•Positioning – turn infant with affected lung down
• Thoracentesis/chest tube
• Affected side up
• If asymptomatic will often resolve without treatment
PNEUMOTHORAX
13
14
1/25/2021
8
REFERENCES
•Gardner, S. L., Carter, B. S., Hines, M. E. & Hernandez, J. A. (2016). Merenstein & gardner’s handbook of neonatal intensive care (8th
ed.). St Louis, MO: Elsevier.
•Karlsen, K. (2013) Post-resuscitation / Pre-transport Stabilization care of sick infants: Guidelines for neonatal healthcare providers (5th ed). Salt Lake City, UT: S.T.A.B.L.E program.
•Verklan, M. T. & Walden, M. (2015) Core curriculum for intensive care nursing (5th ed). St. Louis, MO: Elsevier.
BLOOD GAS INTERPRETATIONStabilization of the Newborn
2020
Ashley Denker, MSN
Sheri Kimmey, MSN
15
16
1/25/2021
9
OXYGENATION
•Oxygenation refers to the supply of oxygen to the tissues
•Oxygenation is affected by cardiac output and O2 bonded to hemoglobin in blood
•O2 saturation – Percentage of hemoglobin carrying oxygen SaO2 – on monitor, PaO2 – lab value
•Hypoxemia – decrease O2 at blood level (amount of O2 carried in the blood)
•Hypoxia – decreased O2 at tissue level
GAS EXCHANGE
•The exchange of oxygen and carbon dioxide between air and blood and then blood and tissue
•Takes place in the alveoli of the lung
•Exchange of oxygen is reflected in the PaO2 (partial pressure of oxygen). PaO2 measures oxygen in arterial blood (“a” in PaO2 means arterial)
•Adequate respiration and cardiac function are necessary for oxygenation and ventilation
17
18
1/25/2021
10
BLOOD GAS COMPONENTS
•pH - numerical value based on hydrogen ions present (H+)
•PaCO2 - the partial pressure of carbon dioxide found in arterial blood
•PaO2 - the partial pressure of oxygen found in arterial blood
•Bicarbonate - the calculated value of the amount of bicarbonate in the blood (HCO3-)
•Base excess (BE) / Base deficit (BD) is another way of looking at the amount of bicarb in the blood. Normal value is -2 to +2 with 0 being ideal
•pO2 Saturation - percentage of hemoglobin carrying oxygen
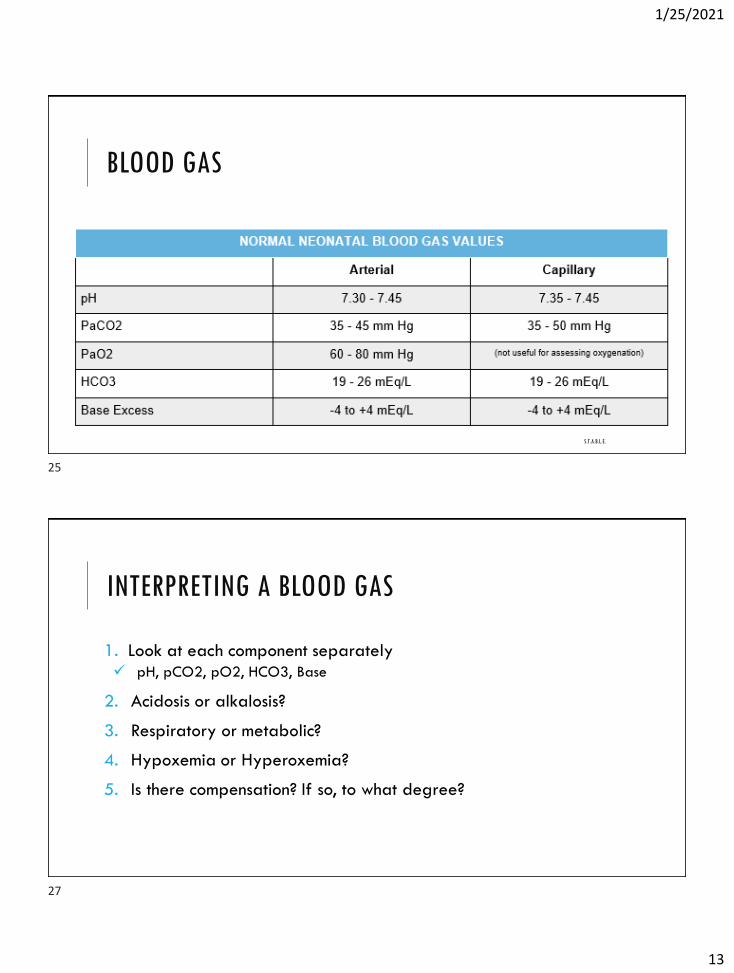
pH
Normal pH ranges are 7.35 - 7.45
Values outside the normal range determine whether acidosis or alkalosis is present
Acidosis: < 7.35
Alkalosis: > 7.45
19
20
1/25/2021
11
PaCO2
•35 – 45 mmHg
•Indication of alveolar ventilation
•Acidity = > 45 mmHg
•Alkalinity = < 35 mmHg
•Think of CO2 as an acid
PaO2
60 – 80 mmHg
Hypoxemia = PaO2 < 60 mmHg
Hyperoxemia = PaO2 > 80 mmHg
21
22
1/25/2021
12
HCO3
•19 – 26 mEq/L
•Renal component of blood gas
•Acidosis = decreased amounts
•Alkalosis = increased amounts
•Think of HCO3 as a base
BASE DEFICIT/EXCESS
-4 to +4
Reflects the concentration of buffer/base available in the blood
Base deficit = metabolic acidosis
Base excess = metabolic alkalosis
23
24
1/25/2021
13
BLOOD GAS
S.T.A.B.L.E.
INTERPRETING A BLOOD GAS
1. Look at each component separately
✓ pH, pCO2, pO2, HCO3, Base
2. Acidosis or alkalosis?
3. Respiratory or metabolic?
4. Hypoxemia or Hyperoxemia?
5. Is there compensation? If so, to what degree?
25
27
1/25/2021
14
COMPENSATION
•Look at system not at fault
•Absent compensation – system not at fault within normal limits
•Partial compensation – opposite system and pH not within normal limits
•Complete compensation – opposite system not within normal limits, pH normal
•What happens on the acid side will be balanced on the base side and vice versa• If the base side declines, the infant will try to blow off CO2 to compensate for the change on the base side
• The purpose of compensation is to maintain a normal pH
RESPIRATORY ACIDOSIS
•Results from the formation of excess carbonic acid because of increased pCO2
•Caused by insufficient alveolar ventilation
•pH –
•pCO2 –
•HCO3 – normal
28
29
1/25/2021
15
RESPIRATORY ACIDOSIS
•Hypoventilation
•Sedation
•PPH
•RDS
•Upper airway not patent
•Pulmonary hypoplasia
•Recurrent apnea
•Central depression
•Pneumothorax
RESPIRATORY ACIDOSIS COMPENSATION
•Over 3 - 4 days, the kidneys increase the rate of H+ secretion and HCO3 reabsorption
•pH – low normal
•pCO2 –
•HCO3 –
30
31
1/25/2021
16
RESPIRATORY ALKALOSIS
•Results from alveolar hyperventilation leading to a deficiency of carbonic acid
•Caused by hyperventilation
•pH –
•pCO2 –
•HCO3 – normal
RESPIRATORY ALKALOSIS COMPENSATION
•The kidneys decrease H+ secretion by retaining chloride and excreting fewer acid salts. HCO3 reabsorption is decreased.
•pH – high normal
•CO2 –
•HCO3 –
32
33
1/25/2021
17
METABOLIC ACIDOSIS
•A deficiency in the concentration of HCO3 in the extracellular fluid
•Caused by any system disease that increases acid production or retention, or problems leading to excessive base losses.
•pH –
•CO2 – normal
•HCO3 –
METABOLIC ACIDOSIS
•Hyperalimentation
•Hypoperfusion/hypovolemia
•PDA
•Rental tubular acidosis
•Cold stress
•Renal failure
•Inborn error of metabolism
•Sepsis
34
35
1/25/2021
18
METABOLIC ACIDOSIS COMPENSATION
•Healthy lungs will blow off additional CO2 through hyperventilation.
•If renal disease is not a problem, the kidneys will respond by increasing the excretion of acid salts and the reabsorption of HCO3.
•pH – low normal
•pCO2 –
•HCO3 –
METABOLIC ALKALOSIS
•Results from an excess concentration of HCO3 in the extracellular fluid
•Caused by problems leading to increased los of acid.
•pH –
•CO2 – normal
•HCO3 –
36
37
1/25/2021
19
METABOLIC ALKALOSIS COMPENSATION
•The lungs compensate by retaining carbon dioxide through hypoventilation.
•pH – high normal
•CO2 –
•HCO3 –
IMPROVING VENTILATION: CO2 ELIMINATION
•Increasing the rate
•Increase the PIP or tidal volume
•Increase the expiratory time
•Increase the flow
38
39
1/25/2021
20
IMPROVING OXYGENATION: INCREASE PaO2
•Increase the FiO2
•Increase PIP or tidal volume
•Increase the inspiratory time
•Increase the flow
PRACTICE
7.36
40
24
Normal
40
41
1/25/2021
21
PRACTICE
7.28
62
24
Respiratory acidosis
PRACTICE
7.28
54
28
Respiratory acidosis – partially compensated
42
43
1/25/2021
22
PRACTICE
7.22
40
20
Metabolic acidosis – no compensation
PRACTICE
A 31 weeker is one hour old. CXR shows diffuse atelectasis with air bronchograms
CBG
•7.29
•59
•42
•26
44
45
1/25/2021
23
PRACTICE
A 33 weeker on mechanical ventilation for severe TTN.
Settings: IMV 25, PIP 18, PEEP 4, .30
ABG
•7.49
•26
•95
•22
PRACTICE
A 26 weeker on mechanical ventilation for 2 weeks for RDS. PIE is present
CBG
•7.37
•55
•65
•29
46
47
1/25/2021
24
PRACTICE
Term infant with tight nuchal cord. Infant pale, grunting, with cap refill of 8 seconds.
ABG
•7.15
•40
•75
•15
• -15
REFERENCES
•Gardner, S. L., Carter, B. S., Hines, M. E. & Hernandez, J. A. (2016). Merenstein & gardner’s handbook of neonatal intensive care (8th
ed.). St Louis, MO: Elsevier.
•Karlsen, K. (2013) Post-resuscitation / Pre-transport Stabilization care of sick infants: Guidelines for neonatal healthcare providers (5th ed). Salt Lake City, UT: S.T.A.B.L.E program.
•Verklan, M. T. & Walden, M. (2015) Core curriculum for intensive care nursing (5th ed). St. Louis, MO: Elsevier.
•Weir, C. (n.d.). Interpreting ABGS – as easy as 1-2-3.