Laparoscopic Colorectal Surgery After 80 John Marks MD MDSection of Colon and Rectal Surgery Lankenau Hospital, Wynnewood PA John Marks MD Chief: Section of Colorectal Surgery Main Line Health System Professor: Lankenau Institute of Medical Research Director: Fellowship in Minimally Invasive Colorectal Surgery and Rectal Cancer Management Speakers Disclosures Covideon- educational grant support, consultant, speakers bureau Wolfe- consultant, speakers bureau Stryker- consultant, speakers bureau Glaxo Smith Kline- consultant Zassi- consultant, honoraria Surgiquest- Scientific Advisory Board Adolor- speakers bureau Can we? Laparoscopic Colorectal Surgery After 80 Can we? Should we? What’s the issue? What is the next Challenges of Laparoscopic Colorectal Surgery It’s hard. Need to learn it or the surgeon will take a wrong turn
Transcript
10/12/2008
1
Laparoscopic Colorectal Surgery After 80
John Marks MD
MDSection of Colon and Rectal SurgeryLankenau Hospital, Wynnewood PA
John Marks MD Chief: Section of Colorectal Surgery Main Line Health System
Professor: Lankenau Institute of Medical Research
Director: Fellowship in Minimally Invasive Colorectal Surgery and Rectal Cancer Management
Speakers Disclosures
Covideon- educational grant support, consultant, speakers bureau
Wolfe- consultant, speakers bureau , pStryker- consultant, speakers bureauGlaxo Smith Kline- consultantZassi- consultant, honorariaSurgiquest- Scientific Advisory BoardAdolor- speakers bureau
Can we?
Laparoscopic Colorectal Surgery After 80
Can we?Should we?
What’s the issue?
What is the next Challenges of Laparoscopic Colorectal Surgery
It’s hard.
Need to learn it or the surgeon will take a wrong turn
10/12/2008
2
Commonly claimed “Problems” laparoscopic colorectal surgery in
the elderly:
1. “Can’t do it”2 “Takes too long”2. Takes too long3. “Dangerous in the elderly”4. “Want to get my hands on
things”5. “Tissue too fragile”
“Convictions are more dangerous enemies of truth than lies.”
Friedrich Wilhelm Nietzche
USA150,000 new colorectal cancers/ year
100,000 colon50 000 rectal
2007
50,000 rectal
Benign diseases
5-15% of colon resectionsdone laparoscopically
% Colorectal Cancer Treated Laparoscopically ????
S. Korea>50%?
Always < 20%
>50%?
A Comparative Evaluation A Comparative Evaluation of Laparoscopicof Laparoscopic--Assisted Assisted
VersusVersusOpen Colectomy for Colon CancerOpen Colectomy for Colon Cancer
COST Study Group TrialCOST Study Group Trial
John Marks, MDJohn Marks, MDWynnewood, PennsylvaniaWynnewood, Pennsylvania
N Engl J Med. 2004 May 13;N Engl J Med. 2004 May 13;350(20):2050350(20):2050--5959
COST Study Group COST Study Group Surgical ParticipantsSurgical Participants
H. AsbunH. Asbun D. FowlerD. Fowler D. Litwin D. Litwin R. Schlinkert R. Schlinkert R. BellR. Bell E. Froines E. Froines J. Lukaszczyk A. Senagore J. Lukaszczyk A. Senagore D. BirchD. Birch J. Greif J. Greif P. Marcello P. Marcello C. Simmang C. Simmang E. BirnbaumE. Birnbaum R. Gould R. Gould J. MarksJ. Marks J. Stauffer J. Stauffer R. Boorse R. Boorse R. Hartmann R. Hartmann S. Oommen S. Oommen E. Suddleson E. Suddleson T. Brown T. Brown G. Hoffman G. Hoffman A. Ortega A. Ortega J. Sutton, Jr. J. Sutton, Jr. B Ch i t G H bb d IIB Ch i t G H bb d II A P kA P k L S tL S tB. Christensen G. Hubbard II B. Christensen G. Hubbard II A. Park A. Park L. Swanstrom L. Swanstrom W. Chapman III J. Hyder W. Chapman III J. Hyder D. Rattner D. Rattner R.C. Thomas, Jr R.C. Thomas, Jr R. Cleary R. Cleary R. Josloff R. Josloff W. T. Reilly W. T. Reilly C. Thibault C. Thibault C. Delaney C. Delaney L. B. Katz L. B. Katz W. K. Ruffin W. K. Ruffin A. Tootla A. Tootla A. Ferrara A. Ferrara H. C. Kim H. C. Kim B. Salky B. Salky S. Wexner S. Wexner A. Fine A. Fine S. Larach S. Larach L. Sand L. Sand R. Whelan R. Whelan R. A. Forse R. A. Forse D. Lauter D. Lauter B. Schirmer B. Schirmer S. WohlgemuthS. Wohlgemuth
T. YoungT. Young--FadokFadokOthers: G. Schroeder, M. O’Connell, J. Weeks, L. Healy, E. Green, Others: G. Schroeder, M. O’Connell, J. Weeks, L. Healy, E. Green,
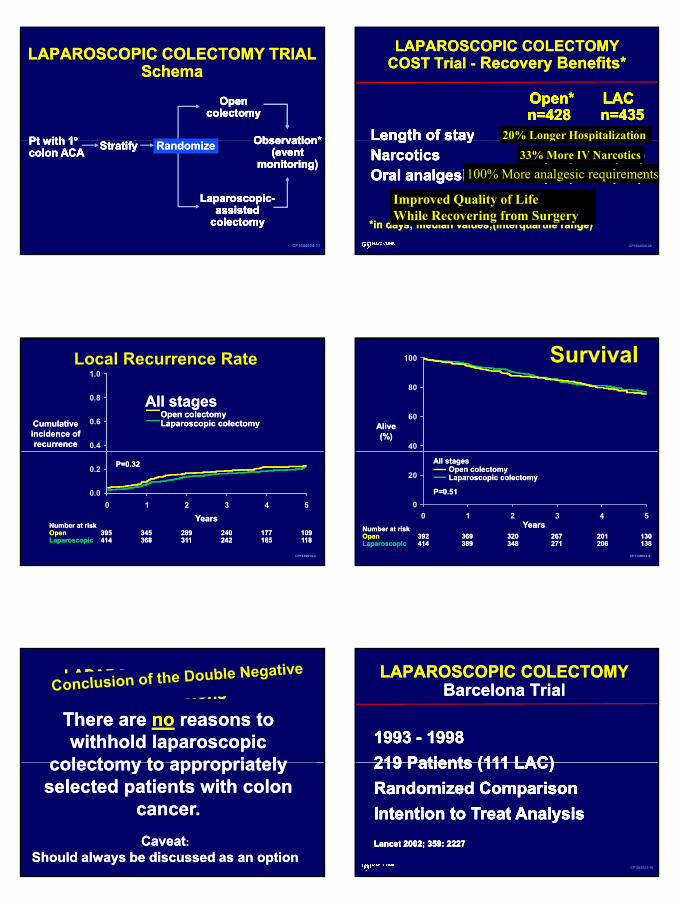
There are There are nono reasons to reasons to withhold laparoscopic withhold laparoscopic
colectomy to appropriatelycolectomy to appropriatelylaparoscopic colectomy to laparoscopic colectomy to appropriately selected appropriately selected patients with colon cancer.patients with colon cancer.
CaveatCaveat::Should always be discussed as an optionShould always be discussed as an option
colectomy to appropriately colectomy to appropriately selected patients with colon selected patients with colon
cancer.cancer.
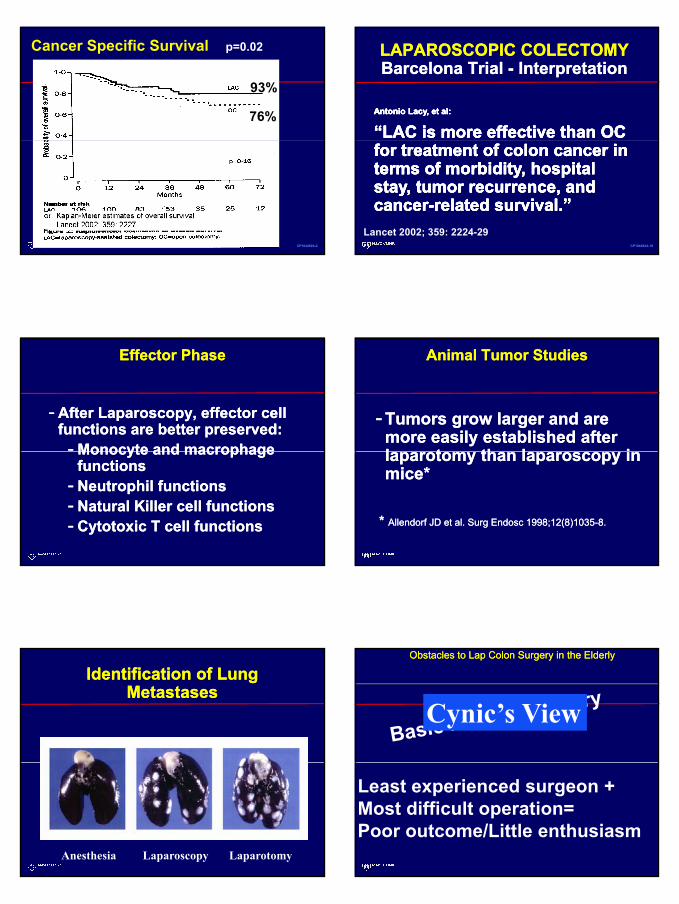
LAPAROSCOPIC COLECTOMY LAPAROSCOPIC COLECTOMY Barcelona TrialBarcelona Trial
LAPAROSCOPIC COLECTOMY LAPAROSCOPIC COLECTOMY Barcelona Trial Barcelona Trial -- InterpretationInterpretation
Antonio Lacy, et al:Antonio Lacy, et al:
“LAC is more effective than OC “LAC is more effective than OC Antonio Lacy, et al:Antonio Lacy, et al:
“LAC is more effective than OC “LAC is more effective than OC
CP1044924-18
for treatment of colon cancer in for treatment of colon cancer in terms of morbidity, hospital terms of morbidity, hospital stay, tumor recurrence, and stay, tumor recurrence, and cancercancer--related survival.”related survival.”
for treatment of colon cancer in for treatment of colon cancer in terms of morbidity, hospital terms of morbidity, hospital stay, tumor recurrence, and stay, tumor recurrence, and cancercancer--related survival.”related survival.”
Lancet 2002; 359: 2224-29
Effector PhaseEffector Phase
-- After Laparoscopy, effector cell After Laparoscopy, effector cell functions are better preserved:functions are better preserved:-- Monocyte and macrophageMonocyte and macrophageMonocyte and macrophage Monocyte and macrophage
functionsfunctions-- Neutrophil functionsNeutrophil functions-- Natural Killer cell functionsNatural Killer cell functions-- Cytotoxic T cell functions Cytotoxic T cell functions
Animal Tumor StudiesAnimal Tumor Studies
-- Tumors grow larger and are Tumors grow larger and are more easily established after more easily established after l t th l il t th l ilaparotomy than laparoscopy in laparotomy than laparoscopy in mice*mice*
* * Allendorf JD et al. Surg Endosc 1998;12(8)1035Allendorf JD et al. Surg Endosc 1998;12(8)1035--8.8.
Identification of Lung Identification of Lung MetastasesMetastases
Anesthesia Laparoscopy Laparotomy
Obstacles to Lap Colon Surgery in the ElderlyObstacles to Lap Colon Surgery in the Elderly
Cynic’s View
Least experienced surgeon + Most difficult operation= Poor outcome/Little enthusiasm
•• Rectal CancerRectal Cancer•• Transverse colon cancerTransverse colon cancer•• Acutely obstructed/perforated cancerAcutely obstructed/perforated cancer•• Advanced local disease (T4)Advanced local disease (T4)Advanced local disease (T4)Advanced local disease (T4)•• Stage IV diseaseStage IV disease•• ASA classification IV or VASA classification IV or V•• Any concurrent or previous malignant tumorAny concurrent or previous malignant tumor•• Associated GI diseasesAssociated GI diseases•• Pregnant womenPregnant women
No Specific Data regarding the elderly
We Can, but should We???We Can, but should We???
Challenges for laparsocopic Challenges for laparsocopic surgery in the elderlysurgery in the elderly














![Liver resection for metastatic colorectal cancer - [email protected]](https://static.documents.pub/doc/80x56/620633768c2f7b1730055cf8/liver-resection-for-metastatic-colorectal-cancer-emailprotected.jpg)


