is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from
Intracranial atherosclerosis, one of the leading causes of ischemic stroke, is associated with an increased risk
for recurrent stroke and dementia.1,2 Individuals of Asian, Hispanic, and African American ancestry are especially affected. Recent European studies revealed a much higher prevalence of intracranial lesions than commonly presumed, suggesting that intracranial atherosclerotic disease is poten-tially the most common cause of ischemic stroke world-wide.1,3 Ischemic strokes are clinically categorized into 5 subtypes based on their underlying cause: large-artery ath-erosclerotic stenosis, small-artery disease (lacunes), crypto-genic, major-risk-source cardiogenic embolism, and unusual (eg, dissections, arteritis). Most nonlacunar ischemic strokes are thought to be thromboembolic, which presumably also accounts for most cryptogenic strokes. Embolic sources include minor-risk or covert cardiac sources, veins via para-doxical embolism, and nonocclusive atherosclerotic plaques in the aortic arch or cervical or cerebral arteries.4 Besides embolic strokes, 2 other mechanisms have been associated with intracranial atherosclerosis-related strokes, namely hypoperfusion through a stenotic artery causing watershed or border-zone stroke and plaque overgrowth of perforator artery ostia, which is associated with penetrating artery dis-ease and lacunar infarcts and has been related to cryptogenic strokes.5–7 Even mild stenosis of intracranial atherosclerotic arteries (<50%) may therefore be clinically relevant, and high-resolution magnetic resonance imaging studies are needed to identify and determine the degree and location of stenosis in this patient group.5,8 The possibly causal role of nonstenotic plaques in ischemic stroke highlights the need for more insight into the mechanisms and occurrence of intracranial atherosclerosis.
In the 1960s and 1970s, large, descriptive autopsy studies were conducted, providing classic morphological features of intracranial arteries. Despite the importance of intracra-nial atherosclerosis to stroke and dementia, there is a lack of more recent mechanistic studies. Therefore, we intend to draw attention to this neglected research field by providing an over-view of available literature and a working model for intracra-nial atherosclerosis.
Search StrategyA MEDLINE search was performed of literature published in English using the MeSH term intracranial atherosclerosis. A total of 8146 search hits were obtained for articles published before October 2013 and screened for relevance to the cause and mechanisms of intracranial atherosclerosis. Other refer-ences were extracted by cross-reference. Only studies includ-ing ≥10 patients were considered relevant. Because of space restrictions, we were able to include only a subset of refer-ences in this study; the remaining references can be found in Table I in the online-only Data Supplement.
EpidemiologyIncidence and PrevalenceIn 45% to 62% of patients with ischemic stroke, intracranial plaques or stenoses were identified, which were causal in ≈10% to 20% of cases (reviewed elsewhere9). The estimated prevalence of symptomatic intracranial stenosis in literature ranges from 20% to 53%, depending on the study population, race, and method of choice (Table II in the online-only Data Supplement), and from 3% to 82% in asymptomatic patients. Most studies revealed a higher incidence of intracranial ath-erosclerosis in Asians and African Americans compared with white Americans. The few studies on white Europeans that are available suggest a high prevalence of intracranial plaques or stenosis. One French autopsy study detected intracranial plaques and stenosis in 62% and 43% of stroke cases, respec-tively, and in a Dutch study, 82% of asymptomatic patients showed calcification of the intracranial internal carotid artery (ICA) by computed tomography.3,8 Notably, magnetic reso-nance angiography, computed tomography angiography, and transcranial Doppler, which measure luminal changes, may underestimate the number of intracranial plaques, partly explaining the large differences in the literature.8
Onset, Course, and DistributionIn the 1960s and 1970s, several large-scale autopsy studies performed in asymptomatic cohorts from fetuses to patients in their 10th decade of life revealed intracranial atherosclerotic
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.114.011147
From the Departments of Pathology (K.R., N.P.D., O.C.G.S., M.J.A.P.D.) and Internal Medicine (J.J.v.L.), Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands; Laboratory for Clinical Cardiovascular Physiology, AMC Center for Heart Failure Research, Academic Medical Centre, Amsterdam, The Netherlands (J.J.v.L.); and MRC/Arthritis Research UK Centre for Musculoskeletal Ageing Research, School of Life Sciences, University of Nottingham Medical School, Queen’s Medical Centre, Nottingham, UK (J.J.v.L.).
The online-only Data Supplement is available with this article at http://circ.ahajournals.org/lookup/suppl/doi:10.1161/CIRCULATIONAHA. 114.011147/-/DC1.
Correspondence to Mat J.A.P. Daemen, MD, PhD, Department of Pathology, Academic Medical Center, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands. E-mail [email protected]
Cause and Mechanisms of Intracranial AtherosclerosisKatja Ritz, PhD; Nerissa P. Denswil, MSc; Olga C.G. Stam, MD;
Johannes J. van Lieshout, MD, PhD; Mat J.A.P. Daemen, MD, PhD
Contemporary Reviews in Cardiovascular Medicine
at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from
changes from the first to second decade, progressing with age.10,11 Advanced atherosclerotic lesions are almost non-existent up to the fourth decade.12 Overall, intracranial ath-erosclerosis develops ≈20 years later in life compared with atherosclerosis in extracranial arterial beds.13 Progression of atherosclerosis was not parallel in different vascular beds. Although aortic atherogenesis progressed linearly, intracra-nial atherosclerosis increased more slowly initially and paral-leled aortic lesions thereafter.12 The steepest gradient for the incidence of intracranial atherosclerosis was reported in the sixth and seventh decades,10 with a steady increase beyond the eighth and ninth decades,11 whereas coronary atherosclerosis progressed more rapidly initially and attenuated between the fifth and eighth decades.12 Three percent to 4% of individu-als >80 years of age exhibited only mild intracranial athero-sclerotic changes.10,12 Intracranial atherosclerotic stenoses were described as dynamic lesions showing progression and regression, but they were less dynamic than coronary stenoses. Repeated magnetic resonance angiography over a 7-year period in patients with ischemic heart disease showed a 1.1% annual progression of the average intracranial stenosis. Differences among the intracranial vessels were evident with stable ath-erosclerosis in the intracranial ICA and dynamic lesions in the anterior (ACA), middle (MCA), and posterior (PCA) cerebral arteries, with 2.6% annual progression of average stenosis. Regression was noted in 14% of intracranial ICAs and 28% of ACAs, MCAs, and PCAs.14 A 5-year longitudinal study of 41 Japanese patients with ischemic heart disease reported the pro-gression of cervical carotid artery stenosis in 5 patients (12%) and in only 1 patient with intracranial stenosis.15 During a 2- to 3-year follow-up of 40 stroke patients, 33% of MCA steno-ses progressed and 8% regressed.16 Intracranial lesions were identified predominantly in the anterior circulation.17 Overall, American and European studies showed a similar pattern: The
ICA was most commonly affected, followed by the MCA, bas-ilar artery (BA), intracranial vertebral artery (VA), PCA, and ACA (Figure 1).10,18 The MCA appeared to be most commonly involved in Asians, followed by the ICA, BA, VA, PCA, and ACA.17 In all cohorts, cerebellar and communicating arteries were barely affected. Atherosclerosis in the intracranial ICA was observed mainly in the cavernous but also in the supracli-noid segment.18,19 The BA was commonly affected in the upper and lower parts and less affected in the middle part.20 MCA lesions were mainly found in the M2 segment.18
MorphologyBasic StructureOne major characteristic that distinguishes healthy intracranial from extracranial arteries is that extracranial arteries such as the aorta and carotid arteries are elastic arteries rich in elastin filaments in the tunica media. In contrast, intracranial arteries are muscular arteries with few elastic fibers.21 The transition from elastic to muscular artery is at the level of the carotid bifurcation22 and embryological junctions between segments of the VA and ICA, which has been attributed to different embryological sites of origin of their primordial mesodermal cells.23 Compared with extracranial arteries of a similar size, a thinner media, less abundant adventitia, and only a few elas-tic fibers have been reported for intracranial vessels13 with a denser internal elastic lamina and without an external elastic lamina.13,21 The external elastic lamina is still present in the petrous portion of the ICA but disappears within the cavernous portion, which forms a hotspot of stenosis.24 A distinct ves-sel wall metabolism was suggested for intracranial arteries. Intima-media preparations of unaffected intracranial arteries showed lower contents of hexosamine, uronic acid, and sulfur; a lower proportion of hyaluronic acid and chondroitin sulfates
Figure 1. Circle of Willis of a 90-year-old subject. Macroscopically, atherosclerotic lesions can be identified by the white vessels, whereas nondiseased arteries appear largely transparent. This case shows prominent atherosclerosis mainly in the internal carotid artery, vertebral artery, basilar artery, left middle cerebral artery, and posterior cerebral artery.
at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from
Ritz et al Mechanisms of Intracranial Atherosclerosis 1409
in the total glycosaminoglycans; and a lower ratio of ester to total cholesterol, whereas the percentage of heparin sulfate was higher compared with normal aorta and coronary arteries.25 In addition, unaffected intracranial arteries of all ages revealed elevated antioxidant enzyme activity (manganese superoxide dismutase, copper-zinc superoxide dismutase, catalase) com-pared with extracranial arteries. Animal studies in rats and rab-bits reported that the BA had less vesicles and caveolae and exhibited tight junctions between endothelial cells, leading to a reduced intimal permeability compared with the aorta and sug-gesting the presence of a barrier function.26,27 In monkeys and rabbits, a distinct composition of the glycocalyx on luminal endothelial cells was suggested in cerebral arteries; the car-bohydrate-binding protein concanavalin A reacted with aorta, coronary, and carotid arteries but not with cerebral arteries. It has been speculated that a specific glycocalyx composition inhibits trapping of chylomicrons and very-low-density lipo-protein, resulting in a reduced deposition of apolipoproteins in the intima of intracranial vessels.28 In cats, histamine stimula-tion showed a 3-fold-stronger contraction of extracranial com-pared with intracranial arteries.29 Smooth muscle cells of rabbit intracranial arteries were relatively insensitive to sympathomi-metic stimulation compared with systemic vessels.
Vasa VasorumVasa vasorum are an essential component of extracranial ves-sels that facilitate nourishing and elimination of wastes; their existence in intracranial vessels is controversial. Most animal studies claim that vasa vasorum are absent beyond the first 1 to 2 cm of dural penetration in studies on Wistar rats, cats, and dogs. In cats, the presence of rete vasorum in the adventitia was suggested, being in continuity with the subarachnoid space, permeable to large proteins, and allowing diffusion between the cerebrospinal fluid and medial layer.30 Rete vasorum were not observed in humans. Vasa vasorum are found mainly in proximal intracranial segments; are associated with aging and vascular pathological processes such as vasculitis, atheroscle-rosis, aneurysm, and thrombosis; and may represent a response to vascular damage (reviewed elsewhere31). Vasa vasorum were reported in the MCA (M1 and A1 segments) and proximal parts of the ICA, VA, and BA.32,33 They were not seen beyond the first 1.5 cm proximal segments of the intracranial arteries after dural penetration, which corresponds to arteries with a thickness of <250 μm and to arteries surrounded by nutrient-rich cerebrospinal fluid.31,32 It is our experience that adventitial stripping, especially of smaller arteries, which is barely avoid-able in autopsy studies, may lead to an underestimation of the presence of vasa vasorum. It has been suggested that vasa vasorum are required only beyond a critical vessel thickness to supplement luminal diffusion.32 The thin media and adven-titia, which may facilitate luminal diffusion, and the absence of the external elastic lamina, which may allow greater diffu-sion from the cerebrospinal fluid, support this theory.31 Recent evidence suggests a critical role for the adventitia, including vasa vasorum in atherogenesis by initiating an inflammatory cascade. Along this line, later onset of more stable intracranial lesions may be explained partly by the initial absence of adven-titial vasa vasorum, at least in normal intracranial arteries.31
Plaque Characteristics and Age-Related ChangesIn intracranial arteries, aging was associated with a gradual loss of elastic fibers and muscular elements in the media and an increase in collagen tissue replacing medial muscle fibers.34 From the second to third decade, reduplication and splitting of the thick internal elastic lamina were observed frequently in combination with intimal thickening, which was most promi-nent from the fifth to sixth decade. In the same age group, fibro-sis and hyalinization of media and adventitia prevailed.20 In the aorta and coronary arteries, fragmentation and reduplication of the internal elastic lamina were common in fetuses, infants, and young juveniles. In contrast to the aorta, lipids were rarely observed in intracranial arteries in patients <15 years of age.34
Intracranial lesions not only developed later in life com-pared with extracranial vessels but developed mainly as fibrous plaques with fewer fatty streaks and complicated lesions. Complicated lesions, which contain calcifications or a plaque rupture, appeared after the fifth decade with a degree of involvement and lipid content similar to that observed in coro-nary arteries and were limited mainly to proximal segments of the ICA, VA, and BA.12,13 Hoff35,36 reported no major dif-ferences in chemical and enzymatic plaque characteristics in intracranial compared with extracranial arteries and no quali-tative differences in apolipoproteins (apolipoprotein A1 from high-density lipoprotein, apolipoprotein B from low-density lipoprotein [LDL], apolipoprotein CIII from very-low-density lipoprotein).
Intracranial arteries of human fetuses from hypercholes-terolemic mothers showed fewer intimal macrophages and less intimal LDL, and oxidized LDL compared with extra-cranial arteries, which is suggestive of divergent atherogenic responses.37,38 Evidence for intracranial protective mechanisms comes from animal studies in rabbits. Hypercholesterolemia alone evoked a reduced intimal permeability and foam cell accumulation in the aorta but not in the BA, whereas the combination of hypercholesterolemia and hypertension also affected the permeability of intracranial arteries.27
Our Histological DataOur review of the literature made clear that histological data in a recent cohort are lacking. Therefore, we screened 283 cir-cle of Willis segments from 18 asymptomatic patients (mean age, 70.2±10.9 years; range, 51–90 years; male, 9; causes of death: cardiovascular disease, 8; malignancy, 3; subarachnoid hemorrhage, 2; Alzheimer disease, 2; sickle cell disease, 1; acute stroke, 1; HIV/hepatitis, 1) for basic structural features (Methods in the online-only Data Supplement). In accordance with previous literature, we identified mainly early lesions (63%) and a few advanced atherosclerotic lesions (15%). Calcifications were rare (6%). Two patients presented with complicated lesions (chronic total occlusion and intraplaque hemorrhage). Intracranial arteries, especially the smaller arteries (ACA, PCA, and cerebellar and communicating arter-ies), show a distinct structure such as the lack of vasa vasorum and an external elastic lamina and only a few medial elastic fibers compared with extracranial arteries. The larger intra-cranial arteries such as the ICA, MCA, VA, and BA, however, show an intermediate phenotype sharing structural features of both the larger extracranial and the smaller intracranial
at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from
arteries (Table 1), which may explain the conflicting results in literature. Macrophage load was low in our series, which is in line which previous observations38 (0.9±0.7% CD68 positivity per plaque area compared with 1.8±2.4% in coronaries).39 In general, intracranial arteries exhibited fewer and more stable lesions, and the few advanced atherosclerotic lesions were identified predominantly in the large intracranial arteries such as the ICA, MCA, and VA.
Risk FactorsNonmodifiable Risk Factors
AgeAge is one of the most important independent risk factors for both intracranial and extracranial atherosclerosis. Several autopsy and imaging studies showed that aging is associated with increasing prevalence and severity of intracranial ath-erosclerosis among all investigated races with, as mentioned above, a distinct disease progression compared with extracra-nial arteries.3,10,19,40
RaceAfrican Americans show a comparable or more severe degree of atherosclerosis compared with white Americans.41 In Asians, intracranial atherosclerosis developed earlier and more extensively compared with white Americans and Europeans.42 In symptomatic patients with transient ischemic attack or ischemic stroke, studies consistently reported the highest inci-dence and severity of intracranial atherosclerosis in Asians and Hispanics, followed by African Americans and whites. The reverse order was found for extracranial lesions.43,44 Differences in incidence and location of atherosclerosis were also observed within countries. Intracranial lesions in symp-tomatic patients were more common in North than in South China, which has been attributed to a more Westernized life-style in North China.45 Within African populations, Nigerians had lower atherosclerotic scores compared with Senegalese, Ugandans, and African Americans, with highest scores in the last group.46,47 Therefore, observed differences among races cannot be attributed to genetic factors only but are highly influenced by lifestyle and other risk factors. In addition, most studies do not take into account differences in the prevalence of vascular risk factors, being higher in Hispanic and African American populations and maybe resulting in an overrepre-sentation of specific races in intracranial atherosclerosis.48
SexThe incidence of extracranial atherosclerosis is higher in men; this correlation is less evident in patients with intracra-nial lesions.19,40,49 This discrepancy may be attributed to the different disease course in men and women. Men showed a high increase in intracranial lesions in the fourth and fifth decades, which steadily progressed with age, whereas women exhibited relatively mild atherosclerotic lesions until the sixth decade, with rapidly increasing lesion formation thereafter. In the eighth and ninth decades, the degree of intracranial ath-erosclerosis was comparable between sexes, whereas women showed higher atherosclerotic scores in the ninth and tenth decades.10,45 It has been speculated that the observed sex dif-ferences can be explained by a distinct risk factor profile
resulting from the influence of sex hormones such as the known hypocholesterolemic effect of estrogens.50
OthersIt has been suggested recently that the circle of Willis and its communicating arteries protect the cerebral artery and blood-brain barrier from hemodynamic stress.51 In line with this hypothesis, variations in the circle of Willis were shown to influence the volume flow rates of the bilateral ICA and BA in healthy individuals and the development of atheroscle-rosis.52,53 Racial differences in atherogenesis that have been discussed before could not be linked to anatomic variations of the circle of Willis.54 No clear genetic risk factors such as 9p21 for coronary heart disease have been identified for intracranial atherosclerosis. Notably, most studies have been conducted in Asian cohorts; data for other countries, especially European countries, are lacking.
Modifiable Risk FactorsHypertensionOne of the most important risk factors for atherosclerosis, especially intracranial lesions, is hypertension. Hypertension has been correlated to the degree of atherosclerosis in intra-cranial arteries in different ethnic cohorts.17,19,55 Some studies reported a higher incidence of hypertension in populations of African and Asian ancestry, which may explain their higher prevalence of intracranial atherosclerosis.43,46,56
Diabetes MellitusDiabetes mellitus is a specific risk factor for intracranial lesions regardless of race in symptomatic and asymptomatic cohorts.3,8,19,40,44 In Koreans, diabetes mellitus was an indepen-dent risk factor for intracranial lesions only after 50 years of age50 and only in posterior, not anterior, circulation diseases in a prospective study.17 As for hypertension, the aforementioned higher incidence of intracranial lesions in patients of African and Asian ancestry may be partly attributed to an increased prevalence of diabetes mellitus.56
Metabolic SyndromeRecent magnetic resonance angiography studies showed an independent association of the metabolic syndrome with
Table 1. Data From This Review on the Basic Characteristics of the Large Intracranial Arteries of 18 Asymptomatic Patients
BA indicates basilar artery; EEL, external elastic lamina; ICA, intracranial internal carotid artery; MCA, middle cerebral artery; and VA, intracranial vertebral artery. See Methods in the online-only Data Supplement for more information.
at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from
Ritz et al Mechanisms of Intracranial Atherosclerosis 1411
intracranial atherosclerosis.17,44 In a prospective Korean study, the metabolic syndrome was related more to intracranial than to extracranial lesions and to posterior and not anterior circu-lation strokes.17
DyslipidemiaDyslipidemia is a known risk factor for coronary atheroscle-rosis and myocardial infarction, but its role in intracranial atherosclerosis is less clear.48,57 High LDL cholesterol was associated mainly with extracranial lesions, whereas a high ratio of apolipoprotein B to apolipoprotein I and low levels of apolipoprotein AI, the major protein component of high-density lipoprotein, correlated with intracranial lesions.49,58 In China, low high-density lipoprotein cholesterol is one of the most common types of dyslipidemia and was associ-ated with the development of intracranial artery stenosis in a cohort of acute ischemic stroke.59 Sex-specific differences were reported in 2 Asian studies. Hypercholesterolemia was an independent risk factor for intracranial atherosclerosis only in asymptomatic men, whereas elderly symptomatic women >63 years of age had significantly more intracranial atherosclerotic lesions and hyperlipidemia than men.45,50 Race and environmental factors may influence the effect of dyslipidemia on atherogenesis. Generally, individuals of Asian and African ancestry exhibited lower serum lipid levels than whites, which may be one factor explaining the lower incidence of extracranial and coronary atherosclerosis in both populations.11,43
OthersExtracranial atherosclerosis was suggested as a risk factor for intracranial lesions. Extensive coronary atherosclerotic disease correlated with intracranial lesions,8,11,60 and patients with concurrent lesions had a higher risk of suffering further (fatal) vascular events.61 In a cohort of symptomatic intracra-nial atherosclerosis, 52% of cases were diagnosed with silent myocardial ischemia caused by coronary artery disease.62 The American Heart Association Stroke Council recommends test-ing for asymptomatic coronary artery disease in patients who have had ischemic events associated with intracranial athero-sclerosis.9,63 In contrast, other studies reported correlations between coronary and carotid but not intracranial lesions64 or failed to show a correlation.15,18 A few studies suggested that smoking, especially duration of smoking, is a risk factor for intracranial lesions.3,49 However, large-scale studies of the effects of smoking on intracranial atherosclerosis are scarce. As for extracranial lesions, moderate hyperhomocysteinemia was a predictor for severity of intracranial atherosclerosis in Asian patients with cerebral infarction.65 A few reports asso-ciated Alzheimer disease, sickle cell disease, systemic lupus erythematosus, radiotherapy, bacterial meningitis, and Herpes zoster infection with intracranial atherosclerosis, but their contribution needs further research.66–71
In conclusion, age, hypertension, diabetes mellitus, and probably the metabolic syndrome are the most consistent risk factors for intracranial atherosclerosis. Race may represent a predisposing factor, which is unfavorable in combination with other risk factors and especially lifestyle. Sex appears to influ-ence intracranial atherosclerosis, and its effects are age depen-dent. Genetics may predispose to intracranial atherosclerosis,
but large-scale association studies in different ethnic groups are lacking.
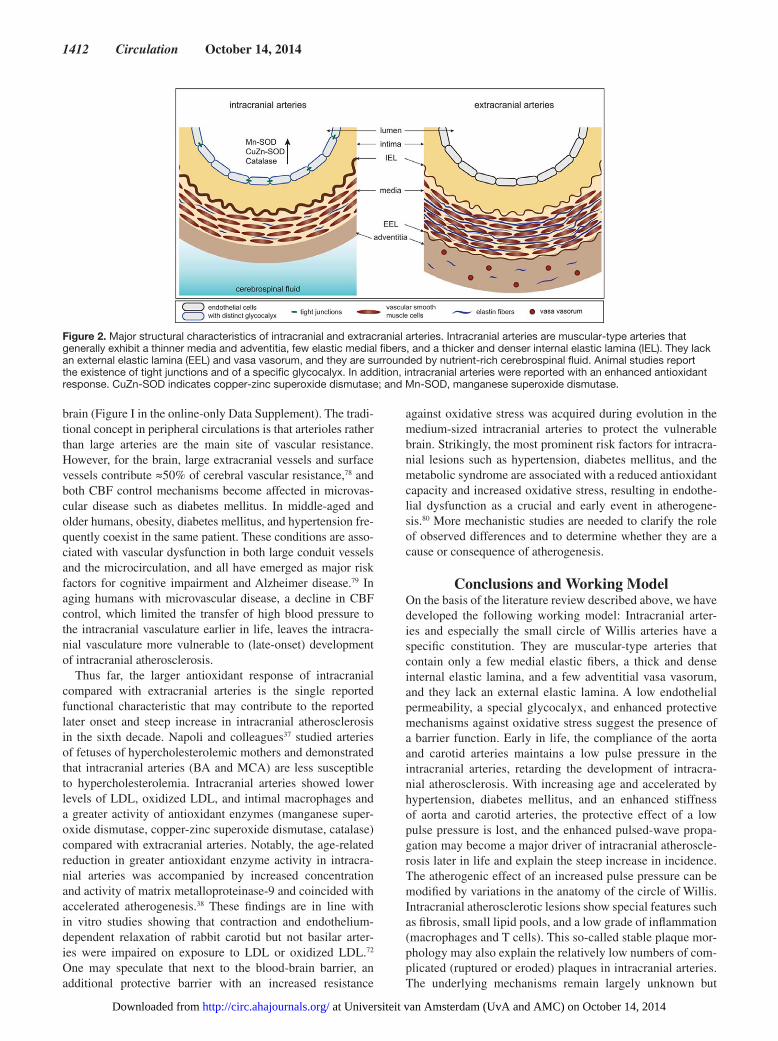
MechanismsTwo major characteristics that distinguish intracranial and extracranial atherosclerosis are the later onset and the more stable plaque phenotype in intracranial arteries, which may be explained by the distinct characteristics of the intracranial arteries (Table 2 and Figure 2). These characteristics may also be linked to the role of intracranial arteries in regulating the cerebrovascular resistance. The control mechanisms of cerebral blood flow (CBF) encompass cerebrovascular responsiveness to O
2 and CO
2, cerebral autoregulation and neurogenic control
of the cerebral vasculature, endothelium-mediated signaling, and neurovascular coupling meeting local cerebral metabolic demand.75 Cerebral artery endothelial cells and pericytes pro-duce nitric oxide in direct proportion to the arterial CO
2 partial
pressure76 and contribute to the resting tone of cerebral arteries and arterioles.77 Impairment of cerebral autoregulation results in pressure-passive CBF; that is, CBF increases and decreases together with cerebral perfusion pressure, whereas reduced CO
2 responsiveness affects the vasodilatory reserve of the
Table 2. Major Characteristics of Intracranial Arteries and Intracranial Atherosclerosis
Structural and functional characteristics of normal intracranial vessels
Muscular-type arteryFew elastic medial fibers; thinner media
and adventitia13,21
Thicker, denser internal elastic lamina21
No external elastic lamina13
Vasa vasorum only in large intracranial arteries, mainly in ICA and VA31
Arteries surrounded by CSFDistinct glycocalyx composition on luminal endothelial cells*28 and distinct chemical composition suggestive of distinct vessel
wall metabolism25
Fewer number of vesicles and caveolae*26,27
Presence of tight junctions*26,27
Reduced endothelial permeability*26,27
Relative insensitivity to sympathomimetic and histamine stimulations compared
with systemic vessels*23,29
Enhanced protective mechanisms against oxidative stress37,38,72
Flow characteristics determined by circle of Willis anatomy52,53
Characteristics of intracranial atherosclerotic plaques
Atherogenesis starts ≈20 y later compared with extracranial arterial beds13
Reduplication and splitting of internal elastic lamina most prominent from fifth decade and
not in fetuses or infants, in contrast to the aorta or coronary arteries20
Mainly fibrous plaques and fatty streaks; rarely complicated lesions, rupture, or calcification13,73
Less inflammation27
Risk factors Age3,8,10,12,19,40,44
Hypertension19,40,49,74
Diabetes mellitus3,8,19,40,44
CSF indicates cerebrospinal fluid; ICA, internal carotid artery; and VA, vertebral artery.
*Evidence from animal studies only.
at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from
brain (Figure I in the online-only Data Supplement). The tradi-tional concept in peripheral circulations is that arterioles rather than large arteries are the main site of vascular resistance. However, for the brain, large extracranial vessels and surface vessels contribute ≈50% of cerebral vascular resistance,78 and both CBF control mechanisms become affected in microvas-cular disease such as diabetes mellitus. In middle-aged and older humans, obesity, diabetes mellitus, and hypertension fre-quently coexist in the same patient. These conditions are asso-ciated with vascular dysfunction in both large conduit vessels and the microcirculation, and all have emerged as major risk factors for cognitive impairment and Alzheimer disease.79 In aging humans with microvascular disease, a decline in CBF control, which limited the transfer of high blood pressure to the intracranial vasculature earlier in life, leaves the intracra-nial vasculature more vulnerable to (late-onset) development of intracranial atherosclerosis.
Thus far, the larger antioxidant response of intracranial compared with extracranial arteries is the single reported functional characteristic that may contribute to the reported later onset and steep increase in intracranial atherosclerosis in the sixth decade. Napoli and colleagues37 studied arteries of fetuses of hypercholesterolemic mothers and demonstrated that intracranial arteries (BA and MCA) are less susceptible to hypercholesterolemia. Intracranial arteries showed lower levels of LDL, oxidized LDL, and intimal macrophages and a greater activity of antioxidant enzymes (manganese super-oxide dismutase, copper-zinc superoxide dismutase, catalase) compared with extracranial arteries. Notably, the age-related reduction in greater antioxidant enzyme activity in intracra-nial arteries was accompanied by increased concentration and activity of matrix metalloproteinase-9 and coincided with accelerated atherogenesis.38 These findings are in line with in vitro studies showing that contraction and endothelium-dependent relaxation of rabbit carotid but not basilar arter-ies were impaired on exposure to LDL or oxidized LDL.72 One may speculate that next to the blood-brain barrier, an additional protective barrier with an increased resistance
against oxidative stress was acquired during evolution in the medium-sized intracranial arteries to protect the vulnerable brain. Strikingly, the most prominent risk factors for intracra-nial lesions such as hypertension, diabetes mellitus, and the metabolic syndrome are associated with a reduced antioxidant capacity and increased oxidative stress, resulting in endothe-lial dysfunction as a crucial and early event in atherogene-sis.80 More mechanistic studies are needed to clarify the role of observed differences and to determine whether they are a cause or consequence of atherogenesis.
Conclusions and Working ModelOn the basis of the literature review described above, we have developed the following working model: Intracranial arter-ies and especially the small circle of Willis arteries have a specific constitution. They are muscular-type arteries that contain only a few medial elastic fibers, a thick and dense internal elastic lamina, and a few adventitial vasa vasorum, and they lack an external elastic lamina. A low endothelial permeability, a special glycocalyx, and enhanced protective mechanisms against oxidative stress suggest the presence of a barrier function. Early in life, the compliance of the aorta and carotid arteries maintains a low pulse pressure in the intracranial arteries, retarding the development of intracra-nial atherosclerosis. With increasing age and accelerated by hypertension, diabetes mellitus, and an enhanced stiffness of aorta and carotid arteries, the protective effect of a low pulse pressure is lost, and the enhanced pulsed-wave propa-gation may become a major driver of intracranial atheroscle-rosis later in life and explain the steep increase in incidence. The atherogenic effect of an increased pulse pressure can be modified by variations in the anatomy of the circle of Willis. Intracranial atherosclerotic lesions show special features such as fibrosis, small lipid pools, and a low grade of inflammation (macrophages and T cells). This so-called stable plaque mor-phology may also explain the relatively low numbers of com-plicated (ruptured or eroded) plaques in intracranial arteries. The underlying mechanisms remain largely unknown but
Figure 2. Major structural characteristics of intracranial and extracranial arteries. Intracranial arteries are muscular-type arteries that generally exhibit a thinner media and adventitia, few elastic medial fibers, and a thicker and denser internal elastic lamina (IEL). They lack an external elastic lamina (EEL) and vasa vasorum, and they are surrounded by nutrient-rich cerebrospinal fluid. Animal studies report the existence of tight junctions and of a specific glycocalyx. In addition, intracranial arteries were reported with an enhanced antioxidant response. CuZn-SOD indicates copper-zinc superoxide dismutase; and Mn-SOD, manganese superoxide dismutase.
at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from
Ritz et al Mechanisms of Intracranial Atherosclerosis 1413
may be related to the above-mentioned special constitution and characteristics of the intracranial arteries such as the scarceness of vasa vasorum, a high antioxidant capacity, low inflammasome activation and response, and protective effects of the cerebrospinal fluid.
Sources of Funding Dr van Lieshout reports receiving funding from Edwards Lifesciences and from the Danish Cardiovascular Research Academy.
Disclosures None.
References 1. Gorelick PB, Wong KS, Bae HJ, Pandey DK. Large artery intracranial
occlusive disease: a large worldwide burden but a relatively neglected frontier. Stroke. 2008;39:2396–2399.
2. Yarchoan M, Xie SX, Kling MA, Toledo JB, Wolk DA, Lee EB, Van Deerlin V, Lee VM, Trojanowski JQ, Arnold SE. Cerebrovascular ath-erosclerosis correlates with Alzheimer pathology in neurodegenerative dementias. Brain. 2012;135(pt 12):3749–3756.
3. Bos D, van der Rijk MJ, Geeraedts TE, Hofman A, Krestin GP, Witteman JC, van der Lugt A, Ikram MA, Vernooij MW. Intracranial carotid artery atherosclerosis: prevalence and risk factors in the general population. Stroke. 2012;43:1878–1884.
4. Hart RG, Diener HC, Coutts SB, Easton JD, Granger CB, O’Donnell MJ, Sacco RL, Connolly SJ; Cryptogenic Stroke/ESUS International Working Group. Embolic strokes of undetermined source: the case for a new clini-cal construct. Lancet Neurol. 2014;13:429–438.
5. Bodle JD, Feldmann E, Swartz RH, Rumboldt Z, Brown T, Turan TN. High-resolution magnetic resonance imaging: an emerging tool for evalu-ating intracranial arterial disease. Stroke. 2013;44:287–292.
6. Liberman AL, Prabhakaran S. Cryptogenic stroke: how to define it? How to treat it? Curr Cardiol Rep. 2013;15:423.
7. Bang OY, Ovbiagele B, Kim JS. Evaluation of cryptogenic stroke with advanced diagnostic techniques. Stroke. 2014;45:1186–1194.
8. Mazighi M, Labreuche J, Gongora-Rivera F, Duyckaerts C, Hauw JJ, Amarenco P. Autopsy prevalence of intracranial atherosclerosis in patients with fatal stroke. Stroke. 2008;39:1142–1147.
10. Resch JA, Baker AB. Etiology mechanisms in cerebral atherosclerosis. Archives of Neurology. 1964;10:617–628.
11. Leung SY, Ng TH, Yuen ST, Lauder IJ, Ho FC. Pattern of cerebral athero-sclerosis in Hong Kong Chinese: severity in intracranial and extracranial vessels. Stroke. 1993;24:779–786.
12. Mathur KS, Kashyap SK, Mathur SC. Distribution and severity of athero-sclerosis of aorta, coronary and cerebral arteries in persons dying with-out morphologic evidence of atherosclerotic catastrophe in North India: a study of 900 autopsies. J Assoc Physicians India. 1968;16:113–122.
13. Moossy J. Morphology, sites and epidemiology of cerebral atherosclero-sis. Res Publ Assoc Res Nerv Ment Dis. 1966;41:1–22.
14. Akins PT, Pilgram TK, Cross DT 3rd, Moran CJ. Natural history of stenosis from intracranial atherosclerosis by serial angiography. Stroke. 1998;29:433–438.
15. Uehara T, Tabuchi M, Mori E, Yamadori A. Evolving atherosclerosis at carotid and intracranial arteries in Japanese patients with ischemic heart disease: a 5-year longitudinal study with MR angiography. Eur J Neurol. 2003;10:507–512.
16. Arenillas JF, Molina CA, Montaner J, Abilleira S, González-Sánchez MA, Alvarez-Sabín J. Progression and clinical recurrence of symptomatic mid-dle cerebral artery stenosis: a long-term follow-up transcranial Doppler ultrasound study. Stroke. 2001;32:2898–2904.
17. Kim JS, Nah HW, Park SM, Kim SK, Cho KH, Lee J, Lee YS, Kim J, Ha SW, Kim EG, Kim DE, Kang DW, Kwon SU, Yu KH, Lee BC. Risk factors and stroke mechanisms in atherosclerotic stroke: intracranial com-pared with extracranial and anterior compared with posterior circulation disease. Stroke. 2012;43:3313–3318.
18. Alkan O, Kizilkilic O, Yildirim T, Atalay H. Intracranial cerebral artery stenosis with associated coronary artery and extracranial carotid artery stenosis in Turkish patients. Eur J Radiol. 2009;71:450–455.
19. Bae HJ, Lee J, Park JM, Kwon O, Koo JS, Kim BK, Pandey DK. Risk factors of intracranial cerebral atherosclerosis among asymptomatics. Cerebrovasc Dis. 2007;24:355–360.
20. Baker AB, Iannone A. Cerebrovascular disease, I: the large arteries of the circle of Willis. Neurology. 1959;9:321–332.
21. Velican C. Studies on the age-related changes occurring in human cerebral arteries. Atherosclerosis. 1970;11:509–529.
22. Hori E, Hayashi N, Hamada H, Masuoka T, Kuwayama N, Hirashima Y, Origasa H, Ohtani O, Endo S. A development of atheromatous plaque is restricted by characteristic arterial wall structure at the carotid bifurcation. Surg Neurol. 2008;69:586–90; discussion 590.
23. Bevan JA. Sites of transition between functional systemic and cere-bral arteries of rabbits occur at embryological junctional sites. Science. 1979;204:635–637.
24. Masuoka T, Hayashi N, Hori E, Kuwayama N, Ohtani O, Endo S. Distribution of internal elastic lamina and external elastic lamina in the internal carotid artery: possible relationship with atherosclerosis. Neurol Med Chir (Tokyo). 2010;50:179–182.
25. Nakamura M, Imaizumi K, Shigemi U, Nakashima Y, Kikuchi Y. Cerebral atherosclerosis in Japanese, part 5: relationship between cholesterol depo-sition and glycosaminoglycans. Stroke. 1976;7:594–598.
26. Kurozumi T. Electron microscopic study on permeability of the aorta and basilar artery of the rabbit–with special reference to the changes of perme-ability by hypercholesteremia. Exp Mol Pathol. 1975;23:1–11.
27. Kurozumi T, Imamura T, Tanaka K, Yae Y, Koga S. Permeation and depo-sition of fibrinogen and low-density lipoprotein in the aorta and cerebral artery of rabbits: immuno-electron microscopic study. Br J Exp Pathol. 1984;65:355–364.
28. Weber G. Delayed experimental atherosclerotic involvement of cerebral arteries in monkeys and rabbits (light, Sem and Tem observations). Pathol Res Pract. 1985;180:353–355.
29. Edvinsson L, Owman C. A pharmacologic comparison of histamine recep-tors in isolated extracranial and intracranial arteries in vitro. Neurology. 1975;25:271–276.
30. Zervas NT, Liszczak TM, Mayberg MR, Black PM. Cerebrospinal fluid may nourish cerebral vessels through pathways in the adventitia that may be analogous to systemic vasa vasorum. J Neurosurg. 1982;56:475–481.
31. Portanova A, Hakakian N, Mikulis DJ, Virmani R, Abdalla WM, Wasserman BA. Intracranial vasa vasorum: insights and implications for imaging. Radiology. 2013;267:667–679.
32. Aydin F. Do human intracranial arteries lack vasa vasorum? A compara-tive immunohistochemical study of intracranial and systemic arteries. Acta Neuropathol. 1998;96:22–28.
33. Takaba M, Endo S, Kurimoto M, Kuwayama N, Nishijima M, Takaku A. Vasa vasorum of the intracranial arteries. Acta Neurochir (Wien). 1998;140:411–416.
34. Zugibe FT, Brown KD. Histochemical studies in atherogenesis: human cerebral arteries. Circ Res. 1961;9:897–905.
35. Hoff HF. A histoenzymatic study of human intracranial atherosclerosis. Am J Pathol. 1972;67:583–600.
36. Hoff HF. Apolipoprotein localization in human cranial arteries, coronary arteries, and the aorta. Stroke. 1976;7:390–393.
37. Napoli C, Witztum JL, de Nigris F, Palumbo G, D’Armiento FP, Palinski W. Intracranial arteries of human fetuses are more resistant to hypercho-lesterolemia-induced fatty streak formation than extracranial arteries. Circulation. 1999;99:2003–2010.
38. D’Armiento FP, Bianchi A, de Nigris F, Capuzzi DM, D’Armiento MR, Crimi G, Abete P, Palinski W, Condorelli M, Napoli C. Age-related effects on athero-genesis and scavenger enzymes of intracranial and extracranial arteries in men without classic risk factors for atherosclerosis. Stroke. 2001;32:2472–2479.
39. Narula J, Nakano M, Virmani R, Kolodgie FD, Petersen R, Newcomb R, Malik S, Fuster V, Finn AV. Histopathologic characteristics of atherosclerotic coronary disease and implications of the findings for the invasive and noninva-sive detection of vulnerable plaques. J Am Coll Cardiol. 2013;61:1041–1051.
40. López-Cancio E, Dorado L, Millán M, Reverté S, Suñol A, Massuet A, Galán A, Alzamora MT, Pera G, Torán P, Dávalos A, Arenillas JF. The Barcelona-Asymptomatic Intracranial Atherosclerosis (AsIA) study: prev-alence and risk factors. Atherosclerosis. 2012;221:221–225.
41. Williams AO, Resch JA, Loewenson RB. Cerebral atherosclerosis: a com-parative autopsy study between Nigerian Negroes and American Negroes and Caucasians. Neurology. 1969;19:205–210.
42. Resch JA, Okabe N, Loewenson RB, Kimoto K, Katsuki S, Baker AB. Pattern of vessel involvement in cerebral atherosclerosis: a comparative study between a Japanese and Minnesota population. J Atheroscler Res. 1969;9:239–250.
at Universiteit van Amsterdam (UvA and AMC) on October 14, 2014http://circ.ahajournals.org/Downloaded from
43. Inzitari D, Hachinski VC, Taylor DW, Barnett HJ. Racial differences in the anterior circulation in cerebrovascular disease: how much can be explained by risk factors? Arch Neurol. 1990;47:1080–1084.
44. Rincon F, Sacco RL, Kranwinkel G, Xu Q, Paik MC, Boden-Albala B, Elkind MS. Incidence and risk factors of intracranial atherosclerotic stroke: the Northern Manhattan Stroke Study. Cerebrovasc Dis. 2009;28:65–71.
45. Pu Y, Liu L, Wang Y, Zou X, Pan Y, Soo Y, Leung T, Zhao X, Wong KS, Wang Y; Chinese IntraCranial AtheroSclerosis (CICAS) Study Group. Geographic and sex difference in the distribution of intracranial athero-sclerosis in China. Stroke. 2013;44:2109–2114.
46. Solberg LA, McGarry PA. Cerebral atherosclerosis in Negroes and Caucasians. Atherosclerosis. 1972;16:141–154.
48. Sacco RL, Kargman DE, Gu Q, Zamanillo MC. Race-ethnicity and deter-minants of intracranial atherosclerotic cerebral infarction: the Northern Manhattan Stroke Study. Stroke. 1995;26:14–20.
49. Ingall TJ, Homer D, Baker HL Jr, Kottke BA, O’Fallon WM, Whisnant JP. Predictors of intracranial carotid artery atherosclerosis: duration of ciga-rette smoking and hypertension are more powerful than serum lipid levels. Arch Neurol. 1991;48:687–691.
50. Kim YS, Hong JW, Jung WS, Park SU, Park JM, Cho SI, Bu YM, Moon SK. Gender differences in risk factors for intracranial cerebral atheroscle-rosis among asymptomatic subjects. Gend Med. 2011;8:14–22.
51. Vrselja Z, Brkic H, Mrdenovic S, Radic R, Curic G. Function of circle of Willis. J Cereb Blood Flow Metab. 2014;34:578–584.
52. Routsonis KG, Stamboulis E, Christodoulaki M. Anomalies of the circle of Willis and atherosclerosis. Vasc Surg. 1973;7:141–145.
53. Hartkamp MJ, van Der Grond J, van Everdingen KJ, Hillen B, Mali WP. Circle of Willis collateral flow investigated by magnetic resonance angi-ography. Stroke. 1999;30:2671–2678.
54. Eftekhar B, Dadmehr M, Ansari S, Ghodsi M, Nazparvar B, Ketabchi E. Are the distributions of variations of circle of Willis different in different populations? Results of an anatomical study and review of literature. BMC Neurol. 2006;6:22.
55. López-Cancio E, Galán A, Dorado L, Jiménez M, Hernández M, Millán M, Reverté S, Suñol A, Barallat J, Massuet A, Alzamora MT, Dávalos A, Arenillas JF. Biological signatures of asymptomatic extra- and intra-cranial atherosclerosis: the Barcelona-AsIA (Asymptomatic Intracranial Atherosclerosis) study. Stroke. 2012;43:2712–2719.
56. Gorelick PB, Caplan LR, Hier DB, Patel D, Langenberg P, Pessin MS, Biller J, Kornack D. Racial differences in the distribution of posterior cir-culation occlusive disease. Stroke. 1985;16:785–790.
57. Sato S, Uehara T, Hayakawa M, Nagatsuka K, Minematsu K, Toyoda K. Intra- and extracranial atherosclerotic disease in acute spontaneous intra-cerebral hemorrhage. J Neurol Sci. 2013;332:116–120.
58. Park JH, Hong KS, Lee EJ, Lee J, Kim DE. High levels of apolipoprotein B/AI ratio are associated with intracranial atherosclerotic stenosis. Stroke. 2011;42:3040–3046.
59. Qian Y, Pu Y, Liu L, Wang DZ, Zhao X, Wang C, Wang Y, Liu G, Pan Y, Wang Y. Low HDL-C level is associated with the development of intracranial artery stenosis: analysis from the Chinese IntraCranial AtheroSclerosis (CICAS) study. PLoS One. 2013;8:e64395.
60. Uekita K, Hasebe N, Funayama N, Aoyama H, Kuroda K, Aizawa H, Kataoka R, Kikuchi K. Cervical and intracranial atherosclerosis and silent brain infarction in Japanese patients with coronary artery disease. Cerebrovasc Dis. 2003;16:61–68.
61. Wong KS, Li H. Long-term mortality and recurrent stroke risk among Chinese stroke patients with predominant intracranial atherosclerosis. Stroke. 2003;34:2361–2366.
J. Silent myocardial ischemia in patients with symptomatic intracranial atherosclerosis: associated factors. Stroke. 2005;36:1201–1206.
63. Adams RJ, Chimowitz MI, Alpert JS, Awad IA, Cerqueria MD, Fayad P, Taubert KA. Coronary risk evaluation in patients with transient ischemic attack and ischemic stroke: a scientific statement for healthcare profession-als from the Stroke Council and the Council on Clinical Cardiology of the American Heart Association/American Stroke Association. Circulation. 2003;108:1278–1290.
64. Seo WK, Yong HS, Koh SB, Suh SI, Kim JH, Yu SW, Lee JY. Correlation of coronary artery atherosclerosis with atherosclerosis of the intra-cranial cerebral artery and the extracranial carotid artery. Eur Neurol. 2008;59:292–298.
65. Yoo JH, Chung CS, Kang SS. Relation of plasma homocyst(e)ine to cere-bral infarction and cerebral atherosclerosis. Stroke. 1998;29:2478–2483.
66. Werner MH, Burger PC, Heinz ER, Friedman AH, Halperin EC, Schold SC Jr. Intracranial atherosclerosis following radiotherapy. Neurology. 1988;38:1158–1160.
67. Pfister HW, Feiden W, Einhäupl KM. Spectrum of complications during bacterial meningitis in adults: results of a prospective clinical study. Arch Neurol. 1993;50:575–581.
68. Ueno M, Oka A, Koeda T, Okamoto R, Takeshita K. Unilateral occlusion of the middle cerebral artery after varicella-zoster virus infection. Brain Dev. 2002;24:106–108.
69. Palacio S, Hart RG, Vollmer DG, Kagan-Hallet K. Late-developing cere-bral arteropathy after pyogenic meningitis. Arch Neurol. 2003;60:431–433.
70. Suri MF, Johnston SC. Epidemiology of intracranial stenosis. J Neuroimaging. 2009;19(suppl 1):11S–16S.
71. Urowitz MB, Gladman D, Ibañez D, Bae SC, Sanchez-Guerrero J, Gordon C, Clarke A, Bernatsky S, Fortin PR, Hanly JG, Wallace DJ, Isenberg D, Rahman A, Alarcón GS, Merrill JT, Ginzler E, Khamashta M, Nived O, Sturfelt G, Bruce IN, Steinsson K, Manzi S, Ramsey-Goldman R, Dooley MA, Zoma A, Kalunian K, Ramos M, Van Vollenhoven RF, Aranow C, Stoll T, Petri M, Maddison P; Systemic Lupus International Collaborating Clinics. Atherosclerotic vascular events in a multinational inception cohort of systemic lupus erythematosus. Arthritis Care Res (Hoboken). 2010;62:881–887.
72. Napoli C, Paternò R, Faraci FM, Taguchi H, Postiglione A, Heistad DD. Mildly oxidized low-density lipoprotein impairs responses of carotid but not basilar artery in rabbits. Stroke. 1997;28:2266–2271.
73. Cornish BR, Paterson JC. Calcium concentrations in sclerotic cerebral arteries. AMA Arch Pathol. 1956;62:177–182.
74. Kim YD, Choi HY, Jung YH, Nam CM, Yang JH, Cho HJ, Nam HS, Lee KY, Heo JH. Classic risk factors for atherosclerosis are not major determi-nants for location of extracranial or intracranial cerebral atherosclerosis. Neuroepidemiology. 2009;32:201–207.
75. Filosa JA, Iddings JA. Astrocyte regulation of cerebral vascular tone. Am J Physiol Heart Circ Physiol. 2013;305:H609–H619.
76. Fathi AR, Yang C, Bakhtian KD, Qi M, Lonser RR, Pluta RM. Carbon dioxide influence on nitric oxide production in endothelial cells and astro-cytes: cellular mechanisms. Brain Res. 2011;1386:50–57.
77. Andresen J, Shafi NI, Bryan RM Jr. Endothelial influences on cerebrovas-cular tone. J Appl Physiol (1985). 2006;100:318–327.
78. Faraci FM, Heistad DD. Regulation of large cerebral arteries and cerebral microvascular pressure. Circ Res. 1990;66:8–17.
79. Barnes JN, Joyner MJ. Cerebrovascular challenges in diabetic patients: the pressure is on to maintain perfusion. Hypertension. 2011;57:674–675.
80. Cai H, Harrison DG. Endothelial dysfunction in cardiovascular diseases: the role of oxidant stress. Circ Res. 2000;87:840–844.