21
Results of the initial analysis on strain-based reporting Eeva Broberg, Olav Hungnes, Adam Meijer, Katarina Prosenc, Brunhilde Schweiger
| Date post: | 06-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | european-centre-for-disease-prevention-and-control |
| View: | 40 times |
| Download: | 1 times |

Results of the initial analysis on strain-based reporting
Eeva Broberg, Olav Hungnes, Adam Meijer, Katarina Prosenc, Brunhilde Schweiger
2
Background
• Discussions with the network since 2010 of enhancing the data collection towards molecular surveillance
• Strain-based reporting for antigenic and genetic characterisation was implemented in TESSy as a pilot in 2013-2014 season
• Variables for antigenic group and genetic clade added to existing antiviral susceptibility data collection
• Sequence accession numbers reported in existing variables
• Used existing reporting scheme for strain-based antiviral data

3
Objective
To analyse the benefits of strain-based over the aggregated reporting through sub-objectives of:
1) To test the feasibility of strain-based reporting of antigenetic/genetic data to TESSy;
2) To study the representativeness of virus characterisation
3) To monitor the evolution of influenza viruses over time
4) To continue monitoring of antiviral susceptibility
5) To analyse distribution of virus (sub)types, genetic clades and antigenic groups by age and gender or any other variable with sufficient completeness.

4
Methods
• Influenza virological data were retrieved from TESSy for the 2013-2014 season.
• Antigenic and genetic data were reported both in aggregate and strain-based manner by the pilot countries
• Descriptive analysis was performed

5
Reporting countries
11 countries agreed to take part in the pilot and found this feasible.
N=1,633
BE DE EL ES FI IE IT NL NO PT SE0
100
200
300
400
500
600
Characterisation data by country
AGAG and GENGEN
Num
ber
of r
ecor
ds

6
Data completeness
subt
ype
repo
rting
cou
ntry
age
gend
er
antig
enic
grou
p
gene
tic cla
de
HA ISD n
r
hosp
italis
atio
n
outc
ome
vacc
inat
ion
stat
us
date
of o
nset
0102030405060708090
100
meaningful completeness (excl. unknowns)
Variable
%

7
Age and gender distribution – no difference by gender
<1
01-05
06-19
20-39
40-64
>=65
250 200 150 100 50 0 50 100 150 200 250
M F
Number of cases
Age-group (y)
Kruskal-Wallis equality of populations, gender vs age-group, p=0.1611; gender vs. subtype p=0.2849

8
Detections and strain-based records
Aggregated detections Strain-based recordsProportion of strain-
based out of detections (%)
SentinelNon-sentinel
Total SentinelNon-sentinel
Unknown Total SentinelNon-sentinel
Total
A(H1N1)pdm09 2089 7690 9779 237 505 5 747 11.3 6.6 7.6
A(H3N2) 1714 3219 4933 311 464 4 779 18.1 14.4 15.8
B (lineage not determined)
60 663 723 0 0 0 0 0.0 0.0 0.0
B(Victoria) 7 9 16 9 11 0 20 128.6 122.2 125.0
B(Yamagata) 50 168 218 29 57 1 87 58.0 33.9 39.9
Total detections (aggregate) or reports (strain-based)
3920 11749 15669 586 1037 10 1633 14.9 8.8 10.4
Nr of specimens 11631 112571 124202 In strain-based the number of specimens is the total of reports.

9
Timing of strain-based records - A(H1N1)pdm09
detections
antigenic characterisations
genetic characterisations

10
Timing of strain-based records - A(H3N2)
detections
antigenic characterisations
genetic characterisations

11
Genetic evolution of viruses – example: B(Yam)
2015-2016 vacc.
2013-2014 vacc.

12
Antiviral susceptibility
-2
-1
0
11.0
1.2
1.4
1.6
1.8
2.02
3
4
5
A(H1N1)pdm09
Antiviral drug
IC50 fold
change (
10lo
g)
I223R (n=1)
S247I (n=1)? (n=1)
HR
IR
IN
I
D199N
D199N
-2
-1
0
11.0
1.2
1.4
1.6
1.8
2.02
3
4
5
A(H3N2)
Antiviral drug
IC50 fold
change (
10lo
g) ?
HR
IR
IN
I?
?
-2
-1
0
0.8
1.0
1.2
1.4
1.6
2
3
4
5
B
Antiviral drug
IC50 fold
change (
10lo
g) ?
HR
IR
IN
I
A(H1N1)pdm09 A(H3N2) B
13
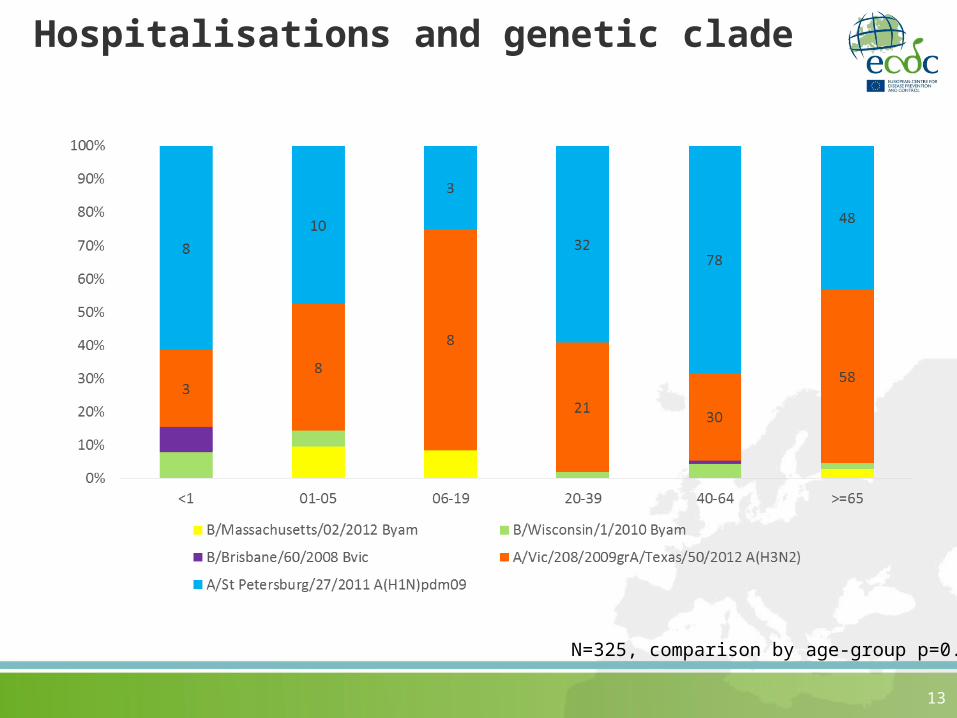
Hospitalisations and genetic clade
N=325, comparison by age-group p=0.0190

14
Genetic clade by age-group
N=1061, comparison by age-group, p=0.0014

15
Age distribution H3 clades during 2014/2015 season
~80% 3C.3b
16
Limitations
– Specimen selection for characterisation is based on individual laboratories’ decision, however, aiming for best possible representativeness by subtype, age, gender, severity and geographic location
– Not population-based or based on a specific study design
– This was a pilot, not an European-wide study– Provision of data by countries was not equal;
resource and approach differences– Data completeness for some variables such as
outcome and vaccination status was low

17
Benefits of strain-based reporting
- Opportunity for deeper analysis- Validation possibility between genetic clade,
antigenic group and subtype reporting- Is of even more value in a season where a variant
strain emerges, e.g. in 2014/15 season where it was possible to analyse the deviation from the vaccine strain
- Gives a “fingerprint” or “pattern” of the season in terms of demographic or e.g. hospitalisation status

18
What the strain-based reporting does not allow
- Draw strong conclusions about severity, mortality and vaccination status as the data is based on surveillance from both sentinel and non-sentinel sources without an agreed sampling scheme especially for the non-sentinel in different countries

19
Conclusions
• Strain-based reporting should be recommended to all countries as it enhances understanding of circulation of influenza viruses in different populations
• Ca 10% of all detections were characterised• Good representation of different age-groups and
genders in data• Timing of characterisations matching well with the
epidemic • Genetic analysis shows e.g. that B/Yamagata Phuket-
strains were in circulation already in season 2013-2014
• Only a few viruses with reduced inhibition to oseltamivir or zanamivir reported from the pilot countries during the season
• Distribution of genetic clades by age-groups differs

20
Acknowledgements
Strain-based reporting country contact points:Isabelle Thomas, Belgium
Niina Ikonen, Finland
Brunhilde Schweiger, Germany
Thanos Kossyvakis, Greece
Allison Waters, Ireland
Isabella Donatelli, Italy
Adam Meijer, Netherlands
Olav Hungnes, Norway
Raquel Guiomar, Portugal
Inmaculada Casas, Spain
Mia Brytting, Sweden
Rod Daniels, WHO CC
Adrian Prodan, ECDC
Working group members: Olav, Adam, Katarina, Bruni
21
Questions to the WG
1. Do you agree with
• the added value of strain-based reporting?
• closing the aggregate reporting after season 2016/17?
2. What type of outputs do you expect with the new reporting and how often?
3. What needs to you have in your institute for support for implementation of strain-based reporting?
4. How can we improve the completeness of the data?
5. Are there possibilities to combine this data with the SARI/ICU reporting?
6. How can we improve the representativeness of the sampling? Should a separate study take place to assess the representativeness?

















