245 Methods and Devices INTRAUTERINE CONTRACEPTIVE DEVICE R. P. SOONAWALA Family Planning Association, India, and Wapia Maternity Hospital, Parel THERE is a need for a more acceptable intrauterine con- traceptive device (i.u.D.) for mass use throughout the world, especially in less developed countries. Available inert r.u.D.s have limitations, however much one may toy around with shape and size. Following my experience with an inert S 1. U .D. developed in 1964, a new bioactive copper i.u.D. has been designed and tried over a period of 15 months. The results have shown a high acceptance-rate, low pregnancy-rate, and low complication-rate. The copper i.u.D. is Y shaped with 250-300 sq. mm. of copper wire wound on its two limbs. The end of one limb is bulbous to cover the tip of the inserter; this makes in- sertion easier and less traumatic. A single polyethylene tail thread is provided. Two types of inserter are now in use. In one the plunger pushes the i.u.D., as in the Lippes loop. In the other the sheath is withdrawn to allow the i.u.D. to open, as in the copper T. In both these, there is a possibility of misusing the inserter and pushing the components or i.u.B. through the uterus. Also, it may be difficult for a worker, especially at a paramedical level, to change from one method to another. The new inserter overcomes these problems. It provides: a stop so that neither i.u.D., plunger, nor sleeving can go beyond a fixed depth in the uterine cavity, hence perforation is most unlikely; a single hand pistol grip so that one hand is free to hold the tenaculum; and a no-touch technique of loading the i.u.D. l.U.D. inserter (a) Guard tube. (b) Plunger. (c) Insertion tubing. (d) Complete assembly, with LU.D. The inserter (see figure) consists of three components: the guard tube, the plunger which is fixed to the guard tube, and the insertion tubing which is to be pulled down. The guard tube remains fixed in the cervix and the plunger is attached to it. Therefore, as the insertion tube is pulled dozen the i.u.D. is released into the uterine cavity. The whole inserter is then withdrawn and the thread cut to a suitable length. Requests for reprints should be addressed to 22B, Empire Estate, Cumballa Hill, Bombay 26, India. Reviews of Books Renal Histopathology ROBERT MEADOWS, M.D., F.R.C.P.A., director of histo- pathology, Queen Elizabeth Hospital, Adelaide. London : Oxford University Press. 1973. Pp. 363. f 14. As Dr Meadows points out, much progress in neph- rology in the past decade is owed to clinico-pathological cooperation in the study of renal-biopsy material. This book, based on the author’s experience as pathologist to a busy renal unit, is intended to show how much can be obtained from the examination by conventional light microscopy of carefully processed kidney specimens. The author illustrates his findings with 589 photomicrographs, all of the highest quality. In this respect-i.e., as an atlas of renal pathology-there can be no doubt that the book succeeds. The presentation is in two parts-the anatomical components of the kidney in health and disease, and the changes in particular diseases. Although having some merit, this approach causes much reduplication of both text and illustrations. A major weakness is that little attention is paid to immunopathological processes in glomerular disease. Although a detailed discussion of pathogenetic mechanisms might be regarded as outside the scope of this work, it is difficult to consider certain his- tological forms of glomerulonephritis (e.g., focal ne- phritis) without recognising the immediate diagnostic value and pathogenetic implications of immunofluorescent findings. Some minor criticisms may also be made. The section on focal glomerular disease does not adequately distinguish between focal glomerulosclerosis and focal proliferation, although it is clear later in the section on nephrotic syndrome that the author supports the distinc- tion. The reference on p. 184, implying identity between C3 and complement, is misleading. Nonetheless Dr Mea- dows presents a competent account of glomerular mor- phology in disease. For this and its excellent illustrations this book can be recommended. Immunologic Disorders in Infants and Children Edited by E. RICHARD STIEHM, M.D., professor of pedi- atrics, University of California, Los Angeles, and VIN- CENT A. FULGINITI, M.D., professor of pediatrics, Uni- versity of Arizona, Tucson. Philadelphia and London : Saunders. 1973. Pp. 637.$26, ill.05. Tms book is the first in a difficult area. When we first meet pathogens and other allergens in early life, many problems arise, so paediatric clinical immunology is vir- tually as large a subject as all adult clinical immunology with developmental concepts added. Maybe a satisfactory book on it cannot yet be written; this one is certainly not ideal, but it is a very valuable start. Rightly, the editors recognise that immunodeficiency is of far greater relative importance in children than in adults, but they really cannot claim that it, as opposed to say immunisa- tion or asthma, is the primary concern in clinical paedi- atric immunology, unless they regard atopy generally as an effect of immunodeficiency, which they do not claim. Inevitably, the book is uneven, ranging from the elegant precision of the section on disorders of complement (by F. S. Rosen and C. A. Alper) to the brief diffuse and chatty section on tumour immunology (in which the reader should have been given the incidence of different cancers in the different immunodeficiencies). Remarkable omis- sions include any mention of fetal antibody responses and the tolerance theory in the chapter on Development, and antireticulin antibodies in coeliac disease. More edi- torial discipline is needed in the next edition on the sev- eral loose and vague chapters, and on the overlap between
Transcript
245
Methods and Devices
INTRAUTERINE CONTRACEPTIVE DEVICE
R. P. SOONAWALA
Family Planning Association, India, andWapia Maternity Hospital, Parel
THERE is a need for a more acceptable intrauterine con-traceptive device (i.u.D.) for mass use throughout the
world, especially in less developed countries. Availableinert r.u.D.s have limitations, however much one may toyaround with shape and size. Following my experiencewith an inert S 1. U .D. developed in 1964, a new bioactivecopper i.u.D. has been designed and tried over a period of15 months. The results have shown a high acceptance-rate,low pregnancy-rate, and low complication-rate.The copper i.u.D. is Y shaped with 250-300 sq. mm. of
copper wire wound on its two limbs. The end of one limbis bulbous to cover the tip of the inserter; this makes in-sertion easier and less traumatic. A single polyethylenetail thread is provided.Two types of inserter are now in use. In one the
plunger pushes the i.u.D., as in the Lippes loop. In theother the sheath is withdrawn to allow the i.u.D. to open,as in the copper T. In both these, there is a possibility ofmisusing the inserter and pushing the components or i.u.B.through the uterus. Also, it may be difficult for a worker,especially at a paramedical level, to change from one methodto another.The new inserter overcomes these problems. It provides:
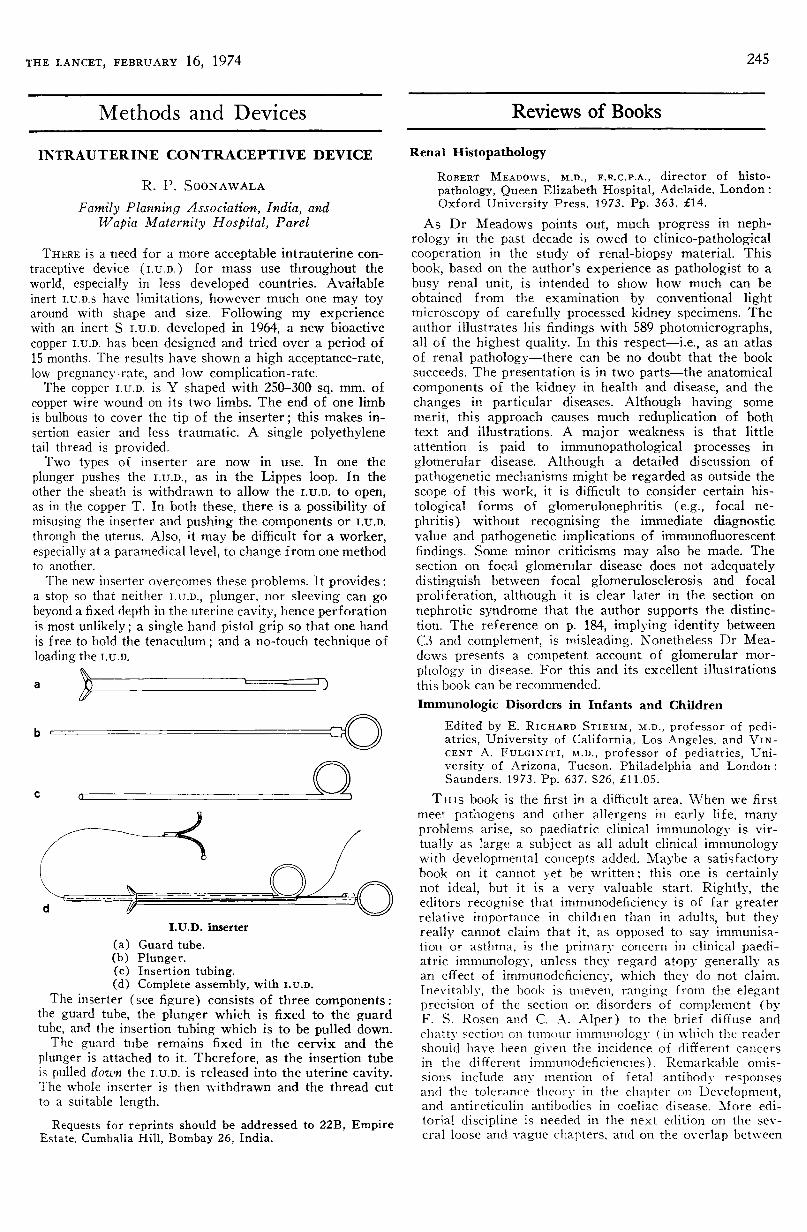
a stop so that neither i.u.D., plunger, nor sleeving can gobeyond a fixed depth in the uterine cavity, hence perforationis most unlikely; a single hand pistol grip so that one handis free to hold the tenaculum; and a no-touch technique ofloading the i.u.D.
l.U.D. inserter
(a) Guard tube.(b) Plunger.(c) Insertion tubing.(d) Complete assembly, with LU.D.
The inserter (see figure) consists of three components:the guard tube, the plunger which is fixed to the guardtube, and the insertion tubing which is to be pulled down.The guard tube remains fixed in the cervix and the
plunger is attached to it. Therefore, as the insertion tubeis pulled dozen the i.u.D. is released into the uterine cavity.The whole inserter is then withdrawn and the thread cutto a suitable length.
Requests for reprints should be addressed to 22B, EmpireEstate, Cumballa Hill, Bombay 26, India.
Reviews of Books
Renal HistopathologyROBERT MEADOWS, M.D., F.R.C.P.A., director of histo-
pathology, Queen Elizabeth Hospital, Adelaide. London :Oxford University Press. 1973. Pp. 363. f 14.
As Dr Meadows points out, much progress in neph-rology in the past decade is owed to clinico-pathologicalcooperation in the study of renal-biopsy material. This
book, based on the author’s experience as pathologist to abusy renal unit, is intended to show how much can beobtained from the examination by conventional lightmicroscopy of carefully processed kidney specimens. Theauthor illustrates his findings with 589 photomicrographs,all of the highest quality. In this respect-i.e., as an atlasof renal pathology-there can be no doubt that the booksucceeds. The presentation is in two parts-the anatomicalcomponents of the kidney in health and disease, and thechanges in particular diseases. Although having some
merit, this approach causes much reduplication of bothtext and illustrations. A major weakness is that littleattention is paid to immunopathological processes in
glomerular disease. Although a detailed discussion of
pathogenetic mechanisms might be regarded as outside thescope of this work, it is difficult to consider certain his-
tological forms of glomerulonephritis (e.g., focal ne-
phritis) without recognising the immediate diagnosticvalue and pathogenetic implications of immunofluorescentfindings. Some minor criticisms may also be made. Thesection on focal glomerular disease does not adequatelydistinguish between focal glomerulosclerosis and focal
proliferation, although it is clear later in the section onnephrotic syndrome that the author supports the distinc-tion. The reference on p. 184, implying identity betweenC3 and complement, is misleading. Nonetheless Dr Mea-dows presents a competent account of glomerular mor-phology in disease. For this and its excellent illustrationsthis book can be recommended.
Immunologic Disorders in Infants and ChildrenEdited by E. RICHARD STIEHM, M.D., professor of pedi-atrics, University of California, Los Angeles, and VIN-CENT A. FULGINITI, M.D., professor of pediatrics, Uni-versity of Arizona, Tucson. Philadelphia and London :Saunders. 1973. Pp. 637.$26, ill.05.
Tms book is the first in a difficult area. When we firstmeet pathogens and other allergens in early life, manyproblems arise, so paediatric clinical immunology is vir-
tually as large a subject as all adult clinical immunologywith developmental concepts added. Maybe a satisfactorybook on it cannot yet be written; this one is certainlynot ideal, but it is a very valuable start. Rightly, theeditors recognise that immunodeficiency is of far greaterrelative importance in children than in adults, but theyreally cannot claim that it, as opposed to say immunisa-tion or asthma, is the primary concern in clinical paedi-atric immunology, unless they regard atopy generally asan effect of immunodeficiency, which they do not claim.Inevitably, the book is uneven, ranging from the elegantprecision of the section on disorders of complement (byF. S. Rosen and C. A. Alper) to the brief diffuse andchatty section on tumour immunology (in which the readershould have been given the incidence of different cancersin the different immunodeficiencies). Remarkable omis-sions include any mention of fetal antibody responsesand the tolerance theory in the chapter on Development,and antireticulin antibodies in coeliac disease. More edi-torial discipline is needed in the next edition on the sev-eral loose and vague chapters, and on the overlap between
246
chapters, such as those on Biology of the Immune Re-sponse, Natural Defence Mechanisms, and Immune Mech-anisms in Infectious Diseases. But there is a great dealof valuable information here, and treatment is usuallystressed though it is sad that so little is effective and se-
curely based on controlled information. This leads bothto the very negative attitude in the chapter on RheumaticDiseases which rightly stresses salicylates, general man-agement, and the avoidance of therapeutic damage to
children with a self-limiting condition in Still’s disease,and to the unsubstantiated positive assertions in the chap-ter on Renal Disorders. Preparations referred to are
American, and it is sad to see that disodium cromoglycatewas not generally available there. This book is recom-mended as the only source book on this wide subject, butit should be read with caution and tolerance.
Young Till We Die
DORIS JONAS and DAVID JONAS. London : Hodder &Stoughton. 1974. Pp. 313. 3.25.
THIS volume written by a New York psychiatrist andanthropologist husband-and-wife team aims at "an ex-
planation for the decline of the position of the elders ofour societies, to show the consequence of this decline totheir personal well-being, and to make suggestions foraction that would ease or remedy their lot". It is inter-
esting that social anthropologists so far have tended to
study underdeveloped and sociologists overdeveloped so-
cieties, yet the premises of their two disciplines are verysimilar. Thus the little work of an anthropological natureconcerning the elderly in Western societies has been car-ried out by sociologists such as Peter Townsend an’l hisco-workers and the French sponsored C.I.G.S. (the In-ternational Centre of Social Gerontology). This largelyanecdotal book fails because it falls between an academicwork and a popular one and is a mixture of general an-thropology, descriptive passages on voluntary servicesavailable for the elderly in the U.S.A., and suggestionson future governmental and voluntary advances to hemade in that country. Nevertheless there are interestingdiscussions on the effect on the elderly of two and threegeneration families and on imaginative foster grandparentschemes pioneered largely in the Mid-West. The authorsrightly emphasise throughout the book the need for con-tinuing physical and mental activity and participation inordinary life by the elderly. However, it is difficult totreat seriously books of this nature without an index, letalone references, when unsubstantiated statements are
made such as that concerning the association with griefof carcinoma of the breast and pernicious anaemia. Per-haps the authors before writing the book had not decidedto what audience it was to be directed.
Human ReproductionConception and Contraception. Edited by E. S. HAFEZ and T.N. EvANS, department of gynecology and obstetrics, Schoolof Medicine, Wayne State University, Detroit. New York:Harper & Row. 1973. Pp. 778.$26.95.
THE main title of this book is deceptive, and the realsubject is stated in the subtitle. The underlying philosophyis clearly stated in the preface: " We can view only withsheer horror the projections of exponential growth of theworld population in the next few decades ". As an
encyclopaedic work on contraception the book must bejudged a considerable success; both the production andthe standards of writing and editing are high. All aspectsof the subject are covered in detail, beginning with achapter on demographic aspects, and proceeding througha long section on the anatomy and physiology of conceptionuntil the meat of the matter is reached: the methods and
consequences of contraception. Finally, there is a short
section on the stimulation of fertility, which adds to theweight of the volume but little to its central theme. Simi-
larly, some of the appendices might seem a little superfluous,and a table detailing the legal implications of fornication,incest, adultery, and rape in all fifty States of the U.S.A.,together with a "severity index" for each, may be
fascinating for the European reader but is unlikely materiallyto advance his clinical practice. But these cavils aside,there is much to admire, not least in the quality of theillustrations; in particular, the scanning electron micro-graphs presented in the chapters by the senior editor canbe described as a work of art. The approach in the clinicalchapters is both scientific and practical. There are, forinstance, detailed and fully illustrated descriptions of bothmale and female sterilisation procedures, information noteasily found under one heading elsewhere. This bookshould be read by practising gynaecologists, and should finda place in the larger medical libraries.
Six Minutes for the Patient
Interactions in General Practice Consultation. Edited byENID BAUNT and J. S. NORELL. London: Tavistock.1973. E2.25.
IN 1966 the late Dr Michael Balint, his wife, twopsychiatrists, and a group of general practitioners withlong experience of his seminars in psychotherapy formed aresearch team. Their purpose was to explore scientificallyand systematically what could be achieved with patientsin the course of an ordinary series of short and fairlyinfrequent interviews such as occur naturally in ordinarygeneral practice-say 10-15 minutes at a time. The
techniques of the long interview and of various shortcuts aimed at uncovering the patient’s psychopathologywere eschewed because they were regarded as being moreappropriate to specialist than to general practice. Attentionwas concentrated much more on what the patient himselfpresented to the doctor, on their relationship, on what iscalled the " overall" as well as the traditional diagnosis, andon prediction of outcome. The research seminars con-tinued for another year after Dr Balint’s death in 1970.Seven of the general practitioners have contributedchapters to this book, most of which has not been pub-lished before. In the verbatim accounts of seminars, inthe disagreements disclosed, in the limited claims ofsuccess both in prediction and in outcome the authors arehonest and human. There were complaints, for example,that one doctor presenting a case was not aware of manydetails of the patient’s background. Yet these could onlyhave been gleaned from the " long interview " methodthat the research group had decided to exclude. A majortopic of interest throughout is the so-called " flash "-theflash of understanding, a tuning-in, a shift in the level ofcommunication-which occurred in 18 of the 41 cases
described, its significance, and what should be done withit. Even if the book is rather difficult it will be valuable,and not only to those in general practice.
Modern First-aid
A. S. PLAYFAIR. London: Hamlyn. 1973. Pp. 159. 50pONLY a fresh approach to the subject would justify an-
other book on first-aid, and the style and format of thispublication do make it well worthwhile. It is probably theonly such work which can be read continuously, almost inthe manner of a novel; whilst abundant dramatic colouredillustrations help ensure that the author’s points are easilyremembered. The book also contains what is arguablythe best exposition yet of both the basic principals ofartificial respiration, and its technical minutiae. The
appeal, text, and low price all promise a very wide circula-tion for this little volume.
247
THE LANCET
Measles and Multiple SclerosisIDEAS about the cause of multiple sclerosis (M.s.)
have long been the weathercock of medicine, swingingfrom one fashionable and unproven theory to another,although for the past few years most have pointed inthe same general direction-towards a virus infectionwhich seems to be related to measles. The evidence
depends on pathological, epidemiological, and
immunological findings of greater or lesser uncer-tainty.
Pathological support for the infective theorydepends on the classic observations of inflammatorycells around blood-vessels in the region of active orrecent plaques of demyelination,l which can be
interpreted as a reaction to infection. There has alsobeen an unconfirmed report 2 of intranuclear inclu-sions in neurons and glial cells near plaques, whichwould be more directly in favour of a viral aetiology.Modem studies of the ultrastructure of plaques havebeen inconclusive and have not shown incontro-vertible viral particles. PRINEAS 4 illustrated aggre-gates of striated tubules in cytoplasm, and similar butnot identical structures have now been seen eitherthere or in nuclei in several cases.5-8 In various
aspects of their detailed structure all the intracellularinclusions have differed from known members of the
myxovirus and paramyxovirus groups; in a recentinstance 8 they were shown not to react with potentlabelled anti-measles and anti-parainfluenza-1 anti-
sera, and they have been compared with very similartubules seen in the nervous system in several unrelateddisorders.8 8 It seems unlikely, therefore, that whatelectron microscopy has revealed can be accepted asevidence of one of the viruses that produces tubularstructures in infected cells. The cytoplasmic struc-tures in particular may resemble more closely thetubulo-reticular formations seen in many types of
1. Lumsden, C. E. in Multiple Sclerosis (edited by D. McAlpine,N. D. Compston, and C. E. Lumsden); p. 208. Edinburgh, 1955.
2. Adams, J. M. Brown, W. J. Int. Archs Allergy, 1969, suppl. 36,p. 83.
3. Andrews, J. M. in Multiple Sclerosis (edited by F. Wolfgram,G. W. Ellison, J. G. Stevens, and J. M. Andrews); p. 23. NewYork, 1972.
4. Prineas, J. Science, 1972, 178, 760.5. Field, E. J. Lancet, 1973, i, 295.6. Narang, H. K., Field, E. J. J. neurol. Sci. 1973, 18, 287.7. Watanabe, I., Okazaki, H. Lancet, 1973, ii, 569.8. Dubois-Dalcq, M., Schumacher, G., Sever, J. L. ibid. p. 1408.
cells from patients with lupus erythematosus 9,10 andother collagen disorders, which are probably cell
organelles such as endoplasmic reticulum, rather thanviral nucleocapsids. In all, neuropathology has doneno more than support the idea of infection in M.S.Epidemiology, too, has been used to bolster aetiologyby association. The classic survey ofM.s. in northern
England, in which the age-incidence was similar to thatof poliomyelitis in an advancing community, has beentaken as support for the concept of M.S. as an aberrantresponse to an enteric infection acquired in earlyteen-age." Similar results have been obtained inother parts of the world,12-15 and have been particu-larly clear in migrants from high to low risk areas.16However, although giving valuable support for thegeneral theory of an infection, epidemiology has onlydemonstrated an effect without a cause.
Serological surveys to detect measles antibodies inM.S. have been of more importance. The first hintof a direct link between measles and M.S. was pub-lished by ADAMS and IMAGAwA/7 who found highertitres of antibodies against measles in the serum andc.s.F. of patients with M.S. than in controls. Similarresults in serum, but often not in the C.S.F., were
reported subsequently by others, 18,19 but were deniedby some ’20-23 for various reasons, usually methodolo-gical and involving selection of a
" normal " groupof patients for comparison. It has been realised
subsequently that choice of suitable controls is diffi-cult because they must be of similar age, sex, andrace, have lived in the same part of the world for an
equal period, and have had clinical measles at a
similar time; in addition, if cerebrospinal-fluidantibody is regarded as more relevant to what is
happening in the central nervous system than titresin serum, then allowance must be made for passivediffusion of antibody from serum into c.s.F., if theblood/brain barrier has been breached for someincidental reason.24 Newer work has met all these
conditions, and there are many accounts now of
abnormally high titres of various measles antibodiesin serum from patients with M.S., in which the selec-
9. Norton, W. R. J. Lab. clin. Med. 1969, 74, 369.10. Klippel, J. H., Decker, J. L., Grimley P. M., Evans, A. S.,
Rothfield, N. F. Lancet, 1973, ii, 1057.11. Poskanzer, D. C., Shapira, K., Miller, H. ibid. 1963, ii, 917.12. Dean, G. Br. med. J. 1967, ii, 724.13. Acheson, E. D. in Multiple Sclerosis, a Reappraisal (edited by D.
McAlpine, C. E. Lumsden, and E. D. Acheson); p. 3. London,1965.
14. Millar, J. H. D. Multiple Sclerosis; p. 12. Springfield, Illinois, 1971.15. Alter, M. in Progress in Multiple Sclerosis (edited by U. Liebowitz);
p. 99. New York, 1972.16. Dean, G. ibid. p. 132.17. Adams, J. M., Imagawa, D. T. Proc. Soc. exp. Biol. Med. 1962, iii,
562.18. Pette, E., Kuwert, E. Archs ges. Virusforsch. 1965, 16, 141.19. Clarke, J. K., Dane, D. S., Dick, G. W. A. Brain, 1965, 88, 953.20. Reed, D., Sever, J., Kurtzke, J., Kurland, L. Archs Neurol. 1964,
10, 402.21. Just, M., Rieder, H. P., Ritzel, G. Klin. Wschr. 1967, 45, 705.22. Caspary, E. A., Chambers, M. E., Field, E. J. Neurology, 1969, 19,
1038.23. Ross, C. A. C., Lenman, J. A. R. Melville, I. D. Br. med. J. 1969,