Seizure activity in the neonatal foal can result fromcerebral trauma, central nervous system inflamma-tion or infection, compressive intracranial lesions,cerebral edema, congenital epilepsy, or electrolytedisturbances secondary to systemic illness. Be-cause the cause of the seizure activity may notreadily be apparent, the first goal of therapy is tocontrol seizure activity and prevent secondary phys-ical injury. Once seizure activity is stabilized, de-termination of any underlying medical conditionscan proceed with an assessment of the systemichealth and metabolic state of the neonate.
2. Seizure Recognition
Seizure activity is an indication of forebrain neu-rological dysfunction as the result of abnormalelectrical activity within the brain. Involuntary,spontaneous muscle contractions are accompaniedby varying degrees of loss of consciousness. Sei-zures may be further divided into focal or partial(initially involving a small part of the brain withlimited manifestations) or generalized (widespreadinvolvement of the brain with recumbency and loss
of consciousness possible). Partial seizures do notnecessarily progress into general seizures. Sei-zures of cerebral origin often remain predictable andnon-progressive with respect to their severity andduration. However, when caused by an underlyingsystemic problem, seizure activity often worsenswith any deterioration in the precipitating diseaseprocess.
Three phases of a seizure episode are recognized.The pre-ictal period may involve depression, abnor-mal activity, and star-gazing. The ictal period(overt seizure) encompasses the recognized manifes-tations of seizure activity: paroxysmal muscle con-traction and altered consciousness. The post-ictalphase is one of depression and possible transientloss of neurological function (e.g., central blindness).
Diagnosis of seizure activity in the neonatal foal ischallenging but an essential component of successfulmanagement of the condition. Only subtle signssuggestive of seizure activity may be displayed.These include any or all of the following: abnormaleye movements, tremors, excessive stretching whenrecumbent, excessive extensor tone, hyperaesthesiato touch and attempts at physical manipulation, and
22 2009 � Vol. 55 � AAEP PROCEEDINGS
MEDICINE—FOAL
NOTES
apneustic breathing.1 Overt seizure activity is eas-ier for the clinician to detect: manifestations includ-ing rapid nystagmus, paddling, focal, or generalizedmuscle fasciculations, hyperextension of the limbsand neck, excessive mouth movements (chewinggum fits), and occasionally abnormal vocalization.
Further complicating diagnosis are unobservedepisodes of seizure activity. The presence of unex-plained physical trauma, for example, nasolabialand gingival excoriation, may be the only evidence ofneurological dysfunction (Fig. 1).
3. Pathogenesis of Seizure Activity
Disruption of neural tissue, whether as a result ofinfection, ischemia, or trauma, involves many pro-cesses including vascular and cellular disruption, freeradical production, breakdown of cell membrane lip-ids, and the release of inflammatory mediators.Apoptosis of neurons occurs as a result of aberrant Caintakes and excitotoxic neurotransmitter release.
Loss of astrocyte functions during cerebral ischemiaalso affects neuronal cell viability.2 Astrocytes pro-vide structural, nutritional and metabolic support toneurons. Furthermore, synaptic activity and glu-tamate uptake are regulated, free radicals are scav-enged, and local inflammatory mediator productionis modulated.
Excitatory amino acids (including glutamate, as-partate) have been shown to be the final commonpathway in many neurologic disorders. Activationof glutamate receptors allows an excessive influx ofcalcium into neurons through ionic channels. Neu-ronal swelling results, with the subsequent mem-brane damage and cell death releasing furtherglutamate from intracellular storage vesicles, facil-
itating a self-sustaining cycle of cell damage andaberrant electrical activity.3
4. Conditions Associated With Seizure or Seizure-LikeActivity
Seizure disorders of the foal can result from compro-mise of the dam or placenta during the fetal periodor from disease processes encountered by the neona-tal foal including hypoxic insult and sepsis. Medi-cal management of the foal at risk from the onset ofseizure activity should ensure adequate ventilation(avoid hypercapnia that leads to central depression),prevention of hypotension, avoidance of hypoglyce-mia/hyperglycemia, and control of any detectedseizure activity.4 Underlying medical conditions(infectious, inflammatory, developmental, congeni-tal) must be managed, and any lesions amenable tosurgical correction addressed concurrently with sei-zure control.
Hypoxic Ischemic Encephalopathy and Perinatal AsphyxiaSyndromeThe result of cerebral hypoxic or ischemia insult tothe neonate, hypoxic ischemic encephalopathy andperinatal asphyxia syndrome (HIE/PAS) is arguablythe most common seizure precipitating syndromefaced by the equine clinician. Excitatory amino ac-ids, calcium ions, free radicals, NO, pro-inflamma-tory cytokines, and products of lipid peroxidationare all thought to contribute to the HIE/PAS syn-drome. Compared with the adult, the immatureneonatal brain seems to have an increased suscep-tibility to excitotoxic and free radical damage, withan increased propensity for apoptotic cell death.5,6
The diagnosis of HIE/PAS is dependent on a com-patible history and clinical examination findingswhile ruling out other conditions.1 Confounding di-agnosis, sepsis and major organ dysfunction mayoccur concurrently. Depressed pulmonary function(decreased ventilation) promotes retention of CO2,leading to central depression and abnormal acid-base balance. Renal compromise (ischemia) can re-sult in electrolyte (sodium) and fluid balancederangements. With the loss of normal gastroin-testinal motility and integrity, intestinal bacterialovergrowth can lead to diarrhea and sepsis.
In the neonatal foal, many recommendations forthe treatment of neurological dysfunction resultingfrom HIE/PAS are empirical and extrapolated fromother species.7
Trauma
Trauma was the cause of 22% of central nervoussystem disorders in one equine study.8 In additionto episodes of seizure activity, trauma can lead toabnormal mentation, gait, and posture. Mild casesoften present with subtle neurological deficits,whereas in others, spinal reflexes may be dimin-ished. Severe cases can present in recumbency.
With any case of overt trauma, there may be di-rect injury of the neural tissue itself. Onset of neu-
Fig. 1. Overt seizure activity may not be noted; unexplainedtrauma may therefore be the only indication of neurologicaldysfunction.
AAEP PROCEEDINGS � Vol. 55 � 2009 23
MEDICINE—FOAL
rological signs may be delayed because thepathophysiology of central nervous system (CNS)injury is complex and progressive. Ongoing hem-orrhage or swelling of neural tissue within the bonyconfinement of the calvarium, sudden displacementof bony fragments, and disturbances of blood pres-sure and perfusion exacerbate the initial cerebralinsult.
Metabolic Derangement
Glucose levels are frequently abnormal in thecompromised neonate, with both hypoglycemiaand hyperglycemia potentially having effects onneurological function. Additionally, although otherelectrolyte disturbances occur, derangements of so-dium and calcium are the most relevant with respectto neonatal seizure disorders.
Hypoglycemia
Considering human neonatal glucose concentrationsin isolation, insufficient information is currently avail-able to determine a minimum value of glucose occur-ring during the neonatal period (for any one time orany period of time) below which irreparable hypogly-cemic injury to the central nervous system ensues.9
However, hypoxia, neonatal seizure, and pathologicaljaundice have been shown to exacerbate hypoglycemicbrain injuries in cases of severe and prolonged neona-tal hypoglycemia.10 Hypoglycemia itself has beenshown to be a risk factor for perinatal brain injury interm infants who require resuscitation and those thathave suffered severe fetal acidemia.11
In a recent review, foals with lower mean bloodglucose concentrations at admission or high maxi-mum and low minimum blood glucose concentra-tions within the first 24 h of hospitalization wereless likely to survive to discharge. This wasthought not to be a result of hypoglycemia causingcerebral dysfunction, but a result of the associationof hypoglycemia with sepsis, bacteremia, and thesystemic inflammatory response syndrome (SIRS).12
The effect of hypoglycemia on seizure activity istherefore not proven.
Hyponatremia and Hypernatremia
The brain has limited ability to adapt to alterationsin serum osmolarity. It is the rapidity with whichthe sodium disturbance develops that determines ifhyponatremia and hypernatremia cause overtneurological deficits. Acute hyponatremia re-sults in cerebral edema caused by the osmoticdraw of the hypertonic cell interior. Seizure ac-tivity, blindness, and depression can result be-cause of compression of the brain against the bonycalvarium. Chronic hyponatremia is less likelyto produce neurologic symptoms because osmoticequilibrium has time to occur. The rapid correc-tion of hyponatremia is likely to cause neurologi-cal signs because of increased plasma osmolality,causing cell shrinkage by the osmotic draw of wa-ter from cells.13
By the same osmotic draw, acute hypernatremiamay cause shrinkage of brain parenchyma. Aswith other causes of cerebral injury, neurons pro-duce idiogenic osmoles (osmotically active metabolicbyproducts) in an attempt to counter the extra-cellular hyperosmolality by maintaining intracellu-lar osmotic draw. Unfortunately, these compoundspromote intracellular edema during correction of hy-pernatremia if the rate of correction is not carefullymonitored. Parenchymal hemorrhages may occurthrough tearing of bridging veins, with these some-times progressing to subdural hematomas in severecases causing compression of the brain.
Hypocalcemia
Seizure activity (focal or generalized) is the mostcommon central neurologic manifestation of hy-pocalcemia. Agitation, confusion, and depressionmay also occur. Tetany is the most frequently rec-ognized peripheral nervous system symptom ofhypocalcemia. When the ionized calcium concen-tration reaches a low enough level, the nerve cellmembrane electrical potential reaches a level allow-ing spontaneous discharge, leading to clusters ofirregular, repetitive action potentials. In a case se-ries reported by Beyer et al.,14 five foals with lowmeasured and corrected total serum calcium showedneuromuscular signs including recumbency and sei-zure-like activity. Corrected total serum calciumlevels were �7.5 mg/dl in all the affected foals.Ionized calcium levels for those foals measured werebelow the normal reference range for the consultinglaboratory (�1.58 mM).
Hepatic Compromise
Hepatic dysfunction leads to the systemic accumu-lation of � amino butyric acid (GABA) and otherundesirable metabolic products such as ammonia.Branched chain amino acids decrease and aromaticamino acids increase. Centrally, these metabolicchanges alter the ratio of GABA (inhibitory) andL-glutamate (excitatory) amino acids in favor of sei-zure propagation. Endogenous benzodiazepine-like compound concentration is increased, leading tocentrally mediated depression.
Hyperbilirubinemia
Bilirubin has many toxic intracellular effects. Oxi-dative phosphorylation is curtailed, membranestructure and function are changed, neurotransmit-ter metabolism is inhibited, and cell regulatoryproteins are altered in structure and function.Prematurity/immaturity, hemolysis, asphyxia, aci-dosis, sepsis, and increased bilirubin itself may in-crease bilirubin absorption by nervous tissue.15
Most important to the neonatal foal is hemolysis,whether by sepsis (intravascular) or neonatal iso-erythrolysis (extravascular). Kernicterus, a condi-tion where bilirubin encephalopathy occurs, hasbeen reported in the foal.16 Degeneration and ne-crosis of cerebral neurons occurs.
24 2009 � Vol. 55 � AAEP PROCEEDINGS
MEDICINE—FOAL
Infectious Agents
Pathogens, whether viral or bacterial, have the abil-ity to cause substantial CNS inflammation by theirown actions or by the initiation of an excitotoxicneurotransmitter cascade. Meningitis and enceph-alomyelitis has been extensively reviewed.17 Theneonatal foal is susceptible to meningitis resultingfrom systemic bacteremia caused by an increasedpermeability of the blood–brain barrier.
Developmental or Congenital Cerebral Abnormalities
In one retrospective study, hydrocephalus occurredin 3% of foals that died or were euthan-ized.18 Hydrocephalus may be clinically silent orprecipitate seizure activity.
Congenital Epilepsy
This condition is reported in some breeds. A recentreview of Egyptian Arabians19 showed seizure activityitself to be self-limiting with age. Complications inaffected foals included head trauma and pneumonia.
5. Aids in the Diagnosis of Seizure Activity
Complete Blood Count and Serum Chemistry
Assessment of the systemic health of any foal display-ing seizure activity is essential. A complete bloodcount (CBC) aids in the diagnosis of systemic infectionthat may have spread to the CNS. Ongoing cerebralhypoxia as a result of anemia will be suggested.Serum chemistry evaluation assesses major organ sys-tem function, chiefly liver (removal of blood borne tox-ins) and kidney (assessment of electrolytehomeostasis). Immunoglobulin G (IgG) levels are adirect measure of the transfer of passive immunityfrom the mare, critical for immune defenses in theotherwise hypogammaglobulinemic neonatal foal.A number of studies have shown a relationship be-tween the IgG concentration and the occurrence ofneonatal disease including sepsis.20,21 Sepsis is amajor differential diagnosis in the neonate affected byneurological disease and can itself contribute to neu-rological dysfunction.22 Blood gas evaluation as-sesses pulmonary gas exchange and enablesdetermination of the acid-base status of the foal.
Cerebrospinal Fluid Analysis
In suspected cases of meningitis, cytology and mi-crobiological culture of the cerebrospinal fluid (CSF)is useful for diagnosis, antimicrobial selection, andprognosis. Total protein concentration, nucleatedcell count, and red blood cell (RBC) count should beroutinely performed. Where increased intracranialpressure is suspected, this procedure should beavoided because aspiration from the atlantal-occip-ital space can lead to herniation of the brain throughthe foramen magnum.
Radiography and Magnetic Resonance Imaging
Both radiography23 and magnetic resonance imag-ing (MRI)24 have been reported in the diagnosis of
neonatal neurological disease. With radiography,congenital malformations, disruption of bony struc-tures, and deviation of neural tissue by trauma canbe visualized. Both plain and contrast studies arepossible. MRI is invaluable in the assessment ofsoft tissue, foci of infection, or vascular disruption.
6. Treatment Goals
Once a diagnosis of a seizure disorder has beenmade, the treatment plan should seek to address thefollowing clinical goals:
● Manage seizure episodes and any concurrentneurologic dysfunction
● Restore cerebral perfusion and oxygenation ifcompromised
● Control cerebral edema and inflammation ifpresent
● Provide metabolic requirements of the debili-tated patient
● Address concurrent physical injuries and med-ical conditions if present
With respect to the precipitation of seizure activ-ity within the brain, consideration of a number oftherapeutic targets is necessary including gluta-mate accumulation, aberrant calcium fluxes, freeradical formation, lipid peroxidation, and genera-tion of arachidonic acid metabolites.3,25,26
Blockade of the N-methyl-D-aspartate (NMDA) re-ceptor mediating excitotoxic neuronal damage hasbeen useful in both in vivo and in vitro models ofcerebral ischemia and trauma.27,28 Cell death resultsfrom excessive activation of the NMDA glutamate re-ceptors, allowing excessive Ca influx through a recep-tor-associated ion channel. Experimental glutamatetoxicity can be decreased by NMDA antagonists ad-ministered after the initial insult.3 In addition toNMDA receptor activation, intracellular Ca accumu-lation may also be caused by calcium-mediated neuro-nal depolarization and loss of cell membraneintegrity.27 Glutamate excitotoxicity is a cause, re-sult, and potentiator of calcium-induced cellularbreakdown; therefore, glutamate control throughNMDA receptor blockade provides a rational thera-peutic target to ameliorate neuronal damage.
7. Readily Available Drugs Useful for Seizure Control
Although many seizure controlling medications areavailable in human medicine, veterinary access tomost is limited. This review will be limited to thosedrugs readily accessible to the practicing equineveterinarian.
BenzodiazepinesDrugs of this class are widely used for their anxio-lytic, sedative, narcotic, anticonvulsant, and musclerelaxant effects, with differences between membersresulting from varying absorption and metabo-lism.29 The benzodiazepines are important in themanagement of seizure disorders associated with
AAEP PROCEEDINGS � Vol. 55 � 2009 25
MEDICINE—FOAL
fever and hypoxic insult and are the first choicetherapy for status epilepticus.30 Benzodiazepinesshow high efficacy rates, a rapid onset of action, andhave minimal toxicity to the patient.
DiazepamDiazepam is best used in the emergency control ofseizures.30 Chronic oral administration of diaze-pam is unsuitable for long-term seizure manage-ment because efficacy is doubtful. Diazepam has avery short half-life, induces hepatic enzymes, andmay create tolerance rendering diazepam ineffectivefor controlling seizures during emergencies.31
The use of diazepam in the control of equine neo-natal seizures is widely reported. Rapid onset ofshort-term control of acute seizures is achieved withminimal depression to the foal. Recurrent seizureactivity is often managed with repeated administra-tion of diazepam as required; however, phenobarbi-tal administration to effect is recommended in caseswhere two or more seizures occur over a shortperiod.
MidazolamMidazolam is the only available water-soluble ben-zodiazepine.30 Midazolam is fast acting, rapidlypenetrates the blood–brain barrier, and has a rela-tively short duration of action. Use in the treat-ment of refractory human neonatal seizures hasbeen reported, with more than one third of all hu-man neonatal seizures being refractory to high dosephenobarbital.32,33
The use of midazolam in the control of neonatalfoal seizures has been reported with administrationthrough both the IV and IM route. Initial control ofa seizure episode can be readily achieved by bolusintravenous administration, with ongoing seizurecontrol maintained with an intravenous constantrate infusion.34 Side effects include respiratory de-pression and hypotension.
Barbiturates
PhenobarbitalPhenobarbital is used in the management of acuteseizure episodes not responding to shorter-actingagents (by IV infusion) and recurrent seizure activ-ity (constant rate infusion, chronic oral dosing).Phenobarbital can be considered a mainstay of sei-zure control. Onset of action is rapid, with thethreshold of neurons to seizure activity initiationand propagation raised. Depression may result oninitial administration of the drug; however, inchronic dosage situations, this is overcome by theinduction of hepatic enzyme metabolism. Serumlevels therefore require monitoring to ensure thefoal remains within the therapeutic range duringlong-term maintenance therapy.35,36
PentobarbitalPentobarbital is an intravenous anesthetic barbitu-rate that depresses neuronal excitability by enhanc-
ing GABA-coupled responses. Pentobarbital is thefirst metabolite of thiopental. In comparison tophenobarbital, pentobarbital penetrates the brainfaster, allowing more rapid seizure control, and hasa shorter half-life, allowing quicker recovery. So-dium pentobarbital is generally reserved for thetreatment of uncontrollable status epilepticus.
Accumulation may occur with prolonged use be-cause of lipid solubility. Pentobarbital use is asso-ciated with respiratory depression, myocardialdepression, hypotension, and low cardiac output.33
Phenytoin
The use of phenytoin in the control of neonatal sei-zures has been reported.33 However, little isknown about the pharmacokinetics of phenytoin inthe equine neonate, with erratic plasma concentra-tions reported. Considerable depression of somefoals has also occurred.
Cyclohexylamines
Ketamine
The use of ketamine in the management of humanrefractory status epilepticus has been reported, al-though this drug has traditionally been avoided inpatients with neurological injury.33 Ketamine hasbeen associated with improved cerebral perfusion,likely by increasing blood pressure because of itssympathomimetic properties.37 This is in contrastwith most medications used for refractory statusepilepticus that reduce blood pressure.
NMDA receptor antagonism, in addition to beingthe most important mechanism causing the analgesiceffects of ketamine, is also thought responsible for itspurported neuroprotective action.38 Blockade of ex-citatory transmission at the NMDA receptor providesan approach to the initial treatment of cerebral isch-emia.39 Blockage of excessive NMDA receptor allowsregulation of intracellular calcium levels and attenu-ated induction of NO, reducing neuronal degenerationand death. Cellular morphology was preserved,cellular energy status and ATP production wereprotected, and reduced cell swelling was notedsubsequent to anoxia-hypoxia or excitatory neuro-transmitter injury.40
Ketamine is useful for the short-term manage-ment of seizure activity, being administered as aconstant rate infusion after control of a seizure epi-sode. In the author’s experience, this technique ismost applicable to those foals maintained in recum-bency because of concurrent debilitating medicalconditions. The foal is first induced to a light planeof narcosis (diazepam followed by ketamine) andthen the infusion is started. Foals vary in theirresponse, some progressing to a state of light butrousable sedation, with others maintaining an ap-propriate level of awareness and responsiveness tostimulation.
26 2009 � Vol. 55 � AAEP PROCEEDINGS
MEDICINE—FOAL
Other
Potassium BromidePotassium bromide (KBr) has been used since the19th century as a human anticonvulsant and seda-tive. After their first use in 1853, bromides (potas-sium, sodium, and ammonium) were the mainstay ofepilepsy control until replacement by phenobarbitalbeginning in 1912.41
It is currently widely used in the management ofrefractory canine epilepsy. Use in horses hasbeen reported chiefly in adults; however, control inidiopathic epilepsy of foals has been reported.19
Pharmacokinetics in adult horses have been re-viewed.42 The author has also found KBr usefuladjunctively in the control of neonatal seizuresincompletely controlled by other agents.
PropofolPropofol is a short-acting intravenous hypnotic an-esthetic agent useful for control of refractory statusepilepticus. Propofol may have anticonvulsant ac-tivity, because it is GABA-mimetic, stabilizingGABA inhibitory neurotransmitter sites. Use incases of prolonged seizure activity or status epilep-ticus has been reported in humans.43 Use in theneonatal foal for refractory seizure activity is possi-ble with the favorable depressant characteristics ofthe drug; however, financial considerations may pre-clude widespread use.
MagnesiumThe magnesium ion acts as an antagonist of cellmembrane calcium channels in many tissues.44
It also acts as a voltage-dependent blocker of theNMDA channel, suggesting beneficial effects in theprevention of neuronal cell death and seizure prop-agation, although this is reduced after neural inju-ry.45 Cell membrane integrity and permeabilityhave also shown to be improved by Mg administra-tion, as has functioning of the Na1/K1 ATPase mem-brane pump, which enables a reduction in celledema.
GabapentinGabapentin is a structural analog of GABA, al-though the exact mode of action is unknown. It hasbeen reportedly used for neuropathic pain in thehorse, and pharmacokinetics have been recently re-viewed.46,47 Use for seizure control in the horsehas not been widely reported. Further study is re-quired before gabapentin can be recommended forseizure control.
8. Supportive Care of Seizure Patients
Treatment of existing trauma, prevention of furtherinjury, strict attention to fluid balance, control ofinflammation, and provision of the metabolic re-quirements of the patient are as integral to success-ful patient management as control of seizureactivity itself.
Wounds, contusions, and decubital ulcerationshould be aggressively locally managed with topicaltreatments and dressings. Concurrent systemicantimicrobials to counter bacterial dissemination inthe compromised neonate will be required.
Appropriate leg wraps will aid in the prevention ofdistal limb edema and secondary limb injury.Head protection “bumpers” minimize the occurrenceof secondary neurological injury from repeated cra-nial trauma in the recumbent or seizing foal. Ifrecumbent, the foal should be provided a supportivebed and a means to cleanly eliminate body waste.Slight elevation of the head can prevent dependentedema affecting the brain. Corneal ulceration sec-ondary to abrasion or exposure keratitis can be pre-vented by regular application of ophthalmiclubricants.
Drug options for sedation of the seizing patient tominimize self-trauma are limited; however, the �2adrenergic agonists and benzodiazepines possess fa-vorable qualities of sedation and muscle relaxation.Contraindicated drugs include butorphanol (be-cause of a potential increase in CSF pressure) andacepromazine (lowers the seizure threshold).
Fluid Therapy
In addition to meeting the metabolic needs of the pa-tient, appropriate fluid therapy is essential to ensureadequate cerebral perfusion, which may have beencompromised by the cerebral insult that precipitatedthe seizure activity. Restoration of cerebral perfusionallows the re-establishment of autoregulation, the pro-cess whereby the brain controls its own perfusion rateand pressure despite fluctuations in arterial blood de-livery. The loss of autoregulation has been reportedafter cerebral ischemia and reperfusion or traumaticbrain injury.48
An appropriate fluid balance maintains cerebralperfusion and oxygenation while avoiding increasedintracranial pressure. Maintenance of appropriateoncotic pressure with sedation to decrease cerebralenergy metabolism is also beneficial.49
Systemic dehydration has not been shown to de-crease existing cerebral edema, and a negative fluidbalance has been proven to be detrimental to overallpatient outcome.50 Overhydration must also beavoided because this potentiates CNS edema aftercranial trauma and exacerbates pulmonary edemain recumbent patients.
Although used widely clinically, hypo-osmolar solu-tions such as 5% dextrose in water increase intracra-nial pressure caused by decreased serum sodium andincreased brain water.51 Iso-osmolar, polyionic fluidsare therefore indicated in the chronic management ofneurologically compromised patients once concerns ofcerebral edema have been overcome.
Control of Cerebral Edema
Edema of the brain causes compression against itsbony confinement and further trauma as well as adecrease in perfusion and oxygenation. Edema
AAEP PROCEEDINGS � Vol. 55 � 2009 27
MEDICINE—FOAL
may be caused by disruption of the blood–brain bar-rier, cellular disruption causing intracellular watercollection, and the result of osmotic imbalances be-tween blood and tissue.52
The mainstay of edema control has traditionallybeen the use of diuretics and hyperosmolar agents.Diuretics such as furosemide have little effect oncerebral edema because establishing an osmoticgradient across the blood–brain barrier does notrequire systemic dehydration.53 Hyperosmolar (os-motic) agents are central to the control of increasedintracranial pressure, although firm guidelines fortheir use do not exist.
MannitolMannitol is a polyol (sugar alcohol) used as an os-motic diuretic. As a hyperosmolar agent, mannitolestablishes an osmotic gradient across the blood–brain barrier and improves overall blood delivery tothe brain while decreasing intracranial pressure.54
Additionally, in common with all hyperosmolaragents, mannitol causes plasma volume expansionwith a resultant decrease in blood hematocrit andtherefore viscosity, and decreases cerebral bloodvolume.55
Hypertonic SalineAn intact blood–brain barrier is less permeable tosaline than to mannitol; hypertonic saline is there-fore a more effective and long-lasting hyperosmolaragent able to resolve cases refractory to mannitolinfusion.53 Hypertonic saline solutions decreasebrain water and intracranial pressure while tempo-rarily increasing systolic blood pressure and cardiacoutput.51 The use of hypertonic saline for in-creased intracranial pressure has been shown toincrease survival compared with mannitol use.56
Concentrations used range from 3% to 10%.57
Loop DiureticsDiuretics such as furosemide will lead to global de-hydration of the foal, which is detrimental to out-come because of the decrease in cerebral perfusionand oxygenation resulting from hypovolemia.50
Therefore, in the absence of peripheral or pulmo-nary edema, loop diuretics are not indicated in sei-zure cases where cerebral edema is suspected.
Inflammation
Anti-InflammatoriesNon-steroidal anti-inflammatory drugs (NSAIDs)attenuate inflammation associated with brain andspinal cord injury. Arachidonic acid metabolitespromote platelet aggregation and facilitate inflam-matory and immune reactions. Experimentally,cyclooxygenase (COX) inhibitors improve cerebralblood flow, decrease edema, protect COX-2–express-ing neurons, and attenuate microglial activation.58
Glucocorticoids are immunosuppressive and di-minish monocyte infiltration after cerebral isch-
emia.59 Glucocorticoids downregulate cytokine-mediated COX-2 expression by monocytes andastrocytes.60 Glucocorticoids inhibit phospholipaseA2, attenuating release of arachidonic acid from thecell membrane and inducible NO synthase (iNOS)expression.61 Upregulation of pro-inflammatorycytokines by nuclear factor �B (NF-�B) is alsoblocked.62
Cyclooxygenase inhibitors, such as the NSAIDs,should therefore have an additive anti-inflamma-tory effect if administered concurrently with glu-cocorticoids. The use of glucocorticoids wherecerebral insult is suspected is controversial; how-ever, utility in cases of acute bacterial meningitishas been shown.63
Dimethyl SulfoxideRecognized as an anti-inflammatory, dimethyl sul-foxide (DMSO) is also credited as a free radical scav-enger, antioxidant, diuretic, vasodilator, and Cachannel blocker. With consideration of the patho-physiology of cerebral insult, DMSO administrationis rational in cases of neural trauma.64 DMSO hasbeen shown to rapidly reduce raised intracranialpressure and increases cerebral perfusion withoutaffecting the systemic blood pressure.65
AntioxidantsLipid peroxidation is considered a major cause of celldamage and death after neurological insult. An-tioxidants have been shown capable of inhibitingedema, metabolic derangements, and ischemia ofaffected tissue.66
Pretreatment of animals with vitamin E (�-tocoph-erol) has been shown beneficial in cases of neurologicaltrauma, decreasing ischemia and enhancing recovery.Vitamin E is thought to act as a peroxyl free radicalscavenger. Chronic dosing is necessary because ofslow uptake by the CNS tissue, making it an imprac-tical agent for acute treatment.67
Vitamin C (ascorbic acid) is associated with glu-tamate release in the brain, suggesting a neuro-protective or neuromodulating effect is possibletherapeutically.68 The synaptic action of dopa-mine is affected, and the NMDA glutamate recep-tor is altered, which blocks NMDA-gated channelfunction.69
NutritionProtein and energy malnutrition has been shown toexacerbate brain injury and worsen functional out-come during periods of global ischemia. This is as aresult of increased oxidative stress and an inflamma-tory response to ischemia.70 In cases of cerebraltrauma, metabolic requirements have been shown tobe increased above maintenance levels.71 Provisionof adequate nutrition is therefore important in allcases of cerebral dysfunction regardless of the pres-ence of seizure activity. However, seizure activityplaces extreme demands metabolically on the affectedanimal, rapidly depleting energy stores.
28 2009 � Vol. 55 � AAEP PROCEEDINGS
MEDICINE—FOAL
9. Case Example
A 7-day-old, 45-kg Thoroughbred foal was hospital-ized for the recurrence of depression and loss ofsuckle reflex. The foal had previously been treatedbeginning at 2 days of age for HIE/PAS, with ther-apies including antimicrobials, anti-inflammatories,antioxidants (DMSO, vitamin C), and supportivecare until the foal could feed itself. The foal wasconsidered to have made a complete recovery after 3days of treatment.
On admission at 7 days of age, the foal was foundto be mildly depressed but in otherwise good condi-tion. Screening blood work did not indicate thepresence of infection, major organ dysfunction, ormetabolic derangement. Treatment consisted ofsupportive care, antimicrobial coverage, anti-in-flammatories, and antioxidants. The foal rapidlyimproved, with a return to normal behavior andfeeding activity within 24 h of admission.
Seizure activity occurred on the third day of hos-pitalization (10 days of age). Head pressing, tet-any, rapid pacing, and dementia were present.Administration of diazepam (5 mg, IV, twice with a
5-min interval) did not resolve the seizures. Phe-nobarbital was infused (10 mg/kg over 15 min twicewith a 20-min interval), which also did not arrestseizure activity. Pentobarbital (3 mg/kg, IV injec-tion) led to a period of narcosis and resolution of theseizure episode. The foal was immediately placedon a ketamine constant rate infusion (induced with0.05 mg/kg diazepam and 1 mg/kg ketamine, IV,followed by 0.02 mg/kg/min ketamine infusion).After 24 h, the infusion rate was halved and main-tained for a further 12 h. During this time, oralphenobarbital maintenance therapy at 4 mg/kgtwice daily was instituted. Supportive therapy wasdiscontinued, with the foal becoming ambulatory,and suckling activity was restored. Oral potassiumbromide was begun (20 mg/kg three times daily for 2days, loading dose decreased to 30 mg/kg once daily)in conjunction with the phenobarbital.
The foal was discharged, and no further incidentsof seizure activity were reported. Serum phenobar-bital levels were measured at 4 days and 3 h afterdosage36,72 to allow peak concentrations to be mea-sured (8 �g/ml). Phenobarbital and potassium bro-
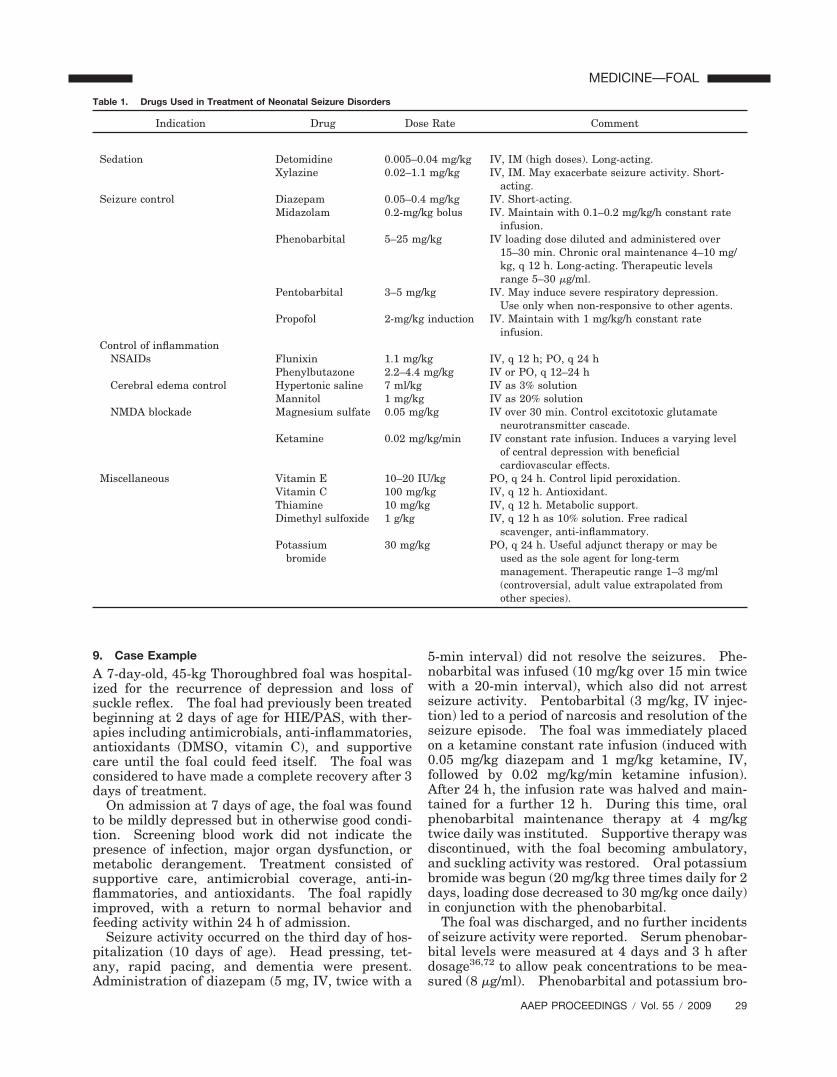
Table 1. Drugs Used in Treatment of Neonatal Seizure Disorders
Indication Drug Dose Rate Comment
Sedation Detomidine 0.005–0.04 mg/kg IV, IM (high doses). Long-acting.Xylazine 0.02–1.1 mg/kg IV, IM. May exacerbate seizure activity. Short-
acting.Seizure control Diazepam 0.05–0.4 mg/kg IV. Short-acting.
Midazolam 0.2-mg/kg bolus IV. Maintain with 0.1–0.2 mg/kg/h constant rateinfusion.
Phenobarbital 5–25 mg/kg IV loading dose diluted and administered over15–30 min. Chronic oral maintenance 4–10 mg/kg, q 12 h. Long-acting. Therapeutic levelsrange 5–30 �g/ml.
Pentobarbital 3–5 mg/kg IV. May induce severe respiratory depression.Use only when non-responsive to other agents.
Propofol 2-mg/kg induction IV. Maintain with 1 mg/kg/h constant rateinfusion.
Control of inflammationNSAIDs Flunixin 1.1 mg/kg IV, q 12 h; PO, q 24 h
Phenylbutazone 2.2–4.4 mg/kg IV or PO, q 12–24 hCerebral edema control Hypertonic saline 7 ml/kg IV as 3% solution
Mannitol 1 mg/kg IV as 20% solutionNMDA blockade Magnesium sulfate 0.05 mg/kg IV over 30 min. Control excitotoxic glutamate
neurotransmitter cascade.Ketamine 0.02 mg/kg/min IV constant rate infusion. Induces a varying level
of central depression with beneficialcardiovascular effects.
Miscellaneous Vitamin E 10–20 IU/kg PO, q 24 h. Control lipid peroxidation.Vitamin C 100 mg/kg IV, q 12 h. Antioxidant.Thiamine 10 mg/kg IV, q 12 h. Metabolic support.Dimethyl sulfoxide 1 g/kg IV, q 12 h as 10% solution. Free radical
scavenger, anti-inflammatory.Potassium
bromide30 mg/kg PO, q 24 h. Useful adjunct therapy or may be
used as the sole agent for long-termmanagement. Therapeutic range 1–3 mg/ml(controversial, adult value extrapolated fromother species).
AAEP PROCEEDINGS � Vol. 55 � 2009 29
MEDICINE—FOAL
mide were tapered after 1 mo of treatment, beingdecreased to half dose for a further 2 wk and thendiscontinued. The foal has continued to developnormally without incident.
The phenobarbital levels measured in this foal areconsidered to be below the established therapeuticrange for horses. Assessment of phenobarbital lev-els should be performed after the establishment ofsteady-state concentrations. This occurs after five orsix elimination half-lives, with each half-life being12 hours long.72 In this case, the adjunctive use ofpotassium bromide may allow a lower level of phe-nobarbital to maintain effective seizure control.
10. Summary
Control of neonate seizure activity presents diagnos-tic and therapeutic challenges to the equine clini-cian. A thorough understanding of the underlyingpathology of neurological dysfunction is required.Concurrent or precipitating medical conditions mustbe managed. Along with management of the sei-zure activity, re-establishment of appropriate cere-bral blood flow, fluid balance, and nutrition isessential to successful management of these cases.
References1. Green SL, Mayhew IG. Neurologic disorders. In: Kot-
2. Chen Y, Swanson RA. Astrocytes and brain injury.J Cereb Blood Flow Metab 2003;23:137–149.
3. Lipton SA, Rosenberg PA. Excitatory amino acids as a finalcommon pathway for neurologic disorders. N Engl J Med1994;330:613–622.
4. Stola A, Perlman J. Post-resuscitation strategies to avoidongoing injury following intrapartum hypoxia-ischemia. Se-min Fetal Neonatal Med 2008;13:424–431.
5. Calvert JW, Zhang JH. Pathophysiology of an hypoxic-isch-emic insult during the perinatal period. Neurol Res 2005;27:246–260.
6. Grow J, Barks JD. Pathogenesis of hypoxic-ischemic cere-bral injury in the term infant: current concepts. Clin Peri-natol 2002;29:585–602.
7. MacKay RJ. Brain injury after head trauma: pathophysi-ology, diagnosis, and treatment. Vet Clin North Am [EquinePract] 2004;20:199–216.
8. Feige K, Furst A, Kaser-Hotz B, Ossent P. Traumatic injuryto the central nervous system in horses: occurence, diagno-sis and outcome. Equine Vet Edu 2000;2:275–280.
9. Rozance PJ, Hay WW. Hypoglycemia in newborn infants:features associated with adverse outcomes. Biol Neonate2006;90:74–86.
10. Montassir H, Maegaki Y, Ogura K, et al. Associated factorsin neonatal hypoglycemic brain injury. Brain Dev doi:10:1016/jibraindev.2008.10.012.
11. Salhab WA, Wyckoff MH, Laptook AR, Perlman JM. Initialhypoglycemia and neonatal brain injury in term infants withsevere fetal acidemia. Pediatrics 2004;114:361–366.
12. Hollis AR, Furr MO, Magdesian KG, et al. Blood glucoseconcentrations in critically ill neonatal foals. J Vet InternMed 2008;22:1223–1227.
16. Loynachan AT, Williams NM, Freestone JF. Kernicterus ina neonatal foal. J Vet Diagn Invest 2007;19:209–212.
17. Pellegrini-Masini A, Livesey LC. Meningitis and encepha-lomyelitis in horses. Vet Clin North Am [Equine Pract]2006;22:553–589.
18. Crowe MW, Swerczek TW. Equine congenital defects.Am J Vet Res 1985;46:353–358.
19. Aleman M, Gray LC, Williams DC, et al. Juvenile idiopathicepilepsy in Egyptian Arabian foals: 22 cases (1985–2005).J Vet Intern Med 2002;20:1443–1449.
20. Robinson JA, Allen GK, Green EM, Fales WH, Loch WE,Wilkerson CG. A prospective study of septicaemia in co-lostrum-deprived foals. Equine Vet J 1993;25:214–219.
21. Clabough DL, Levine JF, Grant GL, Conboy HS. Factors as-sociated with failure of passive transfer of colostral antibodies inStandardbred foals. J Vet Intern Med 1991;5:335–340.
22. Sanchez LC. Equine neonatal sepsis. Vet Clin North Am[Equine Pract] 2002;21:273–293.
23. Mayhew IG, Watson AG, Heissan JA. Congenital occipitoat-lantoaxial malformations in the horse. Equine Vet J 1978;10:103–113.
24. Ferrell EA, Gavin PR, Tucker RL, Sellon DC, Hines MT.Magnetic resonance for evaluation of neurologic disease in 12horses. Vet Radiol Ultrasound 2002;43:510–516.
25. Nilsson P, Laursen H, Hillered L, Hansen AJ. Calciummovements in traumatic brain injury: the role of glutamatereceptor-operated ion channels. J Cereb Blood Flow Metab1996;16:262–270.
26. Amar AP, Levy ML. Pathogenesis and pharmacologicalstrategies for mitigating secondary damage in acute spinalcord injury. Neurosurgery 1999;44:1027–1039.
27. Choi DW, Koh JY, Peters S. Pharmacology of glutamateneurotoxicity in cortical cell culture: attenuation by NMDAantagonists. J Neurosci 1998;8:185–196.
28. Faden AI, Demediuk P, Panter SS, Vink R. The role ofexcitatory amino acids and NMDA receptors in traumaticbrain injury. Science 1989;244:798–800.
29. Shader RI, Greenblatt DJ. Benzodiazepines: some as-pects of their clinical pharmacology. Ciba Found Symp1979;74:141–155.
30. Riss J, Cloyd J, Gates J, Collins S. Benzodiazepines in epi-lepsy: pharmacology and pharmacokinetics. Acta NeurolScand 2008;118:69–86.
31. Podell M. Antiepileptic drug therapy. Clin Tech SmallAnim Pract 1998;13:185–192.
32. Sheth RD, Buckley DJ, Gutierrez AR, Gingold M, BodensteinerJB, Penney S. Midazolam in the treatment of refractory neo-natal seizures. Clin Neuropharmacol 1996;19:165–170.
33. Abend NS, Dlugos DJ. Treatment of refractory status epi-lepticus: literature review and a proposed protocol. Pedi-atr Neurol 2008;38:377–390.
34. Wilkins PA. How to use midazolam to control equine neo-natal seizures, in Proceedings. 51st Conference of the Amer-ican Association of Equine Practitioners 2005;279–280.
35. Mittel L. Seizures in the horse. Vet Clin North Am[Equine Pract] 1987;3:323–332.
36. Knox DA, Ravis WR, Pedersoli WM, et al. Pharmacokinet-ics of phenobarbital in horses after single and repeated oraladministration of the drug. Am J Vet Res 1982;53:706–710.
37. Himmelseher S, Durieux ME. Revising a dogma: ket-amine for patients with neurological injury? Anesth Analg1995;101:524–534.
38. Adams HA. [Mechanisms of action of ketamine]. Anaes-thesiol Reanim 1998;23:60–63.
39. Meldrum B. Protection against ischaemic neuronal damageby drugs acting on excitatory neurotransmission. Cerebro-vasc Brain Metab Rev 1990;2:27–57.
40. Pfenninger E, Himmelseher S. [Neuroprotection by ket-amine at the cellular level]. Anaesthesist 1997;46(suppl 1):S47–S54.
41. Ryan M, Baumann RJ. Use and monitoring of bromides inepilepsy treatment. Pediatr Neurol 1999;21:523–528.
42. Raidal SL, Edwards S. Pharmacokinetics of potassium bro-mide in adult horses. Aust Vet J 2008;86:187–193.
30 2009 � Vol. 55 � AAEP PROCEEDINGS
MEDICINE—FOAL
43. Bleck TP. Management approaches to prolonged seizuresand status epilepticus. Epilepsia 1999;40(suppl 1):S59–S63.
44. Iseri LT, French JH. Magnesium: nature’s physiologic cal-cium blocker. Am Heart J 1984;108:188–193.
45. Mayer ML, Westbrook GL, Guthrie PB. Voltage-dependentblock by Mg2� of NMDA responses in spinal cord neurones.Nature 1984;309:261–263.
46. Davis JL, Posner LP, Elce Y. Gabapentin for the treatmentof neuropathic pain in a pregnant horse. J Am Vet MedAssoc 2007;231:755–758.
47. Dirikolu L, Dafalla A, Ely KJ, et al. Pharmacokinetics of gaba-pentin in horses. J Vet Pharmacol Ther 2008;31:175–177.
48. Zagorac D, Yamaura K, Zhang C, Roman RJ, Harder DR.The effect of superoxide anion on autoregulation of cerebralblood flow. Stroke 2005;36:2589–2594.
49. Eker C, Asgeirsson B, Grande PO, Schalen W, Nordstrom CH.Improved outcome after severe head injury with a new therapybased on principles for brain volume regulation and preservedmicrocirculation. Crit Care Med 1998;26:1881–1886.
50. Clifton GL, Miller ER, Choi SC, Levin HS. Fluid thresholdsand outcome from severe brain injury. Crit Care Med 2002;30:739–745.
51. Zornow MH, Prough DS. Fluid management in patients withtraumatic brain injury. New Horizons 1995;3:488–498.
53. Ogden AT, Mayer SA, Connolly ES Jr. Hyperosmolaragents in neurosurgical practice: the evolving role of hyper-tonic saline. Neurosurgery 2005;57:207–215.
54. Muizelaar JP, Lutz HA III, Becker DP. Effect of mannitol onICP and CBF and correlation with pressure autoregulation inseverely head-injured patients. J Neurosurg 1984;61:700–706.
55. Knapp JM. Hyperosmolar therapy in the treatment of se-vere head injury in children: mannitol and hypertonic sa-line. AACN Clin Issues 2005;16:199–211.
56. Wakai A, Roberts I, Schierhout G, Wakai A. Mannitol foracute traumatic brain injury. Cochrane Database Syst Rev2005;4:CD001049.
57. Infanti JL. Challenging the gold standard: should manni-tol remain our first-line defense against intracranial hyper-tension? J Neurosci Nurs 2008;40:362–368.
58. Wolfe LS. Eicosanoids: prostaglandins, thromboxanes,leukotrienes, and other derivatives of carbon-20 unsaturatedfatty acids. J Neurochem 1982;38:1–14.
59. Kim JS, Gautam SC, Chopp M, et al. Expression of mono-cyte chemoattractant protein-1 and macrophage inflamma-tory protein-1 after focal cerebral ischemia in therat. J Neuroimmunol 1995;56:127–134.
60. Masferrer JL, Seibert K. Regulation of prostaglandin syn-thesis by glucocorticoids. Receptor 1994;4:25–30.
61. Porsti I, Paakkari I. Nitric oxide-based possibilities forpharmacotherapy. Ann Med 1995;27:407–420.
62. De Bosscher K, Vanden Berghe W, Haegeman G. Mecha-nisms of anti-inflammatory action and of immunosuppressionby glucocorticoids: negative interference of activated glu-cocorticoid receptor with transcription factors. J Neuroim-munol 2000;109:16–22.
63. van den Beek D, de Gans J, McIntyre P, Prasad K. Corti-costeroids for acute bacterial meningitis. Cochrane Data-base Syst Rev 2007;1:CD004405.
64. Coles JC, Ahmed SN, Mehta HU, Kaufmann JC. Role offree radical scavenger in protection of spinal cord duringischemia. Ann Thorac Surg 1986;41:551–556.
65. Kulah A, Akar M, Baykut L. Dimethyl sulfoxide in themanagement of patients with brain swelling and increasedintracranial pressure after severe closed head injury. Neu-rochirurgia (Stuttg) 1990;33:177–180.
66. Hall ED. role of oxygen radicals in traumatic injury:clinical implications. J Emerg Med 1993;11(suppl):131–136.
67. Hall ED, Yonkers PA, Andrus PK, Cox JW, Anderson DK.Biochemistry and pharmacology of lipid antioxidants in acutebrain and spinal cord injury. J Neurotrauma 1992;9(suppl):S425–S442.
68. Grunewald RA. Ascorbic acid in the brain. Brain ResBrain Res Rev 1993;18:123–133.
69. Rebec GV, Pierce RC. A vitamin as neuromodulator:ascorbate release into the extracellular fluid of the brainregulates dopaminergic and glutamatergic transmission.Prog Neurobiol 1994;43:537–565.