73
STD Review STD Review
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | nick-gowen |
| View: | 76 times |
| Download: | 3 times |

STD ReviewSTD Review
For which sexually transmitted pathogen has For which sexually transmitted pathogen has screening screening of non-pregnant women been shown to of non-pregnant women been shown to reduce the rate of a particular complication?reduce the rate of a particular complication?a.a. HSV 2HSV 2
b.b. Trichomonas vaginalisTrichomonas vaginalis
c.c. Hemophilus ducreyiHemophilus ducreyi
d.d. Chlamydia trachomatisChlamydia trachomatis
e.e. HSV 1HSV 1
Chlamydia trachomatisChlamydia trachomatis
Annual screening for all sexually-active women less than Annual screening for all sexually-active women less than or equal to 25 years of age and older women with new/>1 or equal to 25 years of age and older women with new/>1 sexual partnersexual partner
Treatment of asymptomatic, infected women reduces the Treatment of asymptomatic, infected women reduces the incidence of pelvic inflammatory diseaseincidence of pelvic inflammatory disease
Scholes D, Stergachis A, Heidrich FE, et al. Prevention of pelvic inflammatory disease by screening for cervical chlamydial infection. N Engl J Med 1996;334:1362–6.
Infection with Infection with Chlamydia trachomatis Chlamydia trachomatis is associated is associated with which of the following:with which of the following:a.a. Tubal factor infertilityTubal factor infertility
b.b. Ectopic pregnancyEctopic pregnancy
c.c. Non-gonococcal urethritis (NGU)Non-gonococcal urethritis (NGU)
d.d. Ophthalmia neonatorumOphthalmia neonatorum
e.e. Infant pneumoniaInfant pneumonia
f.f. All of the above All of the above
Chlamydia trachomatisChlamydia trachomatis
8 I n f e r t i l e 7 c h r o n i c p e l v i c p a i n 5 t u b a l p r e g n a n c y
4 0 P e l v i c I n f l a m m a t o r y D i s e a s e
1 0 0 U n t r e a t e d F e m a l e s w i t h C h l a m y d i a
How is Chlamydia infection diagnosed and How is Chlamydia infection diagnosed and treated?treated?
How is Chlamydia infection diagnosed and How is Chlamydia infection diagnosed and treated?treated? Nucleic acid amplification test done on urine Nucleic acid amplification test done on urine
(women and men) or,(women and men) or, Swab from endocervix, vagina or urethra (men)Swab from endocervix, vagina or urethra (men)
Azithromycin 1 g po onceAzithromycin 1 g po once Alternatives: one week of doxy, erythromycin or Alternatives: one week of doxy, erythromycin or
levofloxacinlevofloxacin
All of the following are an established cause of All of the following are an established cause of non-gonococcal, non-chlamydial urethritis non-gonococcal, non-chlamydial urethritis exceptexcept::a.a. Gardnerella vaginalisGardnerella vaginalis
b.b. AdenovirusAdenovirus
c.c. Mycoplasma genitaliumMycoplasma genitalium
d.d. Trichomonas vaginalisTrichomonas vaginalis
e.e. HSVHSV
What is the most common sexually-transmitted What is the most common sexually-transmitted cause of genital ulcer disease in the U.S.?cause of genital ulcer disease in the U.S.?a.a. Primary syphilisPrimary syphilis
b.b. ChancroidChancroid
c.c. Genital herpesGenital herpes
d.d. Lymphogranuloma venereumLymphogranuloma venereum
e.e. DonovanosisDonovanosis
What are the most common sexually-transmitted What are the most common sexually-transmitted causes of genital ulcer disease in the U.S.?causes of genital ulcer disease in the U.S.? Genital herpesGenital herpes
Primary syphilis (chancre)Primary syphilis (chancre)
Chancroid (soft chancre)Chancroid (soft chancre)
Lymphogranuloma venereum (LGV)Lymphogranuloma venereum (LGV) Donovanosis (Granuloma inguinale)Donovanosis (Granuloma inguinale)
Genital Herpes: Background and Genital Herpes: Background and Burden of DiseaseBurden of Disease
Genital herpes is a chronic, lifelong viral infectionGenital herpes is a chronic, lifelong viral infection Reactivation is precipitated by multiple known and Reactivation is precipitated by multiple known and
unknown factors and induces viral replication unknown factors and induces viral replication The reactivated virus may cause a cutaneous outbreak of The reactivated virus may cause a cutaneous outbreak of
herpetic lesions or subclinical viral sheddingherpetic lesions or subclinical viral shedding HSV-2 causes the majority of cases of recurrent HSV-2 causes the majority of cases of recurrent
genital herpes in the U.S.genital herpes in the U.S. Approximately 1 million new cases occur each yearApproximately 1 million new cases occur each year Up to 90% of persons seropositive for HSV-2 Up to 90% of persons seropositive for HSV-2
antibody have not been diagnosed with genital antibody have not been diagnosed with genital herpesherpes
11
12
Asymptomatic Viral SheddingAsymptomatic Viral Shedding
Most HSV-2 is transmitted during asymptomatic Most HSV-2 is transmitted during asymptomatic shedding shedding
Rates of asymptomatic shedding greater in HSV-2 than Rates of asymptomatic shedding greater in HSV-2 than HSV-1 HSV-1
Rates of asymptomatic shedding are highest in new Rates of asymptomatic shedding are highest in new infections (<2 years) and gradually decrease over time infections (<2 years) and gradually decrease over time
Asymptomatic shedding episodes are of shorter Asymptomatic shedding episodes are of shorter duration than shedding during clinical recurrencesduration than shedding during clinical recurrences
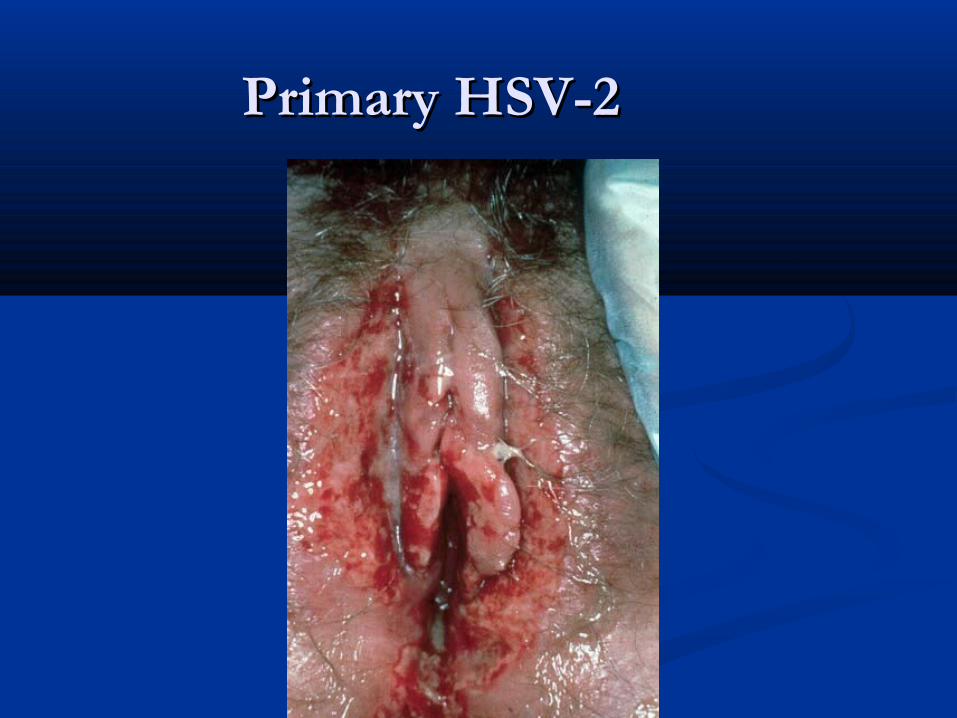
Primary HSV-2Primary HSV-2
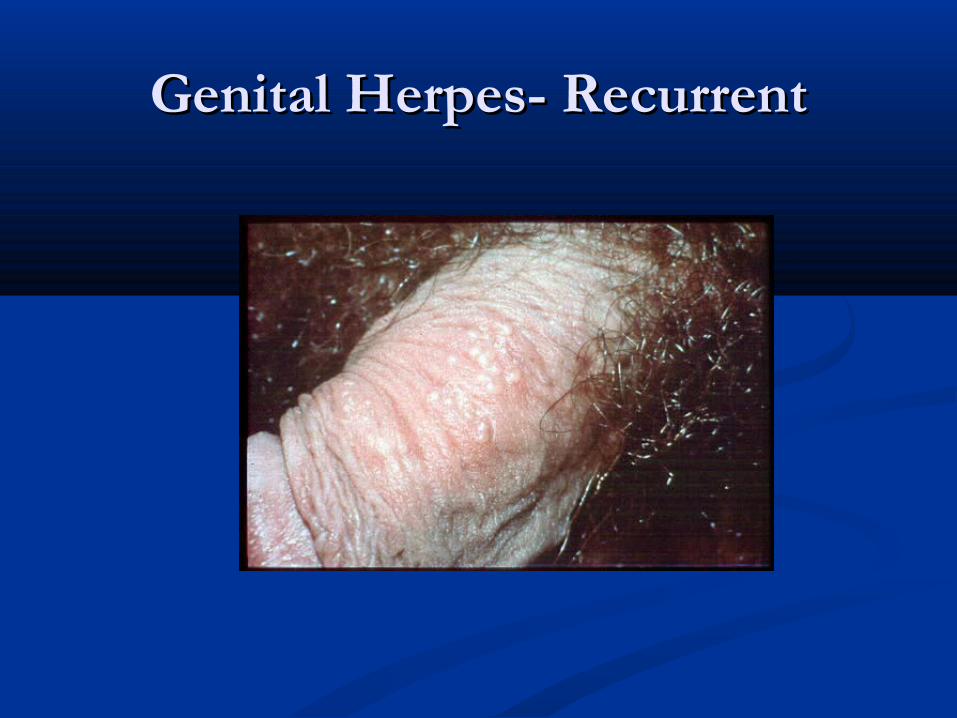
Genital Herpes- RecurrentGenital Herpes- Recurrent

HSV-2 in ImmunosuppressedHSV-2 in Immunosuppressed
Tests for Diagnosis of Genital HerpesTests for Diagnosis of Genital Herpes
Viral culture (gold standard)Viral culture (gold standard) Preferred test if genital ulcers or other mucocutaneous lesions are presentPreferred test if genital ulcers or other mucocutaneous lesions are present Highly specific (>99%) Highly specific (>99%) Sensitivity depends on stage of lesion; declines rapidly as lesions begin to heal Sensitivity depends on stage of lesion; declines rapidly as lesions begin to heal Positive more often in primary infection (80%–90%) than with recurrences Positive more often in primary infection (80%–90%) than with recurrences
(30%) (30%)
Polymerase Chain Reaction (PCR) Polymerase Chain Reaction (PCR) More sensitive than viral culture; has been used instead of culture in some More sensitive than viral culture; has been used instead of culture in some
settings; however PCR tests are not FDA-cleared or widely available settings; however PCR tests are not FDA-cleared or widely available Preferred test for detecting HSV in spinal fluid Preferred test for detecting HSV in spinal fluid
Tests for Diagnosis of Genital HerpesTests for Diagnosis of Genital Herpes(continued)(continued)
Antigen detection (DFA)Antigen detection (DFA) Fairly sensitive (>85%) in symptomatic sheddersFairly sensitive (>85%) in symptomatic shedders Rapid (2-12 hours)Rapid (2-12 hours) May be better than culture for detecting HSV in May be better than culture for detecting HSV in
healing lesionshealing lesions
Cytology (Tzanck or Pap)Cytology (Tzanck or Pap) Insensitive and nonspecific and should not be relied on Insensitive and nonspecific and should not be relied on
for HSV diagnosisfor HSV diagnosis
All of the following are appropriate for the treatment All of the following are appropriate for the treatment of genital herpes of genital herpes exceptexcept::
a.a. AcyclovirAcyclovir
b.b. ValacyclovirValacyclovir
c.c. FamciclovirFamciclovir
d.d. ValganciclovirValganciclovir
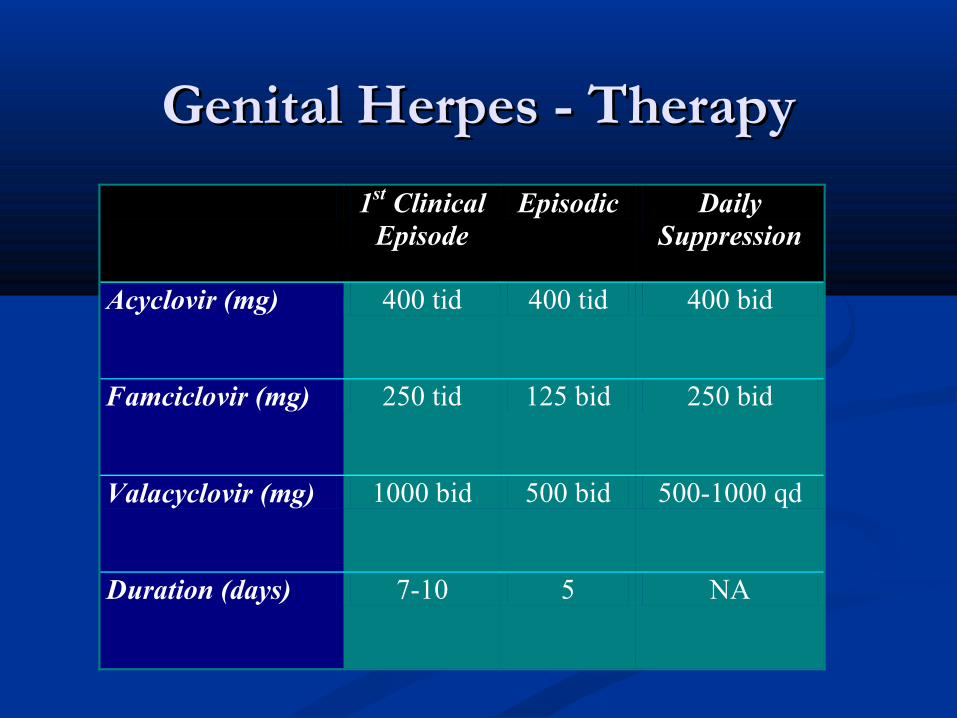
Genital Herpes - TherapyGenital Herpes - Therapy
1st Clinical Episode
Episodic Daily Suppression
Acyclovir (mg) 400 tid 400 tid 400 bid
Famciclovir (mg) 250 tid 125 bid 250 bid
Valacyclovir (mg) 1000 bid 500 bid 500-1000 qd
Duration (days) 7-10 5 NA
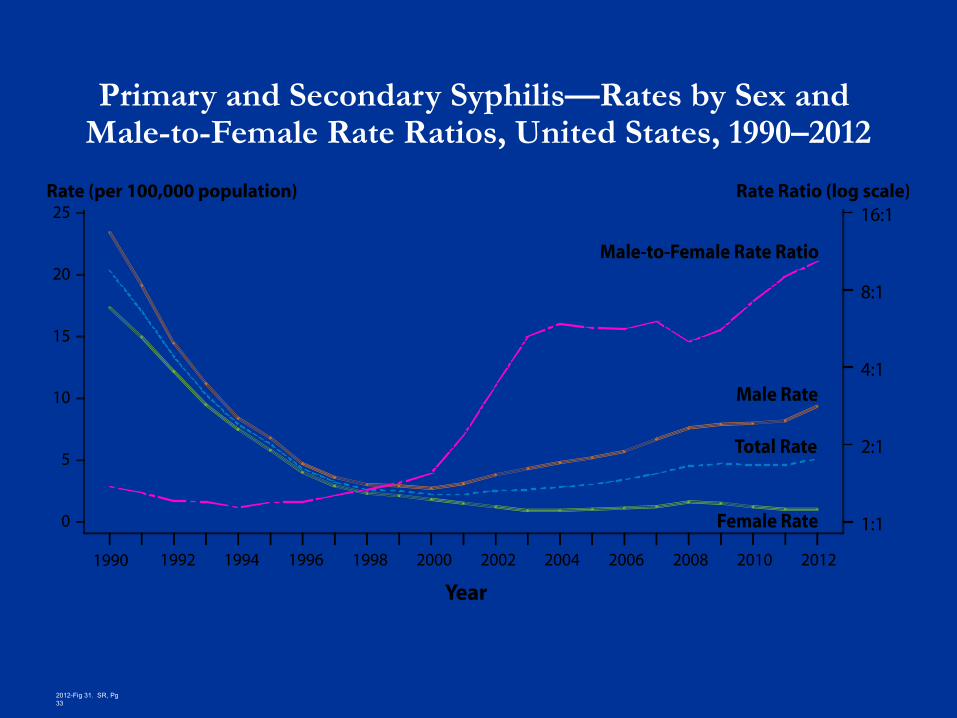
Primary and Secondary Syphilis—Rates by Sex and Male-to-Female Rate Ratios, United States, 1990–2012
2012-Fig 31. SR, Pg 33
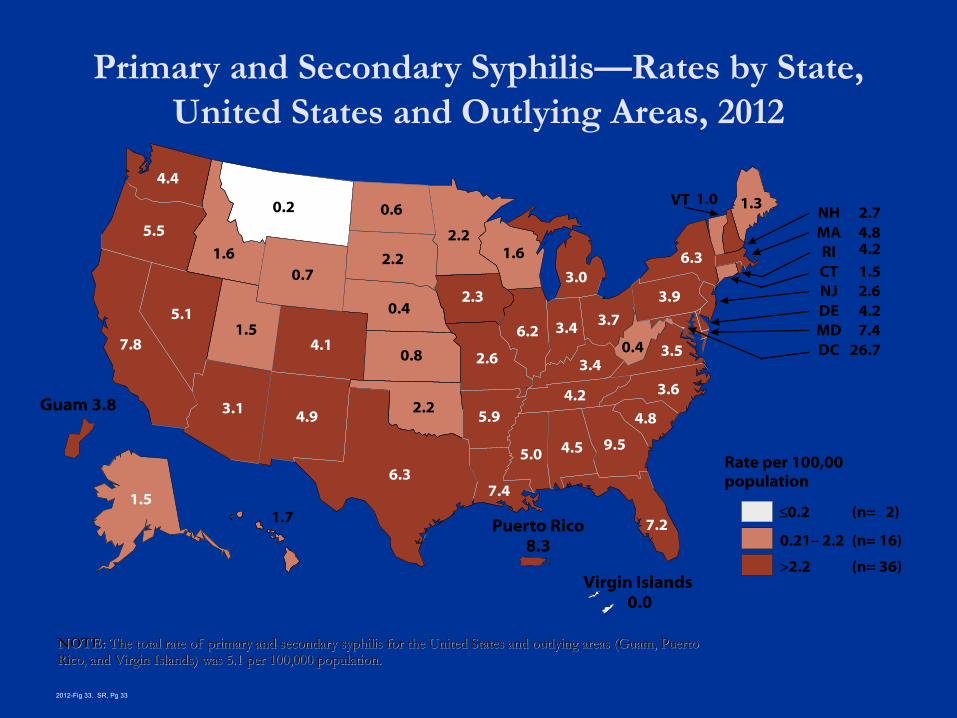
Primary and Secondary Syphilis—Rates by State, United States and Outlying Areas, 2012
NOTE: NOTE: The total rate of primary and secondary syphilis for the United States and outlying areas (Guam, Puerto The total rate of primary and secondary syphilis for the United States and outlying areas (Guam, Puerto Rico, and Virgin Islands) was 5.1 per 100,000 population.Rico, and Virgin Islands) was 5.1 per 100,000 population.
2012-Fig 33. SR, Pg 33
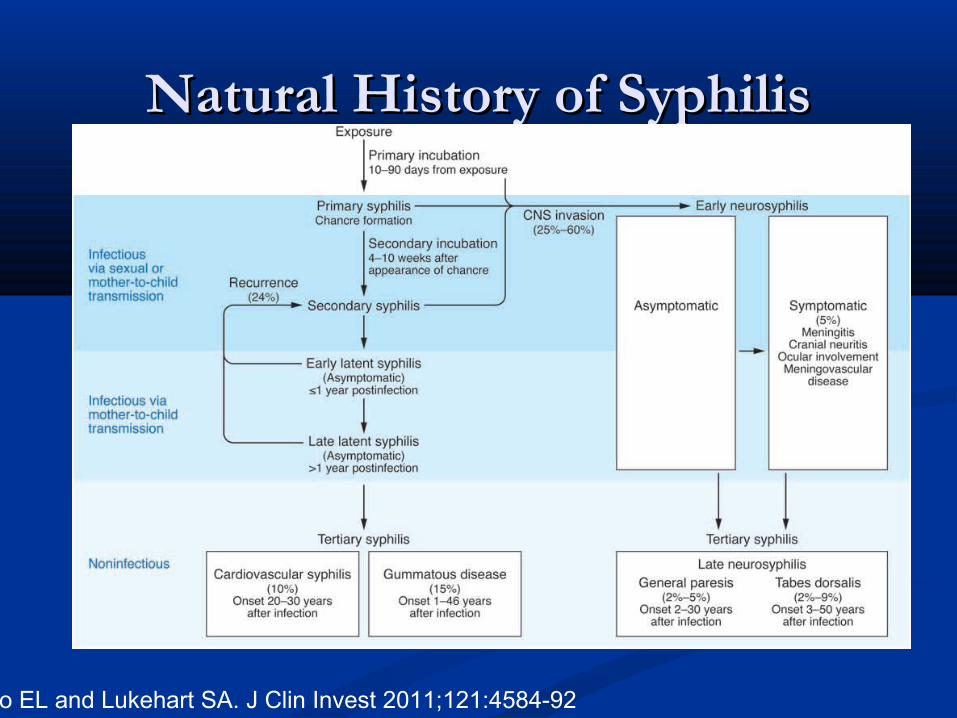
Natural History of SyphilisNatural History of Syphilis
Ho EL and Lukehart SA. J Clin Invest 2011;121:4584-92
All of the following are typical features of All of the following are typical features of the syphilitic chancre the syphilitic chancre exceptexcept::
a.a. PainPain
b.b. IndurationInduration
c.c. Heals spontaneously even without treatmentHeals spontaneously even without treatment
d.d. Accompanied by inguinal lymphadenopathyAccompanied by inguinal lymphadenopathy
e.e. Darkfield positivityDarkfield positivity
Primary Syphilis Primary Syphilis
Primary lesion or "chancre" develops at the site of Primary lesion or "chancre" develops at the site of inoculationinoculation
Chancre: Chancre: Progresses from macule to papule to ulcerProgresses from macule to papule to ulcer Typically painless, indurated, and has a clean baseTypically painless, indurated, and has a clean base Highly infectiousHighly infectious Heals spontaneously within 1 to 6 weeksHeals spontaneously within 1 to 6 weeks 25% present with multiple lesions25% present with multiple lesions
Regional lymphadenopathy: classically rubbery, painless, Regional lymphadenopathy: classically rubbery, painless, bilateral bilateral
Serologic tests for syphilis may not be positive during early Serologic tests for syphilis may not be positive during early primary syphilisprimary syphilis
25
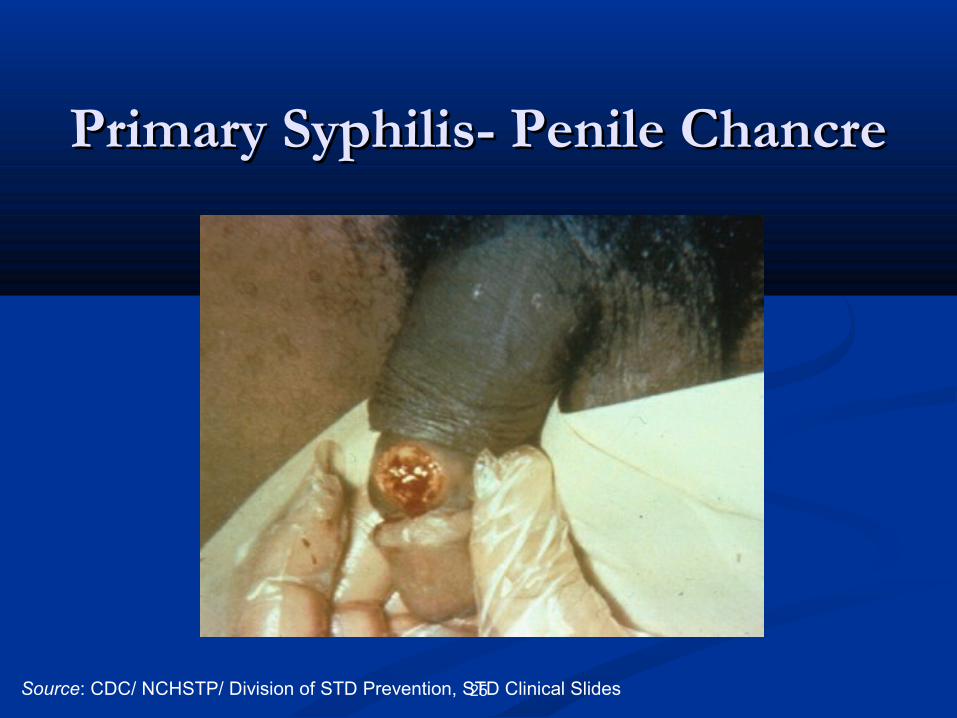
Primary Syphilis- Penile ChancrePrimary Syphilis- Penile Chancre
Source: CDC/ NCHSTP/ Division of STD Prevention, STD Clinical Slides
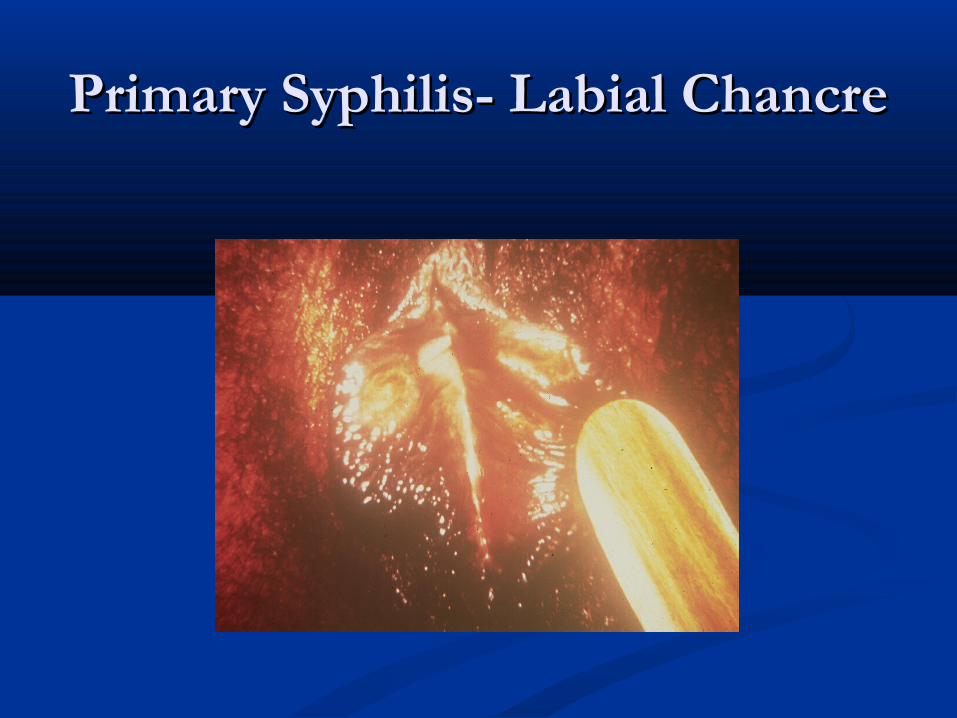
Primary Syphilis- Labial ChancrePrimary Syphilis- Labial Chancre
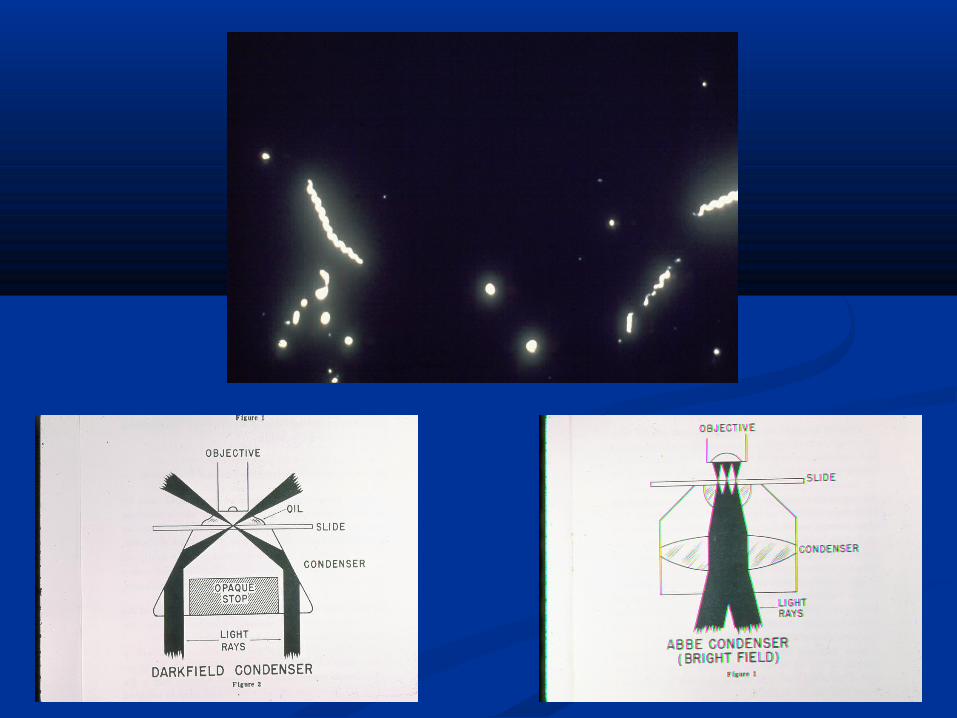
Darkfield MicroscopyDarkfield Microscopy What to look for:What to look for:
T. pallidumT. pallidum morphology and motility morphology and motility
Advantage:Advantage: Definitive immediate diagnosisDefinitive immediate diagnosis
Disadvantages:Disadvantages: Requires specialized equipment and an experienced Requires specialized equipment and an experienced
microscopistmicroscopist Possible confusion with other pathogenic and Possible confusion with other pathogenic and
nonpathogenic spirochetesnonpathogenic spirochetes Must be performed immediatelyMust be performed immediately Generally not recommended on oral lesions Generally not recommended on oral lesions Possibility of false-negativesPossibility of false-negatives
Under what circumstances should the diagnosis Under what circumstances should the diagnosis of chancroid be considered?of chancroid be considered? One or more painful ulcersOne or more painful ulcers Suppurative inguinal lymph nodesSuppurative inguinal lymph nodes Negative serologic test for syphilisNegative serologic test for syphilis Negative dark fieldNegative dark field Negative HSV test on ulcer exudateNegative HSV test on ulcer exudate
30
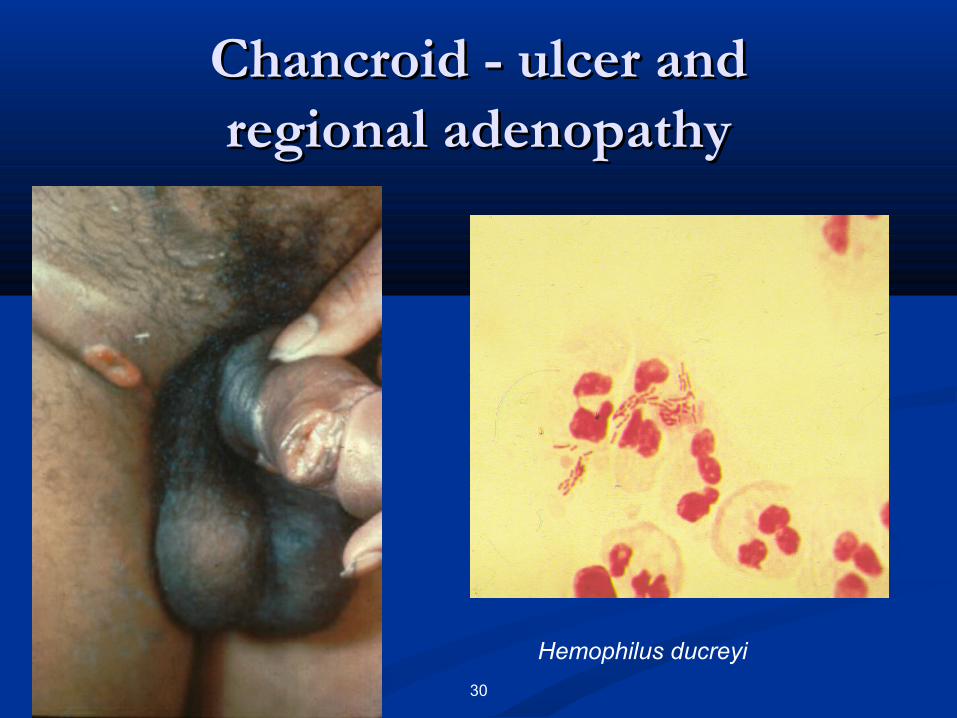
Chancroid - ulcer andChancroid - ulcer andregional adenopathyregional adenopathy
Hemophilus ducreyi
Which of the following is Which of the following is notnot an effective an effective treatment for chancroid?treatment for chancroid?a.a. Single 1 g dose of azithromycinSingle 1 g dose of azithromycin
b.b. Single 250 mg dose of ceftriaxoneSingle 250 mg dose of ceftriaxone
c.c. Ciprofloxacin for 3 daysCiprofloxacin for 3 days
d.d. Erythromycin for 7 daysErythromycin for 7 days
e.e. Benzathine penicillin G 2.4 million units IM times Benzathine penicillin G 2.4 million units IM times oneone
32
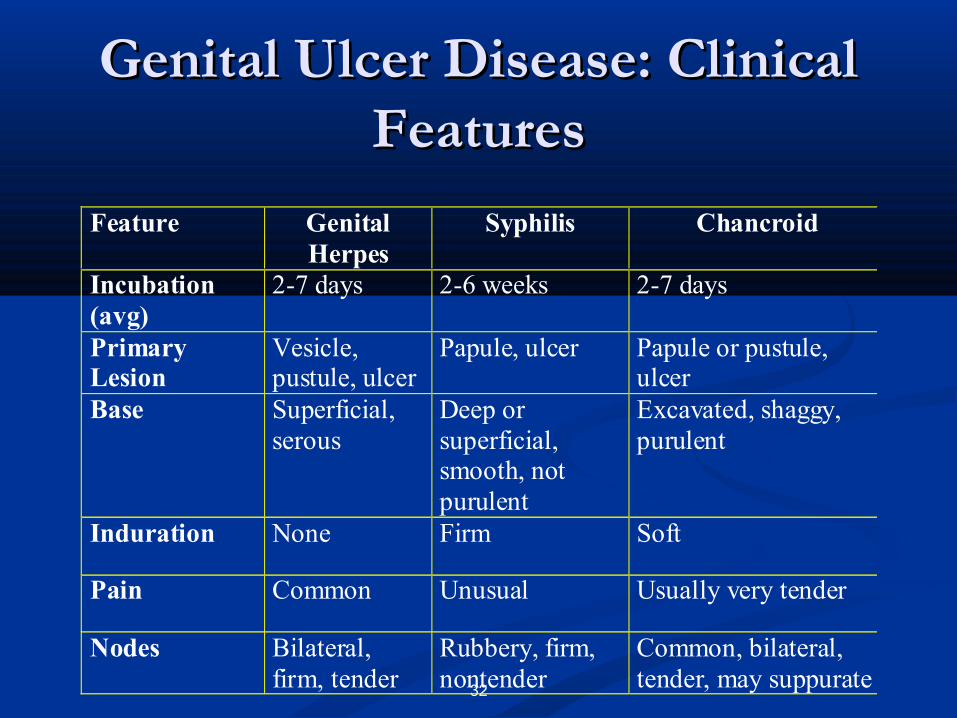
Genital Ulcer Disease: Clinical Genital Ulcer Disease: Clinical FeaturesFeatures
Feature GenitalHerpes
Syphilis Chancroid
Incubation(avg)
2-7 days 2-6 weeks 2-7 days
PrimaryLesion
Vesicle,pustule, ulcer
Papule, ulcer Papule or pustule,ulcer
Base Superficial,serous
Deep orsuperficial,smooth, notpurulent
Excavated, shaggy,purulent
Induration None Firm Soft
Pain Common Unusual Usually very tender
Nodes Bilateral,firm, tender
Rubbery, firm,nontender
Common, bilateral,tender, may suppurate

Courtesy of S. Stroud
Diagnosis?Diagnosis?
Secondary Syphilis Secondary Syphilis
Secondary lesions occur 3 to 6 weeks after the primary Secondary lesions occur 3 to 6 weeks after the primary chancre appears; may persist for weeks to monthschancre appears; may persist for weeks to months
Primary and secondary stages may overlapPrimary and secondary stages may overlap Mucocutaneous lesions most commonMucocutaneous lesions most common Manifestations:Manifestations:
Rash (75%-100%) Rash (75%-100%) Lymphadenopathy (50%-86%) Lymphadenopathy (50%-86%) MalaiseMalaise Mucous patches (6%-30%)Mucous patches (6%-30%) Condylomata lata (10%-20%)Condylomata lata (10%-20%) Alopecia (5%)Alopecia (5%)
Serologic tests are usually highest in titer during this stageSerologic tests are usually highest in titer during this stage
35
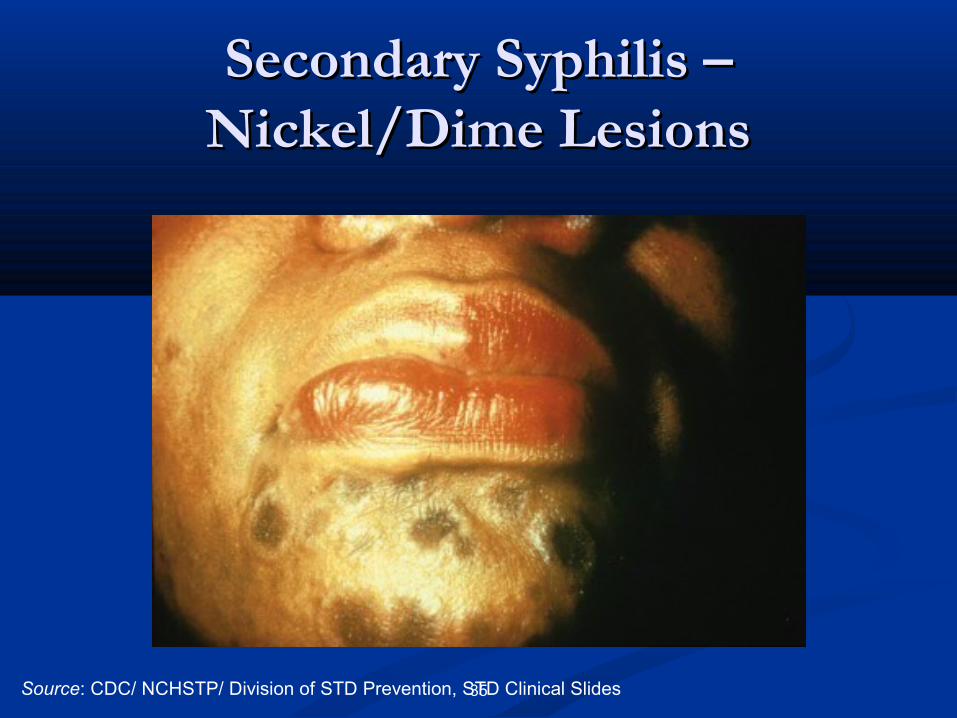
Secondary Syphilis – Secondary Syphilis – Nickel/Dime LesionsNickel/Dime Lesions
Source: CDC/ NCHSTP/ Division of STD Prevention, STD Clinical Slides
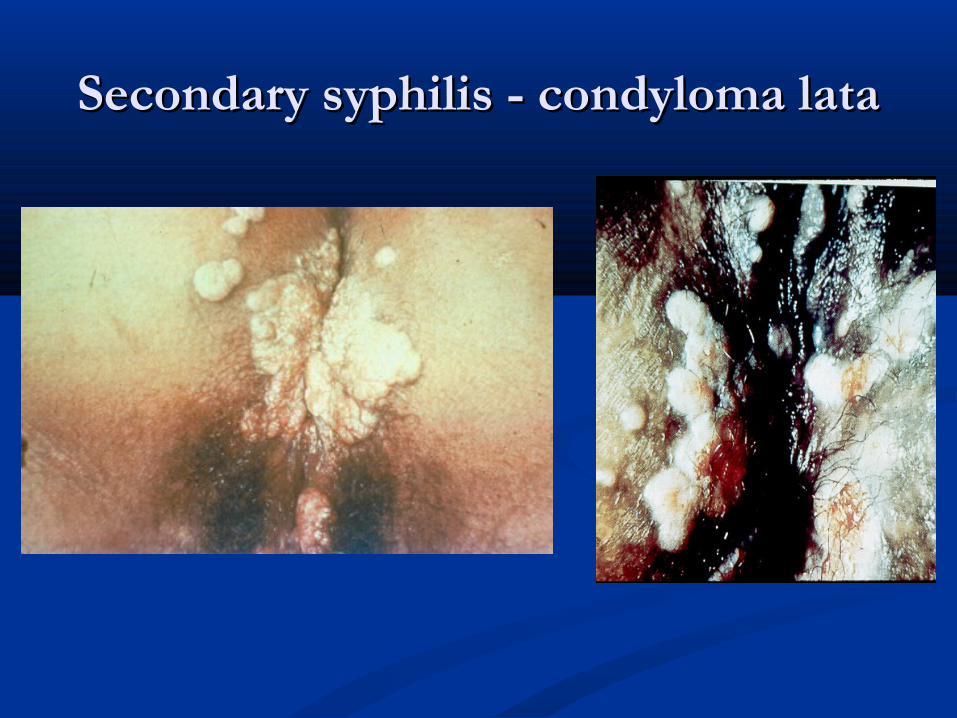
Secondary syphilis - condyloma lataSecondary syphilis - condyloma lata

Lues maligna or Ulceronodular syphilis
Courtesy of J. McCrary
a.a. NoneNone
b.b. Late latent syphilisLate latent syphilis
c.c. Early latent syphilisEarly latent syphilis
d.d. Latent syphilis of unknown durationLatent syphilis of unknown duration
e.e. Tertiary syphilisTertiary syphilis
Your patient has a positive RPR (1:16), a positive FTA-Abs, and no signs Your patient has a positive RPR (1:16), a positive FTA-Abs, and no signs or symptoms of primary or secondary syphilis. 10 months ago, the RPR or symptoms of primary or secondary syphilis. 10 months ago, the RPR
was nonreactive. About 6 months ago, she had a palmar rash, malaise, and was nonreactive. About 6 months ago, she had a palmar rash, malaise, and swollen lymph nodes in her neck. All of this went away without any swollen lymph nodes in her neck. All of this went away without any
intervention after a few weeks, and she has felt perfectly well ever since. intervention after a few weeks, and she has felt perfectly well ever since. What stage of syphilis does your patient have now? What stage of syphilis does your patient have now?
Latent Syphilis Latent Syphilis
Host suppresses the infection enough so that no Host suppresses the infection enough so that no lesions are clinically apparentlesions are clinically apparent
Only evidence is positive serologic test for syphilisOnly evidence is positive serologic test for syphilis May occur between primary and secondary stages, May occur between primary and secondary stages,
between secondary relapses, and after secondary between secondary relapses, and after secondary stage stage
Categories: Categories: Early latent: <1 year durationEarly latent: <1 year duration Late latent: Late latent: ≥≥1 year duration1 year duration
Neurosyphilis Neurosyphilis
Occurs when Occurs when T. pallidumT. pallidum invades the CNS invades the CNS
May occur at any stage of syphilisMay occur at any stage of syphilis
Can be asymptomaticCan be asymptomatic
Early neurosyphilis occurs a few months to a few years after Early neurosyphilis occurs a few months to a few years after infectioninfection Clinical manifestations include acute syphilitic meningitis, Clinical manifestations include acute syphilitic meningitis,
meningovascular syphilis, ocular involvementmeningovascular syphilis, ocular involvement
Late neurosyphilis occurs decades after infection and is rarely Late neurosyphilis occurs decades after infection and is rarely seenseen Clinical manifestations include general paresis, tabes dorsalis, ocular Clinical manifestations include general paresis, tabes dorsalis, ocular
involvementinvolvement
Serologic Tests for SyphilisSerologic Tests for Syphilis
Two typesTwo types Nontreponemal (qualitative and quantitative)Nontreponemal (qualitative and quantitative) Treponemal (qualitative)Treponemal (qualitative)
The use of only one type of serologic test is The use of only one type of serologic test is insufficient for diagnosisinsufficient for diagnosis
Conventional testing: nontreponemal followed Conventional testing: nontreponemal followed by treponemalby treponemal
Nontreponemal (Lipoidal) Nontreponemal (Lipoidal) Serologic TestsSerologic Tests
Rapid Plasma Reagin (RPR), Venereal Disease Rapid Plasma Reagin (RPR), Venereal Disease Research Laboratory (VDRL) testResearch Laboratory (VDRL) test
PrinciplesPrinciples Measure antibody directed against lipoidal antigens released from Measure antibody directed against lipoidal antigens released from
damaged host cells and possibly from the treponemes themselvesdamaged host cells and possibly from the treponemes themselves Not specific for Not specific for T. pallidumT. pallidum Titers usually correlate with disease activity and results are reported Titers usually correlate with disease activity and results are reported
quantitativelyquantitatively Usually, but not always, disappear after effective treatmentUsually, but not always, disappear after effective treatment
Nontreponemal Serologic Tests Nontreponemal Serologic Tests (continued)(continued)
Advantages:Advantages: Rapid and inexpensiveRapid and inexpensive Easy to perform and can be Easy to perform and can be
done in clinic or officedone in clinic or office QuantitativeQuantitative Used to follow response to Used to follow response to
therapytherapy Can be used to evaluate Can be used to evaluate
possible reinfectionpossible reinfection
Disadvantages:Disadvantages: Takes a person to do the test Takes a person to do the test
(can’t be automated)(can’t be automated) May be insensitive in certain May be insensitive in certain
stages (false negative in early stages (false negative in early infection)infection)
Prozone effect may cause a Prozone effect may cause a false-negative reaction false-negative reaction
False-positive reactions may False-positive reactions may occuroccur
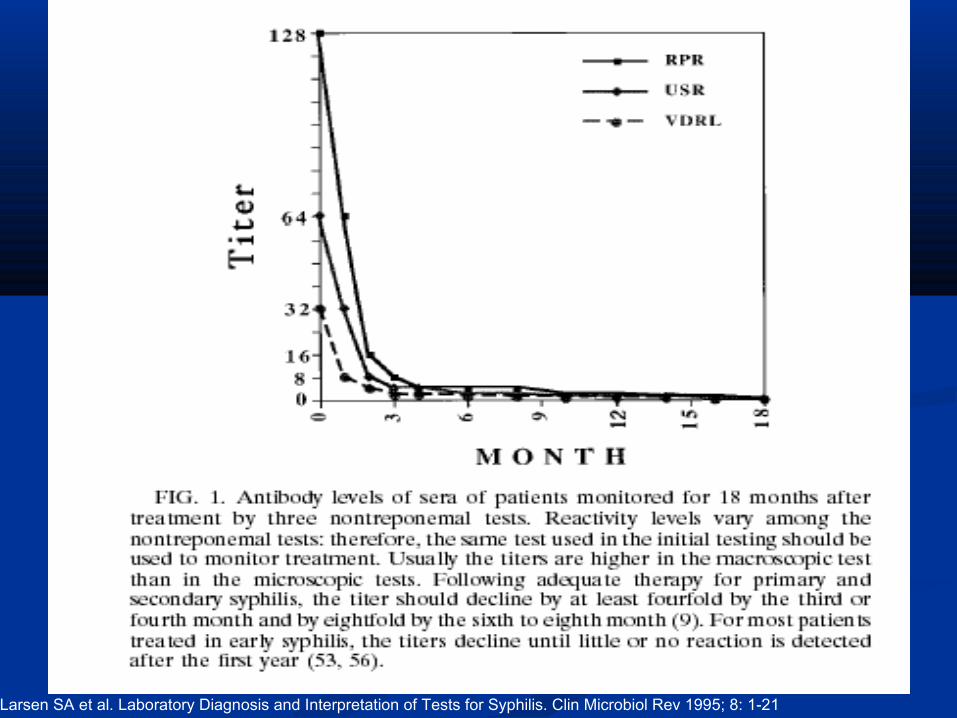
Larsen SA et al. Laboratory Diagnosis and Interpretation of Tests for Syphilis. Clin Microbiol Rev 1995; 8: 1-21
False Positive Non-Treponemal TestsFalse Positive Non-Treponemal Tests
HepatitisHepatitis Infectious monoInfectious mono Viral pneumoniaViral pneumonia VaricellaVaricella MeaslesMeasles MalariaMalaria ImmunizationsImmunizations PregnancyPregnancy Lab or technical errorLab or technical error
SLESLE Diseases associated with Diseases associated with
immunoglobulin immunoglobulin abnormalitiesabnormalities
Narcotic addictionNarcotic addiction LeprosyLeprosy MalignancyMalignancy Aging Aging
Treponemal Serologic TestsTreponemal Serologic Tests
Fluorescent Treponemal Antibody Absorbed (FTA-Fluorescent Treponemal Antibody Absorbed (FTA-ABS) test, ABS) test, T. pallidum T. pallidum particle agglutination (TP-PA) particle agglutination (TP-PA) testtest
PrinciplesPrinciples Measure antibodies directed against Measure antibodies directed against T. pallidumT. pallidum
polypeptidespolypeptides QualitativeQualitative Usually reactive for lifeUsually reactive for life
Not useful for following response to therapyNot useful for following response to therapy Unable to differentiate current from past infectionUnable to differentiate current from past infection
Newer Tests: Treponemal enzyme and Newer Tests: Treponemal enzyme and chemiluminescence immunoassays chemiluminescence immunoassays
(EIA/CIA)(EIA/CIA)
Detect antibodies directed against recombinant Detect antibodies directed against recombinant T. pallidum T. pallidum proteins (e.g. Tp17, Tp47)proteins (e.g. Tp17, Tp47)
Automated to allow screening of large numbers Automated to allow screening of large numbers of specimensof specimens
Unable to differentiate recent from remote or Unable to differentiate recent from remote or treated from untreated infectionstreated from untreated infections
False positivesFalse positives Patients with periodontal disease (and oral Patients with periodontal disease (and oral
spirochetes) have antibody that reacts to Tp47spirochetes) have antibody that reacts to Tp47
Reverse Sequence Syphilis Reverse Sequence Syphilis ScreeningScreening
Screening sera first with EIA/CIA, followed by Screening sera first with EIA/CIA, followed by nontreponemal testing of reactive specimensnontreponemal testing of reactive specimens
The CDC does not recommend this strategy yetThe CDC does not recommend this strategy yet
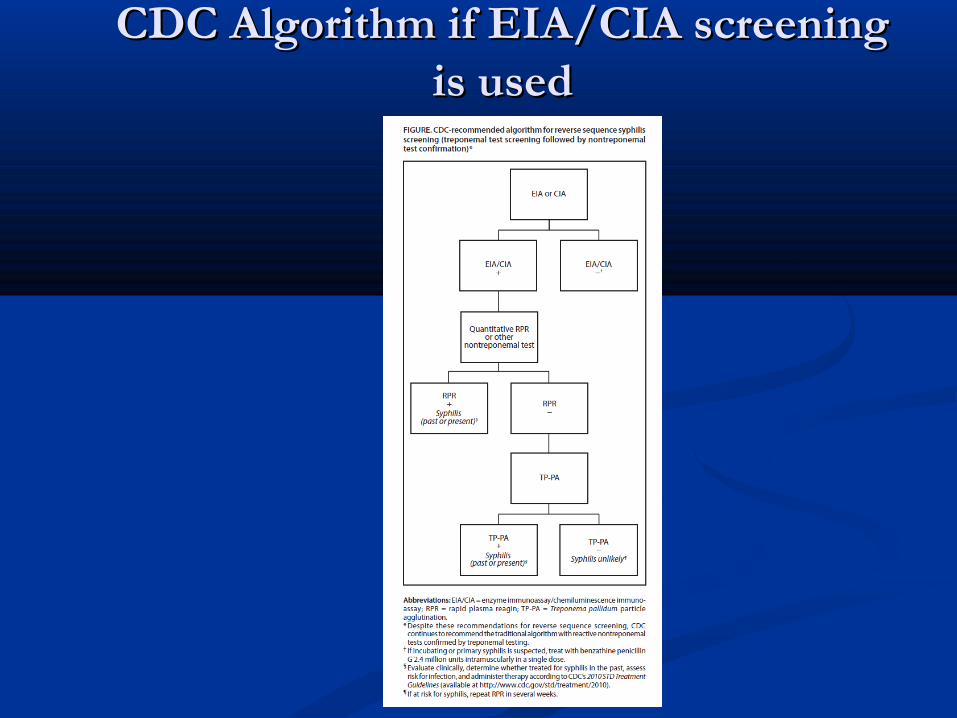
CDC Algorithm if EIA/CIA screening CDC Algorithm if EIA/CIA screening is usedis used
In which of the following situations is an LP In which of the following situations is an LP notnot indicated for a patient with syphilis (positive indicated for a patient with syphilis (positive RPR and confirmatory test)?RPR and confirmatory test)?a.a. Patient has headache and stiff neckPatient has headache and stiff neck
b.b. Patient has hearing loss and diplopiaPatient has hearing loss and diplopia
c.c. Patient was treated for secondary syphilis with BIC Patient was treated for secondary syphilis with BIC 2.4 MU 6 months ago and RPR is now 4 times 2.4 MU 6 months ago and RPR is now 4 times higherhigher
d.d. Patient has aortitisPatient has aortitis
e.e. Patient has no signs or symptoms of syphilis, but is Patient has no signs or symptoms of syphilis, but is coinfected with HIVcoinfected with HIV
Indications for Lumbar PunctureIndications for Lumbar Puncture
Any one of the following criteria should prompt CSF Any one of the following criteria should prompt CSF evaluation:evaluation: Neurologic symptoms/signs (CN deficits, chronic or acute Neurologic symptoms/signs (CN deficits, chronic or acute
meningitis, stroke, altered mentation, loss of vibratory sense, meningitis, stroke, altered mentation, loss of vibratory sense, auditory abnormalities, ophthalmic signs or symptoms) auditory abnormalities, ophthalmic signs or symptoms)
Evidence of active tertiary syphilis (e.g., aortitis, gumma, and iritis) Evidence of active tertiary syphilis (e.g., aortitis, gumma, and iritis) Treatment failure (Failure of expected 4-fold decrease in Treatment failure (Failure of expected 4-fold decrease in
nontreponemal titers over time)nontreponemal titers over time)
REMOVED from latest version of CDC STD treatment REMOVED from latest version of CDC STD treatment guidelines: HIV infection with late latent syphilis or latent guidelines: HIV infection with late latent syphilis or latent syphilis of unknown duration syphilis of unknown duration
Diagnosis of NeurosyphilisDiagnosis of Neurosyphilis
CSF VDRL: highly specific but insensitive; when reactive in CSF VDRL: highly specific but insensitive; when reactive in the absence of gross contamination of the CSF with blood, it the absence of gross contamination of the CSF with blood, it is considered diagnostic of neurosyphilis is considered diagnostic of neurosyphilis
CSF FTA-Abs: highly sensitive but not specificCSF FTA-Abs: highly sensitive but not specific Diagnosis usually depends on the following factors:Diagnosis usually depends on the following factors:
Reactive blood test results,Reactive blood test results, Abnormalities of CSF cell count or protein, or Abnormalities of CSF cell count or protein, or A reactive CSF VDRL with or without clinical manifestations.A reactive CSF VDRL with or without clinical manifestations.
CSF leukocyte count usually is elevated (>5 WBCs/mmCSF leukocyte count usually is elevated (>5 WBCs/mm33) in ) in patients with neurosyphilispatients with neurosyphilis
You are asked to see a 25 year old pregnant woman with You are asked to see a 25 year old pregnant woman with secondary syphilis. She reports an allergy to penicillin that secondary syphilis. She reports an allergy to penicillin that consists of raised itchy skin lesions, wheezing, and swelling of consists of raised itchy skin lesions, wheezing, and swelling of her throat that required emergency treatment with epinephrine her throat that required emergency treatment with epinephrine when she was 10 years old. What is your next step?when she was 10 years old. What is your next step?
a.a. Treat her with BIC 2.4 MU IM times one because she has Treat her with BIC 2.4 MU IM times one because she has probably outgrown her allergyprobably outgrown her allergy
b.b. Desensitize her to penicillin, and then treat her with BIC 2.4 Desensitize her to penicillin, and then treat her with BIC 2.4 MU IM times one MU IM times one
c.c. Don’t treat her at all because the risks outweigh the benefits Don’t treat her at all because the risks outweigh the benefits and you know the secondary manifestations will resolve on and you know the secondary manifestations will resolve on their owntheir own
d.d. Treat her with doxycycline 100 mg po bid for 14 daysTreat her with doxycycline 100 mg po bid for 14 days
e.e. Treat her with erythromycin 500 mg po qid for 14 daysTreat her with erythromycin 500 mg po qid for 14 days
f.f. None of the above are correct None of the above are correct
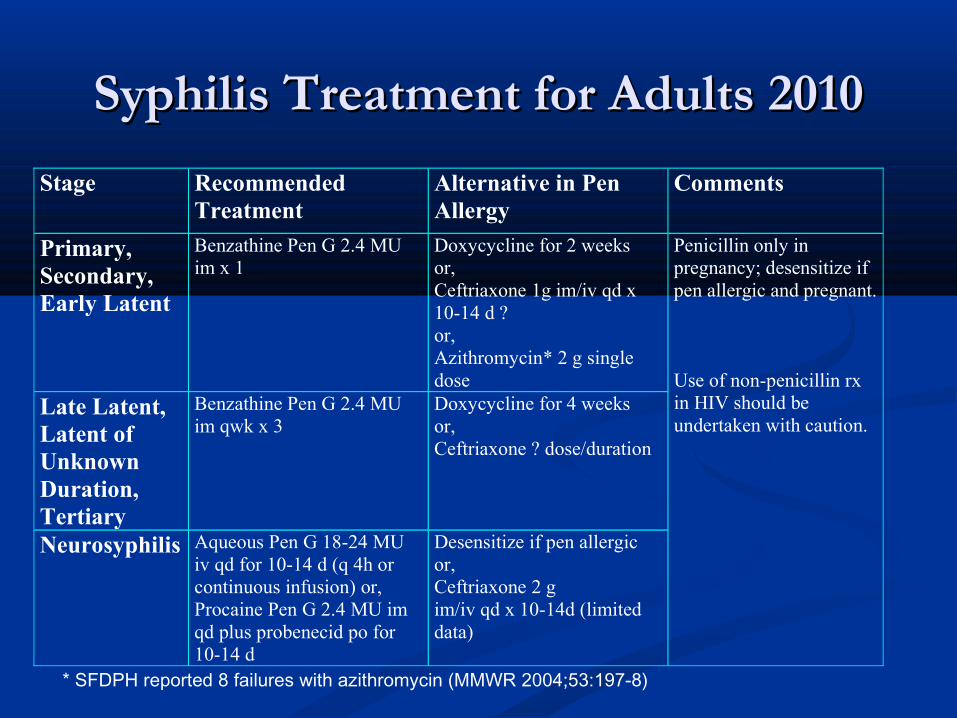
Syphilis Treatment for Adults 2010Syphilis Treatment for Adults 2010
Stage Recommended Treatment
Alternative in Pen Allergy
Comments
Primary, Secondary, Early Latent
Benzathine Pen G 2.4 MU im x 1
Doxycycline for 2 weeks or, Ceftriaxone 1g im/iv qd x 10-14 d ? or, Azithromycin* 2 g single dose
Penicillin only in pregnancy; desensitize if pen allergic and pregnant. Use of non-penicillin rx in HIV should be undertaken with caution.
Late Latent, Latent of Unknown Duration, Tertiary
Benzathine Pen G 2.4 MU im qwk x 3
Doxycycline for 4 weeks or, Ceftriaxone ? dose/duration
Neurosyphilis Aqueous Pen G 18-24 MU iv qd for 10-14 d (q 4h or continuous infusion) or, Procaine Pen G 2.4 MU im qd plus probenecid po for 10-14 d
Desensitize if pen allergic or, Ceftriaxone 2 g im/iv qd x 10-14d (limited data)
* SFDPH reported 8 failures with azithromycin (MMWR 2004;53:197-8)
Alternatives to PenicillinAlternatives to Penicillin CeftriaxoneCeftriaxone
Limited data for early syphilis (Hook EW et al. Limited data for early syphilis (Hook EW et al. J Infect Dis J Infect Dis 1988;158:881-4)1988;158:881-4)
An acceptable alternative for neurosyphilisAn acceptable alternative for neurosyphilis Doxycycline (and tetracycline)Doxycycline (and tetracycline)
Retrospective studies support use for the treatment of early syphilis Retrospective studies support use for the treatment of early syphilis (Wong T et al. (Wong T et al. Am J Med Am J Med 2008;121:903-8 and Ghanem KG et al. 2008;121:903-8 and Ghanem KG et al. Clin Infect Dis Clin Infect Dis 2006;42:e45-9)2006;42:e45-9)
Macrolides (azithromycin)Macrolides (azithromycin) Data for use of alternative agents in HIV-infected patients are Data for use of alternative agents in HIV-infected patients are
limitedlimited Do not use alternative agents in pregnant women with syphilisDo not use alternative agents in pregnant women with syphilis
A patient with secondary syphilis develops fever, A patient with secondary syphilis develops fever, chills, headache, etc after receiving a dose of chills, headache, etc after receiving a dose of penicillin. What is the diagnosis?penicillin. What is the diagnosis?
Jarisch-Herxheimer Reaction Jarisch-Herxheimer Reaction Self-limited reaction following anti-treponemal therapySelf-limited reaction following anti-treponemal therapy More frequent with early syphilis and penicillin More frequent with early syphilis and penicillin Fever/chills, headache, malaise, nausea/vomiting and Fever/chills, headache, malaise, nausea/vomiting and
exacerbation of secondary rashexacerbation of secondary rash Usually occurs 4-6 hours after rx and resolves within 24 Usually occurs 4-6 hours after rx and resolves within 24
hours hours Not an allergic reaction to penicillinNot an allergic reaction to penicillin Due to reaction to released treponemal constituentsDue to reaction to released treponemal constituents Treat with aspirin or NSAIDSTreat with aspirin or NSAIDS Pregnant women should be informed of this possible Pregnant women should be informed of this possible
reaction, that it may precipitate early laborreaction, that it may precipitate early labor
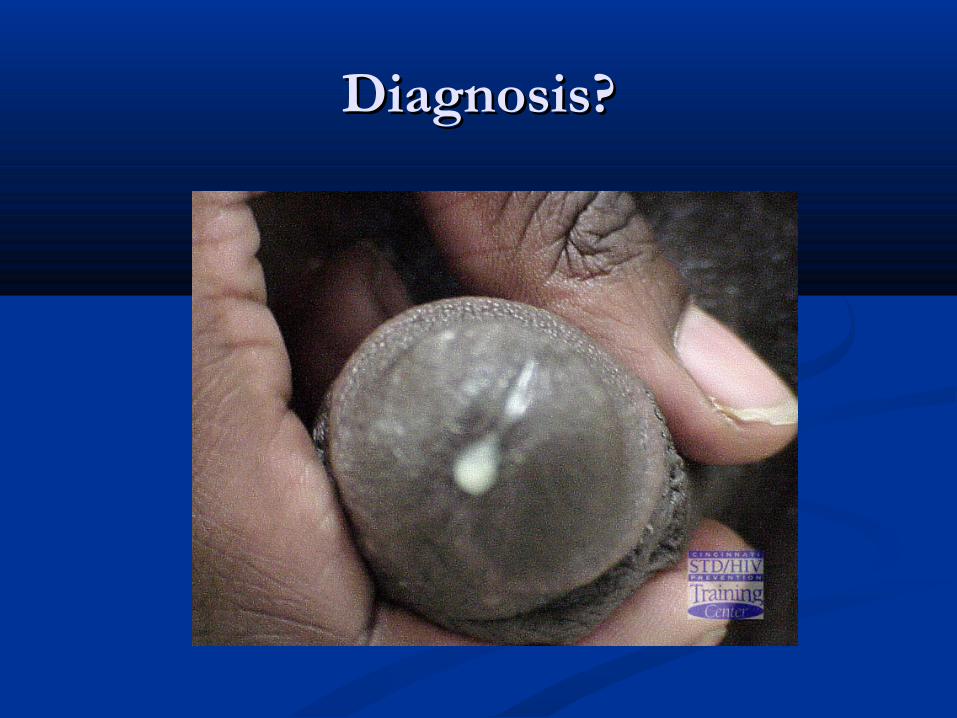
Diagnosis?Diagnosis?
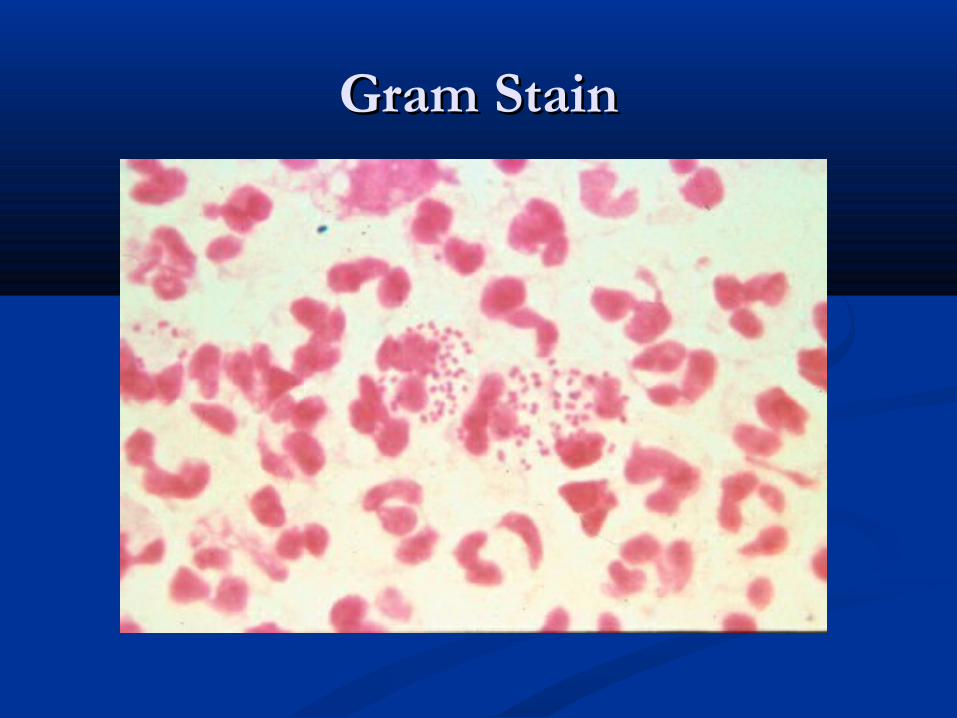
Gram StainGram Stain
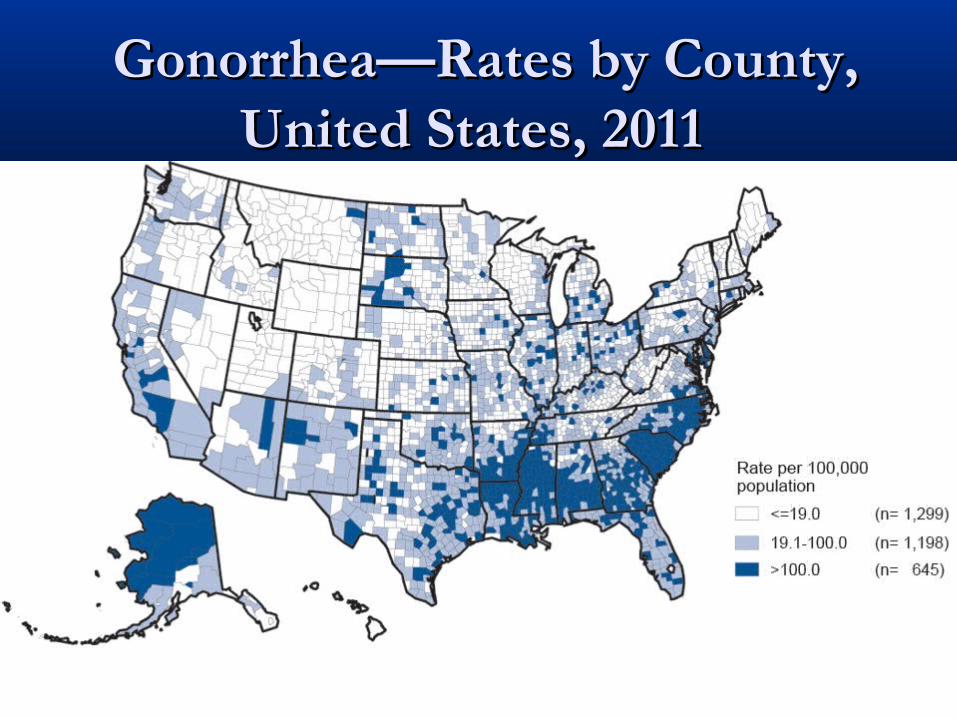
Gonorrhea—Rates by County, Gonorrhea—Rates by County, United States, 2011 United States, 2011
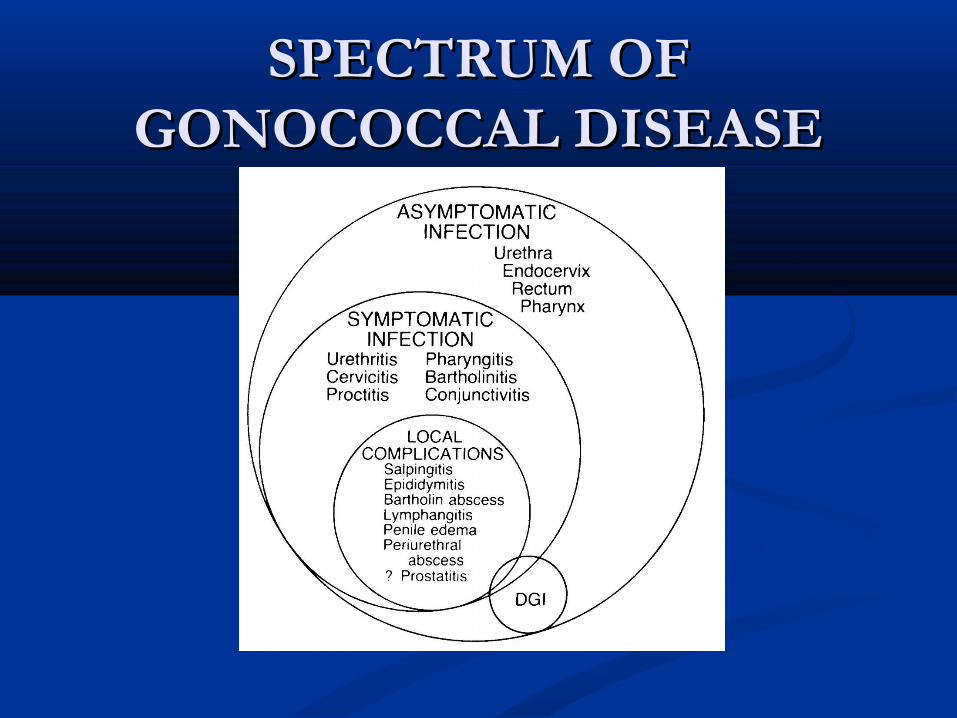
SPECTRUM OF SPECTRUM OF GONOCOCCAL DISEASEGONOCOCCAL DISEASE
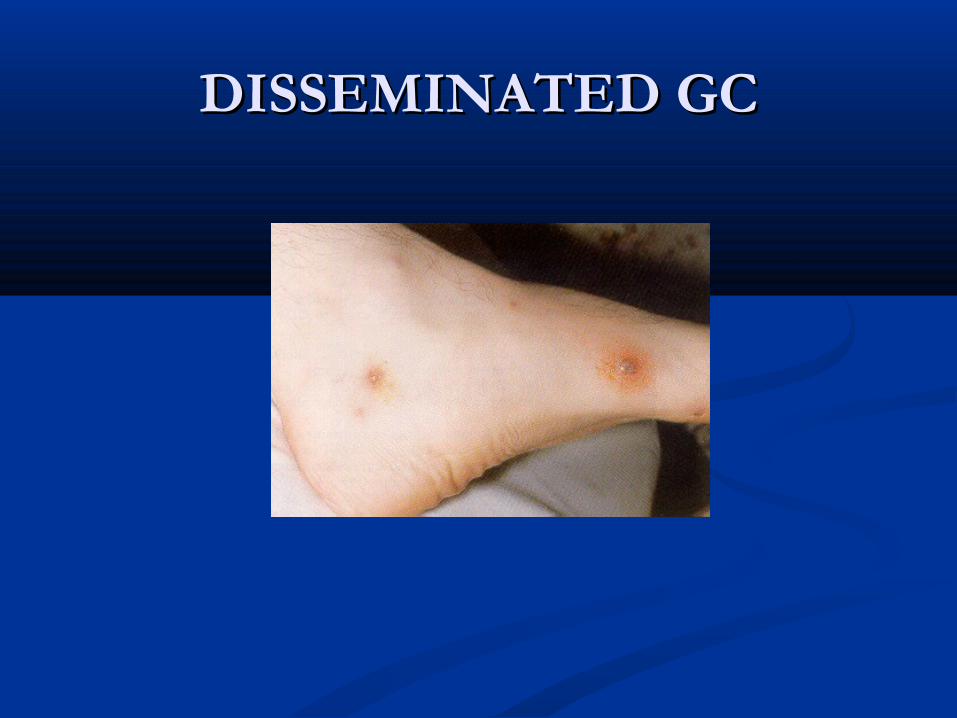
DISSEMINATED GCDISSEMINATED GC
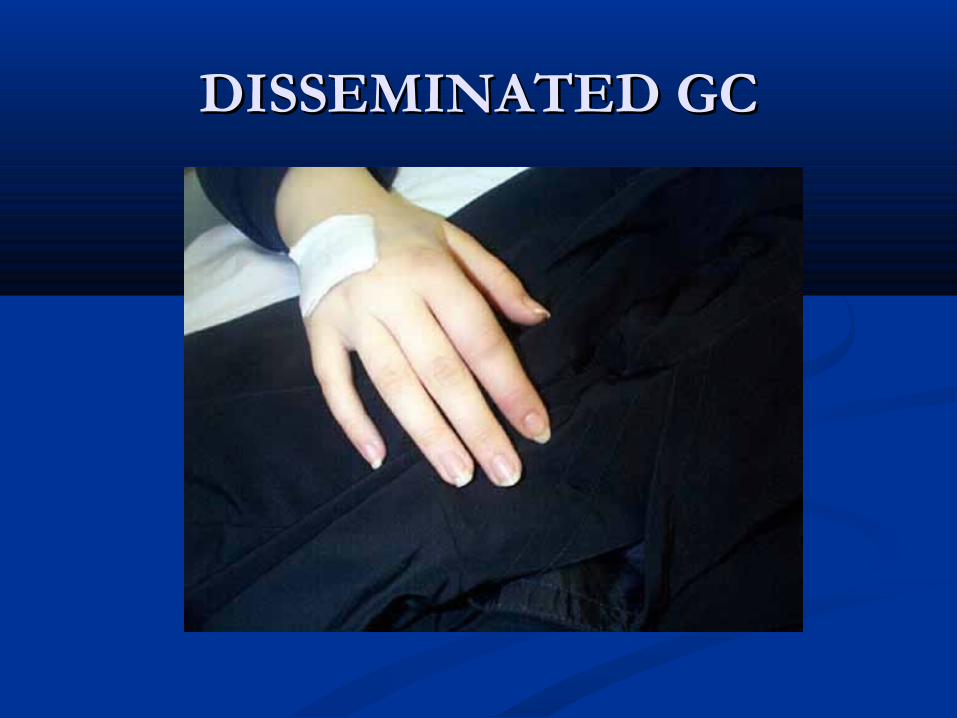
DISSEMINATED GCDISSEMINATED GC
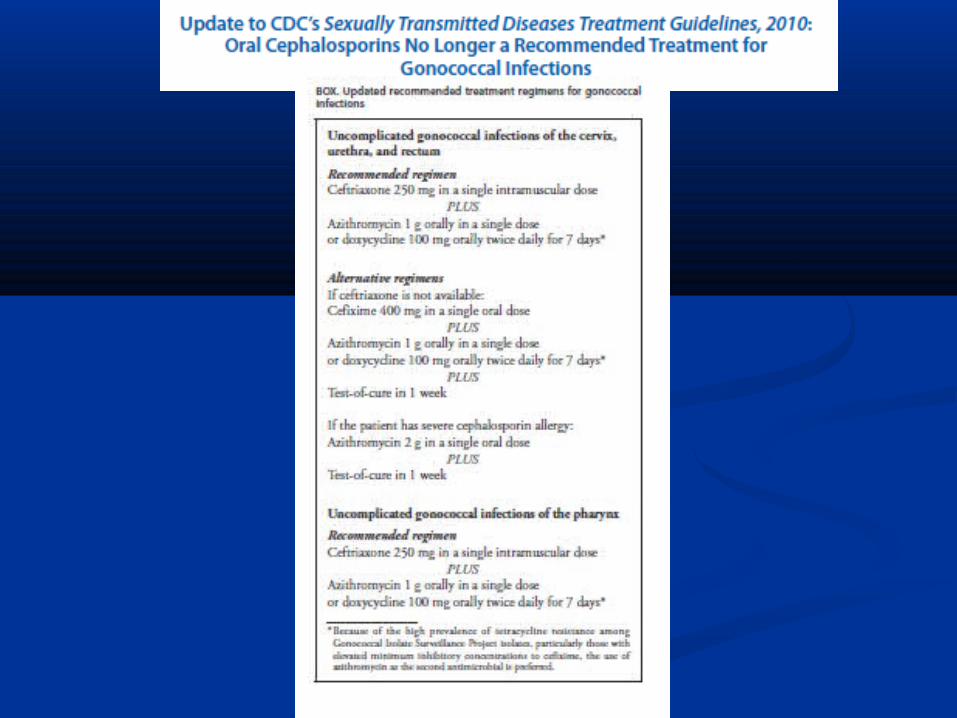
How is uncomplicated gonorrhea treated?How is uncomplicated gonorrhea treated?
Antibiotic Resistance in Antibiotic Resistance in Neisseria GonorrhoeaeNeisseria Gonorrhoeae
The gonococcus possesses extraordinary adaptive abilityThe gonococcus possesses extraordinary adaptive ability Multiple mechanisms of resistance acquired via Multiple mechanisms of resistance acquired via
chromosomal mutations or acquisition of new genetic chromosomal mutations or acquisition of new genetic material plus selection due to antibiotic pressurematerial plus selection due to antibiotic pressure
Usual geographic pathway: Asia to Hawaii to west coast Usual geographic pathway: Asia to Hawaii to west coast of U.S. mainland of U.S. mainland
Resistance determinants persist even though the Resistance determinants persist even though the antibiotic has been removed from recommended antibiotic has been removed from recommended treatment regimens decades beforetreatment regimens decades before
In most cases the diagnosis of gonorrhea is not made In most cases the diagnosis of gonorrhea is not made with culturewith culture
High-Level Gonococcal High-Level Gonococcal Resistance to CeftriaxoneResistance to Ceftriaxone
Strain H041 isolated from the pharynx of a female Strain H041 isolated from the pharynx of a female commercial sex worker in Kyoto, Japan (Ohnishi M commercial sex worker in Kyoto, Japan (Ohnishi M et al. et al. Emerg Infec Dis Emerg Infec Dis 2011;17:148-9)2011;17:148-9) Ceftriaxone MIC 2 µg/mlCeftriaxone MIC 2 µg/ml Related to cefixime resistant strains that are prevalent in Related to cefixime resistant strains that are prevalent in
Japan and are now being seen in EuropeJapan and are now being seen in Europe Due to a unique Due to a unique penApenA mosaic allele with reduced mosaic allele with reduced
affinity for ceftriaxone in synergy with other affinity for ceftriaxone in synergy with other resistance determinants (Ohnishi et al. resistance determinants (Ohnishi et al. Antimicrob Antimicrob Agents Chemother Agents Chemother 2011;55:3538-45)2011;55:3538-45)
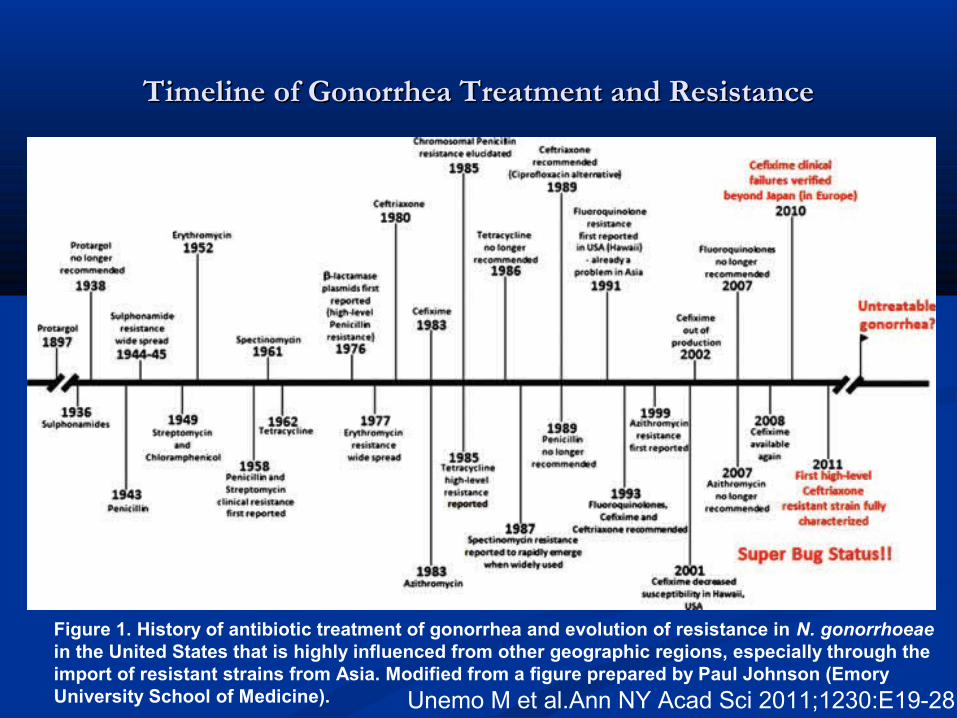
Timeline of Gonorrhea Treatment and ResistanceTimeline of Gonorrhea Treatment and Resistance
Figure 1. History of antibiotic treatment of gonorrhea and evolution of resistance in N. gonorrhoeae in the United States that is highly influenced from other geographic regions, especially through the import of resistant strains from Asia. Modified from a figure prepared by Paul Johnson (Emory University School of Medicine). Unemo M et al.Ann NY Acad Sci 2011;1230:E19-28

Solutions to Ceftriaxone Solutions to Ceftriaxone ResistanceResistance
Hope that these strains are less fit and don’t spreadHope that these strains are less fit and don’t spread Numerous prior examples indicate that gonococcal fitness is not diminished when antibiotic Numerous prior examples indicate that gonococcal fitness is not diminished when antibiotic
resistance occursresistance occurs There has already been a ceftriaxone-resistant strain in France (Unemo M et al. Antimicrob There has already been a ceftriaxone-resistant strain in France (Unemo M et al. Antimicrob
Agents Chemother, published online ahead of print 12 December 2011)Agents Chemother, published online ahead of print 12 December 2011) Higher/multiple doses of ceftriaxoneHigher/multiple doses of ceftriaxone
At best, this would be a short-term solutionAt best, this would be a short-term solution Combinations of existing agentsCombinations of existing agents Gentamicin (used in Malawi)Gentamicin (used in Malawi) CarbapenemsCarbapenems
Most Most penApenA alterations affect carbapenem MICs (Unemo M et al.Ann NY Acad Sci alterations affect carbapenem MICs (Unemo M et al.Ann NY Acad Sci 2011;1230:E19-28)2011;1230:E19-28)
Drugs with unique mechanisms of actionDrugs with unique mechanisms of action Efflux pump inhibitorsEfflux pump inhibitors Inhibition of synthesis of gonococcal lipid AInhibition of synthesis of gonococcal lipid A
Better surveillance, control, prevention, etcBetter surveillance, control, prevention, etc VaccineVaccine
Of the 3 common types of vaginitis, which Of the 3 common types of vaginitis, which one(s) are associated withone(s) are associated with A vaginal pH >4.5?A vaginal pH >4.5? A positive “whiff test”?A positive “whiff test”? The presence of clue cells on wet mount?The presence of clue cells on wet mount?
71
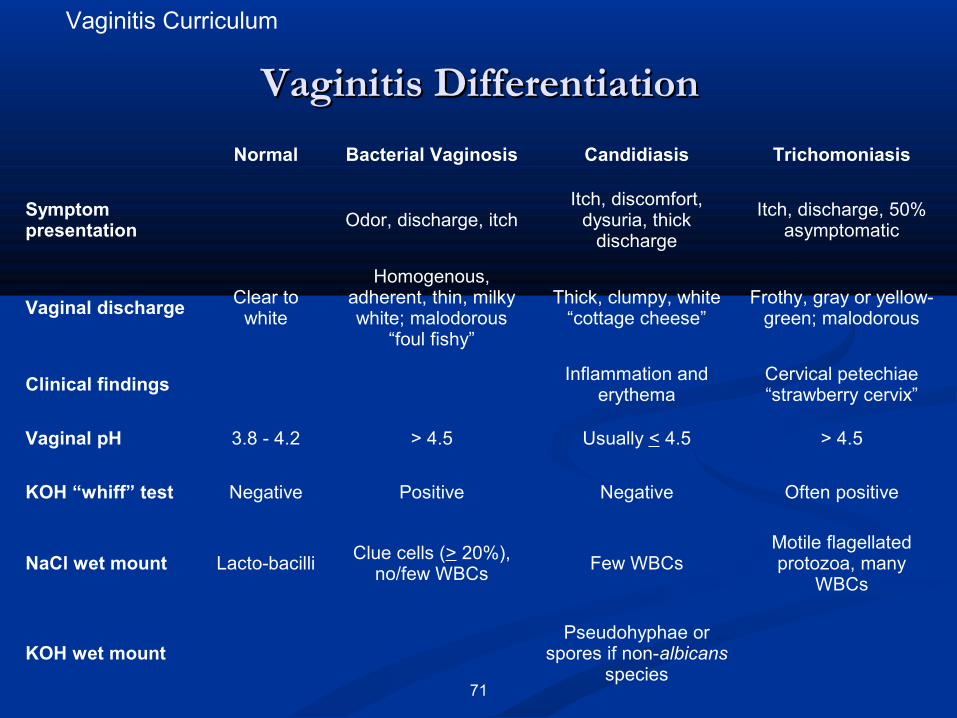
Vaginitis DifferentiationVaginitis Differentiation
Vaginitis Curriculum
Normal Bacterial Vaginosis Candidiasis Trichomoniasis
Symptom presentation Odor, discharge, itch
Itch, discomfort, dysuria, thick
discharge
Itch, discharge, 50% asymptomatic
Vaginal dischargeClear to
white
Homogenous, adherent, thin, milky white; malodorous
“foul fishy”
Thick, clumpy, white “cottage cheese”
Frothy, gray or yellow-green; malodorous
Clinical findingsInflammation and
erythemaCervical petechiae “strawberry cervix”
Vaginal pH 3.8 - 4.2 > 4.5 Usually < 4.5 > 4.5
KOH “whiff” test Negative Positive Negative Often positive
NaCl wet mount Lacto-bacilli Clue cells (> 20%), no/few WBCs
Few WBCsMotile flagellated protozoa, many
WBCs
KOH wet mountPseudohyphae or
spores if non-albicans species
72
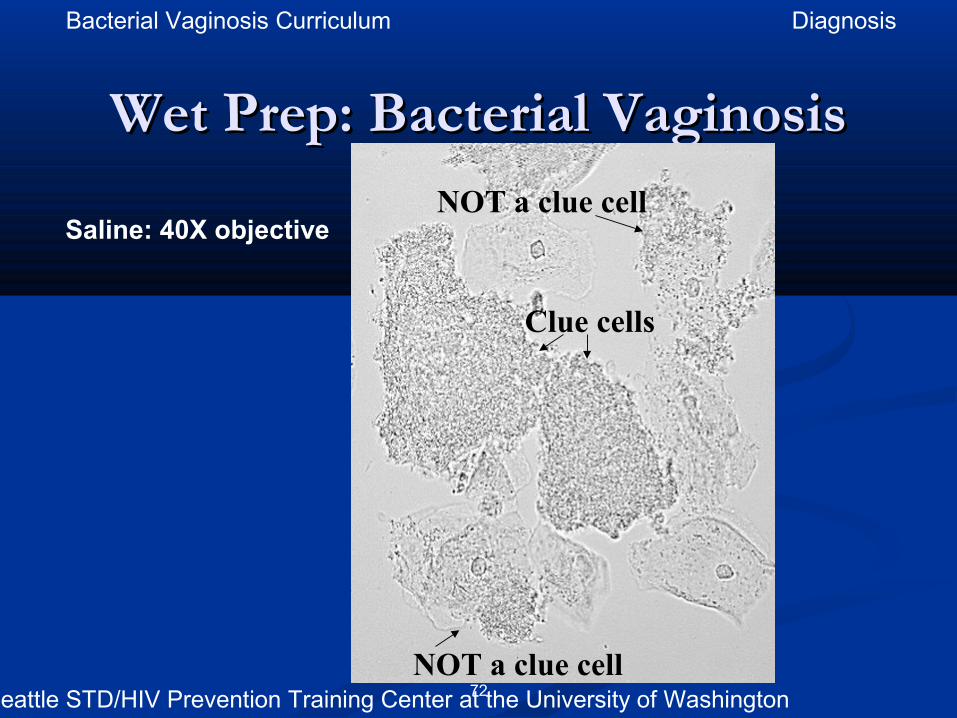
Wet Prep: Bacterial VaginosisWet Prep: Bacterial Vaginosis
Saline: 40X objectiveNOT a clue cell
Clue cells
NOT a clue cellSource: Seattle STD/HIV Prevention Training Center at the University of Washington
Bacterial Vaginosis Curriculum Diagnosis
73
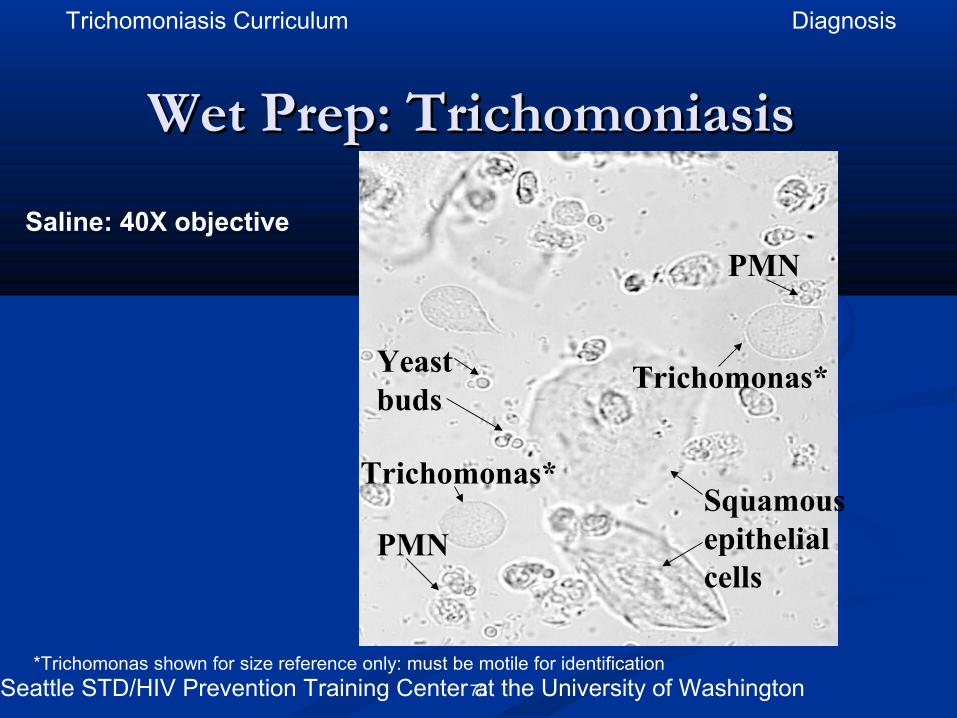
Wet Prep: Trichomoniasis Wet Prep: Trichomoniasis
Saline: 40X objective
*Trichomonas shown for size reference only: must be motile for identification
PMN
Trichomonas*
Squamous epithelial cells
PMN
Trichomonas*
Yeast buds
Source: Seattle STD/HIV Prevention Training Center at the University of Washington
Trichomoniasis Curriculum Diagnosis

















