17
ANNUAL SUMMARY OF REPORTABLE DISEASES 2010 Columbus & Franklin County, Ohio
ANNUAL SUMMARY OF
REPORTABLE DISEASES 2010Columbus & Franklin County, Ohio

ANNUAL SUMMARY OF
REPORTABLE DISEASES 2010Columbus & Franklin County, Ohio
Published July 2012
Compiled And Prepared By:
Allen Emanuel, M.P.H., Epidemiologist, Center for Epidemiology, Preparedness and Response, Columbus Public Health240 Parsons Ave.Columbus, Ohio 43215www.publichealth.columbus.gov
Radhika Iyer, M.P.H., C.P.H., Infectious Disease Epidemiologist and Supervisor, Franklin County Public Health280 East Broad StreetColumbus, Ohio 43215-4562www.myfcph.org
Cover Image: Legionella (Legionnaire’s Disease) Janice Haney Carr, Centers for Disease Control and Prevention

We would like to thank the staff of...
Columbus Public Health Kathy Cowen, M.S.Anne Trinh, M.P.H. Ben DeJesus, M.S. Brian Butler, M.P.H. Suellen Bennett, M.S.P.H.,Dr. Elizabeth Koch, M.D., M.P.H.& T.M. Naomi Tucker, R.N., M.P.H.
Franklin County Public Health Susan Tilgner, M.S., L.D., R.D., R.S. Debbie Wright, C.N.P., M.S. Carol Stasko, M.S., R.N., APHN-BC
We would also like to thank Michelle Groux, M.P.H. for her work on formatting the report.
ACKNOWLEDGEMENTS
Columbus Public Health & Franklin County Public Health July 2012

Introduction ..................................................................................................................................................................................... 1
2010 Demographic Profile of Franklin County ................................................................................................................ 2
Reportable Diseases, Franklin County, Ohio .....................................................................................................................3
Highlights of Selected DiseasesInfluenza-Associated Hospitalizations ..........................................................................................................................5Legionellosis ...........................................................................................................................................................................6Malaria ....................................................................................................................................................................................... 7
Selected Outbreaks 2010E. coli O145 ..............................................................................................................................................................................8Pertussis Outbreak ...............................................................................................................................................................9
Timeliness of Disease Reports ..........................................................................................................................................10-11
Technical Notes ............................................................................................................................................................................12
References .....................................................................................................................................................................................13
TABLE OF CONTENTS
Columbus Public Health & Franklin County Public Health July 2012

Infectious diseases are illnesses caused by microorganisms, such as bacteria, viruses and parasites, and are transmitted from an infected person/animal and/or contaminated food or water source to another person or animal. Most infectious diseases spread from direct contact with the bacteria or viruses that are carried in bodily fluids (e.g., blood) or expelled into the air (in the form of respiratory droplets) by an infected person. Some diseases can be spread only indirectly through contaminated food and water sources. Other diseases are introduced into the body by animals or insects carrying the infectious agent.
This annual summary represents the 2010 reportable diseases that were diagnosed among residents of Columbus City and Franklin County and were reported to Ohio and local public health agencies as required by Ohio Administrative Code 3701-3-02. Only selected infectious diseases determined to be of public health significance are reportable; therefore, the data presented here do not represent all cases of infectious disease that occur in Columbus and Franklin County. Additionally, only confirmed cases of disease have been analyzed for this summary. The data are considered provisional but provide valuable insight into these diseases.
The summary is intended to be a resource for individuals and our public health partners for whom infectious diseases are of concern. Further information on infectious disease may be obtained by contacting either Columbus Public Health or Franklin County Public Health.
For over eleven years, the Columbus and Franklin County Public Health have joined forces to make the reporting, tracking and investigation of infectious disease cases easier and more convenient through the Infectious Disease Reporting System (IDRS) formerly called the Communicable Disease Reporting Systems (CDRS). This allows for early identification of potential outbreaks and new trends in infectious diseases. The Infectious Disease staff ensures proper investigation, timely follow-up of all reports and preventive interventions to reduce secondary cases.
KEY FINDINGS ARE SUMMARIZED BELOW: � In 2010, a total of 1,694 cases of infectious disease (excluding sexually transmitted infections
and tuberculosis) were reported and confirmed among Franklin County residents.
� Franklin County’s total rate of confirmed infectious diseases decreased significantly to 145.6 cases per 100,000 in 2010 from 188.8 cases per 100,000 in 2009.
� The rate of Influenza –associated hospitalizations decreased significantly to 2.3 cases per 100,000 in 2010 from 45.0 cases per 100,000 in 2009.
� The rate of shigellosis decreased significantly to 1.2 cases per 100,000 in 2010 from 21.7 cases per 100,000 in 2009.
� Due to an outbreak, the rate of pertussis increased significantly to 52.0 cases per 100,000 in 2010 from 17.2 cases per 100,000 in 2009.
INTRODUCTION
Columbus Public Health & Franklin County Public Health 1 July 2012
1,118,107
1,129,067
1,150,122
1,163,414
1,100,000
1,110,000
1,120,000
1,130,000
1,140,000
1,150,000
1,160,000
1,170,000
2007 2008 2009 2010
FRANKLIN COUNTY POPULATION: 2007 - 2010
TABLE 1: GENDER
POPULATION PERCENT
Male 566,499 48.7Female 596,915 51.3
TABLE 2: RACE
POPULATION PERCENT
White 805,617 69.2Black or African American 247,225 21.2American Indian and Alaska Native 2,852 0.2Asian 44,996 3.9Native Hawaiian and Other Pacific Islander 746 0.1
Some Other Race 27,272 2.3Two or More Races 34,706 3.0
TABLE 3: AGE (YEARS)
POPULATION PERCENT
0-4 83,117 7.1
5-14 150,546 12.9
15-24 183,640 15.8
25-34 190,763 16.4
35-44 157,860 13.5
45-54 159,905 13.7
55-64 121,877 10.5
65-74 62,634 5.4
75-84 37,550 3.2
85+ 15,522 1.3
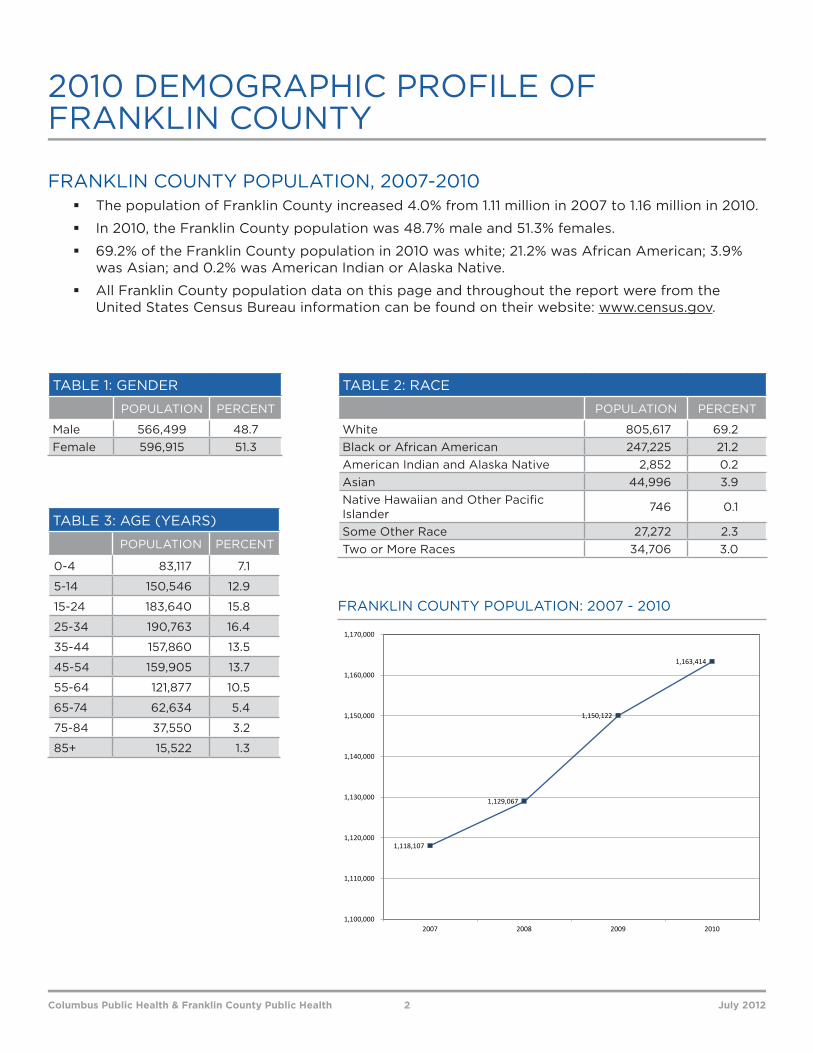
FRANKLIN COUNTY POPULATION, 2007-2010 � The population of Franklin County increased 4.0% from 1.11 million in 2007 to 1.16 million in 2010.
� In 2010, the Franklin County population was 48.7% male and 51.3% females.
� 69.2% of the Franklin County population in 2010 was white; 21.2% was African American; 3.9% was Asian; and 0.2% was American Indian or Alaska Native.
� All Franklin County population data on this page and throughout the report were from the United States Census Bureau information can be found on their website: www.census.gov.
2010 DEMOGRAPHIC PROFILE OF FRANKLIN COUNTY
Columbus Public Health & Franklin County Public Health 2 July 2012

TABLE 4: REPORTABLE DISEASES FOR FRANKLIN COUNTY, OHIOANNUAL COUNTS AND RATES, 2007-2010
2007 2008 2009 2010Population 1,118,107 1,129,067 1,150,122 1,163,414
CLASS DISEASE NAME # of Cases
Case Rate†
# of Cases
Case Rate†
# of Cases
Case Rate†
# of Cases
Case Rate†
B (1) HIV/AIDS* 259 23.2 184 16.3 269 23.4 NA NAB (2) Amebiasis 16 1.4 9 0.8 5 0.4 6 0.5
A Anthrax 0 0.0 0 0.0 0 0.0 0 0.0A Botulism (foodborne) 0 0.0 0 0.0 0 0.0 0 0.0A Botulism (infant) 0 0.0 0 0.0 0 0.0 0 0.0
B (2) Brucellosis 0 0.0 0 0.0 2 0.2 1 0.1B (2) Campylobacteriosis 73 6.5 93 8.2 88 7.7 90 7.7 B (2) Chlamydia* 6,276 561.3 7,255 642.6 7,754 674.2 7,830 673.0
A Cholera 0 0.0 0 0.0 0 0.0 0 0.0B (1) Coccidioidomycosis 0 0.0 0 0.0 0 0.0 4 0.3B (2) Cryptosporidiosis 27 2.4 313 27.7 21 1.8 36 3.1B (2) Cytomegalovirus (congenital) 5 0.4 1 0.1 5 0.4 7 0.6B (1) Dengue 0 0.0 0 0.0 0 0.0 0 0.0
A Diphtheria 0 0.0 0 0.0 0 0.0 0 0.0B (1) E. coli O157:H7 6 0.5 29 2.6 14 1.2 8 0.7B (1) E. coli Unspecified 2 0.2 4 0.4 5 0.4 5 0.4B (1) E. coli Not O157 0 0.0 0 0.0 3 0.3 15 1.3B (1) Encephalitis, (primary viral) 1 0.1 0 0.0 0 0.0 0 0.0B (1) Encephalitis, West Nile 0 0.0 0 0.0 0 0.0 0 0.0B (2) Ehrlichiosis 1 0.1 0 0.0 0 0.0 0 0.0B (2) Giardiasis 112 10.0 167 14.8 181 15.7 191 16.4B (2) Gonorrhea* 3,817 341.4 3,478 308.0 2,933 255.0 2,911 250.2B (1) Haemophilus influenzae 3 0.3 5 0.4 10 0.9 6 0.5B (1) Hantavirus 0 0.0 0 0.0 0 0.0 0 0.0B (1) Hemolytic uremic syndrome 0 0.0 1 0.1 2 0.2 0 0.0B (1) Hepatitis A 10 0.9 10 0.9 7 0.6 7 0.6B (2) Hepatitis B (acute) 10 0.9 14 1.2 19 1.7 32 2.8B (2) Hepatitis B (chronic) 110 9.8 74 6.6 68 5.9 65 5.6B (2) Hepatitis C (acute) 0 0.0 0 0.0 0 0.0 1 0.1B (2) Hepatitis C (chronic) 1,000 89.4 739 65.5 525 45.6 662 56.9B (2) Herpes (congenital) 1 0.1 0 0.0 0 0.0 0 0.0B (2) Influenza-associated hospitalization - - - - 517 45.0 27 2.3B (1) Influenza-associated Pediatric Mortality 0 0.0 0 0.0 2 0.2 0 0.0
A Influenza A-novel virus - - - - 37 3.2 0 0.0** Kawasaki Disease 2 0.2 0 0 0 0 0 0
B (1) Legionellosis 38 3.4 65 5.8 58 5.0 61 5.2B (2) Leprosy 0 0.0 0 0.0 0 0.0 0 0.0B (2) Leptospirosis 0 0.0 0 0.0 0 0.0 0 0.0B (1) Listeriosis 6 0.5 2 0.2 1 0.1 4 0.3B (2) Lyme disease 2 0.2 1 0.1 7 0.6 4 0.3B (1) Malaria 8 0.7 16 1.4 14 1.2 19 1.6
REPORTABLE DISEASES
Columbus Public Health & Franklin County Public Health 3 July 2012

TABLE 4: REPORTABLE DISEASES FOR FRANKLIN COUNTY, OHIOANNUAL COUNTS AND RATES, 2007-2010
2007 2008 2009 2010Population 1,118,107 1,129,067 1,150,122 1,163,414
CLASS DISEASE NAME # of Cases
Case Rate†
# of Cases
Case Rate†
# of Cases
Case Rate†
# of Cases
Case Rate†
A Measles 0 0 0 0.0 0 0.0 0 0.0B (1) Meningitis, aseptic (viral) 74 6.6 62 5.5 125 10.9 99 8.5B (1) Meningitis (other bacterial) 0 0.0 6 0.5 3 0.3 4 0.3
A Meningococcal disease (N. meningitidis) 5 0.4 3 0.3 4 0.3 5 0.4B (1) Mumps 0 0.0 0 0.0 1 0.1 1 0.1
B (2) Mycobacterial Disease, other than tuberculosis (MOTT) 146 13.1 100 8.9 204 17.7 203 17.4
B (1) Pertussis 300 26.8 159 14.1 198 17.2 604 51.9A Plague 0 0.0 0 0.0 0 0.0 0 0.0
B (1) Polio 0 0.0 0 0.0 0 0.0 0 0.0B (1) Psittacosis 0 0.0 0 0.0 0 0.0 0 0.0
A Rabies 0 0.0 0 0.0 0 0.0 0 0.0B (2) Rocky Mountain Spotted Fever (RMSF) 0 0.0 0 0.0 0 0.0 0 0.0
A Rubella 0 0.0 0 0.0 0 0.0 0 0.0B (1) Rubella (congenital) 0 0.0 0 0.0 0 0.0 0 0.0B (1) Salmonellosis 120 10.7 131 11.6 145 12.6 119 10.2
A Severe Acute Respiratory Syndrome (SARS) 0 0.0 0 0.0 0 0.0 0 0.0B (1) Shigellosis 15 1.3 642 56.9 250 21.7 14 1.2
A Smallpox 0 0.0 0 0.0 0 0.0 0 0.0
B (1) Staphylococcus aureus - intermediate resistance to vancomycin (VISA) 0 0.0 0 0.0 0 0.0 1 0.1
B (2) Streptococcal disease-group A, invasive 36 3.2 38 3.4 31 2.7 35 3.0B (2) Streptococcal disease-group B (newborn) 6 0.5 8 0.7 2 0.2 6 0.5B (2) Streptococcal toxic shock syndrome (STSS) 2 0.2 0 0.0 0 0.0 0 0.0B (2) Streptococcus pneumoniae, invasive 125 11.2 51 4.5 181 15.7 168 14.4B (1) Syphilis* 195 17.4 280 24.8 108 9.4 112 9.6B (1) Tetanus 0 0.0 0 0.0 0 0.0 1 0.1B (1) Tuberculosis (TB)* 78 7.0 61 5.4 41 3.6 66 5.7
A Tularemia 0 0.0 0 0.0 1 0.1 0 0.0B (2) Typhoid Fever 1 0.1 2 0.2 5 0.4 2 0.2B (2) Varicella 57 5.1 15 1.3 31 2.7 31 2.7
A Viral hemorrhagic fever (VHF) 0 0.0 0 0.0 0 0.0 0 0.0B (2) Vibriosis - other (non- cholera Vibrio spp) 1 0.1 1 0.1 0 0.0 4 0.3
A Yellow Fever 0 0.0 0 0.0 0 0.0 0 0.0B (2) Yersiniosis 8 0.7 4 0.4 4 0.3 7 0.6
†Population estimates obtained from the United States Census Bureau for each year were used in annual rate calculations. Intercensal Estimates of the Resident Population for Counties of Ohio: April 1, 2000 to July 1, 2010 (CO-EST00INT-01-39). Source: U.S. Census Bureau, Population Division. Release Date: September 2011. 2010 is from decennial census. Case rate is per 100,000 people.
*Notes on specific diseases and rates: � Disease totals and calculated disease rates are limited to confirmed cases. Suspects and probable cases are not included. � In Ohio, Influenza A-novel virus & Influenza-associated hospitalization cases became reportable in 2009. � STDs, TB and HIV/AIDS data are from separate Ohio Department of Health (ODH) sources. HIV/AIDS data are provisional and subject to
change. � Syphilis numbers include primary and secondary cases only.
**These are not reportable conditions as of January 2012; however, the ODH receives frequent inquiries for information or they are of special interest.
Note: A dash (-) in the table means that a reportable condition was not reportable in that year.
REPORTABLE DISEASES, continued
Columbus Public Health & Franklin County Public Health 4 July 2012
0 0
517
27 0
5
10
15
20
25
30
35
40
45
50
0
100
200
300
400
500
600
2007 2008 2009 2010
Cases Rate
Case
s
Rate
per 1
00, 0
00
34
2 21
3
12
0
2
4
6
8
10
12
14
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Case
s
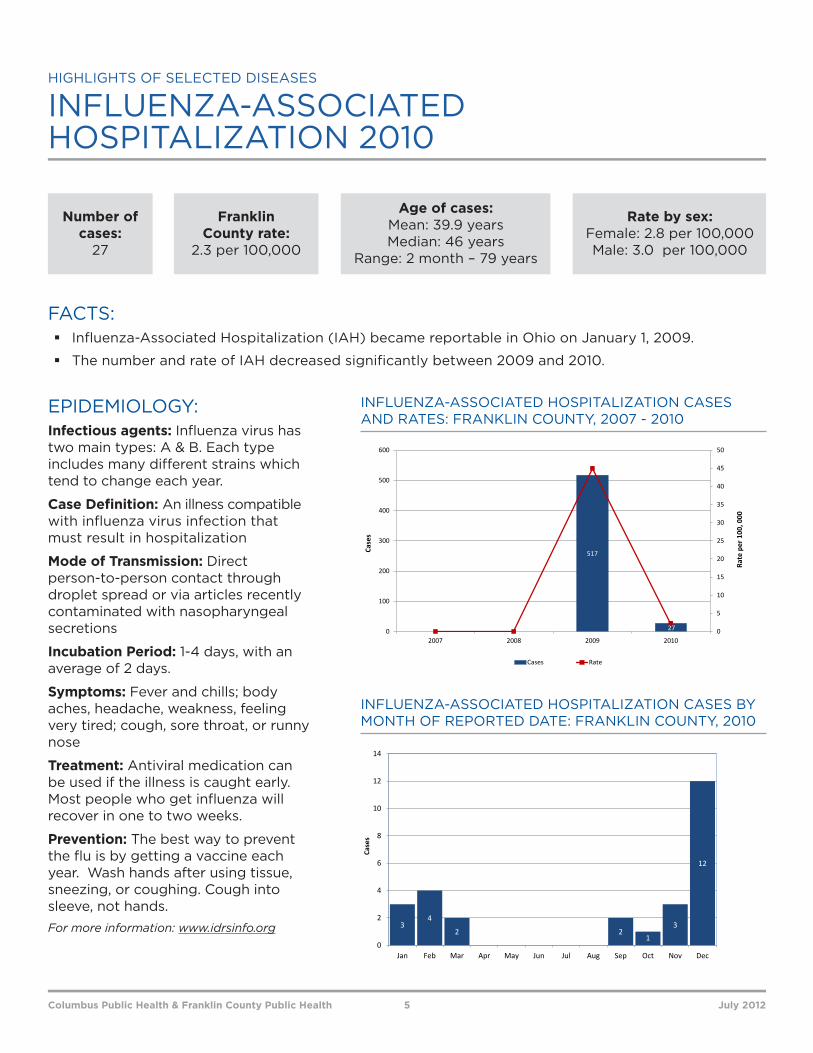
FACTS: � Influenza-Associated Hospitalization (IAH) became reportable in Ohio on January 1, 2009.
� The number and rate of IAH decreased significantly between 2009 and 2010.
INFLUENZA-ASSOCIATED HOSPITALIZATION 2010
Number of cases:
27
Age of cases: Mean: 39.9 years Median: 46 years
Range: 2 month – 79 years
Rate by sex: Female: 2.8 per 100,000 Male: 3.0 per 100,000
Franklin County rate:
2.3 per 100,000
Columbus Public Health & Franklin County Public Health 5 July 2012
INFLUENZA-ASSOCIATED HOSPITALIZATION CASES AND RATES: FRANKLIN COUNTY, 2007 - 2010
INFLUENZA-ASSOCIATED HOSPITALIZATION CASES BY MONTH OF REPORTED DATE: FRANKLIN COUNTY, 2010
EPIDEMIOLOGY:Infectious agents: Influenza virus has two main types: A & B. Each type includes many different strains which tend to change each year.
Case Definition: An illness compatible with influenza virus infection that must result in hospitalization
Mode of Transmission: Direct person-to-person contact through droplet spread or via articles recently contaminated with nasopharyngeal secretions
Incubation Period: 1-4 days, with an average of 2 days.
Symptoms: Fever and chills; body aches, headache, weakness, feeling very tired; cough, sore throat, or runny nose
Treatment: Antiviral medication can be used if the illness is caught early. Most people who get influenza will recover in one to two weeks.
Prevention: The best way to prevent the flu is by getting a vaccine each year. Wash hands after using tissue, sneezing, or coughing. Cough into sleeve, not hands.For more information: www.idrsinfo.org
HIGHLIGHTS OF SELECTED DISEASES
38
6558 61
0
1
2
3
4
5
6
0
10
20
30
40
50
60
70
2007 2008 2009 2010
Cases Rate
Case
s
Rate
per 1
00, 0
00
12
32
7
14
7
3 3
56
8
0
2
4
6
8
10
12
14
16
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Case
s
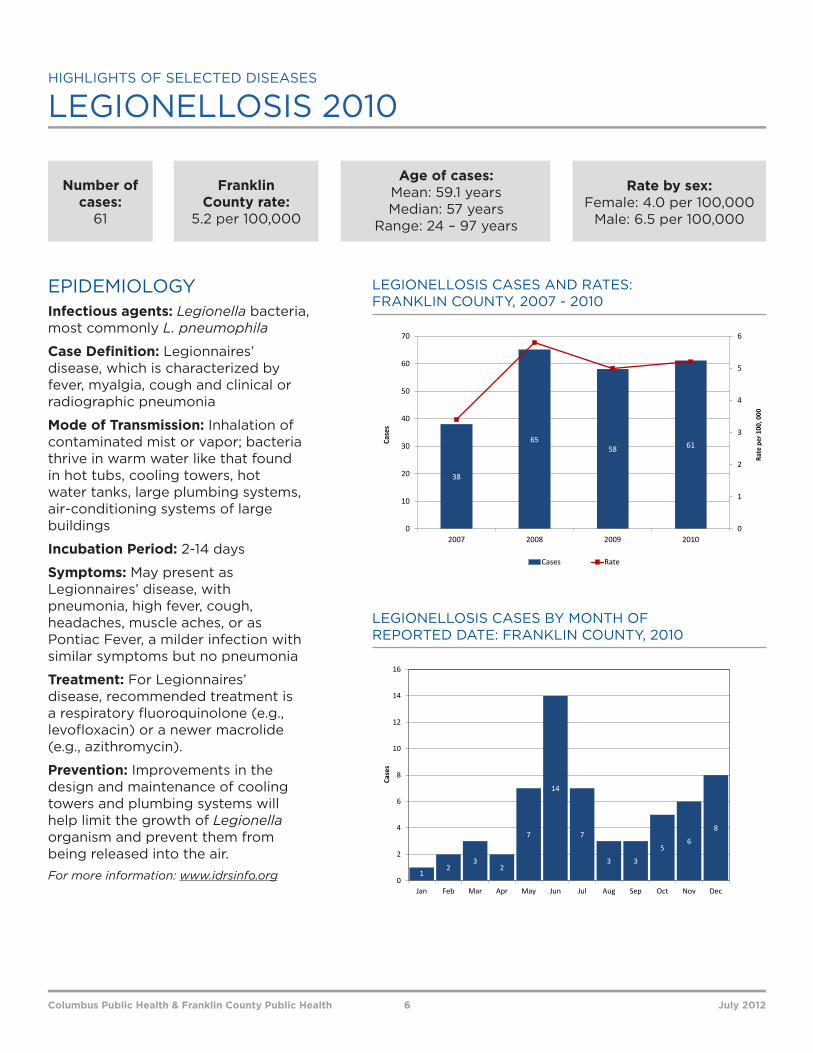
Number of cases:
61
Age of cases: Mean: 59.1 years Median: 57 years
Range: 24 – 97 years
Rate by sex: Female: 4.0 per 100,000
Male: 6.5 per 100,000
Franklin County rate:
5.2 per 100,000
LEGIONELLOSIS 2010
EPIDEMIOLOGYInfectious agents: Legionella bacteria, most commonly L. pneumophila
Case Definition: Legionnaires’ disease, which is characterized by fever, myalgia, cough and clinical or radiographic pneumonia
Mode of Transmission: Inhalation of contaminated mist or vapor; bacteria thrive in warm water like that found in hot tubs, cooling towers, hot water tanks, large plumbing systems, air-conditioning systems of large buildings
Incubation Period: 2-14 days
Symptoms: May present as Legionnaires’ disease, with pneumonia, high fever, cough, headaches, muscle aches, or as Pontiac Fever, a milder infection with similar symptoms but no pneumonia
Treatment: For Legionnaires’ disease, recommended treatment is a respiratory fluoroquinolone (e.g., levofloxacin) or a newer macrolide (e.g., azithromycin).
Prevention: Improvements in the design and maintenance of cooling towers and plumbing systems will help limit the growth of Legionella organism and prevent them from being released into the air. For more information: www.idrsinfo.org
Columbus Public Health & Franklin County Public Health 6 July 2012
LEGIONELLOSIS CASES AND RATES: FRANKLIN COUNTY, 2007 - 2010
LEGIONELLOSIS CASES BY MONTH OF REPORTED DATE: FRANKLIN COUNTY, 2010
HIGHLIGHTS OF SELECTED DISEASES

0
1 1 1 1
3
4
1 1 1
2
3
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Case
s
8
1614
19
0
1
2
3
4
5
6
0
2
4
6
8
10
12
14
16
18
20
2007 2008 2009 2010
Cases Rate
Case
s
Rate
per 1
00,0
00
Number of cases:
19
Age of cases: Mean: 35.3 years Median: 29 years
Range: 10 – 81 years
Rate by sex: Female: 1.5 per 100,000
Male: 1.8 per 100,000
Franklin County rate:
1.6 per 100,000
MALARIA 2010
EPIDEMIOLOGYInfectious agents: Malaria parasite. There are five species of genus Plasmodium known to infect humans: P. falciparum, P. malariae, P. ovale, P. vivax and P. knowlesi.
Case Definition: The first symptoms of malaria (most often fever, chills, sweats, headaches, muscle pains, nausea and vomiting) are often not specific and are also found in others diseases (such as influenza and other common viral).
Mode of Transmission: Malaria in humans is normally transmitted by the bite of a female Anopheles mosquito that is infected with one of four species of Plasmodium.
Incubation Period: P. falciparum: 12 days; P. vivax and P. ovale: 14 days; P. malariae: 30 days. Symptoms: Fever and shaking chills—fever tends to cycle up and down every 1-3 days; headache, muscle aches, tiredness; nausea, vomiting, and diarrhea; paleness or yellowish skin and eyes
Treatment: Malaria can be treated with antibiotics. However, treatment may be ineffective if the parasite is resistant to the drug used or if the patient does not finish all the medicine.
Prevention: Preventive medications are available for those traveling to a known malarial area. Prevent mosquito bites by using mosquito repellents on skin and clothing and sleep under bed nets. Eliminate mosquito breeding sites by covering or discarding items that collect water outdoors.
For more information: www.idrsinfo.org
Columbus Public Health & Franklin County Public Health 7 July 2012
MALARIA CASES AND RATES: FRANKLIN COUNTY, 2007 - 2010
MALARIA CASES BY MONTH OF REPORTED DATE: FRANKLIN COUNTY, 2010
HIGHLIGHTS OF SELECTED DISEASES

Escherichia coli (abbreviated as E. coli) are a large and diverse group of bacteria. Although most strains of E. coli will not cause illness, others can make you sick. Some kinds of E. coli can cause diarrhea, while others cause urinary tract infections, respiratory illness and pneumonia, and other illnesses. Some kinds of E. coli cause disease by making a toxin called Shiga toxin. The bacteria that make these toxins are called “Shiga toxin-producing” E. coli, or STEC for short. The most commonly identified STEC in North America is E. coli O157:H7 (often shortened to E. coli O157 or even just “O157”).
In addition to E. coli O157, many other kinds (called serogroups) of STEC cause disease. These other kinds are sometimes called “non-O157 STEC.” E. coli serogroups O26, O111, and O103 are the non-O157 serogroups that most often cause illness in people in the United States. Outbreaks for the E. coli serogroup O145 are very rare.
On April 16, 2010, the Centers for Disease Control and Prevention (CDC) was notified of a cluster of cases of non-O157 Shiga-toxin producing E. coli (STEC) infection by the Michigan Department of Community Health (MIDOCH). On April 22, the Ohio Department of Health (ODH) also reported to the CDC a cluster of cases of non-O157 in Franklin County. On April 30, ODH requested an Epi-Aid to Ohio to assist ODH and Columbus Public Health (CPH) in conducting an epidemiological investigation of the outbreak. As the investigation progressed, other local and state public health officials - New York, Pennsylvania and Tennessee reported cases of E. coli O145 associated with the outbreak in Franklin County. Subsequently, investigators from the local and state health departments, the CDC Epi-Aid team, Ohio Department of Agriculture and the Food and Drug Administration were able to link these illnesses to a common supplier of romaine lettuce. In Franklin County, 11 people were associated with the outbreak, eight cases were confirmed and three cases were classified as probable. The results of the investigation lead to a market withdrawal of potentially contaminated romaine lettuce in May, 2010.
0
1
2
3
4
Case
s
Date
Confirmed (N=8) Probable (N=3)
E. COLI O145 (NON-O157 STEC) SELECTED OUTBREAK INVESTIGATIONS 2010
Columbus Public Health & Franklin County Public Health 8 July 2012
CLUSTER OF E. COLI O145 CASES BY ONSET DATEFRANKLIN COUNTY, 2010
0
20
40
60
80
100
120
140
160
180
200
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Case
s
Month
Confirmed Cases (N=604) Probable Cases (N=15) Suspected Cases (N=345)
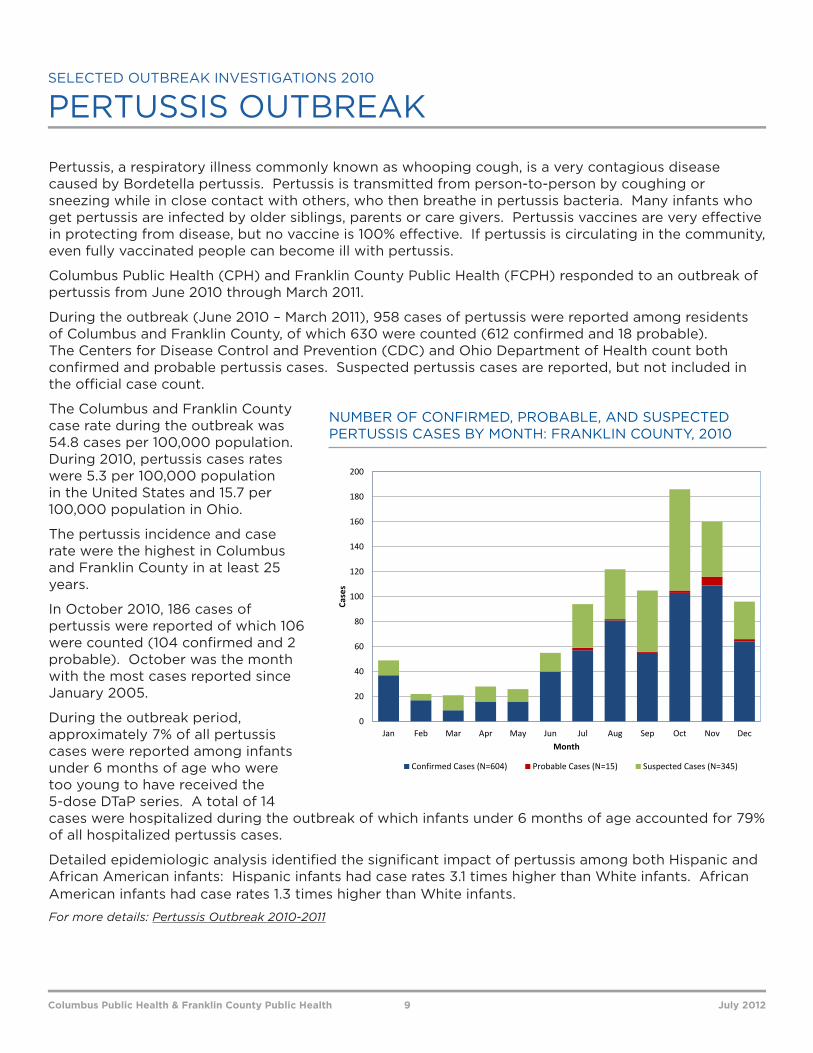
Pertussis, a respiratory illness commonly known as whooping cough, is a very contagious disease caused by Bordetella pertussis. Pertussis is transmitted from person-to-person by coughing or sneezing while in close contact with others, who then breathe in pertussis bacteria. Many infants who get pertussis are infected by older siblings, parents or care givers. Pertussis vaccines are very effective in protecting from disease, but no vaccine is 100% effective. If pertussis is circulating in the community, even fully vaccinated people can become ill with pertussis.
Columbus Public Health (CPH) and Franklin County Public Health (FCPH) responded to an outbreak of pertussis from June 2010 through March 2011.
During the outbreak (June 2010 – March 2011), 958 cases of pertussis were reported among residents of Columbus and Franklin County, of which 630 were counted (612 confirmed and 18 probable). The Centers for Disease Control and Prevention (CDC) and Ohio Department of Health count both confirmed and probable pertussis cases. Suspected pertussis cases are reported, but not included in the official case count.
The Columbus and Franklin County case rate during the outbreak was 54.8 cases per 100,000 population. During 2010, pertussis cases rates were 5.3 per 100,000 population in the United States and 15.7 per 100,000 population in Ohio.
The pertussis incidence and case rate were the highest in Columbus and Franklin County in at least 25 years.
In October 2010, 186 cases of pertussis were reported of which 106 were counted (104 confirmed and 2 probable). October was the month with the most cases reported since January 2005.
During the outbreak period, approximately 7% of all pertussis cases were reported among infants under 6 months of age who were too young to have received the 5-dose DTaP series. A total of 14 cases were hospitalized during the outbreak of which infants under 6 months of age accounted for 79% of all hospitalized pertussis cases.
Detailed epidemiologic analysis identified the significant impact of pertussis among both Hispanic and African American infants: Hispanic infants had case rates 3.1 times higher than White infants. African American infants had case rates 1.3 times higher than White infants.
For more details: Pertussis Outbreak 2010-2011
PERTUSSIS OUTBREAK SELECTED OUTBREAK INVESTIGATIONS 2010
NUMBER OF CONFIRMED, PROBABLE, AND SUSPECTED PERTUSSIS CASES BY MONTH: FRANKLIN COUNTY, 2010
Columbus Public Health & Franklin County Public Health 9 July 2012
TIMELINESS OF DISEASE REPORTS
Timeliness of disease reports is a key part of good public health practice. In order to reduce the burden of disease in our community and to implement appropriate interventions, the public health system relies on healthcare providers and laboratories for identification of infectious diseases. Timeliness requirements for each reportable disease vary based on the communicability and severity of the disease.
In the Ohio Disease Reporting System (ODRS) application, it is possible to query the date when a healthcare provider diagnosed an illness and when the local health department was able to receive notification of the illness i.e., the date a case was reported to the local health department.
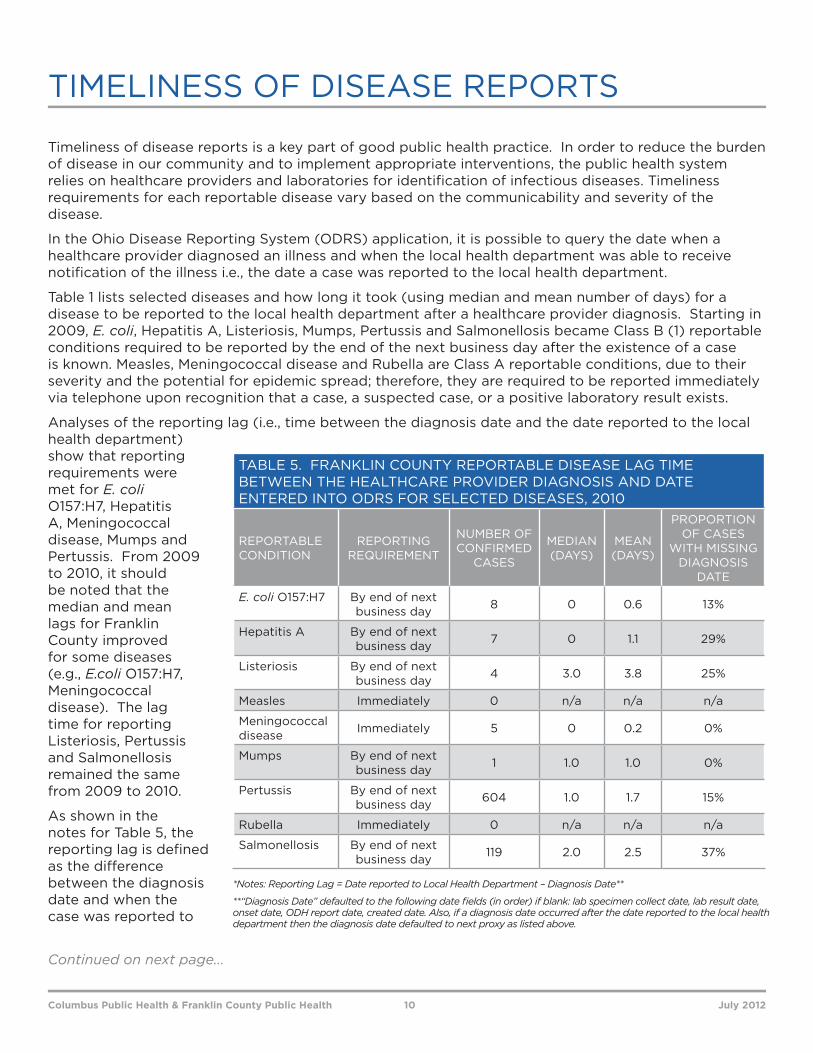
Table 1 lists selected diseases and how long it took (using median and mean number of days) for a disease to be reported to the local health department after a healthcare provider diagnosis. Starting in 2009, E. coli, Hepatitis A, Listeriosis, Mumps, Pertussis and Salmonellosis became Class B (1) reportable conditions required to be reported by the end of the next business day after the existence of a case is known. Measles, Meningococcal disease and Rubella are Class A reportable conditions, due to their severity and the potential for epidemic spread; therefore, they are required to be reported immediately via telephone upon recognition that a case, a suspected case, or a positive laboratory result exists.
Analyses of the reporting lag (i.e., time between the diagnosis date and the date reported to the local health department) show that reporting requirements were met for E. coli O157:H7, Hepatitis A, Meningococcal disease, Mumps and Pertussis. From 2009 to 2010, it should be noted that the median and mean lags for Franklin County improved for some diseases (e.g., E.coli O157:H7, Meningococcal disease). The lag time for reporting Listeriosis, Pertussis and Salmonellosis remained the same from 2009 to 2010.
As shown in the notes for Table 5, the reporting lag is defined as the difference between the diagnosis date and when the case was reported to
TABLE 5. FRANKLIN COUNTY REPORTABLE DISEASE LAG TIME BETWEEN THE HEALTHCARE PROVIDER DIAGNOSIS AND DATE ENTERED INTO ODRS FOR SELECTED DISEASES, 2010
REPORTABLE CONDITION
REPORTING REQUIREMENT
NUMBER OF CONFIRMED
CASES
MEDIAN (DAYS)
MEAN (DAYS)
PROPORTION OF CASES
WITH MISSING DIAGNOSIS
DATE
E. coli O157:H7 By end of next business day 8 0 0.6 13%
Hepatitis A By end of next business day 7 0 1.1 29%
Listeriosis By end of next business day 4 3.0 3.8 25%
Measles Immediately 0 n/a n/a n/a
Meningococcal disease Immediately 5 0 0.2 0%
Mumps By end of next business day 1 1.0 1.0 0%
Pertussis By end of next business day 604 1.0 1.7 15%
Rubella Immediately 0 n/a n/a n/a
Salmonellosis By end of next business day 119 2.0 2.5 37%
*Notes: Reporting Lag = Date reported to Local Health Department – Diagnosis Date**
**“Diagnosis Date” defaulted to the following date fields (in order) if blank: lab specimen collect date, lab result date, onset date, ODH report date, created date. Also, if a diagnosis date occurred after the date reported to the local health department then the diagnosis date defaulted to next proxy as listed above.
Columbus Public Health & Franklin County Public Health 10 July 2012
Continued on next page...

the local health department. If the diagnosis date field was empty, a proxy date was used. These fields were used (in this order) as the proxy: lab specimen collect date, lab result date, onset date, date reported to ODH and date the record was created by the local health department. The diagnosis date field was blank (and a proxy date needed) for a minimum of 13% of cases up to a maximum of 37% of cases for selected diseases. The percentage of cases missing diagnosis date has improved from 2009, when a minimum of 20% of cases to a maximum of 45% of cases for selected diseases were missing the diagnosis date.
CPH and FCBH will periodically monitor the reporting lag times for these diseases. Regular monitoring will help with two key issues: late reporters and missing data. If specific reporters are found to be contributing to longer lags, this information will be shared with them, challenges to timely reporting will be identified and addressed, and closer monitoring of reports will follow. Additionally, filling in missing or incorrect dates will aid in better, more timely interventions and prevention efforts.
Columbus Public Health & Franklin County Public Health 11 July 2012
TIMELINESS OF DISEASE REPORTS, continued
The Ohio Administrative Code 3701-3-02, 3701-5-05, and 3701-3-12 requires by law that communicable diseases be reported to local health departments. Reportable diseases are grouped by class. All the diseases in this summary are class A and B, which is defined as: Disease of major public health concern because of the severity of disease or potential for epidemic spread.
CASE CRITERIA AND DEFINITIONSFor nationally reportable diseases, case definitions are determined by the Council of State and Territorial Epidemiologists (CSTE) in conjunction with the CDC and are published in the MMWR [1997; 46(RR-10)].
In Ohio, case definitions can be found in the Infectious Disease Control Manual.
DISEASES NOT INCLUDED IN THE TABLE 4There were no confirmed cases in Franklin County of the following Class B (1) & (2) reportable diseases; therefore, they were not included in the table: Arboviral neuroinvasive and non-neuroinvasive disease, Chancroid, Cyclosporiasis, Creutzfeldt-Jakob disease, Granuloma Inguinale, Hepatitis D, Hepatitis E, LaCrosse virus disease, Powassan virus disease, Q fever, Toxic shock syndrome (TSS) and Trichinosis. Class C reports are also not included in the table.
NOTES ON REPORTING SYSTEMSData are from the Ohio Department of Health and the Infectious Disease Reporting System (IDRS, a joint effort between Columbus Public Health Department and the Franklin County Public Health). Cases of sexually transmitted diseases, tuberculosis, AIDS, and HIV have separate reporting systems. Cases may have been excluded due to the reporting time, onset date, or when the supplemental information was received.
The Ohio Disease Reporting System (ODRS) was developed as a web-based system to make disease reporting more timely and efficient for disease reporters (e.g. hospitals, laboratories and physicians), and to improve communication about infectious diseases between disease reporters, local health departments, and ODH. Currently, ODH, local health departments and infection control preventionists have the ability to enter and update case and laboratory reports into ODRS. The system uses patient’s address to determine the correct local health jurisdiction in which to electronically send the report for follow-up and investigation. In addition, some laboratories have the ability to electronically up-load batches of reports via Electronic Laboratory Reporting (ELR) from their databases into ODRS, minimizing paperwork and re-entry. If a disease report is inadvertently assigned to an incorrect health jurisdiction, the health department receiving the report can re-direct it to the correct one. Updates to information can be made to the record in the database, and all fields in the ODH and CDC reporting forms are included in ODRS.
TECHNICAL NOTES
Columbus Public Health & Franklin County Public Health 12 July 2012
Centers for Disease Control and Prevention, Disease Factsheets A-Z.
Centers for Disease Control and Prevention - National Center for Immunization and Respiratory Diseases, National Center for Emerging and Zoonotic Infectious Diseases, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
Infectious Disease Reporting System, Disease Factsheets A-Z
Evaluation of Reporting Timeliness of Public Health Surveillance Systems for Infectious Diseases:Ruth Ann Jajosky1 and Samuel L Groseclose2, 3
Published online at BioMed Central, 2004 July 26. doi: 10.1186/1471-2458-4-29. PMCID: PMC50925http://www.biomedcentral.com/content/pdf/1471-2458-4-29.pdf
The Ohio Department of Health Infectious Disease Control Manual: http://www.odh.ohio.gov/healthResources/infectiousDiseaseManual.aspx
REFERENCES
Columbus Public Health & Franklin County Public Health 13 July 2012

















