66
Rounds May 2015 • This talk may be found at AndrewGeller.Weebly.com,
| Date post: | 16-Aug-2015 |
| Category: |
Education |
| Upload: | mary-jane-waite |
| View: | 17 times |
| Download: | 0 times |

Rounds May 2015
• This talk may be found at AndrewGeller.Weebly.com,
ACLS Update for Pediatrics• Sequence of Steps has changed, no longer ABC , it is
CAB even for kids and infants! • CAB For ALL AGES[Anything that delays chest compressions is to be
avoided]Step 1: check responsiveness and for breathing[Look , Listen and Feel for breathing is gone]Step 2: Call for help and an AED[Since we deliver 30 compressions in 18 seconds we are
not delaying breathing by much.]Step 3: check pulseStep 4:Give CompressionsStep 5: Open Airway , now over 2 minutes into careStep 6:Resume compressions
Compressions in Kids• Begin compressions ASAP, within 10 seconds of
recognition of the arrest• Push Hard and Fast: at least 1/3 of the AP diameter of
the chest approximately 2 inches• In infants at least 1/3 of the chest diameter, 1 and ½
inches! • Depth is approximately 2 inches in most children, the
same as adults ! Deeper compressions are necessary to generate the pressure to perfuse the cerebral and coronary arteries.
• Push fast means that each set of compressions takes 18 seconds instead of 23 seconds.
• Chest compressions are before Airway and Breathing, even in children , per the 2010 guidelines.

AED Use in Children and Infants• An AED may now be used in infants [ new ] • A manual defibrillator is preferred, an AED
with a dose attenuator is the second choice, however an AED without a dose attenuator may be used.
• 2-4 joules is suggested [new] for the initial energy dose. There is no data that fairly high energy doses are harmful.
• Subsequent shocks up to 10j/kg or the adult maximum dose may be used.

AED Use in Children and Infants• An AED may now be used in infants [ new ] • A manual defibrillator is preferred, an AED
with a dose attenuator is the second choice, however an AED without a dose attenuator may be used.
• 2-4 joules is suggested [new] for the initial energy dose. There is no data that fairly high energy doses are harmful.
• Subsequent shocks up to 10j/kg or the adult maximum dose may be used.

Breathing Recomendations• Capnography is suggested for all arrests• The Sellick maneuver [cricoid pressure] is
optional and NOT mandatory.• Each breath should take 1 second. • After a rescue airway is placed 8-10 breaths per
minute [1 breath every 6-8 seconds]• Cuffed endotracheal tubes are ok• Avoid excessive ventilations , minimize
interruptions in compressions, allow complete chest recoil!

Drugs • Atropine is out of the cardiac arrest PEA and Asystole
protocols . [It may be used for bradycardia with a BP.]• Adenosine is suggested for Wide Complex REGULAR
Monomorphic Tachycardia[ Only one wave type, fast and wide]. It should not be used if the tachycardia is irregular!
• Calcium is NOT to be given except in specific circumstances [calcium channel overdose , hypocalcemia , hyperkalemia, hypermagnesemia ]
• Lidocaine is NOT recommended for routine use with VF/VT
• Chronotropic infusions can be used as an alternative to pacing with symptomatic bradycardia.

Post Resuscitation
• Turn down the O2. Hyperoxia is harmful with oxidative injury likelyO2 saturation should be < 100 % , as with adults.
• Use capnometry• Use hypothermia if the patient is resuscitated
and remains comatose.

Drowning Epidemiology
• Between 4,00-7,000 cases per year, and 3,000- 6,000 deaths per year in the US.
• Second most common cause of unintentional death for ages 1-4, and 15-19.
• Males 5x more likely to die, and ETOh plays a role in over half of the deaths!
• Fences decrease this risk by 3-4 fold.

Pathophysiology, what causes you to die?
• Two types of drowning wet [inhaled water] and dry [inhaled liquid caused laryngospasm and this resulted in suffocation], probably not an important distinction.
• Death is from asphyxia with hypoxia and then cardiac arrest.
• Historically we made a big deal about fresh versus salt water drowning, but it probably is not important.
• Hypoxia is the key , and 10 % of survivors have residual neurologic damage .Hypothermia may be key here. If the patient is comatose keep them hypothermic. Don’t rewarm them.
• Near drowning is defined as immediate survival after a drowning episode.

Drowning cont’d
• Almost half of drowning victims have no CPR on scene. We must ensure Dispatch provides prearrival instructions , and make a note of this.
• The first step is extraction of the victim from the water. Scene safety is paramount.
• Crowd Control and prevention of secondary victims are essential

Management of Drowning Victims
• Airway management should begin immediately with BVM
• Anticipate Vomiting [86 %!]• Don’t try to clear the airway of water• Near drowning = presence of vital signs “ Near
drowning victims should not be permitted to refuse transport “
• Monitor EKG, v.s., O2 sats, capnometry

Cspines and Drowning• You must consider the potential for cervical spine
injury. In 2 large series each patient with cspine injury had a mechanism of injury to suggest possible cspine trauma
• “routine stabilization of the cervical spine is not necessary unless the circumstances leading to the submersion episode indicate that trauma is likely” [per the AHA]
• H/o diving , water slide use , alcohol intoxication or physical signs of injury suggest the need to immobilize the neck.

Rewarming of Drowned Victims
• For hypothermic patients rewarming is appropriate, if they are mentating .
• First remove the patient from the water• Wet clothing should be removed• Externally and Internally rewarm the victims.
Warm packs, warmed O2, warmed IV fluids, warm the vehicle.
Lightning Injuries, epidemiology
• 22 million lightning flashes per year in the US• Peak time is 3-6 PM• 40-60 deaths per year, males 3x more likely
than females to die , highest risk 10-20 yrs old• 5-10 % mortality with a direct lightning strike• 90% with disability from a strike• Defibrillation in patients with cardiac arrest IS
INDICATED.

Lightning Injuries• Most common cause of death is cardiac arrest from ventricular
fibrillation• A prolonged respiratory arrest may follow a strike , even after
ROSC . Continued attention to the airway may be life saving.• Lightning has extremely high current 30 million volts, for only 1-2
milliseconds. Injuries may be from trauma caused by the strike . Must consider secondary trauma in victims of lightning strikes.
• Lightning victims retain NO RESIDUAL electrical activity and are safe to touch.
• Normally guidelines for MCI events suggest passing over victims in cardiac arrest and attending to those with other injuries. However with lightning strikes “reverse triage “ applies. Patients in arrest are to be treated first because of the data that early CPR and resuscitation is successful for these patients

More on Injuries with Lightning
• A unique feature that may occur is transient paralysis , and or PULSELESS!, keraunoparalysis is thought to be due to vasospasm.
• Approximately 50 % of victims will have rupture of tympanic membranes , ruptured eardrums.
• EKG’s must be performed on all lightning strike victims• Victims of lightning strikes without cardiac arrest may
be discharged from the ER, if their EKG’s are normal both in the field and the ER and there is no LOC.
• You must do a thorough exam and be mindful of the possibility of secondary injuries in these patients

How to Avoid Lightning Strikes• 30/30 Rule. Because most lightning flashes occur within 5-6
miles of the previous strike, you should take cover if the flash –bang is 30 seconds or less. The time from the flash of the lightning to the bang of the thunder should be divided by 5 to estimate the number of miles away. 30/5= 6 miles away.
• Additionally you should remain under cover until the last flash and bang is 30 minutes.
• Indoors stay away from windows, plumbing and wires• A vehicle with a metal roof, fully enclosed with closed
windows is considered safe. Do not use electrical devices during the storm.
• Avoid open fields, ridge tops , water, metal objects , poles

Heat Exposure…… it is getting to that time again [thank goodness]
• Normal body temperature is tightly controlled. Increased and decreased blood flow to the periphery controls our temperature, regulated by the hypothalamus . The sympathetic nervous system controls sweating at the periphery as well . Normally the majority of heat loss is through radiation [transfer of heat directly to the environment], with evaporation of sweat playing a role as well.
Heat cont’d
• An increase in core body temperature will denaturize proteins and cause inflammation and vascular injury eventually causing DIC with hemorrhage and clotting , resulting in widespread cellular destruction and death.
• Volume repletion and electrolyte replacement are 2 keys to prevent injury

Heat Illnesses• Heat Edema: caused by vasodilation of the
periphery to cool off and results in pooling of blood in the legs and consequent edema. This is not dangerous.
• Heat syncope: Same mechanism of injury. Peripheral pooling of blood resulting in a drop in central BP that ends in syncope.
• Heat Cramps: usually though to be due to electrolyte abnormalities. These are not dangerous , but may be a clue to hypokalemia, or hyponatremia.
• Heat Exhaustion: Caused by volume and electrolyte depletion . Symptoms include nausea, headaches , muscle cramps .

Heat Stroke
• The most serious manifestation of heat related injuries . This is a true emergency.
• The patient is hyperthermic [temp > 40 C, 104 F].They have an abnormal mental status and may be confused, or even in coma.The patient s may be wet [sweaty] or dry. There are 3 groups that are particularly at risk :
• Elderly, chronically ill patients during a heat wave• Exercising athletes in very high temps• Patients on certain psychiatric medications like
phenothiazines.

Treatment
• Remove the patients from the heat.• Active cooling . Get the patient wet
[evaporation], provide air movement by air conditioning or fanning [convection]
• Cool packs [for conductive heat loss]• Volume and electrolytes should be replaced.
Give NS , call medical control , EKG is indicated [looking for changes of hyperkalemia ]. If there is a change in mental status a FS glucose …

Insect Stings• Anaphylaxis is well known to us all. So what can I tell
you don’t already know ? • There are 3 families of hymenoptera that can cause
anaphylaxis,1: honeybees and bumblebees 2: vespids like yellow jackets, hornets and wasps 3 : fire ants. The venom in fire ants is identical to bees.
• Remember that IM epi is better than sub Q, remember that the thigh is better than the arm.
• Multiple stings increases the risk of anaphylaxis• If a patient is taking beta blockers they may not
respond to epi. Remember that glucagon in 1 mg increments MUST be used to overcome this effect.
A recent NEJM study on the use of hypothermia in children after cardiac arrests showed that hypothermia resulted in a 30 % higher survival [38 % vs 20 % survival] and a 70 % higher likelihood of a good neurological outcome than normothermia. •Cooling slows metabolic demands , each degree Celsius reduces the metabolic rate by 7 % . It will also decrease intracranial pressure and decrease the heart rate.
Pregnancy and Cardiac Arrest • Cardioversion is safe
Turn the patient on the side, you must get the uterus off the IVC to improve blood flow ACLS recommendations for rx doses and defibrillation do not change If the pregnancy is advanced [uterus at the umbilicus] consider Csection if within 5 minutes of the arrest!

Oxygen• Once again…..• A recent article by Stub,D on STEMI patients
needs to be “aired”. The AVOID trial.• 683 pts with suspected STEMIs,441 confirmed.
They randomized the patients to NO o2 [O2 sat >94%] or 8 L/min by face mask. They found that those who received O2 had larger infarcts.

Cochrane Database• The Cochrane database review in 2010 and
updated in 2013 reported that there are 4 trials of AMI and O2 that looked at 430 patients and there are 17 excess deaths in the patients rx with O2. The RR is over 3. You are more than 3 times more likely to die if O2 is given when you are having an acute MI if the O2 saturation is > than 94 % [you don’t need it ] .

More on O2• Other studies reveal that at cath that coronary
blood flow will decrease by 30 % with 100% FIo2 compared to RA.
• Hyperoxia will decrease cerebral blood flow, shown in a 1988 study.
• These studies make it clear that O2 is a vasoactive drug and that it should be given only to patients who need it…. Per the AHA 2010 guidelines
Alcohol• The subject arises on how to determine
intoxication…..blood tests, breathalyzer etc. “The only reliable test for determining the level of intoxication is the physical examination” Can you carry on a normal conversation without slurring your words, can you walk without ataxia, is your judgment and insight reasonable ?

Tobacco • Smokers die on average more than a decade
before nonsmokers.• It is estimated to cause 480,000 deaths per
year [even more than cardiac arrests!] This is 1/5 of all the deaths in the US. More recently this number has been challenged …. It is thought that it probably causes 550,-600,000 deaths per year ! It has recently been thought to increase breast cancer and prostate cancer mortality.

End Of Life and EMS
• POLST ,physician orders for life sustaining treatment , the replacement for DNR , may allow us to think about how we can help this process along. Maybe think about discussing with nursing homes who does not need CPR , or DNH ,do not transport to the hospital. maybe we should have a list . Maybe …
WELLENS SYNDROME: A LIFE SAVING DIAGNOSIS
• Critical stenosis of the proximal LAD • Classic ECG presentation• • Biphasic or deeply inverted T waves in leads V2 and V3
• Sometimes V1, V4, V5 and V6
• Despite zero or minimal ST elevation, loss of precordial R wave
• progression or pathologic precordial Q waves
Parikh, K.S., et al, Am J Emerg Med 30(1):225.e3, January 2012

WELLENS SYNDROME
• Type 1 (A) (76%) – Deep symmetrically inverted T waves in precordial
leads V2 V3
• Type 2(B) (24%) - Biphasic T waves in V2 V3 identified as a distinctive upsloping followed by a sharp downslope that differs from T wave inversion due to other etiologies


WELLENS SYNDROME: A LIFE SAVING DIAGNOSIS
Use of AVR to Diagnose Left main Occlusions


The value of ST segment elevation in lead aVR for predicting left main coronary artery lesion in patients suspected of acute coronary syndrome.
• 400 Pts with typical chest pain
• PCI performed within 48 hours of CCU admission
• 31% had aVR STE 1 mm
• Men/Women with STE in aVR: 40.7%/43.8%
• Sens/Spec: 62.7%/73.6%
Rom J Intern Med. 2012 Apr Jun;50(2):159 64.

• A second article was written about this entity by Hennings , J.R. et al. There was ST elevation in AVR with diffuse ST depression in many other leads. The patients had L main, Proximal LAD or multivessels CAD with acute coronary occlusions

STEMI with a LBBB
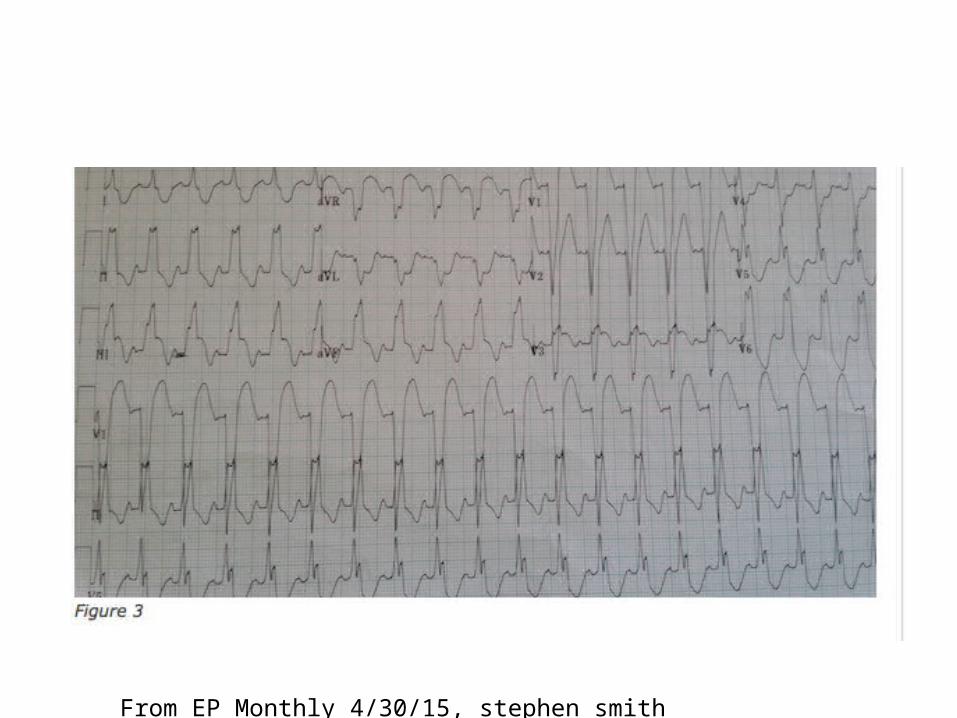
• Sgarbossa criteria: In a normal LBBB the ST segment is in the opposite direction of the QRS. When they are in the same direction a STEMI is likely [70 %] . The EKG that follows shows this.

From EP Monthly Stephen Smith, 4/30/15

From EP Monthly,Stephen Smith, April 30,2015

• In the EKG above the V1-V3 have a predominant S wave and the ST segments are positive. In V5-V6 the R waves are positive and the ST segments are negative. This is normal in a LBBB. However if you look at leads III and AVF there is a positive QRS and ST elevation ..they are in the same direction. This is not ok [concordant ] . It is likely due to a STEMI
From EP Monthly 4/30/15, stephen smith

STEMI and LBBB
• The above EKG is another example of this Now clearly in III and AVF there s ST elevation and a positive QRS. This is diagnostic of a STEMI with a LBBB. Lead V3 is also suggestive of concordance the ST segments and the QRS go in the same direction.

Shock• We have not discussed this in a while and a
brief review seems reasonable• Shock occurs when the body metabolic
demands exceed the supply. Mortality is high. The time to identification can decrease mortality . Early antibiotics for sepsis, earlier door to balloon times for cardiogenic shock, and early interventions with traumatic shock patients may decrease mortality
Shock continued • Classification:• Hypovolemic: either hemorrhage or fluid
losses,• Cardiogenic: the heart cannot maintain an
adequate cardiac output• Distributive : normal volume, but vasodilation
results in shock• Hypovolemia , usually hemorrhagic or volume
losses• Obstructive : Limited cardiac filling or
increased afterload

More shock
• Distributive: normal volume but vascular dilatation causes hypotension. The 3 best examples are sepsis, neurogenic and anaphylactic. All result from vasodilation. The neurogenic occur with a high cervical spinal cord injury and there is usually bradycardia
More on shock
• Obstructive : Tamponade resulting in minimal venous inflow, massive pulmonary embolism [limited RV cardiac output], and pneumothorax [again limited venous input]

Shock • Examination: start with the usual suspects –
primary survey. Assess that the airway is intact, and that the patient is ventilating the lungs.If there are absent BS then a pnemothorax or large effusion may be the cause.
• If there are signs of hemorrhage address these with pressure and potentially tourniquets . If pressure and tourniquets cannot be used , in areas like the axilla then Quickclot may be useful.
Shocking continued• Head to Toe exam is next.• Is the mental status diminished? It often is
with shock. Is there pallor from hemorrhage? Look for neck vein distention – a reflection of CVP and this may indicate tamponade, cardiogenic shock and may clearly show that hypovolemia is not the issue.
• Look at the belly. Is there any ecchymosis to indicate trauma? Is there a pulsatile mass from a AAA?
• Extremities:Pssive leg raise test transiently increases venous return .Hypovolemia present

Shock• Prehospital testing: • A FS glucose may reveal marked
hyperglycemia • EKG A STEMI is often the cause of cardiogenic
shock. Ischemia may also be the result of the hypotension. Electrical alternans suggests tamponade

Electrical Alternans
Electrical alternans is recognized by alternating amplitudes of the QRS complexes. The most frequent cause is a pericardial effusion . It is thought to result from the swinging motion of the heart from the weight of the effusion in the perciardial sac.

From UP TO DATE

STEMI Diagnosis
• Use of reciprocal changes

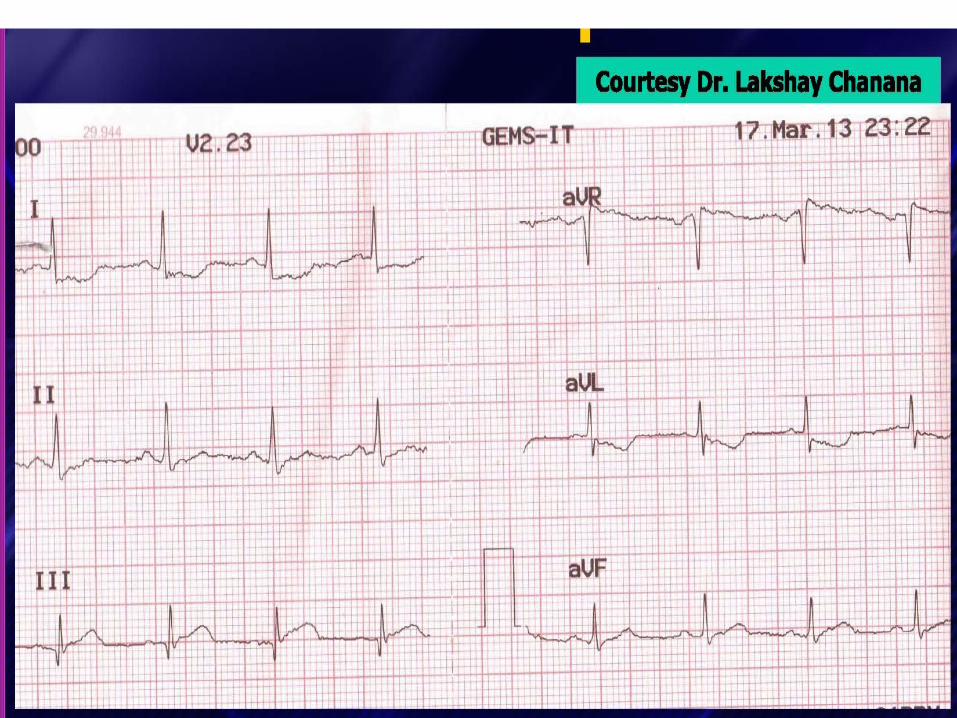
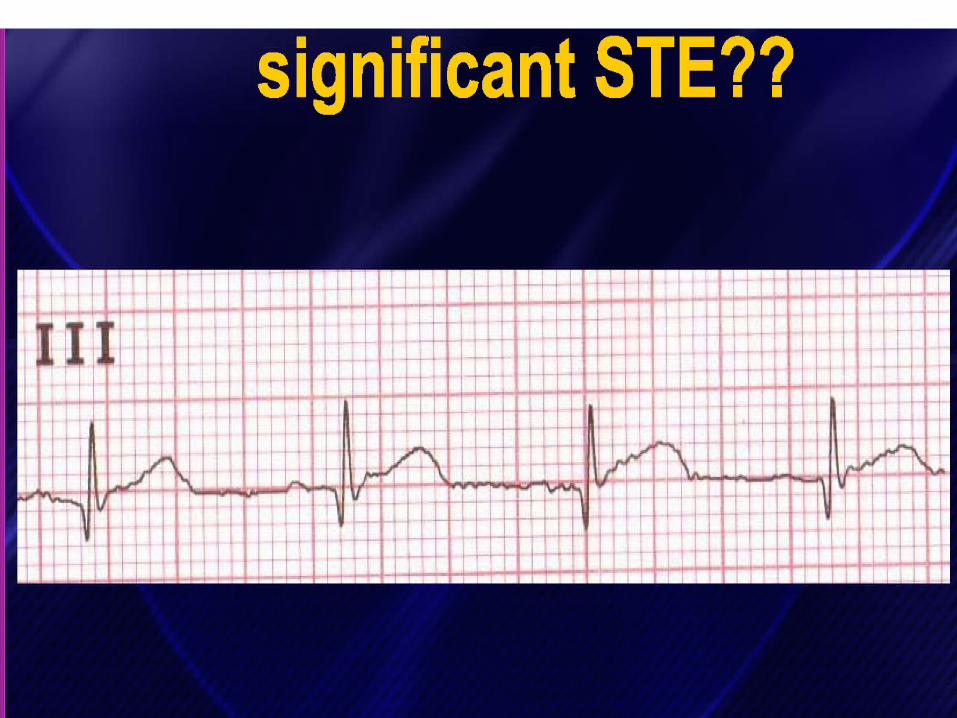





Is There STE?

Is There STE?


















