40
ANNUAL REPORT 2010 - 2011 SMHC: At the Heart of our

A N N U A L R E P O R T 2 0 1 0 - 2 0 1 1
SMHC: At the Heart of our

Our missionSt. Mary’s Hospital Center is a university affiliated community hospital which serves a multicultu-ral population. We seek to provide the highest level of safe patient and family-focused care.
Our valuesWe believe in:• Respectfordignityoflife;• Supportanddevelopmentofourpeople;• Integrityandcompassion.
2

The2010-2011St.Mary’sHospitalCenter(SMHC)AnnualReportseekstoprovideasnapshotofourvibrantandculturallydiversecommunity.OurcommunityextendsfarbeyondthebordersofourCote-des-Neigesneighbourhoodandlocalcommunitymembers,totheMontrealHealthNetwork,tothefarreachesofQuebec,andwiderstilltotheinternationalcommunitywhereSMHCalsodevotesourskillstohelpothercommunitiestobehealthyandthrive.Ourcommunitytranscendstheboundariesofourwalls,embracingourdifferencesandcelebratingourcommonalities.
Overtheyears,SMHChasexpandedanddiversified,alwaysgainingmomentumbutneverneglectingourstrongcommunityroots.
SMHC: At the Heart of our
Community
3

It is our pleasure to present to you the annual report ofSt.Mary’sHospitalCenterforthefiscalyear2010-2011.
AsoneofMontreal’sfinesthospitals,St.Mary’shasaproudheritage of serving the community for over 85 years as anacute care teaching hospital. It provides numerous highlyspecializedservicessuchasrenaldialysis,oncology,geriatricassessment and psycho-geriatrics, nuclear medicine, CTscan,aswellasMRIexams.Itisoneofthelargestbirthingcentres inMontreal.OurEmergencyDepartmenthasbeenrecognizedasoneofthemostefficientinthecity.St.Mary’sisalsooneoftwodesignatedcataractsurgerysitesinMontreal.Weremainoneofthebusiesthospitalsforcataractsurgery,hipandkneereplacement,daysurgeryandinpatientsurgery.We are responsible for the training of a large cohort ofundergraduateandpost-graduatestudentsinMedicineandthealliedhealthdisciplines.
InApril2010,St.Mary’sappointedDr.SusanLawasVice-President of Academic Affairs. This new position wascreated to expand and strengthen the hospital’s educationand research activities as a designated university-affiliatedhospital. After a thorough analysis and wide consultations,theBoardofDirectorsapproved thecreationofa researchcentre. The Department of Clinical Epidemiology andCommunityStudieswasabolishedand the research teamsandfunctionsofthatdepartmentwereincorporatedintotheresearch centre as part of Academic Affairs, as well as allteachingcomponents.Thedirectoratehasawelldefinedplanto develop health services research and further strengthenourroleinteaching.
An Academic Affairs Committee of the Board was alsoestablished for oversight and advisory roles regardingresearchandteaching.
Weareproudtoannouncethatasearchcommitteehasbeen
Message from the President and the Director General & CEO
4
setupforaMcGillChair inCommunityCancerCarewithaprimaryfocusonbreastcancer.ItwillbethesecondMcGillChairtobebasedatSt.Mary’s.
The term of office of the Board members was extendedto 2011, as a new legislation for board governance waspresentedtotheNationalAssembly.ManyrepresentationsbyvariousgroupsweremadeintheParliamentaryCommission.The hospital’s position was well represented by theAssociation québécoise des établissements de santé et de services sociaux (AQESSS)andtheConferenceofrectorsandprincipals of Quebec universities (CREPUQ) to make surethat there would be appropriate community and universityrepresentations in order to meet our mission with a strongBoardofDirectors.
In 2010-2011, threemembers resigned from theBoard ofDirectors.WewouldliketosincerelythankMrs.IdaGraniero,Maureen Simonds and Dr. Marc Cotran who diligentlyserved on the Center Board, respectively as representativeofNon-clinicalpersonnel,UniversityandResidents,fortheircommitmentandcontribution.
St.Mary’sisresponsibleforthetrainingofalargecohortofundergraduateandpost-graduatestudentsinMedicineandthealliedhealthdisciplines.

This year again, the financial situation of thehealthcare systemwas at the forefront.Bill 100waspassed at theNationalAssembly,askingthehealthcareinstitutionstocut10%oftheiradministrativecosts,including25%incostsforeducation,publicityandtravel,upto2013-2014.ForSt.Mary’sthe10%administrativecutamountsto$850,000.Thefollowingthreeelementsmustbeconsideredtoperformthecuts:1)replacing1outof2employeeswhowillberetiring–theMinistrydecidedtoimposecutsof2.4%ofthemasse salariale ofadministrationpersonnelforallinstitutions.ForSt.Mary’sthismeansonefulltimeequivalentforthisyear;2)reductionof25%ineducation,publicityandtravel–thisamountsto$24,000.Theproportionis relativelyhighas it representsonequarterofourexpenses ineducation;3)as for theothermeasures,wehavesomeflexibilityaslongasitdoesnotaffecttheservicestothepopulation.
AfternegotiationswiththeMontrealHealthandSocialServicesAgency,weendedthefiscalyearwithanauthorizeddeficitof$1.85million.St.Mary’sagreedtorespectthetargeteddeficitforthenextthreeyears(until2013-2014).Thiscommitmentismadeinthe lightof thecurrentvolumeofactivitiesanddoesnot take intoaccountunpredictableevents.Moreover, thiscommitmentwillbeattainableonlyiftheAgencygrantstoSt.Mary’sthesamefinancialsupportasitdidinthepast.Weareproud to tell you that theMinistry in itsyearlyevaluationof theefficiencyofhealthcare institutionsshowed thatSt.Mary’sHospitalCenterwasbyfarthemostperformantandunderfinancedhospitalontheislandofMontrealandoneofthebestintheprovince.
FollowingthevisitfromAccreditationCanadaintheFallof2009,wereceivedthefinalreportconfirmingthatwehadmetallrequirements,asindicatedintheir15recommendations.
The Collège des médecins du QuébecmadeatargetedinspectionvisitinMay2010.TheobjectiveoftheProfessionalInspectionCommitteeistoimprovethequalityofmedicalcareprovidedtopatients.TheCollègerequestedthatactionsbetakentoensurebetterandmoretimelychartinginUrologyandGeneralSurgery,aimingforqualityimprovement.TheBoardofDirectorsmandatedtheComité de vigilance et de la qualitétofollowuponthetimelyimplementationoftherecommendationsandtoreportbacktotheBoardofDirectors.
5

Following the investigation that took place last yearconcerningthehighlypublicizedreceptor testing forbreastcancer, St.Mary’s had shown outstanding compliance andresults.Wehavebeeninvitedtosubmitourcandidacytobedesignatedasaregionalcentreforbreastcancertesting.
TheFamilyMedicineresidencyprogramremainsoneofthelargestandmostsoughtafterinCanada.Assuch,allplaceswerefilledafterfirstiterationin2010.Wealsoreceivedtheconfirmation for the financing of the International MedicalGraduate program and we are planning to have the firstcohortinMay2011,assomeconstructionworkisrequiredtoaccommodatethisnewprogram.
AcertificationvisitbytheBabyFriendlyHospitalInitiativetookplaceatSt.Mary’sonMarch29,30and31.ThisinitiativewaslaunchedbyUnicefandtheWorldHealthOrganizationin1991.Itisaworldwideinitiativeaimingtopromotebreastfeedinganditgivesinternationalrecognitiontoinstitutionsthatarecertified.Tobe recognized, the institutionmustprotect,promoteandsupport breastfeeding. The verbal report at the end of thevisitwasextremelypositiveandweareconfidentthatwewillreceivewrittenconfirmationofthisprestigiousdesignation.
TheconstructionoftwoadditionalfloorsovertheWestwingisournumberonepriority.ItwasapprovedbytheMontreal
HealthandSocialServicesAgencyinFebruary2011andtheprojectisnowunderstudyattheHealthandSocialServicesMinistry level. Information sessions with the Hospital’sneighbours tookplace inMarchand theywereverymuchappreciated. The purpose of these two additional floors isto provide space for private and semi-private rooms, thusreducingtheriskofnosocomialinfectionsandimprovingthequalityofworklifeforourhardworkingstaff.Theywillalsoprovide facilities that meet the requirements for increasedteachingactivitiesasauniversity-affiliatedhospitalcentre.
The nosocomial infection situation was followed closelythroughout the year.Regular reports are given to theBoardof Directors concerning C-difficile, MRSA and VRE. A largeamountofresourceshavebeenusedtocontainthespreadingofnosocomialinfections.Alsoanumberofin-serviceeducationsessionshavebeengiventothehospitalstaffthroughouttheyear.
St.Mary’shasalwaysworkedhardat improving itsphysicalplant to answer to the increasing demand for services invariousareasofthehospital.Amongthecurrentandupcomingprojectsare:
• With its constant high volume of tests and theprocessingofsamplesfromotherinstitutions,theBloodProcurementCentrewasupgraded tobetter serveourpatientsandourcommunity.
• AplanwasdepositedtoexpandourEmergencyasthenumberofambulanceshassteadilyincreasedtoreachan average of 20 per day. The Ministry approved theproposed expansion project which will increase theEmergencycapacityfrom15to22stretchers.
• RenovationsofthefrontlobbyareunderwayandshouldbecompletedduringtheSummer.
6
St.Mary’sHospitalCenterwillcontinuetostriveforexcellencetofurtherimprovethepatientcareandqualityofservicesitprovidestoourcommunity.
7
Awards• McGillPsychiatryResidentAssociation–Dr.MichelÉlie,
Best teacher of the year and Dr. Santokh Singh, Bestclinicalsupervisoroftheyear.
• College of Family Physicians of Canada – Dr. MarcCotran, former Board member, has been granted theCFPCFamilyResidentLeadershipAward.
• Mrs.ClaireMullins-Kruyt,Boardmember,receivedtheAwardforoutstandingvolunteeroftheyearonNationalPhilantropyDay.
• Mrs.MarieIskandar,ChiefofthePharmacyDepartment,was named the “Arab Woman of Quebec for the year2010–Healthcare” forherexceptionalcontribution tohealthimprovementinQuebec.
St.Mary’sHospitalCenterwillcontinuetostriveforexcellencetofurtherimprovethepatientcareandqualityofservicesitprovidestoourcommunity.
We would like to acknowledge the continued support andcommitment of our benefactors, volunteers and boards(HospitalCenter,Foundation,GovernorsandAuxiliary).Wealsowouldliketounderlinethecontributionofouremployeesand physicians towards the high standards of quality andcompassionatepatientcare.
Respectfullysubmitted,
MarcW.TrottierPresident
ArvindK.Joshi,M.D.DirectorGeneral&CEO

8
Portrait of the
SMHC CommunityFirst established inMay1924 in theShaughnessyHouse,in downtown Montreal (now the Canadian Centre forArchitecture), St. Mary’s Hospital originated in the Irishcommunity of Montreal. At that time, the Irish Catholichospitalhad45beds.InNovember1934,St.Mary’sHospitalmovedtoLacombeStreet.Duringthisperiod,itwasthemostmodernhospitalinthecity.
AffiliatedwithMcGillUniversity, St.Mary’sHospitalCenter(SMHC)nowhas 271 beds. It is a communityhospital serving a multiculturalpopulation and which seeks toprovide the highest level of safepatient and family focused care.
SMHCisanintegralpartoftheRéseau universitaire intégré de santé (RUIS)McGill.
Today, SMHC is located in the heart of Montreal, in theboroughofCote-des-Neiges-Notre-Dame-de-Grace.Itservesacommunitylocatedintheterritorycoveredbytwohealthandsocialservicescentres:theCentres de santé et de services sociaux (CSSS)CavendishandCSSSdelaMontagne.Withits 338 696 inhabitants, this territory is one of the mostpopulousofthecityandrepresents18.3%ofitspopulationanditisalsooneofthemostculturallydiverse.Nearlyoneoutof two (43.2%)of its residents isbornoutsideCanadaandjustoveroneoutoften(12.3%)isnewlyarrivedinthecountry. It has the largestFilipino,ChineseandRomaniancommunitiesoftheislandofMontreal.
The CSSS Cavendish and de la Montagne territory has asignificantlyhighernumberof familieswithchildren(64%)than all 12 CSSS territories in the Montreal area (62.7%)combined.Incontrast,peopleaged65andoverlivingalonerepresentmorethantheMontrealaverage.
FromourhumblebeginningsasthefirstIrishCatholichospitalontheislandtotheincrediblydiversefacilitywearetoday,SMHChasgrownwithgenerationsofourcommunity.TheSt.Mary’steamtrulyunderstandswhatitmeanstobeattheheartofacommunity,andisdevotedtoservingourcommunitywithgreatpassionandrespect.

Although 59% of people living in the territory are fromEnglish or French mother tongue, English remains thelanguage used commonly in everyday life. Nearly one inthree(26.5%)stillspeaksalanguageotherthanEnglishorFrenchathome.
The CSSS Cavendish and de la Montagne territory has ahighconcentrationofuniversity graduates. If 44.8%of thepopulationaged25andoverhaveauniversitydegree, thisaverageis28.6%throughouttheMontrealarea.Theaverage
9
incomeaftertaxofthepopulationaged15yearsandoverisalsohigher,reaching$31,943versus$26,793forthewholeislandofMontreal.
Besides manufacturing, men are working mainly inprofessional, scientific or technical jobs, while the femalepopulationismainlyspecializedinhealthcareandeducation.These concentrations are explained by the proximity toseveral hospitals, the Université de Montréal and severalothereducationalinstitutions.

2,5 5
kilomètres0
SMHC serves a community located in the Centres de santé et de services sociaux (CSSS) Cavendish and CSSS de la Montagne. With its 338 696 inhabitants, this territory is one of the most populous of the city and represents 18.3% of its population
10
FromourhumblebeginningsasthefirstIrishCatholichospitalontheislandtotheincrediblydiversefacilitywearetoday,SMHChasgrownwithgenerationsofourcommunity.TheSt.Mary’steamtrulyunderstandswhat itmeanstobeat theheartofacommunity,andisdevotedtoservingourcommunitywithgreatpassionandrespect.
Sources:Agencedelasantéetdesservicessociaux(2009):PrincipalescaractéristiquesdelapopulationduCSSSCavendish,Directiondelasantépublique,12pages.Agencedelasantéetdesservicessociaux(2009):PrincipalescaractéristiquesdelapopulationduCSSSdelaMontagne,Directiondelasantépublique,12pages.Dr.J.J.Dinan,St.Mary’sHospital–TheEarlyYears,Optimumpublishinginternational,Ottawa1987,111pages.
CSSS de la Montagne
CSSSCavendish
Health & Social Services Centresin MontrealCentres de santéet de services sociaux (CSSS)
1111
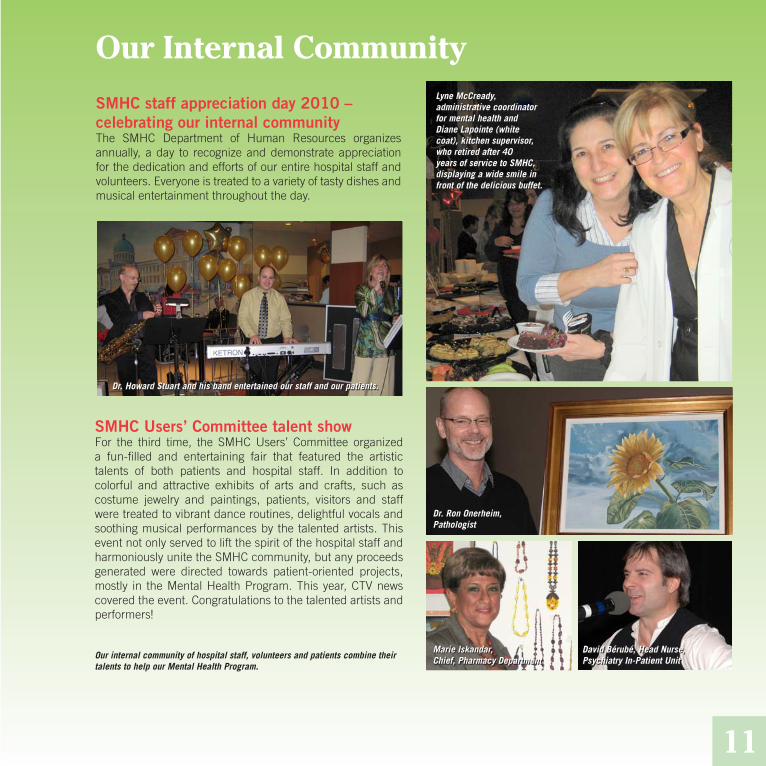
Our Internal CommunityLyne McCready, administrative coordinator for mental health and Diane Lapointe (white coat), kitchen supervisor, who retired after 40 years of service to SMHC, displaying a wide smile in front of the delicious buffet.
SMHC staff appreciation day 2010 – celebrating our internal communityThe SMHC Department of Human Resources organizesannually, aday to recognizeanddemonstrateappreciationforthededicationandeffortsofourentirehospitalstaffandvolunteers.Everyoneistreatedtoavarietyoftastydishesandmusicalentertainmentthroughouttheday.
Dr. Howard Stuart and his band entertained our staff and our patients.
SMHC Users’ Committee talent showFor the third time, the SMHC Users’ Committee organizeda fun-filled and entertaining fair that featured the artistictalents of both patients and hospital staff. In addition tocolorful and attractive exhibits of arts and crafts, such ascostume jewelry and paintings, patients, visitors and staffweretreatedtovibrantdanceroutines,delightfulvocalsandsoothingmusicalperformancesbythetalentedartists.ThiseventnotonlyservedtoliftthespiritofthehospitalstaffandharmoniouslyunitetheSMHCcommunity,butanyproceedsgenerated were directed towards patient-oriented projects,mostly in theMentalHealthProgram.Thisyear,CTVnewscoveredtheevent.Congratulationstothetalentedartistsandperformers!
Our internal community of hospital staff, volunteers and patients combine their talents to help our Mental Health Program.
Dr. Ron Onerheim, Pathologist
Marie Iskandar,Chief, Pharmacy Department
David Bérubé, Head Nurse,Psychiatry In-Patient Unit

SMHCcontinuesitsgreeninitiativewiththeAllégoprogramSt. Mary’s Hospital Center is constantly looking for waysto improve the hospital environment for its patients andcommunity,staff,physiciansandvolunteers.Afterreceivingthe EcoLogo Environmental Stewardship Award, the firsthealthcare facility in Canada to receive this recognition forusing environmentally friendly cleaning products, we haveembarkedonyetanothergreeninitiative:theAllégoprogram.This program, initiated by the Agence métropolitaine de transport (AMT), aims to promote the use of sustainablemodesoftransportation(publictransit,activetransportationlikebikingorwalking,carpooling,etc.).
The objectives of the Allégo program are to facilitate andimproveaccessibilitytothehospitalforourpatientsandourcommunity, employees and volunteers; to find alternativemeansoftransportationandreducesingleoccupantvehicularuse;toallowSMHCtocontinueitsgreeninitiativebyreducingthegreenhousegasesinourenvironment,andtohelpreducetrafficcongestionaroundSMHC.
Our Local CommunityThegenerousspiritofourSMHCcommunityisalsoseenbyourwillingnesstohelpoutourlocalcommunitybycontributingnonperishablegoodsofallkindstoMulticaf,acommunity-basedfoodresourcescentrelocatedintheheartofourCôte-des-NeigesneighborhoodandbydonatingtotheEntraideCampaigntohelptheneedyacrossQuébec.
12
From left to right: Yves Perreault, Avmor; Carlo DeStefano, Manager of Housekeeping Department; Melissa Peneycad, EcoLogo; Mike Kamel, Director of Materials Management and Support Services.

SMHC celebrates our community at “Côte-des-Neiges en fête”The8theditionofthecommunityevent“Côte-des-Neiges en fête”tookplaceatKentPark.Thiswasanoccasionforeveryonetocelebratetherichcultural,artistic,andsocialdiversityofour community. The event was also a great opportunity tospendanafternoonfilledwithfunandentertainmentforthewhole family. SMHC joined the celebrations by hosting aninformationbooth.
St. Mary’s brings its healthcare expertise to the communityAgain this year, St. Mary’s was the only hospital to helpthe “Taste of the Caribbean” community event celebrateits11thanniversaryatPlaceBonaventure.The focusof theSt. Mary’s kiosk was on cardiovascular health. Our nurseclinician,PauletteMorris,encouragedeveryonetobevigilantwith their cardiachealth.Manyvisitors stoppedby tohavetheirbloodpressurechecked,tolearnabouttheirBMI(bodymass index) and to pick up literature about maintaining ahealthy heart. Over 2000 people attended this successfulevent.
13
Dr. Rick Mah, SMHC Chief of the Department of Emergency, and his family were among the visitors.
Gemma Raeburn-Baynes (left), president of “A Taste of the Caribbean” Festival and Paulette Morris, a nurse at SMHC, all smiles after the results of the blood pressure test.

“24 heures de science” at SMHCIncollaborationwiththeQuebec-wide“24 heures de science”whichaimsatpromotingQuébec’sscientificcommunity,andundertheguidanceofDr.IndrojitRoy,DirectorofPathologyatSMHC,membersofourcommunitywerepresentedtheuniqueopportunitytotakeajourneythroughthehumanbody,fromtheorgantothecellularlevel.ParticipantsintheeventincludedteachersandstudentsfromJamesLyngHighSchool,ourownSMHCstaffandthegeneralpublic.Thestudentsalsoparticipatedinaninteractivegamethatinvolvedreconstructingthedigestivesystemorgansonateachingmannequin.TheyallexpressedtheirappreciationtoSMHCforprovidingthemwithafirst-handlookattheinnerworkingsofthehumanbody-whichnowhelpsthemtounderstandtherealimpactofourhabitsonourbodies!
In yet another initiative to share our knowledge with the precious, young members of our communitySMHCsupportedanewinitiativecalledProgramme d’intéressement aux métiers et professions de la santé et des services sociaux,developed by the Montreal Health and Social Services Agency, in collaboration with the Ministry of Immigration and CulturalCommunities(MICC).Theobjectiveoftheprogramwastosupporthighschoolstudentswishingtopursuecareersinthehealthsector.FiftystudentsacrosstheislandofMontrealparticipatedintheprogram.SMHChadthepleasureofwelcomingthreeofthem.
Thethreestudentscompletedaseven-weekstageatSt.Mary’swheretheyhadtheopportunitytolearnaboutthemanycareersthatareavailableinthehospital.Theyhadthechancetovisitvariousdepartmentsandtoobserveouremployeesinaction.Thankstoallthedepartmentswhoparticipatedinprovidinganamazinglearningopportunityforthethreestudents!
Front row, High school graduates from the Côte-des-Neiges sector.Back row, SMHC personnel.
“24 heures de science“ participants reconstruct the digestive system organs on a teaching mannequin.

Our Community Health Care PartnersThe 11th Research and Quality of Care Symposium and First Research Colloquium at SMHCSt.Mary’sannualResearchandQualityofCareSymposiumistheidealoccasionforhealthcareprofessionalsacrosstheislandofMontrealtogatheraroundtodiscusscontroversialissuesinhealthcare.Everyyear,thiseventprovidesourhealthcarenetworkwithavarietyoflectures,debates,discussionsandnetworkingopportunitiestoexchangeknowledgeandsharegoodpracticesfromeverywhere.Thethemeof2010wasonemotionmanagement:“FromTearstoLaughter:ConfrontingtheEmotionalGamut”.
Additionally, inorder to reach the researchcommunity,St.Mary’sHospitalCenter launched itsfirst researchcolloquium inSeptember2010.Thisconferencepromisestobecomeanannualeventwhichwillfocusonadifferentinnovativetopicforeveryedition;thefirsteditionfocusedonvirtualwards,aBritishinnovationtoreorganizehealthcareservicesthatcombineselectroniccapacitieswithhumanorganizationinordertopredictandavoidunforeseenhospitalizations.ExpertscamefromtheUnitedKingdom,NewZealand,Torontoandourownhospitaltosharetheirexperiencesandperspectives.
15

Our International CommunitySHMC helping out our local and international communities
HaitiWhen Phil Carpenter, journalist with The Gazette, wasassignedtocoverthecholeraoutbreakinHaiti,heapproachedseveralhospitalstoseeiftheyhadanymedicalsuppliesthattheycoulddonate tohelpboth thepeopleofHaitiand thededicated medical teams and volunteers stationed there.St.Mary’swasquicktorespondandMr.Carpenterexplainedthathewas“impressedandtouchedbySt.Mary’sdesiretohelp and generous spirit. The supplies that were donatedwere of immeasurable help to both the patients and themedicalcrewsinmanagingthismedicalcrisis”.
NepalRebeccaDyck,whoteachesnursingatDawsonCollegeandisanursing instructoratSMHC,went toTansen,Nepal, toteachnursinglastFall.ShebroughtsomeelectronicvitalsignmonitorsthatweredonatedbySMHCwithher.“Thefirstdaywecametothehospital,themonitorwasusedduringsurgeryona6day-oldinfant.Thesurgeoncreditedthemonitorwithsaving thebaby’s life! It isamazing toseewhatwecandowiththingsthatwediscardasoldherebutwhichcanhaveawholenewlifesomewhereelse,”shesays.
16
Some of the donated medical supplies that Phil Carpenter and The Gazette team brought to Haiti.
Rebecca Dyck and Ganga Jirel, Director of Nursing at Tansen’s Hospital in Nepal.
PHOTO:COURTESYOFTHE GAZETTE,PHILCARPENTER
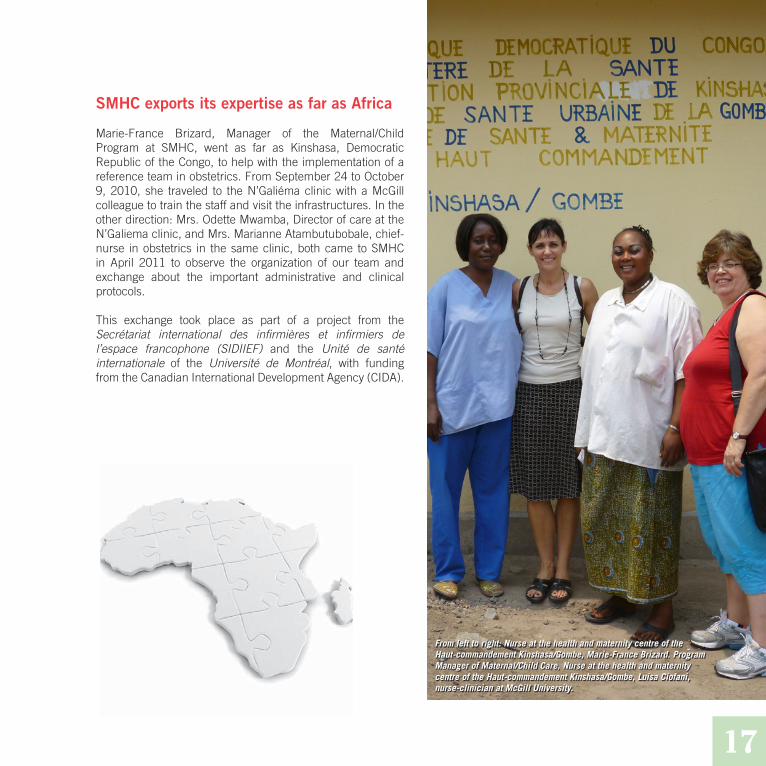
SMHC exports its expertise as far as Africa
Marie-France Brizard, Manager of the Maternal/ChildProgram at SMHC, went as far as Kinshasa, DemocraticRepublicoftheCongo,tohelpwiththeimplementationofareferenceteaminobstetrics.FromSeptember24toOctober9,2010, she traveled to theN’GaliémaclinicwithaMcGillcolleaguetotrainthestaffandvisittheinfrastructures.Intheotherdirection:Mrs.OdetteMwamba,DirectorofcareattheN’Galiemaclinic,andMrs.MarianneAtambutubobale,chief-nurse inobstetrics in thesameclinic,bothcame toSMHCin April 2011 to observe the organization of our team andexchange about the important administrative and clinicalprotocols.
This exchange took place as part of a project from theSecrétariat international des infirmières et infirmiers de l’espace francophone (SIDIIEF) and the Unité de santé internationale of the Université de Montréal, with fundingfromtheCanadianInternationalDevelopmentAgency(CIDA).
17
From left to right: Nurse at the health and maternity centre of the Haut-commandement Kinshasa/Gombe, Marie-France Brizard. Program Manager of Maternal/Child Care, Nurse at the health and maternity centre of the Haut-commandement Kinshasa/Gombe, Luisa Ciofani, nurse-clinician at McGill University.

Combined Balance Sheetas at March 31, 2011
18
2011 2010ASSETSShort TermCash $ 6,036,132 $ 3,908,508 Accounts Receivable - Agency 33,812,267 4,960,619Accounts Receivable - Others 3,721,865 3,017,234Prepaid Expenses 601,505 478,869Inventory 3,372,286 3,496,021Other Assets 2,112 -Long termFixed Assets 75,014,599 69,372,856Funding Receivable - Accounting Reform (3,300,414) (3,585,776)Long Term Investments 1,400 1,400Accounts Receivable - Deferred Leaves 615,264 617,086Total Assets 119,877,116 82,266,817
LIABILITIESShort TermBank Loan 62,222,961 50,998,893Accounts Payable 26,661,351 23,625,498 Accrued Interest Payable 194,196 152,038 Cash advance from the Agency - Enveloppes décentralisées 4,003,879 2,319,772Deferred Revenues 1,324,884 659,639 Other Liabilities 6,162 14,109 Long TermNotes Payable - Capital Fund 14,656,207 16,350,508 Deferred Revenues 17,917,236 21,011,590 Other Long Term Liabilities 631,253 12,105 Total Liabilities 127,618,129 115,144,152 FUND BALANCEFund BalanceOperating Fund (7,813,884) (32,950,206) Capital Fund 72,871 72,871 Special Purpose Fund - -Total Fund Balance (7,741,013) (32,877,335) Total Liabilities and Fund Balances $ 119,877,116 $ 82,266,817

Statement of Operationsfor the Year Ended March 31, 2011
Gross Expenditures of Admissible Activities
19
REVENUES 2011 2010 Agency $ 117,923,414 $ 113,748,403Patient Services 4,703,098 4,893,047Miscellaneous 7,506,448 6,940,906 130,132,960 125,582,356
EXPENDITURESSalaries and Benefits 86,718,373 84,188,894Medication 8,133,663 7,814,130Blood Products 2,820,292 2,924,987Medical Supplies 12,749,500 12,402 643Food and Dietary 941,353 816,814Bad Debt Expenses 636,930 772,681Loan Interest 463,946 268,493General Administration 4,417,166 3,909,113Plant Operation and Maintenance 5,904,479 5,859,939Other Expenses 9,200,237 9,322,967 131,985,939 128,280,661
Excess of Revenues over Expenditures(of Expenditures over Revenues) $ (1,852,979) $ (2,698,305)
Physical Health Program $ 69,216,147 $ 68,058,914Administration and Support Services 20,643,955 19,870,588Non Exclusive Services to a Program 20,624,772 19,659,646Building and Equipment Management 10,847,808 10,959,873Mental Health Program 2,968,064 2,929,742Generic Services Program - Clinical Services 2,510,499 2,242,043Public Health Program 17,009 71,899Employees Benefiting from Stability ofEmployment 19,046 19,039Total Gross Expenditures $ 126,847,300 $ 123,811,744

Statistics 2011 2010
Patient DaysShort Term 90,630 89,055 Long Term - - Newborn 10,158 11,412
AdmissionsAdults 11,449 11,639 Newborns 4,395 4,783
Deliveries 4,370 4,763 Average Length of Stay
Short Term (days) 7.92 7.65 Long Term (days) - -
Occupancy (%) 91.62 90.03 Outpatient Visits 124,844 113,681 Surgical Day Centre - Visits 10,364 10,332 Emergency - Visits 37,445 38,047 Audiology & Speech Therapy - Visits 2,329 1,935 Occupational Therapy - Visits 10,612 10,093 Physiotherapy - Visits 28,724 26,982 Psychiatry - Visits 12,934 12,638 Medical Imaging - Exams 89,148 90,100 Laboratories - Procedures 2,967,715 3,016,345
HUMAN RESOURCESFull Time Equivalent Management Personnel 74 74 Full Time Employees 969 938 Part Time Employees 343 346 Occasional Employees 165 157Number of hours paid during fiscal year for occasional employees 301,356 287,254
20

21
Statement of Data and Controls Reliability Contained in the Annual Management ReportThe information contained in the annual management report is under my responsibility. This responsibility concerns theaccuracy,comprehensivenessandreliabilityofthedata,theinformationandtheexplanationssubmittedinthereport.
Throughout thefiscal year2010-2011, informationsystemsand reliablecontrolmeasuresweremaintained tosupport thisstatement.Moreover,Iensuredthatworkwascarriedoutinordertoprovidereasonableassuranceofthereliabilityoftheresults,andspecificallyregardingthemanagementagreement.
Tomyknowledgethedatacontainedinthe2010-2011annualmanagementreportofSt.Mary’sHospitalCenter,aswellasthecontrolsrelatingtothisdataarereliableandaccuratelyreflectthesituationfortheyearendedMarch31,2011.
ArvindK.Joshi,M.D.DirectorGeneralandCEO
Council of NursesThe Council of Nurses is accountable to theBoard of Directors for assessing the general
quality of nursing acts performed in the hospital centre,making recommendations on the rules of nursing care,makingrecommendationsonrulesgoverningmedicalcareandmedicationusepolicy,makingrecommendationsontheappropriatedistributionofcareandassuminganyfunctionentrustedtoitbytheBoardofDirectors.Inaccordancewiththeby-lawsoftheinstitution,theCouncilofNursesisalsoaccountable to the Director General for giving its opinionon thescientificand technicalorganizationof thehospitalcentre, themeans tobeused toassessandmaintain thecompetencyofnursesandanyotherquestionsbrought toitsattentionbytheDirectorGeneral.
InthepastfiscalyeartheCouncilofNursesdecidedtorefocusitsenergiesontopicsthathavebeensurfacingonanongoingbasis:issuesofprofessionalismandissuesofcommunicationfrom the Council of Nurses to its members. The Councilwantedtosendastrongmessagetoitsmembersinrelationto developing a culture of professionalism that promotespatient focused care, collaboration and accountability.Throughouttheyear,theCouncilworkedonseveralprojectswiththeoverallgoalofredefiningthecultureofnursingandthe importance of an ongoing nursing assessment with anemphasisoncontinuityofcare.
TheCouncil ofNursesalsoworkedon internal restructuringanddevelopment of theCouncil in order topromoteproperchannels of communication from members to the Council.This, additionally, would allow the Council to better gaugeneedsofthefrontlinestaffandassumetheguidancenecessaryforitsmembers.InordertorefocusonqualitynursingcaretheCouncil of Nurses has developed several committees whichwillreporttotheCouncil.
The Council was advised of a professional inspection inJanuaryandhasbeenworkingundertheguidanceoftheVice-PresidentofOperationsandNursinginpreparationforaselfevaluationinOctoberof2011.
Topics of interest during the year were: implementation ofcollectiveprescriptions,theauditingofthetherapeuticnurs-ing plan, recruitment and retention of nurses, professionaladvancementofstaff,NursesDayandawardsofexcellence.
The Council continues to work in collaboration with theLicensed Practical Nurses committee and would like tohighlight theconsiderableextentofworkexecutedby theircommitteeandisaimingtoexpandtheircollaborativeworkingrelationshipwithintheupcomingyear.
CrystalCôté,President
22

23 23
Multidisciplinary Council
24
The Multidisciplinary Council’s (MDC) role is toassessthequalityofprofessionalactivitiesengaged
inbyitsmembersandthecontinuousimprovementofcareandservicesdispensedby thesemembers. It is comprisedof a diverse group of healthcare professionals who share acommitmenttoprovidequalityandcompassionatecaretoaclinicalpopulationthatisalsoremarkablydiverse.
TheExecutiveCommitteeoftheMDCactsthroughitsInter-ProfessionalCommittee(IPC)andtheQualityandEducationCommittee(Q&E)toachieveitsmandate.TheIPCservesasliaison between the Executive and the member disciplineswhile the Q&E Committee promotes education and qualityimprovementthroughprojectsandpresentations,thussharingandcommunicatingtheactivitiesoftheMDCdisciplines.
Objectives Achieved and Accomplishments in 2010-11
A sub-committee of the MDC Executive Committee wasformedtoupdatethebylawsoftheMultidisciplinaryCouncil,taking into consideration our new status as a UniversityAffiliatedHospitalCenterandchangesinlegislationandwillcompleteitsmandatebythefallof2011.
TheMDCthroughitsExecutiveCommitteepresentedtheVice-President of Human Resources with recruitment, retentionandrecognitionsuggestionsforitsmembership.
IncollaborationwithInfectionPrevention&Control,theMDCcontinued to promote vigilance and education for infectioncontrolandpandemicplanning.
ThroughtheIPCandQ&ECommitteestheMDCcontinuedtoencouragepeer review/quality improvement activitieswithinallmemberdisciplines.
The physiotherapy department successfully passedinspection in July 2010 by the Ordre professionnel de la physiothérapie du Québec (OPPQ) on recommended
practices and guidelines for maintenance of equipmentandproducts,withnorecommendationsandprofessionallyinspectedinDecember2010withresultspending.Medicalimaging successfully passed inspection in February 2011withrecommendations.
IncollaborationwiththeCouncilofNursesandtheCouncilof Physicians, Dentists and Pharmacists, a Tri-CouncilConferencewaspresentedoncoloncancer.
TheMDCheldsevenGrandRoundsonsuchvariedsubjectsas wills, mandates & curatorship, osteoporosis, motivatingourpatientsandmaking&keepingresolutions.AttheMDCAnnual General Assembly in 2010, Dr. Jeannie Haggerty,McGill Chair in Family & Community Medicine Researchat St. Mary’s presented “Research at St. Mary’s – A LittleSomethingforEveryone”.Theseeducationalinitiativeswerewellreceivedbythemembership.

25
The MDC strives to assure the delivery of patient-focused,qualitycareinatimely,efficientandsafemanner,withinandbeyondtheconstraintsofourhealthcaresystem.Wepracticecollaboratively with other professions. Our membershipis actively involved in teaching, research and continuingeducation activities. Members are engaged with universityandcollegecommunities,withtheirProfessionalOrdersandparticipateinregional,provincialandnationalorganizations,community support services as well as the community atlarge.
Anne Lacourse, Music Therapist with one of her patients.
Objectives of the MDC for 2011-2012
• Promotepatientsafetywithin theMDCdisciplinesandprofessions.
• Complete the process of updating the MDC bylaws,takingintoconsiderationournewstatusasaUniversityAffiliatedHospitalCenterandchangesinlegislation.
• Encourage and facilitate patient empowerment in allmemberdisciplines.
• Continue to encourage quality improvement activitieswithinallmemberdisciplines.
JudySurette,President
Jeanne Wong, Physiotherapist with a patient.

Council of Physicians, Dentists, and Pharmacists
The Executive Committee represents the Council ofPhysicians, Dentists, and Pharmacists (CPDP), which iscomposedofapproximatelythreehundredmembers.
Fivegoalswereestablishedforthe2010-2011mandate:
• Collège des Médecins du QuébecInspection• InternationalMedicalGraduate(IMGProgram)• RecruitmentofPhysicians–theExecutiveoftheCPDP
tobeactivelyinvolvedinpromotingandrecommendingphysicianstoSMHC
• Bill90• OACISProject
Executive Committee Priorities 2010-2011
1. Collège des médecins du Québec Inspection
The Executive Committee unanimously agreed to actuponthefollowing:- RevisionsoftheDepartmentalby-lawswithrespect
totheCMQrecommendations.- ReviewoftheCouncilofPhysicians,Dentists,and
Pharmacistsby-laws.- Incompletechartsandsurgicalreports.- Qualityassessmentaudits.- Establish an action plan specific to the CMQ
recommendations for the Divisions of GeneralSurgeryandUrology.
- Review criteria and necessary forms forreappointmentofphysicians.
2. International Medical Graduate Program
Withmuchhardworkanddedication,aformaleduca-tional program with dedicated space, was establishedand the first candidates commenced their training inMay2011,underthedirectorshipofDr.EricTremblay.
26
3. Recruitment of Physicians
Recruitment of new physicians is restricted by a longandcomplicatedprocess,hamperedbyvariouslevelsofgovernmentalrequirements.
4. Bill 90
Bill 90 i.e. Collective Prescriptions – most of the yearwas involved in establishing a working paradigm forthe evaluation and acceptance of prescriptions by thevariouscommitteesinvolvedintheiroversight.
5. OACIS Project
Dr. Howard Stuart is actively involved in the OACISproject.ApresentationistentativelyscheduledfornextFall.
ThreecommitteesreportdirectlytotheExecutiveCommittee:
- Medical, Dental, and Pharmaceutical EvaluationCommittee;
- PharmacologyCommittee;- QualificationsCommittee.
Medical, Dental, and Pharmaceutical Evaluation Committee (MDPEC)Foursub-committeesreportregularlytotheMDPEC:
• PerinatalMorbidityandMortalityCommittee Monthly reports are submitted on intrauterine
fetal and neonatal deaths. These reports includerecommendations on management of futurepregnancies,whereapplicable.

27
• MedicalRecordsCommittee Overtheyear,theMedicalRecordsCommitteereviewed
and approved 16 new forms that were integrated intohospitalmedicalcharts.Incompletemedicalchartsarealso reported regularly to the committee. The numberofincompletechartsdecreasedto902(October2010);increased to 1105 (January 2011); and decreased to859inApril2011.
• InfectionControlCommittee Issues and activities addressed included the
following:- On-goingmonitoringofMRSA,VRE,and C-Difficile;- Yearendrateswerepresentedfor2009andwere
slightlyhigherduetoVRE;- OR rate of infections was overall less. Most
recommendationsarebeingfollowedsuchas“skinprepkits”;
- PolicyonPandemicFluisnowcompleteandispartoftheInfectionControlManual;
- Complianceratesforrecordingofpre-opantibioticshave increased. Ratesbeganat45%,nowup to93%.Auditwascarriedoutonthe6thfloorSurgery.
• SurgicalReviewCommittee- Mini projects on rectal cancer will be conducted
withthecollaborationoftheDirectorofPathology.
Pharmacology CommitteeOne of the Committee’s main responsibilities is to monitordrugusewithinthehospital,accordingtoestablishedpoliciesandguidelines.
• Formaldrugutilizationreviewperformed:- ReviewofHyperalimentation;- Total Parenteral Nutrition – implementation of
screeningprescriptionsfornon-medicallyjustifiableprescription. Intervention of ICU physician tosupportdietician.
• Thefollowingguidelineswerealsoapproved:- HyperemesisGravidarunpre-printedprescription&
exitprescription;
- Parathyroidectomypre-printedprescription;- ICUpre-printedprescriptionforSepticShock;- Diabeticketoacidosis–ICUpre-printedprescription;- Hypothermiapost-cardiacarrest– ICUpre-printed
prescription;- Collective Prescription – Ibuprofen (for Triage
NursesinER);- Collective Prescription – Acetaminophen (hospital
wide);- Collective Prescription M-003 for Scopolamine
butylbromide in Medical Imaging, new increaseddosage;
- TemporarydiscontinuationofWarfarin (Coumadin)beforesurgery–bridgingwithFragmin;
- Pre-printed prescription for ChemotherapyHypersensitivity;
- Automaticsubstitutionofmeropenemtoimipenem;- Intralipidprotocol;- PolicyforOncologydruguse(Revision);- Pre-printed prescription for cervical catheter
induction;- AutomaticswitchfromTimentintoTazocin.
Qualifications CommitteeThrough the active participation of the QualificationsCommittee, applications from physicians wishing topursuetheircareeratSt.Mary’sHospitalwerereviewedandsubmittedtotheCPDPExecutiveCommittee.
Quality Improvement Activities
Members of the CPDP also participate in the QualityImprovementactivitiesof thevarioushospital teams.TheseactivitiesarepresentedtotheQualityandRiskManagementCoordinating Committee and are reported to the ExecutiveCommittee of the Council of Physicians, Dentists, andPharmacists.
MarcelFournier,M.D.Chair,CouncilofPhysicians,Dentists,andPharmacists

Quality and Risk Management
28
TheultimategoalofQualityandRiskManagement(QRM)atSt.Mary’sHospitalistomaintainandimproveuponqualityofpatientcareandsafetyinservicedelivery.Themainfunctionof QRM is the support of programs and councils in theirqualityandriskmanagementactivitiesandmaintaining theresponsibilityfortheoverallqualityandriskmanagementattheprogramlevel.
The Quality and Risk Management Coordinating Committee(QRMCC)isthecentralfeatureofthestructureandservesasa reportingbody for the teams. In2010-2011, theQRMCCmet on 13 occasions and reviewed presentation of annualreports on quality and risk management from the followingteams: Geriatrics, Mental Health, Family Medicine, CriticalCare,Emergency,CancerCare,HumanResources,Informa-tionManagement, InfectionPreventionandControl,Dialysis,Maternal-Child,Surgery,Laboratories,Nurses’Council,Multi-disciplinaryCouncil,CouncilofPhysicians,DentistsandPhar-macists,RehabilitationServices,andDiagnosticImaging.
Accreditation Canada
For2010-2011,QRMhasbeeninvolvedinrespondingtoanumberofrecommendationsfollowingtheaccreditationvisitwhichtookplaceOctober4to8,2009.
Principal follow-ups tobecompletedwereon the followingissues:
- need to implementamorestructured riskassessmentandfollow-upfortwoclinicalareas;
- establish data collection process for anaphylacticantibioticadministration;
- process for communicating information on bloodtransfusions;
- implementatimeoutprocessintheOR;- extension of conservation calendar for laboratory
equipment;- plan to have a hand washing station with hands-off
mechanism;
- ensuretheaccesstoradiationmonitoringdevicesforORstaff;
- systematic quarterly reports on incident/accidentreportingtotheBoard;
- establish real-time practices of emergency measuretraining;
- formalize policies and procedures in written form formedicationmanagement.
All of these follow-ups were completed and acceptedby Accreditation Canada who also recognized SMHC’scontinuous engagement in improving quality of care to itspatients.
Research Centre
Therewasnoinstanceofscientificorethicalmisconductinresearchforthe2010-2011fiscalyear.
Incident/Accident Reporting
Thestatisticalprofileofincidents/accidentsforthe2010-2011fiscalyearisincompleteasdelaysinthefullimplementationoftheSISSSprogramhascontinuedtopostponedataentry.Implementationof thenewSISSSprogramhasstartedwiththedataentryofIncident/Accidentreportsbeingenteredasof theendof the2010-2011fiscalyear.Themainfocusofthisimplementationistoensureconsistentcodingofeventssoastobeabletoextractvaliddatafortrendingpurposes.For the 2010-2011, there were 1791 incidents/accidentsreported1.Thisisa9.5%decreasefrom2009-2010.
Whileaspecificdescriptionoftypeoferrorreportedisnotpos-sibleyet,duetolimitationsandchallengeswiththeimplemen-tationoftheSISSSsoftware,specificreviewsofallreportshavenotshownasignificantchangeintypeofincident-accidentorseverity. While waiting for this function to be available, theQRMDepartmentdoesrequestfurtherfollow-uponaselec-tion of adverse events and these are closely monitored intermsofcorrectivemeasuresthatareputinplace.Wehope
1 1. Received by the Quality and Risk Management Department as of June 2, 2010

tobeabletoobtainstatisticalanalysisfromSISSSinordertoshowtrendsinseverityofincident/accidentsreported.
Risk Inventory
Quality and Risk Management monitors various riskmanagement functions in all areas of the hospital. ThefollowinglististheriskinventorymonitoringsystemsthatareinplaceatSt.Mary’sHospitalCenter.
1. Patientcomplaints2. Lawsuits3. Claimsagainstthehospital4. InsuranceClaimsagainstthehospital5. Labourgrievances6. RadioactiveIsotopes7. Councilquality/riskmanagementactivities(Councilof
Physicians,DentistsandPharmacists,MultidisciplinaryCouncil,CouncilofNurses)
8. InfectionControlactivities9. Employee work accidents, occupational diseases &
CSST10. Unsafeworkconditions11. Hazardousmaterialsrelatedrisks12. Workplaceviolence13. Biomedicalequipmentrelatedrisks14. Biomedicalrelatedalert&recalls15. Non-biomedicalequipmentrisks16. Informationsystemsrisks17. Researchrisks(researchethicsannualreport)18. Emergency measures and other security related
incidents19. Incident/Accidents(AH-223)20. Restraintsrelatedrisks21. Sentinelevents
Foreachidentifiedriskdomain,thereisadefinedreportingsystem, including annual reports and defined pathways ofreportingtotheSeniorManagementteam,committeesoftheBoardofDirectorsordirectlytotheBoardofDirectors.
Risk Management Initiatives for 2010-2011
Among many risk-related activities, the main hospital-wideinitiativeswere:
- Monitoring of incident/accidents to ensure appropriateactionistakenbytheappropriateareasinvolved;
- Presentation of the results of Failure Mode EventsAnalysis (FMEA) on narcotics management to theinternalcommunity.
- Ad hoc Sentinel Event Committees have reviewed anumber of situations with corrective measures beingtakeninalltopreventrepetitionoftheaccident.
- Patient Safety Week that included 3 lunchtimepresentations on how to do a quality cycle on thejob, infection prevention and control, and preventingidentification errors, ErroMed (Human Factors andPatientSafety)traininggivento23staffmembers.
Quality Assessment Projects Completed in Support of Quality Improvement Teams
Eleven projects were completed by the Quality AssessmentUnit insupportof theQuality ImprovementTeams.TheQAUnitcompleted6projectsin2010-2011andstarted11newprojectsin2010-2011.Oneprojectstartedin2008-2009andthreefrom2009-2010werestillongoing.

Research Activities
With thesupportof theC.A.R.E.program,anevaluationoftheErroMedtrainingprogramwasconductedin2010-2011.Thisprojectwillbecompletedin2011-2012.Also,theQRMDepartmentisinvolvedinthePatientEngagementProjectinsupportingtheUsers’CommitteeandtheQIteamsinvolvedintheproject.
11th Annual Symposium on Research and Quality of Care
ThegoalsoftheAnnualSymposiumonResearch&QualityofCarearetodisseminateinformationandstimulatediscussionaboutthefollowing:
• Qualityimprovementactivitiesconductedatthehospital,thatdemonstratetheapplicationofresearchevidencetopractice;
• Researchbeingconductedatthehospitalthatisrelevanttoqualityimprovement;
• Importantresearchand/orqualityimprovementinitiativesconductedoutsidethehospitalthatarerelevanttocareandservicesprovidedatSMHC.
The 11th edition of this event, gathered 138 registeredparticipants around the theme “From Tears to Laughter:
30
Confronting the Emotional Gamut” where a number ofspeakers gave attendees different perspectives on dealingwith patient, family and professional’s emotions within thecontext of healthcare. Fifteen posters were also submittedand showcased research and quality projects that wereongoingorhadbeencompletedbytheresearchteamsandtheQIteams.
Annual Audit Regarding Restraints Use
Therewerenoauditsconductedonrestraintsusein2010-2011 due to the revision of the policy and procedure onrestraints.The last studyconducted in2008-2009showedthat the proportion of restraints did not differ greatly overthe three years and also showed improvements in thedocumentationoftheuseofrestraints.Wewillredoanauditin2011-2012toseeifthetrendshavechangedsignificantly.
Follow-up to Coroner’s Report Recommendations
Therewasonerequestforfollow-upbytheCoroner.Aninternalandin-depthinvestigationinthespecificcasewasdoneanditwasdeemedthattheinter-institutioncommunicationtoolsinplacewereusedappropriatelyandweresatisfactory.
Infection Control and Prevention Activities
QI Initiatives & Projects1. The Staph aureus Bacteremia (SA) surveillance,
established by Public Health since 2006-2007, is on-going.Our interventionisbasedonresults.Ouroverallrate of SA Bacteremia that is MRSA is respectively43.75%, 36.59%, 28.13% and 34.62% (ratesfollowingcorrections) for the four lastfiscal years.Ourrate improved in the 2009-2010 fiscal year, we arecomparabletothesamesizehospitalsintheprovince.

31
2. The rate of the provincial Central Line AssociatedBacteremia (CLAB)surveillance in ICUwas2.33% forthe2009-2010fiscalyearand1.88%for2010-2011.
3. Our baseline rate of the provincial Central LineAssociated Bacteremia (CLAB) surveillance in dialysiswas0.26%forthe2010-2011fiscalyear.Wewillbeabletobenchmarkwithsamesizedialysisintheprovincebytheendofthe2011-2012fiscalyear.
Surveillance Activities and Control of Nosocomial InfectionsSurveillance and containment of multi-resistant organismssuch as MRSA and VRE continues. Methicillin resistantStaphylococcus (MRSA) containment continues to be animportant focus of the IC department. Even though thenumberofnosocomialMRSApatientsislowerthanpreviousyears,thetotalnumberremainshighplacingalargeburdenon all resources. We had 118 nosocomial MRSA cases in2010-2011comparedto132in2009-2010.
We have seen a decrease in our nosocomial VRE casescompared to the previous year; we had twelve nosocomialVRE cases in 2010-2011 compared to 23 in 2009-2010.Howeverourprevalencepointishigherthanpreviousyears,leadingtoincreaseriskfornosocomialtransmission.
Surveillance of Surgical Site Infections (SSI) includesadmitted patients only (day surgeries are excluded), andfor the following surgical services: General, Orthopaedic,Gynaecology&PostC-section.
Reportingisdonetoindividualsurgeonsandbycodetothechiefofsurgeryandthechiefofservice.
The on-going Clostridium difficile surveillance systemestablished by Public Health (INSPQ) in 2004-2005throughout the province, is giving us the opportunity tobenchmarkwithsamesizedhospitals.Wearealmostbacktoourbaseline;wehad38nosocomialcasesinthe2010-2011fiscalyearcomparedto45in2009-2010.
Themainobjectiveof thebloodculturecontaminationratesurveillanceistoidentifychangesinthebloodculturecon-taminationrateandtorecommendchangeswhenneeded.
Implicationsofbloodculturecontaminationare:- Unnecessaryantibioticuse- Increasedlengthofstay- Additionalcultureswhichwillleadtoincreasedcost.
Acceptablebloodculturecontaminationratesaregenerally3% or less. For the three periods audited this year, bloodculturecontaminationrateswererespectively0.59%,0.91%and 0.90% – far below the 3% threshold. Blood culturecontaminationsduringthethreeperiodswerenotedmainlyinERandICU.
Outbreak Investigations• During the fiscal year2010-2011, twoVREoutbreaks
occurred on 8 Main and 5 Main in February andNovember2010.Avastamountofresourceshavebeenusedforcontainment.
• We also had in May and April 2010, three MRSAoutbreaks on 5 Main, 5 South and ICU whichnecessitated isolation of many patients and increasedhousekeepingactivities.
EducationA number of in-services have been given to the hospitalstaffthroughoutthe2010-2011fiscalyear.TheICteamhascommitted a total of 36 hours in rendering educational in-services to545attendees, including129 students and416employees.
Duringthe2010-2011fiscalyear,atotalof150hourswerededicated to the training of the Infection Prevention andControlDepartmentstaff:twoinfectioncontrolpractitioners,onesecretaryandonemanagerhaveundergoneeducationaltrainings(threeon-linecourses,weekly teleclasses, two in-classcomputercoursesandthemanager’sInfectionControl

Boardrecertification)whichhaveequippedtheteamwithanin-depthknowledgeofinfectioncontrolpractices,aswellasenablingthemtosharpenthenecessaryskillstoaccomplishtheirjobproperly.
Completed Projects• On-goingrevisionoftheInfectionControlManual(April
2010–March2011).• Infection Control posters, signs, pamphlets and
informationareupdatedandmadeavailableviaVisualCommunicationsServices.
• Snapshotauditstoevaluateinfectioncontrolpracticesand hand hygiene are done when an outbreak isidentified. Intervention is based on findings (a total offiveweredonein2010-2011).
• Ourdepartmentparticipatesattheregionalandnationaltables for nosocomial infections, with the INSPQ,nationalandprovincialinfectioncontrolassociationsandtheInfectionControlMcGillWorkingGroup.
Basedontheresultsoftwoauditsdoneintheoperatingroom(OR)inApril2009,recommendationswerepartly institutedthroughout2010-2011,follow-upisstillon-going.
Upcoming Projects 2010-2011• Continuehandhygieneblitz• HandhygieneauditscheduledforAugust2011;wewill
beabletobenchmarkwithsimilarauditsdonein2007and2009
• Workwiththesurgicalteamtocompletetheimplemen-tationofthe2009-2010ORauditrecommendations.
• Thegoalofthesignageprojectistostandardizeallinfec-tioncontrolprecautionssignsacrosstheMcGillteachinghospitals. A working group composed of infection con-trolpractitioners fromvariousMcGillhospitals lookedattheresearchandwrittenguidelinesavailable,andmadechanges to the infection control signs accordingly. Theaimistomakeiteasierforhealthcareprofessionalsandsupportstaffwhoworkatvarioushealthcareinstitutionstobeabletoeasilyrecognizetheinfectioncontrolsignage,therebyincreasingcompliance.Followingthesameratio-
32
nale,thestandardizationofthesesignswillalsobeben-eficialforpatientsandfamilymemberswhovisitdifferentMcGillhospitals.Thefirststepstartedwithapilotprojecton5Southinmid-Mayandlastedthreeweeks.
• Quality control for compliance with infection controlmeasuresintargetedareasisstillon-going.
Quality and Risk Management Recommendations and Prioritiesfor 2011-2012
• Prepare and organize the self-assessment process inpreparationforthe2012AccreditationCanadavisit.
• Reducethebacklogindataentryfor incident-accidentinSISSS.
• Track Quality Assessment projects and links withaccreditationstandards
• Continuethefollowingfunctions:- Continuous in-service education of staff and
managersonpatientsafetyandriskmanagement;- OrganizePatientSafetyWeek, includinga special
2-day training for staff and managers on humanfactorsandpatientsafety(ErroMed);
- Provide an additional ErroMed training session tostaffeveryyearasof2011-2012;
- SupportQIteamsacrossthehospital;- Support theAnnualSymposiumonResearchand
QualityofCare.

Report from the Comité de vigilance et de la qualité 2010-2011
TheCommitteemetthreetimesduringthefiscalyear2010-2011.Attheheartofitsmandate,theCommitteemakessurethatadequatefollow-upisgiventothemainrecommendationsofthelocalservicequalityandcomplaintscommissionerthatcouldbe retainedby theBoardofDirectors.TheBoardofDirectorsacceptedtherecommendationofthecommissionerfortherevisionoftheprocessrelatedtotelephoneaccesstothevariousclinics.
TheCommitteereviewedthereportonlegalsuitsagainstthehospitalinrecentyears.
Incidentally,theCommitteewasinterestedbytheconclusionsofAccreditationCanadafollowingthevisitoftheorganizationin October 2009. The Committee also received therecommendationsfollowingtheinspectionvisitoftheCollège des médecins andwill ensure their follow-up in theFall of2011.RecommendationsfromtheCommittee,ifany,willbeaddressedtotheBoardofDirectors.
AnupdatedversionoftheCodeofEthicswaspresentedtotheCommitteefollowingitsadoptionbytheBoardofDirectors.
The Committee was also kept abreast of the evolution ofcomplaintsthroughouttheyear.
33
Report from the Local Service Quality and Complaints CommissionerBreakdown of complaintsCompletedwithoutcorrectivemeasures........................ 54%Completedwithcorrectivemeasures............................ 43%Refusedorinterrupted................................................... 1%Abandoned.................................................................... 2%
Summary of complaintsComplaintscarriedoverfrompreviousyear...................... 9Complaintsreceivedduringthecurrentyear................. 189Complaintsconcludedduringthecurrentyear.............. 191Complaintscarriedovertothenextperiod........................ 7
Objects of complaintsAccessibility................................................................... 35Careandservices........................................................... 52Qualityofhumanrelations.............................................. 47Environmentandmaterialresources............................... 30Financialaspect............................................................. 24Individualrights............................................................. 28Other............................................................................... 0
Originator of complaintsPatients...................................................................... 64%Family/Other............................................................... 36%
Processing time-45days.................................................................... 84%+46days................................................................... 16%

Users’ CommitteeThepurposeoftheUsers’Committeeistodefend,protectandensure respect for patients’ rights. Respect for users’ rightsandquality of services are the foundationwhich guides theactionsof thecommittee. It is thecommittee’sresponsibility,uponrequestofauser,toaccompanyandassistauserinanyactionheorsheundertakesincludingthefilingofacomplaintinaccordancewiththeActrespectingtheHealthandSocialServicesOmbudsman.
The Users’ Committee of St. Mary’s Hospital Center iscomprisedofninemembers.OneofthemembersrepresentsthecommitteeontheBoardofDirectorsofthehospital.Wealso have a resource person who acts as secretary of thecommittee.
Meetings are held the last Friday of the month, SeptemberthroughMay.Therewere twoemergencymeetingsheld thispast year. Department heads are invited to speak at somemeetings.
TheCommitteeisamemberoftheRegroupement provincial des comités des usagers.AnEnglishsectorhasbeensetupandwemetthreetimes.
An annual budget is received and is used according to thedirectives issuedby theMontrealHealthandSocialservicesAgency.
34
The Committee is part of the Patient Engagement Project(PEP). This is a two-year research project involving threeareasinthehospital:MentalHealth,EmergencyandCancerCare. This project aims to strengthen the patient voice inqualityimprovementinitiatives.
Wereceivedapproximatelyonehundredcallsthisyear.Someexamples of calls were regarding phones not being answe-red for patients to make appointments, appointments beingcancelled without notifying patients, rudeness by staff, fileslost,anduncleanpatientareas.Patientsareaskedifhe/shewishes to lodgea formalcomplaint.Anycomplaintaboutadoctorautomaticallyisreferredtotheombudsman.
Allgoalssetfortheyear2010-2011weremet.
Goals for 2011- 2012
- Partnering with Risk Management in Patient SafetyWeek.
- Startinga“SpeakOut”campaignforpatients.- Findasolutiontotheproblemofmakingappointments
byphone.- Assist patients with language difficulties acclimate
themselvestothehospital.
Respectfullysubmitted,
PatriciaMcDougallPresident

35
This Code of Ethics governs the members of the Board ofDirectorsintheexerciseoftheirresponsibilities.
General Responsibilities1. MembersoftheBoardshalldemonstraterespectforthe
dignityofhumanlifeandfortheequalrightofindividualstohealthandsocialservicesregardlessofrace,colourorreligiousbackground.
2. Members of the Board shall demonstrate a spirit ofcooperationandactivelyparticipateinthedevelopmentandimplementationoftheHospital’sgeneralpolicies.
3. Members of theBoard shall attendBoardmeetings andshallvoteonallmatterssubmittedtothemunlessdoingsowouldrepresentaconflictofinterest.
4. MembersoftheBoardshallactwithcare,integrity,honour,dignity,honesty,impartiality,loyaltyandobjectivity.
5. Membersof theBoardshall respect theconfidentialityofdebates,exchangesanddiscussions.
Specific Responsibilities1. Members of the Board shall not directly or indirectly
solicit,acceptorrequire fromanyoneanygift, reward,orbenefit sufficiently material to give rise to a reasonableapprehension that itwould compromise their impartiality,judgmentorloyaltyasdirectorsoftheHospital.
2. Members of the Board shall act within the limits of thepowersvestedinthem.
3. MembersoftheBoardwhohaveadirectorindirectinterestinanyenterpriseorendeavourthatplacestheminaconflictof interestwith theHospital or that creates a reasonableapprehensionof suchaconflict shallnotify theBoardofsuch interest in writing as soon as practicable after theybecomeawareofit.
4. Anymemberof theBoardobliged todisclosean interestcontemplated in the preceding paragraph shall abstainfromparticipating indeliberationsordecisions relating tosuchinterest.
5. MembersoftheBoardshallnotifytheBoardinwritingofanycontractsfortheprovisionofgoodsorservicesconcluded
with the Hospital by any enterprise in which they areemployedorinwhichtheyholdapecuniaryinterestassoonaspracticableaftertheybecomeawareofsuchcontracts.
6. WrittennotificationoftheBoardshallbedeemedtohavetaken place when the Executive Director has thus beennotified. The Executive Director shall communicate thenotificationtotheothermembersoftheBoardatthefirstopportunity.
7. Members of the Board shall not use confidentialinformationforthepurposeofderivingdirector indirectpersonal benefits therefrom. Following their mandate,members of the Board shall respect the confidentialityofallinformationofanynaturetowhichtheywereprivyin theexerciseof their functionswhilemembersof theBoard unless such information has entered the publicdomain.
Disciplinary Procedures1. A breach of a duty prescribed in this Code or by law
constitutes a derogatory act and may give rise to adisciplinarysanction.
2. Any person who has reason to believe that a directorhas contravened this Code shall so advise the ExecutiveDirectorinwritinginsufficientdetailtoidentifytheallegedcontravention,whenandwhereitallegedlytookplaceandtheproofthathasledthecomplainanttoconcludethatithas takenplace. If thecomplaintconcerns theExecutiveDirector,thenoticeshallbeaddressedtothePresident.ThemembersoftheBoardshallbeprovidedwithacopyofthecomplaintatthefirstopportunity.
3. After hearing the representations of the director who isthe subject of the complaint, the other members of theBoardmayappointacommitteeof threeof theirnumberto investigate the complaint, to report to theBoard as towhether thecommitteeconcludes that it iswell-founded,and whether it recommends further investigation by theBoardorothers,oradisciplinarysanctioninconsequence.Thecommitteeshallnotifythedirectorwhoisthesubjectofthecomplaintofitssessionsandgivesuchdirectororhisor
Code of Ethics

herrepresentativeareasonableopportunitytobeheardandtomakewrittensubmissionsifdesired.Thedeliberationsofthecommitteeshallbeconfidential.
4. The committee shall make a written report to the Boardassoonaspracticable.Shouldthereportrecommendtheimpositionofadisciplinarysanction,theBoardmayin itsdiscretiondecidetoreprimandthedirectorwhohasbeenfoundtocontravenethisCodeoritmaydecidetorequesthisorherresignation.Itmayalsodecidetoinitiateappropriatecivilorpenallegalproceedings.TheBoard’sdecisionshallbecommunicatedinwritingtothedirectorconcerned.
5. MembersofthecommitteeandtheBoardshallbeimmunefrom legal process in consequence of exercising theirresponsibilitiesingoodfaithpursuanttothisCode.
Dissemination of the Code1. AcopyofthisCodeshallbeprovidedtoeachmemberofthe
Boarduponthecommencementofhisorhermandatewitharequestthatheorshetakecognizanceofitandcomplywithit.
2. AcopyofthisCodeshallbemadeavailablebytheHospitaltoallindividualswhorequestitandshallbepublishedintheHospital’sannualreport.
3. TheannualreportoftheHospitalshallstate:a) thenumberandnatureofcomplaintsreceived;b) thenumberofcaseshandledandtheirdisposition;c) thenumberandnatureofpenaltiesimposed;andd) thenamesofthedirectors,ifany,whoseresignations
havebeenrequested.
ForthefiscalyearendedMarch31,2011,theBoardofDirectorshasnotreceivedanycomplaintsorindicationinregardstothenon-respectofthiscode.
36

As of March 31, 2011ADMINISTRATION
Arvind K. Joshi, M.D.DirectorGeneralandChiefExecutiveOfficer
Linda BambonyeVicePresidentOperationsandNursing
Bruce Brown, M.D.VicePresidentProfessionalServices
Ralph Dadoun, Ph.D.VicePresidentCorporateandSupportServices
Elisabeth DampoliasVicePresidentHumanResources
Susan Law, Ph.D.VicePresidentAcademicAffairs
COUNCIL OFPHYSICIANS, DENTISTSAND PHARMACISTS
Marcel Fournier, M.D.President
Chryssi Paraskevopoulos, M.D.1stVicePresident
Paul Stephenson, M.D.2ndVicePresident
Marie Iskandar, M.Sc.Pharm.Treasurer
Balbina Russillo, M.D.Secretary
COUNCIL OF NURSES
Crystal CôtéPresident
Cindy MarchandVicePresident
Natalie D’AoustTreasurer
Megan FournierPublicRelationsOfficer
MULTIDISCIPLINARY COUNCIL
Judy SurettePresident
Marcela HidalgoVicePresident
Filomena NovelloTreasurer
Marc PineaultSecretary
Flora MasellaPublicRelationsOfficer
BOARD OF DIRECTORS
EXECUTIVECOMMITTEE
Marc W. TrottierPresidentFoundation
Rafik Greiss1stVicePresidentPopulation
Suzanne Gouin2ndVicePresidentUsers’Committee
James C. CherryTreasurerLegalPerson(Governors)
Richard J. RenaudPastPresidentLegalPerson(Governors)
MEMBERS
Samuel Benaroya, M.D.University
Martin CauchonCooptation
Bonnie CuthbertNon-clinicalpersonnel
Anne-Marie d’AmoursPopulation
Rita Lc de SantisMontrealAgency
Lorna DowsonMultidisciplinaryCouncil
Gail Goldman, M.D.CouncilofPhysicians,DentistsandPharmacists
Arvind K. Joshi, M.D.DirectorGeneralandChiefExecutiveOfficer
Liette LapointeUniversity
Michael MacchiagodenaUsers’Committee
Nancy Margaret MarrelliMontrealAgency
ClaireMullins-KruytCooptation
Lina PalazzoCouncilofNurses
Dominique PiperResidents
Murray SteinbergCooptation
Marcel VilleneuveFoundation
CLINICAL DEPARTMENTCHIEFS
Molly McHugh, M.D.Anaesthesia
Roni Berbari, D.M.D. (acting)Dentistry
Rick Mah, M.D.Emergency
Alan Pavilanis, M.D.FamilyMedicine
Joe Dylewski, M.D.Laboratories
Michael Bonnycastle, M.D.Medicine
Robert Hemmings, M.D.ObstetricsandGynaecology
Jaroslav Prchal, M.D.Oncology
Conrad Kavalec, M.D.Ophthalmology
Apostolos Papageorgiou, M.D.Paediatrics
Marie Iskandar, M.Sc.Pharm.Pharmacy
Suzanne Lamarre, M.D.Psychiatry
Jack Glay, M.D.Radiology
John R. Sutton, M.D.Surgery
37

38
OrganizationalStructure
Chief of MedicineChief of Emergency
Chief of Obs./Gyn.Chief of Pædiatrics
Chief of SurgeryChief of AnæsthesiaChief of Obs./Gyn.
Chief of Ophthalmology
Chief of Oncology
Chief of Medicine
Chief of MedicineChief of Surgery
Chief of Psychiatry
Chief of Family Medicine
Chief of Laboratories
Chief of Imaging
Chief of Pharmacy
Health Sciences LibraryClinical Ethics
Quality & Risk ManagementInfection Control and Prevention
Medicine
Maternal/Child
Surgery
Cancer Care
Geriatrics
Ambulatory Care
Mental Health
Family Medicine
Corporate Services
Diagnosis & Therapeutic Services
Support Services
Fam
ily M
edici
ne
Medical Records & AdmittingRespiratory Therapy
Clinical NutritionSocial Services
Rehabilitation Services
Human Resources
Volunteer Resources
Boardof Directors
Ombudsman Users’ CommitteeExecutive &
Administrative Committee
Multidisciplinary Council
Council ofPhysicians, Dentists
& Pharmacists
Director General &CEO
Board of Governors
Councilof Nurses
Vice-PresidentProfessionnal Services
Vice-PresidentOperations and Nursing
Vice-PresidentCorporate & Support Services
Vice-PresidentHuman Resources
Program Coordinating Team
Public Relations
Legal Services
Foundation
Auxiliary
Occupational Health
Vice-PresidentAcademic Affairs
Teaching
Research Centre

39
At SMHC, we have our
communityat heart!
Published by: Public Relations and Communications Department, SMHCGraphic design, photography & production: Visual Communications Services, SMHC
3830 Lacombe Avenue, Montreal, Qc H3T 1M5
Tel.: (514) 345-3511Fax: (514) 734-2692
www.smhc.qc.ca
Disclaimer: Certain information contained in this Annual Report reflect forward-looking expectations or statements.
The data / statistics contained herein reflect the information available at the time of publication.

















