Eur Respir J, 1996, 9, 1029–1054 DOI: 10.1183/09031936.96.09051029 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1996 European Respiratory Journal ISSN 0903 - 1936 Epidemiological studies of the respiratory effects of air pollution M.D. Lebowitz Epidemiological studies of the respiratory effects of air pollution. M.D. Lebowitz. ERS Journals Ltd 1996. ABSTRACT: Environmental epidemiological studies of the health effects of air pollu- tion have been major contributors to the understanding of such effects. The chronic effects of atmospheric pollutants have been studied, but, except for the known res- piratory effects of particulate matter (PM), they have not been studied conclu- sively. There are ongoing studies of the chronic effects of certain pollutant classes, such as ozone, acid rain, airborne toxics, and the chemical form of PM (including diesel exhaust). Acute effects on humans due to outdoor and indoor exposures to several gases/fumes and PM have been demonstrated in epidemiological studies. However, the effects of these environmental factors on susceptible individuals are not known conclu- sively. These acute effects are especially important because they increase the human burden of minor illnesses, increase disability, and are thought to decrease produc- tivity. They may be related to the increased likelihood of chronic disease as well. Further research is needed in this latter area, to determine the contributions of the time-related activities of individuals in different microenvironments (outdoors, in homes, in transit). Key elements of further studies are the assessment of total expo- sure to the different pollutants (occurring from indoor and outdoor sources) and the interactive effects of pollutants. Major research areas include determination of the contributions of indoor sources and of vehicle emissions to total exposure, how to measure such exposures, and how to measure human susceptibility and responses (including those at the cellular and molecular level). Biomarkers of exposures, doses and responses, including immuno- chemicals, biochemicals and deoxyribonucleic acid (DNA) adducts, are beginning to promote some basic knowledge of exposure-response, especially the mechanisms. These will be extremely useful additions to standard physiological, immunological, and clinical instruments, and the understanding of biological plausibility. The out- comes of all this work will be the management of risks and the prevention of res- piratory diseases related to air pollution. Eur Respir J., 1996, 9, 1029–1054. Correspondence: M.D. Lebowitz Pulmonary & Crit. Care Med. Sec. Dept of Medicine Respiratory Sciences Center Room 2332 AHBC Tucson Arizona 85724 USA Keywords: Air pollution asthma chronic bronchitis environment epidemiology Received: December 28 1996 Accepted for publication January 3 1996 This work was supported by USA-NHLBI SCOR Grant HL14136. Previously published reviews of this series 1. Sandström T. Respiratory effects of air pollutants: experimental studies in humans. Eur Respir J 1995; 8: 976–995. 2. Chitano P, Hosselet JJ, Mapp CE, Fabbri LM. Effects of oxidant air pollutants on the respiratory system: insights from experi- mental animal research. Eur Respir J 1995; 8: 1357–1371. 3. Heyder J, Takenaka S. Long-term canine exposure studies with ambient air pollu- tants. Eur Respir J 1996; 9: 571–584. This review of epidemiological studies of the respira- tory effects of exposures to air pollutants follows excel- lent reviews of experimental studies in animals and humans that have recently appeared in the Journal [1–3]. It has relied both on prior reviews of the topic and on the exten- sive literature of the major research reports. It includes, as requested, evaluations of the exposure-response rela- tionships for different respiratory effects and some risk assessment, and also attempts to look at the important issues and hypotheses awaiting further research. Historically, the clearest evidence for an association between air pollution and health outcomes in populations was from acute mortality epidemics. There were a num- ber of well-known acute air pollution episodes [4–10]. These episodes had greatly increased concentrations of sulphur oxides (SO 2 ) and particulate matter (PM), and often increased acidity, usually due to unfavourable meteo- rological conditions and air stagnation. A very signifi- cant increase in daily mortality occurred, primarily among persons with prior cardiac and respiratory disease. These epidemics led to the subsequent epidemiological inves- tigations of environmental health effects. Some guidelines for epidemiological investigations In order to understand exposures to contaminants and the resulting health impacts, it has been suggested [11, 12] that one needs to evaluate: 1) the type of viable and nonviable particles; 2) the various sources of contami- nants and the physicochemical factors leading to expo- sures; 3) the chemical nature of the complex mixtures in the air and the atmospheric physical (including meteo- rological) interactions; 4) the nature and mechanisms of the morbidity effects associated with the contaminants, including the range and distribution of sensitivity in the population; and 5) the methods of evaluation. Epidemio- logical methods provide the opportunity to study pollu- tants and interactions in complex environments within this framework. Assessments differ with the different SERIES 'RESPIRATORY EFFECTS OF AIR POLLUTION' Edited by P. Paoletti and U. Costabel
Transcript
Eur Respir J, 1996, 9, 1029–1054DOI: 10.1183/09031936.96.09051029Printed in UK - all rights reserved
Copyright ERS Journals Ltd 1996European Respiratory Journal
ISSN 0903 - 1936
Epidemiological studies of the respiratory effects of air pollution
M.D. Lebowitz
Epidemiological studies of the respiratory effects of air pollution. M.D. Lebowitz. ERSJournals Ltd 1996.ABSTRACT: Environmental epidemiological studies of the health effects of air pollu-tion have been major contributors to the understanding of such effects. The chroniceffects of atmospheric pollutants have been studied, but, except for the known res-piratory effects of particulate matter (PM), they have not been studied conclu-sively. There are ongoing studies of the chronic effects of certain pollutant classes,such as ozone, acid rain, airborne toxics, and the chemical form of PM (includingdiesel exhaust).
Acute effects on humans due to outdoor and indoor exposures to several gases/fumesand PM have been demonstrated in epidemiological studies. However, the effectsof these environmental factors on susceptible individuals are not known conclu-sively. These acute effects are especially important because they increase the humanburden of minor illnesses, increase disability, and are thought to decrease produc-tivity. They may be related to the increased likelihood of chronic disease as well.Further research is needed in this latter area, to determine the contributions of thetime-related activities of individuals in different microenvironments (outdoors, inhomes, in transit). Key elements of further studies are the assessment of total expo-sure to the different pollutants (occurring from indoor and outdoor sources) andthe interactive effects of pollutants.
Major research areas include determination of the contributions of indoor sourcesand of vehicle emissions to total exposure, how to measure such exposures, and howto measure human susceptibility and responses (including those at the cellular andmolecular level). Biomarkers of exposures, doses and responses, including immuno-chemicals, biochemicals and deoxyribonucleic acid (DNA) adducts, are beginningto promote some basic knowledge of exposure-response, especially the mechanisms.These will be extremely useful additions to standard physiological, immunological,and clinical instruments, and the understanding of biological plausibility. The out-comes of all this work will be the management of risks and the prevention of res-piratory diseases related to air pollution.Eur Respir J., 1996, 9, 1029–1054.
Correspondence: M.D. LebowitzPulmonary & Crit. Care Med. Sec.Dept of MedicineRespiratory Sciences CenterRoom 2332 AHBCTucsonArizona 85724USA
Keywords: Air pollutionasthmachronic bronchitisenvironmentepidemiology
Received: December 28 1996Accepted for publication January 3 1996
This work was supported by USA-NHLBISCOR Grant HL14136.
Previously published reviews of this series1. Sandström T. Respiratory effects of airpollutants: experimental studies in humans.Eur Respir J 1995; 8: 976–995.2. Chitano P, Hosselet JJ, Mapp CE, FabbriLM. Effects of oxidant air pollutants onthe respiratory system: insights from experi-mental animal research. Eur Respir J 1995;8: 1357–1371.3. Heyder J, Takenaka S. Long-term canineexposure studies with ambient air pollu-tants. Eur Respir J 1996; 9: 571–584.
This review of epidemiological studies of the respira-tory effects of exposures to air pollutants follows excel-lent reviews of experimental studies in animals and humansthat have recently appeared in the Journal [1–3]. It hasrelied both on prior reviews of the topic and on the exten-sive literature of the major research reports. It includes,as requested, evaluations of the exposure-response rela-tionships for different respiratory effects and some riskassessment, and also attempts to look at the importantissues and hypotheses awaiting further research.
Historically, the clearest evidence for an associationbetween air pollution and health outcomes in populationswas from acute mortality epidemics. There were a num-ber of well-known acute air pollution episodes [4–10].These episodes had greatly increased concentrations ofsulphur oxides (SO2) and particulate matter (PM), andoften increased acidity, usually due to unfavourable meteo-rological conditions and air stagnation. A very signifi-cant increase in daily mortality occurred, primarily amongpersons with prior cardiac and respiratory disease. These
epidemics led to the subsequent epidemiological inves-tigations of environmental health effects.
Some guidelines for epidemiological investigations
In order to understand exposures to contaminants andthe resulting health impacts, it has been suggested [11,12] that one needs to evaluate: 1) the type of viable andnonviable particles; 2) the various sources of contami-nants and the physicochemical factors leading to expo-sures; 3) the chemical nature of the complex mixtures inthe air and the atmospheric physical (including meteo-rological) interactions; 4) the nature and mechanisms ofthe morbidity effects associated with the contaminants,including the range and distribution of sensitivity in thepopulation; and 5) the methods of evaluation. Epidemio-logical methods provide the opportunity to study pollu-tants and interactions in complex environments withinthis framework. Assessments differ with the different
SERIES 'RESPIRATORY EFFECTS OF AIR POLLUTION'Edited by P. Paoletti and U. Costabel
M.D. LEBOWITZ1030
mechanisms (allergic, infective or irritant/toxic). Epidemio-logical investigators can study effects of real-life expo-sures in various population subgroups, even though itmay be difficult to attribute the specific adverse healtheffects observed to concentrations of any one pollutant.Epidemiology also needs to resolve the methodologicalproblems relating to the measures of exposure, the mea-sures of effect (and avoidance of bias), and the use ofcovariables and confounding variables [4–6, 12–14].
Without adequate exposure data, epidemiological stud-ies may be of little use in studying such refined issues[8, 15, 16]. Personal exposure factors, including time-activity patterns, may cause a given subject to experi-ence pollution levels very different from those measuredat a nearby fixed monitoring station [8, 12, 15]. Forinstance, exposure to sources of indoor pollution maybe critical, given that the majority of time is spent in-doors, and those exposures may have deleterious respi-ratory health effects, as will be discussed [8, 10, 16].
The epidemiological evaluation of the pathogenesisand natural history of respiratory diseases requires exami-nation of human susceptibility and sensitivity of speci-fic subgroups to air pollution [4, 5, 7, 11–15, 17–24].Susceptibility may have been innate (e.g. genetic) and/or induced by events/exposures (infectious, allergenicand/or irritant); physiological and immunological mark-ers of susceptibility and sensitization continue to be found.Those who are susceptible usually hyperrespond whenexposed. Asthmatics are excellent examples of indivi-duals who were susceptible to air pollutants; and once sen-sitized or inflicted with the disease, they are susceptibleto the effects of many environmental (and nonenvironmen-tal) triggers. Furthermore, differences between smokersand nonsmokers suggest that smokers are less responsivethan nonsmokers. Smokers have altered lung functionand an increase in mucus, both of which could influencedose in the different regions of the lung. They also havesmaller airway calibre, predisposing them to bronchialresponsiveness. Age also determines susceptibility; chil-dren appear to be more susceptible. The elderly may bemore susceptible, due mainly to existing disease. Pre-existing conditions are often manifestations of susceptibi-lity, which typically implies that the individual is endowedwith some physiological or biochemical characteristicthat may lead to an enhanced response. The underlyingcharacteristic is not usually idiosyncratic, but shared byothers, usually a small fraction of the population. Like-wise, it is possible that some subgroups have host char-acteristics that protect them or permit them to adapt toexposures. Also, factors associated with lower socioe-conomic status, including crowding and nutrition, maypredispose individuals or increase risk. Even withoutobvious susceptibility, approximately 10–20% of healthysubjects will have symptomatic or lung function respons-es to irritants [5, 13, 14].
Pollutant factors of importance
The deposition of gaseous pollutants depends on theirreactivity, whether they are freely gaseous or adsorbedon particles, and whether they are inhaled through thenose or mouth. Highly reactive-hydroscopic gases (e.g.SO2) are absorbed almost entirely in the nose during
normal nasal breathing; on the other hand, ozone (O3)readily can reach the alveoli. Exercise during exposureincreases the pollutant effect on ventilatory function.Deposition also depends on enlargement of aerosols andany neutralization that occurs in the airways. Meta-bolism will also determine the fate of some gaseous pollu-tants [8, 10, 14, 25]. Deposition of PM and associatedeffects depend on the size of particles as well as on thetype of breathing; tracheobronchial deposition occurs witha fraction of 0.14–0.36 for 10 µm aerodynamic diame-ter (Dae) particles, 0.09–0.27 for 12 µm Dae; it is 0.12under maximally deep inhalation of 16.4 µm Dae. "...there can be a significant deposition of particles >10 µmDae" [5]. Lesser deposition can occur even with largerparticles, including pollen [26].
Short-term exposures and acute effects
Mortality
Acute mortality responses appear to occur in nonepi-demic conditions as well as epidemic. Table 1 providesa compendium of the studies of short-term mortality asso-ciated with air pollutants and meteorology.
Sulphur oxides and particulates. The best-known episodeof mortality associated with sulphur oxides (SOx) andPM was the London fog of December 1952. About 4,000excess deaths occurred, predominantly attributed to bron-chitis/pneumonia [4, 5, 10]. Subsequent episodes inLondon were also documented (table 1), and multiple re-analyses have occurred and been reviewed [5, 10, 29,30, 42, 50]. Some analyses indicate that acidic sulphurmay have played a role [10] (Environmental ProtectionAgency (EPA), in press). A study of the Donora episodeof 1948 also found excess mortality in those with exist-ing disease [51]. There may also have been effects inchildren (op cit. [18]).
In New York City, excess deaths were also found insome episodes, mostly among persons 45 yrs of age andolder, due to influenza, pneumonia and cardiopulmonarycauses; these studies, negative studies, and reanalyseshave been presented and reviewed [4–6, 9, 10, 32]. Simi-lar analyses have been conducted at other times in othercities under conditions of lower pollution; the quantita-tive studies are presented in table 1 and the qualitativestudies have been reviewed previously [53]. Episodesof the duration and intensity reported before the early1960s no longer seem to occur in the cities of the UnitedStates and Western Europe, but probably occur in EasternEurope.
As noted above, not all quantitative studies agree onresults even with the same or similar data bases for thesame locations. This occurred even with inclusion ofweather variables, lag effects, and controls for effects ofother pollutants in the analyses of the death certificatefiles. Some studies, as noted, have found PM to be theremaining significant pollutant, whilst others have foundSOx to be more important; some have found sulphate(the particulate SOx) to be the key pollutant [53]; andconflicting results concerning the effects of acidity con-tinue to appear [46, 54]. Some qualitative studies using
EPIDEMIOLOGICAL STUDIES OF AIR POLLUTION EFFECTS 1031T
able
1.
–
Qua
ntita
tive
rela
tions
hip
of s
hort
-ter
m e
xpos
ure
to d
aily
mor
talit
y 24 h
exp
osur
e µ
g·m
-3
Firs
tau
thor
Y
ear
[R
ef]
L
ocat
ion
SO
2Sm
oke
TSP
PM
10R
esul
ts
LO
GA
N19
53
[27]
L
ondo
n, U
K 1
952
>10
00
>10
00
Thr
eefo
ld i
ncre
ase
duri
ng 5
day
fog
*M
inis
try
Hea
lth
1954
[28]
MA
RT
IN19
60
[29]
L
ondo
n, U
K 1
958–
1960
50
0**
500*
* Si
gnif
ican
t in
crea
se w
hen
exce
edin
g lim
its s
how
n*L
AW
TH
ER
1963
[3
0]
Lon
don,
UK
195
8–19
59
710
750
1.25
fol
d in
crea
seB
UE
CH
LE
Y19
73
[31]
N
ew Y
ork,
USA
50
0 C
orre
latio
n; 2
% e
xces
s at
lev
el s
how
n* C
OH
s N
S
1962
–196
6P O
PE19
92
[32]
Sa
lt L
ake
City
, U
T,
low
47
–297
Si
gnif
ican
t in
crea
se i
n m
orta
lity
(50–
100
µg·
m-3
) -
7.5%
USA
in r
espi
rato
ry d
eath
s (6
.3·d
ay-1
) -
8% i
n to
tal
deat
hs;
NS
in s
umm
er o
r w
ith o
ther
pol
luta
nts
in m
odel
LY
ON
1995
[3
3]
Salt
Lak
e C
ity,
USA
lo
w
47–2
97
No
sign
ific
ant
incr
ease
ove
rall;
som
e in
crea
se i
n th
e el
derl
ySC
HW
AR
TZ
1992
[3
4]
Phila
delp
hia,
PA
, U
SA
Med
=47
<
380
7% i
ncre
ase
in t
otal
mor
talit
y pe
r 10
0 µ
g·m
-2
incr
ease
in
TSP
; w
eath
er,
seas
on,
SO2
in m
odel
sL
I19
95[3
5]Ph
ilade
lphi
a, P
A,
USA
Med
=47
<38
0N
o si
gnif
ican
t in
crea
seS C
HW
AR
TZ
1992
[34]
Steu
benv
ille,
OH
,<
7–>
55<
36–>
209
4% i
ncre
ase
in t
otal
mor
talit
y pe
r 10
0 µ
g·m
-3in
crea
seU
SAin
TSP
; w
eath
er,
seas
on,
SO2
in m
odel
sH
AT
ZA
KIS
1986
[36]
Ath
ens,
Gre
ece
≥80
55–2
50Sm
all
sign
ific
ant
effe
ct o
f SO
2(n
ot s
mok
e) o
n m
orta
lity
in t
he e
lder
lyK
AT
SOU
YA
NN
I19
93[3
7]A
then
s an
d 14
Gre
ek≥8
055
–250
No
inde
pend
ent
effe
ct o
f ei
ther
SO
2or
sm
oke;
Citi
esin
depe
nden
t ef
fect
of
tem
p. (
>30
°C)
and
som
e in
tera
ctio
nof
hig
h te
mp.
and
hig
h SO
2; e
ffec
t of
O3
NS
TO
UL
OU
MI
1994
[38]
Ath
ens
78–3
06Si
gnif
ican
t 3.
4% i
ncre
ase
(50–
100
µg·
m-3
) in
tot
alm
orta
lity,
3 d
ay l
ag;
NS
with
SO
2, C
O i
n m
odel
F AIR
LE
Y19
90[3
9]Sa
n Jo
se,
CA
, U
SAlo
w<
150·
day-
10.
12%
incr
ease
in m
orta
lity
per
incr
ease
of
10 µ
g·m
-3PM
10SH
UM
WA
Y19
88[4
0]L
os A
ngel
es,
CA
,lo
w>
100#
1.1%
inc
reas
e in
mor
talit
y pe
r in
crea
se o
f 10
µg·
m-3
PM10
AB
BE
Y19
95[4
1]L
os A
ngel
es a
ndlo
w>
200
>10
0N
o in
crea
se i
n to
tal
or c
ause
-spe
cifi
c m
orta
lity
othe
r C
A a
reas
KIN
NE
Y19
95[4
2]L
os A
ngel
es a
ndlo
w58
–177
No
incr
ease
in
tota
l or
cau
se-s
peci
fic
mor
talit
yot
her
CA
are
asD
OC
KE
RY
1992
[43]
St.
Lou
is,
MO
, U
SA<
34 µ
g·m
-328
–97
Sign
ific
ant
8% i
ncre
ase
in t
otal
mor
talit
y (5
0–10
0 µ
g·m
-3);
NS
with
O3
in m
odel
†
Kin
gsto
n, T
N,
USA
<34
µg·
m-3
30–6
7N
o si
gnif
ican
t in
crea
se i
n m
orta
lity†
SCH
WA
RT
Z19
93[4
4]B
irm
ingh
am,
AL
, U
SA?
48–1
63Si
gnif
ican
t 5%
inc
reas
e (5
0–10
0 µ
g·m
-3)
in t
otal
mor
talit
y,3
day
lag;
no
othe
r A
P in
mod
el†
OZ
KA
YN
AK
1994
[45]
Tor
onto
, C
anad
a?
40–9
6Si
gnif
ican
t 2.5
% in
crea
se (
50–1
00 µ
g·m
-3)
in to
tal m
orta
lity;
no o
ther
AP
in m
odel
†I T
O19
95[4
6]C
hica
go,
IL,
USA
?38
–128
Sign
ific
ant 2
.5%
incr
ease
(50
–100
µg·
m-3
) in
tota
l mor
talit
y,C
O i
n m
odel
, ≤3
day
lag
†S T
YE
R19
95[4
7]C
hica
go,
IL,
USA
?37
–365
No
sign
ific
ant
incr
ease
in
tota
l m
orta
lity;
3 d
ay l
ag†
OST
RO
1995
[48]
Sant
iago
, C
hile
?11
5–36
7Si
gnif
ican
t 2.
6–7%
inc
reas
e in
tot
al m
orta
lity;
50–
100
µg·
m-3
), ≤
4 da
y la
g, o
ther
AP
in m
odel
s†X
U19
94[4
9]B
eijin
g, C
hina
Ann
ual
Ann
ual
Sign
ific
ant
doub
ling
of r
espi
rato
ry d
isea
se m
ostly
rel
ated
x=93
– 3
90x=
108
vs35
0to
SO
2an
d T
SP;
only
SO
2si
gnif
ican
t fo
r ot
her
mor
talit
yan
d in
win
ter;
oth
er f
acto
rs i
n m
odel
s*:
mul
tiple
rea
naly
sis
perf
orm
ed;
othe
r st
udie
s of
a l
esse
r qu
antit
ativ
e na
ture
gen
eral
ly c
onfi
rmat
ory,
inc
ludi
ng o
ne i
n T
he N
ethe
rlan
ds (
EPA
, 19
82 [
5]);
aci
d m
ay a
lso
have
bee
nin
volv
ed (
WH
O 1
987
[10]
; A
TS
1978
[4]
; It
o et
al.
1995
[46
]);
**:
thre
shol
ds a
ccor
ding
to
WH
O (
1987
);
‡: a
djus
ted
valu
e <
150
µg·
m-3
; #:
fro
m O
stro
& A
bbey
; †:
fro
m E
PA P
MC
rite
ria
Doc
umen
t (1
995)
. E
PA:
Env
iron
men
tal
Prot
ectio
n A
genc
y; W
HO
: W
orld
Hea
lth O
rgan
izat
ion;
AT
S: A
mer
ican
Tho
raci
c So
ciet
y; N
S:no
nsig
nifi
cant
; PM
10:
part
icul
ate
mat
ter
with
aer
odyn
amic
diam
eter
<10
µm
; T
SP:
tota
l su
spen
ded
part
icul
ates
; te
mp:
tem
pera
ture
; x:
mea
n; A
P: a
ir p
ollu
tant
; C
OH
: co
effi
cien
t of
haz
e; M
ed:
med
ian.
different general linear models (GLMs) also demonstratesome disagreement of results for the same cities, thoughmost are in agreement when PM or SO2 concentrationsare above the World Health Organization (WHO)/Euro-pean (EURO) [10] lower limits of such effects, shownin table 1, which are similar to those shown by EPA [4].However, current estimates include estimates below thecurrent standards and guidelines (table 2), which deservefurther discussion.
The studies by certain groups using Poisson & GEEstatistical methods appear to give consistent estimates ofmortality excesses related to exposure to PM, as seen intable 2. The use of these methods as well as other GLMsin theoretically similar data sets which did not yield simi-lar results (table 1), has raised questions about the useof certain models [42]. Disagreements have also arisenas to the biological plausibility of the results as well asaspects of causality [55–57], and the appropriateness ofthe exposure assessments. Current discussions have fav-oured the likelihood that the elderly, cardiopulmonarycases are the most likely to be affected.
The associations may not be simple linear relation-ships, and other determinants of day-to-day changes inmortality make it difficult to specify a pollutant con-centration at which excess deaths begin to occur [4, 12,57]. Many intervening factors, such as temperature ex-tremes, influenza epidemics, holiday weekends, and sea-son of the year, have strong effects on the day-to-daynumber of deaths and may enhance or minimize the effectof air pollution [12, 31, 57–60]. Thus, there is still noagreement as to how many deaths may be attributedspecifically to the air pollutants [4, 5, 61]. There is littledisagreement that the effects of temperature still pre-dominate.
Ozone/oxidants, nitrogen dioxide and carbon monoxide.Temporal analyses of mortality associated with ozone(O3) or total oxidants (Ox) have been less frequent, thoughozone has been incorporated in some of the PM studies.In these latter studies, the effect of ozone is often asstrong as that of PM [52]. Studies in various localeshave found high temperatures to be the primary sourceof mortality, though O3 is sometimes concurrent in lin-ear model solutions with temperature and other pollu-tants [10, 13, 37, 41, 62]. There has been a study in LosAngeles that showed significant associations both of O3
and nitrogen dioxide (NO2) with total and cause-specificmortality [42]; PM was not significant. No lowest obser-ved effect levels (LOELs) have been defined for acutemortality associated with O3 or NO2.
Two studies have shown associations of carbon mon-oxide (CO) with mortality in the Los Angeles area; bothcontrolled for temperature and other pollutants. The first[63] showed only the effect of CO on cardiovascularmortality. The second [40] showed effects both of COand PM on total and cardiovascular mortality.
Summary of current knowledge. Air pollutants togetherwith temperature can cause increases in short-term mor-tality. The issues of such mortality increases have beendiscussed frequently in the past few years (e.g. [52]).Recent findings have generated hypotheses, and there hasbeen agreement that further studies are needed usingappropriate exposure and response measures, and thatstatistical analyses have to be replicated using the samedata sets as used in the prior analyses and investigations.The major statistical issues addressed have indicated thatnone of the methods utilized were invalid per se. Use ofany of the methods needs to include their appropriateuse, the nature and number of variables and of cases,and the nature of temporal trends. Independence and co-linearity of observations and confounding need to beaddressed further, as should testing of assumptions, het-erogeneity, and "sensitivity" (ibid.). As prior differencesin results could be related to any of these factors (ibid.,[6, 55–57]), reanalyses are underway to examine such fac-tors; preliminary results differ quantitatively but not qua-litatively from prior results [64]. New study designsshould have the ability to explore nonlinear thresholdmodels [55]. Evaluation continues of mortality effects inthose (especially the elderly) with existing cardiopul-monary diseases; it is likely that some small shorteningof life (or increased morbidity and disability) could occurunder the circumstances described in studies showingsignificant associations.
Interpretations have too often depended on data fromstationary monitors when individuals' exposures are notreflected by such measurements. Furthermore, the sizeand species of the particulate should be critical aspectsof the exposure measurements, especially as differentparticles produce different physiological and pathologi-cal responses. It was concluded that one needed epide-miological studies that utilized appropriate monitors (with
M.D. LEBOWITZ1032
Table 2. – PM10-acute respiratory and cardiovascular mortality effects studies based on various PM measures*
Original PM Mean % change 95% CImeasurement equivalent per 10 µg·m-3
Health outcome Location (lag) PM10 PM10 equivalent
Respiratory mortality Birmingham, AL, USA PM10 (3 day) 48 1.5 -5.8–9.4Utah Valley, UT, USA PM10 (5 day) 47 3.7 0.7–6.7Philadelphia, PA, USA TSP (2 day) 40 3.3 0.1–6.6Santa Clara, CA, USA COH 35 3.5 1.5–5.6
Cardiovascular mortality Birmingham, AL, USA PM10 (3 day) 48 1.6 -1.5–3.7Utah Valley, UT, USA PM10 (5 day) 47 1.8 0.4–3.3Philadelphia, PA, USA TSP (2 day) 40 1.7 1.0–2.4Santa Clara, CA, USA COH 35 0.8 0.1–1.6
*: EPA Summary, unpublished, 1995. PM: particulate matter; PM10: particulate matter with aerodynamic diameter ≤10 µm; 95%CI: 95% confidence interval; TSP: total suspended particulates; COH: hydrocarbon; EPA: Environmental Protection Agency; lag:number of days between air pollution and increase in mortality.
EPIDEMIOLOGICAL STUDIES OF AIR POLLUTION EFFECTS 1033
respect to simplicity, reliability and quality of data) forpersonal exposure assessments within studies designedto focus on the dose-response nature of the PM and otherpollutant effects [52, 56].
Exacerbations of chronic respiratory diseases
PM/SOx and chronic obstructive pulmonary disease(COPD). Some studies of the daily symptom status ofpatients with COPD show relationships between diseasestatus and air pollution concentrations at relatively highconcentrations of sulphur dioxide and particulates [4, 5,65–68], as seen in table 3. Low temperatures can exerta greater effect than air pollution [98]. An extensive seriesof studies on the effects of air pollution on bronchiticpatients was conducted in the UK between 1955 and1970 [65–68]. They showed that exacerbations of dis-ease were associated with high concentrations of smoke(>250 µg·m-3) and SO2 (>500 µg·m-3), although theywere associated with relative increases rather than abso-lute concentrations. Furthermore, in the UK, examina-tion of sickness absence records, of rates of physicianconsultation and of daily records of hospital admissionsthrough the emergency service, showed associations withperiods of heavy air pollution [4, 5]. With decreasing con-centrations of pollutants in the UK, it has been diffi-cult (since 1969) to relate bronchitics' symptom status tovariations in air pollution (Waller, personal communi-cation).
In Barcelona (Spain), SUNYER et al. [99] demonstra-ted that patients with COPD had significantly increa-sed frequencies of visits to emergency rooms related toPM and SO2 during winter, and SO2 predominantly insummer; the increases in visits related to 25 µg·m-3 SO2were 6 and 9%, respectively; other variables were con-trolled in analyses, and the reliability of diagnoses wasconfirmed. In Ontario (Canada), BURNETT et al. [100]found increases for respiratory hospital admissions inthose aged over 65 yrs of 2.8–3.2%, related to 13 µg·m-3
increases in sulphate, after controlling for O3, tempera-ture and season. (A reliability study of COPD hospitaladmissions in nearby Quebec [101] found a 75.5% cor-respondence with national health insurance data). Onlystudies covering an entire catchment area are consideredto show an accurate relationship between admission ratesand air pollution, and clinical studies in general do notappear to represent events in an entire community. Thereliability of the diagnosis in USA hospitals is usuallyconsidered to be less than elsewhere [5, 13].
Higher annual sulphate levels in the USA have alsobeen associated with increased symptoms in cardiopul-monary patients, and symptoms of acute and chronic res-piratory diseases in children and adults [102]. Childrenwith chronic respiratory disease symptomatology in TheNetherlands had decreased peak flow, increased wheezeand increased bronchodilator use associated with totalsuspended particulates (TSP) >110 µg·m-3 in winter[89–90].
PM/O3 and COPD. Various studies in the USA of res-piratory disease hospital admissions have shown rela-tionships with particulate matter with an aerodynamicdiameter ≤10 µm (PM10) and often with O3 after con-trolling for temperature; increases ranged 1.2–13% in the
elderly per 50 µg·m-3 PM10, and 3.5–57% for COPD per100 µg·m-3 PM10 [103–106]; the lack of known catch-ment areas for the hospitals weaken such findings (seebelow). In a field study of adults with symptoms of COPD[21], O3 was significantly related to peak expiratory flow(PEF) after adjustment was made for smoking, relativehumidity, TSP, and gas-stove use, as was TSP after alladjustments; and there was an substantial O3-TSP inter-action.
Asthma. Asthmatics appear to be more susceptible toshort-term peak concentration of air pollutants, althoughthere is a broad range of sensitivity [4, 17, 107, 108].Oral breathing produces larger and quicker effects, asdoes exercise. Air pollution may also enhance the asth-matic patient's reactivity to other stimuli. Recent studieshave reported a pollutant-induced enhancement of theeffect of pharmacological bronchoconstricting agents atrelatively low concentrations of NO2, O3, and SOx, aloneor together (ibid; [11, 85, 109]). Sulphate, sulphuric acidand nitrate affect asthmatics more in experimental stud-ies, especially as potentiators of exercise or bronchocon-strictor challenges; other chemicals may also act aspotentiators. In addition, these pollutants may act as pot-entiators for exposure to allergens and their effects inallergic asthmatics [8, 11, 85, 110, 111]. Thus, the sen-sitivity of asthmatics to external stimuli, indicates thatvarious air pollutants, allergens, and weather conditionsare important classes of the many that can precipitateattacks.
PM/SOx and asthma. In Donora, during the 1948 air pol-lution episode, 88% of those persons with asthma repor-ted respiratory symptoms during the episode, a rate twicethat of the general population [51]. Increased hospitali-zation was found to be related to SO2 in Vancouver,Canada [112]. In Seattle, PM was found to be similarlyrelated [44], but not in Detroit [105]. SAMET et al.[113] also found very little effect of air pollutants onasthma Emergency Room (ER) visits. Other studies haverecorded increased ER visits for persons with asthmaduring air pollution episodes and during other times ofincreased air pollution concentrations ([4, 5].
Increased rates of asthma attacks and reduced lungfunction were noted in epidemiological studies duringepisodes, or days of higher levels of sulphur oxides/PM(tables 3 and 4). Lagged effects of outdoor PM and tem-perature in asthmatics have been seen in various loca-les. Sulphates are more likely than sulphur dioxide aloneto be responsible for many of the adverse health effectstypically associated with SO2, even after rates were adjust-ed for temperature. The studies conducted in several UScities suggest that even 8–15 µg·m-3 (for 24 h) is asso-ciated with the acute effects [102]. COHEN et al. [73]found such relationships for asthma attack rates (repor-ted and confirmed) in all physician diagnosed asthma-tics in one town. Temperature and pollutants also had asynergistic relationship to attacks. Suspended sulphateshowed the strongest relationship; however, suspendednitrate, SO2 and TSP individually, as well as in combi-nation, explained a significant portion of the residual.MOSEHOLM et al. [147] also reported the effects of NO2,SO2 and weather in Denmark; medication use was also
M.D. LEBOWITZ1034T
able
3.
–
Acu
te s
ympt
oms
asso
ciat
ed w
ith a
ir po
lluta
nts
Exp
osur
es
µg·
m-3
#Fi
rst
auth
or
Yea
r
[
Ref
]
Loc
atio
n
SO2
TSP
PM2.
5/B
S
PM10
O3*
N
O2
Res
ults
HA
MM
ER
1976
[6
9]
New
Yor
k, U
SA
286
145
RSP
ann
ual
x
Incr
ease
in
LR
I in
chi
ldre
n w
ithL
OV
E19
81
[70]
L
OE
L†
LO
EL
28
–43
[SO
410
–14]
in
crea
ses
abov
e th
ese
leve
ls
POPE
1991
[7
1]
Salt
Lak
e lo
w
11–1
95lo
wlo
w
Sign
ific
ant
20%
inc
reas
e in
UR
I in
C
ity,
USA
no
nast
hmat
ic c
hild
ren;
LR
I N
S;
tem
p. i
n m
odel
(w
inte
r)PO
PE19
92
[72]
Sa
lt L
ake
low
7–
251
low
lo
w
Sign
ific
ant
20%
inc
reas
e in
LR
I, 2
9%C
ity,
UT
, U
SA
incr
ease
in
coug
h in
sym
ptom
atic
child
ren;
win
ter;
tem
p. b
ut n
ot o
ther
AP
in m
odel
s (N
Sin
asy
mpt
omat
ic c
hild
ren)
CO
HE
N19
72[7
3]C
umbe
rlan
d,20
015
0[S
O4]
[NO
3]In
crea
se i
n as
thm
a at
tack
s w
hen
WV
, U
SAL
OE
L†
LO
EL
thes
e le
vels
exc
eede
d in
tera
ctio
n w
ithlo
w t
emp;
SO
4an
d N
O3
effe
cts
also
HA
MM
ER
1977
[74]
Bir
min
gham
,26
180–
220
Incr
ease
in
LR
I in
chi
ldre
n w
ith
AL
, U
SAL
OE
L†
LO
EL
incr
ease
s ab
ove
thes
e le
vels
ZA
GR
AN
ISK
I19
79[7
5]N
ew H
aven
,x=
8x=
73.1
[SO
4x=
12.5
;8–
461
Sign
ific
ant
incr
ease
in
sym
ptom
s in
CT
, U
SA(2
0–14
8)1.
5–35
.7]
asth
ma/
alle
rgy
and
smok
ing
adul
ts r
elat
edto
O3
and
pH o
f T
SP, n
ot r
elat
ed t
o SO
4O
STR
O19
91[7
6]D
enve
r, C
O,
?0.
5–73
??
No
sign
ific
ant
incr
ease
in
coug
h in
adu
ltU
SAas
thm
atic
s†O
STR
O19
93[5
3]So
uthe
rn C
A,
?(S
O4:
2–
CO
H:
4–26
20–5
49?
Sign
ific
ant
48%
inc
reas
e (5
0–10
0 µ
g·m
-3
USA
36)
(6 d
ay)
SO4
and/
or 0
.1 p
pm O
3) i
n L
RI
inno
nsm
okin
g ad
ults
; no
sign
ific
ant i
ncre
ase
in U
RI:
tem
p; o
ther
AP,
sto
ves
NS
SCH
WA
RT
Z19
94[7
7]6
citie
s in
Med
ian
Med
ian
Med
ian
Med
ian
Med
ian
Sign
ific
ant
51%
inc
reas
e in
cou
gh a
ndU
SA 1
984–
1988
=10
.5=
18=
30=
36.9
=24
.410
3% i
ncre
ase
in L
RI
in P
M a
nd 2
AP
90th
%=
4790
th%
=37
90th
%=
5390
th%
=54
90th
%=
45m
odel
s; t
emp.
, ci
ty i
nclu
ded
in m
odel
;22
% i
ncre
ase
in c
ough
with
30
ppb
incr
ease
in
ozon
eH
AM
ME
R19
74[7
8]L
os A
ngel
es,
?78
–980
?Si
gnif
ican
t in
crea
se i
n co
ugh,
inc
reas
edSC
HW
AR
TZ
1989
[79]
CA
, U
SAch
est
disc
omfo
rt, i
n yo
ung
adul
ts r
elat
edSC
HW
AR
TZ
1990
[80]
to O
xbu
t no
t to
NO
2, T
SP,
CO
†
WH
ITT
MO
RE
1980
[81]
Los
Ang
eles
,x
51–1
2159
–294
Sign
ific
ant
incr
ease
in
asth
ma
atta
cks
inC
A,
USA
juve
nile
-adu
lt as
thm
atic
s; S
Ox
and
NO
xhi
ghly
cor
rela
ted
with
TSP
MA
RG
OL
IS19
94[8
2]O
rang
e C
ount
y,<
79M
edia
n=0.
05–0
.30
Upp
erSi
gnif
ican
tly i
ncre
ased
sym
ptom
s (a
ndC
A,
USA
SO4
5.7;
ppb
thir
dde
crea
sed
PEF)
in
adul
t as
thm
atic
s≤1
06
h <
29≥1
50re
late
d to
SO
4an
d N
O2,
con
trol
ling
for
othe
r A
P, t
emp.
, se
ason
, m
edic
atio
ns,
polle
n an
d fu
ngi
KR
ZY
ZA
NO
WSK
I19
92[8
3]T
ucso
n, A
Z,
Med
ian=
≤187
29–1
8125
.1±
Incr
ease
in
alle
rgic
and
irr
itant
Q
UA
CK
EN
BO
SS19
91[8
4]U
SA<
81(x
=42
)pp
b. 1
h10
.2sy
mpt
oms
and
AR
Is a
bove
56
ppb
O3
LE
BO
WIT
Z19
92[8
5]75
th%
=<
105
18–1
61in
depe
nden
tly a
nd in
tera
ctiv
e w
ith te
mp.
ppb
8 h
and
with
PM
10>
50 µ
g·m
-3in
door
AP,
and
cova
riat
es;
inde
pend
ent
incr
ease
in
sym
ptom
s w
ith P
M10
; PE
F de
crea
se(3
.8%
per
100
ppb
) al
so s
igni
fica
nt(w
ith n
o th
resh
old)
see
next
pag
e fo
r de
fini
tions
.
EPIDEMIOLOGICAL STUDIES OF AIR POLLUTION EFFECTS 1035T
able
3.
–
Con
t.....
...
Exp
osur
es
µg·
m-3
#Fi
rst
auth
or
Yea
r
[Ref
]
Loc
atio
n
SO2
TSP
PM2.
5/B
S
PM10
O3*
N
O2
Res
ults
LE
BO
WIT
Z19
84[2
1]L
EB
OW
ITZ
1985
[23]
Tuc
son,
AZ
,(S
O4
57–3
8918
0–23
931
9–41
3W
heez
e an
d co
ugh
incr
ease
rel
ated
to
LE
BO
WIT
Z19
85[8
6]U
SAan
nual
=(1
h)
TSP
, O
3an
d N
O2
inde
pend
ently
in
LE
BO
WIT
Z19
87[8
7]3.
39–4
.69)
adul
t as
thm
atic
s, c
ontr
ollin
g fo
rsi
gnif
ican
t ef
fect
s of
tem
p.,
RH
, in
door
AP,
pol
len;
int
erac
tions
with
tem
p.us
ually
sig
nifi
cant
; N
Sin
nor
mal
s;in
crea
sed
rhin
itis,
cou
gh,
sore
thr
oat
in a
llerg
ies
seen
with
TSP
; tim
ein
/out
inc
lude
dV
ED
AL
1987
[88]
Che
stnu
t≤1
76 (
1 h)
CO
H ≤
1.3
≤129
≤79
(1 h
)N
o si
gnif
ican
t re
latio
nshi
p w
ithR
idge
, PA
, U
SA,
units
(1
h)sy
mpt
oms
(or
PEF)
LA
WT
HE
R19
70[6
5]L
ondo
n, U
K50
0–60
0B
S=25
0–50
0?
Incr
ease
in
bron
chiti
cs' s
ympt
oms
1954
–196
4w
ith t
hese
lev
els;
tem
p. i
mpo
rtan
tH
OE
K19
93[8
9]W
agen
inge
n,≤1
05≤1
10≤1
27A
RI
NS;
tem
p. i
n m
odel
(w
inte
r)N
LR
OE
ME
R19
93[9
0]W
agen
inge
n,>
110
Sign
ific
ant
incr
ease
in
coug
h in
NL
sym
ptom
atic
chi
ldre
n in
win
ter
rela
ted
to T
SPD
USS
EL
DO
RF
1994
[91]
Net
herl
ands
?4–
137
?N
o si
gnif
ican
t in
crea
se i
n co
ugh
inad
ults
nea
r st
eel
mill
†
MA
KIN
O19
75[9
2]T
okyo
, Ja
pan
-266
? hi
gh≤4
5 O
x≤2
07*
Sign
ific
ant
incr
ease
in
sym
ptom
s in
MIZ
OG
UC
HI
1977
[93]
child
ren
inde
pend
ently
rel
ated
to
Ox,
SO2,
TSP
and
tem
p.SH
IMIZ
U19
76[9
4]O
saka
, Ja
pan
<15
96*
<37
3 O
x<
226*
Sign
ific
ant
incr
ease
in
sym
ptom
s in
child
ren
rela
ted
to S
O2,
TSP
; w
eath
erin
mod
els
S CH
WA
RT
Z19
91[9
5]5
Ger
man
Med
ian=
Med
ian=
Med
ian=
Sign
ific
ant
26%
inc
reas
e in
AR
I in
Com
mun
ities
9–48
17–5
614
–>50
child
ren;
TSP
NS
with
NO
2in
mod
el;
1983
–198
590
th%
=w
eath
er i
n m
odel
41–1
18V
ON
MU
TIU
S19
95[9
6]L
eipz
ig,
Ger
man
y20
–90
40–2
50N
Ox:
Si
gnif
ican
t in
crea
se i
n U
RI
in c
hild
ren
40–5
00re
late
d to
SO
2, N
Ox,
TSP
, co
ntro
lling
for t
emp.
, ET
S; w
ith p
ossi
ble
inte
ract
ions
FOR
SBE
RG
1993
[97]
Pite
a, S
wed
en1.
3–12
.9B
S=7.
4–55
.8Si
gnif
ican
t in
crea
se i
n dy
spno
ea i
n1.
0–21
.4as
thm
atic
s re
late
d to
BS;
tem
p. a
ndR
H i
n m
odel
#: 2
4 h,
unl
ess
othe
rwis
e no
ted;
*:
1 h
daily
max
imum
val
ues
unle
ss o
ther
wis
e st
ated
; †:
fro
m E
PA C
rite
ria
Doc
umen
ts;
LO
EL
: lo
wes
t ob
serv
ed e
ffec
t le
vel;
x: m
ean;
TSP
: to
tal
sus-
pend
ed p
artic
ulat
es;
PM2.
5: p
artic
ulat
e m
atte
r w
ith a
erod
ynam
ic d
iam
eter
≤2.
5 µ
m;
BS:
bla
ck s
mok
e; R
SP:
resp
irab
le s
uspe
nded
par
ticul
ate
(~PM
3.5)
; C
OH
: co
effi
cien
t of
haz
e; P
M10
:pa
rtic
ulat
e m
atte
r w
ith a
erod
ynam
ic d
iam
eter
≤10
µm
; L
RI:
low
er r
espi
rato
ry i
llnes
s; U
RI:
upp
er r
espi
rato
ry i
llnes
s; N
S: n
onsi
gnif
ican
t; te
mp:
tem
pera
ture
; A
P: a
ir p
ollu
tant
; pp
b: p
arts
per
billi
on;
PEF:
pea
k ex
pira
tory
flo
w;
AR
I: a
cute
res
pira
tory
inf
ectio
n; R
H:
rela
tive
hum
idity
; E
TS:
env
iron
men
tal
toba
cco
smok
e.
M.D. LEBOWITZ1036T
able
4.
–
Acu
te p
ulm
onar
y fu
nctio
n ch
ange
s as
soci
ated
with
air
pollu
tion
Exp
osur
es
µg·
m-3
Firs
tau
thor
Y
ear
[R
ef]
Loc
atio
n
SO2
TSP
PM
2.5/
BS
PM10
O3*
NO
2R
esul
ts
S PE
CK
TO
R19
88[1
14]
Tux
edo,
NY
,?
H2S
O4
≤9?
41–2
43?
Sign
ific
ant
decr
ease
in
spir
omet
ry a
ndU
SAPE
F re
late
d on
ly t
o O
3in
acu
te h
ealth
yex
erci
sing
non
smok
ing
adul
tsSP
EC
KT
OR
1988
[115
]R
ural
NJ,
USA
?H
2SO
4<
19?
78–2
94?
Sign
ific
ant
decr
ease
s in
lun
g fu
nctio
nSP
EC
KT
OR
1991
[116
](1
2 h)
in c
hild
ren
rela
ted
to O
3(1
day
lag
), b
utno
t to
H2S
O4
TH
UR
STO
N19
93[1
17]
Rur
al C
T,
USA
?H
+≤1
10 n
M?
137–
314
?Si
gnif
ican
t de
crea
ses
in P
EF
in a
sthm
atic
child
ren
rela
ted
to O
3: (
effe
ct o
f A
P se
enas
sym
ptom
s al
so),
med
icat
ion,
tem
p. R
Hin
mod
els†
LIP
PLA
M19
83[1
18]
Rur
al P
A a
nd?
≤66
[H2S
O4
(6 h
)≤1
10?
Sign
ific
ant
decr
ease
in
PEF
in c
hild
ren:
LIP
PMA
N19
85[1
19]
NJ,
USA
av ≤
6]≤2
16ot
her
AP
and
tem
p. s
omet
imes
in
BO
CK
1985
[120
]m
odel
s; o
ther
wis
e as
sum
ed n
otL
IOY
1985
[121
]co
nfou
nder
sD
OC
KE
RY
1982
[122
]St
eube
nvill
e,28
0–46
022
0–45
5?
Sign
ific
ant
2–3%
dec
reas
e in
lun
gO
H,
USA
func
tion
in c
hild
ren;
tem
p. i
n m
odel
LE
BO
WIT
Z19
74[1
9]T
ucso
n, A
Z,
low
≤150
≤235
Sign
ific
ant d
ecre
ase
in F
EV
in e
xerc
isin
gU
SAch
ildre
n w
ith i
nter
actio
n w
ith t
emp.
LE
BO
WT
IZ19
85[2
1]T
ucso
n, A
Z,
low
In <
69R
SP I
n <
5074
–235
Sign
ific
ant
decr
ease
s in
dai
ly P
EF
inU
SAO
ut <
170
Out
<12
5ch
ildre
n (T
SP,
O3)
, ad
ults
with
AO
Dda
ilyda
ily(T
SP,
tem
p. g
as s
tove
s) c
ontr
ollin
g fo
rm
eter
olog
y, i
ndoo
r su
rrog
ates
, po
llen,
fung
iQ
UA
CK
EN
BO
SS19
91[8
4]T
ucso
n, A
Z,
low
Med
ian
<81
Out
=29
–181
Out
: m
ean
Sign
ific
ant
decr
ease
in
PEF
in a
sthm
atic
USA
75th
% <
105
≤187
15–4
8ch
ildre
n re
late
d in
depe
nden
tly to
O3,
PM
KR
ZY
ZA
NO
WSK
I19
92[8
3]x=
42In
: m
edia
nan
d N
O2;
tem
p.,
wea
ther
, t-
act.,
In
door
: ≤2
1211
–37
med
icat
ion
in m
odel
NE
AS
1995
[123
]U
nion
tow
n,x=
29.2
x=24
.5x=
35.6
12 h
·day
-1C
hild
ren'
s PE
F si
gnif
ican
tly d
ecre
ased
,PA
, U
SAm
ax=
128.
4m
ax=
88.1
max
=83
.4av
=98
by ≥
1%,
espe
cial
ly i
n th
ose
with
(sum
mer
)H
+x=
102
sym
ptom
s re
late
d to
O3,
H+,
PM t
emp.
nM·m
-3an
d tim
e sp
ent o
utdo
ors
in m
odel
s; c
ough
incr
ease
d 16
% w
ith H
+
SEL
WY
N19
85[1
24]
Hou
ston
, T
X,
low
x=10
≤265
low
No
sign
ific
ant
decr
ease
in
lung
fun
ctio
nU
SAin
hea
lthy
adul
ts w
ith t
emp.
and
RH
in
mod
elJO
HN
SON
1986
[125
]H
oust
on,
TX
,lo
wx=
10-2
49,-
412
low
Incr
ease
d as
thm
a at
tack
s, m
edic
atio
n us
e,H
OL
GU
IN19
85[1
26]
USA
and
othe
r Sx
with
O3
and
decr
ease
d te
mp.
;C
ON
TA
NT
1985
[127
]al
so d
ecre
ased
FE
V1
and
FVC
; SO
2an
dPM
not
in
mod
els
POPE
1991
[71]
Salt
Lak
e C
ity,
low
11–1
95lo
w
low
Sign
ific
ant
decr
ease
s in
PE
F in
ast
hmat
icU
T,
USA
child
ren
rela
ted
to P
M10
: te
mp.
, bu
t no
tot
her
AP,
in
mod
elPO
PE19
93[1
28]
Salt
Lak
e C
ity,
low
≤181
low
low
Sign
ific
ant
decr
ease
in
FEV
in
adul
tsU
T,
USA
rela
ted
to P
M;
tem
p.,
but
not
othe
r A
P,in
mod
else
e ne
xt p
age
for
defi
nitio
ns.
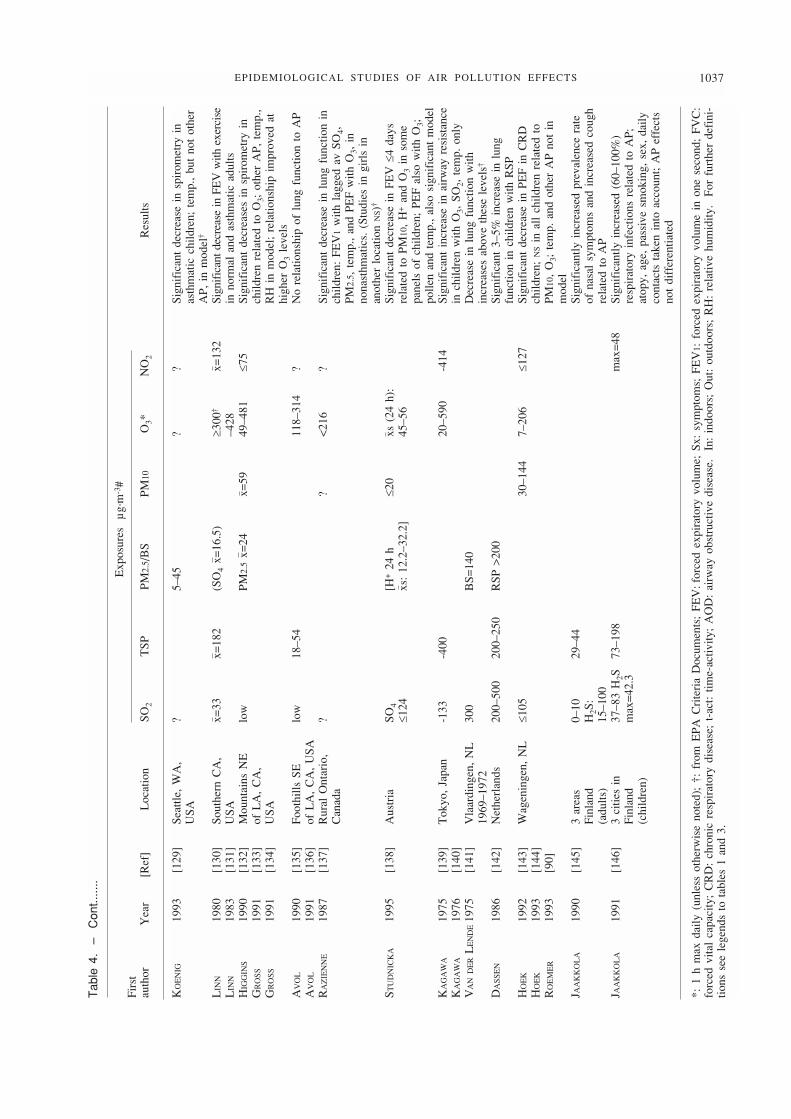
EPIDEMIOLOGICAL STUDIES OF AIR POLLUTION EFFECTS 1037T
able
4.
–
Con
t.....
..
Exp
osur
es
µg·
m-3
#Fi
rst
auth
or
Yea
r
[
Ref
]
L
ocat
ion
SO
2T
SP
PM
2.5/
BS
PM
10O
3*
N
O2
Res
ults
KO
EN
IG19
93[1
29]
Seat
tle,
WA
,?
5–45
??
Sign
ific
ant
decr
ease
in
spir
omet
ry i
nU
SAas
thm
atic
chi
ldre
n; t
emp.
, bu
t no
t ot
her
AP,
in
mod
el†
LIN
N19
80[1
30]
Sout
hern
CA
,x=
33x=
182
(SO
4x=
16.5
)≥3
00†
x=13
2Si
gnif
ican
t dec
reas
e in
FE
V w
ith e
xerc
ise
LIN
N19
83[1
31]
USA
–428
in n
orm
al a
nd a
sthm
atic
adu
ltsH
IGG
INS
1990
[132
]M
ount
ains
NE
low
PM2.
5x=
24x=
5949
–481
≤75
Sign
ific
ant
decr
ease
s in
spi
rom
etry
in
GR
OSS
1991
[133
]of
LA
, C
A,
child
ren
rela
ted
to O
3; o
ther
AP,
tem
p.,
GR
OSS
1991
[134
]U
SAR
H i
n m
odel
; re
latio
nshi
p im
prov
ed a
thi
gher
O3
leve
lsA
VO
L19
90[1
35]
Foot
hills
SE
low
18–5
411
8–31
4?
No
rela
tions
hip
of l
ung
func
tion
to A
PA
VO
L19
91[1
36]
of L
A,
CA
, U
SAR
AZ
IEN
NE
1987
[137
]R
ural
Ont
ario
,?
?<
216
?Si
gnif
ican
t de
crea
se i
n lu
ng f
unct
ion
inC
anad
ach
ildre
n: F
EV
1w
ith l
agge
d av
SO
4,PM
2.5,
tem
p.,
and
PEF
with
O3,
in
nona
sthm
atic
s. (
Stud
ies
in g
irls
in
anot
her
loca
tion
NS)
†
STU
DN
ICK
A19
95[1
38]
Aus
tria
SO4
[H+
24 h
≤20
xs (
24 h
):Si
gnif
ican
t de
crea
se i
n FE
V ≤
4 da
ys≤1
24xs
: 12
.2–3
2.2]
45–5
6re
late
d to
PM
10,
H+
and
O3
in s
ome
pane
ls o
f ch
ildre
n; P
EF
also
with
O3;
polle
n an
d te
mp.
, al
so s
igni
fica
nt m
odel
KA
GA
WA
1975
[139
]T
okyo
, Ja
pan
-133
-400
20–5
90-4
14Si
gnif
ican
t in
crea
se i
n ai
rway
res
ista
nce
KA
GA
WA
1976
[140
]in
chi
ldre
n w
ith O
3, S
O2,
tem
p. o
nly
VA
ND
ER
LE
ND
E19
75[1
41]
Vla
ardi
ngen
, N
L30
0B
S=14
0D
ecre
ase
in l
ung
func
tion
with
1969
–197
2in
crea
ses
abov
e th
ese
leve
ls†
DA
SSE
N19
86[1
42]
Net
herl
ands
200–
500
200–
250
RSP
>20
0Si
gnif
ican
t 3–
5% i
ncre
ase
in l
ung
func
tion
in c
hild
ren
with
RSP
HO
EK
1992
[143
]W
agen
inge
n, N
L≤1
0530
–144
7–20
6≤1
27Si
gnif
ican
t de
crea
se i
n PE
F in
CR
DH
OE
K19
93[1
44]
child
ren;
NS
in a
ll ch
ildre
n re
late
d to
RO
EM
ER
1993
[90]
PM10
, O
3; t
emp.
and
oth
er A
P no
t in
m
odel
J AA
KK
OL
A19
90[1
45]
3 ar
eas
0–10
29–4
4Si
gnif
ican
tly i
ncre
ased
pre
vale
nce
rate
Finl
and
H2S
: of
nas
al s
ympt
oms
and
incr
ease
d co
ugh
(adu
lts)
15–1
00re
late
d to
AP
J AA
KK
OL
A19
91[1
46]
3 ci
ties
in37
–83
H2S
73–1
98m
ax=
48Si
gnif
ican
tly i
ncre
ased
(60
–100
%)
Finl
and
max
=42
.3re
spir
ator
y in
fect
ions
rel
ated
to
AP;
(chi
ldre
n)at
opy,
age
, pa
ssiv
e sm
okin
g, s
ex,
daily
cont
acts
tak
en i
nto
acco
unt;
AP
effe
cts
not
diff
eren
tiate
d
*: 1
h m
ax d
aily
(un
less
oth
erw
ise
note
d);
†: f
rom
EPA
Cri
teri
a D
ocum
ents
; FE
V:f
orce
d ex
pira
tory
vol
ume;
Sx:
sym
ptom
s; F
EV
1: f
orce
d ex
pira
tory
vol
ume
in o
ne s
econ
d; F
VC
:fo
rced
vita
l ca
paci
ty;
CR
D:
chro
nic
resp
irat
ory
dise
ase;
t-a
ct:
time-
activ
ity;
AO
D:
airw
ay o
bstr
uctiv
e di
seas
e.
In:
indo
ors;
Out
: ou
tdoo
rs;
RH
: re
lativ
e hu
mid
ity.
For
fur
ther
def
ini-
tions
see
leg
ends
to
tabl
es 1
and
3.
considered. WHO environmental health criteria (EHCs)have also documented responses related to metal partic-ulate (especially in those sensitized) and to pesticides.
PM and O3/NO2/organics and asthma. BATES and SIZTO
[148] found highly significant associations between ex-cess respiratory admissions, especially asthma (and espe-cially in the young), and average maximum hourly SO4and O3 concentrations, and temperature in SouthernOntario. There appeared to be 24–48 h lags for effects.These correlations were consistent in other years. Otherstudies in the USA confirmed this association with ozone[149–152]. In Helsinki, a combination of temperatureand ozone, as well as other gaseous pollutants, was asso-ciated with increased asthma admissions to hospitals[153], and a combination of temperature and NO2 wasassociated with ER visits in northern Finland [154]. InBirmingham (UK), location near roadways (a surrogatefor NO2) was also associated with hospital admissionsfor childhood asthma [155]. In Mexico City, ER visitsfor childhood asthma increased by 43% per 98 µg·m-3
(50 ppb) increase in ozone, and by 68% if O3 exceeded216 µg·m-3 (110 ppb) for two or more days, controllingfor other pollutants, weather and other factors [156].Asthma attendance was also correlated with spore andpollen counts along with weather factors [157].
Increased rates of asthma attacks and reduced lungfunction were noted in epidemiological studies duringepisodes, or days of higher levels of photochemical oxi-dant air pollution (tables 3 and 4). (Experimental stu-dies also show increased bronchial responsiveness withozone [17]).
WHITTMORE and KORN [81] found significant increa-ses in the probability of asthma attacks in asthmatics inLos Angeles associated with increases of 0.10 ppm (range0.03–0.15 ppm) in oxidant levels; attacks increased on dayswith high TSP, and also cooler temperature. ZAGRANISKI
et al. [75] reported an increased prevalence rate for res-piratory symptoms at about 0.08 ppm (range 0.004–0.235ppm) O3 in patients with asthma in New Haven.
Studies in Tucson [21, 83, 86] showed effects in asth-matics, related to temperature, O3 (0.052–0.12 ppm), andthe two together (clinically significant reductions of 15–24% in PEF); these were related to time-activity (timespent in/out of doors), controlling for other factors. Medi-cation use confirmed the changes. More severe symp-toms usually occurred 1–3 days after significant PEFdeclines. These time-lag effects of ozone (and tempera-ture) have been shown by some other studies [115, 121],but not all [83]. Both 1 and 8 h concentrations of O3have been shown to have significant effects, and to inter-act with PM10 and temperature in producing reductionsin PEF [83]. However, temperature effects were alwaysmore important. In addition, the low humidity in someenvironments probably had a major influence on theeffects seen at concentrations below 120 ppb [86]. Thisgeneral interactive type of relationship has also been seenfor outdoor NO2 and either an indication of gas stoveusage or measured indoor NO2 in asthmatic adults andchildren, in which time spent outdoors was an importantfactor, and medication usage did not prevent the effects[84, 87].
Different forms of particulate, including environmen-tal tobacco smoke (ETS) (and ETS-organic compounds)
indoors also have effects on symptoms and PEF in asth-matics, especially in children [84, 115, 158–161]. It hasalso been demonstrated that there were influences ofindoor particulate matter with an aerodynamic diameter≤2.5 µm (PM2.5) and cigarette smoking on morning PEFin asthmatic children when including previous days' asth-matic medications, an inhibitor of adverse effects on phy-siological status. Thus, nocturnal asthma may well havesignificant physiological decrements associated with en-vironmental stimuli, for which there can be only partialprotection. Indoor formaldehyde (HCHO) exposures haveeffects on symptoms and PEF in asthmatic children; therealso appears to be avoidance of high exposures to HCHOby asthmatics [160]. The impact of bioaerosols (indoorsand outdoors) has also been substantial [8, 16, 162–164],as will be discussed further. The effects of other meteo-rological phenomena have been reviewed previously [17,165].
Summary. Several studies have shown that daily tem-perature variations were often more strongly correlatedwith attack rates, but air pollution still exerted a signifi-cant effect even when temperature-adjusted rates werecomputed. Examination of tables 3 and 4 vis-a-vis asth-matics indicates the LOEL for symptoms and significantPEF reductions of: 157 µg·m-3 (0.08 ppm) O3 based onseveral studies; about 200 µg·m-3 SO2 based on two stu-dies; TSP approximately 80–120 µg·m-3 based on fourstudies; PM10 >50 µg·m-3 based on 1–2 studies; PM2.5>25–75 µg·m-3 based on three studies, but less if pri-marily SO4 effects (as low as 10 µg·m-3 SO4) based onthree other studies. The evidence for NO2 is too con-flicting to determine any LOEL.
The major problems in most studies of exacerbationsof asthma have been the lack of information on time-activity patterns, the possible effects of medications, andthe absence of records for all days on which symptomscould have occurred. Investigators who have been ableto control some of these variables have found consistenteffects of O3 (as well as other pollutants) on asthma andother airway obstructive disease (AOD), though con-trolled exposure studies have not [13, 17]. However, eventhe lack of records for all days, and the presence of medi-cation information implying very good management,have not interfered with the occurrence of effects rela-ted to air pollutants in asthmatics ([88, 83]; Daumer, per-sonal communication). Experimental evidence suggestsa continuum in the dose-response relationship. Peak flowmeasurements have been shown to be most responsiveto pollutant and meteorological exposures as well as tobeneficial effects of medications [166], as also describedabove.
There are some possible long-range effects of bronchialresponsiveness (BR) produced by pollutants (and tem-perature). Several studies [167–169] have shown detri-mental longitudinal effects of BR on lung function,either reduced growth or increased decline. The long-range implications of BR and immunological status havealso been discussed at length [8, 11, 16, 162, 170–172].
In conclusion, a variety of indoor and outdoor pollu-tants, including bioaerosols, have been shown to affectlung function in those with pre-existing disease [8, 10,11, 16, 23, 83–86, 89, 111, 159, 160, 162–164, 166,173–176] as well as symptoms; PEF appears to be a
M.D. LEBOWITZ1038
more sensitive instrument for detecting such changes[166, 177, 178].
Respiratory infections. Air pollution and impaired resis-tance to respiratory infection, shown in animals, has alsobeen seen in studies of humans; a greater incidence ofacute respiratory illness (ARI) supports a probable asso-ciation between increased acute lower respiratory tractdisease (acute bronchitis, pneumonia, other acute chestillnesses) and air pollution [4, 5, 10, 14]. Although im-portant, excess acute lower respiratory illness rates inchildren cannot be accounted for by social class or areadifferences in residential mobility (ibid.).
Atopic status appears to be an additional risk factorfor respiratory illnesses associated with air pollution [179,180]. The role of air pollution as adjuvants to alteredimmunological status, for infections and allergic sensiti-zation, has also been seen in animal models ([181–183];Kagawa, personal communication).
PM/SOx. Several epidemiological studies have obser-ved the increased incidence of acute respiratory illness(spatially and temporally) in populations living in com-munities with more sulphur oxides and particulates [4,6, 69, 102, 184–190]; the quantitative studies are foundin table 3. The frequency and severity of acute lowerrespiratory disease increased with the degree of air pol-lution (ibid.), and appeared to diminish when air qua-lity was improved in the UK [186, 191]. Several recentstudies confirm the effect of various outdoor pollutantson respiratory illnesses and symptoms, especially in chil-dren: PM effects in children in Switzerland [192] andin the US [71]. Several metals have also been associa-ted with acute respiratory infections (ARIs) [25]. IndoorPM has been shown to be a special problem for such ill-nesses in the developing world [193].
Environmental tobacco smoke (ETS). Multiple studieshave found the relationship between ETS and ARIs [159].(There have also been numerous studies showing otherrespiratory effects of ETS in children [159], which arenot discussed here).
NO2. Elementary schoolchildren and infants living in ahigh-exposure community for two or more years alsoexperience increased bronchitis morbidity; this has sug-gested an adverse effect in areas with average NO2 con-centrations of 150–282 µg·m-3 (0.08–0.15 ppm), confirmedby subsequent years of study and analyses by EPA [70,194–197]. In Switzerland, increases in ARIs were foundwith 24 h exposures to ambient NO2 of 150–282 µg·m-3
(NO3 of 3.8 µg·m-3) and no other associated pollutants,adjusting for other factors [192]. QUACKENBOSS et al. [84,176] have found increased respiratory illnesses relatedto monitored PM and NO2, indoors and outdoors, as wellas ETS, controlling for other indoor pollutants and fac-tors. NEES and co-workers [198, 199] found a 40% increasein childhood lower respiratory illnesses (LRIs) per 28µg·m-3 (15 ppb) increase in NO2 in the six city study inthe USA. Some studies [200] have not found such effects,though their NO2 concentrations are often lower.
MELIA and co-workers [201, 202] reported a greaterincidence of lower respiratory illnesses in British chil-dren residing in homes using gas versus electricity for
cooking, in which NO2 monitoring occurred. Illness rateswere adjusted for other significant factors (ETS, age, sex)and other potentially confounding factors. This study andothers have led to major re-evaluations of the role ofNO2, including a meta-analysis by HASSELBLAD et al. [203]confirming the effects in humans [14]; these effectsmirror those found in animal studies [4, 14].
Ozone. Respiratory illness effects have been seen inschoolchildren in Mexico City [204], and adults in LosAngeles (together with sulphate but not particulate haze)[53].
Risk assessments. ARIs appear to be increased by 1.5–2.0times with exposures to PM (including ETS), SO2, NO2.Early childhood LRIs increased by 1.5 (19.4 to 30–34%),2.5 if from the lower socioeconomic status (SES), rela-ted to SO4 and SO2 of 190 µg·m-3, hospitalizations by1.5–2.8 (0/1.1 to 1.0/1.8% for bronchitis or pneumonia,1.1–3.1% for LRIs) with similar concentrations. The levelof NO2 reported to produce acute respiratory illnesses isabout 137 µg·m-3 (1 h) [10].
Implications. These relationships are of particular pub-lic health significance because infections and allergiesof the respiratory tract account for a major portion oftotal acute illness in the general population and exact alarge economic toll in terms of time lost from school orwork, visits to doctors, and admissions to hospitals. Thesum of the studies supports an association with increasedacute lower respiratory illness. The pollutants, or con-centrations, which increase risk of acute illness have usu-ally not been established; though some estimates havebeen made [61]. However, this is difficult given the manyenvironmental and personal factors that contribute to suchrisk [4]. The other reason for concern is that these ill-nesses appear to be related to BR, reduced airway cali-bre, and subsequently to airway obstructive diseases [18,23, 86, 170, 186, 205–211]. The role of ventilatory im-pairment, and BR, cannot be underemphasized [22, 167,169, 170].
Other acute respiratory responses
Nonirritants. The effects of carbon monoxide (CO) stemprimarily from its affinity with oxygen-carrying haemo-proteins, which causes a leftward shift and steeper slopeof the oxyhaemoglobin dissociation curve and decrea-ses the amount of such haemoprotein available for oxy-gen transport. The ultimate effect is a tissue deficit ofoxygen, such that normal function may not be sustained.In the absence of CO exposure, carboxyhaemoglobin(COHb) concentrations are approximately 0.5%. (A pack-per-day cigarette smokers may achieve COHb saturationsof 4–7%). For nonsmokers, exposure to CO at a con-centration of 10 mg·m-3 (9 ppm) for 8 h or to a con-centration of 40 mg·m-3 (35 ppm) for 1 h (the presentUS primary air quality standard) is calculated to causean increase in COHb concentrations to 1.5% during theinterval of exposure. At higher elevations, the oxygendissociation curve shifts further to the left. During heavymuscular exercise, the oxygen consumption rate of thewhole body places maximal stress on the oxygen trans-port system, and the ability of the cardiovascular system
EPIDEMIOLOGICAL STUDIES OF AIR POLLUTION EFFECTS 1039
to transport oxygen to exercising muscles is a determi-nant of the maximal sustained rate of work that a nor-mal person can perform [212]. Thus, CO has been shownto have predictable effects on healthy young men under-going strenuous exercise; over the range of COHb concen-trations of 5–20%, a linear relationship existed betweenincreasing COHb and decreasing maximal oxygen con-sumption. Respiratory function may suffer. Nitrogenoxides, specifically NO, can also diffuse into the circu-latory system, form met-haemoglobin, and by further de-priving cells of oxygen, can have similar effects; therelative potency of met-Hb is about one-third that ofCOHb [213].
Short-term irritant-related symptoms. In Donora, duringthe 1948 air pollution episode, 43% of the general popu-lation reported respiratory symptoms during the episode[51]. Irritation of the nose and throat are the most com-mon outcome of almost all air pollutants; cough can oftenbe induced, and sometimes wheeze [4, 5, 8, 13, 14, 25,61]. The quantitative studies of effects on acute symp-toms are displayed in table 3. Many qualitative studieshave been reported (ibid.). Symptoms may temporarilyimpair performance of normal activities even in healthysubjects. Wood smoke, indoors and out, other forms ofparticulate indoors (especially ETS), and indoor formal-dehyde (HCHO) exposures have acute effects on symp-toms, especially in children [108, 115, 159, 161, 176,214].
Short-term irritant-related reductions in function. A widevariety of human airway responses to most of the pol-lutants has been demonstrated, as seen in table 4. (Thesereflect findings in controlled exposure studies of most ofthe pollutants). There is evidence that they can also causebronchoconstriction (ibid.; [107]). In general, these effectsare reversible, and do not necessarily constitute a riskof disease in healthy subjects.
Several field studies have also shown more prolongeddecreases in pulmonary function during and followingpollution episodes, mostly in children, when exposed torelatively high levels of SO2 [24, 66–68, 122, 139, 140];these exposures usually occur with the presence of somePM, and temperature can also play an important role.The levels of reduction can be clinically significant (morethan 15% decline), but reverse quickly when exercise isstopped or the exposure is removed.
In general, decrements occur in normal children andadults above 110 µg·m-3 PM10 (in the presence of SO2),3,760 µg·m-3 of NO2 (560 µg·m-3 in asthmatics, thus the1 h Air Quality Guideline (AQG) of 400 µg·m-3) [10,71]; above 150–200 µg·m-3 of ozone for 1 h (above100–250 for 8 h).
Decrements related to short-term (1 h) and longer (6–8 h) ozone exposure have also been amply demonstra-ted [4, 13, 61, 215, 216], and recent studies continue toconfirm these results (table 5). In general, these acutefunctional changes in healthy children and young adultsoccur with 1 h O3 concentrations of 0.08–0.15 ppm, andless (>0.06 ppm) for the longer (6–8 h) exposures.
Tolerance and/or adaptation. Humans respond physio-logically to complex environments containing pollutants(exogenous stimuli which usually produce adverse changes)
by adaptive strategies that should be suitable, but maynot be under all circumstances. Recovery from irritantexposures in healthy subjects is generally complete with-in hours, although the recovery period may be longer forsubjects with the most severe responses, and some clini-cally severe responses can occur at higher doses [58].The susceptibility of the humans so exposed is of criti-cal importance to early responses and adaptability, andinfluence changes that help determine later physiologi-cal responses to the same or similar stimuli. For manyof the current pollutants of concern, such as most volatileorganic compounds, either as gases or in particle form(such as from solvents, cleaners and maintenance pro-ducts, and sidestream tobacco smoke), the mechanismsof response are so complex and poorly understood thattoxicological and also some controlled exposure studiesare required first. Furthermore, some pollutant classesmay be well-characterized, but occur in concentrationssufficient for study only in occupational settings (e.g.asbestos, some volatile organic compounds, some mine-ral fibres); the adverse health effects of these pollutantclasses are, therefore, best characterized in occupationalstudies [12, 171].
Although others have found adaptation to ozone incontrolled human exposure studies, no such changes havebeen seen in epidemiological or physiological studies inthe field. This is probably due to prolonged exposure toambient ozone and/or other pollutants, and lagged effectson lung function (supra vida). The studies described doshow some relative adaptation has occurred to high tem-peratures and low relative humidity.
Sometimes, active smokers appear to have adapted tothe effects of irritants, as seen in their lesser reactivityto ozone in chamber studies [5]. It may occasionally bethe case for passive smoking as well, since it appears toinhibit the effects of ozone in children [121].
Chronic respiratory diseases
Mortality
Sulphur oxides and particulate matter. Non-time seriesanalyses of geographic differences in mortality havefavoured an association of sulphur oxides (including sul-phates) and PM with mortality, although there has beenno general agreement from such studies [4, 5, 10, 25].The nature of ecological analyses, and their fallacies andbiases, have been reviewed elsewhere [4, 8, 12, 25, 52,279].
A recent study of childhood mortality in different re-gions of the Czech Republic [280] found a 3.16 excessrelated to TSP, a 5.41 excess related to SO2, and a 2.73excess related to NO2. A significant correlation betweenbronchitis mortality and the acidity of precipitation (pH)has been found in the UK [281]. A recent analysis oflongitudinal data on large populations in six US citiesin which individuals' data were utilized [54] found thattotal and cause-specific mortality in the different citieswas related to the PM concentrations in those cities afteradjusting for personal factors. The consistency of thefindings for PM is significant, in spite of the fact thatother factors might have accounted for some of the
M.D. LEBOWITZ1040
EPIDEMIOLOGICAL STUDIES OF AIR POLLUTION EFFECTS 1041T
able
5.
–
Rel
atio
nshi
p of
chr
onic
ter
m e
xpos
ures
to
spec
ific
pollu
tant
s to
chr
onic
res
pira
tory
dis
ease
(an
nual
mea
sure
men
ts u
nles
s ot
herw
ise
stat
ed)
Exp
osur
es
µg·
m-3
#Fi
rst
Loc
atio
nau
thor
Y
ear
[R
ef]
(po
pula
tion)
SO2
TSP
PM
2.5/
BS
P
M10
O3*
NO
2R
esul
ts
CH
APM
AN
1973
[217
]U
rban
Are
as28
6 (2
4 h)
145
SO4
≤50
low
Incr
ease
d pr
eval
ence
rat
es o
f ch
roni
cH
AM
ME
R19
76[6
9]U
SA(≤
617)
(24
h)br
onch
itis,
sm
okin
g, o
ther
fac
tors
in
(adu
lts)
(≤24
4)m
odel
sC
HA
PMA
N19
76[2
18]
Bir
min
gham
,26
(24
h)
180–
220
RSP
≥45
(NO
xlo
w)
Incr
ease
d pr
eval
ence
rat
es o
f sy
mpt
oms
HA
MM
ER
1977
[74]
AL
USA
(24
h)L
OE
Lan
d de
crea
sed
FEV
rel
ated
to
PM;
othe
r(c
hild
ren)
fact
ors
in m
odel
sSH
Y19
73[2
19]
USA
69–1
6072
–114
86–1
66D
ecre
ased
FE
V w
ith T
SP/s
ulph
ate;
(chi
ldre
n)ot
her
cova
riat
es i
n m
odel
NO
2N
S
SCH
WA
RT
Z19
89[2
20]
USA
??
<78
-150
Dec
reas
ed l
ung
func
tion
rela
ted
to(c
hild
ren)
LO
EL
NO
2, O
3, (
45 m
L/2
8.3
µg·
m-3
NO
2);
16–2
31ot
her
fact
ors
in m
odel
s†SP
EIZ
ER
1980
[221
]6
City
Stu
dy,
90th
%=
39–1
14PM
15?
Est
. 7–
49M
argi
nally
sig
nifi
cant
inc
reas
es i
nW
AR
E19
84[2
22]
USA
55 p
pb20
–59
indo
orre
spir
ator
y ill
ness
es u
nder
age
2 y
rsD
OC
KE
RY
1989
[223
](c
hild
ren)
Stub
envi
lle(3
3 ex
cess
and
decr
ease
s in
lung
func
tion;
com
bine
dN
EA
S19
90[1
98]
if g
as s
tove
)sy
mpt
oms
sign
ific
antly
inc
reas
ed b
y N
EA
S19
91[1
99]
47%
; ot
her
fact
ors
in m
odel
sW
AR
E19
84[2
24]
6 C
ities
, U
SA90
th%
=39
–114
PM15
<42
.5V
ery
larg
e, s
igni
fica
nt in
crea
ses
in L
RIs
,W
AR
E19
86[2
22]
(chi
ldre
n)55
ppb
20–5
9co
ugh
and
bron
chiti
s w
ith T
SP,
PM15
DO
CK
ER
Y19
89[2
25]
(not
PM
2.5)
, ag
e, s
ex,
SES,
mat
erna
lN
EA
S19
94[2
26]
smok
ing
in m
odel
s; o
ther
AP
NS;
bron
chiti
s an
d L
RI
incr
ease
d 13
–18%
CH
APM
AN
1985
[227
]U
tah,
USA
11–1
1539
–108
SO4
5–14
NO
30.
9–75
–95%
inc
reas
ed c
hron
ic r
espi
rato
ry(c
hild
ren)
3.5
sym
ptom
s re
late
d to
SO
2; s
mok
ing
inm
odel
DO
DG
E19
80[2
28]
Ari
zona
, U
SA4–
8637
–72
low
low
Sign
ific
ant l
ower
lung
func
tion
with
TSP
;D
OD
GE
1983
[229
](c
hild
ren)
SO2
NS;
oth
er f
acto
rs i
n m
odel
sL
INN
1976
[230
]L
A v
sSF
, C
A?
??
65–1
30N
o si
gnif
ican
t di
ffer
ence
in
lung
USA
(no
nsm
okin
gfu
nctio
n; n
o in
door
mea
sure
men
ts;
adul
ts)
com
plic
ated
out
door
exp
osur
esD
ET
EL
S19
81[2
31]
Sout
hern
CA
, U
SAlo
w76
–133
78–3
9253
–226
*In
crea
sed
sym
ptom
s an
d so
me
DE
TE
LS
1987
[232
](a
dults
)SO
44.
5–(x
of
24 h
)ev
iden
ce o
f de
crea
sed
lung
fun
ctio
n,D
ET
EL
S19
91[2
33]
13.5
(x
ofbu
t on
ly s
mok
ing
cont
rolle
d fo
r an
dT
ASH
KIN
1994
[234
]24
h)
spec
ific
AP
not
dete
rmin
ed a
nd h
igh
refu
sal
rate
s in
fol
low
-up
exam
sA
BB
EY
1993
[41]
Cal
ifor
nia
<57
–>40
0<
60–>
200
[SO
4<
6–>
15]
<19
6–>
491
<94
–>37
6Pr
eval
ence
and
inc
iden
ce r
ates
of
AB
BE
Y19
93[2
35]
(non
smok
ing
chro
nic
bron
chiti
s an
d as
thm
aA
BB
EY
1995
[236
]ad
ults
)si
gnif
ican
tly r
elat
ed t
o T
SP a
nd o
zone
;ot
her
AP
NS;
tim
e-ac
tivity
, ex
-sm
okin
g,pa
ssiv
e sm
okin
g, S
ES,
age
, ge
nder
,oc
cupa
tiona
l ex
posu
re i
n m
odel
sP E
AR
LM
AN
1971
[194
]C
hatta
noog
a,lo
w?
x ≤2
86Si
gnif
ican
t in
crea
sed
resp
irat
ory
P EA
RL
MA
N19
71[1
95]
TN
, U
SAup
to
1971
sym
ptom
s in
197
2, n
ot i
n 19
73 (
22–
LO
VE
1982
[70]
(chi
ldre
n)N
O3
≤4.1
40 µ
g·m
-3N
O2)
HN
O2=
?19
72:
43–9
1se
e en
d of
tab
le f
or d
efin
ition
s
M.D. LEBOWITZ1042
MO
STA
RD
I19
81[2
37]
Ohi
o, U
SA21
–77
x (9
mo)
:(S
O4
x (9
mo)
:x=
54Si
gnif
ican
t in
crea
se i
n re
spir
ator
yM
OST
AR
DI
1981
[238
](c
hild
ren)
51–5
511
–12)
(27+
)sy
mpt
oms;
sm
all
decr
emen
ts i
n lu
ng(N
O3
4–5)
func
tion;
no
indo
or m
easu
rem
ents
; co
nfou
nder
s in
mod
els
KR
ZY
ZA
NO
WSK
I19
90[1
60]
Tuc
son,
AZ
,lo
wIn
med
ians
:In
<23
5In
TW
A w
ith t
ime-
activ
ities
and
act
ual
QU
AC
KE
NB
OSS
1989
[84]
USA
8.9–
35.7
med
ians
:m
edia
ns:
mea
sure
men
ts o
f PM
; PM
-ET
S,Q
UA
CK
EN
BO
SS19
91[1
76]
75th
% 7
7.8
17.5
–80.
811
.5–3
6.8
HC
HO
-ET
S, N
O2,
pol
len
asso
ciat
edL
EB
OW
ITZ
1990
[85]
(wee
kly)
Out
<60
75th
%w
ith s
igni
fica
nt i
ncre
ase
in p
reva
lenc
eL
EB
OW
ITZ
1992
[161
]75
th%
105
17.7
–47.
2ra
tes
of b
ronc
hial
res
pons
iven
ess;
LE
BO
WIT
Z19
93[1
75]
(wee
kly)
Out
: 34
–48
HC
HO
-ET
S al
so a
ssoc
iate
d w
ith a
sthm
aan
d ch
roni
c br
onch
itis;
SE
S, m
edic
atio
n,al
l A
P, m
eteo
rolo
gy,
age,
sex
in
mod
els
NE
RI
1975
[239
]O
ntar
io,
<85
0<
500
Dec
reas
ed l
ung
func
tion
and
incr
ease
dC
anad
ax=
46–5
2x=
90–9
3pr
eval
ence
rat
es o
f ch
roni
c br
onch
itis
(LO
EL
)B
EC
KL
AK
E19
75[2
40]
Mon
trea
l,15
–123
84–1
31N
o di
ffer
ence
s be
twee
n ar
eas
in l
ung
AU
BR
Y19
79[2
41]
Can
ada
(adu
lts)
func
tion
afte
r sm
okin
g co
ntro
lled
INFA
NT
E-
1993
[242
]M
ontr
eal
??
Pers
onal
Incr
ease
d pr
eval
ence
rat
e of
ast
hma;
RIV
AR
D(c
hild
ren)
1–>
28SE
S an
d E
TS
in m
odel
sST
ER
N19
94[2
43]
Can
ada
low
SO4
1.9
vsx=
18–2
3>
156
low
No
incr
ease
in
chro
nic
sym
ptom
s;(c
hild
ren)
6.6
low
er f
unct
ion
in m
ore
pollu
ted
com
mun
ities
LA
MB
ER
T19
70[2
44]
Bri
tain
90B
S=70
Incr
ease
d pr
eval
ence
rat
es o
f L
RIs
;(c
hild
ren)
incr
ease
d br
onch
itis
prev
alen
ce r
ates
(adu
lts)
>10
0>
100
and
low
er l
ung
func
tion
LU
NN
1967
[187
]B
rita
in18
1–27
5B
S=23
0–30
1In
crea
sed
prev
alen
ce r
ates
of
sym
ptom
sL
UN
N19
70[2
45]
(chi
ldre
n)94
–253
48–1
69an
d fu
nctio
n; n
o ef
fect
s se
enM
EL
IA19
77[2
01]
Eng
land
19–1
45B
S=12
–73
16–5
30In
crea
sed
prev
alen
ce r
ates
of
resp
irat
ory
ME
LIA
1981
[202
](c
hild
ren)
Indo
ors
dise
ase;
mos
t co
nfou
nder
s co
ntro
lled
KE
RR
EB
IJN
1975
[246
]N
ethe
rlan
ds15
0B
S <
30In
crea
sed
coug
h, b
ut l
ung
func
tion
(chi
ldre
n)(L
OE
L)
NS
FISC
HE
R19
85[2
47]
Net
herl
ands
??
15–3
00D
ecre
ased
lun
g fu
nctio
n re
late
d to
FISC
HE
R19
86[2
48]
(adu
lt fe
mal
eN
O2
in m
odel
sR
EM
IJN
1985
[249
]no
nsm
oker
s)D
IJK
STR
A19
90[2
50]
Net
herl
ands
??
?22
–42
No
incr
ease
d re
spir
ator
y sy
mpt
oms
orH
OU
TH
UIJ
S19
87[2
51]
(chi
ldre
n)23
–72
lung
fun
ctio
n de
clin
eB
RU
NE
KR
EE
F19
90[2
52]
SAW
ICK
I19
69[2
53]
Cra
cow
,x=
45,
x=90
,In
crea
sed
CO
PD; o
ther
fac
tors
in m
odel
;S A
WIC
KI
1977
[254
]Po
land
125
170
late
r, J
edry
chow
ski
(com
mun
icat
ion)
sh
owed
rel
atio
n to
mod
elle
d ac
id;
larg
er(a
dults
)ve
ntila
tory
dec
lines
tho
ught
rel
ated
to
occu
patio
nal a
nd e
nvir
onm
enta
l exp
osur
esan
d sm
okin
g ha
bits
. (K
RA
ZY
ZA
NO
WSK
Iet
al.,
1990
[28
4])
RU
DN
IK19
78[2
55]
Nea
r C
raco
w14
8–18
0B
S 15
0–22
7In
crea
sed
resp
irat
ory
sym
ptom
s in
boy
s
see
end
of t
able
for
def
initi
ons
Tab
le 5
. –
C
ont..
......
...
Exp
osur
es
µg·
m-3
#Fi
rst
Loc
atio
nau
thor
Y
ear
[R
ef]
(po
pula
tion)
S
O2
TSP
P
M2.
5/B
S
PM10
O3*
NO
2R
esul
ts
EPIDEMIOLOGICAL STUDIES OF AIR POLLUTION EFFECTS 1043
PAA
RC
1982
[256
]Fr
ance
??
12–1
6N
o ef
fect
s; n
o in
door
mea
sure
men
ts†
PAA
RC
1983
[257
](a
dults
)R
AM
AC
IOT
TI
1977
[258
]G
enev
a,10
–60
?In
crea
sed
chro
nic
bron
chiti
s, p
reva
lenc
eSw
itzer
land
rate
s an
d de
crea
sed
PEF
with
SO
2an
d(a
dult
men
)sm
okin
gB
RA
UN
-19
89[2
59]
Switz
erla
nd?
??
25–5
2In
crea
sed
resp
irat
ory
sym
ptom
s w
ithFA
HR
LA
ND
ER
(chi
ldre
n)(O
ut)
NO
2≥3
0 µ
·m-3
outd
oors
†
6–91
(In
)G
SCH
WE
ND
-19
89[2
60]
Switz
erla
nd?
??
x 26
.2 v
sB
ronc
hial
rea
ctiv
ity i
ncre
ased
in
EIG
EN
MA
NN
(chi
ldre
n)36
.2no
nast
hmat
ic c
hild
ren†
SCH
MIT
ZB
ER
GE
R19
93[2
61]
Aus
tria
n A
lps
12–2
0?
200–
286
15–3
3D
ecre
ased
lun
g fu
nctio
n an
d in
crea
sed
(chi
ldre
n)(p
roba
bly
asth
ma
(O3)
; SE
S, i
ndoo
r su
rrog
ates
,hi
gh)
age,
sex
in
mod
els
KU
EH
R19
91[2
62]
Sout
hern
Ger
man
y?
?I/
OIn
crea
sed
prev
alen
ce r
ate
of a
sthm
a(c
hild
ren)
mea
sure
-w
ith h
ighe
r in
door
NO
2in
dexe
d to
gas
men
tsst
oves
: E
TS
in m
odel
†
VO
NM
UT
IUS
1992
[263
]L
eipz
ig a
nd<
350
<28
018
6x
39Si
gnif
ican
tly i
ncre
ased
pre
vale
nce
rate
sM
unic
h,<
25<
7023
658
of c
hron
ic b
ronc
hitis
in
Lei
pzig
and
of
Ger
man
y(m
onth
ly)
(lig
ht(3
0 m
in)
asth
ma
in M
unic
h; o
ther
fac
tors
(chi
ldre
n)sc
atte
r)co
ntro
lled
ZA
PLE
TA
L19
73[2
64]
Cze
chos
lova
kia
>24
0>
240
Dec
reas
ed p
ulm
onar
y fu
nctio
n(c
hild
ren)
(24
h)(2
4 h)
(flo
ws)
S PIN
AC
I19
85[2
65]
Tur
in,
Ital
y60
–200
110–
150
Initi
ally
, lo
wer
fun
ctio
n w
ith h
ighe
rA
RO
SSA
1987
[266
](c
hild
ren)
50–1
1080
–110
pollu
tion
data
; la
ter,
no
diff
eren
ce;
adju
sted
for
ET
S, S
ES
PET
RIL
L19
66[2
67]
Gen
oa,
Ital
y53
–404
80–8
50hi
ghSi
gnif
ican
tly i
ncre
ased
chr
onic
(a
dults
)(2
4 h)
(24
h)br
onch
itis
with
SO
2; w
eath
er,
othe
r A
Pan
d ot
her
fact
ors
in m
odel
s; a
ll lo
w S
ES
SAR
IC19
81[2
68]
Cro
atia
≤550
x=20
0[S
O4=
3–42
]Si
gnif
ican
t dec
reas
e in
lung
fun
ctio
n an
d(c
hild
ren)
(24
h)(2
4 h)
–360
(24
h)in
crea
sed
sym
ptom
s w
ith T
SP >
130,
SO2
>60
ann
ual
av;
indo
or,
and
othe
rfa
ctor
s in
mod
elP E
RSH
AG
EN
1984
[269
]H
elsi
nki,
Finl
and
??
5–70
CO
PD c
orre
late
s w
ith N
O2;
tem
p. i
n(a
dults
)m
odel
; no
cov
aria
tes†
GO
RE
N19
88[2
70]
Isra
el?
??
x=In
crea
sed
resp
irat
ory
sym
ptom
s;(c
hild
ren)
23 v
s 62
conf
ound
ers
cont
rolle
d†Sp
ekto
r19
91[1
15]
Cub
ata,
Bra
zil
?64
–104
??
Lun
g fu
nctio
n m
easu
res
sign
ific
antly
(chi
ldre
n)de
crea
sed
rela
ted
to P
M10
(abo
ut 1
00m
L·s
-1pe
r 50
µg·
m-3
)†T
SUN
ET
OSH
I19
71[2
71]
Osa
ka,
Japa
n0.
5–4.
6du
stSO
2si
gnif
ican
tly r
elat
ed t
o ch
roni
c(a
dults
)µ
g·10
0fa
llbr
onch
itis
(not
dus
t fa
ll);
smok
ing,
cm-2
daily
othe
r fa
ctor
s in
mod
elY
OSH
IDA
1976
[272
]Ja
pan
110–
120
LO
EL
SO4
40–1
20In
crea
sed
prev
alen
ce r
ates
of
asth
ma
S UZ
UK
I19
78[2
73]
Japa
n (a
dult
58–9
712
2–43
4In
crea
sed
chro
nic
resp
irat
ory
sym
ptom
s,fe
mal
es)
also
rel
ated
to
age
see
end
of t
able
for
def
initi
ons
Tab
le 5
. –
C
ont..
......
...
Exp
osur
es
µg·
m-3
#Fi
rst
Loc
atio
nau
thor
Y
ear
[R
ef]
(po
pula
tion)
S
O2
TSP
P
M2.
5/B
S
PM10
O3*
N
O2
Res
ults
M.D. LEBOWITZ1044
YA
NO
1990
[274
]Ja
pan
(adu
lt?
119–
341
No
incr
ease
in
chro
nic
sym
ptom
s†fe
mal
es)
(win
ter)
NIT
TA
1993
[275
]T
okyo
, Ja
pan
64–7
724
h:
45–
Sign
ific
ant
incr
ease
of
≥35%
in
chro
nic
(adu
lt13
0 (N
O=
resp
irat
ory
sym
ptom
s at
hig
her
NO
2fe
mal
es)
97–1
26 p
pb)
leve
ls;
mod
els
incl
uded
age
, sm
okin
g,du
ratio
n of
res
iden
ce,
SES,
hom
ehe
atin
g; o
ther
AP
not
incl
uded
HE
1993
[276
]W
uhan
, C
hina
8–24
536
–648
51–2
07N
Ox
4–24
43.
8% l
ower
FE
V1
asso
ciat
ed w
ith A
P,(a
dults
)as
wer
e sy
mpt
oms;
eff
ects
of
spec
ific
AP
not
diff
eren
tiate
dX
U19
91[2
77]
Bei
jing,
Chi
na18
–128
261–
449
Sign
ific
antly
red
uced
lung
fun
ctio
n re
late
d(a
dults
)to
SO
2or
TSP
, an
d in
door
hea
ting;
othe
r fa
ctor
s in
mod
els
TA
M19
94[2
78]
2 di
stri
cts
of4–
177
43–1
33R
SP 3
0–68
15–4
9Si
gnif
ican
tly i
ncre
ased
bro
nchi
alH
ong
Kon
gre
spon
sive
ness
, esp
ecia
lly in
non
whe
ezin
g;(c
hild
ren)
nona
sthm
atic
s, m
ostly
in
boys
; ad
just
edfo
r SE
S, h
ouse
typ
e, p
assi
ve s
mok
ing;
effe
cts
of d
iffe
rent
AP
not
dete
rmin
ed*:
mea
n of
dai
ly m
axim
um 1
h u
nles
s ot
herw
ise
stat
ed;
†: f
rom
EPA
Cri
teri
a D
ocum
ents
. SE
S: S
ocio
econ
omic
sta
tus;
TW
A:
time-
wei
ghte
d av
erag
e; H
CH
O:
form
alde
hyde
; E
TS:
env
i-ro
nmen
tal
toba
cco
smok
e; C
OPD
: ch
roni
c ob
stru
ctiv
e pu
lmon
ary
dise
ase;
RH
: re
lativ
e hu
mid
ity;
I/O
: In
door
/Out
door
rat
io.
For
furt
her
defi
nitio
ns s
ee l
egen
ds t
o ta
bles
1,
2 an
d 4.
Tab
le 5
. –
C
ont..
......
...
Exp
osur
es
µg·
m-3
#Fi
rst
Loc
atio
nau
thor
Y
ear
[R
ef]
(pop
ulat
ion)
SO
2T
SP
P
M2.
5/B
S
PM
10O
3*
NO
2R
esul
tsobserved association. In contrast to the six city study, inthe longitudinal study in California with data on indi-viduals, including individual estimates of exposure [41],no association was found with all cause or cause-spe-cific mortality (table 1).
Though previous reviews did not conclude that airpollution could cause lung cancer [4, 5, 12], two recentstudies have indicated an association [50, 282], raisingthe issue once again.
Chronic respiratory morbidity
Only PM is definitely known to produce chronic res-piratory disease, for which AQGs have been written [61,39], but there is evidence that ozone [13], and NO2 [10]may also produce such diseases. Table 5 presents the quan-titative results concerning chronic effects, as obtainedwhen available from the multiple studies mentioned below.It should be noted that the role of the indoor environ-mental contaminants, especially due to combustion prod-ucts and bioaerosols (including allergens), is also consideredquite substantial by itself [8, 16].
PM/SOx. Respiratory symptoms and deterioration in lungfunction in populations (studied cross-sectionally or longi-tudinally), and longitudinal changes, are greater in thosethat reside in polluted areas than those residing in clea-ner areas [4, 6, 8, 9, 12, 13, 15, 25, 41, 61, 102, 179,186, 215, 218, 223–225, 228, 229, 235, 244, 263, 283–288]. The pollutant mix invariably contains PM but alsooften contains SO2, NO2, or O3. The effects of specificspecies of PM have not been delineated, though SO4 andH2SO4 have been implicated specifically in chronic obstruc-tive lung disease (COPD) [10, 236, 243, 289].
Childhood chronic bronchitis was more associated withtypical SO2 and PM pollution in Germany [263], as hadbeen found in the UK [4, 5, 191, 244]. It is thought thatthis may be the case in the parts of Central and EasternEurope that are still polluted primarily by PM and SO2.Chronic lung conditions in children and adults in less-developed countries are thought to be related to indoorcombustion products [12, 15, 17, 18].
PM/NOx. Geographic differences occur in the prevalencerates of asthma as well, based on more recent studies [5,13]. For instance, there is an increased level of asthmaeven when risk factors for asthma in different commu-nities may be similar, when there is more pollution frompower plants [290], or when there is more pollution fromauto exhaust [41, 235, 263]. The relationship of asthmaprevalence (and immunological changes) to auto exhaustwas also noted by ZWICK et al. [291]. These studies implysome possible link to a PM-NO2 complex, and some pos-sible role of hydrocarbons (as has been shown in min-ing). There is an AQG for NO2 to avoid chronic effects[61].
ETS. Passive smoking (ETS) has been found to be asso-ciated with COPD [159, 292]. ETS in the presence offormaldehyde has been shown to relate to increased preva-lence rates of childhood asthma and bronchial respon-siveness, whilst formaldehyde alone was also associatedwith increased prevalence rates of childhood chronic
bronchitis [160]. INFANTE-RIVARD [242] reported thatmonitored NO2 had a dose-response relationship withasthma in a case-control study; she also showed thatquestionnaire information on mothers' heavy smoking,bedroom humidifiers, home heating, a history of pneu-monia, a family history of asthma, and the absence ofbreast-feeding might be important. Other questionnairesurveys, with appropriate controls for these other vari-ables, have yielded conflicting relationships with passivesmoking [159]. Many other surveys have not had appro-priate controls, especially for family history, and havenot measured pertinant pollutants that might affect asth-ma.
Other pollutants. The effect of other chemical pollutantexposures on the incidence of asthma is not sufficientlyknown. However, it is known that aeroallergens are stron-gly associated [8, 249]. There are also some low mole-cular weight chemicals [171, 172, 293] and certain metals,such as chromium and nickel (WHO EHCs) which can,with significant exposures, produce asthma. Chemicalpollutants can also act as adjuvants with allergens in thedevelopment of asthma [8]. In addition, chronic expo-sure to high levels of volatile organic compounds (VOCS)and to NOx are related to chemical pneumonitis [25, 120].
Risk assessment. COPD appears to increase significantly(relative risk (RR) of 1.5–2.5) as annual TSP increasesabove 100 µg·m-3 and SO2 (concurrently). Chronic bronchi-tis appears to increase linearly with SO4: every 2 µg·m-3
above 5.8 µg·m-3 adds 1.24% to the prevalence rate [289].In urban areas, significantly more chronic COPD symp-toms may occur with SO4 above 9 µg·m-3 in the pres-ence of high SO2 and TSP, and 15+ without high TSP[10]. In a Californian study [236], asthma was also foundto increase significantly with SO4 by about 2.9 times per7 µg·m-3. The Cracow study found a 24% prevalencerate of chronic bronchitis in males (11.5% in women)[253, 254]. Many estimates have been made of excessAOD in parts of Europe, due to the excessive PM/SOxpollution in certain locales; they have been quite large(e.g. 2–7 million cases). A 24 h guideline of 180 µg·m-3
of NO2 was also established by the WHO [61] to avoidchronic effects of repeated exposures.
Lung function and particulates
Differences in lung function in children residing invarious areas have also been related to the many differ-ences in air pollution in those areas [4–7, 13]. Fur-thermore, TOYAMA [287] and WATANABE [294] showedimprovement in peak expiratory flow rates in childrenliving in more polluted communities when air pollutionconcentrations decreased. In France, the PAARC study[256] found differences in children but not in adult fe-males related to SO2. The sulphate and nitrate particu-late forms of SOx and NOx appear to have greater impacton lung function in normals than the gaseous form becausethey have greater airway penetration [4, 8, 25, 102].
Several studies of indoor pollution have shown rela-tionships between monitored NO2 and PM and reducedlung function [8, 11, 84, 85, 175, 199, 250]. Passivesmoking over long periods of time in susceptible chil-dren leads to significantly slower and reduced lung growth
[295], and in children in the general population to areduction of 0.1–3% in FEV1 [159].
Significant decrements (3–8%) appear to be related toambient annual TSP above 180 µg·m-3 (PM10 about 110µg·m-3) (also associated with SO2), or 100 µg·m-3 of SO4and SO2 in children. Significant differences (<3%) occurin children related to ETS (mostly PM2.5) differences of60–100 µg·m-3 or more. Decreases occur more frequentlyand are larger in those starting with low lung function,bronchial responsiveness, and/or a chronic respiratorydisease.
Bronchial responsiveness is related to various contami-nants. Increased bronchial responsiveness was found inchildren in relation to O3, possibly related to T-lym-phocyte changes but not to atopy or immunoglobulin E(IgE), in an area of high ozone levels in Austria [291].Increased BR has also been found in an urban-industrialarea in Latium, Italy, even though baseline lung func-tion and atopy were not different, and after controllingfor ETS exposure and other risk factors [296]. It has alsobeen found that the relationship of BR (indexed by diur-nal PEF) and PM2.5 occurred primarily in homes inde-pendent of ETS, although rates of BR were higher inhomes with more PM10 and ETS; the rates of BR in chil-dren were independently related to ETS [161]. Preval-ence rates of BR are independently associated withincreasing exposure to HCHO, and to NO2 [176]; thelatter association has also been found experimentally[109]. Several metals have also been associated withincreased bronchial responsiveness (nickel, chromium,vanadium, platinum salts) [10, 12, 25, 171]. As discussedpreviously, BR is longitudinally associated with reducedlung function (op cit.). Both BR and asthma in child-hood are associated with as much as a 25% decrement infunction at the onset of adulthood ([208]; S. Weiss, per-sonal communication).
Chronic outcomes of acute changes
Do acute morbidity effects lead to chronic effects?Those with chronic obstructive airway disease have ahistory of significantly more frequent and severe ARIs[210, 279] and a significant history of childhood respira-tory problems [205, 210]. It is also known that childhoodARIs are longitudinally associated with a decrement oflung function [208]. A study of acute pulmonary func-tion changes in healthy children in a smelter town [19]indicated significant acute reversible changes. A furtherstudy of children in that town, another smelter townand a control town [228, 229], indicated that pulmonaryfunction values were lower overall in the smelter towns(even despite potential selective migration). Thus, thereare grounds for a possible relationship between acute andchronic pulmonary function changes. Furthermore, it issometimes difficult to separate the acute (peak) exposureeffects from the chronic exposure effects ([84, 102, 176,239]; M. Green, public comments at ERS, Firenze, 1993).
Discussion
The separate effects of gases and PM, though diffi-cult, have been investigated, both epidemiologically as
EPIDEMIOLOGICAL STUDIES OF AIR POLLUTION EFFECTS 1045
well as in controlled human exposure studies. PM andgases appear to have an interactive effect in clinical andepidemiological studies (e.g. formaldehyde particles, radonand particles, gases and particles in passive smoking,ambient ozone and/or NO2 and PM). It is still difficultto evaluate the impact of short-term exposures, includ-ing peak exposures, on chronic conditions (SO2 as in-termittent outdoor peaks, has also been associated withacute and chronic respiratory conditions [5]). The roleof "peak" exposures to gases (NO2, O3, SO2) has alsobeen related to bronchial responsiveness (as discussed).
Factors affecting responses. It has been mentioned thattemperature is usually even more important than air pol-lutants; humidity is also an important factor. For instance,heat and relative humidity (RH) may contribute to symp-toms and physiological impairment. A hot (31–40°C)and/or humid (85% RH) environment, combined withexercise, has been shown to reduce forced expiratoryvolume more than similar exposures (25°C, 50% RH)[297, 298]. Modification of the effects by heat or humi-dity stress may be attributed to increased ventilation as-sociated with elevated body temperature but there mayalso be an independent effect of elevated body tempera-ture on pulmonary function. Also, increased ventilationat altitude, as in exercise, increases doses of pollutantsin the lung (tracheobronchial and alveoli), as adequatelevels of ventilation are necessary to maintain sufficientO2 partial pressures in alveolar and arterial blood. Thus,all considerations of the effects of air pollutants musttake these factors into account.
Effect-modifiers and factors affecting confounding. Hostfactors are significant effect modifiers. Immunologicaland physiological status appear to be the most important[8, 11, 12, 16, 22, 55, 175, 179, 208, 293, 295]. (As dis-cussed above, prior ARIs and concurrent morbidity arealso of importance). These potential links require furtherstudy.
Not all potential confounders are important per se [6].Follow-up studies on a cohort started by DOUGLAS et al.[186] did not confirm original social class differences tobe significant in accounting for health findings later inlife. MANFREDA et al. [285] did not find "urban" charac-teristics to be relevant in explaining results. Thus, oneshould not overemphasize the relative importance ofpotential confounding or covariant factors when thesehave not been specifically ruled out as alternative expla-nations for specific results [6].
Conclusions
The most important aspects of this issue need to beaddressed [4–9, 17, 18, 22, 60, 299, 300]: 1) pollutionexposure is a cause, albeit with others (and not the mostpotent) of chronic respiratory disease; 2) it is a majorcause of exacerbations of asthma and COPD. (both aspectsare responsible for major disability, cost, and reductionin the quality of life); 3) it influences (and is part of) theaetiological and natural history chain of chronic respira-tory disease, which includes increased ARIs, increasedinflammation and bronchial reactivity, and reduced lungfunction. The first two would also imply that at least
some pollutants alter immunological function in morethan one way, as found in animal studies [301], and pos-sibly in human studies [302, 303]. Thus, further studiesof the epidemiology of air pollution and its control arenecessary [8, 10, 304–306].
With regard to asthma and chronic obstructive pul-monary disease, we consider the following to be the futureepidemiological perspectives: methods of interventionand associated studies; methods of ascertaining patho-physiological and immunological changes, including bio-markers of noncarcinogenic and of acute changes; furtherstudies of irritation and reactive airways dysfunction syn-drome (RADS) (with respect to asthma and chronicobstructive pulmonary disease), the study of the role ofacute effects in the aetiology and natural history of chro-nic disease; and methods and studies to ascertain quan-titative exposure dose-response relationships for individualair pollutants and complex mixes.
Acknowledgements: The authors wish to acknowledgeI. Hewitt, administrative assistant, without whom this workcould not have been accomplished.
References
1. Sandström J. Respiratory effects of air pollutants: exper-imental studies in humans. Eur Respir J 1995; 8: 976–995.
2. Chitano P, Hosselet JJ, Mapp CE, Fabbri LM. Effect ofoxidant air pollutants on the respiratory system: insightfrom experimental animal research. Eur Respir J 1995;8: 1357–1371.
3. Heyder J, Takenaka S. Long-term canine exposure stud-ies with ambient air pollutants. Eur Respir J 1996; 9:571–584.
4. ATS (Shy C, Goldsmith J, Hackney J, Lebowitz M,Menzel D). Statement on the Health Effects of AirPollution. American Thoracic Society, NY, 1978.
5. EPA. Particulate Matter and Sulfur Oxides, Air QualityCriteria, R.T.P. (NC), 1982; 2nd Addendum, 1986.
6. Lebowitz MD. Utilization of data from human popula-tion studies for setting air quality standards: evaluationof issues. Environ Health Persp 1983; 52: 193–205.
7. Lebowitz MD, Dodge R, Holberg J. The effects of theenvironment on pulmonary function in children. In:Castello D, ed. Bronchopneumologia Pediatrica. Turin,Verduci Editore, 1983; pp. 187–196.
8. NRC (US National Research Council). Particulate poly-cyclic organic matter, 1972; vapor-phase organic pollu-tants, 1976; Arsenic, 1977; Carbon monoxide, 1977;nitrogen oxides, 1977; Ozone and other photochemicaloxidants, 1977; Airborne particles, 1977; sulfur oxides,1978; Formaldehyde, 1981; Indoor pollutants, 1981;Epidemiology and air pollution, 1985; Human exposureassessment for airborne pollutants, 1991; Indoor aller-gens, 1993. Washington, DC, National Academy Press.
9. Ware J. Assessment of the health effects of SOx andPM: analysis of the exposure-response relationship.Research Triangle Park, NC, US, EPA, 1980.
10. WHO/EURO. Air Quality Guidelines for Europe. Copen-hagen and Geneva, 1987.
11. Lebowitz MD. Pulmonary responses to multipollutantairborne particulate matter and other contaminants, withprevention strategies. In: Hirsh A, ed. Prevention ofRespiratory Diseases. New York, Marcel Dekker, 1993;pp. 209–223.
12. WHO. Guidelines on Studies in Environmental Epidemio-logy. (EHC 27) Geneva, 1983.
M.D. LEBOWITZ1046
13. EPA. Ozone and Other Photochemical Oxidants. Vol.5. Air Quality Criteria, R.T.P. (NC), 1984.
14. EPA. Air Quality Criteria for Oxides of Nitrogen.Washington, DC, 1993.
15. WHO. Estimating human exposure to air pollutants.Geneva and Copenhagen, 1982.
16. WHO/EURO. Indoor air pollutants: exposure and healtheffects (WHO/EURO Reports & Studies 78), 1982;Research (Euro Reports and Studies 103), 1986; Formal-dehyde and radon (Env. Hlth. 13), 1986; Organic pollu-tants (Rep. & Studies 111), 1989; Biological contaminants(Euro. Series 13), 1990; Combustion products, Copen-hagen, (in press).
17. Bates DV. Observations on asthma. Environ HealthPersp 1995; 103(6): 243–247.
18. Bates DV. The effects of air pollution on children.Environ Health Persp 1995; 103(6): 49–53.
19. Lebowitz MD, Bendheim P, Cristea G, et al. The effectof air pollution and weather on lung function in exer-cising children and adolescents. Am Rev Respir Dis 1974;109: 262.
20. Lebowitz MD. Airway responses in children related toenvironmental irritants, (Editorial). Ped Pulmonol 1985;1: 235–236.
21. Lebowitz MD, Holberg CJ, Boyer B, Hayes C. Respiratorysymptoms and peak flow associated with indoor and out-door air pollutants in the Southwest. JAPCA 1985; 35:1154–1158.
22. Lebowitz MD, Burrows B. Risk factors in induction oflung disease: an epidemiologic approach. In: Stein RP,Weinbaum G, eds. Mechanisms of Lung Injury. Phila-delphia, Stickley Co., 1986; pp. 208–222.
23. Lebowitz MD, Quackenboss J, Camilli AE, BronnimanD, Holberg CJ, Boyer B. The epidemiological impor-tance of intraindividual changes in objective pulmonaryresponses. Eur J Epidemiol 1987; 3: 390–398.
24. Stebbings JH, Fogelman DG. Identifying a susceptiblesubgroup: effects of the Pittsburgh air pollution episodeupon schoolchildren. Am J Epidemiol 1979; 110: 27–40.
25. WHO (World Health Organization). EnvironmentalHealth Criteria, Geneva. Oxides of Nitrogen, 1977; Pho-tochemical oxidants, 1978; Sulfur oxides and suspendedparticulate matter, 1979; Carbon monoxide, 1979; Arsenic,1981.
26. Martonen TB, O'Rourke MK. Disposition of mulberrypollen in the human respiratory system: a mathematicalmodel. Grana 1993; 32: 290–301.
27. Logan WPD. Mortality in the London fog incident.Lancet 1953; i (Feb. 14): 336–339.
28. Ministry of Health. Mortality and morbidity during theLondon fog of December 1952. Report on Public andMedical Subjects No. 95. Her Majesty's Stationery Office,London, 1954.
29. Martin AE, Bradley WH. Mortality, fog and atmosphericpollution: an investigation during the winter of 1958–1959. Monthly Bulletin, Minist of Health Public HealthLab (GB) 1960; 19: 56–73.
30. Lawther PJ. Compliance with the clean air act: medicalaspects. J Inst Fuel 1963; 36: 341.
31. Buechley RW, Riggan WB, Hasselbald W, Van BruggenJB. SO2 levels and perturbations in mortality: a studyin New York Jersey metropolis. Arch Environ Health1973; 27: 134–137.
32. Pope CA, Schwartz J, Ransom MR. Daily mortality andPM10 pollution in Utah Valley. Arch Environ Health1992; 47: 211–217.
33. Lyon JL, Mori M, Gao R. Is there a causal association
between excess mortality and exposure to PM10 airpollution? Additional analyses by location, year, seasonand cause of death. Inhal Toxicol 1995; 7(5): 603–614.
34. Schwartz J, Dockery DW. Particulate air pollution anddaily mortality in Steubenville, Ohio. Am J Epidemiol1992; 135: 12–19.
35. Li Y, Roth HD. Daily mortality analysis by using dif-ferent regression models in Philadelphia County, 1973–1990. Inhal Toxicol 1995; 7: 45–58.
36. Hatzakis A, Katsouyanni K, Kalandidi A, Day N,Trichopoulos D. Short-term effects of air pollution onmortality in Athens. Int J Epidemiol 1986; 15(1): 73–81.
37. Katsouyanni K, Pantazopoulou A, Touloumi G, et al.Evidence for interaction between air pollution and hightemperature in the causation of excess mortality. ArchEnviron Health 1993; 48: 235–242.
38. Touloumi G, Pocock SJ, Katsouyanni K, TrichopoulosD. Short-term effects of air pollution on daily morta-lity in Athens: a time-series analysis. Int J Epidemiol1994; 23: 1–11.
39. Fairley D. The relationship of daily mortality to sus-pended particulates in Santa Clara county, 1980–1986.Environ Health Persp 1990; 89: 159–168.
40. Shumway RH, Azari AS, Pawitan Y. Modeling mor-tality fluctuations in Los Angeles as functions of pollu-tion and weather effects. Environ Res 1988; 45: 224–242.
41. Abbey DE, Lebowitz MD, Mills PK, Petersen FF, BeesonWL, Burchette RJ. Long-term ambient concentrationsof particulates and oxidants and development of chronicdisease in a cohort of nonsmoking California residents.Inhal Toxicol 1995; 7: 19–34.
42. Kinney PL, Ito K, Thurston GD. A sensitivity analysisof mortality/PM10 associations in Los Angeles. InhalToxicol 1995; 7: 59–69.
43. Dockery EW, Schwartz J, Spengler JD. Air pollutionand daily mortality: associations with particulates andacid aerosols. Environ Res 1992; 59: 362–373.
44. Schwartz J, Slater D, Larson TV, Pierson WE, KoenigJQ. Particulate air pollution and hospital emergency roomvisits for asthma in Seattle. Am Rev Respir Dis 1993;147: 826–831.
45. Ozkaynak H, Xue J, Severance P, Burnett R, RaizenneM. Associations between daily mortality, ozone, andparticulate air pollution in Toronto, Canada. Presentedat: Colloquim on particulate air pollution and human mor-tality and morbidity, January 1994, Irvine, CA. Universityof California at Irvine, Air Pollution Health EffectsLaboratory, Report No. 94-02.
46. Ito K, Kinney P, Thurston GD. Variations in PM10 con-centrations within two metropolitan areas and their impli-cations to health effects analyses. Inhal Toxicol 1995;7: 735–745.
47. Styer P, McMillan N, Gao F, Davis J, Sacks J. Theeffect of airborne particulate matter on daily death counts.Environ Health Persp 1995; 103(5): 490–497.
48. Ostro B, Sanchez JM, Aranda C, Eskeland GS. Air pol-lution and mortality: results of a study of Santiago, Chile.J Exp Anal Environ Epidemiol 1996; 6: 97–114.
49. Xu X, Gao J, Dockery DW, Chen Y. Air pollution anddaily mortality in residential areas of Beijing, China.Arch Environ Health 1994; 49(4): 216–222.
50. Barbone F, Bovenzi M, Cavallieri F, Stanta G. Air pol-lution and lung cancer in Trieste, Italy. Am J Epidemiol1995; 141: 1161–1169.
51. Ciocco A, Thompson DJ. A follow-up at Donora tenyears after: methodology and findings. Am J Public Health1961; 51: 155–164.
EPIDEMIOLOGICAL STUDIES OF AIR POLLUTION EFFECTS 1047
52. Phalen RF, Bates DV (eds). Proceedings of the collo-quium on particulate air pollution and human mortalityand morbidity. Inhal Toxicol 1995; 7(1): vii-163; 7(5):577–835.
53. Ostro BD, Lipsett MJ, Mann JK, Krupnick A, HarringtonW. Air pollution and respiratory morbidity among adultsin Southern California. Am J Epidemiol 1993; 137: 691–700.
54. Dockery DW, Pope III A, Spengler XX, et al. An asso-ciation between air pollution and mortality in six UScities. N Engl J Med 1993; 329: 1753–1759.
55. Lebowitz MD. Epidemiological and biomedical inter-pretations of PM10 results: issues and controversies. InhalToxicol 1995; 7: 757–758.
56. Utell MJ, Samet JM. Particulate air pollution and health:new evidence on an old problem. Am Rev Respir Dis1993; 147: 1334–1335.
57. Waller RE, Swan AV. Invited commentary: particulateair pollution and daily mortality. Am J Epidemiol 1993;135: 1–3.
58. Lebowitz MD. A comparative analysis of the stimulus-response relationship between mortality and air pollutionand weather. Environ Res 1973; 6: 106–118.
59. Lebowitz MD, Toyama T, McCarroll JR. The relation-ship between air pollution and weather as stimuli anddaily mortality as response in Tokyo, Japan with com-parison with other cities. Environ Res 1973; 6: 327–337.
60. Lebowitz MD. A comparison of the relationships ofmortality and morbidity with air pollution: weather andthe implications for further research. Sci Tot Environ1973; 2: 191–195.
61. WHO. Principles of Studies on Diseases of SuspectedChemical Etiology. Geneva, 1987.
62. Oechsli FW, Buechley RW. Excess mortality associa-ted with three Los Angeles September hot spells. EnvironRes 1970; 3: 277–284.
63. Hexter AC, Goldsmith JR. Carbon monoxide: associa-tion of community air pollution with mortality. Science1971; 172: 265.
64. HEI (Health Effects Institute). Particulate air pollutionand daily mortality: replication and validation of selec-ted studies. The Phase I report of the particle epidemio-logy evaluation project. Cambridge, MA, 1995.
65. Lawther PJ, Waller RE, Henderson M. Air pollution andexacerbations of bronchitis. Thorax 1970; 25: 525–539.
66. Lawther PJ, Brooks AGF, Lord PW, Waller RE. Day-to-day changes in ventilatory function in relation to theenvironment. Part I. Spirometric values. Environ Res1974; 7: 24–40.
67. Lawther PJ, Brooks AGF, Lord PW, Waller RE. Day-to-day changes in ventilatory function in relation to theenvironment. Part II. Peak expiratory flow values.Environ Res 1974; 7: 41–53.
68. Lawther PJ, Brooks AG, Lord PW, Waller RE. Day-to-day changes in ventilatory function in relation to the envi-ronment. Part III. Frequent measurements of peak flow.Environ Res 1974; 8: 119–130.
69. Hammer DI, Miller FJ, Stead AG, Hayes CG. Air pollu-tion and hildhood lower respiratory disease. I. Exposureto sulfur oxides and particulate matter in New York,1972. In: Clinical Implications of Air Pollution Research.Publishing Sciences 1976; pp. 321–337.
70. Love GJ, Lan S-P, Shy CM, Riggan WB. Acute respi-ratory illness in families exposed to nitrogen dioxideambient air pollution in Chattanooga, Tennessee. ArchEnviron Health 1982; 37: 75–80.
71. Pope CA, Dockery DW. Respiratory health and PM10
pollution: a daily time series analysis. Am Rev RespirDis 1991; 144: 668–674.
72. Pope CA, Dockery DW. Acute health effects of PM10
pollution on symptomatic and asymptomatic children.Am Rev Respir Dis 1992; 145: 1123–1128.
73. Cohen AA, Bromberg S, Beuchley RW, Heiderscheit LT,Shy CM. Asthma and air pollution from a coal-fueledpower plant. Am J Public Health 1972; 69: 1181–1188.
74. Hammer DI. Respiratory disease in children exposed tosulfur oxides and particulates. (EPA-600/1-77-043) USEPA, Research Triangle Park, NC, 1977.
75. Zagraniski RT, Leaderer BP, Stolwijk JA. Ambient sul-fates, photochemical oxidants, and acute health effects:an epidemiological study. Environ Res 1979; 19: 306–320.
76. Ostro BD, Lipsett MJ, Wiener MB, Selner JC. Asthmaticresponses to airborne acid aerosols. Am J Public Health1991; 81: 694–702.
77. Schwartz J, Dockery DW, Neas LM, et al. Acute effectsof summer air pollution on respiratory symptoms report-ing in children. Am J Respir Crit Care Med 1994; 150:1234–1242.
79. Schwartz J, Hasselblad V, Pitcher H. Air pollution andmorbidity: a further analysis of the Los Angeles studentnurses data. JAPCA 1988; 38: 158–162.
80. Schwartz J, Zeger S. Passive smoking, air pollution, andacute respiratory symptoms in a diary study of studentnurses. Am Rev Respir Dis 1990; 141: 62–67.
81. Whittmore AS, Korn EL. Asthma and air pollution inthe Los Angeles area. Am J Public Health 1980; 70:687–696.
82. Margolis HG, Colome SD, Westerdahl FD, Jin S, LebowitzMD. Pulmonary function and symptomatic responses ofasthmatics to acidic ambient air pollutants (Abstract).Epidemiol (in press). Presentation at ISEE-ISEA, Septem-ber 1994, RTP, NC.
83. Krzyzanowski M, Quackenboss JJ, Lebowitz, MD. Sub-chronic respiratory effects from long-term exposure toozone in Tucson. Arch Environ Health 1992; 47: 107–115.
84. Quackenboss JJ, Krzyzanowski M, Lebowitz MD. Exposureassessment approaches to evaluate respiratory healtheffects of particulate matter and nitrogen dioxide. J ExpAnal Environ Epidemiol 1991; 1: 83–107.
85. Lebowitz MD, Quackenboss JJ, Krzyzanowski M, O'RourkeMK, Hayes C. Multipollutant exposures and health res-ponses to particulate matter. Arch Environ Health 1992;47: 71–75.
86. Lebowitz MD, Collins L, Holberg C. Time series analy-sis of respiratory responses to indoor and outdoor envi-ronmental phenomena. Environ Res 1987; 43: 332–341.
87. Lebowitz MD. The effects of environmental tobaccosmoke exposure and gas stoves on daily peak flow ratesin asthmatic and nonasthmatic families. Eur J RespirDis 1984; 65 (Suppl. 133): 90–97.
88. Vedal S, Schenker MB, Munoz A, Samet JM, BattermanS, Speizer FE. Daily air pollution effects on children'srespiratory symptoms and peak expiratory flow. Am JPublic Health 1987; 77: 694–698.
89. Hoek G, Brunekreef B. Acute effects of a winter airpollution episode on pulmonary function and respira-tory symptoms in children. Arch Environ Health 1993;48: 328–335.
90. Roemer W, Hoek G, Brunekreef B. Effect of ambientwinter air pollution on respiratory health of children with
M.D. LEBOWITZ1048
chronic respiratory symptoms. Am Rev Respir Dis 1993;147: 118–124.
91. Dusseldorf A, Kruize H, Brunekreef B, Hofschreuder P,de Meer G, van Oudvorst AB. Associations of PM10 andairborne iron with respiratory health of adults living neara steel factory. Am J Respir Crit Care Med 1995; 152(6):1932–1939.
92. Makino K, Mizoguchi I. Symptoms caused by photoche-mical smog. Nippon Koshu Eisei Zasshi 1975; 22: 421–430.
93. Mizoguchi I, Makino K, Kudo S, MIkami R. On the rela-tionship of subjective symptoms to photochemical oxi-dant. In: Dimitriades B, ed. Proceedings of the internationalconference on photochemical oxidant pollution and itscontrol. EPA, 1977.
94. Shimizu T, Harada M, Miyata M, Ishikawa S, MizoguchiI. Effect of photochemical smog on the human eye: epi-demiological, biochemical, ophthalmological and exper-imental studies. Rinsho Ganka 1976; 30: 407–418.
95. Schwartz J, Spix C, Wichmann HE, Malin E. Air pol-lution and acute respiratory illness in five German com-munities. Environ Res 1991; 56: 1–14.
96. Von Mutius E, Sherrill DL, Fritzsch C, Martinez FD,Lebowitz MD. Air pollution and upper respiratory symp-toms in children from East Germany. Eur Respir J 1995;8: 723–728.
97. Forsberg B, Stjemberg N, Falk M, Lundback B, Wall S.Air pollution levels, meterological conditions and asth-ma symptoms. Eur Respir J 1993; 6: 1109–1115.
98. Burrows B, Kellogg AL, Bushey J. Relationship of symp-toms of chronic bronchitis and emphysema to weatherand air pollution. Arch Environ Health 1968; 16: 406–413.
99. Sunyer J, Saez M, Murillo C, Castellsague J, MartinezF, Anto JM. Air pollution and emergency room admis-sions for COPD: a five year study. Am J Epidemiol1993; 137: 701–705.
100. Burnett RT, Dales R, Krewski D, Vincent R, Dann T,Brook JR. Associations between ambient particulate sul-fate and admissions to Ontario hospitals for cardiac andrespiratory diseases. Am J Epidemiol 1995; 142: 15–22.
101. Delfino RJ, Becklake MR, Hanley JA. Reliability ofhospital data for population-based studies of air pollu-tion. Arch Environ Health 1993; 48(3): 140–146.
102. Finklea J. Health consequences of sulfur oxides. Environ-mental Protection Agency (EPA 650/1-74-004), 1974.
103. Hefflin BJ, Jalaludin B, McClure E, et al. Surveillancefor dust storms and respiratory diseases in WashingtonState, 1991. Arch Environ Health 1994; 49(3): 170–174.
104. Schwartz J. PM10, ozone, and hospital admissions forthe elderly in Minneapolis-St. Paul, Minnesota. ArchEnviron Health 1994; 49(5): 366–374.
105. Schwartz J. Air pollution and hospital admissions forthe elderly in Detroit, Michigan. Am J Respir Crit CareMed 1994; 150: 648–655.
106. Schwartz J. Short-term fluctuations in air pollution andhospital admissions of the elderly for respiratory disease.Thorax 1995; 50: 531–538.
107. Horstman D, Roger LJ, Kehrl H, Hazacha M. Airwaysensitivity of asthmatics to sulfur dioxide. Toxicol IndHealth 1986; 2: 289–298.
108. Koenig JQ, Hanley QS, Rebolledo V, et al. Lung func-tion changes in young children associated with particu-late matter from wood smoke. Am Rev Respir Dis 1990;141: A425.
109. Bylin G, Hedenstierna T, Lindvall T, Sundin B. Ambientnitrogen dioxide concentrations increase bronchial respon-siveness in subjects with mild asthma. Eur Respir J1988; 1: 606–612.
111. Molfino NA, Wright SC, Katz I, Tarlo S, et al. Effectof low concentrations of ozone on inhaled allergen res-ponses in asthmatic subjects. Lancet 1991; 338: 199–203.
112. Bates DV, Baker-Anderson M, Sizto R. Asthma attackperiodicity: a study of hospital emergency visits inVancouver. Environ Res 1990; 51: 51–70.
113. Samet JM, Bishop Y, Speizer FE, Spengler JD, FerrisBG Jr. The relationship between air pollution and emer-gency room visits in an industrial community. JAPCA1981; 31: 236–240.
114. Spektor DM, Lippmann M, Thurston GD, et al. Effectsof ambient ozone on respiratory function in healthy adultsexercising outdoors. Am Rev Respir Dis 1988; 138:821–828.
115. Spektor DM, Thurston GD, Mao J, He D, Hayes C, Lipp-mann M. Effects of single- and multiple-day ozone expo-sures on respiratory function in active, normal children.Environ Res 1991; 55: 107–122.
116. Spektor DM, Lippmann M, Lioy PJ, et al. Effects ofambient ozone on respiratory function in active, normalchildren. Am Rev Respir Dis 1988; 137: 313–320.
117. Thurston G, Lippmann M, Bartoszek M, Fine I. Air pol-lution associations with asthma exacerbations, peak flowchanges, and respiratory symptoms in children at a sum-mer asthma camp. Am Rev Respir Dis 1993; 147: A633.
118. Lippman M, Lioy PJ, Leikauf G, et al. Effects of ozoneon the pulmonary function of children. In: Lee SD, ed.International symposium on the biomedical effects ofozone and related photochemical oxidants. Princeton,NJ, 1983.
119. Lippman M, Lioy PJ. Critical issues in air pollutionepidemiology. Environ Health Persp 1985; 62: 243–258.
120. Bock N, Lippmann M, Lioy P, Munoz A, Speizer FE.The effects of ozone on the pulmonary function of chil-dren. In: Lee SD, ed. Evaluation of the Scientific Basisfor Ozone/Oxidants Standards. Pittsburgh, PA, 1985.
121. Lioy PJ, Vollmuth TA, Lippmann M. Persistence ofpeak flow decrement in children following ozone expo-sures exceeding the national ambient air quality stand-ard. JAPCA 1985; 35: 1068–1071.
122. Dockery DW, Ware JH, Ferris BG Jr, Spelzer FE, CookNR, Herman SM. Change in pulmonary function inchildren associated with air pollution episodes. JAPCA1982; 32: 937–942.
123. Neas LM, Dockery DW, Koutrakis P, Tollerud DJ, SpeizerFE. The association of ambient air pollution with twicedaily peak expiratory flow rate measurements in chil-dren. Am J Epidemiol 1995; 141: 111–122.
124. Selwyn BJ, Stock TH, Hardy RJ, et al. Health effectsof ambient ozone exposure in vigorously exercising adults.In: Lee SD, ed. Evaluation of the Scientific Basis forOzone/Oxidants Standards. Pittsburgh, PA, 1985.
125. Johnson DA, Winters RS, Woolley T, Graham D, Hender-son FW. Ozone effects on alpha1-proteinase inhibitor invivo: blood plasma inhibitory activity is unchanged. ExpLung Res 1986; 11: 95–103.
126. Holguin AH, Buffler PA, Contant CF Jr, et al. Theeffects of ozone on asthmatics in the Houston area. In:Lee SD, ed. Evaluation of the Scientific Basis forOzone/Oxidants Standards. Proceedings of an APCAinternational specialty conference. Pittsburgh, PA, AirPollution Control Association, 1985; pp. 262–280.
EPIDEMIOLOGICAL STUDIES OF AIR POLLUTION EFFECTS 1049
Buffler PA. Estimation of individual ozone exposuresusing microenvironment measures. In: Lee SD, ed.Evaluation of the Scientific Basis for Ozone/OxidantsStandards. Pittsburgh, PA, Air Pollution Control Associa-tion, 1985; pp. 250–261.
128. Pope CA, Kanner RE. Acute effects of PM10 pollutionon pulmonary function of smokers with mild-to-moder-ate chronic obstructive pulmonary disease. Am Rev RespirDis 1993; 147: 1336–1340.
129. Koenig JQ, Larson TV, Hanley QS, et al. Pulmonaryfunction changes in children associated with fine parti-culate matter. Environ Res 1993; 63: 26–38.
130. Linn WS, Jones MP, Bachmayer EA, et al. Short-termrespiratory effects of polluted ambient air: a laboratorystudy of volunteers in a high-oxidant community. AmRev Respir Dis 1980; 121: 243–252.
131. Linn WS, Shamoo DA, Venet TG, et al. Response toozone in volunteers with chronic obstructive pulmonarydisease. Arch Environ Health 1983; 38: 278–283.
132. Higgins ITT, D'Arcy JB, Gibbons DI, Avol EL, GrossKB. Effect of exposures to ambient ozone on ventila-tory lung function in children. Am Rev Respir Dis 1990;141: 1136–1146.
133. Gross KB, Higgins ITT, D'Arcy JB, Gibbons DI, AvolEL. Daily changes in lung ventilation induced by expo-sures to ambient ozone. In: Berglund RL, Lawson DR,McKee DJ, eds. Tropospheric Ozone and the Environ-ment. Papers from an international conference, March1990, Los Angeles, CA, Pittsburgh, PA, Air and WasteManagement Association, 1991; pp. 100–110 (A&WMAtransaction series No. TR-19).
134. Gross KB, White HJ, Sargent NE. The effect of ozoneinhalation on metabolic functioning of vascular endothe-lium and on ventilatory function. Toxicol Appl Pharmacol1991; 109: 336–351.
135. Avol EL, Trim SC, Little DE, et al. Ozone exposure andlung function in children attending a southern Californiasummer camp. Presented at 83rd annual meeting andexhibition of the Air & Waste Management Association,June, Pittsburgh, PA. Pittsburgh, PA, Air & Waste Mana-gement Association. Paper No. 90-150.3, 1990.
136. Avol EL, Trim SC, Little DE, et al. Ozone exposureand lung function: a southern California summer campstudy. In: Berglund RL, Lawson DR, McKee DJ, eds.Tropospheric Ozone and the Environment. Pittsburgh,PA, Air & Waste Management Association. 1991; pp.90–99.
137. Raizenne M, Stern B, Burnett R, Spengler J. Acute res-piratory function and transported air pollutants: obser-vational studies. Presented at 80th annual meeting ofthe Air Pollution Control Association, June, New York,NY. Pittsburgh, PA, Air Pollution Control Association.Paper No. 87-32.6, 1987.
138. Studnicka MJ, Frischer T, Meinert R, et al. Acidic par-ticles and lung function in children: a summer camp studyin the Austrian Alps. Am J Respir Crit Care Med 1995;151: 423–430.
139. Kagawa J, Toyama T. Photochemical air pollution: itseffects on respiratory function of elementary school chil-dren. Arch Environ Health 1975; 30: 117–122.
140. Kagawa J, Toyama T, Nakaza M. Pulmonary functiontest in children exposed to air pollution. In: Finkel AJ,Duel WC, eds. Clinical Implications of Air PollutionResearch. Acton, MA Publishing Sciences Group Inc.,1976; pp. 305–320.
141. Van der Lende R, Huygen C, Jansen-Koster EJ, et al.A temporary decrease in ventilatory function of an urban
population during an acute increase in air pollution. BullEur Physiopathol Respir 1975; 11: 31–43.
142. Dassen W, Brunekreef B, Hoek G, et al. Decline in chil-dren's pulmonary function during an air pollution epi-sode. JAPCA 1986; 36: 1223–1227.
143. Hoek G, Brunekreef B. Time trends in repeated spiro-metry in children. Eur Respir J 1992; 5: 553–559.
144. Hoek G, Fischer P, Brunekreef B, Lebret E, HofschreuderP, Mennen MG. Acute effects of ambient ozone on pul-monary function of children in The Netherlands. AmRev Respir Dis 1993; 147: 111–117.
145. Jaakkola JJK, Vilkka V, Marttila O, Jappinen P, HaahtelaT. The South Karelia air pollution study: the effects ofmalodorous sulfur compounds from pulp mills on respi-ratory and other symptoms. Am Rev Respir Dis 1990;142: 1344–1350.
146. Jaakkola JJK, Paunio M, Virtanen M, Heinonen OP.Low-level air pollution and upper respiratory infectionsin children. Am J Public Health 1991; 81(8): 1060–1063.
147. Moseholm L, Taudorf E, Frosig A. Pulmonary functionchanges in asthmatics associated with low-level SO2 andNO2 air pollution, weather, and medicine intake: an 8month prospective study. Allergy 1993; 48: 334–344.
148. Bates DV, Sizto R. Relationship between air pollutionlevels and hospital admissions in Southern Ontario. CanJ Public Health 1983; 74: 117–133.
149. Cody RP, Weisel CP, Birnbaum G, Lioy PJ. The effectof ozone associated with summertime photochemicalsmog on the frequency of asthma visits to hospital emer-gency departments. Environ Res 1992; 58: 184–194.
150. Thurston GD, Ito K, Kinney PL, Lippmann M. A multi-year study of air pollution and respiratory hospital admis-sions in three New York State metropolitan areas: resultsfor 1988 and 1989 summers. J Exp Anal Environ Epide-miol 1992; 2: 429–450.
151. Thurston GD, Ito K, Hayes CG, Bates DV, LippmannM. Respiratory hospital admissions and summertime hazeair pollution in Toronto, Ontario: consideration of therole of acid aerosols. Environ Res 1994; 65: 271–290.
152. White MC, Etzel RA, Wilcox WD, Lloyd C. Exacerbationsof childhood asthma and ozone pollution in Atlanta.Environ Res 1994; 65: 56–68.
153. Ponka A. Asthma and low level air pollution in Helsinki.Arch Environ Health 1991; 46: 262–270.
154. Rossi OVJ, Kinnula VL, Tienari J, Huhti E. Associationof severe asthma attacks with weather, pollen, and airpollutants. Thorax 1993; 48: 244–248.
155. Edwards J, Walters S, Griffiths RK. Hospital admis-sions for asthma in preschool children: relationship tomajor roads in Birmingham, United Kingdom. ArchEnviron Health 1994; 49(4): 223–227.
156. Romieu I, Meneses F, Sienra-Monge JJL, et al. Effectsof urban air pollutants on emergency visits for child-hood asthma in Mexico City. J Epidemiol 1995; 141:546–553.
157. Hobday JD, Stewart AJ. The relationship between dailyasthma attendance, weather parameters, spore count andpollen count. Aust NZ J Med 1973; 3: 552–556.
158. Chilmonczyk BA, Salmun LM, Megathlin KN, et al.Association between exposure to environmental tobaccosmoke and exacerbations of asthma in children. N EnglJ Med 1993; 328: 1665–1669.
159. EPA. Environmental Tobacco Smoke and RespiratoryDiseases. Washington, DC, 1992.
160. Krzyzanowski M, Quackenboss JJ, Lebowitz MD. Chronicrespiratory effects of indoor formaldehyde exposure.Environ Res 1990; 52: 117–125.
M.D. LEBOWITZ1050
161. Lebowitz MD, Quackenboss JJ. The effects of envi-ronmental tobacco smoke on pulmonary function. IntArch Occup Environ Hlth 1990; (Suppl): 147–152.
162. Lebowitz MD. Indoor Bioaerosol Contaminants. In:Lippmann M, ed. Environmental Toxicants: HumanExposures and Their Health Effects. New York, vanNostrand Reinholt, 1991; Chp. 11, pp. 331–359.
163. O'Rourke MK, Quackenboss JJ, Lebowitz MD. An epi-demiological approach investigating respiratory diseaseresponse in sensitive individuals to indoor and outdoorpollen exposure in Tucson, Arizona. Aerobiologia 1989;5: 104–110.
164. O'Rourke MK, Lebowitz MD. The importance of envi-ronmental allergens in the development of chronic andallergic lung diseases. In: Demeter SL, Cordasco E, ZenzC, eds. Environmental Respiratory Disease, Van NostrandReinhold, 1995.
165. Beggs PJ, Curson PH. An integrated environmental asth-ma model. Arch Environ Health 1995; 50(2): 87–94.
166. Lebowitz MD. The use of peak expiratory flow rate mea-surements in respiratory disease. Ped Pulmonol 1991;11(2): 166–174.
167. Postma DS, de Vries K, Koeter GH, Sluiter HJ. Indepen-dent influence of reversibility of airflow obstruction andnonspecific hyperreactivity on the long-term course oflung function. Am Rev Respir Dis 1986; 134: 276–280.
168. Sherrill D, Sears MR, Lebowitz MD, et al. Airwayhyperresponsiveness and lung function in children. PedPulmonol 1992; 13: 78–85.
169. Taylor RG, Joyce H, Gross E, Holland F, Pride NB.Bronchial reactivity to inhaled histamine and annual rateof decline in FEV1 in male smokers and ex-smokers.Thorax 1985; 40: 9–16.
170. Lebowitz MD. The trends in airway obstructive diseasemorbidity in the Tucson epidemiological study. Am RevRespir Dis 1989; 140: S35–S41.
171. Newman-Taylor A, Tee RD. Environmental and occu-pational asthma. Chest 1990; 98(5): 209S–211S.
172. Thurmond LM, Dean JH. Immunological responses fol-lowing inhalation exposure to chemical hazards. In:Gardner D, et al., eds. Toxicology of the Lung. NewYork, Raven Press, 1986; pp. 375–392.
173. Lebowitz MD, O'Rourke MK, Dodge RR, et al. Theadverse health effects of biological aerosols, other aero-sols, and microclimate indoors on asthmatics and non-asthmatics. Environ Int 1982; 8: 375–380.
174. Lebowitz MD. Health effects of indoor pollution. AnnRev Public Health 1983; 4: 203–221.
175. Lebowitz MD, O'Rourke MK, Burrows B, et al. Immuno-markers of Aeroallergen Exposure and Pulmonary Res-pones. Proc. 6th International Indoor Air Conference,Helsinki. 1993; 1: 627–632.
176. Quackenboss JJ, Lebowitz MD, Hayes C, Young CL.Respiratory responses to indoor/outdoor air pollutants:combustion products, formaldehyde and particulate mat-ter. In: Combustion Processes and the Quality of theIndoor Air Environment. (Peer-reviewed transactions).Pittsburgh, APCA, 1989; pp. 280–293.
177. Albertini M, Politano S, Berard E, Boutte P, Mariani R.Variation in peak expiratory flow of normal and asymp-tomatic asthmatic children. Ped Pulmonol 1989; 7:140–144.
179. Corbo GM, Forastiere F, Dell'Orco V, et al. Effects of
environment on atopic status and respiratory disorders inchildren. J Allergy Clin Immunol 1993; 92: 616–623.
180. Kagamimori S, Katoh T, Naruse Y, et al. The chang-ing prevalence of respiratory symptoms in atopic chil-dren in response to air pollution. Clin Allergy 1986; 16:299–308.
181. Matsumara Y. The effects of ozone, nitrogen dioxide,and sulfur dioxide on the experimentally-induced aller-gic respiratory disorder in guinea-pigs. Am Rev RespirDis 1970; 102: 430–443.
182. Riedel F, Kramer M, Scheibenbogen C, Rieger CH.Effects of SO2 exposure on allergic sensitization in theguinea-pig. J Allergy Clin Immunol 1988; 82: 527–534.
183. Takafuji S, Suzuki S, Koizumi K, et al. Diesel-exhaustparticulates inoculated by intranasal route have an adju-vant activity for IgE production in mice. J Allergy ClinImmunol 1987; 79: 639–645.
184. Cassell EJ, Lebowitz MD, McCarroll JR. The relation-ship between air pollution, weather, and symptoms in anurban population: clarification of conflicting findings.Am Rev Respir Dis 1972; 106: 677–683.
185. Colley JRT, Holland WW. Social and environmentalfactors in respiratory diseases. Arch Environ Health 1967;14: 157–161.
186. Douglas JWB, Waller RW. Air pollution and respiratoryinfection in children. Br J Prev Soc Med 1966; 20: 1–8.
187. Lunn JE, Knowelden J, Roe JW. Patterns of respira-tory illness in Sheffield junior schoolchildren: a follow-up study. Br J Prev Soc Med 1970; 24: 223–228.
188. McCarroll J, Lebowitz MD, Fairchild G. Possible effectsof air pollution on the course of infectious respiratorydiseases. In: Crocker TT, Goldsmith J, eds. Project CleanAir. Berkeley, University of California, 1970.
189. McCarroll JR, Lebowitz MD, Cassell EJ, Wolter D,Thompson DJ. Health and the urban environment. JOccup Med 1972; 14: 309–316.
190. Thompson DJ, Lebowitz MD, McCarroll JR. Health andthe urban environment. VIII. Air pollution, weather andthe common cold. Am J Public Health 1970; 60: 731–739.
191. Colley JRT, Reid DD. Urban and social origins of child-hood bronchitis in England and Wales. BMJ 1970; 2:213–217.
192. Braun-Fahrlander C, Ackermann-Liebrich U, SchwartzJ, Gnehm HP, Rutishauser M, Wanner HU. Air pollu-tion and respiratory symptoms in preschool children. AmRev Respir Dis 1992; 145: 42–47.
193. Lancet (Editorial). Indoor air pollution and acute respi-ratory infections in children. Lancet 1992; 339: 396–398.
196. Shy CM, Creason JP, Pearlman ME, McClain KE, BensonFB, Young MM. The Chattanooga schoolchildren study.I. Methods, description of pollutant exposure, and resultsof ventilatory function testing. JAPCA 1970; 20: 539.
197. Shy CM, Creason JP, Pearlman ME, McClain KE, BensonFB, Young MM. The Chattanooga schoolchildren study:effects of community exposure to nitrogen dioxide. II.Incidence of acute respiratory illness. JAPCA 1970; 20:582–588.
198. Neas LM, Ware JH, Dockery DW, Spengler JD, FerrisBG Jr, Speizer FE. The association of indoor nitrogendioxide levels with respiratory symptoms and pulmonaryfunction in children. In: Indoor Air 1990: Proceedings
EPIDEMIOLOGICAL STUDIES OF AIR POLLUTION EFFECTS 1051
of the 5th international conference on indoor air qualityand climate. Vol. Human health, comfort and perfor-mance: Ottawa, ON, Canada. International Conferenceon Indoor Air Quality and Climate Inc. 1990; pp. 381–386.
199. Neas LM, Dockery DW, Ware JH, Spengler JD, SpeizerFE, Ferris BG Jr. Association of indoor nitrogen dio-xide with respiratory symptoms and pulmonary functionin children. Am J Epidemiol 1991; 134: 204–219.
200. Samet JM, Lambert WE, Skipper BJ, et al. Nitrogendioxide and respiratory illness in infants. Am Rev RespirDis 1993; 148: 1258–1265.
201. Melia RJ, Florey CD, Altman DG, Swan AV. Associa-tion between gas cooking and respiratory disease in chil-dren. BMJ 1977; 2: 149–152.
202. Melia RWJ, Florey C du V, Chinn S. Respiratory ill-ness in British schoolchildren and atmospheric smokeand sulphur dioxide 1973-1977. II. Longitudinal find-ings. J Epidemiol Commun Health 1981; 35: 168–173.
204. Romieu I, Cortes Lugo M, Ruiz Velasco S, Sanchez S,Meneses F, Hernandez M. Air pollution and schoolabsenteeism among children in Mexico City. Am JEpidemiol 1992; 136: 1524–1531.
205. Burrows B, Knudson RJ, Lebowitz MD. The relation-ship of childhood respiratory illness to adult obstructiveairway disease. Am Rev Respir Dis 1977; 115: 751–760.
206. Horn M, Gregg I. Role of viral infection and host fac-tors in asthma and chronic bronchitis. Chest 1973: (Suppl.63): 44S–48S.
207. Krzyzanowski M, Sherrill D, Holberg C, Lebowitz MD.Modelling of longitudinal effects of ARIs on pulmonaryfunction. Am J Epidemiol 1990; 131(3): 412–422.
208. Lebowitz MD, Holberg CJ. Effects of parental smok-ing and other risk factors on the development of pul-monary function in children and adolescents: analysis oftwo longitudinal population studies. Am J Epidemiol1988; 128(3): 589–596.
209. Lebowitz MD, Quackenboss JJ, Kollander M, Soczek ML,Colome S. The new standard questionnaire for estimationof indoor concentrations. JAPCA 1989; 39: 1411–1419.
210. Paoletti P, Prediletto R, Carrozzi L, et al. Effects ofchildhood and adolescent-adult respiratory infections ina general population. Eur Respir J 1989; 2: 428–436.
211. Trigg CJ, Davies RJ. Infection, asthma and bronchialresponsiveness. Respir Med 1993; 87: 165–167.
212. Mitchell JH, Sproule BJ, Chapman CB. The physio-logical meaning of the maximal oxygen intake test. JClin Invest 1958; 37: 538.
213. Case GD, Dixon JS, Schooley JC. Interactions of bloodmetalloproteins with nitrogen oxides and oxidant air pol-lutants. Environ Res 1979; 20: 43–65.
214. Tuthill RW. Woodstoves, formaldehyde, and respira-tory disease. Am J Epidemiol 1984; 120: 952–955.
215. Lippmann M. Health effects of ozone: a critical review.JAPCA 1989; 39: 672–695.
217. Chapman RS, Shy CM, Finklea JF, House DE, GoldbergHE, Hayes CG. Chronic respiratory disease in militaryinductees and parents of school children. Arch EnvironHealth 1973; 27: 138–142.
218. Chapman RS, Hasselblad V, Hayes CG, Williams JVR,Hammer DI. Air pollution and childhood ventilatoryfunction. I. Exposure to particulate matter in twoSoutheastern cities, 1971–1972. In: Finkel AJ, Duel
WC, eds. Clinical Implications of Air Pollution Research.Acton, MA, Publishing Sciences Group, 1976.
219. Shy CM, Hasselblad V, Burton RM, Nelson CJ, CohenA. Air pollution effects on ventilatory function of USschoolchildren: results of studies in Cincinnati, Chatta-nooga, and New York. Arch Environ Health 1973; 27: 124.
220. Schwartz J, Dockery D, Ware J, et al. Acute effects ofacid aerosols on respiratory symptom reporting in chil-dren. Presented at 82nd annual meeting and exhibitionof the Air and Waste Management Association, June,Anaheim, CA. Pittsburgh, PA, Air and Waste ManagementAssociation. Paper No. 89-92.1, 1989.
221. Speizer FE, Ferris B Jr, Bishop YMM, Spengler J.Respiratory disease rates and pulmonary function in chil-dren associated with NO2 exposure. Am Rev Respir Dis1980; 121: 3–10.
222. Ware JH, Dockery DW, Spiro A III, Speizer FE, FerrisBG Jr. Passive smoking, gas cooking, and respiratoryhealth of children living in six cities. Am Rev RespirDis 1984; 129: 366–374.
223. Dockery DW, Spengler JD, Neas LM, et al. An epi-demiologic study of respiratory health status and indi-cators of indoor air pollution from combustion sources.In: Harper, JP, ed. Combustion processes and the qual-ity of the indoor environment. Pittsburgh, PA, Air &Waste Management Association, 1989; pp. 262–271.
224. Ware JH, Ferris BG Jr, Dockery DW, Spengler JD, StramDO, Speizer FE. Effects of ambient sulfur oxides andsuspended particles on respiratory health of preadoles-cent children. Am Rev Respir Dis 1986; 133: 834–842.
225. Dockery DW, Speizer FE, Stram DO, Ware JH, SpenglerJD, Ferris BG Jr. Effects of inhaled particles on respi-ratory health of children. Am Rev Respir Dis 1989; 39:587–594.
226. Neas LM, Dockery DW, Ware JH, Spengler JD, FerrisBG Jr, Speizer FE. Concentration of indoor particulatematter as a determinant of respiratory health in children.Am J Epidemiol 1994; 139: 1088–1099.
227. Chapman RS, Calafiore DC, Hasselblad V. Prevalenceof persistent cough and phlegm in young adults in rela-tion to long-term ambient sulfur oxide exposure. AmRev Respir Dis 1985; 132: 261–267.
228. Dodge R. The respiratory health of school children insmelter communities. Am J Ind Med 1980; 1: 359–364.
229. Dodge R. The respiratory health and lung function ofAnglo-American children in a smelter town. Am RevRespir Dis 1983; 127: 158–161.
230. Linn WS, Hackney JD, Pedersen EE, et al. Respiratoryfunction and symptoms in urban office workers in rela-tion to oxidant air pollution exposure. Am Rev RespirDis 1976; 114: 477–483.
231. Detels R, Sayre JW, Coulson AH, et al. The UCLApopulation studies of chronic obstructive respiratory dis-ease. Am Rev Respir Dis 1981; 124: 673–680.
232. Detels R, Tashkin DP, Sayre JW, et al. The UCLA popu-lation studies of chronic obstructive respiratory disease.9. Lung function changes associated with chronic expo-sure to photochemical oxidants: a cohort study amongnever-smokers. Chest 1987; 92: 594–603.
233. Detels R, Tashkin DP, Sayre JW, et al. The UCLA pop-ulation studies of CORD. X. A cohort study of changesin respiratory function associated with chronic exposureto SOx, NOx, and hydrocarbons. Am J Public Health1991; 81: 350–359.
234. Tashkin DP, Detels R, Simmons M, et al. The UCLApopulation studies of chronic obstructive respiratory dis-ease. XI. Impact of air pollution and smoking on annual
M.D. LEBOWITZ1052
change in forced expiratory volume in one second. AmJ Respir Crit Care Med 1994; 149: 1209–1217.
235. Abbey DE, Colome SD, Mills PK, Burchette R, BeesonWL, Tian Y. Chronic disease associated with long-termconcentrations of nitrogen dioxide. J Exp Anal EnvironEpidemiol 1993; 3(2): 181–202.
236. Abbey DE, Petersen FF, Mills PK, Kittle L. Chronicrespiratory disease associated with long-term ambientconcentrations of sulfates and other air pollutants. J ExpAnal Environ Epidemiol 1993; 3(51): 99–115.
237. Mostardi RA, Ely DL, Woebkenberg NR, Richardson B,Jarrett MT. The University of Akron study on air pol-lution and human health effects. I. Methodology, base-line data, and aerometrics. Arch Environ Health 1981;36: 243–249.
238. Mostardi RA, Woebkenberg NR, Ely DL, Conlon M,Atwood G. The University of Akron study on air pollu-tion and human health effects. II. Effects on acute res-piratory illness. Arch Environ Health 1981; 36: 250–255.
239. Neri LC, Mandel JS, Hewitt D, Jurkowski D. Chronicobstructive pulmonary disease in two cities of contrast-ing air quality. Can Med Assoc 1975; 113: 1043–1046.
240. Becklake MR, Aubry F, Soucie J, et al. Health effectsof air pollution in the greater Montreal region: a studyof selected communities. Final Report. Dept of Epidemio-logy and Health, McGill University, 1975.
241. Aubrey F, Gibbs WG, Becklake MR. Health effects ofair pollution in the greater Montreal region: a study ofselected communities. Arch Environ Health 1979; 34(5):360–368.
242. Infante-Rivard C. Childhood asthma and indoor environ-mental risk factors. Am J Epidemiol 1993; 137: 834–844.
243. Stern BR, Raizenne ME, Burnett RT, Jones L, KearneyJ, Franklin CA. Air pollution and childhood respiratoryhealth: exposure to sulphate and ozone in ten Canadianrural communities. Environ Res 1994; 66: 125–142.
244. Lambert PM, Reid DD. Smoking, air pollution, and bron-chitis in Britain. Lancet 1970; i: 853–857.
245. Lunn JE, Knowelden J, Handyside AJ. Patterns of res-piratory illness in Sheffield infant schoolchildren. Br JPrev Soc Med 1967; 21: 7–16.
246. Kerrebijn KF, Mourmans ARM, Brersteker K. Study ofthe relationship of air pollution to respiratory disease inschoolchildren. Environ Res 1975; 10: 14–28.
247. Fischer P, Remijn B, Brunekreef B, Van der Lende R,Schouten J, Quanjer P. Indoor air pollution and its effecton pulmonary function of adult nonsmoking women. II.Associations between nitrogen dioxide and pulmonaryfunction. Int J Epidemiol 1985; 14: 221–226.
248. Fischer P, Remjin B, Brunekreef B, et al. Associationsbetween indoor exposure to NO2 and tobacco smoke andpulmonary function in adult smoking and nonsmokingwomen. Environ Int 1986; 12: 11–15.
249. Remijn B, Fischer P, Brunekreef B, Lebret E, BoleijJSM, Noij D. Indoor air pollution and its effect on pul-monary function of adult nonsmoking women. I. Expo-sure estimates for nitrogen dioxide and passive smoking.Int J Epidemiol 1985; 14: 215–220.
250. Dijkstra L, Houthuijs D, Brunekreef B, Akkerman I,Boleij JS. Respiratory health effects of the indoor envi-ronment in a population of Dutch children. Am RevRespir Dis 1990; 142: 1172–1178.
251. Houthuijs D, Remijn B, Brunekreef B, De Koning R.Exposure to nitrogen dioxide and tobacco smoke andrespiratory health of children. In: Seifert B, Esdorn H,Fischer M, Rueden H, Wegner J, eds. Indoor Air 1987.Proceedings of the 4th international conference on indoor
air quality and climate. Vol. 1. Volatile organic com-pounds, combustion gases, particles and fibres, and micro-biological agents. August, Berlin, Federal Republic ofGermany. Institute for Water, Soil and Air Hygiene.1987; pp. 463–467.
253. Sawicki F. Chronic nonspecific respiratory disease inthe city of Cracow. XI. The cross-section study. EpidemiolRev 1969; 23: 242.
254. Sawicki F, Lawrence PS, eds. Chronic nonspecific respi-ratory disease in the city of Cracow: report of a 5 yearfollow-up study among adult inhabitants of the city ofCracow. National Institute of Hygiene, Warsaw, Poland,1977.
255. Rudnik J. Epidemiological study on long-term effectson health or air pollution. Probl Med Wieku Rozwojowego1978; 7a (Suppl.): 1–159.
256. PAARC Co-operative Group. Pollution atmospheriqueet affections respiratoires chroniques ou a repetition. II.Resultats et discussion. (Air pollution and chronic orrepeated respiratory diseases. II. Results and discus-sion). Clin Respir Physiol 1982; 18: 101–116.
257. PAARC Co-operative Group. Pollution atmospheriqueet affections respiratoires chroniques ou a repetition. I.Methodes et sujets. (Air pollution and chronic respira-tory disease. I. Methods and material). Clin RespirPhysiol 1982; 18: 87–99.
258. Ramaciotti DM, Bahy B, Voinier B, Rey P. The SO2pollution level and the incidence of bronchitis. MedSociale Prev 1977; 22: 189–190 (Tran.).
259. Braun-Fahrlander C, Ackermann-Liebrich U, WannerH-U, Rutishauser M, Gnehm HE, Minder CE. Auswir-kungen von Luftschadstoffen auf die Atemwege vonKleinkindern. (Effects of air pollutants on the respira-tory tract in young children). Schweiz Med Wschr 1989;119: 1424–1433.
260. Gschwend-Eigenmann S, D'Apuzzo V, Schoeni MH,Kraemer R. Einfluss der Luftschadstoffbelastung aufgesunde und lungenkranke Kinder im Suedtessin. (Effectsof air pollution on healthy children and children withrespiratory diseases in southern Ticino). Schweiz MedWshr 1989; 119: 1868–1874.
261. Schmitzberger R, Rhomberg K, Buchele H, et al. Effectsof air pollution on the respiratory tract of children. PedPulmonol 1993; 15: 68–74.
262. Kuehr J, Hendel-Kramer A, Karmaus W, et al. Luft-schadstoffbelastung und Asthma bronchiale bei Schulkin-dern. (Air pollution and asthma among school children).Soz Praeventivmed 1991; 36: 67–73.
263. Von Mutius E, Fritzsch C, Weiland SK, Roll G, MagnussenH. Prevalence of asthma and allergic disorders amongchildren in united Germany: a descriptive comparison.BMJ 1992; 305: 1395–1399.
264. Zapletal A, Jech J, Paul T, Samanek M. Pulmonary func-tion studies in children living in an air-polluted area. AmRev Respir Dis 1973; 107: 400–409.
265. Spinaci S, Arossa W, Bulgiani M, Natale P, Bucca C,de Candussio G. The effects of air pollution on the res-piratory health of children: a cross-sectional study. PediatrPulmonol 1985; 1: 262–266.
266. Arossa W, Spinaci S, Bugiani M, Natale P, Bucca C, deCandussio G. Changes in lung function of children afteran air pollution decrease. Arch Environ Health 1987; 42:170–174.
EPIDEMIOLOGICAL STUDIES OF AIR POLLUTION EFFECTS 1053
267. Petrilli FL, Agnese G, Kanitz S. Epidemiologic studiesof air pollution effects in Genoa, Italy. Arch EnvironHealth 1966; 12: 733–740.
268. Saric M, Fugas M, Hrustic O. Effects of urban air pol-lution on school-age children. Arch Environ Health1981; 36(3): 101–108.
269. Pershagen G, Hrubec Z, Lorich U, Ronnqvist P. Acuterespiratory symptoms in patients with chronic obstruc-tive pulmonary disease and in other subjects living neara coal-fired plant. Arch Environ Health 1984; 39: 27–33.
270. Goren AI, Hellmann S. Prevalence of respiratory symp-toms and diseases in schoolchildren living in a pollutedand in a low polluted area in Israel. Environ Res 1988;45: 28–37.
271. Tsunetoshi Y, Shimizu T, Takahashi H, et al. Epidemio-logical study of chronic bronchitis with special referenceto effect of air pollution. Int Arch Arbeitsmed 1971; 29:1–27.
272. Yoshida RK, Motomiya H, Saito ??, Funabashi S. Clinicaland epidemiological studies on childhood asthma in airpolluted areas in Japan. In: Clinical Implications of AirPollution Research. Acton, Massachusetts, PublishingSciences Group, Inc., 1976.
273. Suzuki T, Ishinishi N, Yoshida R, Tsunetoshi Y, HitosugiM. The relationship between air pollution and the res-piratory symptoms and functions of housewives. JapanPublic Health Society Foundation, Tokyo, Japan, 1978.
274. Yano E, Yokoyama Y, Higashi H, Nishi S, Maeda K,Koizumi A. Health effects of volcanic ash: a repeatstudy. Arch Environ Health 1990; 45: 367–373.
275. Nitta H, Sato T, Nakai S, Maeda K, Aoki S, Ono M.Respiratory health associated with exposure to automo-bile exhaust. I. Results of cross-sectional studies in 1979,1982 and 1983. Arch Environ Health 1993; 48(1): 53–58.
276. He Q-C, Lioy PJ, Wilson WE, Chapman RS. Effects ofair pollution on children's pulmonary function in urbanand suburban areas of Wuhan, People's Republic of China.Arch Environ Health 1993; 48(6): 382–391.
277. Xu X, Dockery DW, Wang L. Effects of air pollutionon adult pulmonary function. Arch Environ Health 1991;46(4): 198–206.
278. Tam AYC, Wong CM, Lam TH, Ong SG, Peters J,Hedley AJ. Bronchial responsiveness in children exposedto atmospheric pollution in Hong Kong. Chest 1994;106: 1056–1060.
279. Lebowitz MD. A critical examination of factorial eco-logy and social area analysis for epidemiological res-earch. J Ariz Acad Sci 1977; 12: 86–90.
280. Bobak M, Leon DA. Air pollution and infant mortalityin the Czech Republic, 1986–1988. Lancet 1992; 340:1010–1014.
281. Gorham E. Bronchitis and its acidity of urban precipi-tation. Lancet 1958; ii: 691.
282. Blindauer KM, Erickson L, McEllwee N, Sorenson G,Gren LH, Lyon JL. Age and smoking-adjusted lung can-cer incidence in a Utah county with a steel mill. ArchEnviron Health 1993; 48(3): 184–190.
283. French JG. Effects of suspended sulfates on humanhealth. Environ Health Persp 1975; 10: 35–37.
284. Krzyzanowski M, Camilli AE, Lebowitz MD. Relation-ships between pulmonary function and changes in chro-nic respiratory symptoms: comparison of Tucson andCracow longitudinal studies. Chest 1990; 98: 62–70.
285. Manfreda J, Nelson N, Cherniak RM. Prevalence of res-piratory abnormalities in a rural and an urban commu-nity. Am Rev Respir Dis 1978; 117: 215–226.
286. RIVM. Indoor environment. In: A national environ-
mental survey 1985–2010: concern for tomorrow. TheNetherlands, National Institute of Public Health andEnvironmental Protection. 1989; pp. 243–254.
287. Toyama T. Air pollution and its health effects in Japan.Arch Environ Health 1965; 8: 1153.
288. Viegi G, Paoletti P, Carrozzi L, Giuntini C, LebowitzMD. Prevalence rates of respiratory symptoms in Italiangeneral population samples exposed to different levelsof air pollution. Environ Health Persp 1991; 94: 95–99.
289. Leaderer BP, Berman MD, Stolwijk JAJ. In: KasugaS, et al., eds. Proceedings of the Fourth InternationalClean Air Congress. Tokyo, JUAPPA. 1977; pp. 1–4.
290. Henry RL, Bridgman HA, Wlodarczyk J, Abramson R,Adler JA, Hensley MJ. Asthma in the vicinity of powerstations: II. Outdoor air quality and symptoms. PedPulmonol 1991; 11: 134–140.
291. Zwick HW, Popp W, Wagner C, et al. Effects of ozoneon the respiratory health, allergic sensitization, and cel-lular immune system in children. Am Rev Respir Dis1991; 144: 1075–1079.
292. Robbins AS, Abbey DE, Lebowitz MD. Passive smok-ing and chronic respiratory disease symptoms in non-smoking adults. Int J Epidemiol 1995; 22: 809–817.
293. Turner-Warwick M. In: Immunology of the Lung. London,E Arnold. 1978.
294. Watanabe H. Air pollution and its health effects in Osaka.Presented at 58th Annual Meeting of Air Pollution ControlAssociation, Toronto, Canada, June 20–24, 1965.
295. Lebowitz MD, Sherrill D, Holberg C. Effects of pas-sive smoking on lung growth in children. Ped Pulmonol1992; 12(1): 37–42.
296. Forastiere F, Corbo GM, Pistelli R, et al. Bronchialresponsiveness in children living in areas with differentair pollution levels. Arch Environ Health 1994; 49:111–118.
297. Folinsbee LJ, Horvath SM, Raven PB, et al. Influenceof exercise and heat stress on pulmonary function dur-ing ozone exposure. J Appl Physiol: Respirat EnvironExercise Physiol 1977; 43: 409–413.
298. Gibbons SI, Adams WC. Combined effects of ozone ex-posure and ambient heat on exercising females. J ApplPhysiol: Respirat Environ Exercise Physiol 1984; 57:450–456.
299. Cassell E, Lebowitz MD. Causality in the environmentand health: the utility of the multiplex variable. PerspectBiol Med 1976; 19(3): 338–341.
300. Hill AB. The environment and disease: associationsand causation. Proc Roy Soc Med (Occup Med) 1965;58: 272.
301. Sanstrom T. Respiratory effects of air pollutants: ex-perimental studies in humans. Eur Respir J 1995; 8:976–995.
302. Chitano P, Hosselet JJ, Mapp CE, Fabbri LM. Effectsof oxidant air pollutants on the respiratory system: insightsfrom experimental animal research. Eur Respir J 1995;8: 1357–1371.
303. Koren H, Devlin RB, Graham DE, et al. Ozone-inducedinflammation in the lower airways of human subjects.Am Rev Respir Dis 1989; 139: 407–415.
305. WHO/EURO Acute Effects on Health of Smog Epi-sodes. (Euro Series No. 43). Copenhagen, 1992.
306. Soyseth V, Kongerud J, Haarr D, Strand O, Bolle R, BoeJ. Relation of exposure to airways irritants in infancyto prevalence of bronchial hyperresponsiveness in school-children. Lancet 1995; 345: 217–220.