45
| Date post: | 07-Apr-2017 |
| Category: |
Education |
| Upload: | mary-jane-waite |
| View: | 171 times |
| Download: | 2 times |

Cases

Cases
• O2 and a Sat of 98 %• Anaphylaxis and benadryl use • Heroin Overdose and a cardiac arrest

Hypoglycemia
• Why do we use D50 ? • An ampoule of D50 has 25 gms of glucose .
We normally have only 5 gms of glucose in our bloodstream. We are giving 5 x that dose. At a normal glucose level we cannot transport any more glucose to the brain. This results in hyperglycemia.

Hypoglycemia cont’d
• Furthermore D50 is very hypertonic. The osmolality of D50 is 2,525 milliosms and normal is 295. It is almost 10 fold higher. This results in skin necrosis if the D50 leaks. It also may sclerose the vein .
• D10 has 10 gms of glucose and is twice the normal amount in the bloodstream. It is not very hypertonic [twice normal] and is unlikely to cause skin necrosis if it leaks or cause a vein to sclerose.

Hypoglycemia
• In a recent study of 164 hypoglycemic adult patients only 18 % of patients required a second dose of 10 gms and only 1 patient needed a third dose. There were no reported adverse events.
• We should only use D10 [assuming we have it] . It is less likely to wreak havoc on the veins, and it is far less likely to cause rebound hyperglycemia . No down side and plenty of upside.

Videolaryngoscopy
• In a recent EMS study from Texas and Mississippi they showed a marked difference in the rate of intubation with the use of a video laryngoscope versus direct laryngoscopy. First pass success was 74 % vs 44 %. Overall success was 92 % with the video laryngoscope vs 65 % for direct laryngoscopy.

Synthetic Cannabinoids
• Marijuana…active ingredient is THC. There are now many synthetic cannabinoids [SC] available . They first appeared in 2008 and they have proliferated. Sold as liquid for e cigarettes , dissolved in energy drinks , sold as “legal alternatives to marijuana” , they are dangerous. Over 26 synthetic cannabinoids are considered schedule 1 drugs [highly illegal] .

Toxicology of the MonthK2, Spice, and Synthetic Cannabinoids
• 1. What are they? They are full agonists of the cannabinoid receptor with an affinity 100 x greater than THC!
• Usually bought from China, sprayed on inert plant material.
• Earlier this year NYC reported 2,300 ED visits in 2 months ! Marijuana is the most frequently used substance, synthetic cannabinoids are 2nd , with up to 10 % of high school students reporting use in one survey !

More K2
• These are sold in gas stations, smoke shops, and widely available online. They are cheap to buy [$5 per gram in some cases] .
• They are smoked as joints or in pipes in 50 %, or in a water bong in half %. They are occasionally ingested in cookies or cakes.

ER Presentations
• In a recent case series over half had hyperglycemia, and over half had a tachycardia . A low k was seen in 41 v%, and nausea and vomiting were seen in 1/3. Confusion was seen in 1/3, aggressive behavior [like PCP or bath salts] in 1/3 or lethargy in 1/3. One fourth needed an ICU and required intubation. This can be a big deal.

RX
• 1. Toxic screens are negative for these drugs. More advanced labs can identify the drugs .
• 2 . Treatment is supportive…. Benzos and haldol prn. The effects of these drugs are usually shortlived [thank goodness] .

More
• Three side effects of cannabis will be noted. Cannabis use increases the likelihood of psychosis by 1.5-2 fold. You are one and one half to twice as likely to become psychotic if you smoke marijuana.
• Marijuana use decreases testosterone levels and lowers sperm counts . It will decrease fertility in men.

Dietary Supplements
• Between 2004 and 2014 the CDC estimates that there are 23,000 ER visits per year from adverse effects from dietary supplements. Weight loss and energy products caused ¾ of these events. Unsupervised kids had overdoses accounting for 1/5 of the ER visits. These include weight loss products, vitamin pills, energy products, iron supplements. In men, body building and sexual enhancement products were implicated in 1/7 of the ER visits.

Treatment of Hypoglycemia
• Why do we use D50 ? • An ampoule of D50 has 25 gms of glucose .
We normally have only 5 gms of glucose in our bloodstream. We are giving 5 x that dose. At a normal glucose level we cannot transport any more glucose to the brain. This results in hyperglycemia.

Hypoglycemia cont’d
• Furthermore D50 is very hypertonic. The osmolality of D50 is 2,525 milliosms and normal is 295. It is almost 10 fold higher. This results in skin necrosis if the D50 leaks. It also may sclerose the vein .
• D10 has 10 gms of glucose and is twice the normal amount in the bloodstream. It is not very hypertonic [twice normal] and is unlikely to cause skin necrosis if it leaks or cause a vein to sclerose.

Hypoglycemia
• In a recent study of 164 hypoglycemic adult patients only 18 % of patients required a second dose of 10 gms and only 1 patient needed a third dose. There were no reported adverse events.
• We should only use D10 [assuming we have it] . It is less likely to wreak havoc on the veins, and it is far less likely to cause rebound hyperglycemia . No down side and plenty of upside.

Oxygen ?
High flow, low flow or no flow? What evidence do we have that it is
harmful?

Cochrane Database and O2• The Cochrane database review in 2010 and in
2013 reported that there are 4 trials of AMI and O2 that looked at 430 patients. You are more than 3 times more likely to die if O2 is given when you are having an acute MI if the O2 saturation is >than 94 % [you don’t need it ] .

Oxygen and Acute MI, CVA and ACS
• The 2010 ACLS guidelines suggest that EMS care include oxygen only if the O2 saturation is < 94 % for all patients with acute MI, CVA and ACS patients.
• The use of oxygen is also suggested for patients with dyspnea, obvious heart failure, or if the oxygen saturation is unknown.

More on O2• Hyperoxia will decrease cerebral blood flow,
shown in a 1988 study. • These studies make it clear that O2 is a
vasoactive drug and that it should be given only to patients who need it…. Per the AHA 2010 guidelines

Oxygen and Acute MI, CVA and ACS
• The 2010 ACLS guidelines suggest that EMS care include oxygen only if the O2 saturation is < 94 % for all patients with acute MI, CVA and ACS patients.
• The use of oxygen is also suggested for patients with dyspnea, obvious heart failure, or if the oxygen saturation is unknown.

Harm
• “ There is no single threshold of FiO2 defining a safe upper limit for prevention of oxygen toxicity .” [UPTODATE 2011] How long the patient is exposed to a high FiO2 , and the concentration of the oxygen determines how likely the patient is to suffer harm.

Harm From Intubation
• The ROC investigators showed a 6.8 x increase in the risk of aspiration pneumonia after prehospital intubation

Anaphylaxis
• Definition: remember skin plus either upper or lower respiratory involvement with shortness of breath , hypoxemia, wheezes , or stridor .
• OR • Skin or mucosa, plus decreased BP, or
respiratory symptoms, or syncope, or GI symptoms.

Anaphylaxis contd
• The Rx of choice is epinephrine.It should be given in the thigh IM. Do not give it in the arm, do not give it sub Q.
• Benadryl is slow in onset and has no effect on BP, upper airways and lower airways.
• If the BP does not rise with the epinephrine a fluid bolus of 1-2 liters is indicated.

Heroin Overdose and Cardiac Arrest
• Case

Epinephrine and Cardiac Arrests
• There has been a lot of question about the utility of epinephrine in cardiac arrests. Three recent papers should help guide our efforts. Our resuscitation rates are 40 %. This is markedly better than most communities. Epinephrine is a part of our protocol and we should continue to use it given our success. But what does the recent literature and scientific data reveal ?

Two recent papers from the AHA database using the GWTG on adults and children
• BMJ 5/2014 Donnino, Michael et al . They studied 120,000 in patient PEA and Asystole cardiac arrests to examine the question of timing in administering epinephrine. What they found was that if given at 1 minute 12 % survival was seen and if given at 7 minutes there was only a 7% survival. Neurologically the patients who got the drug early did much better neurologically. There was a 10-20 % decrease in survival for every 3 minutes in administration of epi. YOU MUST GIVE IT EARLY.

Pediatric nonshockable arrests and Epinephrine
• In JAMA August 2015, 1 month ago by Lars Anderson [really !] et al . They had 1558 patients and again the time to epinephrine was critical. If the time to epi was >5 minutes the survival to discharge was 21 %. If the epi was given in <5 minutes the survival to discharge was 33%. There was a stepwise decrease in survival, neurological outcome for delays in administration of epinephrine just as was seen in adults. GIVE IT EARLY

Epinephrine in Cardiac Arrests
• Newest data from North Carolina supports the AHA suggesting that TIMING of use is paramount. Vasopressin is out of the AHA protocol. There is a 4 % decline in ROSC for every minute of delay in the use of epinephrine !!!

Post Medication Hypotension
• Use of opioids and benzos is more likely to result in hypotension if the patient is intubated [ 5 x increase] , needs a drug to keep their pressure up [DUH] , or has a surgical diagnosis [ like maybe they are bleeding …] .

Accidental Hypothermia
• Hypothermia is defined as a core temperature less than 35 C [95 F].
• The severity is defined by the temperature • Mild [stage I], 32-35C, 90-95 F, accompanied by
shivering, tachycardia , usually awake and alert• Moderate [stage II], 32-28 C, 89-82 F, NOT shivering
with altered mental status• Much of this talk is derived from UP TO DATE and a
NEJM article from 2012 by Brown, Brugger, Boyd and Paal.

Hypothermia stages cont’d
• Stage III, 28-24 C, 81-75 F, unconscious and not shivering , these patients still have VS!
• Stage IV , 13.7-24 C, 75-56 F. No VS. • Stage V temp ,13.7 C or 56 F is dead. Irreversible
hypothermia. • The stages are paramount. If you have a conscious
patient who is cold and shivering …if you have a conscious patient who is very cold and not shivering , or a patient who is unconscious and not shiveering , or a patient who has no VS and is very cold...

Pathophysiology• Body temperature is a result of production of
heat and loss of heat. Heat is generated by metabolism , mostly of the heart and liver, heat is lost mostly by the skin and lungs.
• Evaporation [sweat]• Radiation• Conduction [direct heat transfer from a body to
an adjacent cooler objet [like snow or water] • Convection [direct loss to the air]
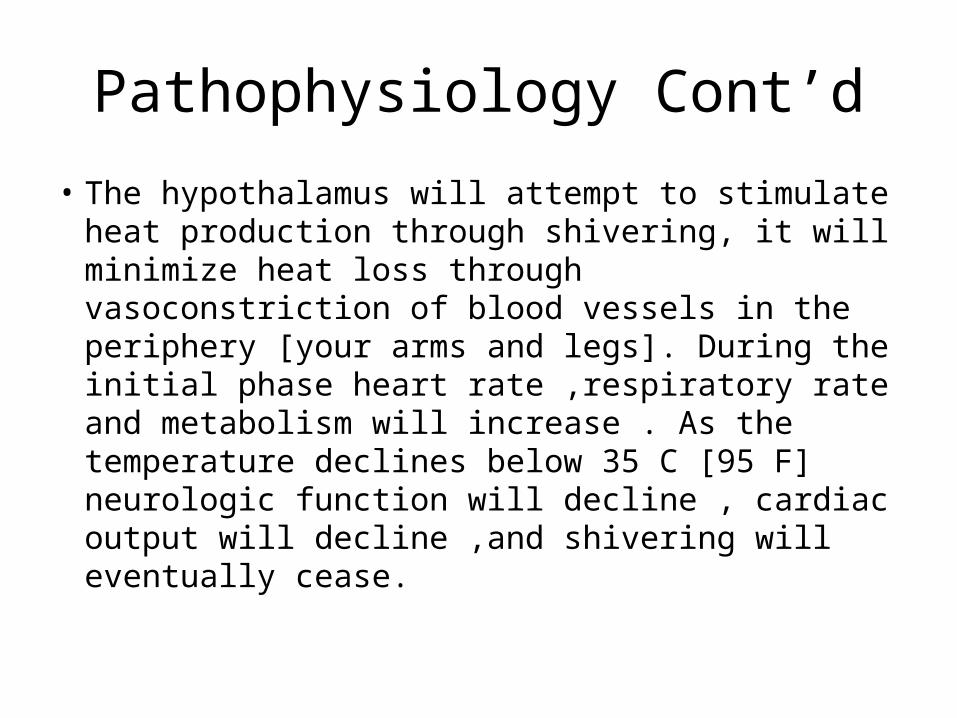
Pathophysiology Cont’d
• The hypothalamus will attempt to stimulate heat production through shivering, it will minimize heat loss through vasoconstriction of blood vessels in the periphery [your arms and legs]. During the initial phase heart rate ,respiratory rate and metabolism will increase . As the temperature declines below 35 C [95 F] neurologic function will decline , cardiac output will decline ,and shivering will eventually cease.

Clinical Presentations
• With mild hypothermia you will see shivering, tachycardia, tachypnea , dysarthria , and impaired judgment
• With moderate hypothermia you may see decreased heart rate, cardiac output and BP, lethargy, and loss of shivering. The patient may paradoxically undress ! Afib may occur and should not be treated.
• With severe hypothermia ventricular arrhythmias may occur, eventually asystole ensues

Pearls
• Beware of VS inconsistent with the degree of hypothermia! The level of consciousness should be consistent with the temperature
• Risk factors for hypothermia also suggest other diagnoses to be aware of: ETOH, IVDA, Psychiatric disease [and the rx they take], old patients [sepsis may present with hypothermia],

Assessment
• See above, additionally a FS glucose and an EKG are indicated, oximetry , capnometry . The oximetry may be problematic , they are vasoconstricted, try the ear.
• The Ekg may be slowed, may have Osborne waves. There may be slowed conduction with a bradycardia , prolonged PR, QRS and QT intervals.
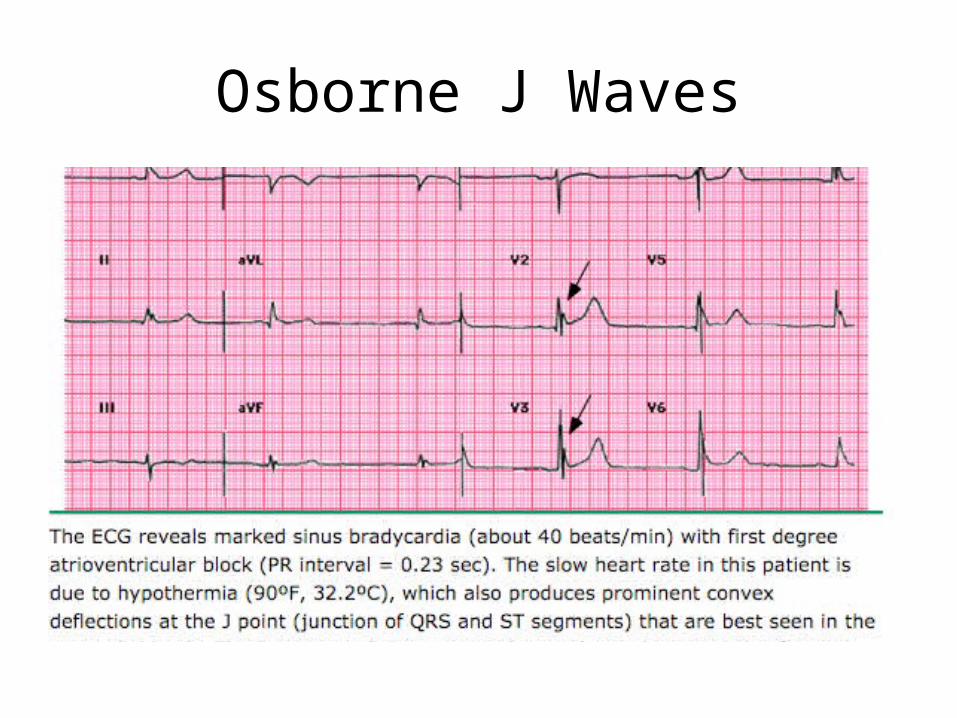
Osborne J Waves

Management• ABCs, preventing further heat loss, initiation of rewarming• Peripheral pulses can be very difficult to palpate in a
vasoconstricted , bradycardic patient . Check for a central pulse for 60 seconds!.
• “Always assume that some perfusion is occurring if there is any signs of life. CHEST COMPRESSIONS SHOULD NOT BE DONE IF THERE IS AN ORGANIZED RHYTHM ON THE EKG.” Even if you feel no pulse, don’t start CPR. The reasoning is that the rhythm may be interrupted by chest compressions and that the “PEA” is likely to be transitory.
• Asystole equals CPR• Initiate 2 I/O lines or 2 large bore IV’s, these patients
typically get hypotensive .

Management Cont’d
• Full body insulation with warmed blankets etc, cutting away any wet clothing, and initiating rewarming . DO NOT DELAY CPR if indicated : no signs of life and asystole.
• Heated O2, warmed IV fluids.• Persistent movement or breathing should prompt
watchful waiting and delaying CPR.• The longest reported survival with CPR and rewarming
was over 6 hours ! Remember they are hypothermic and their cerebral oxygen requirement are very low!

Rescue Collapse
• Rescue collapse is a cardiac arrest that occurs during extrication . All of the literature emphasizes the need to be very gentle with these patients.
• The patient should be extracted in the horizontal position, “even low intensity use of peripheral muscles should be avoided… to avoid afterdrop of temperature”. “Rough handling of the patient may precipitate ventricular fibrillation.”

Other Pearls
• “Bradycardia may be physiologic in severe hypothermia”
• “Ventricular arrhythmias may be refractory until the patient is rewarmed”. The definitive rx of the arrhythmia is focused on aggressively rewarming the patient”, in conjunction with CPR [if needed]
• They suggest a single shock and no further shocks until the temperature is one degree higher!

Other Interesting Information
• Avalanche burial. The burial time may be estimated by the core temperature, a temperature <35 C correlates with a burial time of more than 35 minutes.
• Drowning in cold water has a better likelihood of a good outcome than in warm water. The longest submersion survival with intact neurological outcome is 66 minutes in a child.
• The lowest body temperature recorded in a patient with full recovery is 57 F!


















