'" 1 seRUM GLUTAMATE nEHYDROGENASE DETERMINAT_fON IN CHRONIC ALCOHOLICS by Richard Jan pivon " A th&sis submi tted ta the Facu1ty of Graduate Studies lt a né!." Research in partial fu1fillment of the requirernents for the degree of Master of Science Departrnent of Experimental Surgery McGi1l university Montreal, Canada August 1985. ® pivon 1985 . .,
Transcript
'"
1
seRUM GLUTAMATE nEHYDROGENASE DETERMINAT_fON
IN
CHRONIC ALCOHOLICS
by
Richard Jan pivon
"
A th&sis submi tted ta the Facu1ty of Graduate Studies lt
a né!." Research in partial fu1fillment of the
requirernents for the degree of
Master of Science
Departrnent of Experimental Surgery
McGi1l university
Montreal, Canada August 1985. ® pivon 1985 .
.,
CHAPTER l
CHA PT ER II
CHAP'PER III
CHAPTER IV
- l -
TABLE OF CONTENTS - ./,
PREFACE
INTRODUCTION
HEPATOTOXICITY
SERUM GLUTAMATE DEHYDROGENASE AS REFLECTING LlVER FUNCTION
METHODOLOGY
1
A - Methodology· pt! Serum GDH Determination 0 L
B Studies in Chronic Alcoholics l - Studies in :Norma l Sub jects 2 - Patient Population of Chronic Alcoholics
..
a) Studies a~ the Montreal General Hospital b) Studies on Patients admitted to Half-Way
Center 3 - Dipstick Methodology of Serum Alcohol
Determina tIon
CHAPTER V RESULTS ~
A - Serum GDH and Other Li ver Enz'yme Determinations in Control Subjects
B - ~erum GDH and Other Li ver Enzyme Determinations in Chronic Alcoholics
1 ...: Pilot Studies 2 - Studies of serum enzyme levels in Chronic
Alcoholics admi tted to l:he Half~Way Center a) Relationship between the different rang~s
of serum a>lcohol level and the serum GDa concentration ranges
b) Relationship between the different ranges of serum alcohol levels and the GGTP, Alk. Phos., SGOT and SGPT levels on admission
t)
CHAPTER VI DISCUSSION
A - Methodology of GDH Determina tion B -" Assays of GDH and other serum enzymes in
Chronic Alcoholics C - Perspectives of GDH assay in liver diseases
CHAPTER VII CONCLUSIONS
REFERENCES
PAGE 1
6
10
17
33
56
69
81
83
}
•
FIGURES
Fig.l
Fig.2
Fig.3
Fig.4
Fig.5
Fig.6
Fig.7
Fig.8
Fig.9
TABLES
Table l
- II -
LIST'· OF tLLUSTRATIONS
structural changes in serum GDH during transamination
The reversible reaction catalyzed by GDH
Glutamate Dehydrogenase Reactions with Different Transaminases
niagram illustrating the two ports of entry into the mitochondrial respiratory chain
The Dependence of the speed of GDH reaction on co-enzyme~ substrate and EDTA concentration, as weIl as pH level
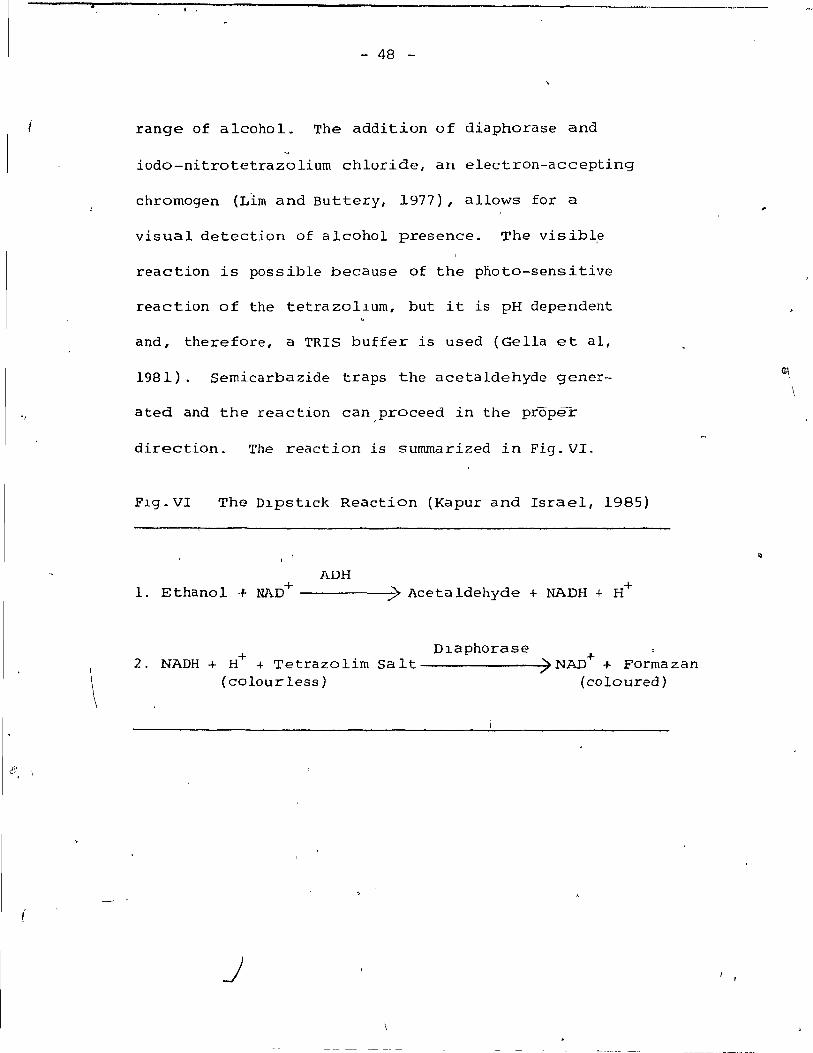
The Dipstick Reaction
Blood Alcohol Level vs Serum GDH
Blood Alcohol Level vs ç;GTP
Comparison' of GDH and GGTP
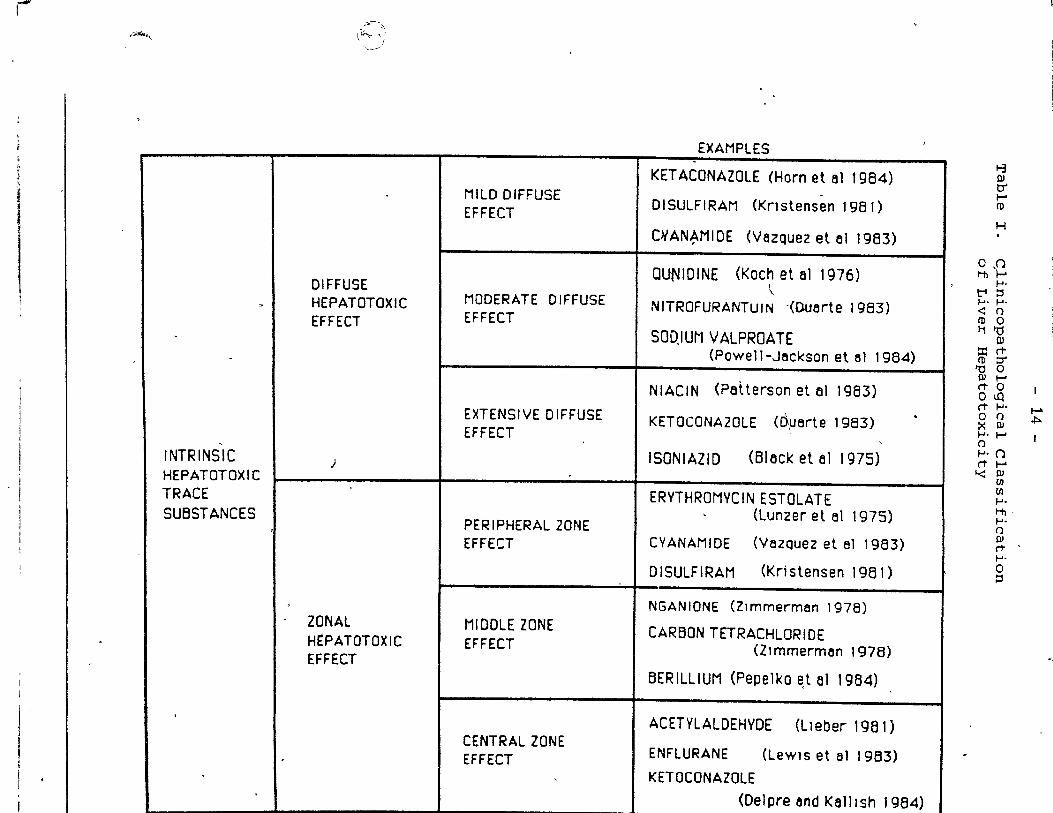
'Clinicopa thological Classification of Liver Hepatotoxicity
Table II GDH content in h\,lman tissue
Table III GDH content of tumour tissue in b hurnan sub jects
Table IV verification' of Dipstick Methodology using a PMO 2-Zeiss chromatogram Spectrophotorneter
PAGE
p.24
p.25
p·.28
p.31
p.34
p.48
p.62
p.64
p.65
.
p.14
p.20
B~21
p.51
Table V
Table VI
Table VII
- III -
\
Classification of Alcohol Dipst~ck Results - Scale for Low Serum Ethanol Content
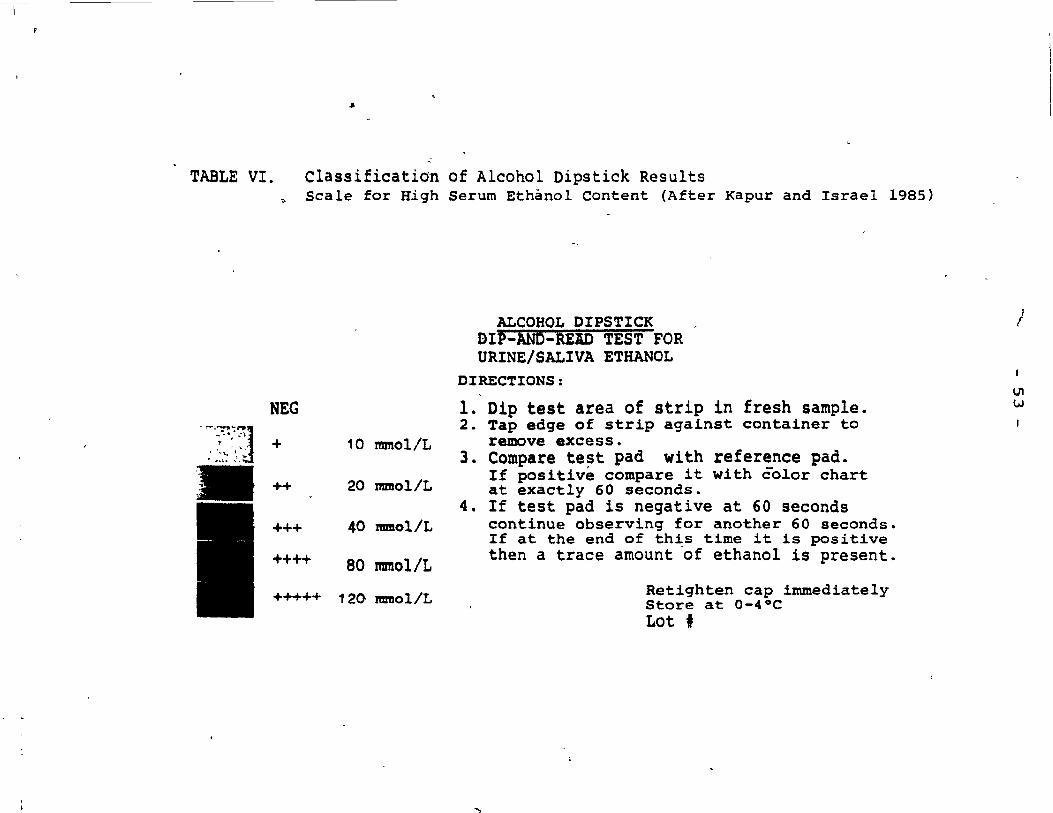
Classification of Alcohol Dipstick R~sults - S~ale for High Serum Ethanol Content
Compar~son of urine ethanol determination by Alcohol Dipstick Methodology with'U.V. methodology
Table VIII Comparative study of alcohol levels in serum using Dipstick Methodology and Gas Chromatography
Table IX
Table X
• Table XI
Table XII
1
Normal Values of serum enzyme levels as reflecting hepatic function
Serum GGTP and Alkaline Phosphatase in 12 Chronic Alcoholics
Relationship between serum GDH level and serum Alcohol level on admission (60 cases)
p.52
p.53
p.54
p.55
p.56
p.S8
p.59
p.63
Table XIII Nurnber of cases with NorJ;llal (N=) and p.68 significantly elevated (H=) enzymes in the four groups of serum ethanol conc'entrations on admission (60 cases)
Table XIV Serum GOH and other liver enzyme .. values in a patient with obst~uctive
jaundice l fOliowing choledocho-.' jejunostorny
p.79
o
, - 'IV
Résumé
DETERMINATION DE LA DESHYDROGENASE DU GLUTAMATE (GOlO SERIQUE CHEZ LES .,ALCOOLIQUES CHRONIQUES
Les facteurs sériques GDB, GGTP, Alk. Phos .. SGOT et SGPT furent ,
étudiés chez 72 patients souffrant d'alcoolisme. chronique. pAu cours de
projets pilotes impliquant 12 patients, une modification fut apportée à la
méthode de détermination de la GDH et les au tres enzymes furent analysés. Cette
méthode modifiée de détermination du facteur GDH (Koch et Pivon) s'est avérée
plus précise et plus simple que la méthode utiÙsée jusqu'alors. Chez
60 alcooliques chroniques admis dans un centre de réhabilitation, les niveaux
d'enzymes furent: déterminés aux 1er et 21 ième jours de leur s,éjour et mis 'en
corrélation avec les diffé~ents niveaux d'éthanol sérique. Ceci fut f!tabli
d'après le procédé de jaugeage (Kapur et Israel - 1985). Lors de crises
intenses d'alcoolisme, la.hausse du taux de la GDH sérique était directement
rekiée au niveau d'éthanoi dans le sang (Sensibilité:. 81.25%; Sp~cificité: 90.91%;
Valeur de prédiction positive: 76.47%; Valeur de prédiction négative: 93.02%).
Au 2lième jour, tous les taux de la GDH se situaient dans les limites normales. /
Même au-delà de 48 heures après le retour à la normale des taux de la GDH, le
facteur GGTP s~ révéla un bon indicateur de la condition hépat:i.~ue. Cette
méthode modifiée .... de détermination de la GDH sérique chez les alcooliques
chroniques semble apporter un nouveau paramètre pour - évaluer l'état de ceux
qui, lors d'épisodes aigus d r alcoolisme t présentent des lésions aux
mitochondries des cellules du foie et possiblement pour dépister d'autres
maladies hépatiques.
"
. . IV ..:.
Abstract ,
SERUM GLUTAMATE DEIIYDROGENASE DETERMINATION IN CHRONIC ALCOHOLICS
Serum GDH, GGTP, Alk. Phos., SGOT and SGPT were s tudied
alcohol~c patients. In pl lot studies on 12 in 72 chr~c
patients, the modification of GDII determination was devel-
oped, and the other enzynles tested. The modiflcation of ~
GDH determinatlon (Koch and Pivon) was found to be more
accurate and simple than previous methodology. In 60
chronic aicoholics admi tted te a half-way center 1 the , )
enzyme levels were determined at days land 21 and correla'ted
to serum ethanoi levels, determined by dipstick methodology
(Kapur and Israel 1985). During acute alcoholic episodes 1
serum GDH elevation was directly roelated to ethanol b100d
NewshQ1rne and Leech (1983), the reaction is ca11ed '-
transdeanimation~ according to Krebs (Krebs et .al, 1973),
the reaction 1 s direction is determined by the concentra-
tion of substrates involved. These reactions are appar-
ently the reason for sorne of the accumulation of high
energy bonds formed during mitochondrial oxidation of
glutamate .. According to McGilvery (1983), as rnany as
12 (ADP + p) are changed to 12 ATP. The Krebs Cycle is
considered by Armstrong (1983) t"o be amphibo1ic, since
the O:::-ketog1utarate is used not only as a port of entry
int~ the Kreb; Cycle, but also OC-keto'g).utarate, by, the
reverse reaction of GDH, can be used in L-g1ut'amélte
synthesis. The significance of the Krebs Cycle in dis-
posing of arnrnonia is evident in patients with a1coholic
cirrhosis, where arnmonia accumulation g~rs and tremors
Q
may deve10p (Smith and Thier, 1981). It has been sugges-
ted by Smith and Thier (1981) that the arnrnonia is a'ccum-
ulated as a resu1t of glutamate dehyd~ogenase catalysing
, ,
the reverse reaction by which depletion of OC-ketoglutarate
occurs and interferes with the Krebs Cycle in carrying out
itlS function, disposaI of ammonia or urea synt,hesis. It
is obvious that the reactions of transaminases (SGOT, SGPT)
- 30 -
, "
and glutamate dehydrogenase must be in close equili-, , 1
~ \ 1
br1u~. However, as Newsholme and Leech (1983) point
out, certain conditions must be met: oxacids, such as
ketoglutarate, oxaloace'tate, pyruvate, must 'be avail-
able; the process must be reversible i and the amino
acids, such as glutamate, asparate and alanine" must
not only be degraded b~t a1so synthesized.
WeIl ba1anced rneals' provide conditions for trans-
deamination, but as stated by Newsho1rne and Leech (1983),
certain criteria have ta be present: the ainrnonia and
oxacids musLundergo further metaboll.sm; ?nd the NAD(P)H
must be oxidized to NAD(P) by passing through the 'eIectron
transport chain, where it is first cata1yzed by NADH dehy-G
drogenase, according to SmitJ:;l. and Thier (1981), where l ,
ATP is produced and two more ATP are generated along the"
, chain giving a total of 3 A.TP generated for 1 NAD(P)H
oxidized (Fig.4).
One possibi1ity that should' be considered in GDH
s~ructure i~ that two biochemical1y different forms of
G~utamate dehydrogenase may exist in human subjects: ~
one form consisting of NADP-GDH, used fox: synthesis of
glutamate and a second forro consisting of NAD-GDIt which \"J 'j,
Q
- - -- - -
".
.,.,
.1
1 ,
l , ~ 1
,,', .'
0"
~,
't
Fig.4 Diagra~ i~lustratin~~he two ports Df entry into the mitochondria1 respiratory chain.' Port l shows entry of'NADH; Port II shows site,
, "-
of entry of FADH2. The pathway from Port l pro~s 3 'ATP a10ng the respiratory chain, whi1e the pathway from Port II produces only 2 ATP through the tèspiratory chain. (Diagram modified from pub1~cations of wnite et al (1973), Harper (1973), smith and Thier (1981) .
'\.?
~ li'
----
l' port 1 port 1I
"FADH FAD
(Fe-S) 0: >-< (Fe-S)Re
l
1 " 1
NAD(P)H2
NAO(P)
FMN X[Fe-Sl ' , Re
FMNH2 [Fe;Slox
ADP+Pl AlE.
Q
~
. ....
Q X Cyl b[Fe2+]X Cytc 13+
Q'~ Cyt bIFe 3+] '; CYt~-12+_,
ADP+Pl .AI.!:
/ ~
. ,
"
Î
Cylc 2+xcyt t)3+ X' Cyt 113 [Fe2+]
Cyt c 3+ Cyt a2+ Cyt <:I3[Fe2+]
ADP+P'l ATP
"
'-
,0
~
~
1/2 °2
H20
W 1-"
(
- 32
is used in the o-xidative deamination of glutamate
resulting in OC -ketogll.:ltarate formation: This presump-
tion is s trengthened by the finding 6f Henunings (1984),
who found that " yeas t has the capacity to synthesize
two genetically distinct glutamate dehydrogenases". /
if '.
-
IP
•
•
\
o
-------------------- -
< ,
, . . 1 "1 .~
} 1 1
----.,.=-,
(
{)
CHAPTER IV
- 33 -}
t ,
MET HO DO LOGY
A. Methodology of Glutamate Dehydrogenas~ Determinations.
The methodology of serum GDH determinations was
developed during the last 20 years. The original
methodology has been modified several times and the
results correlated with morphological findings,
obtained from 11ver biopsy materia1. Schmidt and
Schmidt (1962) used a reaction mixture of DPNH2 ,
TRAD (triethano1amine), EDTA and Ammonium Acetate
with serum and found the Sérum GDH conc~ntrations
tp be 100% (±S) on the first day and gradual1y decl-
ining to 70% (±21) within 12 àays. , when GDH was
injected intrave~ously in dogs, the activity remained
high in the first 2 ·~ours (over 80%) and then declined
./'
to .20% over a period of 54 hoursi a marked, drop. trom
60% occurred at Il hours. Schmidt and scpmidt (1962)
studied 127 normal individuals and found the GDH
activity to be below 1 mU/ml.. They have shown the
dependence of GDH activity on coenzymes, substrate, pH
and EDTA concentration (Flg.5). Ellis and Goldberg
(1~72) assayed GDH activity and established the u1ti-
l ,', mat'e conditions of reaction mlxtures 1 activators and
~
Fig.5 The Dependence of the speed of GDH reaction on co-enzyme substrate and EDTA concentration as weIl as pH lev~. (After Schmidt and Schmidt 1962)
"""'" .... ",., ~ .... " .. ,. lIo"sl,nl' ~ .. ,,,.,, 1'"""'"' ",'O"JH IG '.h"i' H DPNH ,."ftl' H OPNH t,6.,fi"~ DP,* ~(j.I(J' ,.., OPNII 1,0.1#1'114 lIHi. ',0 ,'~, H NH, UddJ H KGS 6,6.,::J1M Y.GS 6,6.'0"1 • .., J(G~ U.,(/J/lfEDrA 1.",(/J /If lDrA 1, •• ,61 H EDlA ',o,rü'H NH/ ,.o.,~, H Nil,· pH U pH U pH 1.5 pH 7,5 2,fuf(JJ,., EDlA l'-
li
2. w
\ .j:>.
Dt 1 \ 1 1 1 \ Il \ 1 lA Q
10
" " ,. Il
1" i , ,
~ , NH~·I l' :1 DPNHI ..
pH ... ·KGS _ EOrA . .. 1 , 1 " , • 10 J " G , ID Il ." tG l " Goa 7.l 7.6 4,0 1.' .1tJC1I _ .,d Il .• ld2 H .,O~
- 35 -
reagents. ~hey,found that ADP was the best activator
and that the pH should be optimally at 7.4 and the ,
temperature at 37 oC. Oxoglutarate was used in these
studies as the initlatùr of the reaction. In previous
studies, serum liver transaminase levels did not
o •
correlate with histological findings obtained in the --course of liver biopsies (Rallai et al, 1964). It was
VanWaes and Lieber (1977) who first carried out GDH
measurements and correlated them with liver biopsy
materia1 obtained from chronic alcoholics. Worner
and Lieber (1980a) carried out a study to determine the
clinicai ap~lication of GDH determinations and use as
a marker in assessing liver damage produced by aicohoi
abuse (Worner and Lieber, 1980b). This study was
carried out on aicoholics who were admitted for detox-
lfication or treatment of complicatlons arising from
severe alcohol abuse. GDH was chosen as an indicator
of aicohoi toxicity to liver mitochondria. A very
high concentration of GOH was observed in liver tissue
extracts of these patients. It was found that not only
does ethanol exert its main effect on the central zone
of the hepatic lobule, but aiso that GDH appears to
- 36 -
play a major role in the derangement of mitochondrial
metabo1ism in chronic alcoholics. The half-1ife of,
GDH is short, therefore,measurements of GDH were
carried out on blood samples obtained within 24 hours
of the intoxication episode. Since cellular lesions
persist longer than serum GDH e1evations, the biopsies
were still positive at day 10 after admission. Other r"
tests carried out by Worner and ~ieber {198üa,b}
included PT, SGOT, SGPT, GGTP and bilirubin. No sig-
nificant or consist~nt relationship wa~ found between
these parameters and liver b~opsies, because of the
large overlaps and perhaps due to differences. in time, when
serum samples were tak~n.
The liver biopsies were carried out using double
blind methodology (VanWaes and Lieber, 1977; Worner and \
Lieber, 1980a,b). The morphological changes observed
included Ma110ry bodies, fibrosis and necrosis, as
weIl as steatosis and inflammatory changes. VanWaes
and Lieber {1977} graded the degree of necrosis as
folrows: O-absence of necrosis an parenchymal inflam-
Dlaphorase 2 + l' 1 ~ + " NADH + H + Tetrazo lm Sa t -------~7 NAD + Forma zan
(colourless) (coloured)
J
,.
~,
\
- 49 -
The enzyme stabi lizer is a~bumin from bovine serum,
with either dithiothreitol or dithloerythritol. A
predetermined amount of buffered enzyrne-cofactor-
inhibitor is used to impregnate strips of filter
\ . paper, WhlCh are 111:0philised and attached to a plastic
strip at one end. This allowed for determining alcohol
ln the range of 5-160 mg/dl (1-35 mmol/L and 20-120 mmol/L)
/ by comparing to a scaled chart tne color change observed
(from light pink to dark red) on the strlp tested.
f' The dipsticks were first checked on a PMQ 2-Zeiss Chroma-
togram-Spectrophotometer at 530nm, wi th light absorption
relating weIl to the square root of a1cohol ~evel
(Table IV). It tnrned out that the naked eye cou Id al so
discriminate colour changes for the specific ranges
considered, using a six-point colour chart (Tables V and VI).
Patients from various centers were tested. Dipstick ~nalysis
was carrled out on 931 urine samples and 631 serum samples.
For urine, alcohol 1evel ver ifica tIan (Table VII) was
carrled out uSlng a U.V. spectrophotometer and the correlatIon
coeffIcient was fa und to be 0.90 for ranges 0-160 mg/dl and
2-160 mg/dl. The serum alcohol levels were verified by gas
chromatography (Table VIII) with a correlatIon coefficient 7
- 50 -
of 0.90 for the ranges of 0-140 mg/dl and 3-140 mg/dl.
Saliva specimens were also studied on 51 subjects
and the correlation coefficient was greater than 0.90.
The sensitivity was found to be 98.8%, specificity ,
was 97.5% and efficiency 98%. The a1cohol dipstick
can also be converted into a quantltative method by
using reflectance spectrophotometry to measure the
co1our lntenslty. The false positlves were found to
be below 2.2 mM (10 mg/dl). The dipstlck at -15 0 C
is stable for 12 months ~ at 4°C for 7 months and at
room temperature for up to 31 days.
In our studies, the dipstick methodology was, used
to correlate o ethano1 leve1s i~ body f1ulds with serum
1iver enzyme concentrations, both of WhlCh were deter-
mined on the same individual serum sample of each patient.
This permitted correlation of serum liver enzyme leve1s
with actual concentration of alcohol in serum in the
same sample.
- 51 -
TABLE IV. Verification of Dipstick Methodology
150
125
Peak 100 Height (mm) 75
50
25
,
as checked for reflectance densitornetry on a PMQ 2-zeiss Chrornatograrn Spectrophotometer at 530 nm. The square root of the ethano1 level was cornpared to peak heights of deflection for urine, serum and saliva (after Kapur and Israel 1985)
URINE SERUM SALIVA
r = 0.99 r = 0.95 r = 0.99
• 1
.i 1
20 30 40· 10 20 30 40 10 20 30 40
\/ Ethanol Concentration (mg/I) 1
II}
TABLE v.
NEG
~~<'J + _. ,"-- ... ;,,':.,"'~
++
+++
++++ .
~
~
Classification of Alcohol Dipstick Results Sca1e for Low Serum Ethanol Content (After Kapur and Israel 1985)
3 mmo+/L
6 mm61/L
13 mmo1/L
21 mmo1/L
ALCOHOL DIPSTICK OIP-ANb-REiD TEST FOR URINE/SALIVA ETHANOL
DIRECTIONS: 1. 2.
J.
4.
Dip test area of strip in fresh sample. Tap edge of strip against container to remove excess. Compare test pad with reference pad. If positive compare it with ëo1or chart at exactly 60 seconds. If test pad is neqative at 60 seconds continue observinq for another 60 seconds. If at the end of this time it is positive then a trace amount of ethanol ls present.
+++++ 30 mmol/L .. ... Reference Pad 'It+ Test Pad
Retighten cap immediate1y Store at 0-4°C Lot f
jO.
/
'\ llbJ
V1
'"
..
TABLE VI. Classification of Alcohol Dipstick Results
-~'''''''~1'1 ~~~",'" .:'-y •
• ' .. \." ~ fl
\-.;.f • _lo, ~''''''
1
'" Scale for High Serum Ethànol Content (After Kapur and Israel 1985)
NEG
+ 10 mmol/L
++ 20 mmol/L
+-1-+ 40 mmol/L
++++ 80 mmol/L
+++++ 120 mmol/L
ALCOHOL OIPSTICK DIP-AND-REiD TEST FOR URINE/SALIVA ETHANOL
DIRECTIONS:
1. Dip test area of strip in fresh sample. 2. Tap edge of strip against container to
remove excess. 3. Compare test pad with reference pad •
If positive compare it with ëolor chart at exactly 60 seconds.
4. If test pad ls negative at 60 seconds continue observing for another 60 seconds. If at the end of this time 1t 1s positive then a trace amount 'of ethanol ls present.
">
Retighten cap immediately Store at 0-4°C Lot t
)
V1 W
------------------------
- 54 -
T~LE VII. comparison of urine ethanol determination by Alcohol Dipstick Methodology with that obtained by u.v. Methodology using standards with pre-determined optimal ranges (after
TABLE VIII. Comparative study of alcohol levels using Dipstick Methodology and Gas Chromatography carried out on serum standards with pre-determined optimal ranges (after Kapur and Israel 1985)
(over 100 U/L) in 5 cases, when serum ethanol level
was over 20 mmol/L; ~here were 13 cases of elevated
GDH in the same category of ethanol level. This
finding suggests, if confirmed in a larger number of
cases, that the rise in GGTP following an acute alcoholic
episode is much slower than that of GDH.
Alkaline phosphatase does not seem to be a good
1ndicator of hepatic irijury by alcohol. When the Alk.
Phos. level of 150 U/L or more is considered abnormal,
it was found to be elevated in only 2 cases of serum
ethanol level of 20-30 mmol/L, and in l case of ethanol (\ !lI)
levei over 30 mmol/L. Perhaps in this higher range of
simuitaneous GGTP and AIk.Phos. elevation, the GGTP/Alk.
Phos. ratio may be usefui as far as judging the severity
of the in jury.
The SGOT was considered elevated when the serum ,
value was higher than 75 U/L; in this category, there 1 . were 8 cases; in aIl of these, other enzymes were aiso
significantly higher to various degrees. SGPT was
elevated on adrn1ssion (over 80 U/L) in only patient
out of 60 cases studied; in this instance, aIl other
enzymes were aiso elevated.
- 67 -
The number of cases in Low and high level groups
of GDB, GGTP, Alk.Phos., SGOT .and SGPT, in the four
groups of serum ethanol concentrations as determined
by the method of Kapur and Israel (1985), are,listed in
Table XIII.
- 68 -
Table XIII. Number of cases with Normal (N) and signlficantly elevated (H) enzymes ln the four groups of serum ethanol concentrations on adrnlsslon (60 cases).
t t---------------------------~--------~--------------------------1 o •
, 0 o
GROUP 1 :
GDH
N = 31 H = 1
GROUP II :
GDH
N = 9 H = 3
SERUM ALCOHOL RANGE = 0 - < 5
GGTP AP SGOT -- ...... --- ..... ----- ------N = 23 N = 31 N = 32 H = 9 H = 1 H = 0
Aldrldge W.N., Barnes J.M. and Denz F.A. 1949. Experimental berl11ium polsoning. Brlt. J. Exp. Patho 1. 30 , 376- 389.
Al1ard C., de Lamirande G. and cantero A.' 1957. Behavlour of enzymes in 11ver of starved rats. Exp. Cell Res. 13: 69-77.
Armstrong F.B. 1983. Biochemistry, ~ ed., Oxford University Press, 134-313.
Beaufay H., Bendall D.S., Baudhuin P. and de Duve C. 1959. Intracellular dlstributlon of some dehydrogenases, Alkaline Deoxyrlbonuclease and rat-1iver tissue. l - Tlssue Fractionation Studies. Biochem. J. 73: 623-628.
Black M., Mitchell J .R., Zimmerman H.J., Ishak K.G. and EpIer G.R. 1975. lsoniazid-associated hepatitis in 114 patients. Gastroenterology 69: 289-302.
Christie G.S., Judah J.D. 1953. Intrace11ular distribution of enzymes. Proc. Roy. Soc. B141: 420-433.
De Duve C., Pressman B.C., Glanetto R., wattiaux R. and Appe1mans F. 1955. Tissue Fractionation Studies. Intracel1u1ar distributio~ patterns of enzymes in rat 1iver tissue. Biochem. J. 60: 604-617.
Delpre, G. and Kallish U. 1984. Ketoconazo1e and the 1iver: further considerations. Gastroenterology 87s 985-986.
Diaz-Rivera R.S., Ca11azo J.P., Pons E.R. and Torregrossa M.V. 1950. Acute phosphorus poisoning in man: a study of 56 cases. Medicine 29: 269-298.
8 Duarte P.A., Chow C.C., Fimmons F. and Ruskin J. 1983. Fatal hepatitis associated with ketaconazo1e therapy. Arch. Inter. Med. 144: 1069-1070.
Ellis G., Goldberg D.M. 1972. Optimal Conditions for the Kinetic Assay of Serum Glutamate Dehydrogenase Acti: Ilty at 37°C. Clin. Chem. 18: 523-527.
•
- 84 -
Fersht A. 1985. Enzyme structure and Mechan~sm. 2 ed. W.H. Freeman and Company, New York, 136-616.
French S.W. and Burblge E.J. 1979. Alcohol~c hepatitis: Cl~nical, morpholog~ca1, pathogen~c and therapeut~c agents. pp. 557-559. In: progress in liver disease, PopperH. and SchaffnerF., Eds., Vo1.6, Grune and Stratton, New York.
Gella F.J., Oilvella M.T., Pegueroles F. and Gener J. 198L CO lorimetry 0 f Diaphorase in Commercia l Preparations and Clinical Chemical Reagents by Use of Tetrazo1ium Salts. Clin. Chem. 27: 1686-1689.
Geokas M.C. 1981. Ethanol, the l~ver and the gastrointestinal tract. Ann. Intern. Med. 95: 193-203.
Harper H.A. 1973. ReVlew of Physiological Chemistry. Lange Mèdical Pub1icat~on, Los Altos, california, 171-179.
Hemmings B.A. 1984. The role of protein phosphory1ation in the regula tion of the NAD-dependent glutamate dehydrogenase from yeast, pp. 155-165. In: Enzyme, regulation by reversible phosphorylation - further advances. Cohen P., Ed., Elsevier SClence Publishers, B.V.3.
Henry R.J., Cannon D.C. and Winkelman J.W. 1974. Clinical Chemistry, 2nd Ed., New York, Harper and 'Row, 1043.
Hogeboom G.H. and Schneider W.c. 1953. Intracellular Distribution of Enzymes, XI Glutamic dehydrogenase, J. Biol. chem. 204: 233-238.
Hogebo9m G.H., Schneider W.C. and Paliade G.E. 1948. Cytochemical studies of mammolian tissues, 1: Isolation of intact mitochondria from rat liver. Sorne Biochemical
------ properties of mitochondria1 and submicrosoma1 particulate material. J. Biol. Chem. 172: 619-635.
Hogeboom G.H., Schneider W.C. and Striebich M.J. 1~52. Cytochemical studies, V: On the isolation and biochemica1 properties of 1iver cell nuclei. J .Biol. Chem. 196: 111-120.
'- / , r
....
- 85 -
Horn J.L., sklnner H.A., Wanberg K. and Foster F.M. 1984. Alcohol use questlonnalre (Alcohol Dependence Scale). Add. Res. Found., Toronto, Ont., 1-4.
Israel Y. 1981. Early Identiflcatlon of Alcohol Abuse: Deflnitlonal Issue's and Dlagnostlc Dllemmas. Introduc tory Rernarks, In: Internatlonal Alcohol Research Seminar, Washlngton, D.C.
Kallai K.,'Hahn A., Roder V. and Zupanlc V. 1964. Correlation between hlstolog1C flndings and serum transarnlnase values in chronlC dlseases of the liver. Acta Med. Scand. 175: 49-56.
Kapur B.M. and Israel Y. 1985 (In Press). Alcoho1 DipstlCk -A Rapid Method for analysls of Ethan~l in Body Fluids .
. Res. Monograph No 17 ~ U.S. Dept. of Health and Human Services.
Kay H.D. 1930. l - Methodology of determination: Sorne properties of the enzyme. J. Bio 1. Chem. 89: 235-247.
Klatskin, G. 1974. Drug-induced hepatlc inJury. pp.163-175. In: The 11ver and its diseases, Schaffer F. and Sherlock S., Eds., Int. Med. Books, New York.
Koch P. and pivon R.J. 1985 (In Press). Modified method for Glutamate Dehy~rogenase determination.
Koch M.J., Seeff L.B., Crumley C.E., Rubin L. and Burns W.A. 1976. Quinidine hepatotoxicity. Gastroenterology 70: 1136-1140.
Krebs H.A., Hems R. and Lund P. 1973. Accumulation of, amino acids by the perfused rat liver in the presence of ethano1. Biocl}em. J. 134: 697 - 705.
Lewis J.H., Zimmerman H.J., Ishak K.C. and Mullick F.G. 1983. IEnf l-urene hepa totoxici ty. Ann. Intern. Med. 98, 984-992.
Lieber C. S. 1981. Pa thogenesis of alcoholic" 1iver in jury . pp. 199-203. In: Ethanol, the liver and the gastrointestinal tract, Geokas M.C., Ed., Ann. Intern. Med. 95.
~~- -~~~ ~ - -- ----
- 86 -
Lieber, C.S. and Leo M.A. 1982. Liver inJury by ethanol. pp. 259-312. In: Ma Jor prob1ems in interna 1 medicine, Lleher c.S. and Leo M.A., Eds.
Lim H.H. and Buttery J.E. 1977. DetermlnatJOn of ethanol 'ln serum by enzymatlc PMS-I.NT Colorlmetrlc Method, C1ln. Chem. Acta, 75: 9-12.
Lunzer M.R., Huang S.N., Ward I<'H. and Sherlock S. 1975. Jaundlce due to erythromycln estolate. Gastroenterology 68: 1284-1291.
McGllvery R.A. 1983. Bl0chemistry: A Functlona1 Approach. Saunders W .B., Philadelphia, 576-643.
Meyer R.E., Glueck B.C., O'Brien J.E., Babor T.F., Jaffe J.H. and Stabenan P., Eds., 1981. Evaluation of the alcoholic: lmp1ications for research, 'theory and treatment. Proc. Farmington Conf. U.S.H.H.S., Res. Mono 5: 409.
Newsholme E .A. and Leech A. R. 1983. Blochemïstry for the Medical Sc lences. John Wiley & Sons, Toronto, 398-629.
Patterson D.J., Dew E.W., Gyorkey F. and Graham D.Y. 1983. Nlacin hepatitis. South. Med. J. 76, 239-241.
Pepelko W., Dourson M.L. and stara J.F. 1984. Ambient water qua1lty criteria for beri1llum and health assessment. E_PA 440-5-80-024 and 600-8-84-026A, Env. Prot. Agency Pub1., washington, D.C.
Plvon R. J. and Skoryna S.C. 1985. Clinicopatho1ogic classification of hepa. totoxic effects of trace substances. Trace Elem. Med. In Press.
Powell-Jackson P .R., Tredger J .M. and williams R. 1984. Hepatotoxicity to sodium và1proate: a review. GUT 6, 673-681.
Powers S. G. and Melster A. 1982. Urea 1 Synthesis and Ammor-iia Metabolism. pp.251-263. In: The Liver: Blology and Pathobio1ogy. Arias I., Popper H. 1 Schacter D. and Shafritz D.A., Eds., Raven Press, New york.
\ /
l' ,
1
- 87 -
purich D.L. 1983. Contemporary Enzyme Kinetics and Mechanism. Acad. Press, New York, 71.
Rappaport A.M., Borowy Z.J. and Lotto W.N. 1954.
( ,
Subdlvision of hexagonal liV'er lobules into s"t;ructural and functional unit: role of hepatic physiology and pathology. Anat. Rec. 119, 11-33.
Rawn J.D. 1983. Blochemistry. New York, Harper and Row. 822-826.
Reynier M. 1969. Pyrazole Inhibitlon and Kinetic Studies of Ethanol and Retinol Oxidation Catalyzed by Rat Liver Alcohol Dehydrogenase. Acta Chem. Scand. 23: 1119-1129.
Schellenberg F., Weill J. ,and Lamy J.N. 1983. Place de la glutamate déshydrogénase dans le déplstage biologique des beuveurs excessifs. Ann. Biol. Clin. 41: 255T"~'62.
Schmidt E. and Schmidt F.W. 1962. Methode und Wert de' Bestirnmung der Glutaminsaure - Dehydrogenase -Aktivitat in Serum ein Beitrag zur Bedentung Untersüchung von Enzym-Re latlonen in Serum. Klin. Wochenschr., 40: o ••
962-969.
Schpeider W.C. and ~og oom G.E. 1950. Intracel1ular Distribution of Enzyme , V: Further study onrthe Distribution of Cytochrome in rat liver homogenates. J.Biol.Chem. 183: 123-128. -
Sherlock S. 1982. Alcohol related liver disease: Clinica'l , aspects and management. Brit.Med. Bul1.38: 67-70.
Smith L.E. Jr. and Thier s.o. 1981. pathophysiology: The Biological Principles of niseases, Saunders W.B., Philidalphla, 496-1721.
Sund H. and Theorell H. 1963. Alcohol Dehydrogenases, pp. 25-86. In: The Enzymes, Boyer P.D., Lardy H.A. and Myrback K., Eds., New! York, Acad. Press 7.
1
1
,- 88,-
vanwaes L. and Lieber C.S. 197'n. Glutamate Dehydrogenase.: A reliable marker of liver cell necrosis in the aleoh<?lie. ar.M~d.J. 2: 1508-1510'.
vazquez J _ J. 1 Diaz de otazu R., Guillen F.J., zozaya J. and Pardo F.J. 1~83. Hepatitis induced by drugs u~ed as alcohol aversion therapy. Diagn. Histopathol. 6: 29-J,? •
P. and smith E.L. 1973. (5th ed) 1 McGraw Hill/A. Montreal, 357.
pr inciples of Blakiston
witzleben C .L. 1972. Physiologie and morph61ogie natural history of a model of intrahepatic cholestasis_ Arn. J. Path. 66: 577-588.
Worner T.M. and Lieber C.S. 1980a. Plasma Glutamate Dehydrogenase: Clinical Application in Patients with Alcoholic Liver Disease. Alcoholism:' Clinical and Experimenta 1 Research 4: 431-434.
Worner T .M. and Lieber C.A. 1980b. Plasma Glutamate Dehy .. drogenase: A Marker of Alcoholic Liver Injury. Phar-
,/ macology Biochemistry and Behaviour 13 (1) : 107-110.
Worner T .M. 1983. Blood Tests in Alcoho1ic Li ver Diseases. Hematological Correlates of Alcoholism. In: International.
~ Alcohol Research Seminar, Washington, D.C.
Zimmerrnan H.J. 1978. Hepatotoxicity. Appleton - Century -Crofts, New York, 144. \
\
Zimmerrnan H.J~ 1983. Hepatotoxic evaluatio~ methodology, pp. 159-194 . In: Diagnostic procedures 'in the evaluation of hepatotoxic diseases. Laboratory and Researc;h Methods in Biology and Medicine. zimmerman 'H.J., Ed., Alan R. Liss, New York.