42
University of Pittsburgh Fall 2002 School of Health and Rehabilitation Sciences

U n i v e r s i t y o f P i t t s b u r g h
F a l l 2 0 0 2
S c h o o l o f H e a l t h a n d R e h a b i l i t a t i o n S c i e n c e s

School of Health and Rehab i l i tat ion Sc i ences — Fall 2002 — Contents
About the covers: Front: Behind every successful college football team is a dedicated support cast.Take an inside look at the world of athletic training. Page 15
Back: During the 1930s and ’40s, manufacturers developed body-worn designsthat housed vacuum tubes and microphoneswithin a single unit, which allowed forportability. These early body-worn vacuumtube hearing aids were cumbersome andrequired wires to connect the batteries andthe earpiece to the microphone/amplifierunit. Hearing aid batteries were at least aslarge as the other components and weighedup to 2.5 pounds.
Communication Science & DisordersListening Carefully for the Clues
Discovering the Factors Behind Childhood Communication Disorders
Health Information ManagementPreventing the Preventable
Eliminating Errors from Patient Records
Occupational TherapyA Soldier’s Story
An O.T. Graduate Applies His Skills in Time of WarOrganizing Knowledge for Evidence-Based Practice
New Curriculum Design Puts the Universal Language of Human Function into Practice
Physical TherapyDirect Access Coming to PA
Act 6 of 2002 Lets Physical Therapists See Patients Without a Physician Referral
Emergency MedicineKnowledge without Borders
Extending the Reach of Emergency Medicine Expertise
Rehabilitation Science & TechnologyThe Final Phase
The HERL Machine Shop Turns Research into Reality
Sports Medicine & NutritionAthletic Training Goes International
Japanese Students Visit Athletic Training Program
DialogueA Conversation with Congresswoman Melissa Hart
AdministrationCliff’s Notes
Dean Cliff Brubaker on a Leaner Look Giving
Karen Khan on Planned Giving FeedbackThanks to our Donors and Friends Masters of Studies in Law
Disabilities Law ConcentrationAccess
Dr. Malcolm McNeil Discusses the Dwindling Number of Ph.D. Students
Team Leader Board of Visitors Chair Andy Kuzneski Says SHRSFielding a Winning Team
Faculty, Alumni and StudentsPanther Pride
Brian Beinecke Works Hard On and Off the FieldOlin Teague Award
Dr. Rory Cooper Honored by the VAClass Acts New and Noteworthy Community of Neighbors
Nancy Mizak, Chris Marchionda, and Working OrderYearbook Summer in America
A Pittsburgh Sabbatical for Dr. Lucas van der WoudeCalendar of Events
Inside Look Training Day
The Challenges and Rewards of Clinical Education in Athletic Training
3
5
568
12
13
8
9
91011
1114
38
15
w w w . s h r s . p i t t . e d u
20
22
24
27
28
30
32
36
39

Upon reading this issue of FACETS you may notice that it is a bit leanerand has a slightly different look. It has been quite a challenge to convey
comprehensive information and include feature articles for six departments with nine distinct professional academic disciplines.
The major change has been a reduction in the number of “feature” articles. Instead of running major articles for each program in each issue, we shall now include features according to the timeliness, relevance, andimpact on the individual and collective interests of our community. We shall focus on the three to four mostnewsworthy events and present them in greater depth. We believe these changes will enable us to present youwith a more focused and more efficient publication without diluting the dissemination of information on theprograms of our school.
We shall continue to present information and news in a dedicated section for each program of SHRS. It is our intent to continue to feature individuals and events for all programs. We anticipate that each program will be featured in due course.
Significant changesBy now it is generally evident that entry-level training in the Health and Rehabilitation professions has evolved from what began almost exclusively as baccalaureate degree programs to graduate level training and now to professional doctoral degrees. These changes have resulted both from curricular pressures and the ever-increasing sophistication and maturation of our several fields of endeavor.
We, of course, must both adapt and provide leadership to facilitate these transitions. A significant consequence of the trend toward professional doctorates is a substantial increase in enrollment. The transition from two-yearto three- and four-year professional training programs has the obvious consequence of a 50 percent to 100 percent growth in student enrollment and a necessary relative increase in faculty. I shall note parentheticallythat this growth will be realized without any increase in class sizes.
What appeared as spacious, perhaps even excess, space when we moved from Pennsylvania Hall to the newForbes Tower in 1996 has now become saturated. With rapidly expanding enrollment over the next three to four years and a combined research enterprise that is currently expanding by more than 20 percent annually, SHRS again is confronted with space problems.
How we shall resolve our growing space needs is not yet completely evident. We shall certainly respond to this challenge. We shall most surely do this with greater facility and ease with your advice, participation, and assistance.
We are most interested in hearing from you on the “new look” for FACETS. We also would like to hear from youon other issues and events.
With kindest regards,
Clifford E. Brubaker
From the Dean
CLIFF’S NOTES A Leaner Look
3

University of Pittsburgh
PublisherClifford E. BrubakerExecutive EditorKaren T. KhanEditorPatrick T. MangusCreative DirectorVince J. LongoArt DirectorDiana L. BaierEditorial StaffDaryl ClemmensLinda DickersonDavid FrielJames HodgesBrendan MangusLauren TrocanoPhotographyBill BoydAnnie O’Neill
University of Pittsburgh
FACETS is published by the Office of the Dean, School of Health andRehabilitation Sciences. It is produced three times yearly for alumni, students, staff, faculty, andfriends of SHRS.
The University of Pittsburgh is an affirmative action, equal opportunityinstitution.
U n i v e r s i t y o f P i t t s b u r g h
F a l l 2 0 0 2
S c h o o l o f H e a l t h a n d R e h a b i l i t a t i o n S c i e n c e s
WhatDo You Think?
Have an opinion about something you read in FACETS?
E-mail your thoughts to Karen Khan at
We’ll print letters to the editor as space allows.
School of Health andRehabilitation Sciences
Board of Directors2002 ROSTER
EXECUTIVE COMMITTEEPaul Rockar, President
MS/PT ‘81
Karl Gibson, Vice PresidentBS/PT ’76; MS/PT ‘83
Neil J. Szuminsky, SecretaryBS/CLS ’76; MS/CLS ‘80
EX-OFFICIO MEMBERSClifford E. Brubaker, Ph.D.
Dean
Juli GasperiCoordinator of Alumni Affairs
Karen KhanDirector of Development
Board At-LargeMeghan Bartlett
MA/CSD ’00
Kevin ConleyMS/SM ‘93
Phillip HolowkaBS/EM ‘99
Alicia KoontzPh.D./RS ‘01
Lori MurrayMS/CDN ‘01
Pamela TotoBS/OT ’89; MS/HSM ‘96
Colleen WhiteBS/OT ’86; MS/HSM ‘92
Linda Dickerson (Chair)
S. Tyrone AlexanderKellie Anderson
Robert BarryJoyce A. Bender
George Board III, Ph.D.Christopher K. Gleason
Charles KeenanBrian Limbach
Tammie McNaughtonH. Lee Noble
Barbara Pippin, MDSargit Singh, MD
Joan SteinRoss Zafonte, DO
Andrew J. Kuzneski, Jr. (Chair)
Susan L. AldreteBruce Baker
John C. BollingerDudley Childress, Ph.D.
Linda A. DickersonAlexandra Enders, OTRChristopher K. Gleason
David B. Gray, Ph.D.Peter F. Koehler, Ph.D.William K. Lieberman
Valerie McDonaldMichele M. McKenneyRobert Nerem, Ph.D.
Winfred M. Phillips, Ph.D.Nino Pionati, M.B.A.
Albert Reynolds, Ph.D.Leopold G. Selker, Ph.D.
Sargit Singh, MDRonald D. Stewart, MD
Board of Visitors
We sincerely appreciate the advice and counsel of the members of our Board of Visitors, our Development
Advisory Council, and our Alumni Society Board
DevelopmentAdvisory Council
Alumni Society

5
the university can provide youand your financial advisor withcharitable and estate planning expertise, andexplain the gift options available to you.
A planned gift helps you make the best use ofyour investments. It combines your interest inmaking a lasting contribution with tax benefitsand savings to your estate.
Karen KhanDirector of Development
If you would like to create a planned gift, makean outright gift, or need more information,please contact me at [email protected] 412-383-6548.
The simplest and mostprevalent type of plannedgift is the bequest: assetsleft by the donor in a willthat will be distributedafter the donor dies.According to GivingUSA, individual donors
gave an astonishing $160.72 billion to philanthropic and charitable causes in 2001,representing 75.8 percent of all giving for theyear. While an exact figure for all planned gifts is not known, bequests accounted for $16.3 billion, or about 8 percent of total individual contributions.
There are many different types of planned gifts,from bequests to gift annuities, charitableremainder unitrusts to pooled income funds.While these terms may sound a little daunting,
Perhaps you’ve been thinking
about making a gift to SHRS, but
are a little hesitant, given today’s
uncertain market. You can achieve
your philanthropic goals, yet retain
your assets or even derive an
income, with a planned, or
deferred, gift.
Unlike an outright gift, where a transfer ofassets benefits the university immediately, adeferred gift is a transfer or pledge of assets thatwill benefit the university at a future time designated by the donor.
Planned gifts fulfill several donor needs:• Preserves capital• Provides current income
(through a trust or annuity)• Maintains current use of asset by the
donor (bequest)• Helps donor achieve philanthropic goals
While planned gifts are not used to meet theimmediate needs of the university, they per-form a vital role by ensuring that resourceswill be available to meet future needs.
GivingA planned gift
helps you make the best
use of your investments.
Going through the pile of mail at the end of a longWednesday, I found the FACETS publication from yourschool. It is indeed a pleasure to read, and it looks so good!I have not seen anything as pleasant from any other schoolanywhere. That article on Looking at the Other Side (of thebrain) was great.
Thanks for sending it to me on a regular basis. It is one of the few things left in my mail that is worthgoing through!
George K. Michalopoulos_________________
I had to write and congratulate you on your exceptionalpublication. I just received a copy a few days ago. What awonderful vehicle for carrying your work to the world!
Kathleen Curtis_________________
Just wanted to let you know that I really enjoyed theFACETS publication. I hope that I will continue to receive it. I appreciated the various articles related to specifichealth professions.
Terri Haupt, PT ’85_________________
I enjoyed the article about Watson. I was in Carol Levin’sclass and one of my affiliations was at the Oakland VAwhile Jane Linn was the director. I went to Watson at agenineteen, graduating two months after I turned 20. I got ajob at Rusk Institute for $4800 year, not the usual $5200,because I did not have a license. You see, I passed my stateboards, but at that time you could not get your license untilyou were 21. So my license is dated July 18, 1964, my 21st birthday.
We had an excellent education. Dr. Wright made usstand at attention if any physician came in to lecture. The instructors watched how we walked (we had to toe in), how we talked. We had 42 in our class. 38 made it.Memories!!!!!
Arlene Chodock Adelman ’63_________________
That was a great article on D. T. Watson. I am a graduate of the school, and the article brought back manymemories of Anne Pascasio and Mary Elizabeth Kolb. I alsofondly remember Dr. Rex Newton who instructed us onPathology. Keep up the good work and certainly the schoolis to be commended for its 100% pass rate on the PA StateBoard Examination.
Francis H. Adams III ’65_________________
Enjoyed reading FACETS. Nice job. I was troubled to findthat the article “Teaching the Hands that Heal” focused onlyon PT and did not even mention the influence of OT. Thewoman treating a child on the right bottom of page 35 is aregistered OT. Note patch on her right arm. I wonder if yourhistory overlooked the other students or therapists whomade significant contributions to D.T. Watson. It was won-derful to get this piece of PT history, but no other servicesare mentioned. I hope that you might expand the historyand help us to a deeper understanding of this institution.
Ruth Schemm_________________
I was in one of the last classes to graduate from D.T.Watson in the Fall of 1966. I, of course, loved the article. Our class was quite unique, besides being the best. We had20 male students and 20 female students and we all livedquite happily in the big house. Of course, we had a housemother on each floor. I have our graduation schoolpicture which was recently published in the APTA PrimeTimers magazine.
Faith Beckerman Goldman ’66
Faith Beckerman Goldman would like to hear from her classmates.She can be reached at [email protected]
Feedback
Karen Khan
Thank
Corporations,Foundations, andOrganizations3M Foundation, Incorporated*American Physical Therapy AssociationArthritis FoundationArthritis Foundation National OfficeAssociated Therapy ResourcesBradford Educational FoundationCIGNA Foundation*Community Nursing ServiceFord Motor Company Fund*Foundation for Physical TherapyJohnson & Johnson*Keystone Paralyzed Veterans of AmericaMahoning Physical Therapy, Inc.Marsh & McLennan Companies*National Athletic Trainers AssociationP. T. Unlimited, Inc.Paralyzed Veterans of AmericaPennsylvania Lions Hearing
Research FoundationPhi Delta GammaPhysical Therapy ClinicRehabilitation Services of
Columbus, Inc.Spinal Cord Research FoundationSunrise Medical HHG, IncorporatedThe Herbert G. Feldman
Charitable FoundationTri-County RehabilitationUnited Way of Allegheny CountyUnited Way of
Southwestern Pennsylvania
*denotes matching gift
Individual DonorsBequestsEstate of Yolanda Barco, Esq.
$500,000Estate of Madeline Pascasio
$ 10,000
Over $5000Pascasio, Anne
$1000 - $4999Brubaker, CliffordChase, ChristineChilds, John D.DiVincenzo, Joseph & Mary JaneDodd, Judith LomakinGibson, Karl & Alice SpringerGrzybek, Geraldine MichelleRockar, Paul AndrewScully, Rosemary M.
$500 - $999Cooper, Rory A. & RosemarieHale, Lynn Hudson & Wayne AndrewHalliwell, Betty AllenHenson, James Barton &
Kristin KlingensmithKelly, William L.Leonard, Laurence BakerMangus, Patrick T.Rubin, Herbert and Judith Aron
$100 - $499Allen, Dorothy B.Barker, Susan AurandtBaumgardner, Judy MarieBeatty, Lee V.Bencic, Amy SorgBennighoff, Brian RaymondBertrand, Timothy JosephBoyd, Miriam RandolphBrienza, David M.Brown, Dalthea D.Buning, Mary EllenCarey, Paula BuckleyChisholm, DeniseChuong Slaby, JenniferCohn, Ellen R.Confer, Michael LeeCook, Judy ShannonCorella, Colleen K. & Joseph AnthonyCramer, Margaret M.Cramp, DavidCremen, Frank J. & Lynn KaraffaDelitto, AnthonyDunwoody, Colleen JaneElsesser, Carol Ann DeemerFerguson, Sandra JeanFisher, John CharlesFletcher, Daniel H.Fogarty, Denise PatriciaFrattali, Carol MarieGilchrist, Paula LizakGlumac, Thomas Eli & Lorraine FisherGoodwin, Patricia DannhardtGraver, Gloria Jean NeubeckGrenke, Dawnyel ReneeGwilt, B. ThelmaHeadley, Sharon K.Hendricks, Mark J. & Sharon
ZahorchakHerring, Deborah EidemHess, Barbara AnnHolm, Margo B.Hosak, Mary AnnHovanec, FrancineHubert, Joshua PaulKaridis, Sara LynnKeener, Suzanne HelmKennedy, Robert AllenKhan, Karen ThereseKing, Colleen O.Klauger, Toni DeniseKlein, Herold R.Knapp, Kathleen KomisinKnepper, Janet D.Kolb, Mary ElizabethKuzneski, Anthony Richard &
Jodell FoleyKwiatkowski, James ThomasLally, Valerie MaggosLarson, Patricia Stump &
Christopher ElliotLerner, Jolie SchockerLesh, Ellen J.Lester, Anne Peretin & Mark A.Lewis, Suzanne BemLong, Barbara G.Love, Ann RenoLovrinic, Jean M.
Luckey, Mary JaneLuncher, Thomas EdwardMadtes, Robert OwenMartin, Palmira MascaroMaziarz, Cynthia AnnMcCoy, Raymond L.McCracken, Thomas D.McKenzie, Patrick A. & Cynthia AnnMcMillen, Cynthia GrygierMiles, CynthiaMolitor, Cynthia BlackMunn-Goins, OpheliaMurphy, Robert A.Musgrave, John KerrNasby, Shirley CampbellNassau, Sharyn Lerner & Richard JoelNixon, Patricia AnnNoviello, Jerry T.Nowaczyk, Mark AO'Connor, Margaret M.O'Hara, NancyPerez, Violet PapadopoulosPoulton, Reece EversonPratt, SheliaRiedman, Richard MerlinRogers, Joan C.Scialabba, Mary AnnShapcott, Nigel G.Shemancik, Ellen GosnellSherwood, Arthur M.Shovlin, Rosanne P. & Timothy DanielSpiegelman, Arlene RobinStaudenmeier, Carolyn Wukitch &
Paul LawrenceStrigle, Kay Shuster & Joseph P.Swaim, Ann DegrawSweeney, Mary PatriciaSweithelm, Ralph CharlesTarplee, Sue CurrieThomas, StacieUhlman, Stephen F.Van Swearingen, Jessie M.Vogt, Molly T.Walk, Gerrilynne Siren & David HomerWelles, Jean CrothersWertheimer, J. B.Weston, Bruce C.Whitman, Steven A.Wiesen, Christine M.Wisneski, Susan EngleWolf, Lois BarnhartWood, Mildred L.Wright, Susan JaneYoung, R. LeeZack, Kathleen McClainZavadak, Kathryn Haffner & Daniel G.Zupances, Walter Edward
$50 - $99Allen, MiltonAnthony, Karen RayeBaginski, Timothy L. & Olive M.Bartlett, Brooks M. & Helen S.Battaglia, Carmela M.Beachler, James DurkinBerman, Natalie S.Beyda, Margaret V.Bianchi, William RussellBojarski, James DennisBrandenstein, M. Jane Schofiel &
Robert EdwardBrehm, JillBresticker, Carol Gentile
Brown, Lori R.Burke, Stephen Patrick &
Rosemary UlyanCarney, John DavidChomas-Bianchi, MargaretColantoni, Lynn Crossman &
Michael JosephColeman, Christine VeselyCover, Brenda K.Csonka, James PaulCurtis, Jean GilmoreDe Como, Peter Michael & Kate MattaDettor, M. Lucille MooreDeuben, Caroll Johnston &
Roger RaymondDixon, Catharine MerrittDohrman, Kimberly BernerDonenwirth, Jaclyn FreemanDunyak, Denise AnnEisaman, Donald F.Emert, Stephanie RayErnst, Mary ZehEustis, Mary-Jo LupesFerrell, Dorothy ShoopFoust, Jean FellowsFox, Elizabeth DianaFranks, ThomasGeld, Susan R.Gentile, Pamela AnnGibson, Karen CollinsGinsburg, Vicki GartenbergGoetz, Tracy AnnGoff, Sean FrancisGreenblatt, Lisa BethGrohe, Anna MarieGross, Anne SiegeGroszkiewicz, Paul D.Guarriello, Karen F.Guo, SongfengHarrington, Paul T.Hatfield, Lisa BrownHenry, Timothy J.Hildebrand, Merry AnnHoerster, LauraHolsinger, Kimberly Anne &
David FranklinHolt, Judith MillerJankowski, Jerome B.Jovanelly, Carol MelissaKamide, Cynthia PeiferKanar, Philip BernardKelly, M. KathleenKelner, Lesley MusselmanKeltz, Margaret MaryKessler, Mark T.Klan, Andrew T.Knight, Barbara RosenKolumban, Evelyn Fetterman &
Michael J.Kraetsch, Vernon W.Lander, Tammy Briggs & Benjamin L.Landers, Maryann GilmartinLeary, David E.Levi, Sandra JeanLiebergott, Jacqueline WeisLindell, David WynnLipsett, Robert J.Lynch, Suzanne B.Lyons, Donna CameronMacner, Jack
6
We want to thank all of our
alumni and friends for their
generous support of the School
of Health and Rehabilitation
Sciences during fiscal year
2002. Your contributions to
the Annual Fund have allowed
us to award scholarships based
on need and academic merit,
provide program support,
graduate research support, and
services to the community.

you7
Thank you
Madigan, Beverly Fogarty & James Eugene
Madler, Patricia JoanMahrer, David J.Malloy, Janet L.Marhefka, Nikki SopcisakMcCloy, Denise,Lyons & James LouisMcGrew, MarybethMcHugh, Linda D.Mechling, Floyd FranklinMilikowski, Karen AnnMinnehan, Peter JamesMolchen, Wanda VirtueMolinero, Ashli MichelleMoya, Carol MutschlerMusselman, Valerie Henigin &
Thomas AndrewMyer, Russ W. & Rebecca FinlanNowotarski, David EdwardO'Brien, Patricia Paris & Patrick JosephOgden, DavidOlson, Patti DonleyPensis, Bobbi J.Pickering, Lee AnnPolosky, Brenda MariePrelock, Patricia AnnProtho, James L.Raju, Barbara SchickReighn, CathleenRematt, Denise IreneReynolds, Scott A.Rhodes, Deborah L. & Robert D.Rich, Wendy BoydRichardson, Fred E. & Mary T.Rogers, SharonRoss, Robin LeighRuberto-Beachler, Nancy J.Rudy, Jeffrey P.Ruttle, Dorothy M.Santa, Victoria LouiseSavor, Christie SueSchaad, Judith Rolley & Joseph WilliamSheaffer, Karl JohnShostek, Mary AnnSimon, Yvonne P.Simpson, Lola Ward & John MiltonSkrabski, Cynthia Jane & Albert WalterSmith, Johnny L.St. Clair, Isabel AnnStankovic, Louise PaulaSteiner, Cynthia WagnerSweeney, Colleen D.Tomazich, Cynthia White & James WesleyToto, Pamela E. BandaloUnrath, Daniel EdwinUrbansky, Kevin Edward &
Deborah MosherVarley, Nancy AllshouseVereb, Christopher AndrewVideon, Tracy M.Viktorin, Carol B.Walter, George Joseph & Kelly KeaneWardrop, Richard B.Watson, Lauren M. & Robert RichardWeibel, Elizabeth SpringerWellman, Maureen SmuroWenstrom, N. Jill DaviesWida, Lori Denise & Thomas PaulWidenhofer, Sharon HahnWilliams, Claire L.Winner, Thomas D.Winters, Katherine RockarYoder, Patricia C.Zakoworotny, Cynthia A.
$25 - $49Altug, ZiyaAndria, Holly Parke & William MarkAskew, Carla L.Ausman, Michele LynnAyala, Clara LozanoBacallao, Pamela Freeman &
Andrew StephenBaker, Sue AnnBarbary, Thelma BarbaraBeal, Nancy DianeBereton, Kimberly LynnBerna, Janet Mary HoltzBertholf, Virginia R.Black, Barbara HoffmanBlair, Jennifer LynnBlaskovich, Anna RoseBoers, Thomas A.Bonville, Susan KellyBoone, SharonBostick, David LawrenceBrown, Julie Kuntz & Michael A.Browne, Mary BehlingBuczak, Kathleen RogelBurns, Robert J.Bynum, Harriett SmithCalabrese, Michael AnthonyCaplan, PhyllisCapra, Mary DeitrichCarey, Charlotte PolesiakClark, Gail AlspaughCollins, Susan FayloColosi, Beth A.Constable, Dianna ChartreauCox, ChristineCox, Sue CoopermanCruikshank, Henrietta SmithDeal, Frances PaulineDenne, Helen LutkusDolby, Elizabeth AnnDougherty, Dorothy K.Doughty, Amy FrancesDurkin, Janet VellikyEckert-Mehaffey, KathleenEger, Diane LevyEllison, Grace SchmittErksa, Sandra GrolockEversole, Jane HendersonFallat, Barbara AnnFeeney, Andrea GorneyFeldman, Sheila ReneeFeroce, Janet Zuck & Kenneth A. Fisher, Theresa SkrippsFitzgerald, Kelley G.Follmer, Laura S.Frank, Hilary M.Franz, Virginia HulshultFucci, Donald James & Joan YurickFurnas, Bobbi JohnsonGalletta, Carole Hostettler & DennisGartley, Linda BienkowskiGerneth, Eileen Jordan & George J.Greenberg-Schroeder, KarenGrimenstein, Jacqueline T.Guilfoyle, Crystal TurnerGurgiolo, Marie A.Hagerty, Kathleen SchultzHahn, Shelly E.Harris, Mary JaneHeiser, Sherry PerozichHeller, Dean Stanley & Susan ShookHemmerle, Margaret West
Henderson, Suzanne EileenHerb, WilliamHockenberry, Peggy SueHolton, Anne BrintonHutchinson, GeoffreyIrvin, Patricia S.Issadore, Lawrence I.Jules, Virginia PeilJurovcik, Kara RaeKalupanov, Margaret K.Kamandulis, MichaelKelly, Mary Jane ParkerKenniston, Nancy ShannahanKernic, JohnKopczyk, Theodore A.Krueger, Robert AndrewKuhns, Doris D.Landgraff, Nancy CrumLarkee, Linda ChubonLilley, Ryan PaulLinhart, Julie GandLombardi, GeorgannLutz, Nancy J.MacDonald, Barbara MellottMarkle, Deborah J.Maruska, MaryMcCorkel, Nancy JanssenMcCullough, Pearl W.McGowan, Marilyn R.McMaster, Edward P.Menzies, Lori Johnson & James CraigMiller, Cari McNelisMiller, Mary M.Mills, Scott AndrewMishock, John R.Moner, Marcia L.Montet, Dennis C.Morales, Dora B.Mostert, Deborah HoltzMoyer, Walter A.Mulzet, John DavidNeidich, Jay S. & Robin BermanNoble, Dorothy BrallierNorth, Barbara L.Owen, Mary NasserPalmer, Paula Joanne & Paul D.Parks, Beth NypaverPatterson, Michael Wilson &
Elizabeth Ann AungsPettler, Joan MaePowers, Cynthia J.Pry, Judith BrownQueen, Florence IrbyRabinowitz, Lisa HoffmanRamsey, Cynthia SerkochRao, Sheela KatikineniRecker, Deborah LynnReicherter, Elizabeth AnneReiner, Yvette Meitner & FrankRepak, Antoinette SoleckiRiccelli, Angelina E.Rick, Rosemarie B.Riddle, Jean ClarkRizzo, Laura SmolkoRoelofs, Jennifer PoehnerRoseto, Patricia MorsaintRotko, John R.Sampogna, Mark P.Schlough, Kathleen
Schmeler, Mark R.Schneider, Janice King & Glenn EricSchomburg, Frederick L.Schreiber, Valerie K.Schroeder, Christine AnnSchuetz, RobertSchwartz, Betty PayneSchwesinger, Ronald W.Scislowicz, Linda R.Scott, Edward L.Shafer, Mary Beth B.Shellenberger, Robert DavidSimpson, John MiltonSmith, Cynthia AnnSmith, Mary JoSowers, John B.Sparto, Patrick JosephSpector, AlexanderSquires, Stephen JohnSquires-Roehl, Barbara AnnStafford, Lori LynnStauffer, Krista MarieSteinhart, Jo AppleStitley, Judith AudreyStortz, Nancy EdwardsStyer-Acevedo, Jane L.Tarquinio, RoseThomson, William R.Trinchere, Susanne ShaheenTurner, Linda MarieVan Volkenburg, Mark DanielVanwie, Renee VolpeVeenis, Andrea Cornell & Blake ConradVerdi PatriciaVoithofer, Michelle SmithWalker, Jeannine BowenWalker, Lynetta AnnWargo, Mary Louise PollinoWeigel, Marjorie JaneWeiss, Donna RayWilloe, Maria CasteWilson, Deborah MenkWinters, Donna MarieWitt, Lynda SpottsYanco, Audrey E. RudolphYobbi, Alisha MarieYontz, Robin RadcliffZell, Jeanne Medvitz & Gerald TruxalZimmerman, Michael Anthony
Under $25Anthony, Lauren & G. D. Atkins, Leslie BillowBackstrom, Don AllenBauer, Suzanne MarieBaumgardner, Judy MarieBenedict, Barbara MurphyBlock, Ina L.Boyle, Maureen P.Brandt, Deborah SuzanneBrobst, Christopher MichaelCapristo, Anita LevoCarson, Linda RuthChitty, Gail Harmon & Alton L.Clements, Charlotte LynneClifford, Lynn CowardCounts, Gail FalkensteinCrothers, Charles J.Danley, Mary Ann S.Demarzi, Martha E.Dill, Susan M.Doster, Ellizabeth I.
DuBois, Linda CandeeFast, David MichaelFisher, James P.Fitzgerald, Lynn MaryGallaher, Lorraine JayGehenio, Nancy M.Gehringer, Jean MarieGilbert, Craig A. & Kathleen McLeighGolish, Lawrence GeorgeGowaty, Diane BethHanna, Susan PuruckerHays, Barbara Ann & Richard M.Heika, Theresa RitaHilliard, Susan L.Howe, Pamela SchlegelJones, Bethany R.Kamenski, Ruth & Robert ScottKerestan, Mark AlanKilleen, Amy MarieKopp, DonnaKoskos, Doris KoplerLasher, Marie BertonLinn, Dorothea JaneLong, Brenda K.McKinley, Peggy ArmburgerMcMinn, Patricia GouldMowry, Krista ZanettiMuller, Patricia MarzullaNewton, Barbara AnneOrpneck, Karen Miller &
Richard MichaelOrr, Victoria JoanParri, Louis JosephPepin, Gail DonahuePetrash, Evelyn GibasPierce, Frank L.Pinsky, Maryann DebelakRavnikar, John J.Rochford, Jean SwallopSaggio, Georgetta Chulick &
Anthony StephenSchaffer, Susan UberSchladenhaufen, Regis J.Shames, George H. & Joan KramerSilverman Langue, JillSmith, Kathryne KingSullivan, Claudia AnnSweany, Lyle M.Szarnicki, John RaymondVance, Janice ElizabethWeidner, Kari JoWhitney, Janet LorenZimmerman, Joseph E.
This list reflects gifts and pledges toSHRS from July 1, 2001 - June 30, 2002.Every effort was made to ensure theaccuracy of this list. If there are anyerrors or omissions, please contactKaren Khan [email protected]

America’s top 50 law schools withoutenrolling in a three-year program.They will learn how to think like alawyer and use law in their work.Participants can obtain this degree inone year full-time, or part-time overthe course of as many as four years.
The MSL-Disability Law programrequires six courses of all participants:the law of disability discrimination,constitutional law, health law & policy,introduction to law and legal reasoning, mental health law, and torts.
Students may also take courses in a wide range of relevant areas, including: child welfare law, law andeducation, elderly and the law, alternative dispute resolution, employee benefits and discrimination,workers compensation, equal protection, gender and the law, healthcare law and abuse, law and science, legislation, healthcare financing, non-profit tax exemptorganizations, foundations of legalresearch, scientific evidence, andneteracy. For further informationabout the program, contact:Professor Alan MeiselDirector Master of Studies in Law ProgramUniversity of Pittsburgh School of Law3900 Forbes AvenuePittsburgh, PA 15260
[email protected]: 412-648-1384
8
New Graduate Program
Masters ofStudies in Law
The law exerts a powerful and directimpact on the lives of persons withdisabilities. It is estimated that close to 20 percent of the U.S. population,nearly 54 million people, have a disability, with a dramatic increase inthe proportion since 1970. Peoplewith disabilities comprise one of thelargest, least employed, and most disenfranchised minority groups insociety. Universally accessible socialand physical environments willempower students, demolish barriersto employment, and increase thehealth and well-being of millions ofpeople in our society.
The University of Pittsburgh School of Law’s Masters of Studies in Law-Disability Law Concentration (MSL-Disability Law) is a unique effort to provide legal education tothose working in the administrationand provision of disabilities programs.Administrators, educators, health practitioners, advocates, social workers, architects, city planners,attorneys, and business leaders,among others, could potentially benefit from the program’s instruc-tional content.
MSL-Disability Law was conceived in concert with the School of Health and Rehabilitation Sciences to develop professionals in both law and rehabilitation with a mutual understanding of disability law. TheMSL program consists of regular lawschool courses with JD students.
Program participants will have theopportunity to study law at one of
Disabilities Law Concentration
Brian Beinecke is no stranger to hard work. As astarting linebacker on the Pittsburgh Panthers and afull-time doctoral student in the Physical Therapyprogram, he has time for little else.
Most of his day consists of adelicate balancing actbetween his duties forschool and his responsibilityto the team. Says Beinecke,“During the week, I attendclass from 8:00 a.m. tonoon. Then, I generallygrab a bite to eat and amout on the practice fieldwith the team from 2:30p.m. until 7:30 p.m. About an hour ortwo of our afternoon practice is spent studying gameplans and reviewing film, but that makes for a longday any way you cut it. After football, it’s back tostudying for class. I usually spend the duration of myevenings studying.”
To say Beinecke’s days are long is an understatement.But, he believes his commitment and discipline willpay off. “It’s hard to juggle the course load of a doctoral program and everything involved with football,” admits Beinecke. “But you will never getbetter at anything without hard work, and that’s howI approach everything I do.”
This approach to academics and sports is nothingnew, though, for Beinecke. He earned an undergraduate degree in exercise science in threeand a half years with a solid 3.3 grade point average.During two of those years he was also sharing starting duties for the Panthers. Beinecke has beenengaged in this balancing act for much of his post-high school career.
Even with a tight schedule and a heavy workload,Beinecke has no regrets. He explains, “This wholeexperience will prepare me for my career and forthe rest of my life. I’m just happy that I’ve been having a lot of fun along the way.”
Beinecke plans to use his gridiron experience evenafter his playing days are over. His focus will be foot-ball-related injuries. Says Beinecke, with confidenceand pride, “I hope to give back to football all that ithas given to me and more. And I’d like to continuebeing part of the Panther organization even after myplaying days are over.”
Brian Beinecke Works Hard On and Off the Field
PANTHERPRIDE

I n our recent undergraduate brochure, wedescribed the disciplines within the School of Health and Rehabilitation Sciences as
“real science helping real people.”While the focus on the compassionatecare embodied in our professions isapt, hidden within this feel-goodphrase is the kernel of a problemthat may have a deleterious effect onour future. Namely, that those students drawn to helping professions like audiology, speech-language pathology, andoccupational therapy, prefer theclinical to the empirical. And as a result, theresearch ranks within the professions are growingfrighteningly thin.
Dr. Malcolm (Mick) McNeil, Chair of theDepartment of Communication Science andDisorders, is on the Executive Board of theCouncil of Academic Programs in CommunicationScience and Disorders. This organization isdirecting a substantive portion of its researchefforts to uncovering the extent of the problemand to identify possible solutions. I’ve asked Dr. McNeil to share his perspective.
There is a great deal to like about being a professor. You teachbright and interesting people. You research important topics thatare largely under your selection and your control. You serve as arole model for the next generation of professionals.
But recently, I’ve been questioning just how good a role modelI’ve been. Not that I’ve doubted the efficacy of my classroom styleor research methods. I’ve certainly had my share of extramuralfunding and our program continues to draw some of the top students in the country. But why, I’ve asked myself, don’t my students want to follow in my footsteps? Why don’t they want tobe professors?
My colleagues around the country have been conducting similarself-examinations. It’s been the primary topic of conversation atmore than one national conference. And while there have been anumber of theories thrown about, no clear answer has emerged.
Part of the problem is the personality of our students. They enter the field because they want to help people. They want to applyknowledge rather than expand the profession’s knowledge base. We recently surveyed several consecutive classes of about 35 graduate students each as to their future plans. In each class,only one or two have indicated an interest in pursuing a researchPh.D. A clinical doctorate was the first choice for 80 percent of the respondents.
As highly trained practitioners, the graduates of clinical doctoralprograms will be consummate consumers of research and they will advance the translation of research to direct patient care. But with everyone working clinically, there are few persons trainedin the discipline to advance the science. How will we know more tomorrow than we do today?
One answer to the problem may be found overseas. Brazil, forexample, has a fairly sophisticated communication science and disorders program at the Universidade Federal De São Paulo and a potentially large supply of interested scientists. We’re exploringthe possibility of creating a joint doctoral program. Australiaalready competes successfully with us. There’s certainly a pent-up
demand in Asia, where, for example, one speech pathology training program supplies professionals for 270 million people. Recruitinginternationally could be a viable option.
But there is a potential downside. By lookingabroad for the next generation of teachers andresearchers, the U.S. runs the risk of losing itsleadership position. Without the empirical, audiology and speech pathology could becomelittle more than service fields. And, if this occurs,we could lose the professional autonomy that
stands as a centerpiece of the professions and as a pillar of evidence-based clinical practice and service delivery.
I don’t want to appear to be an alarmist. The scenario that I paintedhas not occurred overnight and it will not be brought to crisis proportions overnight. Discussion of methods and plans for diverting this projection are under way nationally. In fact, there aresigns for optimism. Right now we have been able to recruit well-qualified students to assemble one of the largest research doctoralprograms in the country. An increase in extramural research dollars supports this research mission and the recruitment of a critical mass of doctoral students in several laboratories contributesto the production of new knowledge and to an exciting and effectiveeducational atmosphere.
But if the projections hold true, a crisis is inevitable. Not just inaudiology and speech pathology, but it is likely to occur in other disciplines such as occupational therapy and physical therapy aswell. If we are to have next generation expertise, then we mustmimic the medical profession by providing well-trained doctorallevel practitioners and abundant researchers creating new knowledge and evidence-based practice. We must infuse the professorate with high status. And high pay.
We’d like to hear your reaction to this column. E-mail your comments to Karen Khan at [email protected]. They will be printed as space allows.
ACCESSD r . K a t e S e e l m a n
Administration
Malcom (Mick)McNeil
Kate Seelman
12

points to the business plans that each department head mustsubmit annually as an example of Brubaker’s ability “to thinkoutside the box.”
He credits Brubaker and his team for recognizing what hedescribes as “a totally different paradigm for the treatment of
people with disabilities.” This, he says, has fueled an influx ofresearch dollars into the school. “They are staying on top ofthe issues. They are perfectly in tune with the changing natureof the profession.”
Kuzneski describes the role of the Board of Visitors as bothconsultant and advocate. “We provide advice and insight onthe school’s planning efforts and offer candid, comprehensive,and informed reaction to the school’s educational objectivesand programs,” he explains. “We also play a major communications role. Internally, we are a link between theschool and the university’s senior administration. Externally,we’re SHRS ambassadors.” He applauds the efforts of his fellow board members. “They are outstanding,” he enthuses.“They are wonderful people.”
Kuzneski says that his tenure at the helm of the Board of Visitors has given him “ a respect and appreciation for a fieldin which he had no experience. We are helping people whoneed special help. It is a service to society that is unique. It’s an honor to serve.”
TTeeaammLLeeaaddeerr
Board of Visitors Chair Andy Kuzneski Says SHRS Fielding a Winning Team
“We are helping people who need special help.
It is a service to society that is unique.”
13
WOver 40 years ago, a University of Pittsburgh footballscholarship financed Andrew J. “Andy” Kuzneski’scollege education. He’s been repaying that
scholarship ever since. He is past president of both the Golden Panthers and the Alumni Association. He is a member of the university’s Board of Trustees. He is NationalChair of the regional capital campaign. And he is also Chair of the SHRS Board of Visitors.
One of five sons of an Indiana Countypotato farmer, Kuzneski spent hiscollege years lined up alongside thelegendary Mike Ditka. But Kuzneskipoints out that Ditka’s “Iron Mike”nickname is a misnomer. “I hadmore playing time than he did, ” hesays with a grin. But unlike Ditka, Kuzneski did not pursue a professional football career following graduation, optinginstead to return to his hometown, where in 1965 he startedthe employee benefit and financial planning agency that bearshis name. “The football scholarship,” he says, “was the catalyst for my success in the business world.”
While Kuzneski exudes a “can do” attitude, he admits to having some reservations when Chancellor Mark Nordenbergasked him to chair the SHRS board. “I reminded him that I had no medical background,” he relates. But he agreed tomeet with Dean Cliff Brubaker to discuss the position.
“The first thing I said to him was ‘Dean, I’m not a doctor,”remembers Kuzneski. “And he replied, ‘Andy, neither am I.’From that day on, we’ve had a wonderful relationship.”
Kuzneski asserts that under the leadership of Dean Brubaker,the school has undergone “a complete renaissance. He is aprofessor, a researcher, and an administrator. He has all theskills necessary to move the school forward. And,” he adds,“he can motivate people. He is like a football coach. He getsthem to work together as a team, to work cohesively.” He
Andy Kuzneski

Nonprofit Org.U.S. Postage
PAIDPittsburgh, PA
Permit No. 511
University of PittsburghSchool of Health and Rehabilitation Sciences4031 Forbes TowerPittsburgh, Pennsylvania 15260
Change Service Requested
A Gift to SHRS isa Sound Investment.
To hear why . . . Contact: Karen Khan Director of Development 412-383-6548 [email protected]
The Latest In Hearing Aid Technology Circa 1940Central Institute for the Deaf
Bernard Becker Medical Library, Washington University.
It’s
real
science
helping real
people.
s h r s

20
ListeningCarefully for
the CluesDiscovering the Factors
Behind Childhood Communication Disorders
Everything can change in the blink of aneye. A child, once happy, verbal, andvibrant, can become non-communicative
or unintelligible in an instant when serious headtrauma strikes.
Fortunately, due to groundbreaking work at theCenter for Research on Acquired and NeurologicCommunication Disorders in Children – a jointventure between the School of Health andRehabilitation Sciences and Children’s Hospitalof Pittsburgh – there is a growing pool of knowledge that will hopefully unlock the mysteries of childhood communication disorders resulting from traumatic brain injury and other neurological deficits.
“The mission of the Center is to conductresearch on the underlying processes associated with children who have acquiredand neurological communication disorders,”observes Tom Campbell, Associate Professorand Director of the Department of Audiologyand Communication Disorders and the Program Director of the Center. “We also concentrate our efforts on children who haven’t experienced head injuries but haveacquired a neurological problem that impactstheir ability to communicate.”
Funded by grants provided through the NationalInstitute on Deafness and Other CommunicationDisorders, Campbell and his combined teamfrom SHRS and Children’s have been workingtogether for close to seven years.
“This partnership provides excellent opportunities for SHRS students to participate in significant research into pediatric communication disorders,” commentsCampbell. “We currently have three majorstudies underway – one that studies the recovery of speech skills after severe traumaticbrain injury, another that’s focused on the physiological development of speech production,and a third that concerns itself with genetic factors that contribute to severe speech-soundproduction disorders in children. All threestudies offer SHRS students opportunities towork with some of the leading researchers and clinicians in the country, as well as with the children who need our help in overcomingthese serious communications conditions.”
Communication Science and Disorders
Reflectors are used to measure movement coordination of the lips in both infants and pre-schoolers.
21
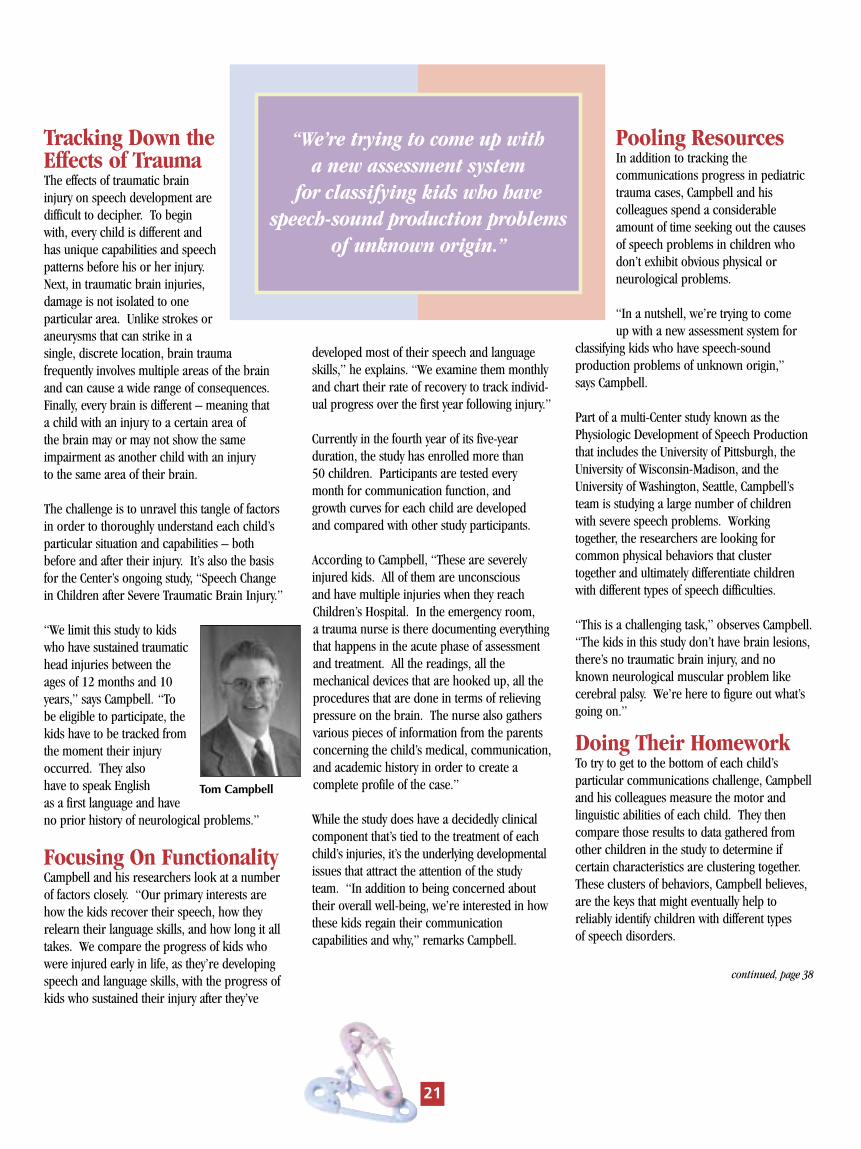
Pooling ResourcesIn addition to tracking the communications progress in pediatrictrauma cases, Campbell and his colleagues spend a considerableamount of time seeking out the causesof speech problems in children whodon’t exhibit obvious physical or neurological problems.
“In a nutshell, we’re trying to come up with a new assessment system for
classifying kids who have speech-sound production problems of unknown origin,” says Campbell.
Part of a multi-Center study known as thePhysiologic Development of Speech Productionthat includes the University of Pittsburgh, theUniversity of Wisconsin-Madison, and theUniversity of Washington, Seattle, Campbell’steam is studying a large number of childrenwith severe speech problems. Working together, the researchers are looking for common physical behaviors that cluster together and ultimately differentiate childrenwith different types of speech difficulties.
“This is a challenging task,” observes Campbell.“The kids in this study don’t have brain lesions,there’s no traumatic brain injury, and no known neurological muscular problem likecerebral palsy. We’re here to figure out what’sgoing on.”
Doing Their HomeworkTo try to get to the bottom of each child’s particular communications challenge, Campbelland his colleagues measure the motor and linguistic abilities of each child. They thencompare those results to data gathered fromother children in the study to determine if certain characteristics are clustering together.These clusters of behaviors, Campbell believes,are the keys that might eventually help to reliably identify children with different types of speech disorders.
Tracking Down theEffects of TraumaThe effects of traumatic braininjury on speech development aredifficult to decipher. To beginwith, every child is different andhas unique capabilities and speechpatterns before his or her injury.Next, in traumatic brain injuries,damage is not isolated to one particular area. Unlike strokes oraneurysms that can strike in a single, discrete location, brain trauma frequently involves multiple areas of the brainand can cause a wide range of consequences.Finally, every brain is different – meaning that a child with an injury to a certain area of the brain may or may not show the same impairment as another child with an injury to the same area of their brain.
The challenge is to unravel this tangle of factorsin order to thoroughly understand each child’sparticular situation and capabilities – bothbefore and after their injury. It’s also the basisfor the Center’s ongoing study, “Speech Changein Children after Severe Traumatic Brain Injury.”
“We limit this study to kidswho have sustained traumatichead injuries between theages of 12 months and 10years,” says Campbell. “Tobe eligible to participate, thekids have to be tracked fromthe moment their injuryoccurred. They also have to speak English as a first language and haveno prior history of neurological problems.”
Focusing On FunctionalityCampbell and his researchers look at a numberof factors closely. “Our primary interests arehow the kids recover their speech, how theyrelearn their language skills, and how long it alltakes. We compare the progress of kids whowere injured early in life, as they’re developingspeech and language skills, with the progress ofkids who sustained their injury after they’ve
developed most of their speech and languageskills,” he explains. “We examine them monthlyand chart their rate of recovery to track individ-ual progress over the first year following injury.”
Currently in the fourth year of its five-year duration, the study has enrolled more than 50 children. Participants are tested everymonth for communication function, and growth curves for each child are developed and compared with other study participants.
According to Campbell, “These are severelyinjured kids. All of them are unconscious and have multiple injuries when they reachChildren’s Hospital. In the emergency room, a trauma nurse is there documenting everythingthat happens in the acute phase of assessmentand treatment. All the readings, all the mechanical devices that are hooked up, all theprocedures that are done in terms of relievingpressure on the brain. The nurse also gathersvarious pieces of information from the parentsconcerning the child’s medical, communication,and academic history in order to create a complete profile of the case.”
While the study does have a decidedly clinicalcomponent that’s tied to the treatment of eachchild’s injuries, it’s the underlying developmentalissues that attract the attention of the studyteam. “In addition to being concerned abouttheir overall well-being, we’re interested in howthese kids regain their communication capabilities and why,” remarks Campbell.
Tom Campbell
continued, page 38
“We’re trying to come up with a new assessment system
for classifying kids who have speech-sound production problems
of unknown origin.”

38
To take the measurements, each child is connected to instrumentation that measuresthe movement of their rib cage and their larynx, as well as the airflow through theirnose. These readings are captured by theequipment and analyzed by a sophisticatedcomputer system that sorts and categorizesthe data. In the long run, Campbell wouldlike to determine whether children with specific clusters of behaviors respond morefavorably to treatment. To gather data for thestudy, Campbell and his colleagues will betesting 300 children over the next five years –240 with speech disorders and 60 with normal speech skills.
“If you know that speech problems beganwith a traumatic brain injury, you at leastknow what the cause was,” observesCampbell. “With kids that have no knownneurological problems or obvious physicalimpairments, pinpointing what’s going on can be extremely challenging. We’re buildinga baseline for comparison that will provideresearchers – and later on, practitioners –with a place to start untangling the mystery ofeach child’s speech production difficulties.”
Getting A Handle OnGeneticsWhile traumatic injuries and speech production problems from unknown sourcescomprise significant segments of the Center’swork, genetic research rounds out theresearch agenda.
According to Campbell, “We think that genetics, particularly in kids who don’t haveany other obvious problems, could be a significant factor in the speech deficits ofthese children. However, we don’t think it’s a simple, single-gene issue that causes theseproblems. Combinations of factors, includingenvironmental and sociodemographic variables, can put some kids at high risk forspeech disorders. Right now, we’re trying
to determine what those combinations are.Down the road, we’re hoping to discover howto respond to them most effectively.”
To support this research, a third study,Molecular Genetics of Apraxia of Speech inChildren, is being conducted by the Center.Apraxia of Speech (AOS) is a condition thatimpairs the motor planning that is necessaryfor speech production. Recent studies haveshown that this disorder tends to run in families. While the origin of apraxia isunknown, some researchers believe that theunderlying cause of AOS may involve geneticpredisposition to some degree.
Campbell’s team is building on that hypothesisand has recruited 50 families with childrenafflicted with AOS to participate in the study.The children have been carefully analyzed inthe Center’s lab, and DNA samples have beengathered from both the children and theirparents. The DNA material is currently beinganalyzed for genetic markers that are associ-ated with this speech disorder.
“Hopefully, we’ll get some insights into thiscomplicated disorder that will help guide our future assessment and treatment efforts,” says Campbell.
Comparing Notes“There’s a great deal of crossover between the three studies in the Center,” observesCampbell. “In all three research initiatives,we’re trying to untangle the factors that could be underlying causes of the variouscommunication conditions. We’re alsoattempting to develop procedures to reliablyclassify these kids, determine what kind ofspeech disorder they have, as well as gainsome insight into the underlying mechanismsassociated with these speech disorders.
The studies are also providing the team withinsights into what triggers certain conditions.“Down the road, it’s my hope that we’ll drawsome solid conclusions that will translate intoeffective treatments on the clinical side,” sumsup Campbell. “The only way to effectivelytreat children with severe speech disorders is to understand the potential causes.”
For more information, contact Tom Campbellat [email protected]
continued from page 21C a l e n d a r
o fE v e n t s
N o v e m b e r
November 1-2: Continuing Education
Workshop – “Ergonomic Assessment and
Risk Prevention.” Presenter: Nancy Baker,
ScD, OTR/L. Sponsored by the Department
of Occupational Therapy.
November 2: Host site for the Mayo
Clinic 13th Annual Audiology
Videoconference. 10 a.m. – 4:30 p.m.
Call Tim Lucas at 412-383-6542.
November 12: Eighth Annual Endowed
Scully Visiting Lecture Program. Speaker:
Shirley Sahrmann, Ph.D., PT, FAPTA.
Reception at 6:30 p.m. followed by
lecture at 7 p.m. in the William Pitt
Union Ballroom.
F e b r u a r y
February 6-7: Tools and The Talents
Conference 2003. Sponsored by the
Department of Emergency Medicine. For
more information, contact Deb Lenart at
ListeningCarefully for
the Clues

Eiman Al-Jafar, Department of HealthInformation Management, defended herdissertation, “Factors Affecting Diffusion ofthe Electronic Medical Record (EMR) froma Physician’s Perspective,” becoming thefirst doctoral student graduated by thedepartment.
Denise Chisholm, Erica Kopcha, AmyKurowski, Tamara Mills, and ElizabethSkidmore, Department of OccupationalTherapy, were selected to participate in theJewish Healthcare Foundation/CoroPittsburgh Health Sciences Fellowship.
Diane Collins, Department ofRehabilitation Science and Technology, hasreceived a VA Pre-Doctoral AssociatedHealth Rehabilitation Research Fellowship.
Christopher Scialabba, Department ofHealth Information Management, wasawarded the New Economy TechnologyScholarship (NETS).
Tepanta Fossett, Department ofCommunication Science and Disorders, hasreceived a National Institutes of Health F 31Minority Pre-Doctoral Fellowship.
Eric Wallis, Department of HealthInformation Management, was selected bythe Pennsylvania Health InformationManagement Association (PHIMA) toreceive its 2002 Student Scholarship Award.
C L A S S A C T S
Cooper Wins Olin E. Teague Award
9
Faculty, Alumni, and Students
The Teague Award, named for the late longtime chairman of the U.S. HouseCommittee on Veterans Affairs, honors anemployee of the Department of VeteransAffairs who makes exemplary contributionstoward improving the lives of war-injuredveterans. Cooper is Director of the VAPittsburgh Healthcare System’s NationalCenter of Excellence for Wheelchair andRelated Technology and is a VA SeniorCareer Research Scientist.
Cooper, who is acknowledged as one of theworld’s foremost authorities in wheelchairdesign and technology, was recognized forhis major contributions to the treatmentand rehabilitation of paralyzed individuals,particularly in the design of modern manual and electric-powered wheelchairsand the development and implementation ofwheelchair standards. Thanks to his work,thousands of individuals who use wheel-chairs now have access to higher qualitywheelchairs.
Dr. Rory A. Cooper, Professor and Chair,Department of Rehabilitation Science andTechnology, was awarded the prestigious Olin E. Teague award at a special ceremony in Washington, DC on September 18.
Dr. Rory Cooper (l) receives his award fromThe Honorable Leo S. Mackay, Jr., DeputySecretary of Veterans Affairs
Left to right
Dr. Bob Chen, Assistant Professor, The Hong Kong Polytechnic University
Dr. Clifford E. Brubaker, Professor and Dean, SHRS
Dr. Christina W. Y. Hui-Chan,Chair of Rehabilitation Sciences, Head of Department of Rehabilitation Sciences, The Hong Kong Polytechnic University
Ms. Amy Fu, Assistant Professor, The Hong Kong Polytechnic University
10
Faculty News
Dr. Mervat Abdelhak, Associate Professor and Chair, Department of Health InformationManagement, has been invited to be a member ofthe peer review panel reviewing grant applicationsfor the U.S. Department of Health and HumanServices, Health Resources and Administration.She is also serving as a reviewer for the ScientificPeer Advisory and Review Services Division of theAmerican Institute of Biological Sciences.
Dr. Nancy Baker, Assistant Professor, Departmentof Occupational Therapy, had an article publishedin Work titled, “The Association Between Children’sComputer Use and Musculoskeletal Discomfort.”Baker also has received grants to develop aninstrument to measure personal typing style and to test the use of an ergonomic keyboard.
Carmela Battaglia, Assistant Professor,Department of Occupational Therapy, conducteddisability awareness sessions at the YWCA SummerCamp and at Camp Cadet, which is operated by thePennsylvania State Police. She was assisted bythree students from the second year class, ElaineHolt, Amy Kurowski, and JessicaPuzausky.
Dr. Cliff BrubakerProfessor and Dean,School of Health andRehabilitationSciences, is co-authorof “The Six SigmaBook for Healthcare:Improving Outcomes byReducing Errors.”
The Center for Assistive Technology (CAT) hasreceived the UPMC DSI (Diversified Services Inc.)President’s Award for Quality Improvement. TheCAT was recognized for its Power Wheelchair LeaseProgram for people with terminal diseases who areon the UPMC Health Plan.
Denise Chisholm, Assistant Professor, Department of Occupational Therapy, was elected a Pennsylvania representative to the RepresentativeAssembly of the American Occupational Therapy Association.
Dr. Ellen Cohn, Assistant Professor, Departmentof Communication Science and Disorders, andDirector of Instructional Development, is an initialrecipient of the University of Pittsburgh CareerServices “Faculty Partners” award, honoring thosefaculty members who have demonstrated a consistently high level of interest in their students’career goals.
Laura Cohn, Research Associate, Department of Rehabilitation Science and Technology, has been named a member of the editorial board ofThe Journal of Assistive Technology.
Dr. Al Condeluci, Adjunct Professor, has published, “Cultural Shifting: CommunityLeadership and Change.” The book, his fourth,explores ways and means that new ideas, products, or people can be incorporated into the greater mix of the community. Condeluci isalso chief executive officer of United Cerebral Palsy of Pittsburgh.
Dr. Rory Cooper, Professor and Chair,Department of Rehabilitation Science andTechnology, has been recognized as a 2002 Fellow and Mentor by the RehabilitationEngineering and Assistive Technology Society of North America (RESNA). He is also the new president-elect of the organization. Cooper hasalso been named to the National Advisory Board on Medical Rehabilitation Research, the NationalInstitute of Child Health and Human Development.
Dr. Mary Jo Geyer, Visiting Assistant Professor,Department of Rehabilitation Science andTechnology, has been elected to the Board ofDirectors of the National Pressure Ulcer Advisory Panel.
Dr. Malcolm McNeil, Professor and Chair,Department of Communication Science andDisorders, has been elected for a second, two-year term as Treasurer and Executive BoardMember of the Council of Academic Programs in Communication Science and Disorders.
It’s easy to share your good news about a newjob, a promotion, or an honor or award. Simply e-mail the information to Karen Khan at [email protected] and we’ll include it in the “Yearbook” section as space allows.
?What’sNew
Newa n d N o t e w o r t h y Dr. Catherine Palmer, Associate Professor,
Department of Communication Science andDisorders, will investigate the new AdaptiveDirectional Microphone Technology for Siemens, Inc.
Dr. Joan Rogers, Professor and Chair, and Dr. Margo Holm, Professor, Department ofOccupational Therapy, received a grant from theNational Institute for Disability and RehabilitationResearch to investigate a health promotion intervention for adults with fibromyalgia.
Dr. Kate Seelman was elected to the RESNABoard of Directors and has been appointed an “at large” member of the RESNA ExecutiveCommittee. She also has been asked to serve as aEUCLID Center Auxiliary Faculty member as well asa pro bono consultant to the FISA Foundation.Seelman delivered the keynote address at thePennsylvania Association of Rehabilitation Facilitiesannual conference.
Elizabeth Skidmore, Research Associate,Department of Occupational Therapy, presentedlectures on constraint-induced movement therapyat Peterson Rehabilitation Hospital and GeriatricCenter, Wheeling, WV, and Forum Health Care,Warren, OH.
Dr. Walt Stoy, Program Director, EmergencyMedicine, has been elected to the University Senate.
Dr. Connie Tompkins, Professor, Department of Communication Science and Disorders, was the keynote speaker at the 2002 European Aphasia Conference in Zeist, the Netherlands, theFlorida Association for Language, Speech, andHearing, and the Wyoming Speech-Language-Hearing Association.

Says Mizak, “The experience was a wonderfulopportunity to apply what I had learned in theclassroom in a clinical setting. As rehabilitationcounselors, we’re taught to work with clients as a team examining challenges to developworkable solutions. This was the perfect opportunity to turn theory into practice, and in the process, help someone to grow theirbusiness.”
Having earned an undergraduatedegree in business, Mizak usedher background as a businesscoach while incorporating her knowledge of assistive technology to conduct clientassessments in computeraccess. “I could add value tothe Practicum on a businessdevelopment level, but therewas also an assistive technologyelement that I could bring tothe experience,” she relates.
“One woman that I worked with in-depth hadcerebral palsy, with very limited use of herhands. But she operated a greeting card designcompany and needed to use a computer. Shecouldn’t use a traditional mouse, so we triedout various assistive technology options, allowing the client to choose the option thatworked best for her. In this case, it was anadaptive joystick.”
A Community OfN e i g h b o r s
Based on her work, Mizak compiled aFrequently Asked Questions section in the organization’s help manual pertaining to assistive technology. It will help access assistivetechnology information quickly.
Even now that his Practicum is over, Marchiondacontinues to work with a client, helping himaddress issues regarding accessing information.
“The gentleman I worked with has becomeinvolved in a tutoring program, where he willact as a conversationalist for individuals whoare learning English as a second language,”explains Marchionda. “Working Order suggestedI meet this gentleman to determine if I couldoffer any suggestions that would allow him tobetter access information, whether it be in
written form, or via hiscomputer. As a result ofhis MS, he has difficultypicking up a book toread about subjects hemay want to learn moreabout. Our goal was to identify solutions that would allow for an easier system toaccess knowledge. We identified a variety of options for him,including a reorganiza-tion of his workspace
and desktop computer, along with simple technologies such as audio books and videocassettes.”
Adds Marchionda, “Solutions to problems withaccess to information almost always exist, andthere are usually a variety of ways to overcomeobstacles. In many, if not most, cases it’s theperson with a disability who identifies the solution, and as a counselor, you can only hopeto help in facilitating a successful or satisfactoryend result.”
And the benefits go both ways. Says Mizak, “I knew I’d never forget the experience whenmy client gave me a card she had made thanking me for my help. That gesture saidmore to me than any words ever could.”
To learn more about Working Order, contactSusan Chase at 412-782-5344.
Graduate degree practicumsoffer the opportunity for
students to apply the lessonslearned in the classroom to reallife situations. The students gainexperience and confidence whilethe organizations with whichthey partner get hands-on helpfrom the next generation of professionals.
Nancy Mizak and Chris Marchionda, both master’s students in Rehabilitation Science andTechnology with a focus on rehabilitation counseling, recently completed an AssistiveTechnology Practicum. Only what they gainedproved to be more than graduate credits andon-the-job experience. They gained friends –and memories – that will last a lifetime.
Mizak’s Assistive Technology Practicum wasarranged with Working Order, a local nonprofitincubator for entrepreneurs, most of whomhave disabilities. The organization offers itsclients shared office space, technical training,and one-on-one coaching. Marchionda, whohad recently completed a Practicum, had been encouraged to meet with staff and entrepreneurs to further his experience.
’90sKristie Spencer – CSD ’92, is an AssistantProfessor of Speech and Hearing Sciences atthe University of Washington in Seattle.
Dr. Margaret Lehman Blake – CSD ’99, is an Assistant Professor of Communication Disordersat the University of Houston, Texas.
In MemoriamMichelle Fecko Tomaro PT ’83Jean Crothers Welles HRP ’80
YYEEAARRBBOOOOKK
What they gained
proved to be
more than
graduate credits
and on-the-job
experience.

14
Summer inAmerica
Dr. Lucas van der Woude has worked in the fieldof wheeled mobility for 20 years, almost exclu-sively in Europe and with colleagues at TheInstitute for Fundamental and Clinical HumanMovement Sciences at theVrije Universiteit inAmsterdam. When hedecided on a sabbaticalabroad, he was lookingfor a fresh perspectivethat would enhance his work in humanmovement sciences and ergonomics. Hewanted a chance to evaluate his own position and discovernew ways of doingresearch. So he carefullyfit his sabbatical betweenteaching and researchobligations inAmsterdam, leaving him a window from June to October which hecould spend doing whathe does the rest of theyear – researching andteaching about wheeledmobility.
According to van der Woude, there was only oneplace in the world where he could find researchon a caliber with his Amsterdam program, andthat place was the Department of Rehabilitation
Science and Technology chaired byDr. Rory Cooper.
“My group in Amsterdam approachesthe field from a biological perspective. We look primarily at human systems – the physiology,biomechanics, and even psychologyof how an individual interacts withassistive technology,” says van derWoude. “In Pittsburgh, there is amuch stronger focus on the engineering aspect of wheeledmobility – how the design engineercan improve the assistive technologyfor the human system.”
He adds, “The engineering perspective is more outcome-oriented. In Amsterdam, the focus is on theory and understanding.Here, it extends the understandingtoward innovation of new technologies and therapies. The research focus is really on solving problems.”
The National Veterans Wheelchair Games, heldthis year in Cleveland, offered van der Woude a practical perspective on outcome-basedresearch. In fact, no fewer than four ongoingresearch projects collected data on almost 80 subjects at the Games, which were founded nearly 20 years ago to highlight the athletic abilities of paralyzed veterans.
One project involved evaluatingthe effects of different floor surfaces on wheelchair propulsion. “There is not a lot of material that gives us aclear picture of strain caused by floor surface, and the Games gave us good data and answered many questions.Perhaps a paper will be forthcoming,” notes van der Woude.
Van der Woude observes that in the field of academic research, groups who are not collaborating consider themselves competitors. “I hope that when I leave here I have been able to transfer some of the deepunderstanding of the Amsterdam group to myAmerican colleagues, but also that I will be ableto take the important perspective of problemsolving back to my colleagues in theNetherlands. Collaboration was the true outcome of this visit.”
For van der Woude, the point of all the work –the collaboration, research, study and teaching– is simple and universal. The end result contributes to the well-being of others.
★
A Pittsburgh Sabbatical for Dr. Lucas van der Woude
“The research focus is really on
solving problems.”
“Collaboration was the
true outcome of this visit.”

Says Mizak, “The experience was a wonderfulopportunity to apply what I had learned in theclassroom in a clinical setting. As rehabilitationcounselors, we’re taught to work with clients as a team examining challenges to developworkable solutions. This was the perfect opportunity to turn theory into practice, and in the process, help someone to grow theirbusiness.”
Having earned an undergraduatedegree in business, Mizak usedher background as a businesscoach while incorporating her knowledge of assistive technology to conduct clientassessments in computeraccess. “I could add value tothe Practicum on a businessdevelopment level, but therewas also an assistive technologyelement that I could bring tothe experience,” she relates.
“One woman that I worked with in-depth hadcerebral palsy, with very limited use of herhands. But she operated a greeting card designcompany and needed to use a computer. Shecouldn’t use a traditional mouse, so we triedout various assistive technology options, allowing the client to choose the option thatworked best for her. In this case, it was anadaptive joystick.”
A Community OfN e i g h b o r s
Based on her work, Mizak compiled aFrequently Asked Questions section in the organization’s help manual pertaining to assistive technology. It will help access assistivetechnology information quickly.
Even now that his Practicum is over, Marchiondacontinues to work with a client, helping himaddress issues regarding accessing information.
“The gentleman I worked with has becomeinvolved in a tutoring program, where he willact as a conversationalist for individuals whoare learning English as a second language,”explains Marchionda. “Working Order suggestedI meet this gentleman to determine if I couldoffer any suggestions that would allow him tobetter access information, whether it be in
written form, or via hiscomputer. As a result ofhis MS, he has difficultypicking up a book toread about subjects hemay want to learn moreabout. Our goal was to identify solutions that would allow for an easier system toaccess knowledge. We identified a variety of options for him,including a reorganiza-tion of his workspace
and desktop computer, along with simple technologies such as audio books and videocassettes.”
Adds Marchionda, “Solutions to problems withaccess to information almost always exist, andthere are usually a variety of ways to overcomeobstacles. In many, if not most, cases it’s theperson with a disability who identifies the solution, and as a counselor, you can only hopeto help in facilitating a successful or satisfactoryend result.”
And the benefits go both ways. Says Mizak, “I knew I’d never forget the experience whenmy client gave me a card she had made thanking me for my help. That gesture saidmore to me than any words ever could.”
To learn more about Working Order, contactSusan Chase at 412-782-5344.
Graduate degree practicumsoffer the opportunity for
students to apply the lessonslearned in the classroom to reallife situations. The students gainexperience and confidence whilethe organizations with whichthey partner get hands-on helpfrom the next generation of professionals.
Nancy Mizak and Chris Marchionda, both master’s students in Rehabilitation Science andTechnology with a focus on rehabilitation counseling, recently completed an AssistiveTechnology Practicum. Only what they gainedproved to be more than graduate credits andon-the-job experience. They gained friends –and memories – that will last a lifetime.
Mizak’s Assistive Technology Practicum wasarranged with Working Order, a local nonprofitincubator for entrepreneurs, most of whomhave disabilities. The organization offers itsclients shared office space, technical training,and one-on-one coaching. Marchionda, whohad recently completed a Practicum, had been encouraged to meet with staff and entrepreneurs to further his experience.
’90sKristie Spencer – CSD ’92, is an AssistantProfessor of Speech and Hearing Sciences atthe University of Washington in Seattle.
Dr. Margaret Lehman Blake – CSD ’99, is an Assistant Professor of Communication Disordersat the University of Houston, Texas.
In MemoriamMichelle Fecko Tomaro PT ’83Jean Crothers Welles HRP ’80
YYEEAARRBBOOOOKK
What they gained
proved to be
more than
graduate credits
and on-the-job
experience.

14
Summer inAmerica
Dr. Lucas van der Woude has worked in the fieldof wheeled mobility for 20 years, almost exclu-sively in Europe and with colleagues at TheInstitute for Fundamental and Clinical HumanMovement Sciences at theVrije Universiteit inAmsterdam. When hedecided on a sabbaticalabroad, he was lookingfor a fresh perspectivethat would enhance his work in humanmovement sciences and ergonomics. Hewanted a chance to evaluate his own position and discovernew ways of doingresearch. So he carefullyfit his sabbatical betweenteaching and researchobligations inAmsterdam, leaving him a window from June to October which hecould spend doing whathe does the rest of theyear – researching andteaching about wheeledmobility.
According to van der Woude, there was only oneplace in the world where he could find researchon a caliber with his Amsterdam program, andthat place was the Department of Rehabilitation
Science and Technology chaired byDr. Rory Cooper.
“My group in Amsterdam approachesthe field from a biological perspective. We look primarily at human systems – the physiology,biomechanics, and even psychologyof how an individual interacts withassistive technology,” says van derWoude. “In Pittsburgh, there is amuch stronger focus on the engineering aspect of wheeledmobility – how the design engineercan improve the assistive technologyfor the human system.”
He adds, “The engineering perspective is more outcome-oriented. In Amsterdam, the focus is on theory and understanding.Here, it extends the understandingtoward innovation of new technologies and therapies. The research focus is really on solving problems.”
The National Veterans Wheelchair Games, heldthis year in Cleveland, offered van der Woude a practical perspective on outcome-basedresearch. In fact, no fewer than four ongoingresearch projects collected data on almost 80 subjects at the Games, which were founded nearly 20 years ago to highlight the athletic abilities of paralyzed veterans.
One project involved evaluatingthe effects of different floor surfaces on wheelchair propulsion. “There is not a lot of material that gives us aclear picture of strain caused by floor surface, and the Games gave us good data and answered many questions.Perhaps a paper will be forthcoming,” notes van der Woude.
Van der Woude observes that in the field of academic research, groups who are not collaborating consider themselves competitors. “I hope that when I leave here I have been able to transfer some of the deepunderstanding of the Amsterdam group to myAmerican colleagues, but also that I will be ableto take the important perspective of problemsolving back to my colleagues in theNetherlands. Collaboration was the true outcome of this visit.”
For van der Woude, the point of all the work –the collaboration, research, study and teaching– is simple and universal. The end result contributes to the well-being of others.
★
A Pittsburgh Sabbatical for Dr. Lucas van der Woude
“The research focus is really on
solving problems.”
“Collaboration was the
true outcome of this visit.”
The RealWorld
The Challenges andRewards of Clinical
Educationin Athletic Training
They’ve sat
through hundreds
of hours of
lectures. They’ve
pored through
dozens of
textbooks. Now
comes the time
to put that
knowledge to
work. To move
from the didactic
to the clinical.
In each issue of
FACETS, we follow
first and second
year students as
they get their
first taste of being
a professional.
I n s i d e L o o k
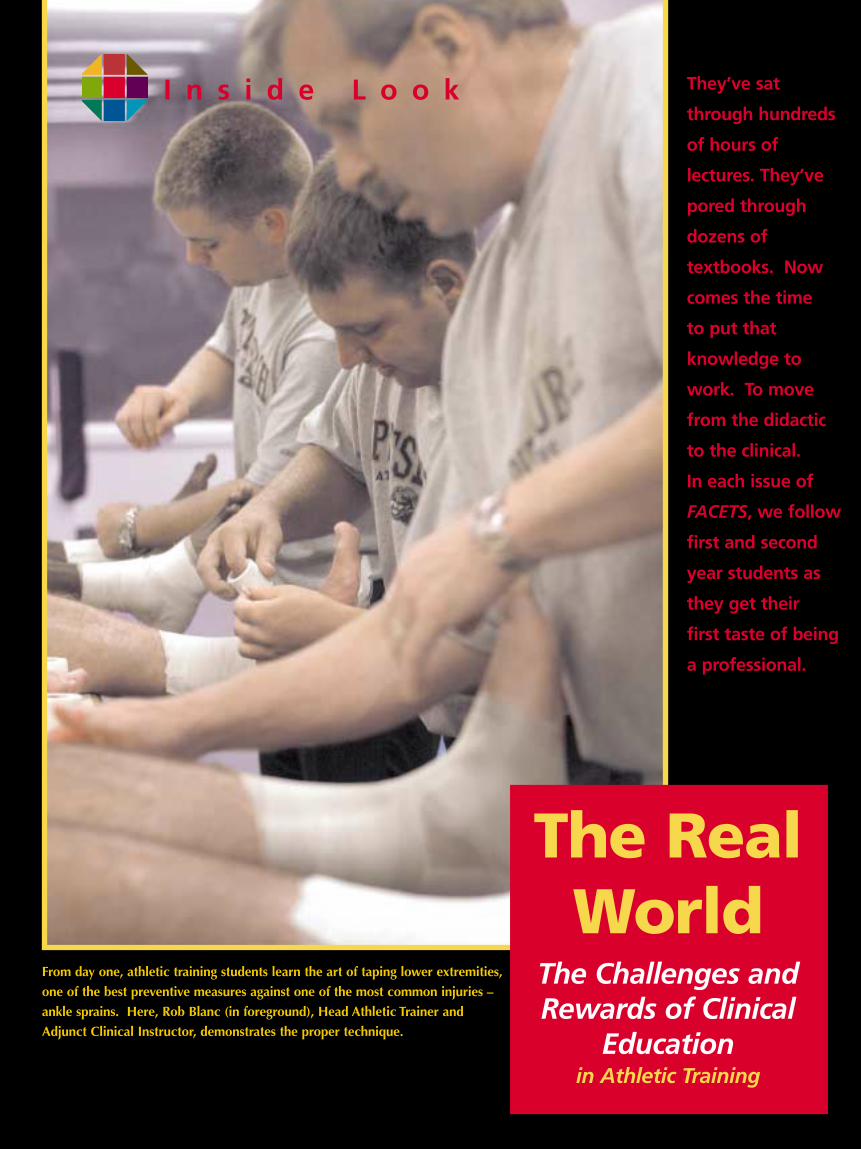
From day one, athletic training students learn the art of taping lower extremities,
one of the best preventive measures against one of the most common injuries –
ankle sprains. Here, Rob Blanc (in foreground), Head Athletic Trainer and
Adjunct Clinical Instructor, demonstrates the proper technique.

The crowd, the pageantry, the thrill of victory,the agony of defeat – all the necessary ingredients for a Saturday afternoon rife withcollegiate fanfare.
But there’s more than meets the eye when youwatch the Pitt Panthers do battle. To the casualobserver, the players decked out in helmets andpads tell the whole story. However, to those inthe know, the weekly slugfest on the field beliesthe sweat and toil that goes into preparing theteam. It’s no mystery that behind every successful college football team lies a dedicated
16
Hope springs eternal this time of year inOakland. Classes are back in session,the heat and humidity have passed and
crisp autumn days envelop the campus, and thePitt football team suits up to try to capture gridiron glory. Ah, football. A religion of sortsin southwestern Pennsylvania that takes place inits own house of worship – Heinz Field.
Sports Medicine & Nutrition
The RealWorld
The Challenges and
Rewards of Clinical
Education
Training Day

“While we’re taking care of the athletes, we’re teaching the athletic training
students what it is we’re doing, why we’re doing it, and how we’re doing it,”
says Blanc. “So it works out very well because they’re gettinghands-on experience right from the get-go.”
17
supporting cast, and some ofthe most important players inthat cast are the athletic trainers.
The School of Health andRehabilitation Sciences boasts one of the top athletic training programs in the country, and sixundergraduate students from the
program are on the frontlineworking with Pitt’sfootball team thisyear. Rob Blanc,who has spent 15years as the Pantherfootball team’s HeadAthletic Trainer, overseesthe six undergrads in addition to one graduate assistant and an assistant athletic trainer.
Simultaneously, he looks after the players and the athletic training students.
“While we’re taking care of the athletes we’reteaching the athletic training students what it iswe’re doing, why we’re doing it, and how we’redoing it,” says Blanc. “So it works out very wellbecause they’re getting hands-on experienceright from the get-go.”
Twenty-seven students are enrolled in the athletic training program, and they spend their freshman and sophomore years taking prerequisite courses before applying to it. An additional prerequisite is spending 45 hoursobserving athletic training rooms on campus, in hospitals, and in high schools for an overview of the options available to studentsafter graduation.
To fulfill the program’s clinical requirements,students work with a total of four differentsports teams during their junior and senioryears, for which they receive a total of six academic credits. The 19 sports covered in the program are divided into equipment-based,
Athletic training studentsfind the time commitmentone of the biggest challenges, but seeing aplayer go through the rehabilitation process andreturn to the playing fieldis a reward in itself.
Athletic training studentsgo through a “game day”routine to get players readyfor each practice, such astaping, stretching, and massaging. They’re alsoinvolved in rehabilitatinginjured players.
Advances inAthletic Training
Walk into a training room and you’ll still find rolls of tape, layers of gauze, and piles of elastic bandages. But according to Tony Salesi, Coordinator ofAthletic Training for Olympic Sports and an Adjunct Clinical Instructor inthe Athletic Training Education Program, these items are virtually the only tools of the trade that previous generations of practitioners would recognize.
“Research-based practice and advances in technology have molded thefield of athletic training into what it is today,” asserts Salesi. “Twentyyears ago, athletic trainers based their knowledge in the clinical set-ting on experiences they had with patients over the years. Treatmentmethods were as simple as what worked and what didn’t. Therewas very little documentation to back up what we were doing. Butnow that we have clinical research and the tools of technology,we’ve created a far superior educational environment, and likewise, better prepared athletic trainers.”
Rob Blanc, Head Athletic Trainer and Adjunct Clinical Instructor,says that athletic training has evolved along a path similar toother medical professions. “We’ve been able to incorporate all of the technological advances of medicine into our field and our facilities. For instance, we have digital radiology capability from the UPMC Center for Sports Medicine righthere in our athletic training facilities to help in our injuryassessments. The technology that we have at our disposal is just incredible.”
John Vairo, Assistant Athletic Trainer and Adjunct ClinicalInstructor, agrees. “We now have online access in ourphysicians’ examination rooms that gives us access to anyathlete’s medical history. We can look at an injured athlete’s past X-rays, MRIs, CT scans, you name it,” heexplains. “The technology gives our athletic training students and staff a huge advantage in an injury situation, but also requires a more highly trained individual to ensure that everything is done correctly.”
To ensure that students are prepared for the challenge,the Commission on Accreditation of Allied HealthEducation Professionals (CAAHEP) is moving towardstandardization of athletic training education.According to Josh Hubert, Assistant Athletic Trainerand Adjunct Clinical Instructor, “Students will beexpected to demonstrate competency in over1,000 proficiency skills in both the classroom and clinical settings before being permitted to sit for the national certification exam. Thiswill guarantee that athletic trainers are thoroughly prepared and will be in the position to continue the learning process well into their career.”
Jill Kirby, Assistant Athletic Trainer andAdjunct Clinical Instructor, supports raisingthe performance bar. “Athletic trainers needto be prepared for future technologicalinnovations,” she says. “The constant shifttowards greater reliance on technologywill put current and future students in good stead to adapt to whatever challenges they may face.”
continued

18
In the month of Augustthe team practices threetimes a day, and the athletic trainers gothrough a similar routine to get the playersready for each practice – taping, stretching,massaging, taping, icing, more taping. They’realso involved in rehabilitating injured players.Each student focuses on players in one or twodifferent positions, such as running backs andwide receivers.
During “three-a-days” the athletic training students ostensibly live three days in the timespan of one. Their day starts around 6 a.m. toprepare for the morning’s first practice. Theywork straight through the morning – duringwhich the team practices twice – grab a quicklunch, take a well-deserved catnap (some ofthem, anyway), and then get the players readyfor afternoon practice. While the team practices, athletic training students scramble to and fro tending to the players’ every need.Practicing under the boiling August sun whereheat exhaustion and dehydration are players’mortal enemies, athletic training students makesure fluids are plentiful and readily available.
The third practice of the day winds down in thelate afternoon, but it isn’t until 8:30 p.m. that athletic training students call it a wrap – almost15 hours after their day began. On game days,
upper-extremity, lower-extremity, and generalmedical. Every student is required to work withat least one sport in each category. Althoughdedicated exclusively to football, Blanc overseesall 19 sports. Some athletic training studentsalso gain clinical experience by working withathletes from Carnegie Mellon University.Because CMU does not have an athletic trainingprogram of its own, some of the program’s students work with CMU’s sports teams,enabling them to gain insight into the DivisionIII level of athletics.
Preparation, prevention, hydration, tape. Thereare miles of it laying around the training roomat Pitt’s Southside practice facility. Enough tomummify a team full of 300-pound pharaohs.Before each practice Blanc and his undergradu-ate protégés go through dozens of rolls whilediligently taping players’ lower extremities, oneof the best preventive measures against one ofthe most common injuries – ankle sprains. Ifthere’s one thing these trainers-in-training learnto master early, it’s the art of taping. Andthey’re getting plenty of practice.
The RealWorld
The Challenges and
Rewards of Clinical
Education

their schedule can run even longer. “The time commitment is definitely the biggest challenge,” says
Kristen Pinskey, a first-year student in the program. “But it’s a lot of fun. We like working with the players and coaches.” Pinskeysays there’s mutual respect between the playersand athletic training students, and an invisibleline exists between the two that neither sidecrosses. The greatest reward for all their timeand effort? “Seeing someone go through therehabilitation process and actually get back toplay at their full playing potential,” says second-year student Lauren Golofski. Traveling with theteam to away games doesn’t hurt either.
After graduation, all six athletic training students will likely pursue a master’s degreein athletic training – a necessary step tobecome a professional in the field. Whentheir studies conclude, they’ll set their
sights on becoming full-time athletic trainers in any number of clinical settings, from the traditional – high schools colleges and clinics –to more contemporary venues like the industrialsector, where there’s a growing demand for theirunique skills. And perhaps a shorter work day.
The Tim Kerin Memorial
ScholarshipFund
Tim Kerin was a dedicated athletic trainer whoworked at the University of Pittsburgh from1970 to 1976 as the Head Athletic Trainer. He was responsible for starting the athletictraining curriculum and was devoted to promoting the profession of athletic trainingand the National Athletic Trainer’s Association.He was extremely loyal and reliable, a personwho was the epitome of a “team player.” Hisdevotion touched the lives of many who havegone on to be successful in the profession. In1992, at the age of 44, Tim Kerin passed away.
In 1994, the Department of Athletics, theAthletic Training Program, and the OptimistClub of Wilmerding established the Tim KerinMemorial Scholarship, which helps worthystudents obtain their undergraduate degree inAthletic Training. The scholarship committee isnow working to fully endow the award so thata full scholarship can be given. Anyone who isinterested in contributing to the Tim KerinMemorial Scholarship should contact KarenKhan, Director of Development, [email protected]
While the team practices, athletic training students tend to the players’ every need.Practicing up to three times a day, heatexhaustion and dehydration are a major concern. To guard against the adverse effects of heat and humidity, athletic training students make sure fluids are plentiful andreadily available.

= qh or qn
22
Health Information Management
Eliminating Errorsfrom Patient Records
It happens more often than we’d care toimagine. A patient is admitted to the hospital sick and comes out sicker. But
the headline grabbers – stories about wronglimbs being amputated – are just the tip of the iceberg. Those are the major, or “active”medical errors. It’s the “latent”errors – the omission of dischargeorders, sloppy medical records – thatthe National Academy of Science’sInstitute of Medicine (IOM) Reportnotes are a major threat to the safetyof patients.
Dr. Valerie Watzlaf, AssociateProfessor, Department of HealthInformation Management (HIM),argues that HIM professionals canplay an active role in reducing or eliminatingthose latent errors.
“HIM professionals see errors in medicalrecords all the time that may appear to beminor,” she says. “But even something as benignas failing to record a patient’s height and weightcould result in an anesthesiologist administeringan under- or overdose of medication.”
Watzlaf, along with Diane Lares Frndak, a doctoral student, detailed their concerns in anarticle for the Journal of Health InformationManagement that appeared earlier this year. Inthe article, they discussed several commonerrors, the potential results, and what the HIMprofessional can do to correct the error as wellas the system that allowed it to occur.
“HIM professionals sit on a variety of committeeswithin a hospital: patient safety, risk management,case management, and many more,” Watzlafnotes. “It’s our job to ensure that medicalrecords are complete and legible and to educateclinicians, nurses, and others about how latenterrors can compromise patient safety.”
I Can’t Read Your WritingIt’s an age-old joke. A physician prescribes
medication or a lab test and it appearsto be in hieroglyphics. But it’s really notamusing. Whether on a prescription pad or a patient chart, illegible handwriting can compromise the safety of the patient.
Watzlaf points out that many of the common abbreviations used in themedical field can be misread – with thepotential of dangerous consequences.For example, “qn,” which means night-
ly or at bedtime, could be mistaken for “qh,” orevery hour.
Explains Frndak,“It’s the HIM professional’sobligation to reduce the number of handwrittenentries in the medical records and ensure thatall physicians are aware of the Institute for Safe Medication Practices table, “DangerousAbbreviations”.” Frndak is also a trainer withthe Pittsburgh Regional Healthcare Initiative,
which, among its goals, lists patient safety – zero medication errors and
hospital-acquired infection – as its aim.
Illegible medical record entries could also resultin a patient being denied insurance coverage. If entries such as adverse conditions are unreadable, an insurance company may have no choice but to refuse to cover treatment.
The Sin of OmissionWhen a patient is finally discharged from thehospital, more often than not, their focus is onjust getting home. Perhaps they’re thinkingabout a good meal, or a good night’s sleep without interruption. They may not be thinking,“What do I do now?” But they should be, and that’s what discharge instructions are for –to specifically detail the course of continuedrecovery.
Watzlaf cites a Harvard study that found thatinadequate follow-up of medication therapy,which is part of the discharge instructions,occurred in 45 percent of the patients theresearch followed in studying adverse events in hospitalized patients.
“It’s a challenge for HIM professionals to ensurethat discharge instructions are documented andgiven to patients,” Watzlaf notes, indicating thatdesigning an electronic medical record (EMR)that requires discharge instructions to be included before moving on to the next sectioncould go a long way toward protecting thepatient once they’ve left the hospital.
Valerie Watzlaf
Preventing the

nightly?
?
Failing to prominently display any allergies onthe patient’s chart or to accurately document a patient’s medication history also represent “accidents waiting to happen.” This is particularlytrue for older patients who may be on multiplemedications that could have contraindications toadditional medications that may be prescribedwhile they are hospitalized.
Again, Watzlaf says, the HIM professional’s participation in teamsthat evaluate the effectiveness ofEMRs is essential. She points out that concurrent evaluation ofpatient records is essentialto uncover and flagsuch errors and correct them whilethe patient is stillhospitalized.
“While not ourprimary concernin developing thispaper,” notesWatzlaf, “informationomitted from patientrecords could compromiseresearch projects where the protocoldemands that all information on patients be comparable.”
The Future is Technology In 1983, Medicare developed the ProspectivePayment System, creating diagnosis-relatedgroups (DRGs) and requiring hospitals to significantly upgrade their medical record-keeping capabilities. The result was a new prominence for HIM professionals.
“Hospitals look to us for ourexpertise, for the standards that
need to be incorporated, for newand better ways to improve medical
record keeping,” states Watzlaf.
Medical information has been computerizedfor over a decade, but as always, the resultingrecords are only as good as the data that’sinput. New voice recognition systems that eliminate the need for a transcriptionist, forexample, are coming on-line, potentially eliminating errors caused by inaudible dictation.
In addition, research is being conducted thatwill apply Internet search technology to currentsystems, making record searches for bothresearch and clinical purposes more efficientand effective.
Medication packaging is also getting help fromtechnology. Bar codes,familiar to anyone who grocery shops, can create a direct link between theright medication and theright patient, with the added advantage of automated billing.
“HIM professionals shouldbe advising their hospital’sadministration about theuse of all of these new technologies,” notes
Frndak. And while it may appear that financesand reimbursement are a driving force, Watzlafinsists that the health and safety of patients, bothin the hospital and after discharge, should be the key motivation in ensuring that inaccuratemedical records are not the underlying cause oflatent errors that threaten the health of patients.
For more information, contact Valerie Watzlaf [email protected]
23
every hour?
Preventable
“It’s our job to ensure that medical records
are complete and legible and to educate
clinicians, nurses, and others
about how latent errors can
compromise patient safety.”

24
Two summers ago, the career of an occupational therapist in the ArmyMedical Specialty Corps typically focused
on ergonomics and upper extremity therapy. Butas it did for so many Americans, September 11marked a turning point for Robert D. Montz,CPT, SP. That morning, he was called away from his O.T. patients at Womack Army MedicalCenter at Fort Bragg, NC, to help prepare Critical Event Stress Debriefings (CESDs) foremergency responders and military personnel at the Pentagon.
“We were ready to go up to the Pentagon thatday,” says Captain Montz. “We support all of the units in the 18th Airborne Corps, so weknew we would be going somewhere. Eventhough we didn’t deploy on 9-11, we knew it was just a matter of time before we would be used elsewhere.”
Moving OutIn a “go to war” mission like Operation EnduringFreedom, O.T.s are assigned to Combat StressControl Units, focusing their skills in the mentalhealth arena. A mental health “Prevention Team”is usually made up of a psychologist, a socialworker, and two enlisted mental health specialists.
An O.T. GraduateApplies His Skills in
Time of War
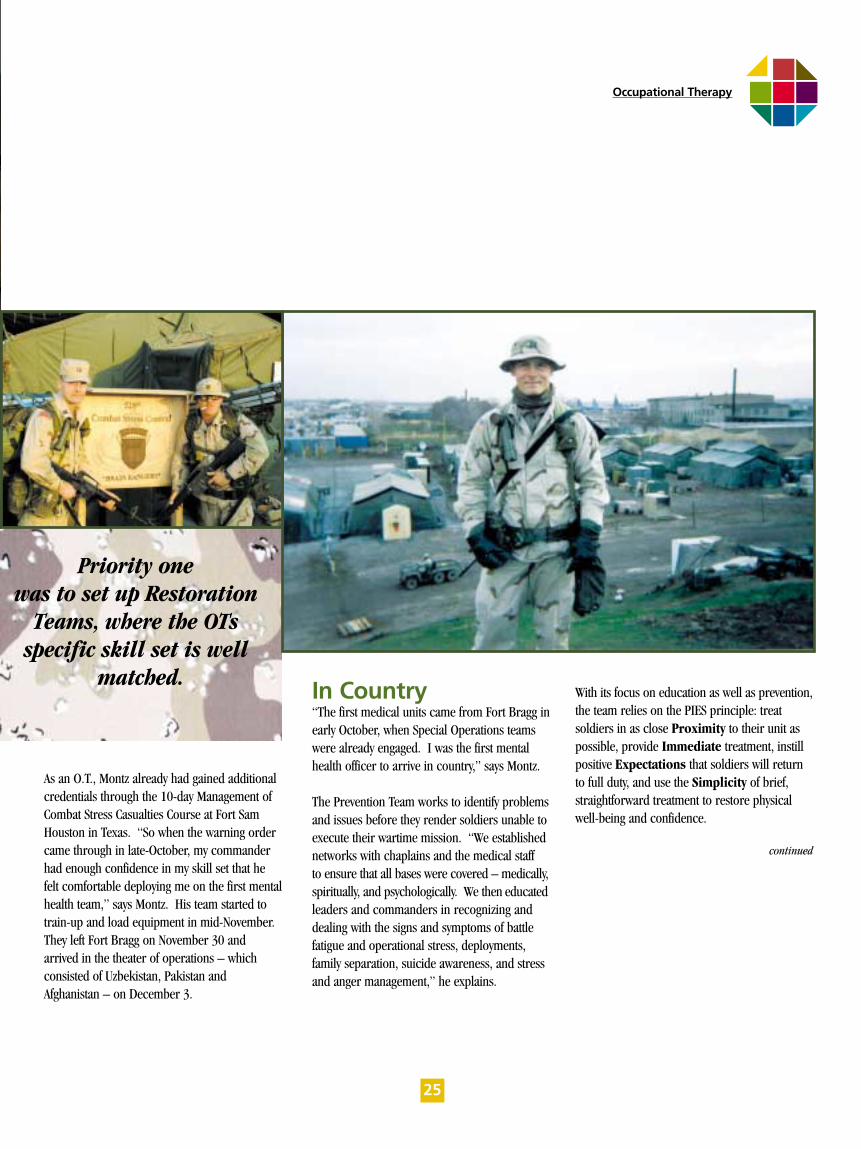
25
As an O.T., Montz already had gained additionalcredentials through the 10-day Management ofCombat Stress Casualties Course at Fort SamHouston in Texas. “So when the warning ordercame through in late-October, my commanderhad enough confidence in my skill set that hefelt comfortable deploying me on the first mentalhealth team,” says Montz. His team started totrain-up and load equipment in mid-November.They left Fort Bragg on November 30 andarrived in the theater of operations – which consisted of Uzbekistan, Pakistan andAfghanistan – on December 3.
In Country“The first medical units came from Fort Bragg inearly October, when Special Operations teamswere already engaged. I was the first mentalhealth officer to arrive in country,” says Montz.
The Prevention Team works to identify problemsand issues before they render soldiers unable toexecute their wartime mission. “We establishednetworks with chaplains and the medical staff to ensure that all bases were covered – medically,spiritually, and psychologically. We then educatedleaders and commanders in recognizing anddealing with the signs and symptoms of battlefatigue and operational stress, deployments, family separation, suicide awareness, and stressand anger management,” he explains.
With its focus on education as well as prevention,the team relies on the PIES principle: treat soldiers in as close Proximity to their unit aspossible, provide Immediate treatment, instillpositive Expectations that soldiers will returnto full duty, and use the Simplicity of brief,straightforward treatment to restore physicalwell-being and confidence.
Priority one was to set up Restoration
Teams, where the OTs specific skill set is well
matched.
Occupational Therapy
continued

26
Looking Behind…and Ahead“Our work was made easier by the groundworkand operations we have done in Bosnia andKosovo over the last several years. Standardoperating procedures and forms were all inplace, so it allowed us to create a nice, fluidmotion to the many roles we had in OperationEnduring Freedom,” says Montz, who was incountry for just under seven months, and whofully expects to return during what promises tobe a long war. “A prevention team is supposedto go to the troops, so we went everywhere wecould – not into the caves, but as far forward aspossible,” he adds.
Back home at Fort Bragg with his wife, Marcia,and two children, Montz continues to hone hisskills and leadership. “I’ll be at the JointReadiness Training Center at Fort Polk, LA, foran exercise in combat service support. I’ll be incharge of a four-person team, getting them all onthe same sheet of music and ready for futuredeployments,” he says.
Advancing the Fieldas an Army O.T.Although he is a self-described Army/Navy bratwho spent his early years in many parts of thecountry, Montz has his deepest roots in WesternPennsylvania. He attended the University ofPittsburgh, earning his B.S. in OccupationalTherapy in 1997. Robert did his Level Two fieldwork while on active duty at Madigan ArmyMedical Center in Fort Lewis, WA.
Very seldom do Army occupational therapists getto deploy, especially on the prevention team.But with the number of deployments and thedecrease in personnel in the military, Montzseized a unique opportunity, not only to servebut also to widen the understanding of an O.T.’svalue as a mental health officer. “Our mission isto get soldiers back to the war. It’s all aboutfunction, and that’s where occupational therapyfits so perfectly,” he says. “I got very well-versedin explaining the O.T.’s role on a mental healthteam. I tell leaders and soldiers that the psychologists and psychiatrists do the talking,and the O.T.s put that talking into practice.”
Since Montz first landed in Uzbekistan, two otherArmy O.T.s have deployed in this war. Theirefforts will surely make a difference in whatpromises to be a long and complicated effort.
Occupational Therapy
“A prevention team is supposed to go to the troops, so we went
everywhere we could – not into the caves,
but as far forward as possible,”

New Curriculum DesignPuts the UniversalLanguage of HumanFunction into Practice
In the classroom, in the lab, and in the field,occupational therapy students are activelyengaged in learning to evaluate, modify, and
improve human function.
Supporting this learning is a new curriculum design that provides an organizational structure for the knowledge and skills taught by theOccupational Therapy faculty. In the past, the department’s curriculum delineated courses basedonly on the three roles of an entry-level occupationaltherapist – practitioner, manager, and contributor. The new curriculum design also incorporates concepts about human functioning from theInternational Classification of Functioning, Disabilityand Health (ICF) published by the World HealthOrganization. The ICF proposes a universal languagefor rehabilitation that encompasses and links theroles of the occupational therapist in meaningful and practical ways. It helps faculty and studentsunderstand the relationship between different courses and where they fit in the occupational therapy process.
“The difference – and the greater value to occupational therapy – is that the ICF gives us a wayto look at health and wellness, not just disability,” says Dr. Joan C. Rogers, Professor and Chair,Department of Occupational Therapy. “It creates a framework that resonates with the viewpoint of people with disabilities today. It looks at people’s abilities and the environmental factors that limit or enhance function.
“For example,” she continues, “if I’m in a wheelchair,and there is no curb cut, then I can’t get to the storeor to work. If the curb cut is there, then I’m not dis-
abled. Or if I’m ina long-term carefacility, and therules prevent mefrom bathing myselfbecause of safetyconcerns – but I
can bathe – then the facility is making me more disabled than I need to be.”
Rogers points out that occupational therapists assessstrengths as well as weaknesses and help people compensate for their disabilities with their abilities.
“Rehabilitation is a team venture that focuses on functioning, but individual team members often carrytheir own interpretation of function,” says Rogers.“The ICF establishes a common language for describing health and human functioning in order to improve communication betweenclinicians, patients, advocates, andeven policy-makers and the public.”
The ICF creates this language byapproaching human function fromtwo perspectives. In theory, the ICFlooks at functioning and disability interms of the human body and humanactivities and it addresses the contextin which humans function in terms ofenvironmental and personal factorsthat affect functioning. In the new curriculum design,these concepts are interwoven with the roles of practitioner, manager, and contributor.
“In practice, it forces us to ask questions like, ‘If weimprove range of arm motion by five degrees, doesthat in fact increase the person’s ability to dress himself, reach food on a shelf, or perform his worktasks?’ ” explains Rogers. “It also reminds us not toassume that all problems are based solely on medicalpathology. There are psychological and social phenomena as well as biological factors that affect a person’s functioning.”
But what does this new curriculum design mean in practical terms – in the classroom and during students’ fieldwork experience? “It is helping us, asfaculty, to address clinical reasoning – how to usejudgment, set priorities, and use outcomes measuresto make evidence-based decisions more effectively,”says Rogers.
ICF is a health classification system used internationally,as a statistical tool to monitor disability trends, as aresearch tool to measure health outcomes, as a clinical tool to match client needs to interventions,and as a social policy tool to plan health care services.Says Rogers, “It is also an educational tool for helpingthe Department turn today’s occupational therapy student into tomorrow’s engaged, compassionate, and scientific health care professional.”
For more information, contact Joan Rogers [email protected]
Organizing Knowledge for Evidence-Based Practice
Joan Rogers
“Occupational therapists help people compensate for their disabilities
with their abilities.”

You’re having a great workout at thelocal gym. Suddenly, you experience a twinge of pain in your lower back.
Ouch! So a trainer working the gym floor advises you to do the next set of reps differently.
Up until now, if that trainer had been a physicaltherapist and a physician hadn’t referred you,that advice would have been illegal. The trainer,or even your massage therapist, had more cloutthan a physical therapist.
But on February 21, Pennsylvania GovernorMark Schweiker signed into law Act 6 of 2002,giving physical therapists the authority alreadyenjoyed by colleagues in 34 other states – tosee patients directly without a physician referral.
And while the law may not be a practical realityuntil early 2003, the passage of Act 6 of 2002 is the culmination of a decade of hard work by the Pennsylvania Physical TherapyAssociation (PPTA), individual physical therapists, and others.
“It was a tough battle that required a lot of consensus building,” says PPTA President PaulRockar, Jr., who is also an Adjunct AssistantProfessor of Physical Therapy and President ofthe SHRS Alumni Association. There were
plenty of groups amongwhich to build consensus: physicians, insurers,
chiropractors, athletictrainers, the Department
of State, and the Governor’soffice. “This is a progressivemove for the profession and
we’re pleased to have finally joined the otherstates who have recognized that direct access is in the best interest of the patient.”
28
“ This is a progressive
move for the
profession.”
According to Dr. Anthony Delitto, AssociateProfessor and Chair, Department of PhysicalTherapy, “Currently, a patient must be referredby his or her physician, even if they experiencea recurrence of the original symptom for whichthey were treated.” That can result in delays intreatment as well as increased expense. “It maytake several days or even weeks for the patientto be seen by their primary care physician for a referral, when we can usually see them within24 or 48 hours.”
Curriculum in PlaceBecause other states have allowed direct access– in some cases for 20 years or more – since1990, the Physical Therapy Commission onAccreditation has required that all students be
Direct AccessDirect Access Coming to Pennsylvania

29
educated in areas such as evaluativeprocedures. “Students learn to recognize problems that are out ofthe realm of their training,” statesDelitto. “We call them ‘red flags’.”For example, there are classic signsand symptoms of serious pathology,such as cancer, or signs that couldsuggest that surgery for a kneeproblem might be the appropriatecourse of action.
According to Rockar, under the new legislation,a physical therapist who graduated before 1990will be required to demonstrate appropriatecontinuing education in evaluative proceduresin order to receive a certificate of authorization.“During every licensing period, a physical therapist who opts to practice in the directaccess mode must complete at least 20 hours of continuing education,” he points out. “And,10 of those hours must be in areas related tothe ability to treat a patient without a referral.”Rockar is also Executive Vice President andPartner with the Center for Rehab Services, a partner of UPMC Health System.
Still Hurdles to LeapWhile Act 6 of 2002 became law in February,the wheels of government grind slowly. TheState Board of Physical Therapy must write therules and regulations that pertain to the act,which then must go through eight levels ofreview and public comment. A draft of thepromulgated rules has not yet emerged, so itlikely will be months before direct access willbe a reality.
Also, it is unclear whether direct access physicaltherapy will be covered by insurance. “There isnothing in the act that will preclude an insureror other third-party payor from requiring thatthe patient be referred,” notes Rockar. In statesthat currently have direct access, third-partypayors are the norm.
“We believe that the insurance compa-nies recognize that direct access is, infact, a cost-saving measure,” statesDelitto. In fact, the American PhysicalTherapy Association (APTA) points to a1994 study that found that the costsincurred for physical therapy visits were123 percent higher when patients werefirst seen by a physician. TheAPTA has mounted an effort to
get direct access for Medicarepatients nationwide.
AccoladesAboundOver the years, literally hundreds of individuals haveplayed a role in the passageof direct access, but sincebecoming President of thePPTA in 1999, Rockar has been dogged in his pursuit of the legislation. “We owe a great debt of gratitude to Paul,”states Delitto. “Therewere many people like mewho provided input withinour areas of expertise, but Paul was the onewho brought it all together. He was selfless in his pursuit of this legislation.”
And Rockar’s work did not go unnoticed. The APTA recently awarded him the 2002 State Legislative Leadership Award. Clearly, a well-deserved honor.
For more information, contact Anthony Delittoat [email protected]
Physical Therapy
Anthony Delitto

30
KnowledgeK nowledge is moving much farther –
and much faster – than ever. Thanksto improved, affordable international
travel, electronic communication, and more frequent collaboration between countries andcultures around the world, the fruits of today’sacademic research and education initiatives arebeing nurtured, harvested, and shared likenever before. More important, the results ofthese international educational initiatives – particularly developments in the field ofEmergency Medicine – are having a markedeffect on the well-being of people living acrossthe street and on the other side of the globe.
“Graduates from our Diploma ParamedicProgram in Emergency Medicine are playingkey roles in improving the quality of emergencymedical care in several countries,” commentsDr. Walt Stoy, Associate Professor and ProgramDirector of the Emergency Medicine Program.“We welcome students from any country that is willing and able to upgrade its health care system, and we’re committed to sending themhome versed in the latest EMS knowledge and techniques.”
Educating Students fromNear and FarThe Diploma Paramedic Program in EmergencyMedicine grew out of the Center for EmergencyMedicine, which was founded in 1978. Since its inception, the program has attracted a steadystream of students from more than 20 countriesas diverse as Canada, Iceland, Saudi Arabia, and Qatar.
Designed for completion in one year under normal circumstances, the program has garnered an outstanding worldwide reputation.It has also become a solid foundation for international students who are interested inearning a Bachelor of Science degree inEmergency Medicine. Credits from the one-yeardiploma curriculum can be credited toward the B.S. program – a benefit that allows students to move smoothly into the university if theychoose to do so.
“We do not make special adjustments to the curriculum for international students,” remarksStoy. “If they meet our stringent entry standards,they can matriculate the same way any other student would. In fact, we have found that as
long as international students are fairly fluent in English and are able to keep pace with thecoursework, everything works out quite well.However, if our instructors notice that an international student is having difficulty due to language issues or cultural factors, we recommend a lighter load that will extend the duration of that student’s studies at Pitt.”
In cases where English skills are a problem, thedepartment will defer admission until studentshave completed necessary remedial languagecourses. These students are also encouraged to seek out native-speaking communities withinthe Pittsburgh area that can be particularly supportive in helping students make the transition into the domestic educational system.
The Right FitThe program’s flexibility is another attractivepoint for students coming from abroad.“Because we are part of SHRS, our studentshave direct access to the educational experiencesoffered by the other six departments that comprise the school,” observes Stoy. “An interdisciplinary approach is both acceptedand supported by our department, and we
Emergency Medicine
W I T H O U T B O R D E R S
“We have a great deal of knowledge to share withcurrent and potential students . . .
31
encourage our students to look into areas ofinterest that lie beyond the boundaries of ourprogram. For example, one of our internationalstudents came to us to pursue the diploma certification and ultimately ended up graduatingfrom the SHRS Health Information Managementprogram. Others have taken elective courses in disciplines that complement ours. The endresult is a more rounded educational experience, and ultimately, a skill set that makes our students exceptionally marketable.”
While the program is quite successful in accommodating the academicinterests of its international students, the events ofSeptember 11 have had a significant impact on studentsfrom abroad. “We are findingthat it takes considerablylonger to process our international students, but weare happy to comply with thearray of new regulations thathave arisen since the tragedy,”says Stoy. “In a nutshell, international students, theEmergency Medicine Program, andSHRS have all found that thingsmust be done sooner than they
had in the past. Procrastinationcan result in students having adifficult time enteringthe country andthose delays cantranslate into lost timein earning their paramedic or B.S. credentials.”
On the HorizonLooking toward the future, Stoy hopesto see continued growth in the diploma program, as more students from around the
world come to Pittsburgh to learn fromthe faculty and staff. “We have a greatdeal of knowledge to share with currentand potential students. When countrieslook beyond their borders and worktogether on improving health care, everybody wins.”
For more information, Walt Stoy [email protected]
When countries look beyond their borders and work togetheron improving health care, everybody wins.”
Walt Stoy

32
The Final PhaseThe HERL Machine Shop Turns Research into Reality
Rehabilitation Science & Technology

At the Human Engineering ResearchLaboratories (HERL) Machine Shop, the spacebetween “what if” and “what can be” is continually being narrowed for a growing number of students. Through hands-on opportunities to learn about materials and operate high-tech equipment, SHRS is continuingto produce graduates who understand assistivetechnology from the ground up.
“This is basically a support area for all of thelabs,” explains Bill Ammer, TechnicalCoordinator at HERL. “We build and test theassistive technology devices that are designedin the labs, and give students and researchers
the opportunity to learn about materials and fabrication techniques first hand.”
Staffed by Ammer, machinist Mark McCartney,and assistants JohnDuncan and Emily Zipfel,the shop is a three-wayventure between the
university, the UPMC Health System, and the VAPittsburgh Healthcare System. Founded nineyears ago by Dr. Rory Cooper, Professor andChair, Department of Rehabilitation Science andTechnology, and Director of the HumanEngineering Research Laboratories, the shop islocated at the VA’s Highland Drive facility andsupports work on a wide range of research anddevelopment projects.
A Hands-On Environment“All of our research is funded by grants or contracts,” notes Ammer. “Most of the assistivetechnology equipment we build and test herewas designed in our labs. However, we do collaborate with other institutions and participate in a number of multi-site studies to collect and compile data.”
But that’s just the beginning. Beyond buildingand testing for research, the shop focuses onhelping graduate students acquire the hands-onskills that are critical to a successful career.
“Our goal is to educate graduate students on how to actually function in a shop environment,” remarks Mark McCartney, the shop’s machinist, who divides his timebetween HERL and the Center for AssistiveTechnology on the Oakland campus. “We show students how to operate some extremely sophisticated equipment, choose materials, and ultimately make the components they’vedesigned. By learning how to do all of this, theyget a feel for what it’s like in a real-world shopenvironment and find out how to handle thingswhen they need something to be made.”
The shop is equipped with a number of Computer Numerical Control (CNC) machines.Set up to work in all types of materials, fromwood and metals to plastics and composites, the facility features carpentry and welding capabilities that complement the machiningoperations.
Crossing DisciplinesThe shop also offers a number of opportunitiesfor team building. “It’s been said that there areengineers and there are therapists, and never the twain shall meet,” comments Ammer. “In this program, and particularly in this shop,they do get together and learn from each other.They see how the disciplines intertwine. I thinkthat’s probably one of the neatest things aboutthis program. We have electrical engineers andmechanical engineers in the grad programs.And there are some bioengineers, exercisephysiologists, physical therapists, and occupational therapists, too. They all comedown here to learn the same things. They learn how to pick materials and machine. And they learn to work together as a team toovercome challenges. That goes a long waywhen they get out into the working world.”
“what-ifs,”
“what can be.”
There’s considerable
distance between
the birth of an idea
and implementation.
While ideas can freely
explore the realm of
implementation provides
the direct connection
to the reality of
33
continued

For McCartney,watching novicestudents evolve intotechnically-literate professionals is one of the most
rewarding things to come out of the shop operation. “It’s pretty hard to design somethingif you don’t have shop knowledge and havenever made anything before. Many of the students have backgrounds in physical or occupational therapy, but don’t really know how a device is made. However, when theyleave here, they can take a part off of a wheelchair or some other assistive device anddetermine fairly accurately how it was made.They also have a pretty good understanding ofmetals and how they perform under differentconditions. Helping them gain that knowledgeis one of the best parts of our whole program.”
Real World PayoffsThe shop is also helping SHRS graduatesbecome more marketable. One of the grad students working at HERL got an internship thispast summer at the Quickiemanufacturing facility inBoulder, Colorado. His supervisor was impressed by the fact that he could walk into the shop and startworking with their team.
Explains Ammer, “Dr. Cooper initially designed the forward-folding wheelchair in one of hiswheelchair design classes.He then partnered with oneof the students to design the second generationof the chair. The student worked in the shop to create the components for the new chair.
When a representative from Quickie was touring our facility, she saw the new chair andasked who was involved in the project. The restis history.”
Access to the shop is not limited solely to graduate students. In the Spring 2002 semester, Ammer andMcCartney started anew undergraduatecourse – EngineeringMethods andMaterials. Thecourse is growing in popularity amongSHRS and bioengi-neering students.
“We try to make basic machinists out of them,”says McCartney. “Our first semester was a trial.None of the students had any machine or engi-neering background. They were all therapists.”
Rehabilitation Science & Technology
The
Final
Phase

This term, it’s been adopted as an undergraduatecourse at the university. There are six studentsregistered for the course. We feel good aboutthat,” says Ammer.
A Productive PartnershipAmmer and McCartney also continue to partnerwith Cooper on a number ofongoing projects. “Aside fromthe forward-folding chair, one ofour most ambitious projects hasbeen the SmartWheel™, aninstrumented wheel outfitted withstrain gauges that fits any wheel-chair and calculates stressesbeing exerted on shoulders,elbows, and other joints by theuser of the chair. It’s somethingDr. Cooper developed about 10years ago and over time it hasgone through several refinements to improve its accuracy and effectiveness. We have built thelast several versions of the wheel,including the last model that eliminates outsidecabling and operates off of infrared circuitryhoused in the wheel’s hub.” Now theSmartWheel™ is in commercial production,and is being used in four countries and morethan 10 laboratories.
“I think almost everyproject we’ve donehere has been adopted by someother university oroutside company thatwants to develop itfurther,” says Ammer.“We’ll work on
something to a point and decide we’ve gone as far as we want to take it or can takeit. Then, we transfer the technology to someone else who can carry it into final production. Our job is tobasically prove that a device can orcan’t work, then we work withother organizations to bringit into production.”
35
While there’s always something new and different going on in the shop, Ammer andMcCartney never lose sight of the fact that learning is the primary objective. “I don’t knowof too many places where schools will let theirstudents have hands-on experience with thekind of equipment and materials we have here,”notes McCartney. “They may let them into themachine shop, and they may let them watch, butvery few places let them actually learn. We justdon’t work that way. That’s not reality.”
For more information, contact Bill Ammer [email protected]

W i s d o m
Japanese StudentsVisit Athletic TrainingProgram
As a testament to its growing stature as oneof the world’s top athletic training programs, thissummer, the Athletic Training program hosted a group of 32 graduate and undergraduate technical school students from Tokyo for aweek of sightseeing and study.
“The visit was arranged by a Japanese companycalled Try Works for students interested in athletic training,” explains Kevin Conley,Program Director and Instructor in the AthleticTraining Education program. “The idea was todivide the students’ time between athletic training studies and demonstrations and toursof the city. We spent half of the day teachingthem about the latest developments in sportsmedicine and the rest of the day going to places like PNC Park and Heinz Field.”
36
Sports Medicine & Nutrition
Continues Conley, “We wanted to givethem every opportunityto learn about athletictraining, but not overwhelm them. For instance, we presentedthe anatomy for both theupper and lower extremi-ties, showed them how toevaluate commonly seeninjuries, and then followedthat by demonstrating various management andtreatment techniques whichthey were then given anopportunity to practice on each other.”
For many of the students, the trip was an eye-opener. Not only did they experience a new culture. They got their first taste of a new profession.
Explains Daisuke Uematsu, Japanese himselfand a second-year undergraduate student in theAthletic Training program, “In Japan there arevery few professional athletic trainers. Theoccupation is not widely known. Likewise,there is nothing comparable to SHRS’s academic program or clinical facilities. Youwon’t see anything like the UPMC Center for Sports Medicine and the NeuromuscularResearch Laboratory in Japan.”
Athletic Training GoesInternational

L e a r n , S c i e n c e
37
But the visit gave some of the students hope thatwhat they saw and learned will one day be areality in Japan. Says Shingo Nakai, a student in the Waseda University Graduate School ofHuman Sciences, “There is nothing comparableto these buildings in Tokyo now. But, seeingthem makes me believe that there will be. It isonly a matter of time.”
Yoshiaki Tsuboyama, an undergraduate studentin the Juntendo University School of SportsSciences, echoes that sentiment. “This is thefuture for Japan. Seeing how much technologythere is for athletic training in America makesme feel that it will eventually be the same inJapan. I have come here to learn so I can helpmake the change.”
T e a c h e r

39
Q: Is there sufficient awareness at the federal level of the significant impending problems associated with vastly increasingnumbers of individuals living beyond age 80?Will the services that these individuals typicallyneed be available to them?
A: “The government is just not going to beable to afford to provide people with all ofthe care that they need. There’s a lot ofideas, such as low-cost insurance, but weneed to come up with more clear solutions.”
Q: What are some of the ideas that areunder discussion?
A: “Incentivizing people to take a moreactive role in their own health care is important. One of the bills we’re working onin Congress addresses the issue of providingincentives for families to care for older family members, while also planning fortheir own future. There simply isn’t enough discussion about long-term careinsurance. We need to encourage people to buy more long-term care insurance whenthey’re young.”
Q: Since the first large influx of over 80-somethings demanding social services and healthcare is likely to occur in Pittsburgh,should this community be more proactive on this issue?
A: “Affordable health care is everybody’sproblem, and the problem is becoming moreacute. The good thing about D.C. is thatthere’s always a healthy exchange of ideas inthe air, and that promotes useful discussion.We need to make sure that solutions ariseout of these discussions, and sooner ratherthan later.”
Q: Since you serve on the House ScienceCommittee, what do you see as the most promising areas in research?
A: “There’s a lot of genetic research, especially about the predisposition for disease. Research about how to alter thesepredispositions is becoming increasinglyimportant, while issues of what we shouldeven do with such information emerges. We need to deal with questions not just aslegislators, but as society as a whole.”
Q: Are there other promising areas, especially for the Pittsburgh region?
A: “Biotech is a one of the fastest growingfields in the region as well as the entire scientific community. We have some verywell-known local researchers who have delivered consistent results. Theseresearchers can attract significant federalresearch dollars to this region. It is incredible how far research has advanced.”
Q: Where do rehabilitation sciences fare onthe national research agenda?
A: “It is obviously a significant part ofpeople’s lives, and this is reflected in thebudget of the Department of Health andHuman Services and other funding streams.Rehab is the same idea as teaching people,getting them to realize their fullest potential.For Pitt to command big dollars in this area,you want them to remain on the cuttingedge with their research and approach tonew therapies.”
Q: Does the University of Pittsburgh’s recentextensive collaboration with Carnegie MellonUniversity help their cause?
A: “Absolutely. I think that we have outstanding leaders at the University ofPittsburgh who saw real value in this collaboration. The planets are aligning. The leaders at both Pitt and CMU are bright individuals who work successfully togetherto get the best for each institution.”
A Conversation with U.S. Representative Melissa HartDialogue

















