SELF-AsSESSMENT Self-Assessment examination of the American Academy of Dermatology* Identification No. 894-207 Learningobjectives: At the conclusion of this self-assessment learningactivity, physicianparticipants shouldbe able to assess their owndiagnostic and patient management skills with respectto thoseof their colleagues in the field, use the resultsof the self-assessment to helpdeterminepersonal learning needs that can be addressed through subsequentCME involvement, and enhance their abilityto complywiththe requirements for certificationin the specialtyof dermatology. Instructionsfor CategoryI CME creditappearin thefrontadvertisingsection.Seelast page ofContents for pagenumber. Instructions: In answering each question, refer to the specific directions provided. Becauseit isoften necessary to provide informationin questions occurring later in a seriesthat give away answers to earlier questions, please answer the ques- tionsin each seriesin sequence. QUESTIONS 1-10 A 73-year-old man had a 6-month history of an enlarging nodule arising with a scar on the nose (Fig. 1). A basal cell carcinoma had been treated 30 years previously in this location with radiation therapy. 1. The clinical differential diagnosis includes (Choose as many as apply. All, some, or none of the choices may be correct.) a. basal cell carcinoma b. squamous cell carcinoma c. Merkel cell carcinoma d. lymphoma e. eccrine poroma A biopsy specimen shows sheets of small blue cells in the dermis (Fig. 2). 2. The histologicdifferential diagnosis includes (Choose as many as apply. All, some, or none of the choices may be correct.) a. sebaceous carcinoma b. basal cell carcinoma c. Merkel cell carcinoma d. metastatic small-cell carcinoma of the lung e. lymphoma 3. Immunocytochemical staining with low-molecular- weight cytokeratins (Fig. 3) shows (Choose single best response.) a. artifactual staining lilaCTheSelf- Assessment examination is supported in part by an HO<!J educational grant from the Procter & Gamble Company, Cincinnati, Ohio. *Membersof the Self-Assessment Committeeof the American Acad- emy of Dermatology are: Kenneth J. Tornecki, MD, chairman, Bur- ton S. Belknap, MD, Mary R. Buchness, MD, Ponciano D. Cruz, MD, C. Ralph Daniel III, MD, Gary R. Kantor,MD,Francisco A. Kerdel,MD, Tobi B. Richman,MD,Theodore Rosen, MD, Robert A. Schwartz, MD, Norman W. Walton III, MD, and Ronald G. Wheeland, MD. b. mitochondrial staining c. cytoplasmic positivity d. specificparanuclear positivity e. none of the above 145
Transcript
SELF-AsSESSMENT
Self-Assessment examination of theAmerican Academy of Dermatology* Identification No. 894-207
Learningobjectives: At the conclusion of this self-assessment learningactivity, physicianparticipants shouldbe able toassess their owndiagnostic and patient managementskills with respectto thoseof their colleagues in the field, use theresultsof the self-assessment to helpdeterminepersonal learningneeds that can be addressedthrough subsequentCMEinvolvement, and enhance their abilityto complywiththe requirements for certificationin the specialtyof dermatology.
InstructionsforCategoryI CME creditappearin thefrontadvertisingsection.Seelast page ofContents for pagenumber.
Instructions: In answering each question, refer to the specificdirections provided. Becauseit isoften necessary to provideinformationin questions occurring later in a seriesthat give away answers to earlier questions,please answerthe questionsin each series in sequence.
QUESTIONS 1-10
A 73-year-old man had a 6-month history of anenlarging nodule arising with a scar on the nose (Fig.1). A basal cell carcinoma had been treated 30 yearspreviously in this location with radiation therapy.
1. The clinical differential diagnosis includes (Chooseas many as apply. All, some, or none ofthe choicesmay be correct.)a. basal cell carcinomab. squamous cell carcinomac. Merkel cell carcinomad. lymphomae. eccrine poroma
A biopsy specimen shows sheets of small blue cellsin the dermis (Fig. 2).
2. The histologicdifferential diagnosis includes (Chooseas many as apply. All, some, or none of the choicesmay be correct.)a. sebaceous carcinomab. basal cell carcinomac. Merkel cell carcinomad. metastatic small-cell carcinoma of the lunge. lymphoma
lilaCTheSelf-Assessment examination issupported in partby anHO<!J educational grant from the Procter & Gamble Company,
Cincinnati, Ohio.
*Membersof the Self-Assessment Committeeof the American Academyof Dermatology are: Kenneth J.Tornecki, MD, chairman, Burton S. Belknap, MD, Mary R. Buchness, MD, Ponciano D. Cruz,MD, C. Ralph Daniel III, MD, Gary R. Kantor,MD,Francisco A.Kerdel,MD, TobiB. Richman,MD,Theodore Rosen, MD, RobertA. Schwartz, MD, Norman W. Walton III, MD, and Ronald G.Wheeland, MD.
b. mitochondrial stainingc. cytoplasmic positivityd. specific paranuclear positivitye. none of the above 145
146 Self-Assessment examination
4. Immunocytochemical staining with neuron-specificenolase (Fig. 4) shows (Choose singlebest response.)a. artifactual stainingb. diffuse perinuclear positivityc. cytoplasmic positivityd. specific paranuclear positivitye. none of the above
5. Electron microscopy of this lesion would demonstrte(Choose as manyas apply.All, some, or noneofthechoices may becorrect.)a. Birbeck granulesb. dense-core granulesc. fibrous bodiesd. numerous melanosomese. lipid-containing vacuoles
6. A correct diagnosis of Merkel cell carcinoma may beconfirmed by (Choose as many as apply. All, some,or noneof the choices may be correct.)a. positive juxtanuclear labeling of tumor cells with
low-molecular-weight cytokeratinsb. marked cytoplasmic reactivity with neuron-spe
cific enolasec. marked cytoplasmic reactivity with chromog
raninsd. focal presence of neurofilament proteins in a
paranuclear locatione. negative staining for leukocyte common antigen
Journal of the American Academy of DermatologyJuly 1994
A diagnosis of Merkel cell carcinoma has been established. The patient has no lymphadenopathy orhepatosplenomegaly.
7. Further evaluation of this patient should include(Choose as many asapply. All, some,or noneofthechoices may be correct.)a. baseline chest x-rayb. computed tomographic scan of thorax, abdomen,
and pelvisc. liver function testsd. carcinoembryonic antigen levelse. lymph node biopsy
Chest x-ray findings and liver function tests arewithin normal limits.
8. The patientundergoes widelocal excisionfollowedbyradiation therapy but a new left submandibular massdevelops 2 months after treatment. He undergoesunilateral prophylactic lymph node dissection followed by radiation therapy to the draining lymphnodes bilaterally. The likelihoodthat this patient willdie of his disease despite these aggressive measures is(Choose single best response.)a. 20%b.33%c.50%d.66%e.99%
9. The most effective chemotherapeutic regimens usedin the treatment of metastatic Merkel cell carcinoma(Choose as many as apply. All, some,or noneofthechoices may be correct.)a. are those used in the treatment of small-cell car
cinoma of the lungb. are those used in the treatment of cervical carci
nomac. most often produce a long-lasting clinical responsed. most often produce dramatic clinical responses of
short duratione. are also the treatment of choice for recurrent lo
calor regional disease
10. The most common site of presentation of Merkel cellcarcinoma is the (Choose single best response}a. trunkb. lower extremitiesc. upper extremitiesd. head and necke. oral cavity
QUESTIONS 11-20
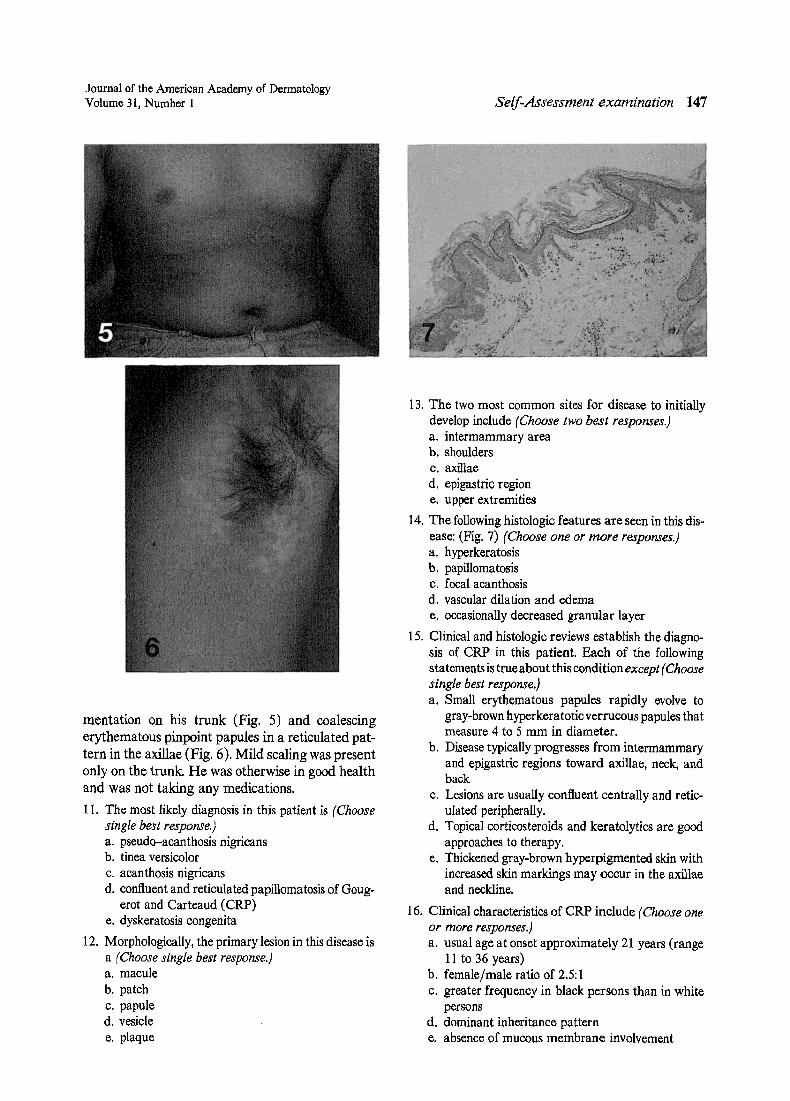
A 17-year-old Oriental boy had a slightly pruriticeruption on his chest, abdomen, axillae, upper arms,and shoulders of 4 years' duration. Physical examination revealed confluent light brown hyperpig-
Journal of the American Academy of DermatologyVolume 31, Number I
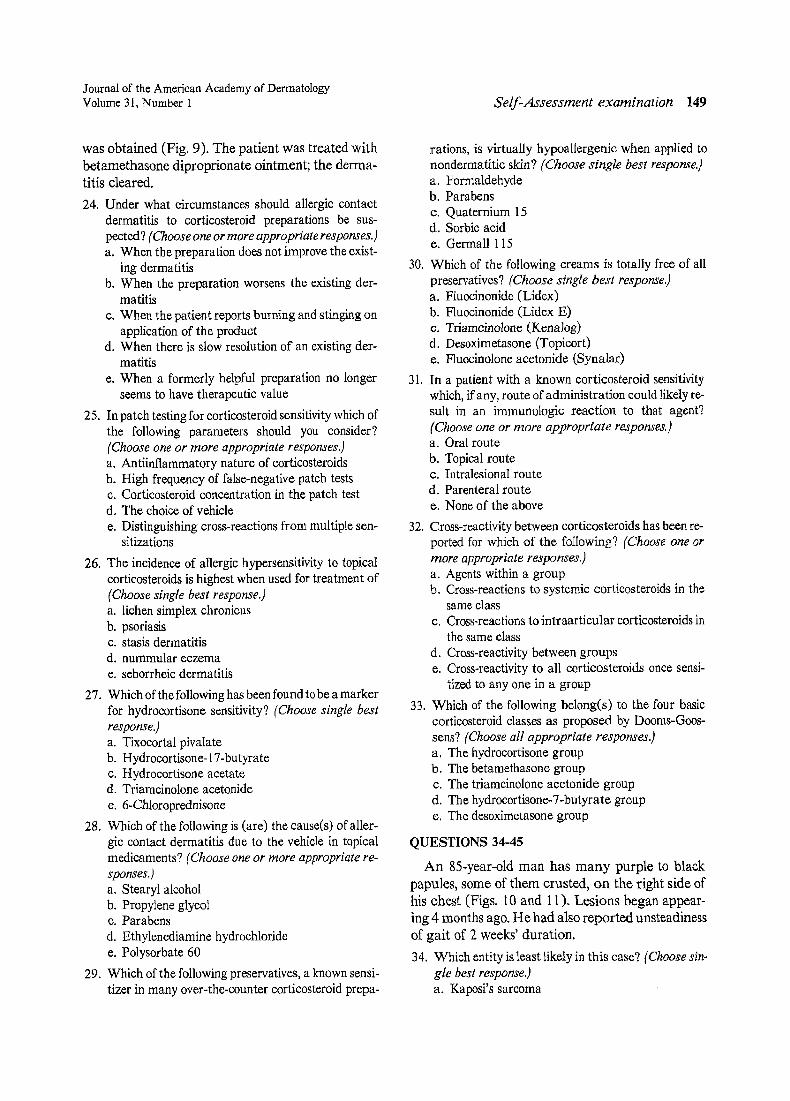
mentation on his trunk (Fig. 5) and coalescingerythematous pinpoint papules in a reticulated pattern in the axillae (Fig. 6). Mild scaling was presentonly on the trunk. He was otherwise in good healthand was not taking any medications.
II. The most likely diagnosis in this patient is (Choosesingle best response.)a. pseudo-acanthosis nigricansb. tinea versicolorc. acanthosis nigricansd. confluent and reticulated papillomatosis of Goug
erot and Carteaud (CRP)e. dyskeratosis congenita
12. Morphologically, the primary lesion in this disease isa (Choose single best response}a. maculeb. patchc. papuled. vesiclee. plaque
Self-Assessment examination 147
13. The two most common sites for disease to initiallydevelop include (Choose two best responses.)a. intermammary areab. shouldersc. axillaed. epigastric regione. upper extremities
14. The followinghistologic features are seen in this disease : (Fig. 7) (Choose one or more responses.)a. hyperkeratosisb. papillomatosisc. focal acanthosisd. vascular dilation and edemae. occasionally decreased granular layer
15. Clinical and histologic reviews establish the diagnosis of CRP in this patient. Each of the followingstatements is trueabout this conditionexcept(Choosesinglebestresponse.]a. Small erythematous papules rapidly evolve to
gray-brown hyperkeratotic verrucous papules thatmeasure 4 to 5 mm in diameter.
b. Disease typically progresses from intermammaryand epigastric regions toward axillae, neck, andback
c. Lesions are usually confluent centrally and reticulated peripherally.
d. Topical corticosteroids and keratolytics are goodapproaches to therapy.
e. Thickened gray-brown hyperpigmented skin withincreased skin markings may occur in the axillaeand neckline.
16. Clinical characteristics of CRP include (Choose oneor moreresponses.)a. usual age at onset approximately 21 years (range
11 to 36 years)b. female/male ratio of 2.5:Ic. greater frequency in black persons than in white
personsd. dominant inheritance patterne. absence of mucous membrane involvement
148 Self-Assessment examination
17. The specific cause of confluent and reticulated papillomatosis is (Choose single best response.)a. a tissue reaction to Pityrosporum orbiculare col-
onizationb. a disorder of keratinizationc. unknownd. an underlying endocrine disordere. a genetically inherited disease
18. The three diseases considered as the papillomatosesinclude (Choose three best responses.)a. pseudo-acanthosis nigricansb. Dowling-Degos diseasec. CRPd. acanthosis nigricanse. dermatopathia pigmentosa reticularis
19. Features of acanthosis nigricans include (Choose oneor more responses.)a. definite association with endocrinopathyb. involvement of the entire body surfacec. mucous membrane involvementd. vast majority of cases around pubertye. hyperpigmented velvety plaques in neck and axil
lae most common
Journal of the American Academy of DermatologyJuly 1994
20. Features of pseudo-acanthosis nigricans include thefollowing (Choose one or more responses.):a. occurrence in obese personsb. predominance in black personsc. frequent involvement of mucous membranesd. reversible condition with weight losse. definite association with endocrinopathy
QUESTIONS 21-33
A 49-year-old white woman had an eczematousdermatitis involving the right ear and right side ofthe neck (Fig. 8). She had been treated by her family physician with polymyxin B sulfate-bacitracinzinc-neomycin sulfate-hydrocortisone ointment(corticosporin) and desonide cream without improvement.
21. The differential diagnosis of this eruption includes(Choose one or more appropriate responses.)a. seborrheic dermatitisb. allergic contact dermatitisc. subacute cutaneous lupus erythematosusd. psoriasise. tinea corporis
22. Which of the following laboratory examinationsmight be useful for diagnosis? (Choose one or moreappropriate responses.)a. Biopsy for routine histologic examinationb. Patch testing with standard screening patch test
tray (Hermal Pharmaceutical Laboratories)c. Potassium hydroxide examination of scaled. Serum for detection of antinuclear antibodye. All of the above
Histologic examination showed a spongiotic dermatitis. Screening patch testing revealed positive resultsto ethylenediamine, fragrance, and neomycin. Fungiwere not identified in affected scale and antinuclearantibodies were negative. The patient was treatedfor a presumed allergic contact dermatitis to neomycin with triamcinolone acetonide 0.025% ointment in a petrolatum base, which resulted in worsening of the dermatitis.
23. Diagnostic evaluation atthis pointinclude(s) (Chooseone or more appropriate responses.)a. patch testing to various corticosteroidsb. challenge with oral corticosteroidsc. patch test to vehicle and preservative allergensd. provocative use testing of corticosteroid ointmentse. all of the above
The patient was then patch tested to triamcinoloneacetonide 0.025% ointment and a moderate reaction
Journal of the American Academy of DermatologyVolume 31, Number I
was obtained (Fig. 9). The patient was treated withbetamethasone diproprionate ointment; the dermatitis cleared.
24. Under what circumstances should allergic contactdermatitis to corticosteroid preparations be suspected? (Choose oneormoreappropriate responses.)a. When the preparation does not improve the exist
ing dermatitisb. When the preparation worsens the existing der
matitisc. When the patient reports burning and stinging on
application of the productd. When there is slow resolution of an existing der
matitise. When a formerly helpful preparation no longer
seems to have therapeutic value
25. In patch testing for corticosteroid sensitivitywhich ofthe following parameters should you consider?(Choose one or more appropriate responses.)a. Antiinflammatory nature of corticosteroidsb. High frequency of false-negative patch testsc. Corticosteroid concentration in the patch testd. The choice of vehiclee. Distinguishing cross-reactions from multiple sen
sitizations
26. The incidence of allergic hypersensitivity to topicalcorticosteroids is highest when used for treatment of(Choose singlebest response.)a. lichen simplex chronicusb. psoriasisc. stasis dermatitisd. nummular eczemae. seborrheic dermatitis
27. Which of the followinghas been found tobe a markerfor hydrocortisone sensitivity? (Choose single bestresponse]a. Tixocortal pivalateb. Hydrocortisone-17-butyratec. Hydrocor tisone acetated. Triamcinolone acetonidee. 6-Chloroprednisone
28. Which of the following is (are) the cause(s) of allergic contact dermatitis due to the vehicle in topicalmedicaments? (Choose oneor more appropriate responses.)a. Stearyl alcoholb. Propylene glycolc. Parabensd. Ethylenediamine hydrochloridee. Polysorbate 60
29. Which ofthe following preservatives, a known sensitizer in many over-the-counter corticosteroid prepa-
Self-Assessment examination 149
rations, is virtually hypoallergenic when applied tonondermatitic skin? (Choose single best response]a. Formaldehydeb. Parabensc. Quaternium 15d. Sorbic acide. Germall 115
30. Which of the following creams is totally free of allpreservatives? (Choosesingle best response]a. Fluocinonide (Lidex)b. Fluocinonide (Lidex E)c. Triamcinolone (Kenalog)d. Desoximetasone (Topicort)e. Fluocinolone acetonide (Synalar)
31. In a patient with a known corticosteroid sensitivitywhich, if any, route of administration could likelyresult in an immunologic reaction to that agent?(Choose one or more appropriate responses.}a. Oral routeb. Topical routec. Intralesional routed. Parenteral routee. None of the above
32. Cross-reactivity between corticosteroids has been reported for which of the following? (Choose one ormore appropriate responses.)a. Agents within a groupb. Cross-reactions to systemic corticosteroids in the
same classc. Cross-reactionsto intraarticular corticosteroids in
the same classd. Cross-reactivity between groupse. Cross-reactivity to all corticosteroids once sensi
tized to anyone in a group
33. Which of the following belong(s) to the four basiccorticosteroid classes as proposed by Dooms-Goossens? (Choose all appropriate responses]a. The hydrocortisone groupb. The betamethasone groupc. The triamcinolone acetonide groupd. The hydrocortisone-7-butyrate groupe. The desoximetasone group
QUESTIONS 34-45
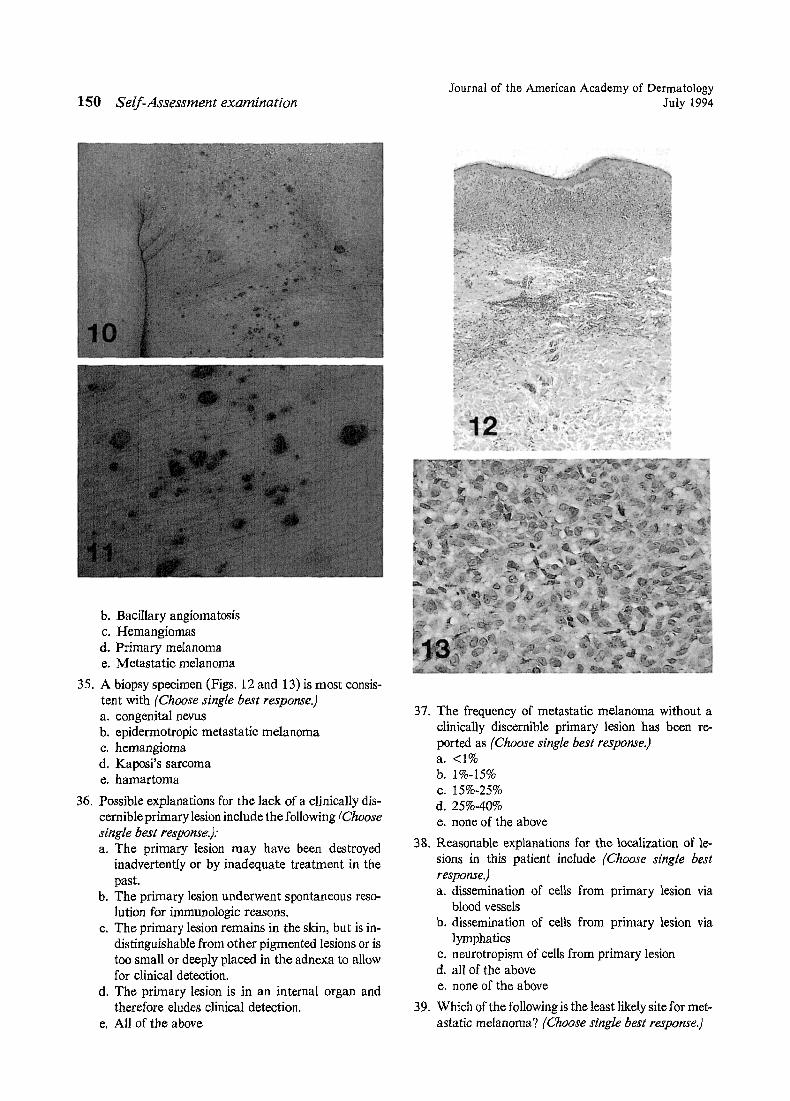
An 85-year-old man has many purple to blackpapules, some of them crusted, on the right side ofhis chest (Figs. 10 and 11). Lesions began appearing 4 months ago. He had also reported unsteadinessof gait of 2 weeks' duration.
34. Which entity is least likely in this case? (Choose single best response.)a. Kaposi's sarcoma
150 Self-Assessment examination
b. Bacillary angiomatosisc. Hemangiomasd. Primary melanomae. Metastatic melanoma
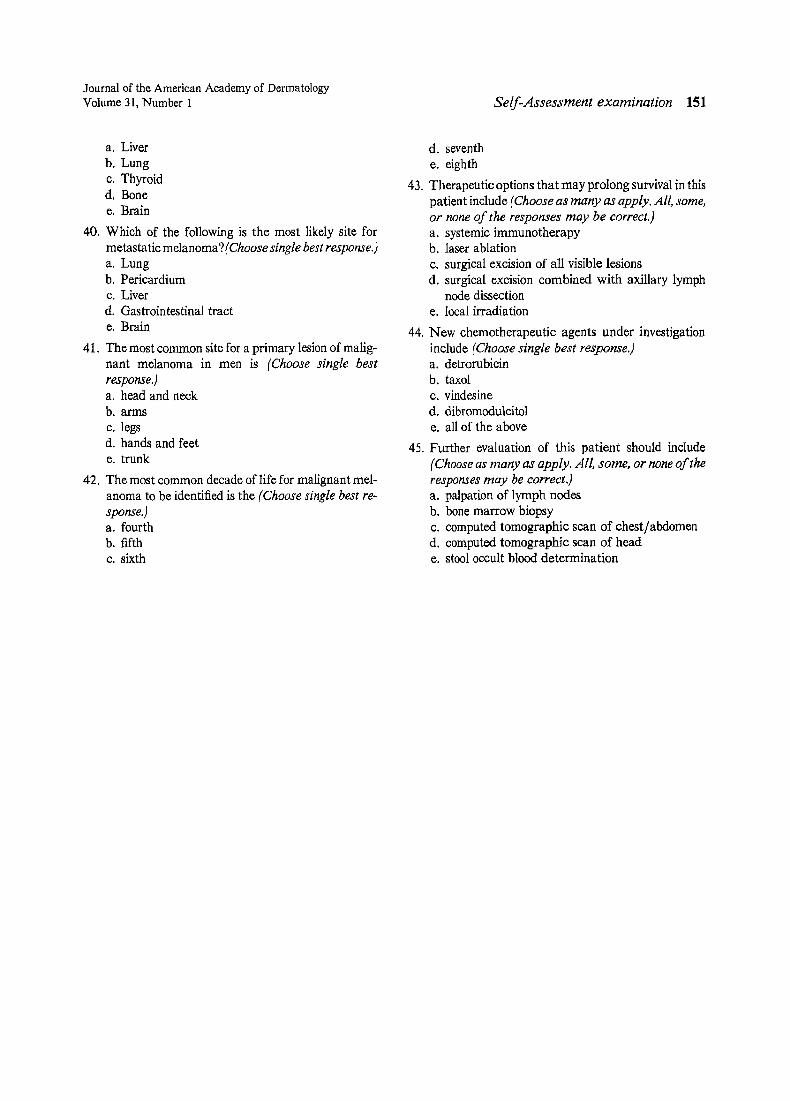
35. A biopsy specimen (Figs. 12 and 13) is most consistent with (Choose singlebest response.)a. congenital nevusb. epidermotropic metastatic melanomac. hemangiomad. Kaposi's sarcomae. hamartoma
36. Possible explanations for the lack of a clinically discernibleprimary lesion includethe following (Choosesingle best response]:a. The primary lesion may have been destroyed
inadvertently or by inadequate treatment in thepast.
b. The primary lesion underwent spontaneous resolution for immunologic reasons.
c. The primary lesion remains in the skin, but is indistinguishable from other pigmented lesions or istoo small or deeply placed in the adnexa to allowfor clinical detection.
d. The primary lesion is in an internal organ andtherefore eludes clinical detection.
e. All of the above
Journal of the American Academy of DermatologyJuly 1994
37. The frequency of metastatic melanoma without aclinically discernible primary lesion has been reported as (Choose single best response.)a. <1%b. 1%-15%c. 15%-25%d.25%-40%e. none of the above
38. Reasonable explanations for the localization of lesions in this patient include (Choose single bestresponse.]a. dissemination of cells from primary lesion via
blood vesselsb. dissemination of cells from primary lesion via
lymphaticsc. neurotropism of cells from primary lesiond. all of the abovee. none of the above
39. Which of the following is the least likely site for metastatic melanoma? (Choose singlebest response]
Journal of the American Academy of DermatologyVolume 31, Number 1
a. Liverb. Lungc. Thyroidd. Bonee. Brain
40. Which of the following is the most likely site formetastatic melanoma?(Choose single bestresponse.)a. Lungb. Pericardiumc. Liverd. Gastrointestinal tracte. Brain
41. The most common site for a primary lesion of malignant melanoma in men is (Choose single bestresponse.)a. head and neckb. armsc. legsd. hands and feete. trunk
42. The most common decade of life for malignant melanoma to be identified is the (Choose single bestresponse.)a. fourthb. fifthc. sixth
Self-Assessment examination 151
d. seventhe. eighth
43. Therapeutic options that may prolong survival in thispatient include (Choose as many as apply.All, some,or none of the responses may be correct.)a. systemic immunotherapyb. laser ablationc. surgical excision of all visible lesionsd. surgical excision combined with axillary lymph
node dissectione. local irradiation
44. New chemotherapeutic agents under investigationinclude (Choose single best response.)a. detrorubicinb. taxolc. vindesined. dibromodulcitole. all of the above
45. Further evaluation of this patient should include(Choose as many as apply. All, some, or none oftheresponses may be correci.)a. palpation of lymph nodesb. bone marrow biopsyc. computed tomographic scan of chest/abdomend. computed tomographic scan of heade. stool occult blood determination