Risks of Serious Risks of Serious Maltreatment Without Maltreatment Without Additional Child Welfare Additional Child Welfare Services Services Richard P. Barth Richard P. Barth School of Social Work School of Social Work University of Maryland University of Maryland [email protected][email protected]Race & Child Welfare--Disproportionality, Disparity, Discrimination: Re-Assessing the Facts, Re-Thinking the Policy Options Harvard Law School January 28-29, 2011
Transcript
Risks of Serious Risks of Serious Maltreatment Without Maltreatment Without
Richard P. BarthRichard P. BarthSchool of Social WorkSchool of Social Work University of MarylandUniversity of [email protected]@ssw.umaryland.edu
Race & Child Welfare--Disproportionality, Disparity, Discrimination: Re-Assessing the Facts, Re-Thinking the Policy Options
Harvard Law SchoolJanuary 28-29, 2011
3 Main Ideas3 Main Ideas1.1. African American (AA) children are at least as African American (AA) children are at least as
likely to be likely to be underunderserved as served as overoverserved—an served—an adequate discussion of child protection reform adequate discussion of child protection reform requires serious consideration of underservice to requires serious consideration of underservice to AA childrenAA children
2.2. The current analysis of disproportionality leads to The current analysis of disproportionality leads to the conclusion that there is a problem that can be the conclusion that there is a problem that can be solved, primarily, by better solved, primarily, by better decision makingdecision making —we —we need to expand the discussion to include the need need to expand the discussion to include the need for better for better servicesservices
3. Child welfare services are not well designed or sufficiently available to children and families of any race or ethnicity and require continuous improvement
3 Further Conclusions3 Further Conclusions Available evidence indicates that African Available evidence indicates that African
American children may be more likely than American children may be more likely than white or Hispanic children to experience white or Hispanic children to experience maltreatment, to experience severe maltreatment, to experience severe maltreatment, and to experience serious maltreatment, and to experience serious consequences from the maltreatmentconsequences from the maltreatment
Reducing disproportionality is not a primary Reducing disproportionality is not a primary goal of CWS, per se—our goal is to improve goal of CWS, per se—our goal is to improve the quality of child and family services for all the quality of child and family services for all childrenchildren
There is currently not substantial scientific There is currently not substantial scientific evidence that cultural competency training is evidence that cultural competency training is an important path to CWS improvements, no an important path to CWS improvements, no matter how laudable it soundsmatter how laudable it sounds
The Central Question in Lay Terms
Should we be so worried that the Should we be so worried that the child welfare system is unfair or child welfare system is unfair or racist that we allow minority racist that we allow minority children to be underserved and children to be underserved and unprotected?unprotected?
Are our interventions failing to Are our interventions failing to mitigate the greater risk and needs mitigate the greater risk and needs of minority children and their of minority children and their families?families?
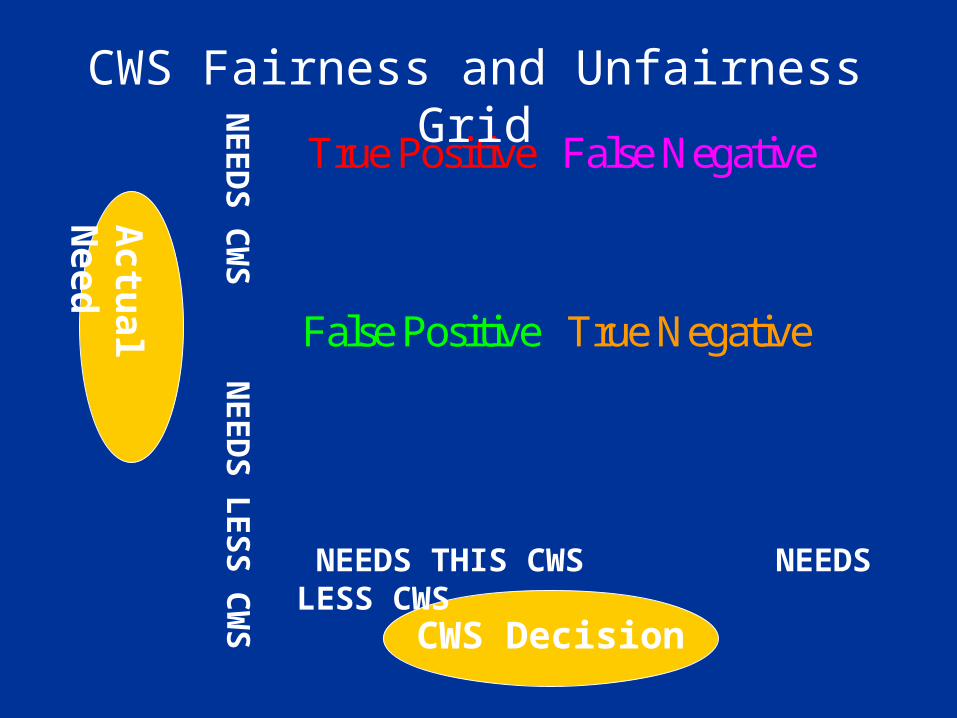
True Positive
False Negative
False Positive
True Negative
CWS Decision
Actu
al Need
NEEDS THIS CWS NEEDS LESS CWS
NE
ED
S C
WS
NE
ED
S L
ES
S C
WS
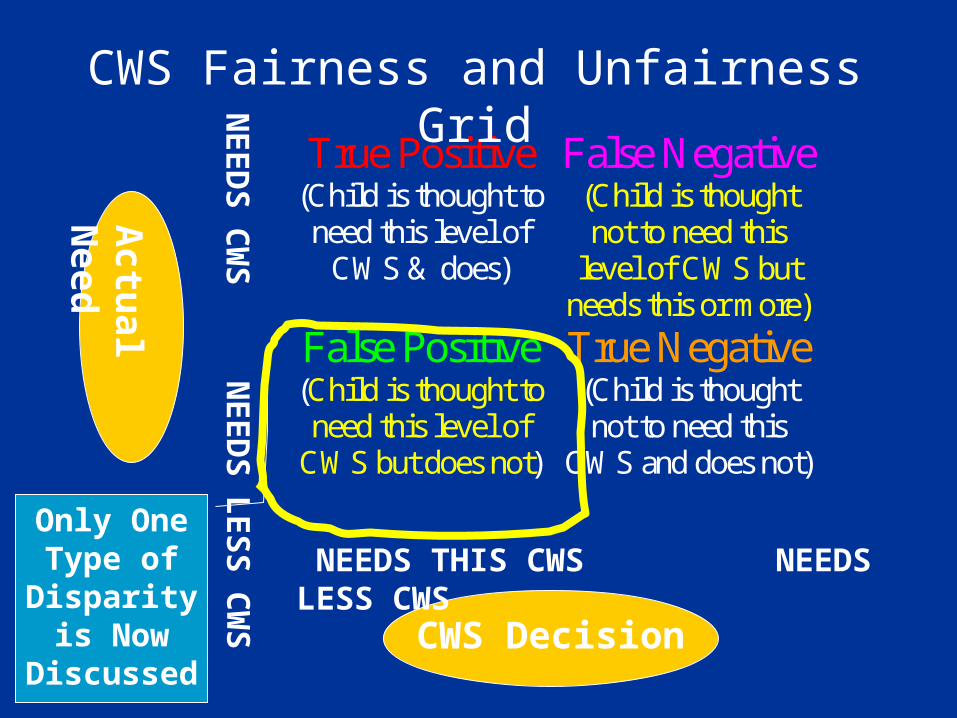
CWS Fairness and Unfairness Grid
True Positive (Child is thought to need this level of
CWS & does)
False Negative (Child is thought not to need this
level of CWS but needs this or more)
False Positive (Child is thought to need this level of
CWS but does not)
True Negative (Child is thought not to need this
CWS and does not)
CWS Decision
Actu
al Need
NEEDS THIS CWS NEEDS LESS CWS
NE
ED
S C
WS
NE
ED
S L
ES
S C
WS
CWS Fairness and Unfairness Grid
Only One Type of
Disparity is Now
Discussed
True Positive (Child is thought to need this level of
CWS & does)
False Negative (Child is thought not to need this
level of CWS but needs this or more)
False Positive (Child is thought to need this level of
CWS but does not)
True Negative (Child is thought not to need this
CWS and does not)
CWS Decision
Actu
al Need
NEEDS THIS CWS NEEDS LESS CWS
NE
ED
S C
WS
NE
ED
S L
ES
S C
WS
CWS Fairness and Unfairness Grid
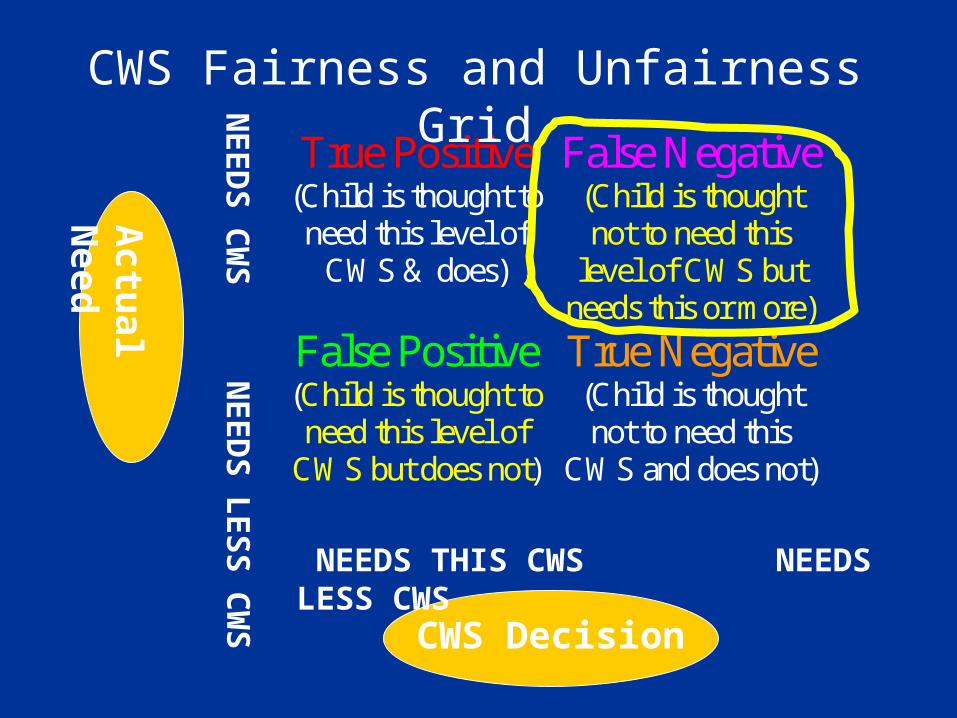
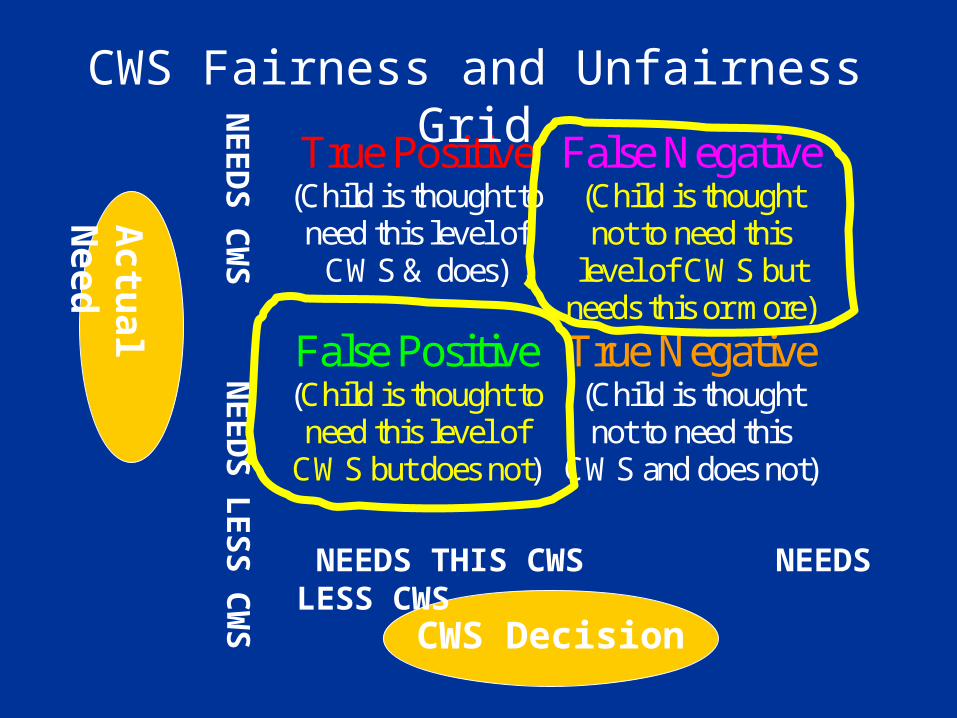
True Positive (Child is thought to need this level of
CWS & does)
False Negative (Child is thought not to need this
level of CWS but needs this or more)
False Positive (Child is thought to need this level of
CWS but does not)
True Negative (Child is thought not to need this
CWS and does not)
CWS Decision
Actu
al Need
NEEDS THIS CWS NEEDS LESS CWS
NE
ED
S C
WS
NE
ED
S L
ES
S C
WS
CWS Fairness and Unfairness Grid
Refocus on Risk of False Refocus on Risk of False NegativesNegatives
FOCUS ON FALSE POSITIVES, ONLY FOCUS ON FALSE POSITIVES, ONLY [OVERSERVICE][OVERSERVICE] The disproportionality argument shifts the child The disproportionality argument shifts the child
welfare field from one that has had a lower level of welfare field from one that has had a lower level of acceptability for false positives to one that has a high acceptability for false positives to one that has a high level of UNacceptability for false positives (i.e., level of UNacceptability for false positives (i.e., treating an African American family as if child abuse treating an African American family as if child abuse has occurred when it has not is the major concern). has occurred when it has not is the major concern).
FOCUS ON FALSE NEGATIVES, TOO FOCUS ON FALSE NEGATIVES, TOO [UNDERSERVICE][UNDERSERVICE] The remainder of my comments will be an argument The remainder of my comments will be an argument
for refocusing on the seriousness of rejecting true for refocusing on the seriousness of rejecting true positives (i.e., not serving children who need positives (i.e., not serving children who need protection at the level of service needed a refocusing protection at the level of service needed a refocusing toward avoiding underservice)toward avoiding underservice)
4 Reasons to Refocus on False Negatives
1. African American children are maltreated more often
2. African American children are not overserved
3. African American children are maltreated more severely
4. African American children are more likely to experience poor outcomes following maltreatment
AA Children More Likely to be Maltreated
NIS 1- 4 (Brett Drake has made this case) Maternal arrest is a predictor of child abuse
reports and placement into foster care and 3.5Xs as many black women as white women are incarcerated (Albert, et al., 1996; Pew, 2008; Phillips et al., 2004)
Higher rate of traumatic brain injury (TBI) for African American (AA) children (Martin & Falcone, 2008), typically occurring while with family members
Probably Not Overserved Misdiagnosis of abusive head trauma (AHT) was higher for white children
indicating that they may be more often underreported and the accuracy of reporting for African American children is greater (Jenny, et al., 1999) [Suggests underservice for whites which later cost them their lives, in this study]
Higher rates of injury death for young (0-5) AA children in California when they were reported to CWS and screened out (Putnam-Hornstein, 2010)
African American children remaining in foster care had lower mortality than those that left and the general population of African American children in California (Blackwell & Barth, 1998).
African American children have less access to quality emergency health care (Riera & Walker, 2010); and mental health care (Burns et al., 2006) .
Abused More Severely NSCAW: By parent’s self-report, twice as many AA caregivers
(18.1%) investigated for maltreatment reported (on the CTS) using severe violence than white caregivers (5.6% at intake and during the next 36 months (19% v. 9%, OR = 2.3Xs) (Kohl, 2007).
Intentional injury deaths for CWS-involved children (0-5) 5.5Xs as high for Black children than white in CA (Putnam-Hornstein, 2010)
Nationally, a 3Xs higher rate of homicide victimization among AA children (CDC, 2006-2009); most of these murders are by family members
In study using the National Pediatric Trauma Registry, AA children had significantly increased indication of penetrating trauma and violent intent (Haider et al., 2007)
Experience Worse Outcomes Marginally higher rates of death for AA children following
child abuse in MO (Jonson-Reid, Drake, & Chance, 2007),
Higher mortality for African Americans even when controlling for severity of TBI (Haider et al., 2007) and insurance (Falcone, Brown, Garcia, 2007; Mushkudiani, et al., 2007);
For infant deaths from TBI, AA race has bivariate association (p < .14) but is not an independent factor (income and insurance matter) (Rangel, Burd, & Falcone, 2010)
Higher rates of mortality among children who have experienced referral to child welfare services in California (Putnam-Hornstein, 2010).
Caveat: Underservice is not Proven
Research is not definitive and may never be: These are dense issues with many confounding factors Little independently funded research exists with models
that are adequately specified Understanding human behavior without any self-report ed
data about maltreatment is extraordinarily difficult
Underservice in CWS is likely because we see so much of it in human services—basically, poorer people live in communities with poorer services
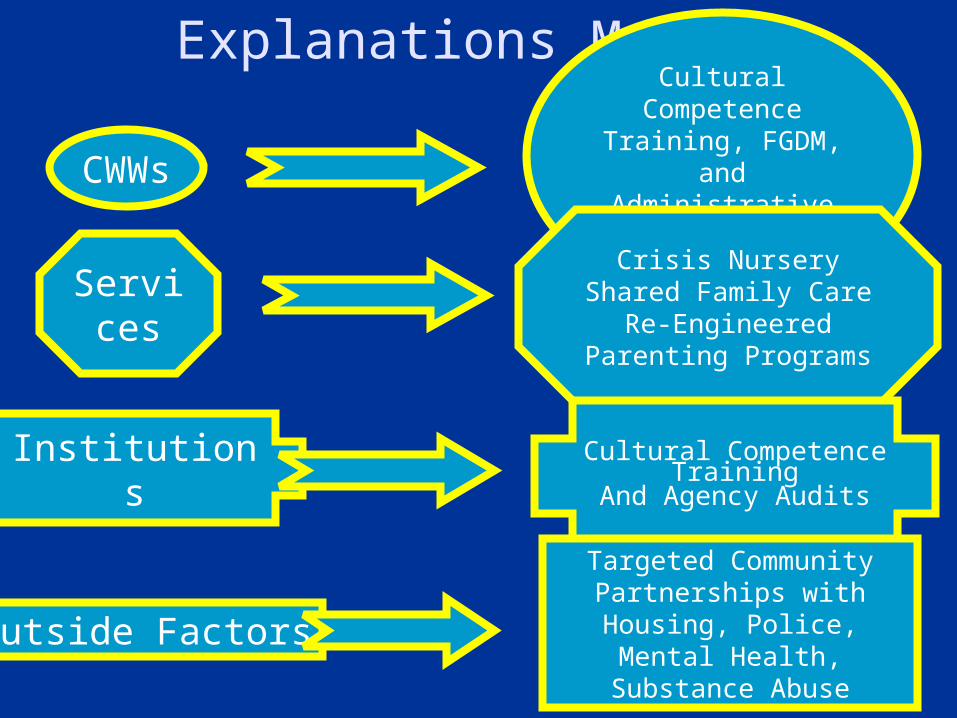
Explanations Matter
CWWs
Services
Institutions
Outside Factors
Cultural Competence
Training, FGDM, and Administrative
Review
Crisis NurseryShared Family Care
Re-Engineered Parenting Programs
Cultural Competence Training
And Agency Audits
Targeted Community Partnerships with
Housing, Police, Mental Health, Substance Abuse
Closing Caveats Nothing in this presentation should be
interpreted to suggest that African American children receive child welfare services that are meeting their needs as well, are as comprehensive as, or are as helpful as those provided for other children. Available research cannot speak to that issue.
Nothing in these data should be taken to indicate that the disproportionately high (per population) involvement in child welfare services for African Americans cannot be reduced with service improvements.
Partial ReferencesAnderson, L. M., Scrimshaw, S. C., Fullilove, M. T., Fielding, J. E., & Normand, J. (2003).
Culturally competent healthcare systems: A systematic review. American Journal of Preventive Medicine, 24(3, Supplement 1), 68-79.
Barth, R. P., & Blackwell, D. L. (1998). Death rates among California's foster care and former foster care populations. Children and Youth Services Review, 20, 577-604.
Brown, R. L. (2010). Epidemiology of injury and the impact of health disparities. [Review]. Current Opinion in Pediatrics, 22(3), 321-325. doi: 10.1097/MOP.0b013e3283395f13
Burns, B. J., Phillips, S. D., Wagner, H. R., Barth, R. P., Kolko, D. J., Campbell, Y., & Landsverk, J. (2004). Mental health need and access to mental health services by youth involved with child welfare. Journal of the American Academy of Child and Adolescent Psychiatry, 43, 960-970.
Center for Disease Control. (2009). Deaths, percent of total deaths, and death rates for 15 leading causes of death in 10 year age groups, by race and sex: US, 2003. Atlanta, GA: Author, http://www.cdc.gov/nchs/data/dvs/lcwk2_2003.pdf.
Chipps, J. A., Simpson, B., & Brysiewicz, P. (2008). The effectiveness of cultural-competence training for health professionals in community-based rehabilitation: A systematic review of literature. Worldviews on Evidence-Based Nursing, 5(2), 85-94.
Partial ReferencesFalcone, R.A., Jr, Brown, R.L., & Garcia, V.F., (2007) Disparities in child abuse mortality are
not explained by injury severity. Journal of Pediatric Surgery 42(6),1031–1037.
Haider, A.H., Efron, D. T., Haut E.R., Dirusso, S. M., Sullivan, T., Cornwell, E.E., & Stallion, A. (2007). Black children experience worse clinical and functional outcomes after traumatic brain injury: An analysis of the National Pediatric Trauma Registry. Journal of Trauma, 62, 1259–1262; discussion 62–3.
Jenny, C., Hymel, K., Ritzen, A., Reinert, S., & Hay, T. (1999). Analysis of missed cases of abusive head trauma. The Journal of the American Medical Association, 621-626.
Jonson-Reid, M., Chance, T., & Drake, B. (2007). Risk of death among children reported for nonfatal maltreatment.(vol 12, pg 86, 2007). Child Maltreatment, 12(2), 199-199.
Kohl, P. L. (2007). Unsuccessful in-home child welfare service plans following a maltreatment investigation: Racial and ethnic differences. Seattle, WA: Casey Family Programs.
Martin, C.A., & Falcone, R. A. Jr. (2008). Pediatric traumatic brain injury: An update of research to understand and improve outcomes. Current Opinion in Pediatrics. 20(3), 294-299.
Partial References Mushkudiani, N.A., Engel, D.C, Steyerberg, E.W., Butcher, I., Lu, J., Marmarou, A., Slieker, F. et
al. (2007). Prognostic value of demographic characteristics in traumatic brain injury: results from the IMPACT study. Journal of Neurotrauma, 24(2), 259-269.
Phillips, S., Burns, B. J., Wagner, H. R., & Barth, R. P. (2004). Parental arrest and children involved with child welfare services. American Journal of Orthopsychiatry, 74, 174-186.
Putnam-Hornstein, E. (2010).. Do “Accidents” Happen? An Examination of Injury Mortality Among Do “Accidents” Happen? An Examination of Injury Mortality Among Maltreated Children. Maltreated Children. Berkeley, CA:: University of Caliifornia, School of Social Welfare. Unpublished Dissertation..
Rangel, E. L., Burd, R. S., Falcone, R. A., & Multictr Child Abuse Disparity, G. (2010). Socioeconomic Disparities in Infant Mortality After Nonaccidental Trauma: A Multicenter Study. [Proceedings Paper]. Journal of Trauma-Injury Infection and Critical Care, 69(1), 20-25. doi: 10.1097/TA.0b013e3181bbd7c3.
Riera, A., & Walker, D. M. (2010). The impact of race and ethnicity on care in the pediatric emergency department. [Review]. Current Opinion in Pediatrics, 22(3), 284-289. doi: 10.1097/MOP.0b013e32833973a5
U.S. Department of Health and Human Services Administration for Children and Families. (2005). National Survey of Child and Adolescent Well-Being: Children involved with the child welfare sservices (Baseline Report). Washington, DC: Author.