69
Role of immunohistochemistry and molecular diagnostics in soft tissue tumors Wasan Yotchai, MD Siriraj Hospital

Role of immunohistochemistry and molecular diagnostics in soft tissue tumors
Wasan Yotchai, MD
Siriraj Hospital

REFERENCE
The limited sample: doing more with less
Limited biopsies of soft tissue tumors:
The contemporary role of immunohistochemistry and molecular diagnosis
Jason L. Hornick MD. Ph.D.

• Diagnosing Soft Tissue Tumors is challenging
• Soft tissue sarcomas are rare, but diverse
• > 40 distinct types of sarcomas and >80 types of benign and intermediate
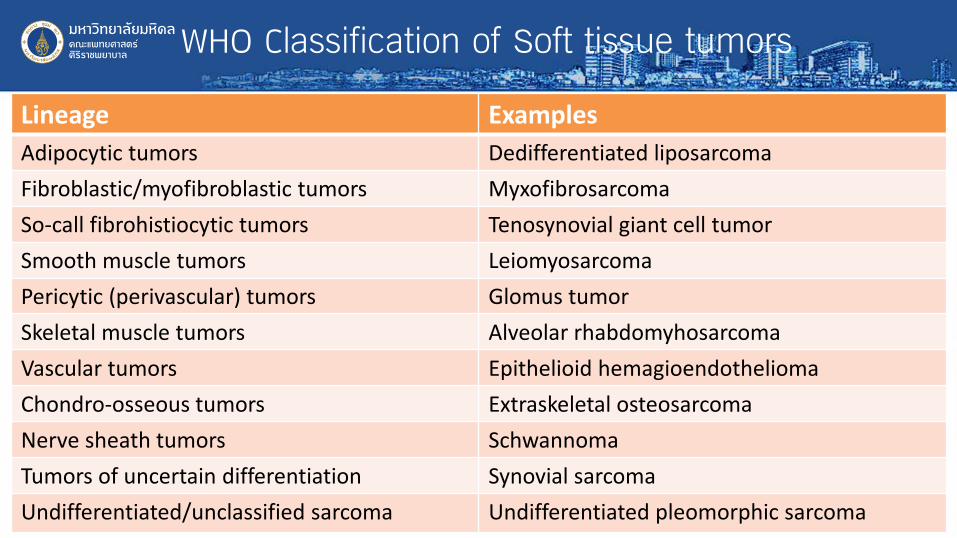
WHO Classification of Soft tissue tumors
Lineage Examples Adipocytic tumors Dedifferentiated liposarcoma Fibroblastic/myofibroblastic tumors Myxofibrosarcoma So-call fibrohistiocytic tumors Tenosynovial giant cell tumor Smooth muscle tumors Leiomyosarcoma Pericytic (perivascular) tumors Glomus tumor Skeletal muscle tumors Alveolar rhabdomyhosarcoma Vascular tumors Epithelioid hemagioendothelioma Chondro-osseous tumors Extraskeletal osteosarcoma Nerve sheath tumors Schwannoma Tumors of uncertain differentiation Synovial sarcoma Undifferentiated/unclassified sarcoma Undifferentiated pleomorphic sarcoma

Problems with applying WHO Classification in clinical practice
• Base on line of differentiation
• Differentiation not always obvious
• Some tumor types are of uncertain lineage
• Tumors of diverse lineages can show similar histologic appearance
• Benign, intermediate, and malignant soft tissue tumors can be difficult to distinguish

Limited biopsies of soft tissue tumors: What do our colleaues need to know?
Question Potential Reasons Benign VS malignant? Surgical planning (marginal VS wide excision)
Neoadjuvant radiation therapy (radiation or chemotherapy)
Histologic grade? Neoadjuvant radiation therapy Specific diagnosis Surgical planning, extent of margins: e.g.,
myxofibrosarcoma, epithelioid sarcoma) Some sarcomas require specific chemotherapy protocols (e.g., Ewing sarcoma, rhabdomyosarcoma, synovial sarcoma

Grading of soft tissue sarcoma-FNCLCC

Differentiation score for selected sarcoma types

Sarcomas for grading is of no (or limited) value
Tumor type Alveolar soft part sarcoma Clear cell sarcoma Epithelioid sarcoma Extraskeletal myxoid chondrosarcoma Low-grade fibromyxoid sarcoma Sclerosing epithelioid fibrosarcoma

Sarcomas that are high grade by definition
Tumor type Alveolar rhabdomyosarcoma Angiosarcoma BCOR-CCNB3 sarcoma CIC-DUX4 sarcoma Embryonal rhabdomyosarcoma Ewing sarcoma Malignant rhabdoid tumor

Conventional Immunohistochemistry
Line of differentiation IHC markers Myofibroblastic SMA Smooth muscle SMA, Desmin Skeletal muscle MSA, Desmin Vascular CD31, CD34 Nerve sheath (Schwann cell) S100 Cartilage S100

Lineage-Restricted Transcription Factors
Line of differentiation Skeletal muscle Myogenin, MYOD1 Endothelium FLI1, ERG Neuroectoderm SOX10 Notochord Brachyury Osteoblast SATB2
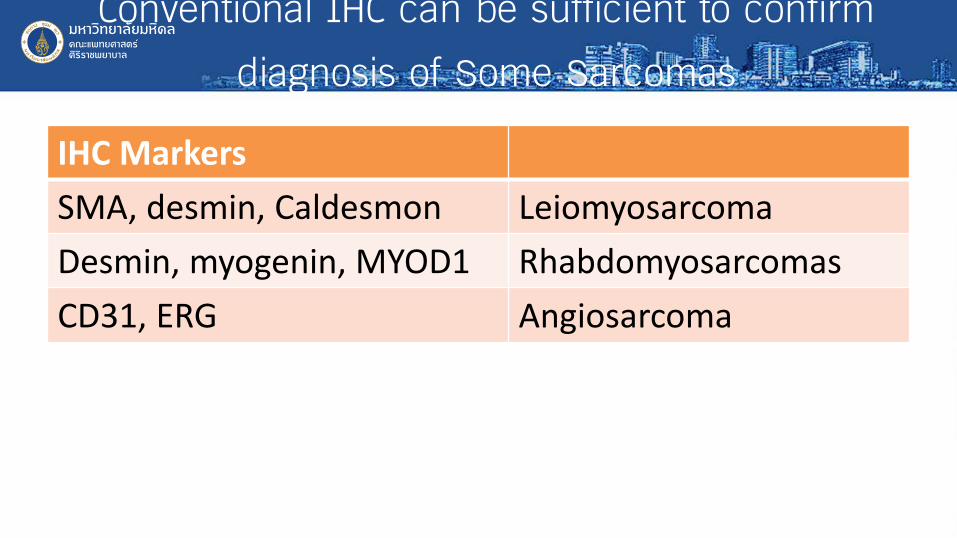
Conventional IHC can be sufficient to confirm diagnosis of Some Sarcomas
IHC Markers SMA, desmin, Caldesmon Leiomyosarcoma Desmin, myogenin, MYOD1 Rhabdomyosarcomas CD31, ERG Angiosarcoma

Limited biopsy of Soft Tissue Tumors: The Good News
• Many new much more specific IHC markers have been developed based on molecular findings
• Moleculars diagnostic techniques work wonderfuly on core biopsies, cell blocks, and smears/touch preps
– FISH, RT-PCR, NGS, new fusion assays

21st century IHC markers for Soft Tissue Tumors
ALK FOSB RB1 β-catenin H3K27me3 ROS1 BCOR MDM2 SDHB CAMTA1 MUC4 SMARCA4 CCNB3 MYC SMARCB1 CDK4 NKX2-2 TFE3 DOG1 PAX3 TLE1 ETV4 PDGFRA TRK

BREAK-APART FISH FOR EWSR1
EWSR1 22q12 5’ (c) 3’ (t)

Bad news in limited biopsy specimen
• Requires appropriate and limited differential diagnosis
– We can’t order 20 stains on every cases
• Molecular genetic alterations are often shared by diverse tumor types – most have limited specificity

Pattern-based approach to diagnosis

Spindle cell tumor of soft tissue
Tumor type Markers Desmoid-type fibromatosis β-catenin Solitary fibrous tumor STAT6 Malignant peripheral nerve sheath tumor
H3K27me3
Low-grade fibromyxoid sarcoma MUC4 Monophasic synovial sarcoma TLE1

Solitary Fibrous Tumor
• Anatomically ubiquitour fibroblastic neoplasm (pleura, retroperitoneum, abdomen, head & neck)
• Patternless architecture, varying cellularity, prominent stromal collagen, dilated branching (staghorn) vessels
• Hemangiopericytoma synonymous with SFT (uniform hypercellularity)
• CD34 positive in 95% of cases, but not specific (many other tumor types positive)

Malignant SFT


CD34-positive Spindle cell tumors
Tumor type Solitary fibrous tumor Dermatofibrosarcoma protuberans Spindle/pleomorphic lipoma Kaposi sarcoma Soft tissue perineurioma
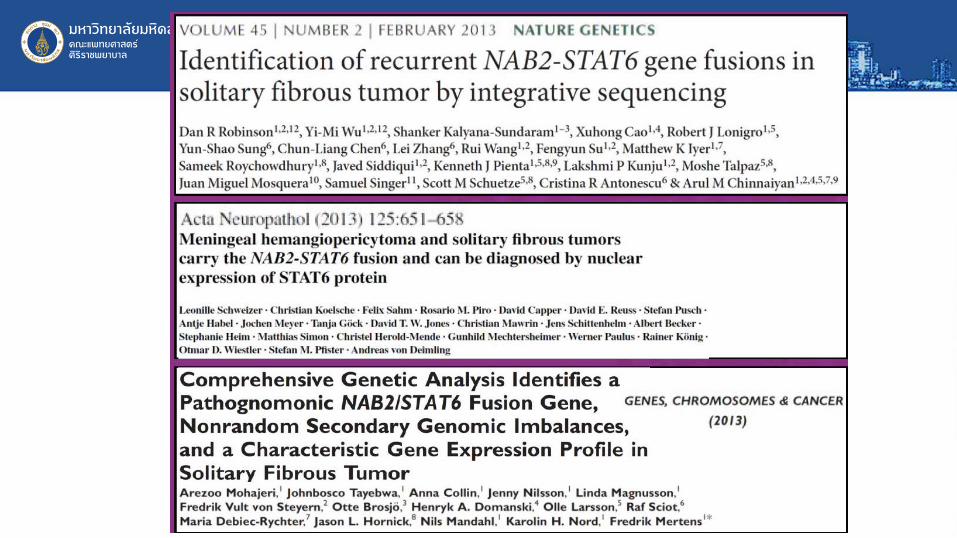

Solitary fibrous tumor and STAT6
• NAB3-STAT6 consistent fusion gene
• Both genes on chromosome 12q13 in close proximity (overlapping)
• Conventional FISH cannot be used
• Nuclear STAT6 expression highly specific for SFT

Doyle et all. Mod Pathol 2014


Malignant peripheral nerve sheath tumor
• Arise in patients with NF1, sporadically, or following radiation therapy • Challenging diagnosis • Diagnostic criteria:
– Origin from a nerve or a neurofibroma – Spindle cell sarcoma in a patient with NF1 – Evidence of Schwann cell differentiation by IHC or EM
• S100 protein and SOX10 only 30-50% sensitivity
• Diagnosis in sporadic setting relies on distinctive histology and exclusion of mimics

H3K27me3
• Epigenetic modification of chromatin:
• PRC2 recruits to chromatin and trimethylates histone H3 at lysine 27
• Physiologic regulation of cell fate and proper stem cell differentiation
• Deregulation -> cancer development

PRC2 and MPNST
• PRC2 alterations (SUZ12 or EED mutations) in 85-90% of MPNST
• Homozygous mutations result in loss of H3K27me3 (histone H3 lysine 27 trimethylation) in 65% of MPNST
• Rate of H3K27me3 loss depends on grade
• IHC for H3K27me3 highly specific diagnostic marker

IHC for H3K27me3 in MPNST
MPNST grade Low grade 35% Intermediate grade 65% High grade 85%

H3K27me3 in other spindle cell neoplasms Tumor type H3K27me3 loss
Cellular schwannoma 0%
Atypical neurofibroma 0%
Monophasic synovial sarcoma 0%
Leiomyosarcoma 0%
Myxofibrosarcoma 0%
Malignant solitary fibrous tumor 0%
Low-grade fibromyxoid sarcoma 0%
Spindle cell shabdomyosarcoma 0%
Gastrointestinal stromal tumor 0%
Dedifferentiated liposarcoma 6%
Spindle cell melanoma 7%





Epithelioid tumors of soft tissue
Tumor type Markers Alveolar soft part sarcoma TFE3 Epithelioid sarcoma INI1 (SMARCB1) Epithelioid hemangioendothelioma
CAMTA1
Epithelioid MPNST INI1 (SMARCB1)

Epithelioid hemangioendothelioma
• Distinctive sarcoma showing endothelial differentiation; less aggressive than angiosarcoma
• Epithelioid cells arranged in cords and nests • Myxohyaline stroma typical • Occasional cytoplasmic vacuoles • Keratin expression common • May be confused with metastatic carcinoma, especially lobular
breast and signet-ring-cell gastric




IHC for CAMTA1
• Nuclear staining in most cases of EHE
• Negative in epithelioid hemangioma and epithelioid angiosarcoma
• Negative in nearly all carcinomas
• Negative in other epithelioid mesenchymal tumors
• Useful diagnostic marker for EHE







Pleomorphic sarcoma of soft tissue
Tumor type Metastatic rate Dedifferentiated liposarcoma 15-20% Myxofibrosarcoma (high grade) 25-30% Undifferentiated pleomorphic sarcoma 50% Pleomorphic liposarcoma 50% Extraskeletal osteosarcoma 60% Pleomorphic leiomyosarcoma 70% Pleomorphic rhabdomyosarcoma >90%

Dedifferentiated liposarcoma
• MDM2 and CDK4
• On chromosome 12q13-15; role in cell cycle regulation
• Amplified in nearly all cases of well-differentiated and dedifferentiated liposarcoma – MDM2 98%
– CDK4 92%
• Rign and giant marker chromosomes
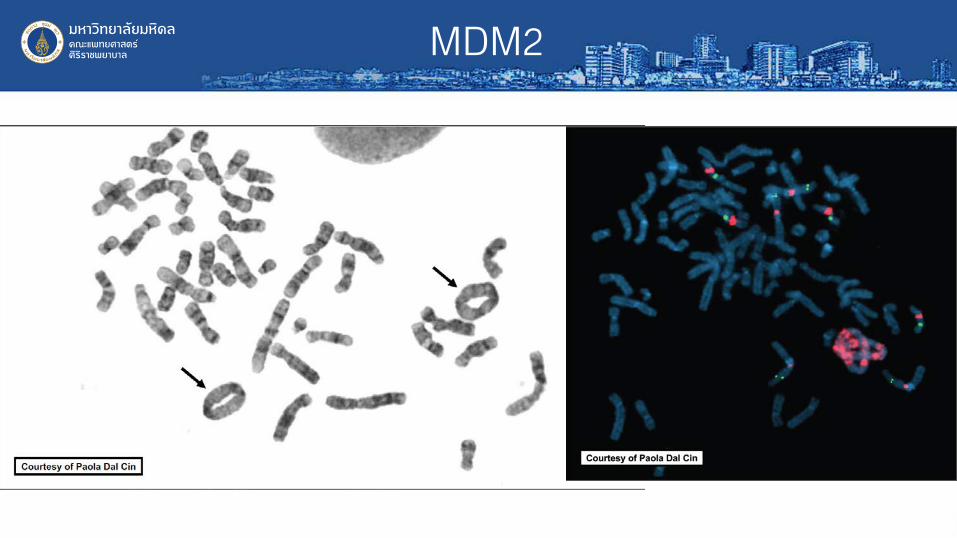
MDM2

IHC for MDM2 and CDK4
• Highly sensitive for DDLPS, but not entirely specific: – Positive in some myxofibrosarcoma and MPNSTs
– FISH more specific
• In proper context, can be very helpful in differential diagnosis: – DDLPS vs other pleomorphic/spindle cell sarcomas (especially
in small biopsies)

Tumor type MDM2 CDK4 DDLPS 98% 92% MPNST 65% 10% Myxofibrosarcoma 40% 15% Leiomyosarcoma 5% 1% GIST 0% 0%



Round cell sarcoma of soft tissue Tumor type KRT DES MYOG CD99 WT1 NKX2-2 ETV4 BCOR PHOX2B
Ewing sarcoma + - - ++ - ++ - - -
CIC-rearranged sarcoma + - - ++ ++ - ++ - -
BCOR-rearranged sarcoma - - - + - - - ++ -
Poorly differentiated synovial sarcoma
+ - - + - - - + -
Alveolar rhabdomyosarcoma + ++ ++ + + - - - -
Desmoplastic small round cell tumor
++ ++ - + ++ - - - -
neuroblastoma - - - - - - - - ++

Fusion genes in round cell sarcoma
Tumor type Gene fusions Ewing sarcoma EWSR1-FLI1, EWSR1-ERG CIC-rearranged sarcoma CIC-DUX4 BCOR-rearranged sarcoma BCOR-CCNB3 Alveolar rhabdomyosarcoma PAX3-FOXO1, PAX7-FOXO1 Desmoplastic small round cell tumor EWSR1-WT1 Poorly differentiated synovial sarcoma
SS18-SSX1, SS18-SSX2
Myxoid (round cell) liposarcoma FUS-DDIT3, EWSR1-DDIT3

CIC-rearranged sarcoma
• Most common “Ewing-like” (undifferentiated) round cell sarcoma that lacks EWSR1 gene fusions (at least 70%)
• Majority with CIC-DUX4 fusions • Wide age range; peak in young adults • Deep soft tissue of extremities and trunk most frequent • Bone and visceral sites rare • Much more aggressive clinical course and worse survival than Ewing
sarcoma; currently treated similarly



CIC-rearranged sarcoma: Genetics
• CIC-DUX4 in most cases (FISH for CIC)
• CIC-FOXO4 in rare cases
• FISH negative in 15% (cryptic rearrangement)
• ETV transcriptional upregulation more sensitive

CIC-rearranged sarcoma: IHC
Marker Positive Comments CD99 85% Usually pathcy; 20% diffuse WT1 90% Nuclear +/- cytoplasmic ETV4 95% Nuclear


Practical points
• Diagnosing soft tissue tumors in limited biopsies is particularly challenging
• Molecular pathogenetic alterations continue to be discovered, leading to new molecular diagnostic tests
• Novel IHC markders increasingly available, many serving as surrogates for molecular genetic alterations
• In some cases, a specific diagnosis is not possible

Thank you

















