26
SINCOPE ED ADENOSINA Michele Brignole Centro Aritmologico, Ospedali del Tigullio, Lavagna

SINCOPE ED ADENOSINA
Michele Brignole
Centro Aritmologico, Ospedali del Tigullio, Lavagna

Explanatory case 1
• Cinzia, 20 yrs, female
• 50 syncopes/last 2 yrs, no prodromes or very short (<5 sec) blurring of
the vision
• normal heart, normal ECG
• negative tilt testing
Explanatory case 2
• Marcello, 50 yrs,male
• 5 syncopes no prodromes or very short (<5 sec) blurring of the vision;
1 car crash
• normal heart, normal ECG
• positive tilt testing, mixed response (no asystole)
“Low-adenosine syncope” - sincope adenosino-sensibile
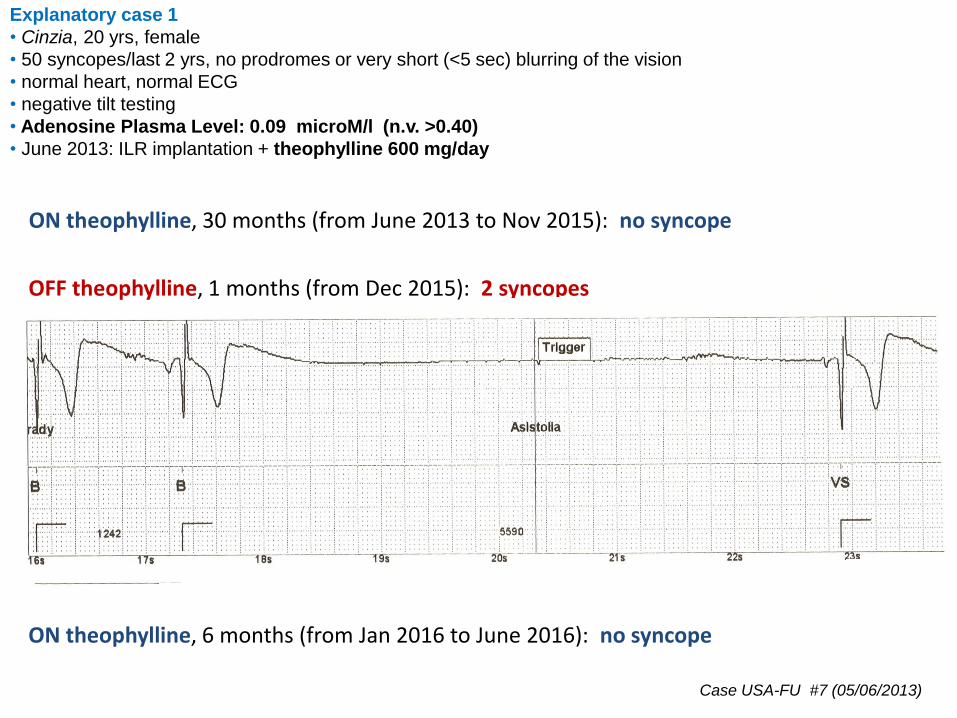
Explanatory case 1
• Cinzia, 20 yrs, female
• 50 syncopes/last 2 yrs, no prodromes or very short (<5 sec) blurring of the vision
• normal heart, normal ECG
• negative tilt testing
• Adenosine Plasma Level: 0.09 microM/l (n.v. >0.40)
• June 2013: ILR implantation + theophylline 600 mg/day
Case USA-FU #7 (05/06/2013)
ON theophylline, 30 months (from June 2013 to Nov 2015): no syncope
OFF theophylline, 1 months (from Dec 2015): 2 syncopes
ON theophylline, 6 months (from Jan 2016 to June 2016): no syncope

Explanatory case 2
• Marcello, 50 yrs,male
• 5 syncopes no prodromes or very short (<5 sec) blurring of the vision; 1 car crash
• normal heart, normal ECG
• positive tilt testing, mixed response (no asystole)
• adenosine plasma level: 0.01 microM/l (n.v. >0.40)
• Sept 2015: ILR implantation
• Feb 1, 2016: 2 syncopes
Case USA-FU #18 (22/09/2015)
30 sec asystole
13 sec asystole
• Sept 2016: ON theophylline 600 mg/d ; no symptoms
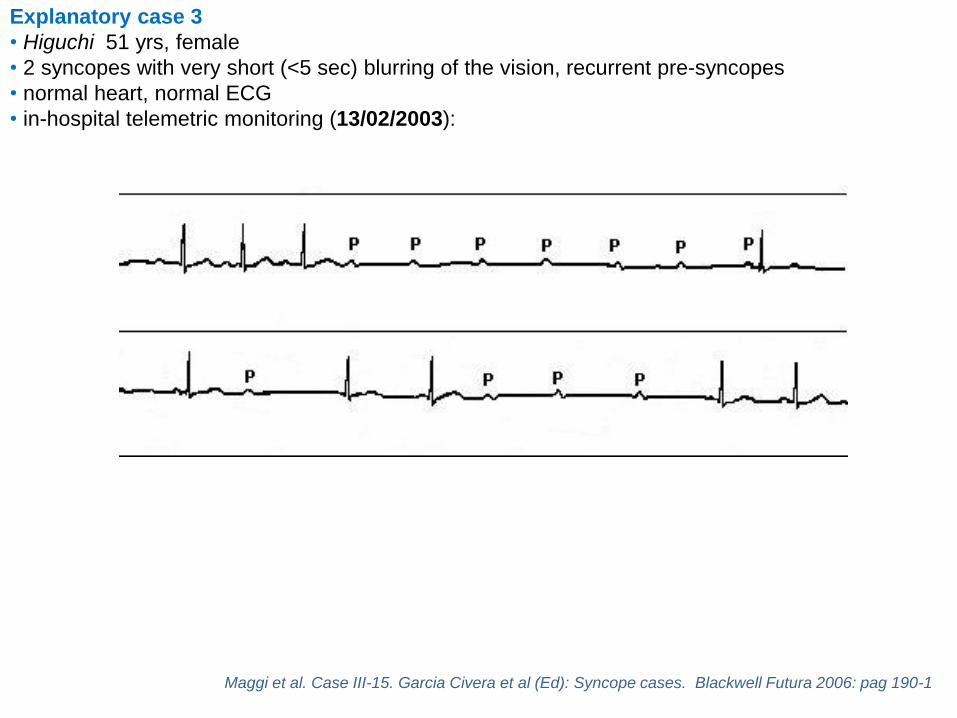
Explanatory case 3
• Higuchi 51 yrs, female
• 2 syncopes with very short (<5 sec) blurring of the vision, recurrent pre-syncopes
• normal heart, normal ECG
• in-hospital telemetric monitoring (13/02/2003):
Maggi et al. Case III-15. Garcia Civera et al (Ed): Syncope cases. Blackwell Futura 2006: pag 190-1

Explanatory case 3
• Higuchi , 51 yrs, female
• 2 syncopes with very short (<5 sec) blurring of the vision, recurrent pre-syncopes
• normal heart, normal ECG
• EP study (15/02/2003): PA: 60 ms; AH: 70 ms; HV: 35 ms; Wenckebach cycle: 370 ms; SNRT:1190 ms ms
• ATP test:
• Ajmaline test: negative
• Theophylline 240 mg i.v + ATP test:
0
100
50
150
mm Hg
HRA
BP
A
V
A
V
Case III-15. Garcia Civera et al (Ed): Syncope cases. Blackwell Futura 2006: pag 190-1
Explanatory case 3
• Higuchi, now 64 yrs
ON theophylline, 13 year (from 2003 to 2016): no syncopeHolter: nocturnal paroxysmal AV block with max pause of 3.5 sec
Follow-up: May 2016
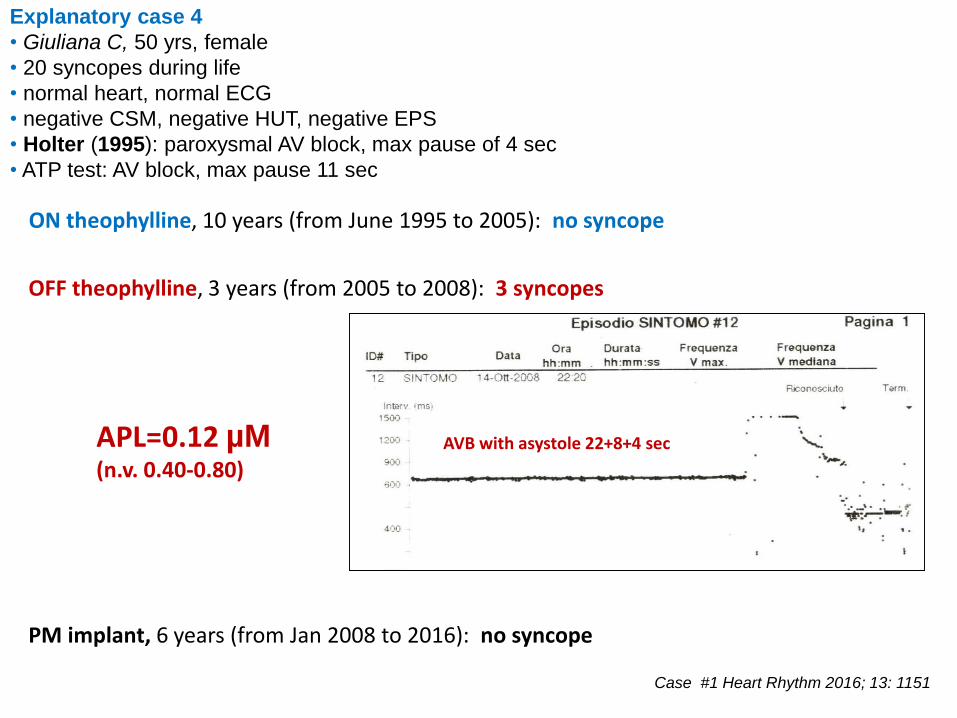
Explanatory case 4
• Giuliana C, 50 yrs, female
• 20 syncopes during life
• normal heart, normal ECG
• negative CSM, negative HUT, negative EPS
• Holter (1995): paroxysmal AV block, max pause of 4 sec
• ATP test: AV block, max pause 11 sec
Case #1 Heart Rhythm 2016; 13: 1151
ON theophylline, 10 years (from June 1995 to 2005): no syncope
OFF theophylline, 3 years (from 2005 to 2008): 3 syncopes
PM implant, 6 years (from Jan 2008 to 2016): no syncope
AVB with asystole 22+8+4 secAPL=0.12 µM(n.v. 0.40-0.80)

Explanatory case 5
• Michele 72 yrs, male
• 2 syncopes w/t prodrome
• normal heart, normal ECG, negative EPS
• negative tilt testing; negative ADO test
• July 2013: ILR implantation
• August 26, 2013:
P P P P PP
P P P P
APL=0.09 µM(n.v. 0.40-0.80)

PP P P P P
PP
Case #2, M, 72 yrs
B) ON theophylline (Jul 29, 2014)
Case #2, M, 72 yrs
PP

C)
PP P P P P
PP
Case #2, M, 72 yrs
OFF theophylline (Dec 31, 2014)

Extended follow-upNumber of pauses >3 s per month
1
8
0
2
1
0 0 0 0
5
0 0
1 1
0 0 0
2
0 0
1 1
0 0 0 0 0 0 0 0 0 0 0
1
Month 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4
Year 2013 Year 2014 Year 2015 Year 2016
No therapy
Theophylline
Case #2, M, 72 yrs
Heart Rhythm 2015 Dec 9 [Epub ahead of print]
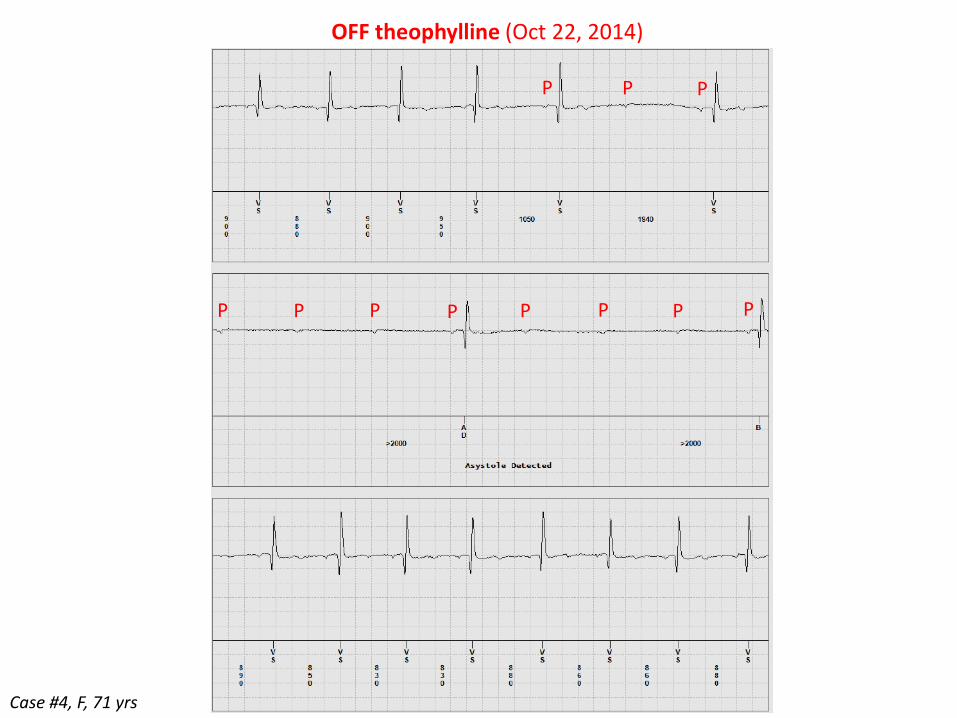
Case #4, F, 71 yrs
OFF theophylline (Oct 22, 2014)
P
P
P P P P PP P
PP
OFF theophylline (Oct 22, 2014)

0
1
2
0
1
4
1
2
6
1
4
5
3
0 0 0 0 0 0 0
Month 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5 6 7
Year 2013 Year 2014 Year 2015
Case #4, F, 71 yrs
Number of pauses >3 s per month
No therapy
Theophylline
Heart Rhythm 2015 Dec 9 [Epub ahead of print]

J Am Coll Cardiol 2013;62:1075–80

APL (µM)
APL µM (median) 0.33 µM 0.25 µM 0.85 µM 0.49 µM
J Am Coll Cardiol 2013;62:1075–80
“Low adenosine” syncope:
syncope w/t prodrome, normal heart & normal ECG

High affinity A1 receptors saturation curve
AV block zone Sinus arrest/bradycardiazone
% saturation
Low APL High APL
100%
50%
0.7 (Kd)
Mostly freereceptors
Mostly saturatedreceptors
0.10.01 2 10
APL (M)J Am Coll Cardiol 2011; 58: 167–73
Pathophysiological observations
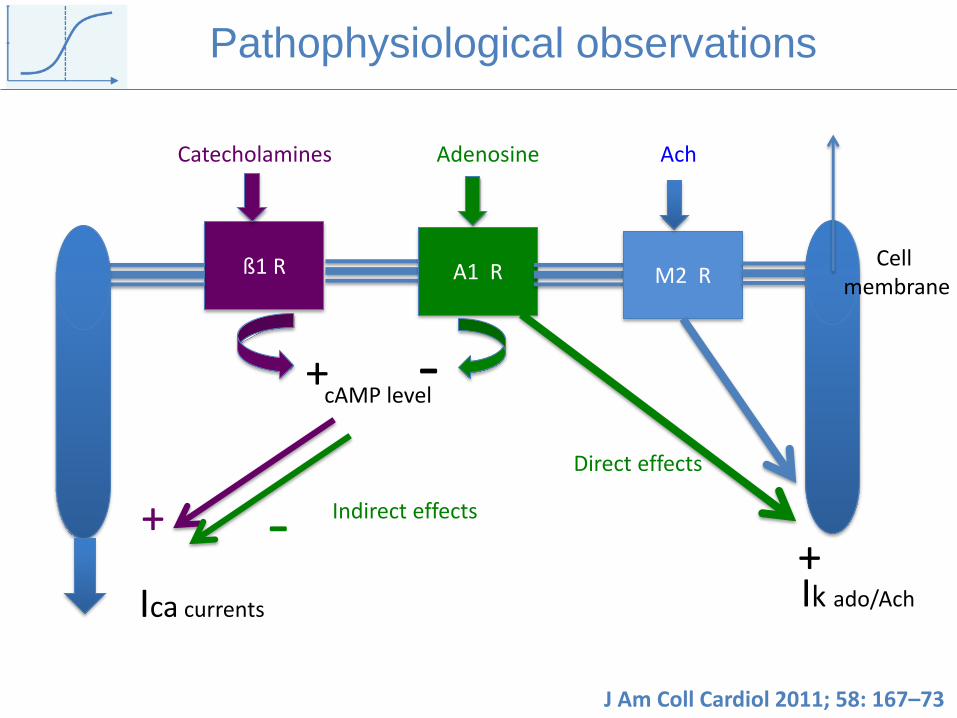
ß1 R A1 R M2 R
Catecholamines Adenosine Ach
+ -cAMP level
Ica currents
+ -+Ik ado/Ach
Direct effects
Indirect effects
Pathophysiological observations
J Am Coll Cardiol 2011; 58: 167–73
Cellmembrane

Syncopal faint
Cardiac intrinsic
cause
Neurally-mediated
(reflex) cause
Low
Adenosine
(asystole)
Normal
Adenosine
High
Adenosine
(hypotension)
Adenosine phenotypes
and neurally-mediated syncope
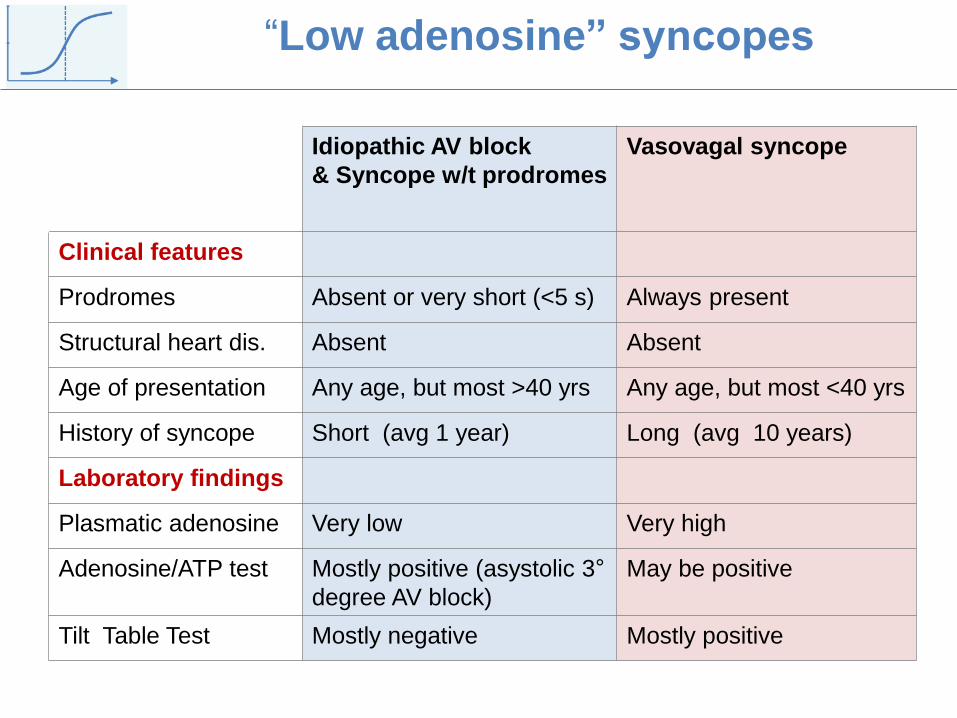
“Low adenosine” syncopes
Idiopathic AV block
& Syncope w/t prodromes
Vasovagal syncope
Clinical features
Prodromes Absent or very short (<5 s) Always present
Structural heart dis. Absent Absent
Age of presentation Any age, but most >40 yrs Any age, but most <40 yrs
History of syncope Short (avg 1 year) Long (avg 10 years)
Laboratory findings
Plasmatic adenosine Very low Very high
Adenosine/ATP test Mostly positive (asystolic 3°
degree AV block)
May be positive
Tilt Table Test Mostly negative Mostly positive

66%5%
31%No or mild
rhythm variations
Asystole
(avg 11±5 s)Tachycardia
2-year diagnostic yield of
Implantable Loop Recorder (ILR)
in 58 patients with
unexplained syncope,
no prodrome and normal heart
NND=number needed for diagnosis
32%
54%
NND = 1.8NND = 3.1
Mechanism of syncope
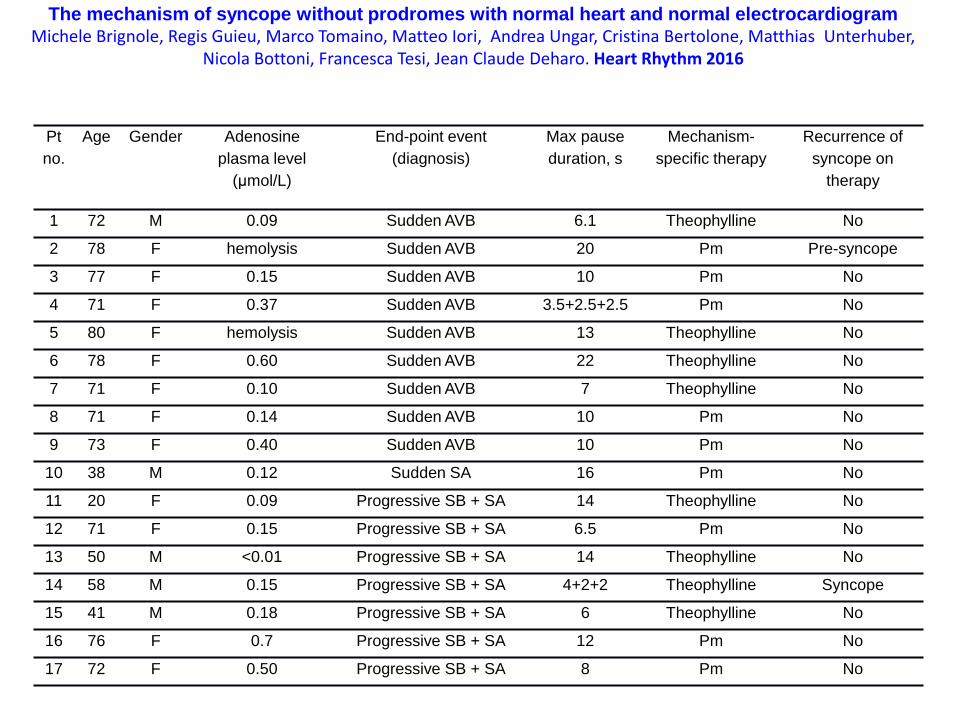
The mechanism of syncope without prodromes with normal heart and normal electrocardiogramMichele Brignole, Regis Guieu, Marco Tomaino, Matteo Iori, Andrea Ungar, Cristina Bertolone, Matthias Unterhuber,
Nicola Bottoni, Francesca Tesi, Jean Claude Deharo. Heart Rhythm 2016
Pt
no.
Age Gender Adenosine
plasma level
(μmol/L)
End-point event
(diagnosis)
Max pause
duration, s
Mechanism-
specific therapy
Recurrence of
syncope on
therapy
1 72 M 0.09 Sudden AVB 6.1 Theophylline No
2 78 F hemolysis Sudden AVB 20 Pm Pre-syncope
3 77 F 0.15 Sudden AVB 10 Pm No
4 71 F 0.37 Sudden AVB 3.5+2.5+2.5 Pm No
5 80 F hemolysis Sudden AVB 13 Theophylline No
6 78 F 0.60 Sudden AVB 22 Theophylline No
7 71 F 0.10 Sudden AVB 7 Theophylline No
8 71 F 0.14 Sudden AVB 10 Pm No
9 73 F 0.40 Sudden AVB 10 Pm No
10 38 M 0.12 Sudden SA 16 Pm No
11 20 F 0.09 Progressive SB + SA 14 Theophylline No
12 71 F 0.15 Progressive SB + SA 6.5 Pm No
13 50 M <0.01 Progressive SB + SA 14 Theophylline No
14 58 M 0.15 Progressive SB + SA 4+2+2 Theophylline Syncope
15 41 M 0.18 Progressive SB + SA 6 Theophylline No
16 76 F 0.7 Progressive SB + SA 12 Pm No
17 72 F 0.50 Progressive SB + SA 8 Pm No
The mechanism of syncope without prodromes with normal heart and normal electrocardiogramMichele Brignole, Regis Guieu, Marco Tomaino, Matteo Iori, Andrea Ungar, Cristina Bertolone, Matthias Unterhuber,
Nicola Bottoni, Francesca Tesi, Jean Claude Deharo. Heart Rhythm 2016

Prodrome (*)
No prodrome
* Prodrome group: reflex syncope treated with pacemaker (age/sex matched from ISSUE trial)
7%
25%
Brignole et al. Heart Rhythm 2016

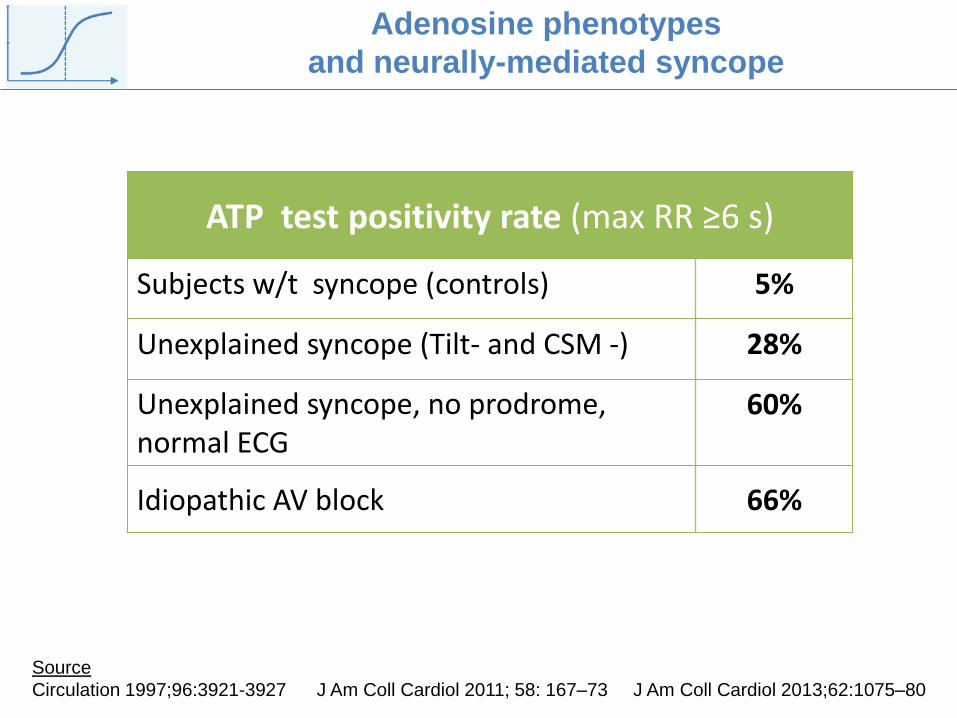
ATP test positivity rate (max RR ≥6 s)
Subjects w/t syncope (controls) 5%
Unexplained syncope (Tilt- and CSM -) 28%
Unexplained syncope, no prodrome,normal ECG
60%
Idiopathic AV block 66%
Source
Circulation 1997;96:3921-3927 J Am Coll Cardiol 2011; 58: 167–73 J Am Coll Cardiol 2013;62:1075–80
Adenosine phenotypes
and neurally-mediated syncope

Adenosine phenotypes
and neurally-mediated syncope
24%35%
73%
Low adenosine(No prodr + CSS)
Normal adenosine(Situational)
High adenosine(VVS)
Tilt test positivity rate
Guieu et al. JACC 2015: 66: 204

















