16
1 1 Dr. Maoyi Tian on behalf of SimCard working group Simplified Cardiovascular Management (SimCard) Study in Tibet, China and Haryana, India

11
Dr. Maoyi Tian on behalf of SimCard working group
Simplified Cardiovascular Management (SimCard) Study in Tibet, China and Haryana, India
22
24million
80% LMIC
40%
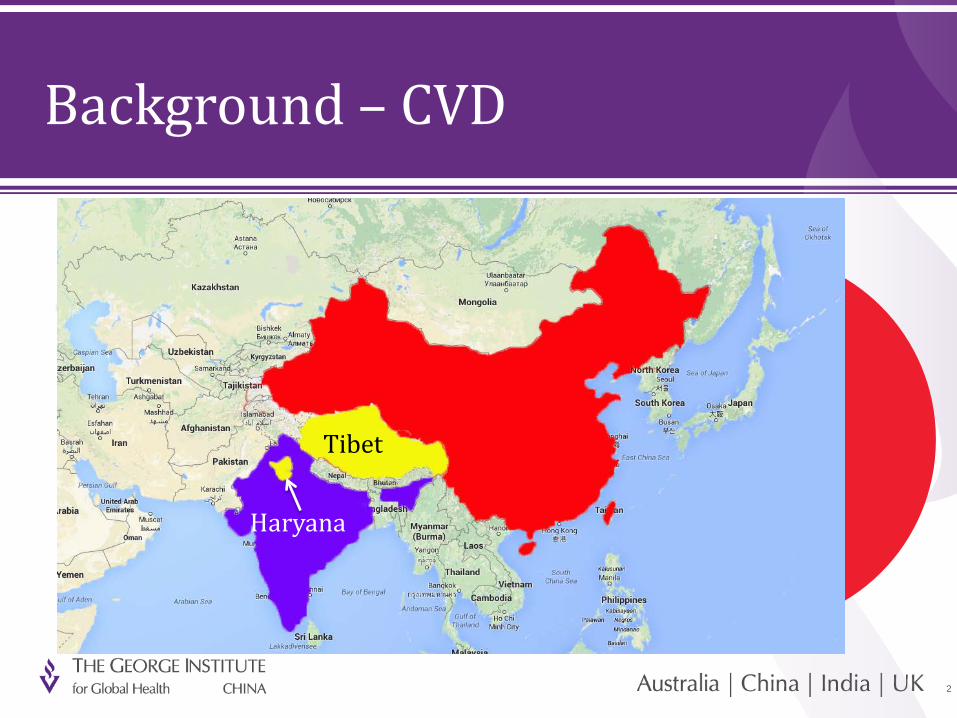
Background – CVD
17millionChina
IndiaTibet
Haryana

33
• To develop,• Pilot-test and • Evaluate the feasibility and effectiveness of a
SIMPLIFIED, but GUIDELINE-BASED cardiovascular disease management program delivered by the COMMUNITY HEALTH WORKERS (CHWs) in resource-constrained settings in Tibet, China and Haryana, India
Aim

44
Inclusion criteria
• Age ≥ 40
• Resident in the selected village
Screening
Method – subjects
Single-blinded cluster randomized controlled trial (47 clusters)
Exclusion criteria
• Bed-ridden • Unable to stay >8 months in a year
• Life-threatening disease • CVD related complications that can’t be managed

55
Screening
Non CVDHigh-risk
CVD High-risk Baseline
Usual Care(24 clusters)
1-year Intervention(23 clusters)
Follow-up
Method – design
CVD high-riskMeeting any one of the following conditions:
• History of diabetes
• History of stroke
• History of coronary heart disease
• Both SBP ≥ 160mmHg at two different time points in the same day during the survey

66
Salt Reduction
SmokingCessation
BP lowering
agentAspirin
2 Lifestyle Modifications
2 Drug Prescriptions
Electronic Decision Support System
(EDSS)
Method – intervention

77
Method – outcome
• Primary outcome:The binary outcome of anti-hypertensive medication use of all high-risk
individuals. The significance test is for the net difference in the proportion of anti-hypertensive medication use between the groups.
• Secondary outcomes:• The binary outcome of aspirin use of all high-risk individuals;• The difference in pre-and-post mean SBP of high-risk individuals. • Others
• Outcome evaluation:• Baseline and post-intervention follow-up survey• Identical standardized instruments for both surveys

88
Method – statistical analysis
• Power (>90%)• Primary outcome: assuming 20% in control group, detect a 10% difference ,
ICC=0.02• Secondary outcome: assuming SD of the change in SBP =15mmHg, detect a
3mmHg difference, ICC=0.02• Adequate power for sub-group analysis by country
• Method• Intent-to-treat using last observation carried forward• Analysis accounts for cluster effect and repeated measurements• Mixed models were used – logistic model (binary), linear model (continuous)

99
Enrollment
Allocation
Follow-up
Analysis
Result – flow chart
52 villages (China: 30, India: 32)
5 villages were excluded
47 villages were recruited. 2,086 high-risks were identified (China: 1,036, India: 1,050) as high-risk.
Intervention Group1,095 high-risks from 23 villages
(China: 557, India: 538)
Control Group991 high-risks from 24 villages
(China: 479, India: 512)
962 high-risks from 23 villages (China: 478, India: 484)
866 high-risks from 24 villages (China: 431, India: 435)
IIT: 1,095 were analyzed. IIT: 991 were analyzed.

1010
Result – baseline characteristics
Characteristics (Mean, SD or %)Total
Intervention Control
Age (years) 59.7, 11.7 60.4, 11.8
Female (%) 65.4 66.8
Illiterate (%) 59.3 61.9
Body mass index (kg/m2) 23.6, 4.2 24.0, 4.4
Current smoker (%) 36.7 37.5
Coronary heart disease (%) 39.5 31.9
Stroke (%) 10.4 9.9
Diabetes (%) 13.4 9.8
Characteristics (Mean, SD or %)China
Intervention Control
Age (years) 59.5, 11.6 59.3, 11.3
Female (%) 72.0 70.8
Illiterate (%) 62.0 63.7
Body mass index (kg/m2) 23.0, 3.5 23.4, 3.8
Current smoker (%) 37.5 36.5
Coronary heart disease (%) 50.1 53.0
Stroke (%) 6.8 9.4
Diabetes (%) 2.9 1.9
Characteristics (Mean, SD or %)India
Intervention Control
Age (years) 59.9, 11.8 61.5, 12.1
Female (%) 58.6 63.1
Illiterate (%) 56.4 60.3
Body mass index (kg/m2) 24.1, 4.7 24.5, 4.8
Current smoker (%) 35.9 38.7
Coronary heart disease (%) 28.4 12.1
Stroke (%) 14.1 10.4
Diabetes (%) 24.3 17.2
Characteristics (Mean, SD or %)India
Intervention Control
Age (years) 59.9, 11.8 61.5, 12.1
Female (%) 58.6 63.1
Illiterate (%) 56.4 60.3
Body mass index (kg/m2) 24.1, 4.7 24.5, 4.8
Current smoker (%) 35.9 38.7
Coronary heart disease (%) 28.4 12.1
Stroke (%) 14.1 10.4
Diabetes (%) 24.3 17.2

1111
Result – primary outcome
Total China India

1212
Result – secondary outcomes
Total Aspirin (%)
SBP (mmHg)
Current smoker (%)
Awareness of high salt harm (%)
InterventionPre 6.0 161.3, 29.6 36.7 46.9
Post 18.8 151.0, 27.0 37.7 59.6
ControlPre 4.7 161.4, 27.8 37.5 36.8
Post 2.8 153.2, 27.7 36.7 55.8
Net 11.7 -2.1 1.8 -6.3
P value <0.001 0.03 0.46 0.08
Total Aspirin (%)
SBP (mmHg)
Current smoker (%)
Awareness of high salt harm (%)
InterventionPre 6.0 161.3, 29.6 36.7 46.9
Post 18.8 151.0, 27.0 37.7 59.6
ControlPre 4.7 161.4, 27.8 37.5 36.8
Post 2.8 153.2, 27.7 36.7 55.8
Net 11.7 -2.1 1.8 -6.3
P value <0.001 0.03 0.46 0.08
China Aspirin (%)
SBP (mmHg)
Current smoker (%)
Awareness of high salt harm (%)
InterventionPre 7.0 166.2, 30.8 37.5 64.1
Post 23.7 155.3, 27.8 38.8 87.1
ControlPre 5.6 164.4, 28.8 36.2 52.9
Post 1.9 157.3, 29.2 36.1 76.2
Net 20.4 -3.8 1.4 -0.3
P value <0.001 0.006 0.65 0.19
China Aspirin (%)
SBP (mmHg)
Current smoker (%)
Awareness of high salt harm (%)
InterventionPre 7.0 166.2, 30.8 37.5 64.1
Post 23.7 155.3, 27.8 38.8 87.1
ControlPre 5.6 164.4, 28.8 36.2 52.9
Post 1.9 157.3, 29.2 36.1 76.2
Net 20.4 -3.8 1.4 -0.3
P value <0.001 0.006 0.65 0.19
India Aspirin (%)
SBP (mmHg)
Current smoker (%)
Awareness of high salt harm (%)
InterventionPre 5.0 156.2, 27.4 35.9 29.1
Post 13.8 146.6, 25.3 36.5 31.1
ControlPre 3.7 158.5, 26.5 38.7 21.4
Post 3.7 149.5, 25.7 37.2 36.7
Net 8.8 -0.5 2.1 -13.3
P value <0.001 0.71 0.22 <0.001
India Aspirin (%)
SBP (mmHg)
Current smoker (%)
Awareness of high salt harm (%)
InterventionPre 5.0 156.2, 27.4 35.9 29.1
Post 13.8 146.6, 25.3 36.5 31.1
ControlPre 3.7 158.5, 26.5 38.7 21.4
Post 3.7 149.5, 25.7 37.2 36.7
Net 8.8 -0.5 2.1 -13.3
P value <0.001 0.71 0.22 <0.001

1313
Result - summary
• Effectively changed CHWs and patients' behaviors in increasing
uptake of evidence-based medicine (anti-hypertensive medication
and aspirin)
• No significant changes in lifestyle factors
• Reduced systolic blood pressure by 2.1 mmHg

1414
Strength/Limitation
• Strength• Strong local government support• Adaptive intervention design in two countries• Active engagement of the CHWs• The use of EDSS
• Limitation• Generalizability• Unable to distinguish the effectiveness of different
intervention component

1515
Conclusion
Simplified evidence-based culturally-appropriate interventions
based on the high-risk approach could improve quality of primary
care and have the potential to reduce disease burden in resource-
constrained settings.

1616
• Collaborators
o Tibet University
o Public Health Foundation of India
o China Mobile Research Institute
o University of Oxford
• Funding source
National Heart, Lung, and Blood Institute (National Institutes of Health)
Acknowledgement
China site:Z Liu, D Dunzhu, X Zhao, H Chen, K ChoR Li, C Li, X Li, J Ji, E Delong, E PetersonY Wu, L Yan
India site:V Ajay, S Hameed, D JindalI Rawal, M Ali, R AmachandA Krishnan, N Tandon, D Prabhakaran

















