89
Richard C. Stabb, D.O. Memorial Symposium Concussion: A Gray Matter, Understanding Concussion
| Date post: | 22-Aug-2019 |
| Category: |
Documents |
| Upload: | nguyenthuy |
| View: | 217 times |
| Download: | 0 times |
Richard C. Stabb, D.O. Memorial Symposium
Concussion:A Gray Matter, Understanding Concussion
Objectives
• To review current, traumatic brain injury (TBI), concussion terminology, evaluation and management.
• To review what the current medical/scientific research tells us about acute and chronic effects of concussion.
• Review indications for imaging (CT, MRI) in patients who present with concussion, TBI.
• What is practical for a physician to know about concussion, and patient care with concussion.
• Provide resource guidance for protecting patients (athletes) after concussion.
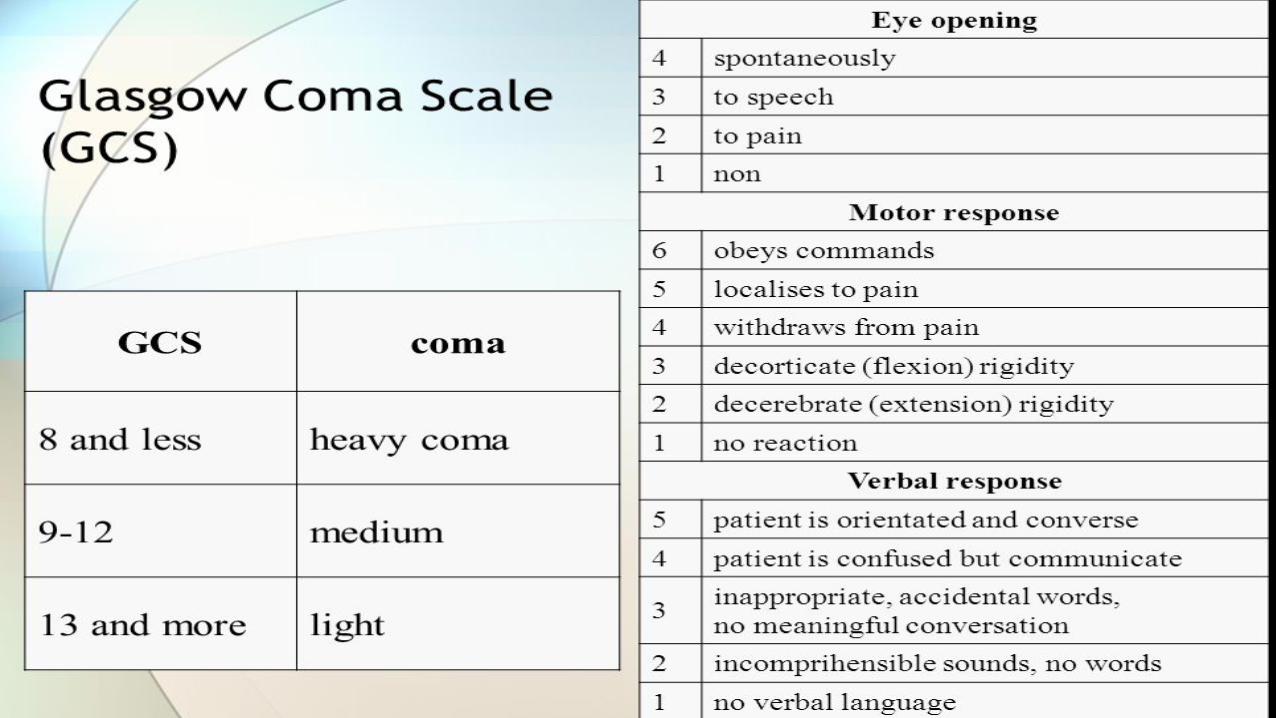
How is head injury (not concussion) classified?Glasgow coma scale • Mild - 13 to 15 • Moderate - 9-13 • Severe - Less than 8 -3
Definitions: Mild Traumatic Brain Injury
• Mild traumatic head injury (TBI)- Head injury due to contact and/or acceleration/deceleration forces.
• A Glasgow Coma Scale (GCS) of 13-15 measured at 30 minutes after head injury.
• Please note its not infrequent for patients to be classified with a mild TBI to still harbor various brain pathologies. Skull fracture, sub-dural hematomas etc.
Concussion? Definition?
• There are 43 and counting different “accepted” definitions of concussion, only one is evidence based.
• Concussion is not defined well neurologically• We do not understand the natural history of concussion.• We have little, if any, data on the neurobiological recovery of
concussion.
Concussion: Definition
• Concussion is recognized as a clinical syndrome of biomechanically induced alteration of brain function typically affecting memory and orientation along with other symptoms and networks which may involve loss of consciousness.
• Note: This can be injury to the head directly, TBI, or by blast injury, rapid acceleration, deceleration injury, rotational injury etc.
• Think of it as a symptom complex, a syndrome that occurs when the brain is pertubated by whatever mechanism.
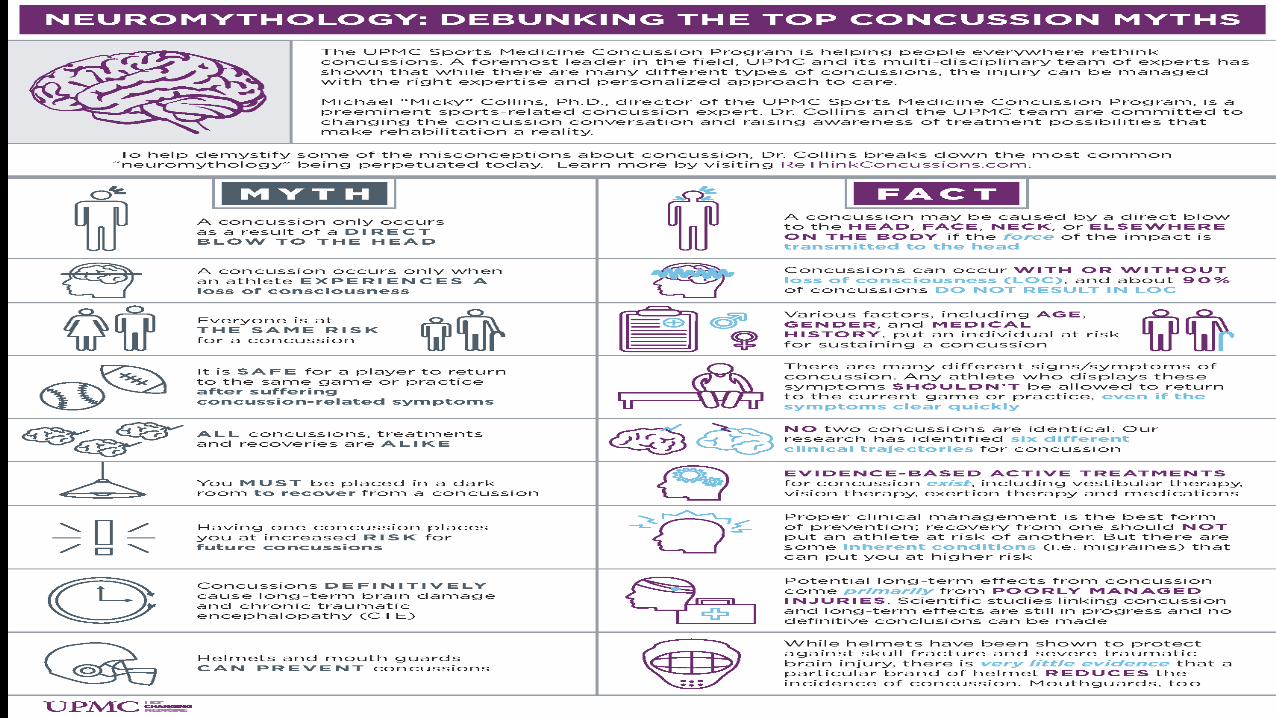
Concussion Myths and Facts(just a few there are many)
Myth• Concussion will only occur with
a blow to the head
Fact • Concussion occurs from a force
transmitted to the head from anywhere in the body, and forces even outside the body (blast injury etc.)
Concussion Myths and Facts:
Myth • Concussion by definition
requires a Loss of consciousness (LOC)
Fact• Concussion is independent of
LOC. Most patients with symptoms of concussion may describe themselves as dazed, rattled etc. The vast majority do not have a LOC
Concussion Myths and Facts:
Myth • Everyone reacts the same to
concussion and has the same susceptibility.
• Patients often feel like if they are involved in a traumatic experience they should have “some” symptoms.
Fact• Age, Gender, medical history,
genetic susceptibility, are all features that contribute to concussion susceptibility. Think of it as genotypic and phenotypic heterogeneity.
Concussion Myths and Facts:
Myth • A concussion will lead to definite
long term brain injury or Chronic traumatic encephalopathy (CTE)
Fact• No definite conclusions about
that can be made at this time. • For that reason and the
presumed link between head injury and CTE prevention is paramount.
Concussion Myths and Facts:
Myth • Helmets and mouth guards will
prevent concussion.
Fact• There will not be a helmet, or
mouth guard in my lifetime that will prevent concussion.
• Helmets are to prevent skull fractures, facial lacerations and trauma.
• There will not be a boxing glove that will prevent concussion either.
Epidemiology:
• 2.5 million people sustain a Traumatic brain injury (TBI) in the united states each year.
• 75-95% are mild. • Many cases go unreported • Most are motor vehicle accidents (young), falls(elderly), industrial
accidents, recreational accidents and assaults.• Mild TBI is a common injury in military infantry soldiers (combat) and
contact sports.
Epidemiology:
• Male female ratio 2.5:1• 50% of all patients with mild TBI are between the ages of 13-35 years
of age. • Patients at greater risk are patients less than 5 and those greater than
60.
Epidemiology: Sports that are High risk
• Males – Football, rugby, ice hockey, wrestling. • Females – Soccer and basketball. • Females have 2 times the rate of concussion in sports with
comparable rules. Possible reasons include, neck strength, hormonal susceptibility differences, symptom reporting.
• One distinct component of sports related concussion is the propensity for repeat injuries.
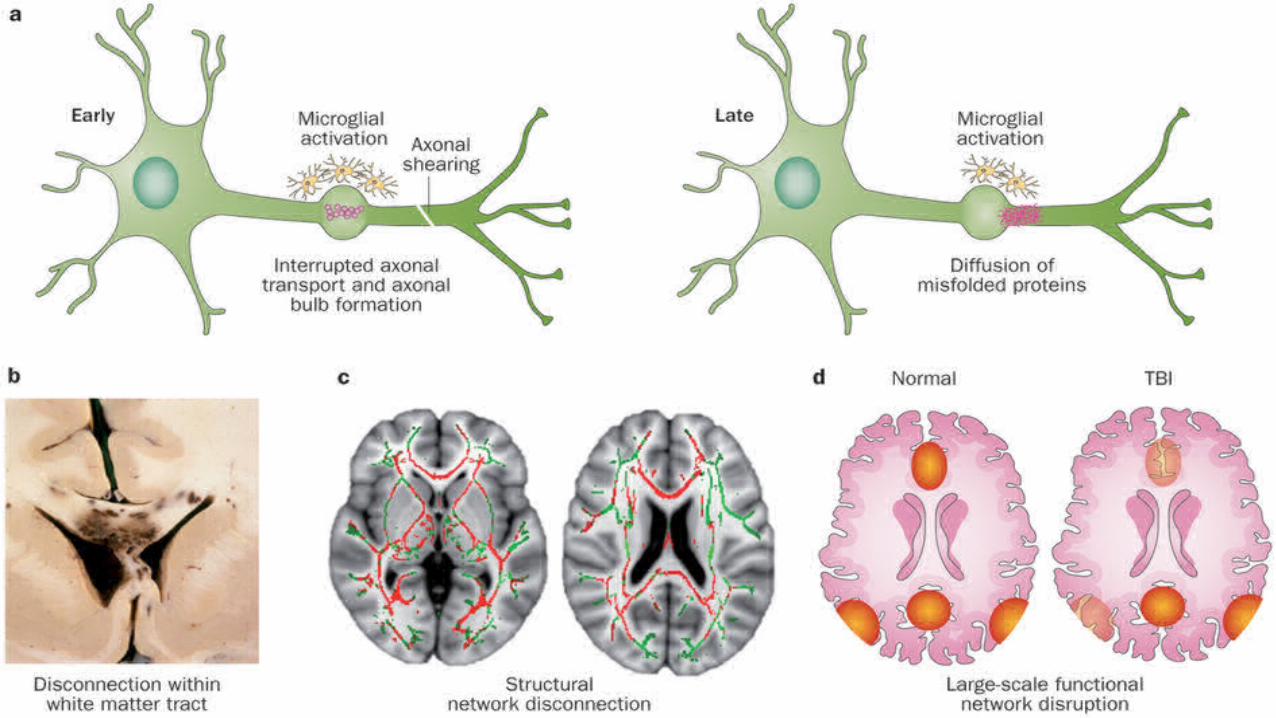
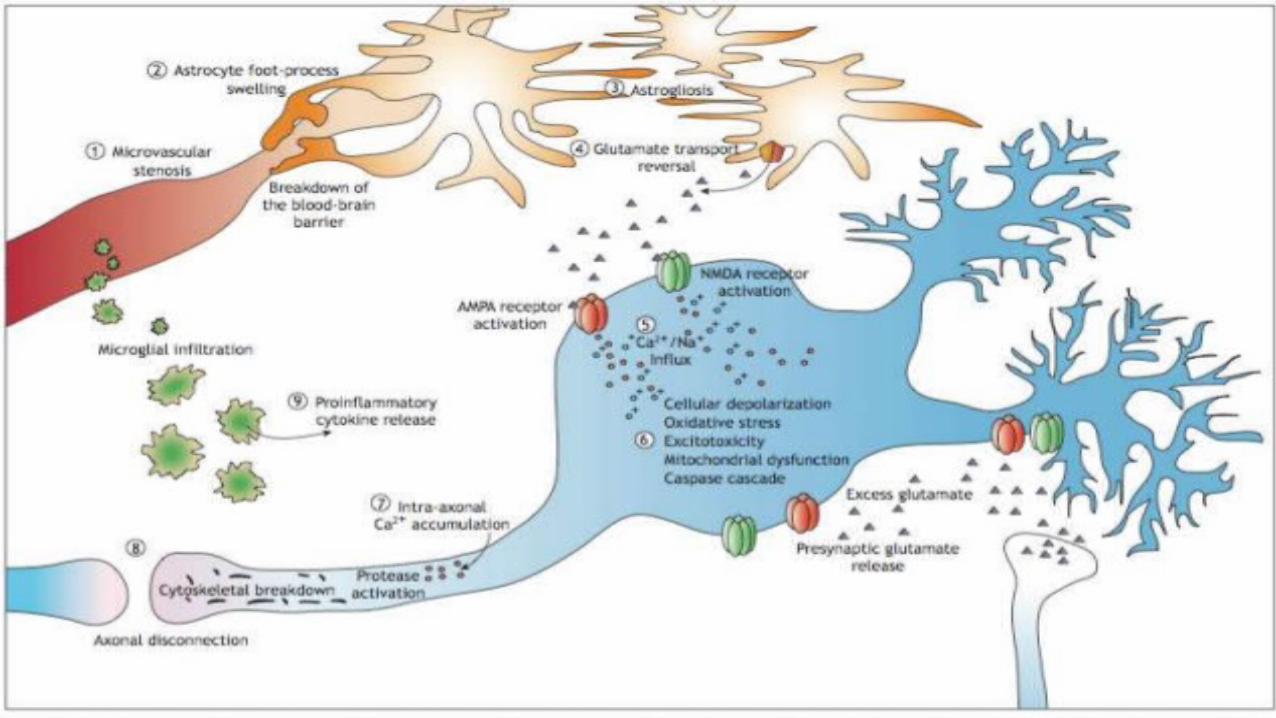
Pathophysiology: Concussion(Get to the point version)• Biomechanical forces that induce a metabolic cascade of impaired
neurotransmitter function, excitotoxicity, and abnormal concentrations of intracellular and extracellular ions.
• These effects may last hours or days, susceptibility to these effects vary greatly.
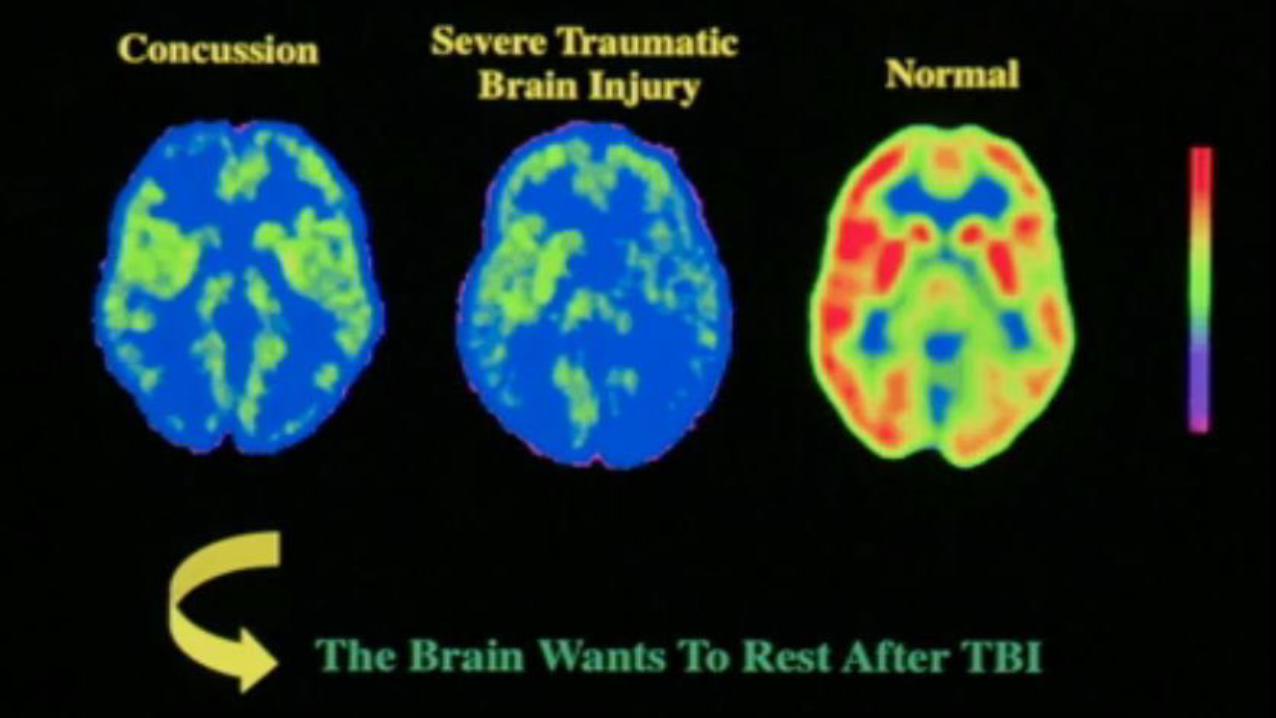
• Decreased cerebral blood flow, 50% of normal is seen in animal models for several days following experimentally induce concussion in animals.
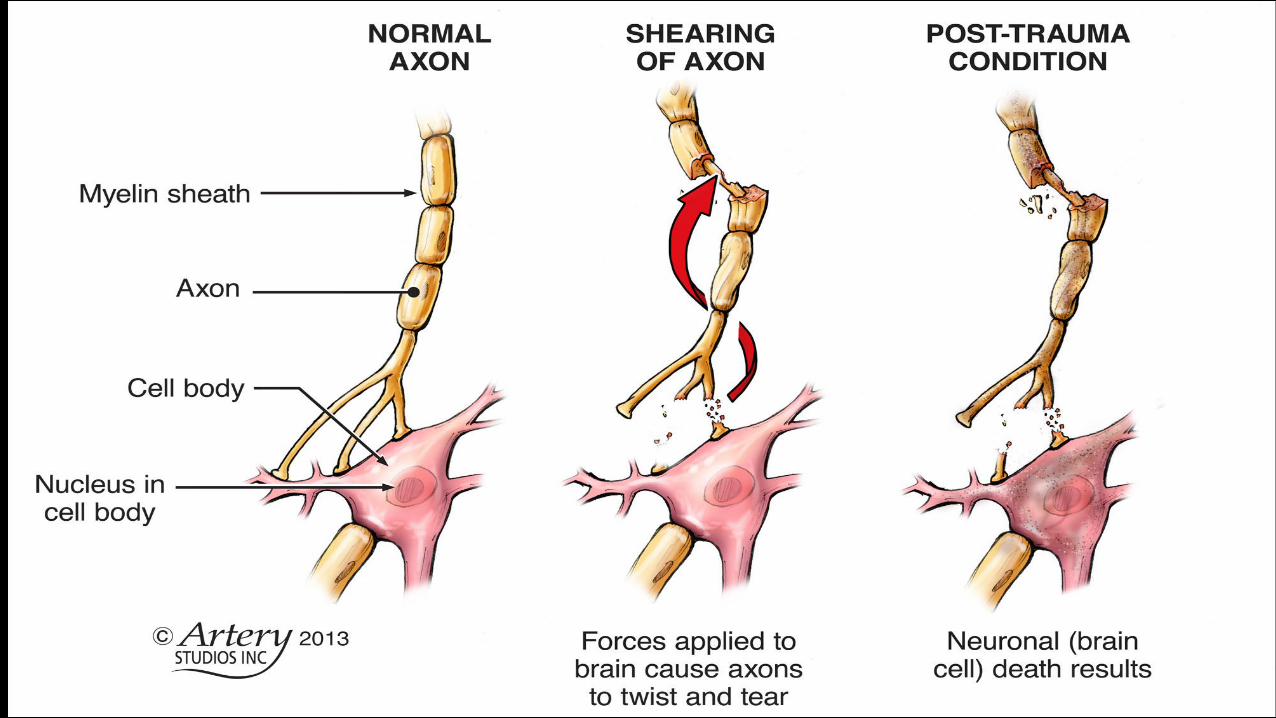
• Axonal disruption and shear forces are likely a part of this.

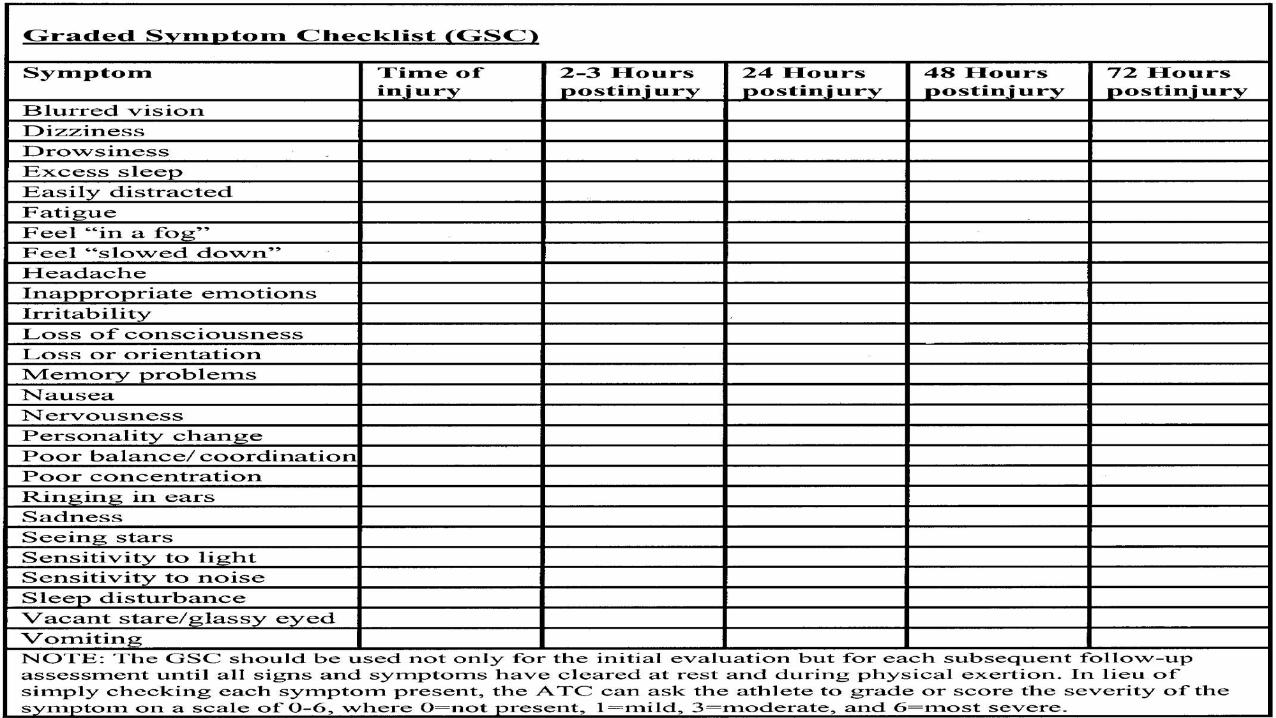
The Concussion Syndrome
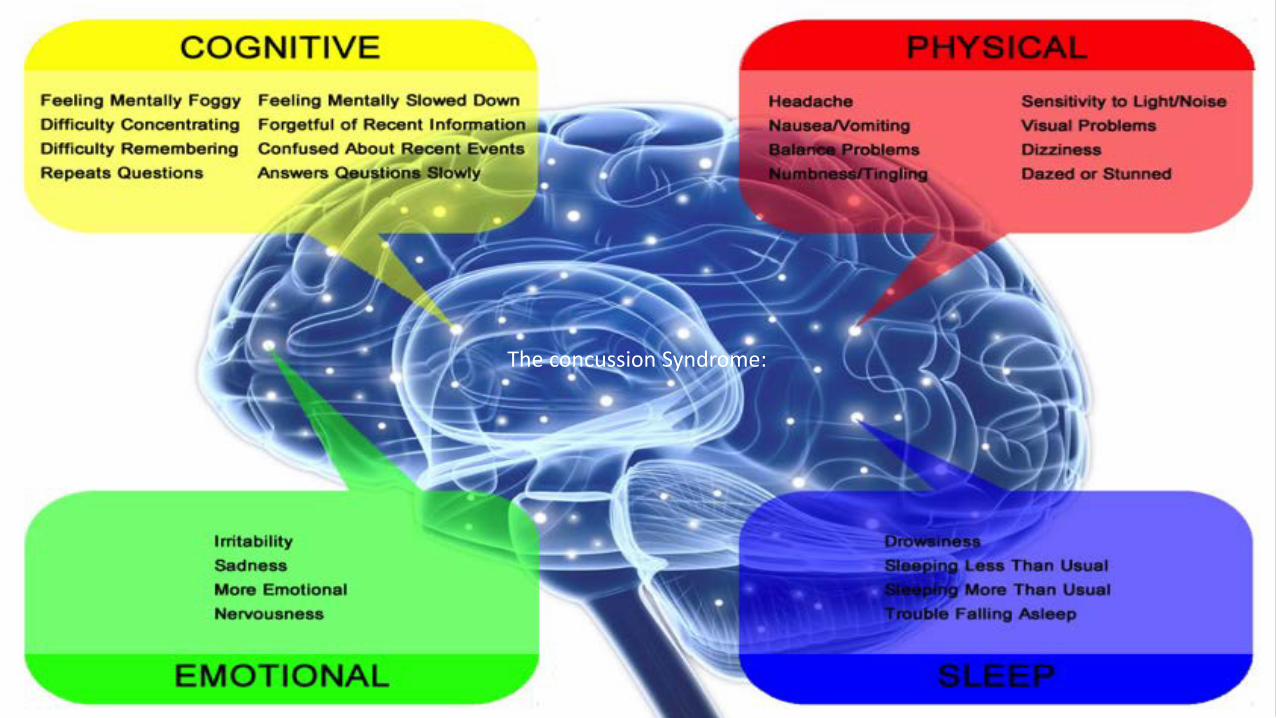
The concussion Syndrome:
Natural history of Concussion:
• Symptoms tend to be maximal in minuets to hours after the impact in question, and then resolve slowly and improve by 7-10 days.
• Any deviation from this (worsening) suggests a possible neurosurgical or medical issue.
• The difference in Athletic, military concussion vs most patients with concussion is they presumably will not be re-exposed to a second traumatic event that could put them at risk for further neurologic injury.
Concussion Caveats:
• Concussion is often used in the medical literature as a synonym for a mild TBI, but this is incorrect.
• The term concussion is specifically used to describe the characteristic symptoms and signs that an individual may experience after a mild TBI.
• Loss of consciousness does not define concussion. The majority of patients with concussion retain consciousness and have, if anything very short anterograde and retrograde amnesia.
Concussion Caveats:
• The signs and symptoms of concussion may take several hours to develop.
• The signs and symptoms of concussion may not be present until the person performs physical or cognitive activities.
• Think of it as a diffuse pathologic process that produces brain network dysfunction. Not a focal lesion.
Concussion Caveats:
• Studies have compared mild TBI to asymptomatic controls. There is a high prevalence of similar symptoms in both.
Eur J Neurol. 2004;11(6):411
• Patients expect symptoms after head injury. J Neurol Neurosurg Psychiatry. 1992,55(3):200.
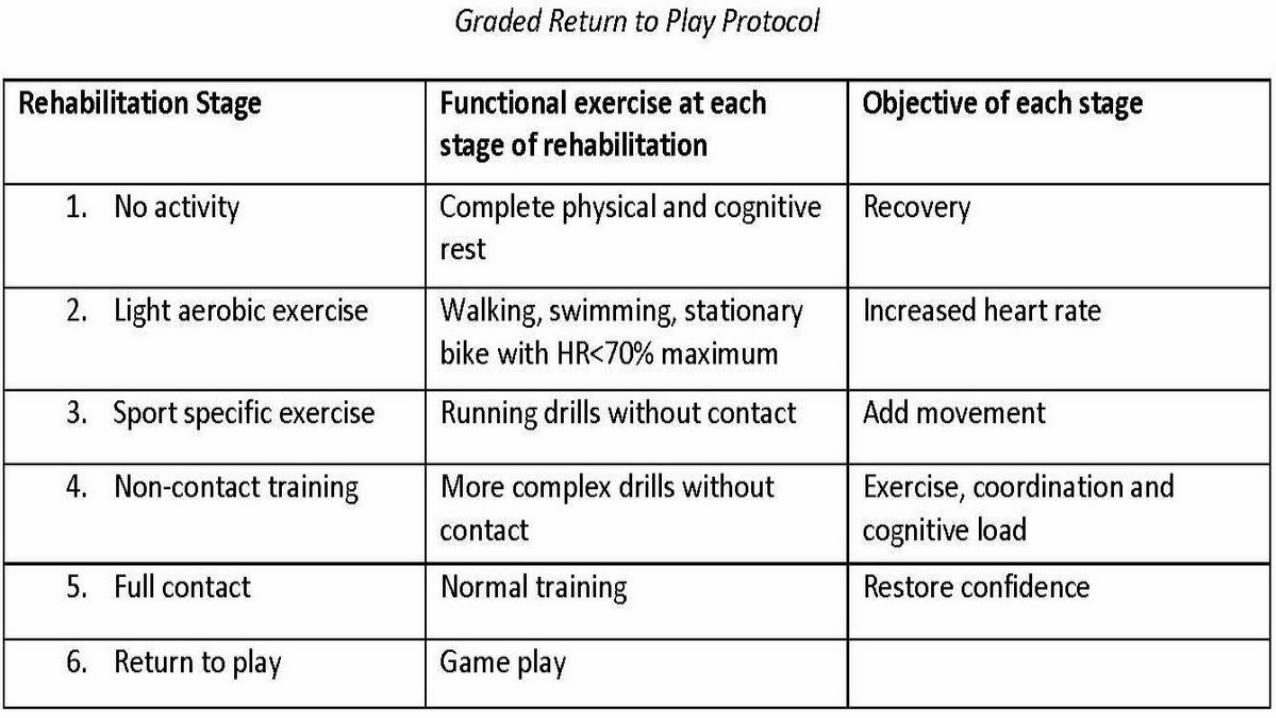
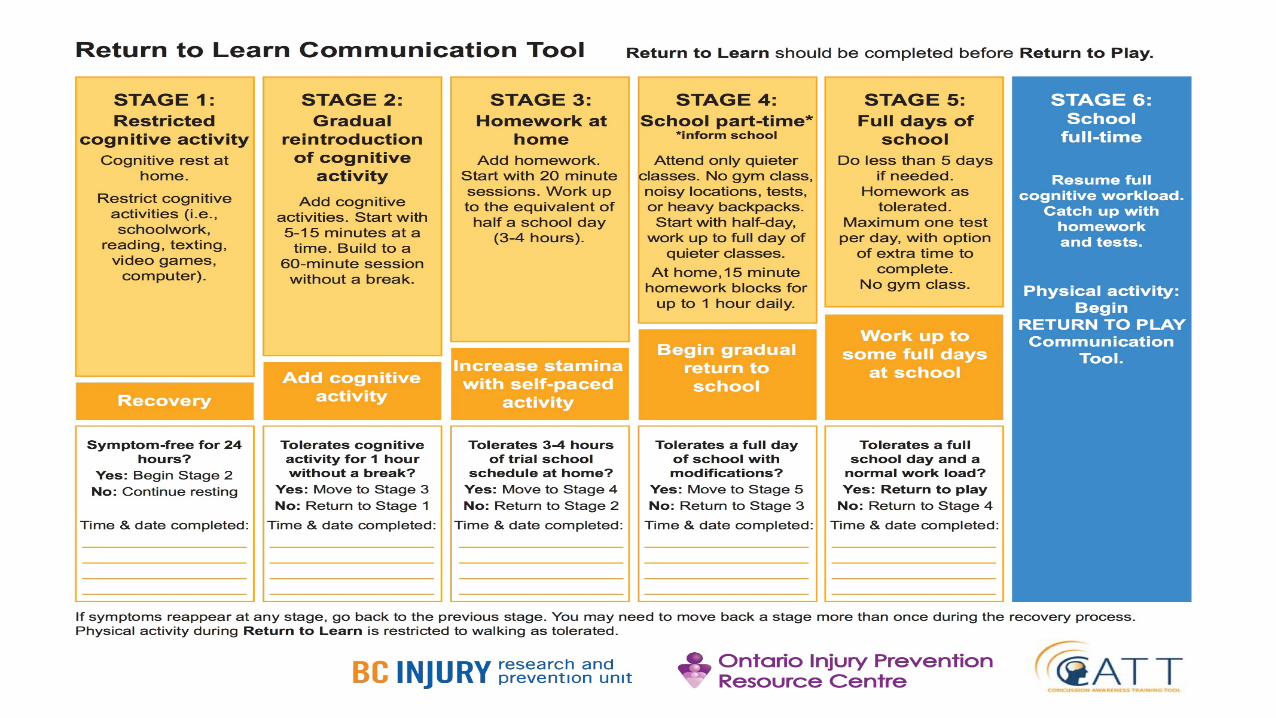
Treatment of acute Concussion
Treatment of Concussion:
• Please note if the syndrome occurred with a risk activity the patient might return to, they should be advised not to return to the activity until they are symptom free.
• Note if the patient is an athlete that is participating in organized, Oklahoma secondary school activity association (OSSAA) there are laws that the athlete must be removed from the activity and cleared by physician before returning to the activity. See Oklahoma Statute 24-155 of title 70 (Senate Bill 1700)

Sequelae of Concussion
• Second impact syndrome• Post concussion syndrome• Post-traumatic headaches• Sleep disturbance• Post traumatic Epilepsy• Post-traumatic vertigo and dizziness

Second Impact Syndrome:
• A term used when diffuse cerebral swelling develops in the setting of a second concussion.
• This definition requires the patient still be symptomatic of the first concussion.
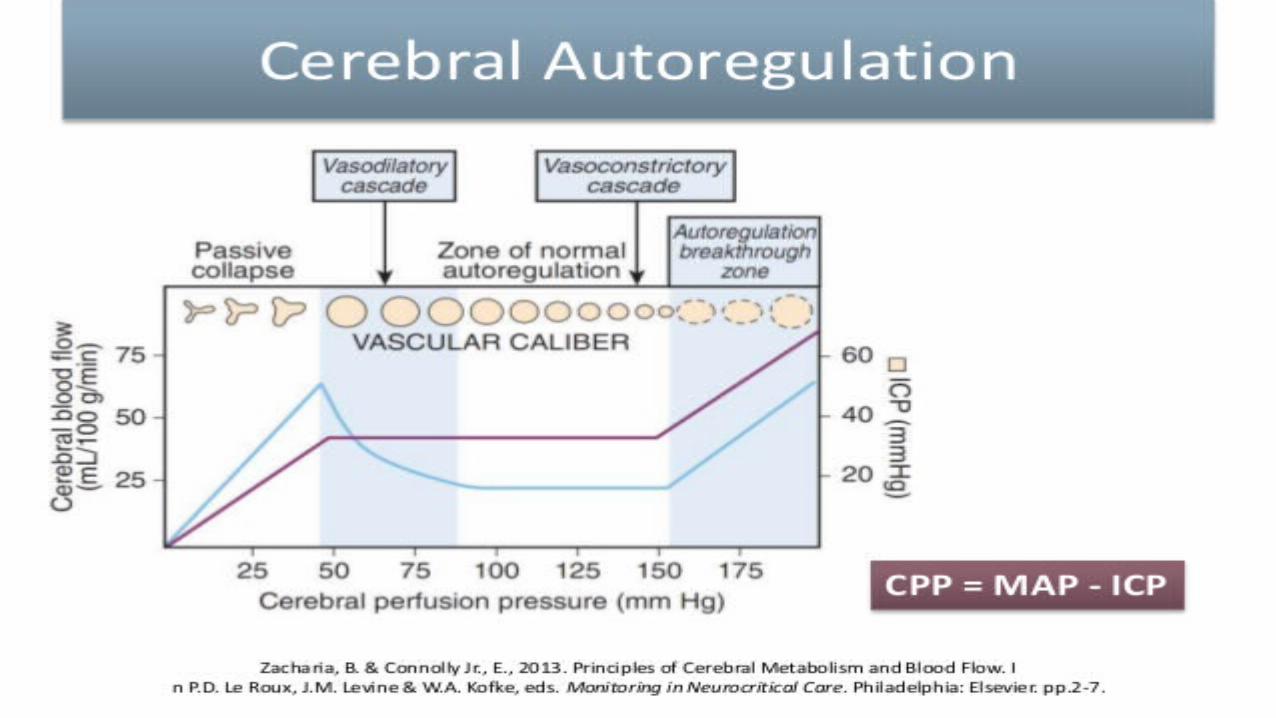
• This is a rare syndrome, and is controversial.• Thought to be related to loss of cerebral auto regulation.
Post concussion Syndrome:
• Post concussion syndrome- These include the symptoms of concussion that last longer than the natural history of “typical” concussion
• The majority of patients with concussion are baseline by 7-10 days. 85% by a month.
• Persistent post concussion syndrome- Patients that have concussion symptoms that persist more than a year. Emotional symptoms are often particularly prominent in this group.
• Please note patients with severe head injury and recovery often have a number of the symptoms of concussion indefinitely.
Sequelae of Mild TBI and Concussion (headache)• Post-traumatic headaches- Frequently occur after head injury. The
onset of the post traumatic headache should be within 7 days of the trauma. Most patients the headache is immediate or within hours of the trauma.
• You treat the headache based on the type of headache syndrome you identify. Migraine, tension type headache etc.
Sequelae of Mild TBI and Concussion (Sleep disturbance)• Common after head injury.• Insomnia and difficulty maintaining sleep are the most common.• Increased need for sleep (pleosomnia) is common.• A high percentage of patients have problems for months after head
injury. • After evaluating for possible underlying medical problems. Sleep
study and sleep evaluation is suggested.
Sequelae of Mild TBI and Concussion (Seizures/Epilepsy)• A seizure at the time of the head injury (immediate post-traumatic
seizure is not considered a risk factor for subsequent epilepsy in general.
• Seizure in the 1st week of injury are acute symptomatic events, provoked, and are not considered epilepsy.
• Half of patients who develop post-traumatic epilepsy do so in the first year.
• 80 % will occur in 2 years.• Prophylactic treatment with anti-epileptic medications (AED’s) does
not prevent post-traumatic epilepsy and is not recommended.
Post traumatic Vertigo and dizziness:Multiple possible clinical syndromes
• Benign paroxysmal positional vertigo• Vestibular migraine• Vertebral artery dissection and subsequent infarction
Post-Traumatic vertigo and dizziness: Mechanisms Multiple possible clinical syndromes
• Direct injury to the cochlear and or vestibular structures, temporal bone fractures.
• Labyrinthine concussion• Perilymphatic fistula
“Other” Cranial nerves:
• CN I- anosmia and hyposmia• Diplopia – Most common is CN IV• Facial nerve palsy usually secondary to fracture of the temporal bone• Facial pain (secondary to blunt force trauma to the face), and occipital
neuralgia
Spectrum of Chronic Traumatic Brain Injury
• Posttraumatic dementia- Patient meets criteria for dementia after a single moderate to severe head injury.
• Posttraumatic cognitive impairment- Patients with long term neurocognitive deficits from a single moderate to severe brain injury and do not meet criteria for dementia.
• Posttraumatic parkinsonism- is characterized as a Parkinsonian like syndrome secondary to a single or repetitive moderate to severe TBI
Spectrum of Chronic Traumatic Brain Injury
• Dementia pugilistica- Typically represents a sub-type of CTE, the patients have severe end stage dementia, secondary to a long boxing career.
• Chronic post concussion syndrome- Post concussion symptoms that don’t resolve.
• Chronic neurocognitive impairment
Spectrum of Chronic Traumatic Brain Injury
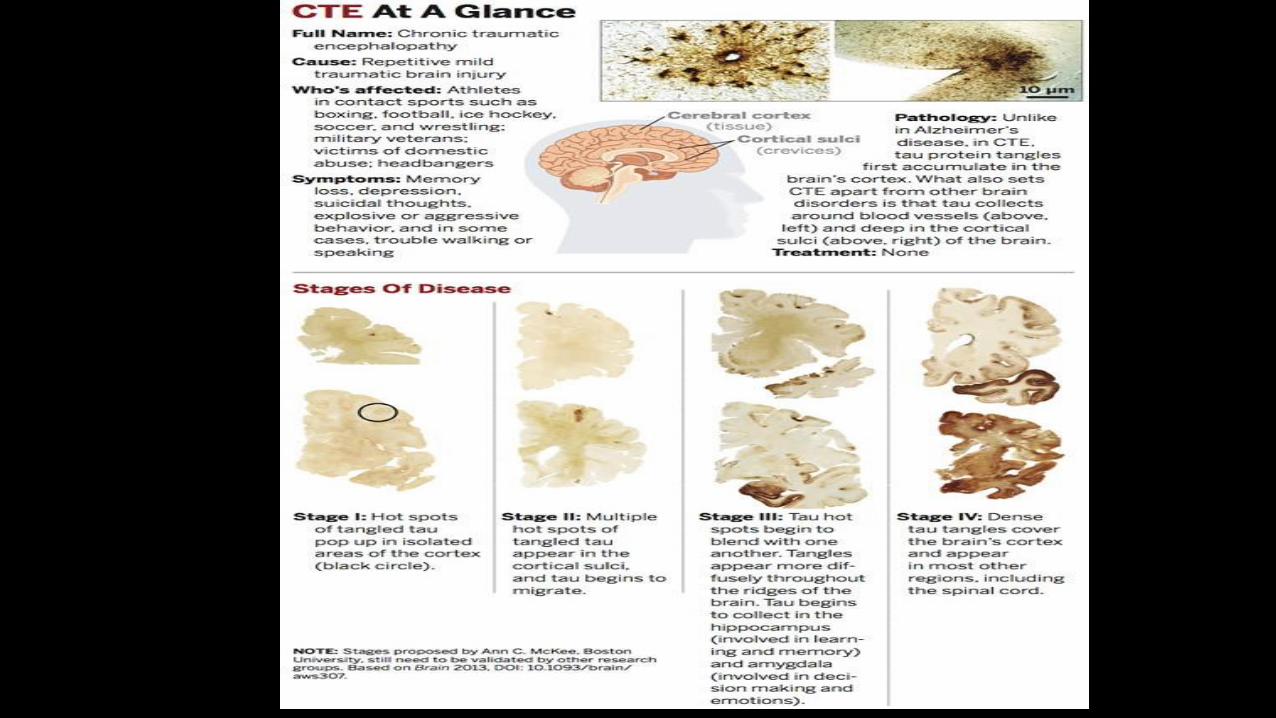
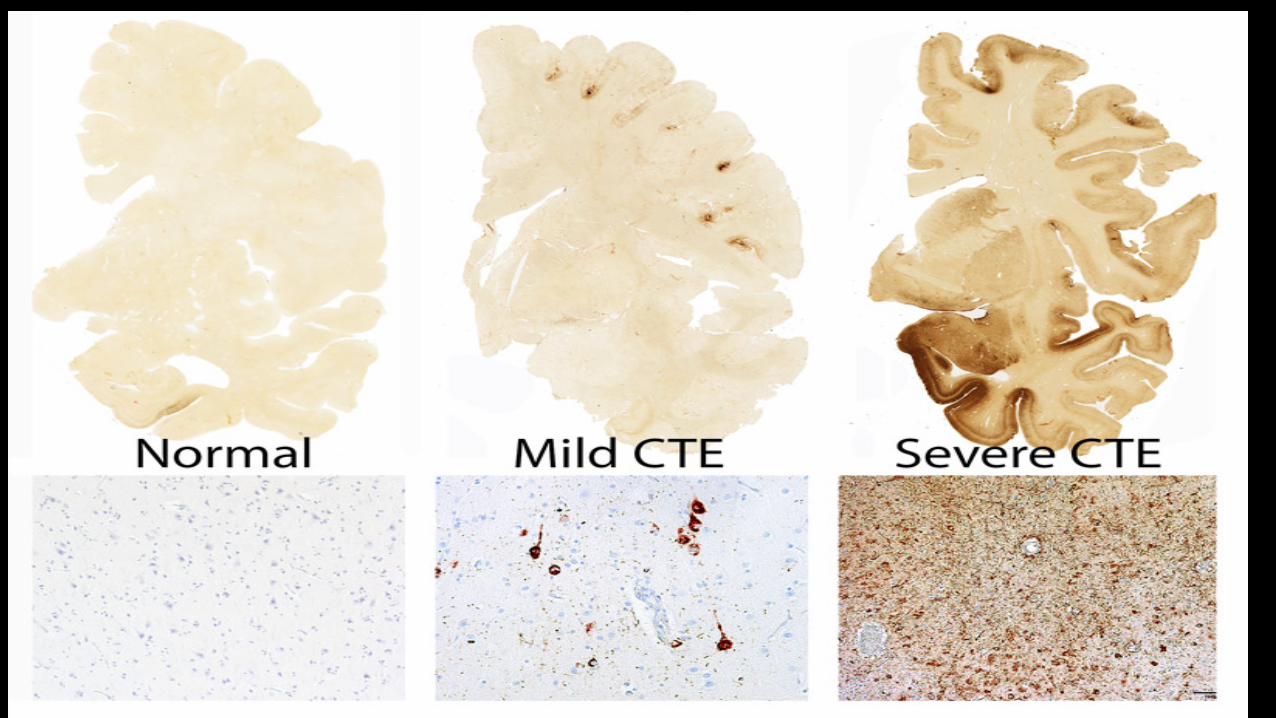
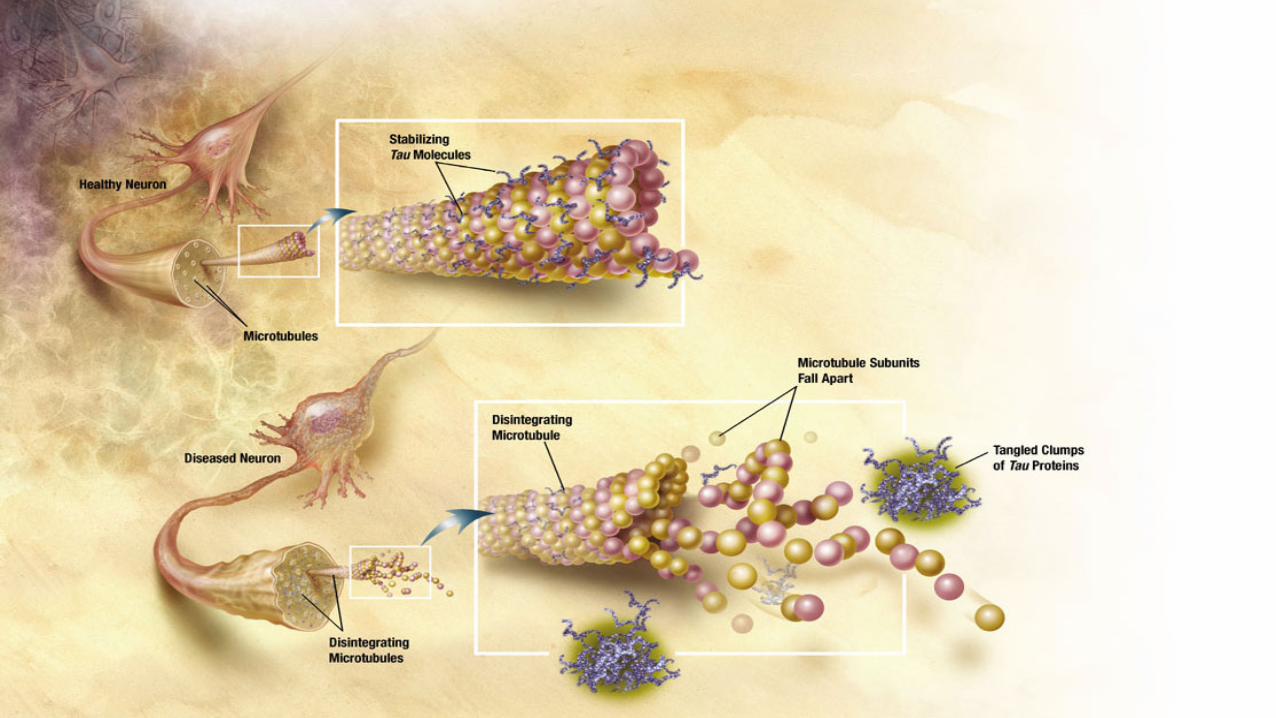
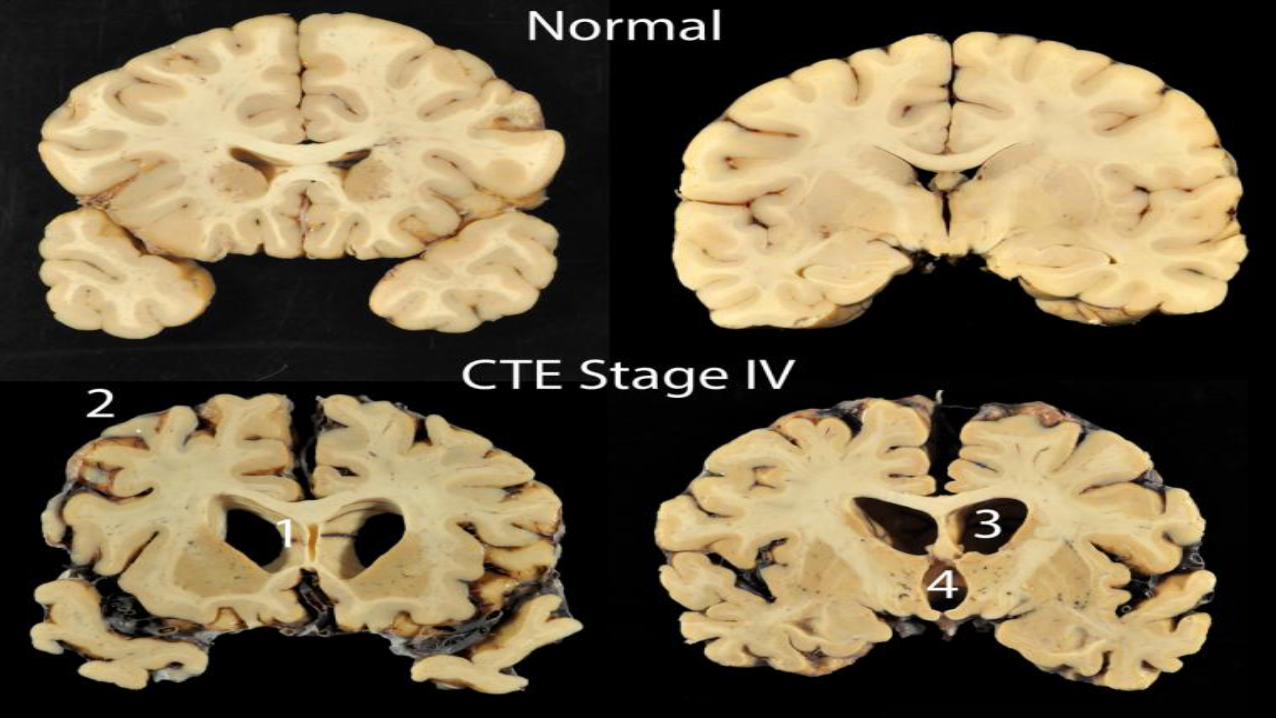
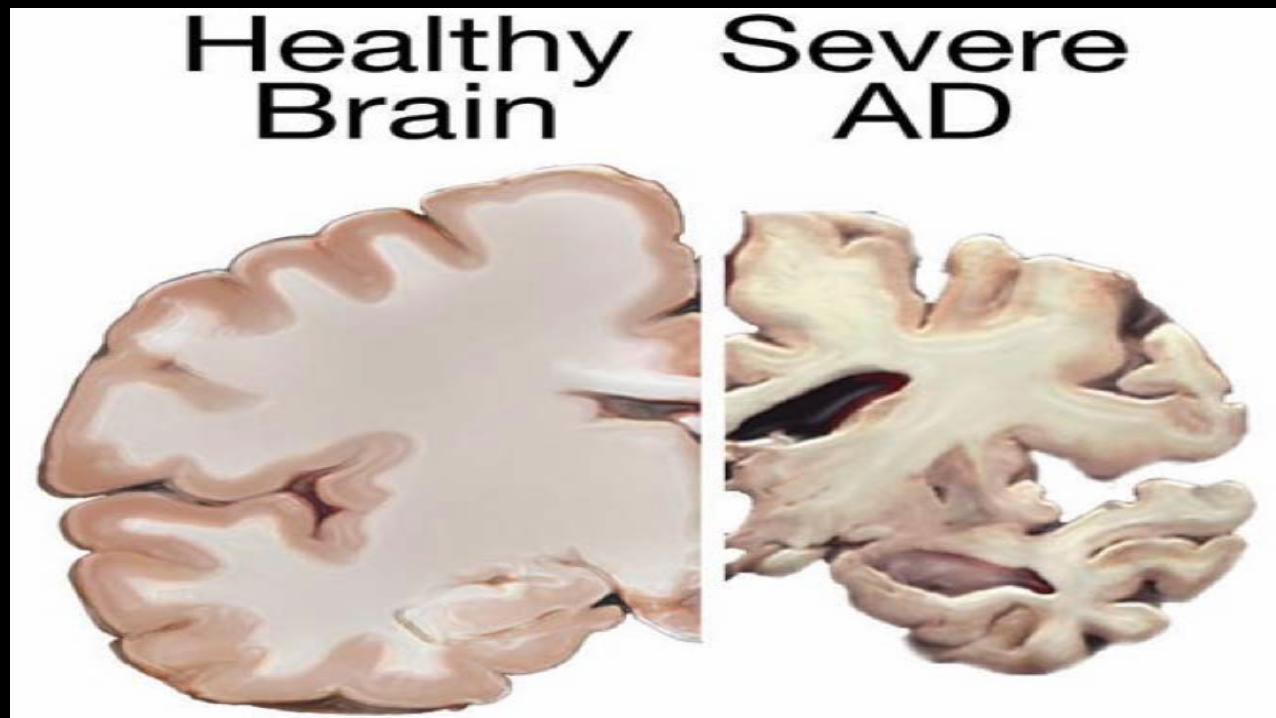
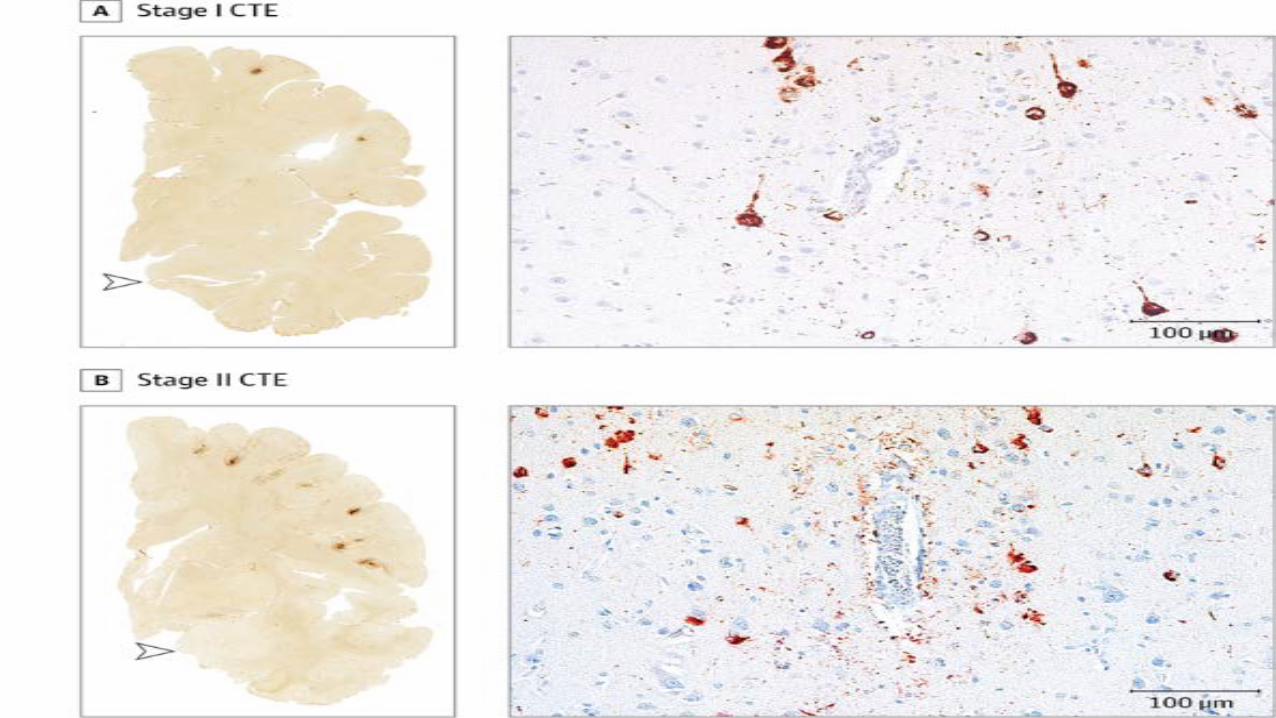
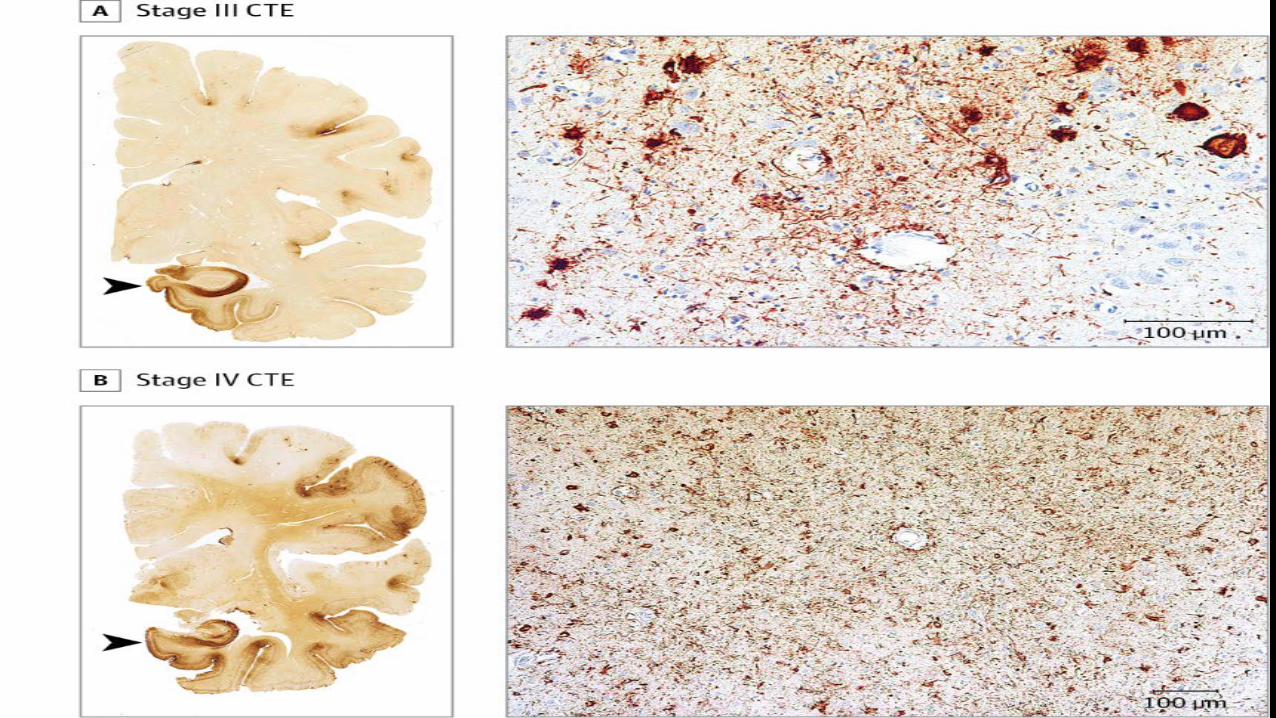
• Chronic traumatic encephalopathy (CTE)- Represents long term neurologic consequences of repetitive concussion and mild TBI. The condition is progressive. The pathology is Tau accumulation.
• It can only be diagnosed post-mortem.
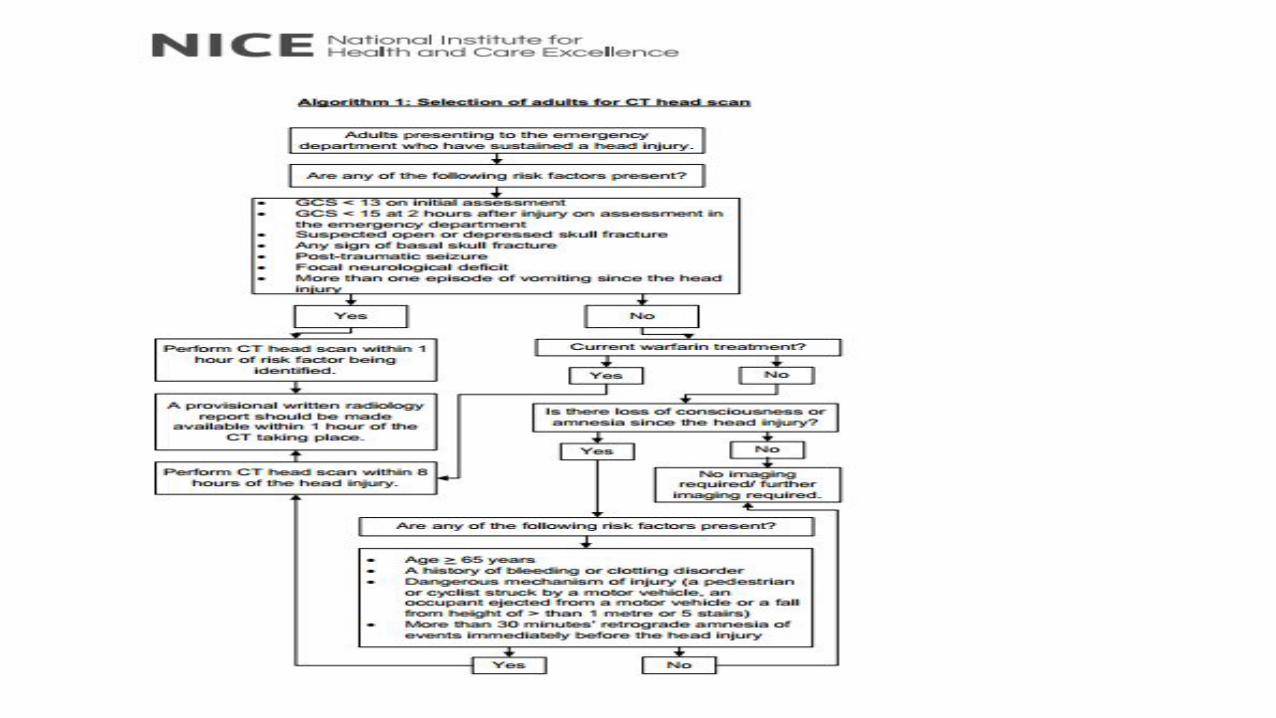
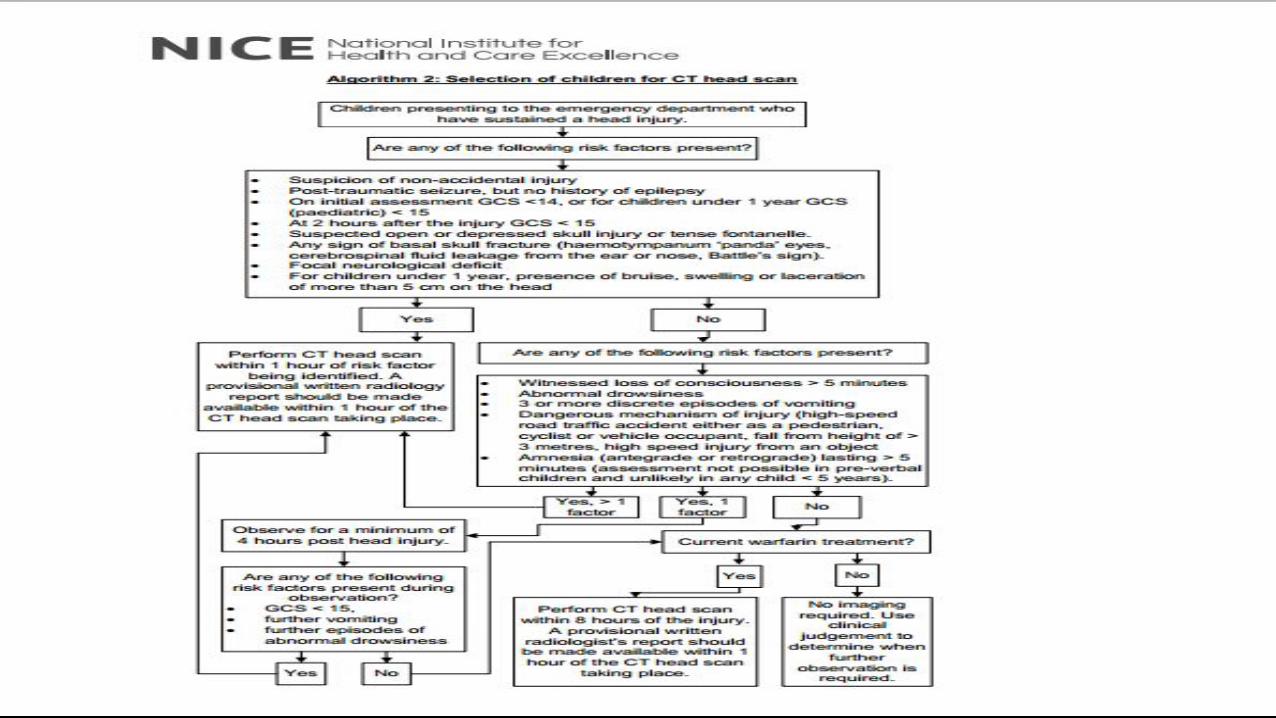
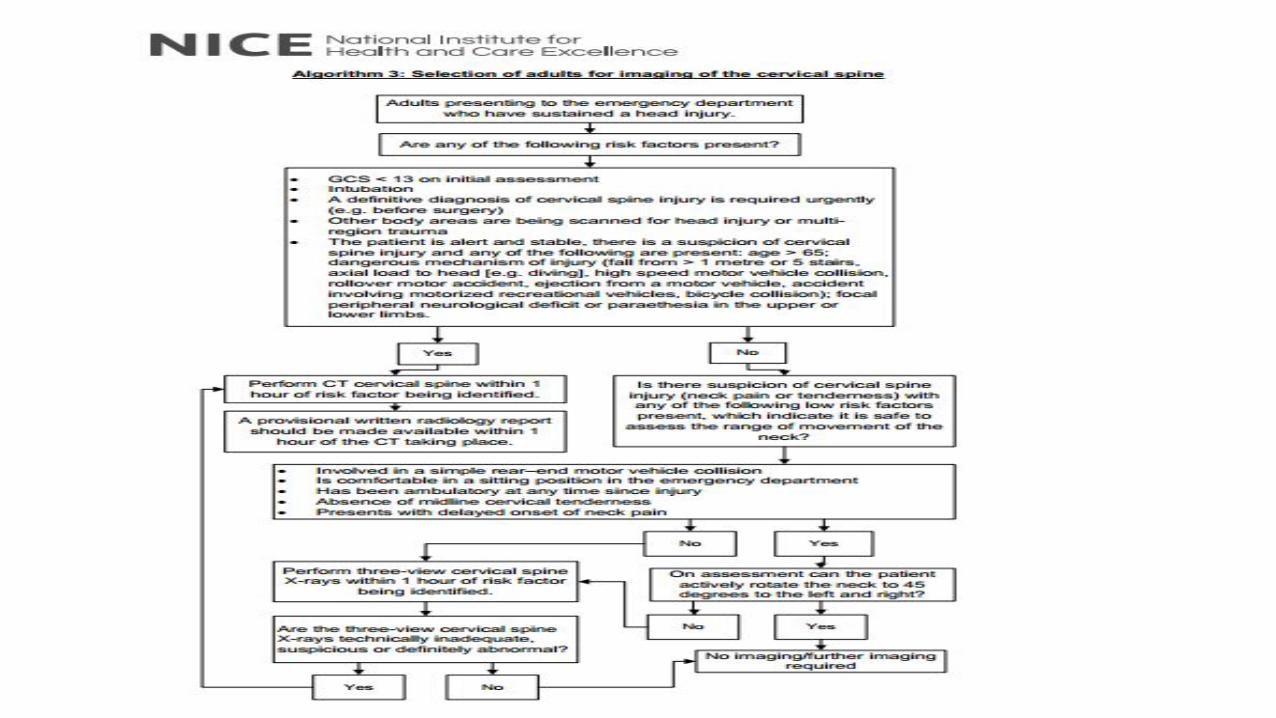
When to do Neuro-imaging?
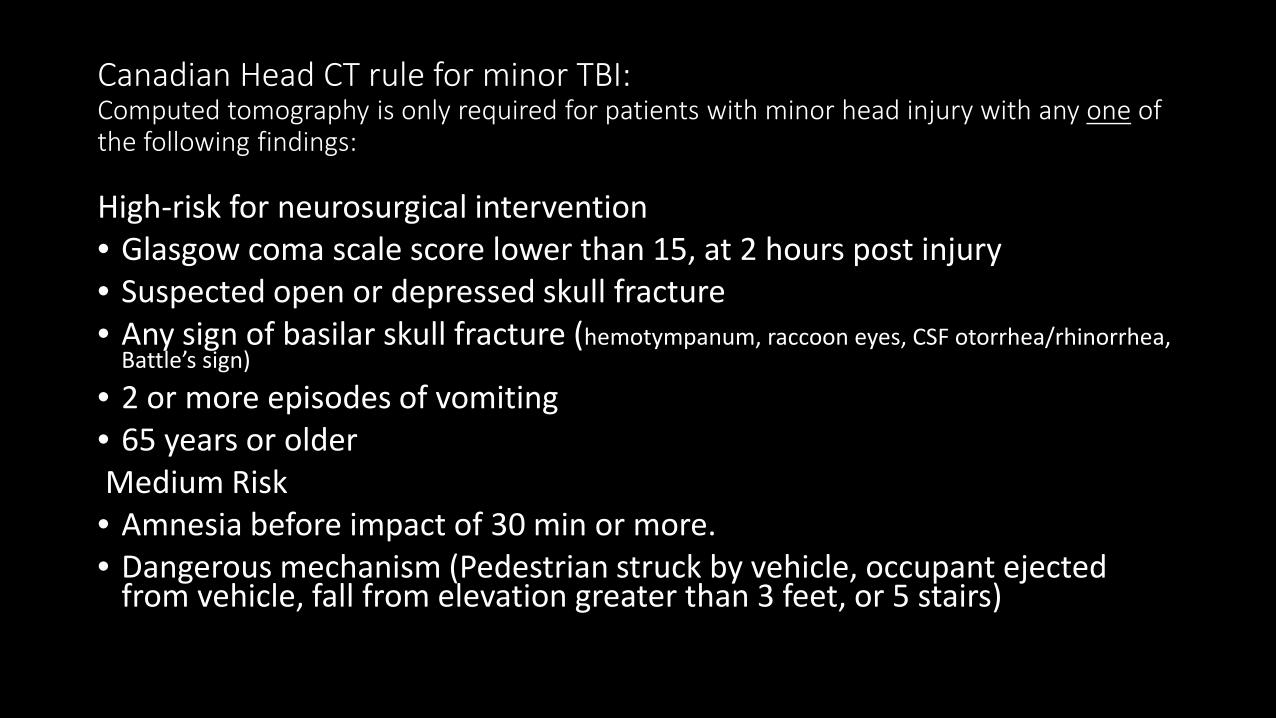
Canadian Head CT rule for minor TBI:Computed tomography is only required for patients with minor head injury with any one of the following findings:
High-risk for neurosurgical intervention• Glasgow coma scale score lower than 15, at 2 hours post injury• Suspected open or depressed skull fracture• Any sign of basilar skull fracture (hemotympanum, raccoon eyes, CSF otorrhea/rhinorrhea,
Battle’s sign)
• 2 or more episodes of vomiting• 65 years or olderMedium Risk• Amnesia before impact of 30 min or more.• Dangerous mechanism (Pedestrian struck by vehicle, occupant ejected
from vehicle, fall from elevation greater than 3 feet, or 5 stairs)
When to do Neuroimaging?
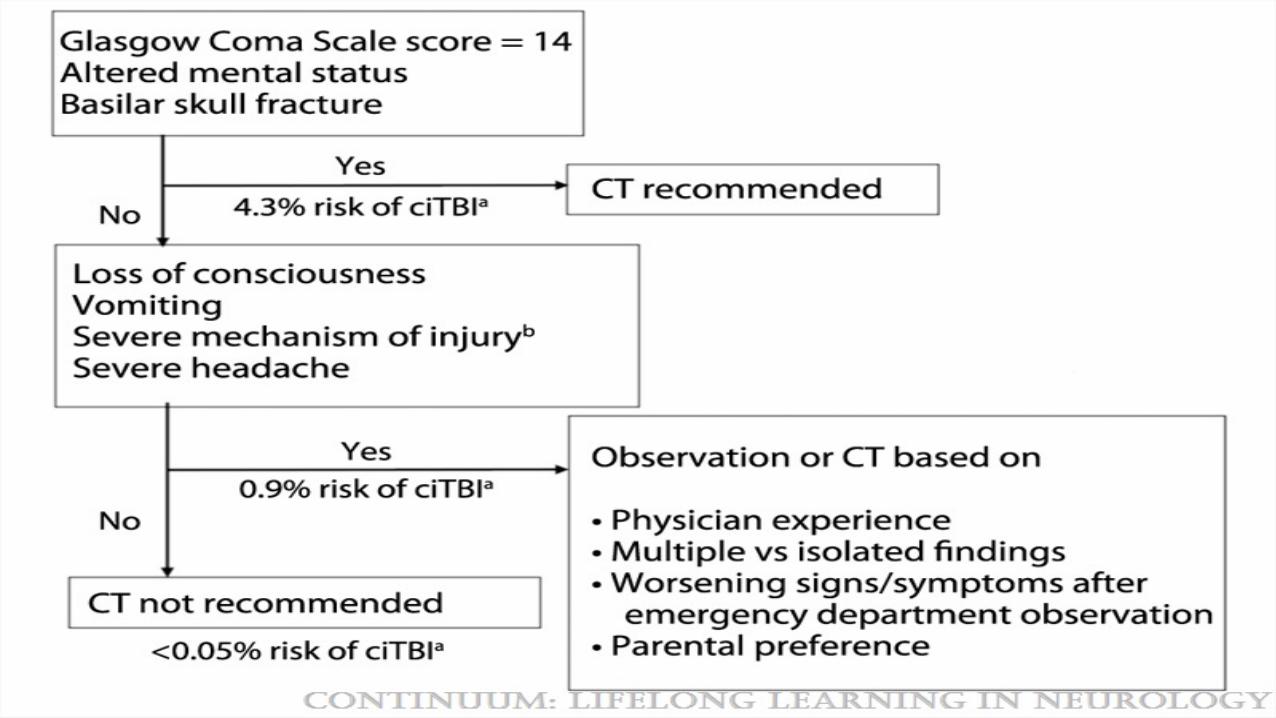
• a=ciTBI = Clinically important traumatic brain injury. This includes death due to TBI, TBI that requires neurosurgical intervention, intubation for more than 24 hours, or hospitalization for more than 2 days.
• B= Severe mechanism of injury (MVA with ejection, death of another passenger, rollover, pedestrian or cyclist without helmet struck by motor vehicle, fall more than 1.5 meters, or head hit by high impact object)
CONCLUSION: The professional football players most vulnerable to concussions are quarterbacks, wide receivers, and defensive secondary. Concussions involved 2.74 symptoms/injury, and players were generally removed from the game. More than one-half of the players returned to play within 1 day, and symptoms resolved in a short time in the vast majority of cases.
Neurosurgery. 2004 Jan;54(1):81-94; discussion 94-6Pellman EJ1, Powell JW, Viano DC, Casson IR, Tucker AM, FeuerH, Lovell M, Waeckerle JF, Robertson DW.Concussion in professional football: epidemiological features of game injuries and review of the literature--part 3.
CONCLUSION: This case highlights potential long-term neurodegenerative outcomes in retired professional National Football League players subjected to repeated mild traumatic brain injury. The prevalence and pathoetiological mechanisms of these possible adverse long-term outcomes and their relation to duration of years of playing football have not been sufficiently studied. We recommend comprehensive clinical and forensic approaches to understand and further elucidate this emergent professional sport hazard.Omalu BI1, DeKosky ST, Minster RL, Kamboh MI, Hamilton RL, Wecht CH.
Neurosurgery. 2005 Jul;57(1):128-34; discussion 128-34.Chronic traumatic encephalopathy in a National Football League player.
Concussion: “History”
• In the early 20th century mild traumatic brain injury and concussion were debated, but it was generally accepted it wasn’t a serious injury.
• Joseph Babinski, and Derek Denny-Brown published papers detailing effects of concussive and blast injuries. Many of their contemporaries argued against the injuries very existence. Denny-Brown DE, Experimental concussion. Proc R Soc Med 1941;34(11):
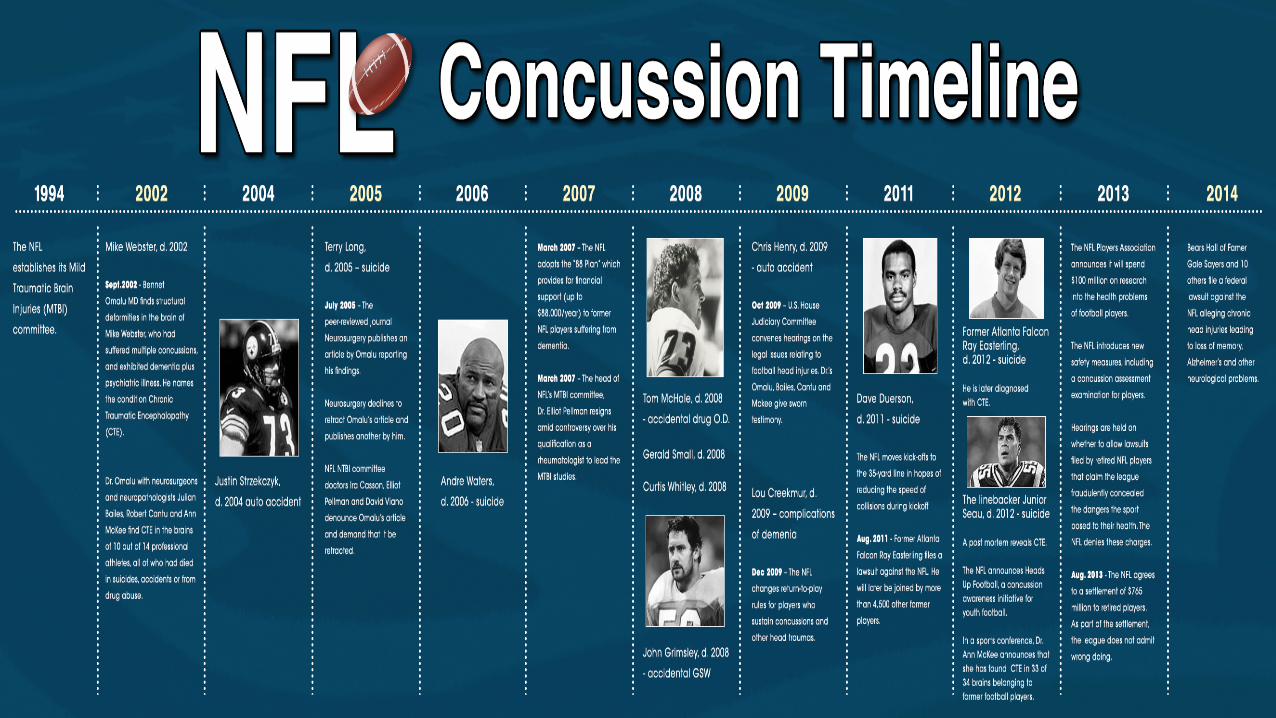
• 1994 NFL establishes the committee on mild traumatic brain injury.
Concussion “History”
• 1997 The American Academy of Neurology (AAN) published its first practice parameter on sports concussion. Neurology 1997;48(3):581-585
• September 2002 – Bennet Omolu finds structural abnormalities in the brain of former NFL player Mike Webster, who had symptoms of dementia, psychiatric illness. He named the pathologic findings Chronic traumatic encephalopathy ( CTE)
• Dr. Omolu and colleagues find CTE in the brains of 10-14 professional athletes all of whom died in suicides, accidents, or from drug abuse.
Concussion “History”
• NFL first implemented the concussion protocol in 2009.• Revised it in 2011 and continue to “tweak” it.• 2016 NFL issues fines to teams that don’t follow the protocol.
Hits to the head not concussions cause CTE:Brain, Volume 141, Issue 2, 1 February 2018, Pages 422–458,
• Concussion may be irrelevant to the onset of CTE. It’s the hit, likely sub-concussive injury.
• Brain samples observed in teenagers with head injury unrelated to concussion
• The findings provide strong causal evidence linking head impact to TBI and early CTE independent of concussion.
• This may explain why approx. 20 % of athletes with CTE never suffered a diagnosed concussion.
• Therefore we may be looking at the wrong thing. The focus on concussion doesn’t tell you anything about a TBI or CTE.
Resources
• Oklahoma State Department of health website has a online course for physicians, coaches, and anyone interested in concussion. www.ok.govsearch concussion.
• American Academy of Neurology- They also support and App that is very useful and comprehensive on common signs and symptoms of concussion, return to play etc. https://www.aan.com/concussion.
• CDC has an excellent website on concussion training, provider tools, discharge instructions, return to play, laws on concussion. http://www.cdc.gov/Concussion/HeadsUp/online_training.html
• National Federation of State High School Association Training Courses:http://www.nfhslearn.com/index.asp
Conclusion:
• Concussion is a clinical syndrome related to brain trauma, but may be indirect trauma. It’s a syndrome.
• The vast majority of patients you will see are not involved in future at risk activities but need to be aware of current treatment recommendations.
• Be aware of complications of concussion. • Sports related concussion is in its infancy and is evolving.• Be aware of the laws regarding sports related concussion in your
state. Every state has them.





![REVIEW Open Access Traumatic brain injury: pathophysiology ...homeostasis [1], neurotransmitter release (e.g., glutamate excitotoxicity) [2], mitochondrial dysfunction [3], neur-onal](https://static.documents.pub/doc/80x56/6090d88d03865410793ff8f2/review-open-access-traumatic-brain-injury-pathophysiology-homeostasis-1.jpg)











