.0, this small study was undertaken with the aim of gathering information which may be useful in discussions of possible hygiene education interventions 1
especially related to dish-washing practices. A brief summary of some existing studies and reports on hygiene and health education is necessary.
5.1 Health and Hygiene Education in Thailand
5.1.1 Background
Within the Masterplan for Rural Water Supply and Sanitation in Thailand, prepared by_ the _ _b~!-_f!!l __ I_n~ti!-ute of Technology (AIT, 1985), health and hygiene education have a reasonably high profile. This was especially the case for rural sanitation, where they were one of four major
. activities (AIT, 1985: Vol. I: 29, 35). The programmes identified were:
"Health education curriculum will be designed by the Health Education Division in the Office of the Undersecretary of State for Public health in close coordination with the Ministry of Education. Basic hygiene practices, such as proper toilet utilization, mu.st be· highlighted.
Construction of latrines in all primary schools will be undertaken by the Sanitation Division of the Department of Health in collaboration with local schools and government officials. Actual use of these facilities by school children must be encouraged. It will be the duty of school teachers to teach proper defecation habits and maintenance of toilet facilities.
Design and preparation of radio programs, shows, posters, leaflets, and comics will be carried out by the Sanitation Division of the Department of Health. Cooperation from the local government officials and other persorinelmust be sought in the distribution of educational materials to the community. Radio programs and films to be shown must be made in such a way that the program objectives are reflected.
14
* VHV VHC
Information dissemination by personal contacts 1
with a view to changing local attitude, will be conducted by the VHVs and VHCs* at the villages through the Primary Health Care program. In addition, the VHVs/VHCs may be utilized to distribute the educational materials to the villagers during their household visits".
In further discussing the data required for evaluation of water supply and sanitation, emphasis was placed on three areas which are related to health and hygiene education (AIT, 1985, Vol. II: VI-18-21):
1) Face-to-face contact with VHVs and VHCs -- assess their impact in imparting messages on health.
2) Water storage habits -- assess households storing water in manner.
the proportion of a more hygienic
3) Handwashing after defecation -- this is one of the aims of health education, and the impact of such education should be assessed.
All of this was based on an assessment that "no improvement in public health is likely to take place without the proper utilization of water and sanitation services". It was considered "imperative" that hygiene education be promoted as "one of the important components of the rural water supply and sanitation program". This was aimed to "enhance the involvement of the villagers ••• 11 (AIT, 1985, Vol. II: III-80). More specifically, the proposed programme targeted children, young people and women. For children, school programmes were to be emphasised, using school latrines. The crucial role of women was noted and it was strongly argued that they should be considered as users, trainers and educators (AIT, 1985, Vol. II: III-83).
Thus, within the Masterplan, hygiene education had a __ high profile, even if the potential areas for such education were not clearly identified. The Water and Sanitation for Health Project (WASH) also noted the positive emphasis given to hygiene education in the Masterplan. They stated, however, that there were a number of potential problems (Warner and Karlin, 1985: 15, 32):
Village health volunteer Village health communicator
15
5.1.2
1) Hygiene education appears to be virtually the sole responsibility of the Sanitation Division of the Ministry of Public Health, but this Division has placed most of its effort in human waste disposal, and it was considered that its budget might not be sufficient to support a major increase in hygiene education and associated strategies.
2) The creation of mobile health education 14 million baht) would take two-thirds health education budget.
units (at of total
3) Proposed health education programmes were largely passive in delivery.
4) Hygiene education had not been developed as a programme.
5) Lack of trained personnel.
Unfortunately, when the Masterplan was operationalised as an Action Plan for water resource development (Faculty of Engineering, Khon Kaen University et. al., 1987), almost all reference to health and hygiene education was removed. The only issue of significance in this area was assigned to a research and development sub-programme where water user practices, at the village level,· were to be studied. In the Sanitation Action Plan, being developed in 1989, however, considerable emphasis has again been given to health and hygiene education. Even so, the issues of hygienic water storage and handwashing, noted in the Masterplan, remain largely unaddressed. It should be noted, however, that Thailand's successful primary health care programme has, in part, attempted to promote health education (Wandee, et. al., 1982:357).
Health and hygiene education
The WASH report argued clearly and strongly a case for more hygiene education. Health education, they say, is 11 a process of systematically bringing about changes in health beliefs, attitudes, and practices in order to increase people's value for health, to promote healthful practices, and to reduce illness and premature death" (Warner and Karlin, 1985: 14).
16
5.1.3
If the importance of health and hygiene education has been increasingly recognised in recent years (Feachem, 1984:474), results from such educational interventions have not often produced highly significant results (Feachem, 1984; Stanton and Clemens, 1987). There are many reasons for this. For example, the important role of women was often ignored (Elmendorf and Isely, 1983); research methodologies were inappropriate; evaluations have not been conducted (Feachem, 1984); and an undue emphasis on prohibitions rather than on empirically based interventions (Stanton and Clemens, 1987).
Pinfold (1988: 7) has summarised these issues as follows:
1) "The design of the education message ·is often based on theory which is not proven to be an effective health intervention for the target group".
2) "The education package does not always take into consideration the target group and cultural sensitivities. Often messages consist of activities that require too much effort and expenditure on behalf of recipients, •• or expects people to do too many things where a direct benefit is not immediately apparent".
3) "The relationship. between the education message and behaviour change is tenuous ••• ".
4) The "whole area is inherently difficult to monitor and evaluate".
Considerations on increasing the effectiveness of health and hygiene education
Given these problems, a survey of literature suggests that there are certain elements required or which should be considered if any health or hygiene education programme is to be effective.
The following is a list of factors, drawn from various studies, both. Thai and international, which might be considered if health and hygiene education is to be promoted.
17
a. Selection of behaviours
In implementing hygiene education it is important to clearly ident{fy the behaviour/s which are to be targeted. Pinfold (1988: 8) notes that it is necessary to select a behaviour where a causal relationship can be demonstrated with the outcome indicator. This is supported by Stanton, Clemens, Khair, et. al. (1987:275) who argue that the selected behaviour should have been "shown to be empirically correlated with reduced rates of diarrhoea". In additional if the targeted behaviour is one which is already practiced, by some households, then there is a greater chance that behaviour changes will be accepted by others (Pinfold, 1988: 8; Stanton, Clemens, Khair, et. al., 1987:275). Feachem's (1984: 472) assessment of hygiene education suggests some caution is required however: "Hygiene practices that would have required expenditure [by those whose behaviour was targeted] .•• were not significantly changed".
b. Implementation
In implementing a hygiene behaviour programme requires, of course, careful planning. Even ·so, some authors stress that much attention should be given to design and tmplementation but that this is not always done (Stanton; Clemens, Khair, et. al., 1987: 275). At an early stage, community members should be involved in project goal determination, and their experience must be seen as valuable, especially as they are drawn in as trainees (Stanton, Clemens, Khair, et. al., 1987: 275, 2 76).
Implementation must begin with thorough introductory training and social preparation and hygiene messages should be kept as simple as possible (Stanton, Clemens, Khair, et. al., 1987: 275, 276; Simpson-Herbert, 1987: 13). The timing of visits to the target community might well be considered as the time available to people varies by season and economic activity (Stanton, Clemens, Khair, et. al., 1987: 280). Feachem (1984: 472) found that the adoption of hygienic behaviours can be strongly influenced by sustained and culturally sound educational programmes. These programmes can be feasible at either a localised level or as national programmes, with both mass media campaigns and direct face-to-face interaction programmes having been successful (Feachem, 1984: 474).
18
c. Target groups
Two main groups have been identified as major targets in hygiene education programmes associated with water supply and sanitation -- women and their children.
Women, especially those who are mothers of young children, are seen as being very significant targets because of the central role they play in the education of the young and within traditional health care networks (Elmendorf and Isely, 1983: 199). In addition, women tend to have a more permanent presence in the household and community. These features suggest that women are an appropriate group when selecting trainers and trainees for hygiene education programmes at the household and community levels (Elmendorf and Isely, 1983:199; Simpson-Herbert, 1987: 14; and Stanton, Clemens, Khair, et. al., 1987: 276).
Children are considered important for it is they who are generally most at risk from diseases which may be related to poor hygiene practices. School children may serve as teachers of their younger siblings, while schools are an appropriate place to target young girls who are already concerned with issues of motherhood and household management (Elmendorf and Isely, 1983: 198).
d. Training
In community and household level programmes, training should be kept as informal as possible, with the trainees being actively involved ~- they should not be passive recipients of training. Frequent feedback between project organisers, trainers and the target community is crucial (Stanton, Clemens, Khair, et. al., 1987: 276).
Person-to-person community level, sophisticated or (Simpson-Herbert,
interaction is and trainers
highly literate 1987: 13-15).
19
important at the should not require skills of trainees
Trainers should, wherever possible, be aware of local cultural realities, and be able to communicate effectively in local languages. Such cultural considerations are crucial (Simpson-Herbert, 1987). It should be added that in addition to cultural sensibilities, effective trainers should also be aware of social status and class trainers whose dress, bearing and language clearly distinguishes them as being of a different status and class or in a rural context, clearly urban in outlook, may not be acceptable to the trainees, or their messages may be rejected.
e. Educational materials
The production of hygiene and health education materials should be culturally appropriate, pre-tested, preferably at local-level, in local languages, and simple (Simpson-Herbert 1987: 13-15; Elmendorf and Isely, 1983: 198). If they can be with and by the community, so much the better.
It is important to determine which media will be most appropriate to the target groups. For example, in urban Bangladesh it was found that women as mothers were most interested in work related pictures, pictorial stories and discussion groups. Children liked listening to stories, flexiflans (story boards), and active drama (Stanton, Clemens, Khair, et. al., 1987: 279-280).
f. Evaluation
As noted by Pinfold (1988) and others, evaluation is a crucial activity, but it must be in relation to outcomes which may be measured and where the targeted behaviours are causal.
For governments and their planning agencies, however, such indicators may not be seen as meaningful -- it is easier to enumerate hardware (e.g. number of latrines) than software (e~g. hygi~ne education). The~efore, methods of reporting and evaluating software aspects need to be considered prior to implementation.
All of these points lead inexorably to the conclusion that the community and household levels are the crucial levels for hygiene education programmes.
20
6.0 DISHWASHING AND HYGIENE EDUCATION
Dishwashing behaviour may be targeted for hygiene education. As noted below (section 7.0), more local-level research, observation, and planning is required before a small project proceeds, but it is an activity which may be pursued.
From the survey noted above, there are a number of factors which may be considered useful in beginning project planning or identification. These are:
1) The target group would be women, of child-bearing age, and with a primary school education -- this means they are probably basically literate. School-age children seem not to be involved with dishwashing.
2) Most people (83 percent) say they wash dishes two or three times a day.
3) Dishwashing usually occurs in the kitchen area, using groundwater or water from surface supplies.
4) About half of the respondents regularly soak dishes.
5) The vast majority rinse their dishes twice or more after washing.
6) About half of the respondents stored dishes wet and that their dishes were not always dry when used for the next meal~
7) One-third of respondents stored their dishes in conditions which are not necessarily hygienic.
For marketing, the following information was determined:
1) All report using soap for dishwashing.
2) None use dishwashing detergents.
3) Breeze brand soap powder is used by more than half of ·the- respondents~-
4) Most buy their soap powder at a village store.
5) The average monthly amount dishwashing is 6.2 baht.
21
spent on soap for
7.0 FURTHER INVESTIGATION REQUIREMENTS
A number of issues remain unresolved or have been raised even by this small study. These are:
l) What, exactly, is the hygiene problem associated with dishwashing? Is it the increased potential for the ingestion of pathogens with highly contaminated soaking water, or is it contaminated dishes?
2) When do people wash? Soaking and washing patterns must be more fully understood. This requires observation.
3) Is the washing tub used for clothes as well as dishes, or any other purposes?
4) Does rinsing of dishes reduce contamination? Why do village women rinse dishes? Is there a perceived health benefit?
5) How do dishwashing patterns vary by season?
6) A traditional taboo was found in the dishwashing area 1
but it is likely that there are more -- it would be useful to further examine this area.
7) No information was collected on what happens to soaking and dishwashing water after use -- or if it is reused. More observation is required.
8) Research should be conducted on the use of cloth which is also used for dish drying and wiping •
. 22
8.0 REFERENCES
Asian Institute of Technology (AIT). (1985). Masterplan for Rural Water Supply and Sanitation in Thailand, Bangkok: Regional Research and Development Center.
Simpson-Herbert, Mayling. (1987). Hygiene Education Strategies for Region 1 for the Ministry of Public Health in Thailand, Washington D.C.: WASH Field Report No. 210, April.
Faculty of Engineering, Khan Kaen University, et. al. (1987). Action Plan of the Rural Water Supply Program During the Sixth National Economic and Social Plan Period (1987-1991), Khan Kaen: NEVWR Project and NESDB.
Department of Health. (1987). Handbook for Implementation of the Rural Food Sanitation Programme, Bangkok: Ministry of Public Health, Office of the Food Sanitation Project (in Thai).
Elemendorf, Mary.L. and Isely, Raymond B. (1983). "Public and Private Roles of Women in Water Supply and Sanitation Programs", Human Organization, 42, 3, pp. 195-204.
Feachem, R. G. (1984). "Interventions for Diarrhoeal Diseases Among Young Children: Personal and Domestic Hygiene," Bulletin
the Control of Promotion of of ·the World ,-----------------------Health Organization, 62, 3, pp 467-476.
Hewison, Kevin. (1987). ~W~a~t~e_r __ ~S~t~o_r~a~g~e~J_a_r_s~a~n~d ___ T_h_e_i7r __ U_s_e_: ____ A
Case Study of King Amphur Kae Dam Mahasarakham, Khan Kaen: NEVWR Project Report No. 54.
Pinfold, John. (1988). A Hygiene Intervention Study, Khon Kaen: NEVWR Project Report No. 48.
Stanton, Bonita F. and Clemens, John D. (1986a). "Soiled Saris", Dialogue on Diarrhoea, No. 26.
Stanton, Bonita F. and Clemens, John D. (l986b). "Soiled Saris: a vector of disease transmission", Transactions of the Royal Society of Tropical Medicine and Hygiene, pp. 485-488.
23
Stanton, Bonita F. and Clemens, John D. (1987). "An Educational Intervention for Altering Water-Sanitation Behaviors to Reduce Childhood Diarrhoea in Urban Bangladesh," American Journal of Epidemiology, 125, 2, pp. 292-301.
Stanton, F.F., Clemens, J.D., Aziz, K.M.A. and Rahman, M. (1987)" "Twenty-four-hour Recall, Knowledge-Attitude-Practice Questionnaires, and Direct Observations of Sanitary Practices: A Comparative Study," Bulletin of the World Health Organization, 65, 2, pp. 217-222.
Stanton, F.F., Clemens, J.D., Khair, T., Khatun, K. and Jahan, D.A. (1987). "An Educational Intervention for Altering Water - Sanitation Behaviours to Reduce Childhood Diarrhoea in Urban Banbladesh: Formulation, Preparation and Delivery of Educational Intervention," Soc. Sci. Med., 24, 3, pp. 275-283.
Wandee Varavithya, Thara Viriyapanich, Sakorn Dhananitta and Aree Valyasevi. (1982). "Primary Health Care and Diarrhoeal Diseases in Thailand," Southeast Asian Journal of Tropical Medicine and Public Health, 13, 3, pp. 357-360.
Warner, Dennis B. and Karlin, Barry. (1985). Proposed Water Supply and Sanitation Strategies for the Ministry of Public Health in the Thailand Sixth Five-Year Plan, 1987 - 1991, Washington D.C.: WASH Field Report No. 153, November.
24

















