49
Substance Abuse in Children and Adolescents Jessica Stewart CEP 504 – Fall 2011
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | helena-miles |
| View: | 214 times |
| Download: | 0 times |

Substance Abuse in Children and AdolescentsJessica StewartCEP 504 – Fall 2011

street names Whippersnappers Hoodlums Rugrats Ankle Biters Punks Tweens
Just Kidding…

The vast majority of people who suffer from addiction encountered the beginnings of their illness when they were teenagers. Ninety-five percent of people who are dependent on alcohol or other drugs started before they were 20 years old.
- Dr. Mark Willenbring, Director of Treatment and Recovery Research at the National Institute on Alcohol Abuse and Alcoholism

It is also important to keep in mind that substance abuse in adolescence does not always lead to substance addiction later in life.
(Heyman, 2009)

trends in drug use Slow but steady increase in overall illicit
drug use over the past several years
Any Illicit Drug Use
8th-Graders 10th-Graders 12th-Graders
2007 2008 2009 2010 2007 2008 2009 2010 2007 2008 2009 2010
Lifetime 19 19.6 19.9 21.4 35.6 34.1 36 37 46.8 47.4 46.7 48.2
Past Year 13.2 14.1 14.5 [16.0] 28.1 26.9 29.4 30.2 35.9 36.6 36.5 38.3
Past Month 7.4 7.6 8.1 [9.5] 16.9 15.8 17.8 18.5 21.9 22.3 23.3 23.8
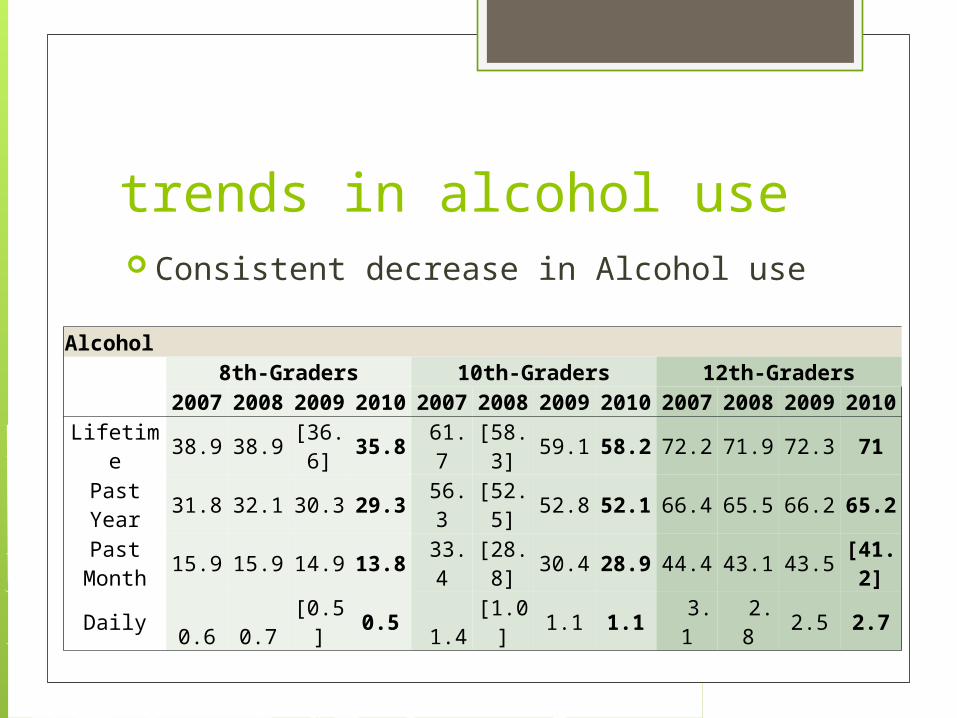
trends in alcohol use Consistent decrease in Alcohol use
Alcohol 8th-Graders 10th-Graders 12th-Graders 2007 2008 2009 2010 2007 2008 2009 2010 2007 2008 2009 2010
Lifetime 38.9 38.9 [36.6] 35.8 61.7 [58.3] 59.1 58.2 72.2 71.9 72.3 71
Past Year 31.8 32.1 30.3 29.3 56.3 [52.5] 52.8 52.1 66.4 65.5 66.2 65.2
Past Month 15.9 15.9 14.9 13.8 33.4 [28.8] 30.4 28.9 44.4 43.1 43.5 [41.2]
Daily 0.6 0.7 [0.5] 0.5 1.4 [1.0] 1.1 1.1 3.1 2.8 2.5 2.7

trends in marijuana use Daily marijuana use increased among 8th, 10th, and
12th graders from 2009 to 2010. Among 12th graders, use was at its highest point since the early 1980s, at 6.1 percent
THC levels in marijuana are at their highest ever – 9.6 percent in 2007
Marijuana/Hashish
8th-Graders 10th-Graders 12th-Graders
2007 2008 2009 2010 2007 2008 2009 2010 2007 2008 2009 2010
Lifetime 14.2 14.6 15.7 17.3 31 29.9 32.3 33.4 41.8 42.6 42 43.8
Past Year 10.3 10.9 11.8 [13.7] 24.6 23.9 26.7 27.5 31.7 32.4 32.8 34.8
Past Month 5.7 5.8 6.5 [8.0] 14.2 13.8 15.9 16.7 18.8 19.4 20.6 21.4
Daily 0.8 0.9 1 [1.2] 2.8 2.7 2.8 [3.3] 5.1 5.4 5.2 [6.1]

a few more trends Teen smoking rates are at their lowest point
in the history of the survey. After several years of decline, current and
past-year use of ecstasy(MDMA) has risen among 8th and 10th graders.
Amphetamine use peaked in 1996 at 15.5 percent and decreased to 8.9 percent in 2010.
Methamphetamine use declined from 6.5 percent in 1999 to 2.2 percent in 2010.

are children and adolescents more vulnerable to substance abuse? Immature brain of adolescents associated with poor
judgment, impulsivity, inability to contemplate consequences
Greater feelings of social disinhibition with alcohol (less shyness in social settings reinforces use)
Lower sensitivity to intoxicating effects of alcohol resulting in use of larger amounts
Combination of these effects may contribute to initial decision to use and make experience rewarding enough to repeat
May lead to substance use disorders-abuse and dependency

adolescent brain development During childhood and adolescent, the
brain is still plastic Parietal lobe (spatial reasoning), frontal lobe
(planning and impulse control) and temporal lobe (language and non-verbal communication) are all still developing
So how does drug and alcohol use during this stage of development affect the brain?

adolescent brain development Alcohol produces greater cognitive
dysfunctions in adolescents (Spear, 2002). more disruption in memory impairment of neurotransmission in
hippocampus and cortex Adolescents with a history of alcohol use
disorder have a smaller hippocampus (Tapert & Schweinsburg, 2005) the hippocampus encodes new information to
the memory

adolescent brain development Heavy drug use during times of critical brain
development may cause permanent changes in the way the brain works and responds to rewards and consequences:

adolescent brain development Methamphetamines and cocaine are known to
cause a flood of dopamine into the brain – which is one reason they are so addictive: their use is associated with a tremendous sense of reward. It has been found, though, that cocaine addicts have a decreased sense of perception for certain types of reward, and it is thought that cocaine, and meth, over time override the brain’s ability to sense rewards accurately. The effects of these drugs can be devastating to the ability of the user to feel satisfaction from life.
adolescent brain development Adolescent perceptive abilities are not fully
developed. Adults use their frontal lobes to determine facial expressions, while teens use their amygdala – the more primitive brain structure that is associated with emotions such as worry or fear. Adult perception is more accurate. Marijuana, like all drugs, changes perception. And like most drugs, it provokes perception that is fearful, emotional, defensive, and often inaccurate. If marijuana use is chronic or constant enough to hinder perceptual maturation, an adolescent user may misinterpret failures in school, work, and relationships, which in turn re-enforce the desire to retreat to drugs.

adolescent brain development the human brain is sculpted by
experience. Pruning of unused neural connections and strengthening of regularly used neural connections occurs throughout childhood and adolescence If the brain is not developing a pattern of
logical thought (pre-frontal cortex)during this plastic stage, the neurons that are used for logical thinking will be pruned.

risk factors - individual Begins use at an early age (10-12 years old) Attention Deficit Hyperactivity Disorder History of abuse (physical, emotional or sexual) Learning disabilities Excessive aggression, impulsivity or risk-taking Mental health disorders such as depression, anxiety
and conduct disorders Rebelliousness Unable to control impulses Low self-esteem Poor social skills

risk factors - family Family history of substance abuse (even smoking) Poor child-parent relationships Lack of supervision Enabling Family conflict Inconsistent or severe discipline Conditional love Unrealistically high expectations from parents Depression, anxiety or trauma within the parents Access to alcohol or drugs in the home

risk factors - community Availability of alcohol/other drugs Transitions and mobility (moving a lot) Low neighborhood attachment &
community disorganization Poverty
protective factors - individual High self esteem Treatment of depression, anxiety or
other mental health issues Tutoring, counseling, medication,
resolutions of behavioral problems, and better supervision in attending school
Religious or spiritual involvement
protective factors - family Family connectedness Positive parenting style Living in a two parent family Higher parent education High parental expectations about school Parental abstinence of drugs and alcohol Religious or spiritual involvement Parental supervision

protective factors - community Positive connection to other adults Safe, supportive, connected neighborhood Strong community infrastructure (services
for those in need) Local, state policies and practices that
support healthy norms and child-youth programs
Range of opportunities in the community for meaningful youth engagement

physical signs of substance abuse Changes in sleep patterns Speech is slurred, or talking excessively and rapidly. Red, watery or glassy eyes Staggering or walking very slowly. Poor motor coordination. Change in eating habits Shaking hands; excessively sweaty hands; very cold hands. Unusual skin abrasions or bruises; needle marks; rashes around nose and
mouth. Neglecting appearance, not bathing. Nose bleeds; runny nose; sniffing excessively; hacking cough; smoker's
cough. Nausea, throwing up, excessive sweating, dizziness, frequently feeling
faint. Excessive nervousness, irritability, anxiety, restlessness. Irregular heartbeat Paranoid, irrational, or bizarre thoughts.

behavioral signs of substance abuse
Sudden personality changes that include abrupt changes in work or school attendance, quality of work, work output, grades, discipline
Unusual outbreaks of temper Withdrawal from responsibility General changes in overall attitude Loss of interest in hobbies Changes in friends Unusual borrowing of money Stealing items from employer, home or school

what’s a parent to do? Educate themselves about drugs, alcohol and their
child’s world http://www.theantidrug.com
Talk about the use with your teen be honest and specific about your concerns
Don’t make excuses for your teen Be prepared (with info and what you are going to say) Take care of yourself Act now
setting and enforcing new rules getting outside help if necessary
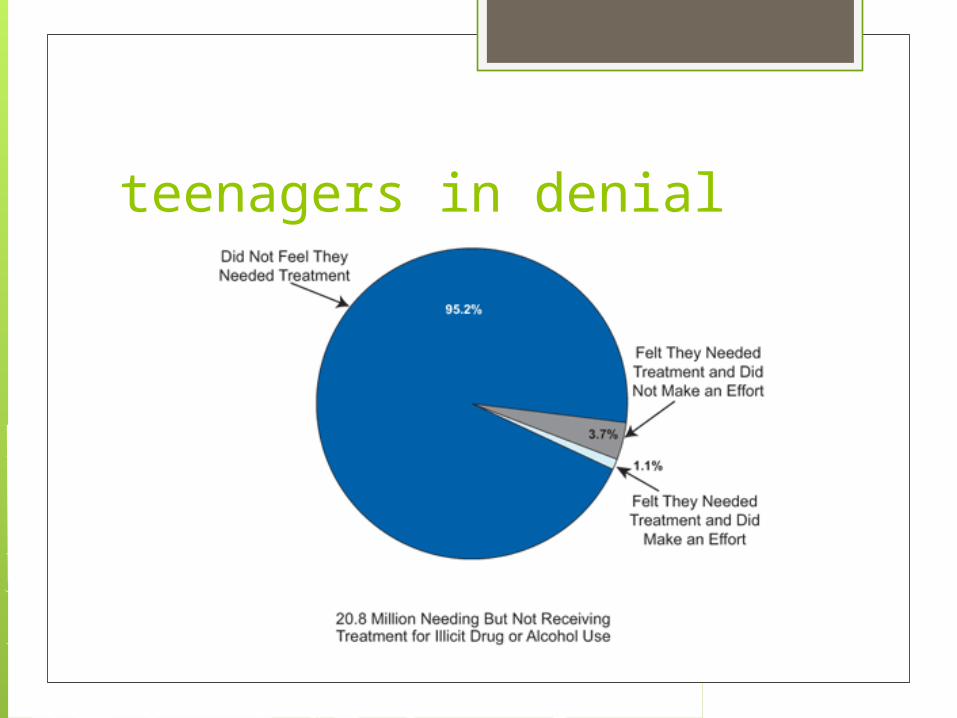
teenagers in denial

getting a teen into treatment Laws vary by state as to whether or not
a parent can force a child into rehab. Court mandated treatment is common In WNY, there are only a few inpatient
treatment facilities specifically for adolescents

treatmentAddiction treatment has three stages
1. Detoxification/Stabilization not treatment - only preparation for
treatment. Detoxification must be followed by continued rehabilitative treatment for lasting improvement.

treatmentAddiction treatment has three stages
2. Rehabilitation Rehabilitation care typically offers an
array of treatment components to help to address the many health and social problems associated with substance use

treatmentAddiction treatment has three stages
3. Continuing Care The first 3-6 months following addiction
treatment is the period of greatest vulnerability to relapse. Continuing care services are designed to monitor the emotional health of recovering people, remind them of their commitment to lifestyle change and support their needs as they attempt the difficult job of living their former lives with a new perspective and resolve.

treatment Treatment for teens can not just be scaled
down adult treatment plans. Adolescents have different concerns and needs have more family difficulties more likely to have psychological problems more likely to have attempted suicide Their alcohol and drug-use patterns are also
different. Teens tend to abuse multiple substances, while
adults are more singular in their focus.

treatment Once in treatment, adolescents seek out
different treatment than adults: favoring group therapy over individual need to have their family included in treatment must have a school-based component if in
inpatient or residential treatment most adult treatment programs are not set up
to deal with the oppositional or acting-out behaviors characteristic of adolescent substance abusers

treatment Adolescent treatment centers must not only address
substance use but help an adolescent navigate the normal developmental tasks of identity formation that are often neglected while using chemicals.
problem solving and social skills need to be learned in order to build self-esteem
Basic trust must be built or rebuilt Basic feelings must be identified and a
language of emotional communications must be established
Coexisting mental health issues such as depression, anxiety and post-traumatic stress disorder (PTSD) must be evaluated
neurofeedback Neurofeedback, also called EEG biofeedback, is a
computer-based technology that teaches the brain to function more efficiently by arousing or calming the nervous system. Using a computer and sensors that detect brain waves, patients learn how to control the brain’s electrical patterns by responding to images on a screen or sounds that reflect the electrical activity in their brain
As patients focus their attention on the screen and work to control their emotions, they receive feedback indicating when their brain waves are in the desired zone. After repeating the process a number of times, the brain waves become conditioned to stay within a certain range, eliminating the need for ongoing neurofeedback sessions.

neurofeedback After just a few sessions, patients often report:
• Improved ability to focus and pay attention• Decreased impulsivity• Better ability to cope • Less anxiety• Improved ability to maintain sobriety
It is non-invasive and has no negative side effects (no chemical or electrical impulses enter the body at any time).
Based on learning - more practice results in more lasting changes
Patient-guided - the patient decides which training they’d like repeated
It creates lasting change - studies show few patients return for the same problem

neurofeedback meets the American Academy of Child and Adolescent
Psychiatry criteria for clinical guidelines established for the treatment of addiction, ADHD, seizure disorders, anxiety, depression and learning disabilities
Patients receiving neurofeedback: Spend more time in treatment Are less dependent on medication Are better able to manage emotional symptoms, such as
anxiety, depression and impulsivity Are more likely to have maintained abstinence one year
after completion of treatment According to a 2005 study published in the American
Journal of Drug and Alcohol Abuse, patients recovering from drug and alcohol addictions have an 80 percent abstinence rate after completing neurofeedback training.
community resources Erie County Medical Center
462 Grider StreetBuffalo, NY 14215(716) 898-3415 Downtown Alcoholism Clinic
1280 Main StreetBuffalo, NY 14209(716) 883-4517
Northern Erie Clinical Services2282 Elmwood AvenueBuffalo, NY 14217(716) 874-5536
Vocational Rehabilitation and Recovery Center c/o Downtown Alcoholism Clinic 1280 Main Street Buffalo, NY 14209 (716) 881-8357

community resources Alcohol & Drug Dependency Services (ADDS)
Renaissance Campus960 Harlem RoadWest Seneca, NY 14224
Renaissance House(716) 821-0391
Promise House(716) 332-3391
Stepping Stones(716) 821-9220
Alcohol and Drug Dependency Services Family Addiction107 Delaware Avenue Suite 555 Statler TowersBuffalo NY 14202(716) 855-0163
Horizon Health Servicesmulitiple locationswww.horizon-health.org

community resources Buffalo General Hospital
Chemical Dependency Outpatient Clinic80 Goodrich Street Buffalo NY 14203(716) 859-1576 ext. 3729
Beacon Center Sheridan Drive3140 Sheridan Drive Buffalo NY 14226(716) 831-1937
Beacon Center Ellicott SquareEllicott Square Building 295 Main Street Suite 112Buffalo NY 14203(716) 853-0243

community resources Elmwood Counseling Clinic
City of Buffalo DSAS656 Elmwood Avenue Suite 201Buffalo NY 14222(716) 886-3982
Genesee-Moselle Counseling ClinicCity of Buffalo DSAS1532 Genesee Street Buffalo NY 14211(716) 891-8334
Lifetime Health Chemical DependencyOutpatient Clinic130 Empire Drive Buffalo NY 14224(716) 668-6170 ext. 5030(716) 668-3600

community resources Mid-Erie Counseling and Treatment Services
Suburban Clinic:1526 Walden Avenue, Suite 400Cheektowaga, New York 14225(716) 895-6700
City Clinic:1131 BroadwayBuffalo, New York 14212(716) 896-7712
BryLin Hospital1263 Delaware AveBuffalo NY 14209 (716) 886-8200
BryLin Williamsville Outpatient Addictions Clinic5225 Sheridan DriveGeorgetown SquareWilliamsville NY 14221 (716) 633-1927

online resources www.samhsa.gov
Substance Abuse and Mental Health Services Administration
www.teens.drugabuse.gov The National Institute on Drug Abuse
www.inspirationsyouth.com www.abovetheinfluence.com http://www.tgcoy.com/addiction
online resources Alcoholics Anonymous
http://www.buffaloaany.org Narcotics Anonymous
http://www.nawny.org

online resources for parents www.timetoact.drugfree.org http://www.byparents-forparents.com/

bibliography - websites www.makeachangewny.org www.samhsa.gov www.nida.nih.gov www.monitoringthefuture.org www.samafoundation.org www.hbo.com/addiction www.timetoact.drugfree.org www.byparents-forparents.com www.tgcoy.com/addiction www.hss.state.ak.us www.adolescent-substance-abuse.com http://www.drugrehabtreatment.com
bibliography - lectures Thomas, K (July7, 2011). Classroom lecture on puberty and
cognitive changes. University at Buffalo, Buffalo, NY.
bibliography – books Doweiko, A. E. (2011). Concepts of chemical dependency.
(Eighth ed.). a Crosse, WI: Brooks/Cole Pub Co.

bibliography – articles Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E.
(2011). Monitoring the Future national results on adolescent drug use: Overview of key findings, 2010. Ann Arbor: Institute for Social Research, The University of Michigan. Monitoring the Future (MTF) is a long-term study of American
adolescents, college students, and adults through age 50. It has been conducted annually by the University of Michigan’s Institute for Social Research since its inception in 1975 and is supported under a series of investigator-initiated, competing research grants from the National Institute on Drug Abuse.

Bibliography - articles Substance Abuse and Mental Health Services Administration, Results
from the 2010 National Survey on Drug Use and Health: Summary of National Findings, NSDUH Series H-41, HHS Publication No. (SMA) 11-4658. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2011. This report presents the first information from the 2010 National
Survey on Drug Use and Health (NSDUH), an annual survey sponsored by the Substance Abuse and Mental Health Services Administration (SAMHSA). The survey is the primary source of information on the use of illicit drugs, alcohol, and tobacco in the civilian, noninstitutionalized population of the United States aged 12 years old or older. The survey interviews approximately 67,500 persons each year. Unless otherwise noted, all comparisons in this report described using terms such as "increased," "decreased," or "more than" are statistically significant at the .05 level.

bibliography – articles Spear, L. P. (2002). Alcohol’s effects on adolescents. Alcohol
Health and Research World, 26(4), 287-291 Tapert, S. & Schweinsburg, A.D. (2005). The human
adolescent brain and alcohol use disorders (p 177 -197), Recent developments in alcoholism, Vol XVII. Washington D.C.: American Psychiatric Press
Heyman, G.M. (2009). Addiction: A disorder of choice. Cambridge, MA: Harvard University Press

















