Suite A East Wing ARS Medicae Building No. 14, 6 th Avenue, Belleville St Michael Barbados Tel (246) 429 6859 Fax (246) 435-0569 email:[email protected]www.aidincorporated.org Associates for Associates for International Development International Development Social and Economic costs of HIV and AIDS Current issues Costs, cost-effectiveness & Sustainability Sarah Ann Adomakoh
Transcript
Suite A East Wing ARS Medicae Building
No. 14, 6 th Avenue, Belleville St Michael Barbados Tel (246) 429 6859Fax (246) 435-0569
Associates forAssociates forInternational DevelopmentInternational Development
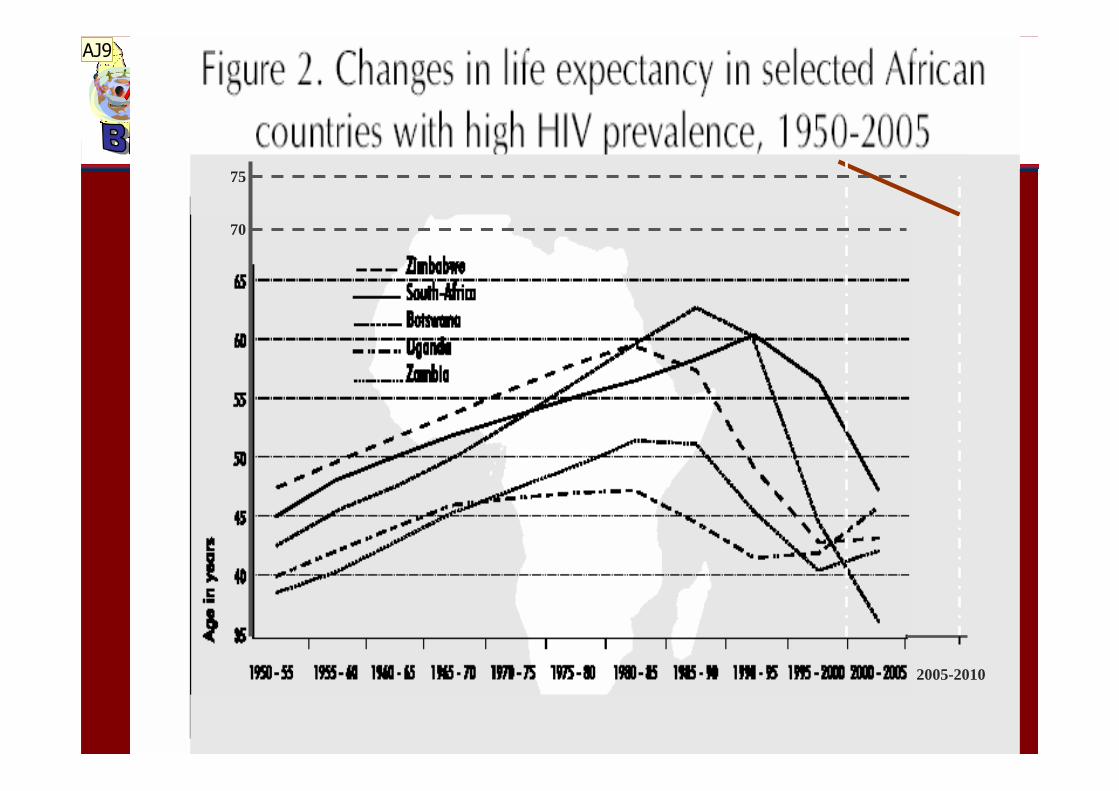
Social and Economic costs of HIV and AIDS
Current issues
Costs, cost-effectiveness & Sustainability
Sarah Ann Adomakoh
Low prevalence estimates indicate, 2 new cases every 3 days, but estimates are as high as 1 new HIV case every 30 hours
� Human suffering
�Morbidity
�Social functioning
�Participation- reduced output
�Reduced Quality of life
� Loss of human capital
�Increased and unexpected mortality in productive age-group
�Reduced Transmission of abilities to next generation
� Child rearing
1980s to 2000Impact of AIDS - lost lives &
livelihoods
HIV/AIDS
Illness or Death
Supply of labour Savings/capital
Prevention & Treatment
Public/Private Expenditure
Actual health expenditure
Socialcapital
GDP
Required health expenditure
HIV/AIDS & the Economic System
Economic impact on affected households
� Before HAART, out of pocket household expenditure due to treatment of HIV/AIDS is an average of 28-62% of annual household income for various subgroups, ranging from 24% for those covered by social welfare and 76% for those not covered
� Post HAART - In 2004 the range narrowed: 10% to 35%
� Survey Data demonstrated following reasons; � Household income did not rise (no return to work) and expenditure fell
due to free access
� Household income fell further and expenditure fell due to lack of funds and unmet needs
70
75
2005-2010
AJ9
Slide 6
AJ9 SarahYou just need to make passing reference to this slide and point to the exact location on the graph where you are making the comparisonAlies Jordan; 14/10/2005
Microeconomic and macroeconomic, impact on development.
- Microeconomic impact on households, families, local/
regional food production, and productivity of various
economic sectors.
- Macroeconomic models to take into
account the impact on human capital.
A new Era
The Cost of Sustaining lives through Treatment
Those who don’t know are almost 2 thirds of those with HIV!!!
Reduction in deaths by 42% and maintaining this trend- overall apprx. 73% reduction in deaths between 2001 and 2004
Sexual practices, mixing
Transmission probabilities -effectiveness of viral suppression
Access to treatment & VCT
Prevention efforts
Reported cases - PLWHA
Impact issues on Universal access to ARV Treatment, care,support
- Are we maximising efficiency in the delivery of our programs?
� Maximising outcomes?� cost savings , benefits and cost effectiveness
� Minimizing costs? � What is an adequate drug pricing strategy for Barbados � Service scope?� The right balance: Integratign within exisiting services and prevention programmes� Shared care between private and public settings� Effective and Community care approaches � Shared staff within institutions
- Balance of Coverage - Are we promoting equity in access to ART ? � Enabling environment – promote more trust , respect, less stigma, discrimination, rejection � Equity of access for higher SES: reverse sitiation most developing contries � Making patients pay can reduce effectivenss of outcomes � Equity of access for kep populations - effect of Stigma discrimination in households and
health care settings
� Can we sustain a positive impact of ARVs on the epidemic at minimised cost to minimise negative impacts ?• Sustainability plans:
� health financing and investments
� What are the other global impacts of the universal program ( accoridng to current and planned configurations) on public health, economic, social and human development ?
No. of clients followed up and on HAART at the LRU
0
200
400
600
800
1000
1200
2003 2004 2005 2006
Year
No.
No. of clientsfollowed up
No. of clients onHAART
Outcomes: Key Findings
� Overall reduction in deaths of clinic registered patients by approximately 56%
� Median CD4 rise of over 100cells/mm3 observed in AIDS patients
� 85% of patients achieving greater than 95% adherence (LB41)
� Baseline total cost of inpatient care for HIV patients is $1,367,964 compared with the inpatient cost post HAART of $810,045 (02/3) $457,391 (03/4); $465,052 (04/5)
� Therefore, cost of inpatient care reduced by 40.8% in first year and 66% between 2001 and 2004.
� Rise in patients attending clinic from apprx. 380 to 744 between 2003 to 2004
� Overall reduction in AIDS related events observed in clinic attendees
� Rise in outpatient visits by 128%
� Reduction in death rate 18 months by 42%
� Apprx. Incremental cost effe9ctiveness ratio: $2171 per death averted (life year saved in 2002) increased to $13,173 per death averted between 2002 and 2004.
Sustainability- Clinical effectiveness is not enough!!
Direct BenefitsPotential reductions in hospitalization costsPrevention - Potential reductions in new infections due to lower viral loads
� Indirect Benefits� Increased Quality of Life?� Increased productivity of the labour force� Increased stability and longevity of families- child rearing , impact on next
generation – sustainable development
� Returns on investment � Increased economic and social Productivity and increased saving� Shared costs � Increase client base to wider population beyond borders for cost recovery
� Reduce impact to other sectors � Save money
HRQoLHRQoL Short Form 29Short Form 29--itemitem--Barbados (SF29Barbados (SF29--Bds.) Bds.) Measures Physical and Mental Components of Measures Physical and Mental Components of
Health Health
Issues of Concern to Employersin the ARV Treatment Era
� Stigma: Life years lost due to mental health impact of non-disclosure of employees
� Over 30% of employed PLWHA leave workforce long before health effects take hold. Average up to 2 years before AIDS onset
� 13% left as result of enacted stigma or overt discrimination
� Almost 20% would not disclose, manifested social cost in terms of reduced mental health and quality of life
� Economic: mental health problems � reduced quality and output
� Employer denial of threat of HIV � self stigma enforces failure to act
� Refusal to face the cost of mitigation - what will it cost?
� Insurance firms may feel no impact due to failure to claim through company health plans (delayed effect of stigma)
� Households spendings and savings decline instead
� Impact of delayed stigma in higher SES on sectors and economy islethal and profound
Employee level impact- what lies beneath?
� Due to all forms of stigma and discrimination…..
� Partial or complete withdrawal from social and economically productive life
� ……mental health impact is observed
� …….Poor Quality of Life
� Leading to � Pressure on existing workers
� reduced output,
� days lost from work due to self stigma.
� Low self esteem, vitality and poor mental health as a result of non disclosure and inability opt openly seek effective counseling support
�Will reduce levels and quality of output
Staff won’t die, but……………
Strategies for Reducing the Burden on Employers
� Diminish the size of the burden.
�Invest in HIV prevention interventions.
�Invest in HIV/AIDS care and treatment interventions.
�Invest in replenishment of human capital (training).
Only sure cost-effective response
CE depends on cost of treatment, survival rate, level of employee, etc
Mitigation strategy to provide staff back up - need s close assessment off at risk workers to be CE• Shift the burden onto others
The Greatest Threat -Stigma & Discrimination
Source: S Adomakoh PhD Thesis
The case of William, age 35
� What do you do to relieve your depression?
“When I get depressed I take a long walk from the hostel to Browns Beach and walk on the beach instead”
� Instead of what?“Instead of the alternative (laughs and throws head back)”
� Which is what?
“I would get a gun and put it to my head”“……….But I am trying to stay alive to see my 13 year boy graduate
– he is much cleverer than I was and has a future………”
� William was also abusing substances to self treat his depression. This ranged from Marijuana, to crack to pethadine. He was also on HAART.
� William died 2 weeks later.
Increased Cost-effectiveness optimize therapeutic strategies depends on :
� Optimal pricing of � brand name drugs (non-generics)� Use of generic drugs.
� Increased tolerance, adherence, and acceptability of treatment (increased life years saved)
• 85% of patients achieving greater than 95% adherence
� Enabling environment � Policies regarding health fencing, equity of access issues
� Increased numbers of asymptomatic HIV and HIV negative patients attracted to the new programme through � a strengthened voluntary counseling and testing