JMed Genet 1997;34:499-503 Syndrome of the month Pure hereditary spastic paraplegia Evan Reid The hereditary spastic paraplegias are a group of neurological conditions which are character- ised by the presence of progressive spasticity, predominantly affecting the legs. They may be subclassified into pure and complicated forms based on the presence of additional neurological or non-neurological features. (YMed Genet 1997;34:499-503) Keywords: pure hereditary spastic paraplegia; differen- tial diagnosis; molecular genetics Pure hereditary spastic paraplegia (pHSP) The first clear description of pHSP was by Strumpell in 1880,2 who reported a family in which two brothers were affected by a late onset spastic paraplegia. Autosomal dominant inheritance was likely, since their mother was "a little lame". Subsequent reports have described autosomal dominant, autosomal recessive, and X linked recessive patterns of inheritance.' 3-12 Autosomal dominant inherit- ance accounts for approximately 70-80% of families, with autosomal recessive inheritance being responsible for most of the remainder.5 8 X linked recessive inheritance is very rare. PREVALENCE Pure hereditary spastic paraplegia is the most common form of hereditary spastic paraplegia (HSP). '3 A rigorously conducted epidemiologi- cal study in the Cantabria region of Spain sug- gested a prevalence for pHSP of 9.6 per 100 000.14 Department of Medical Genetics, University of Cambridge, Box 134, Addenbrooke's NHS Trust, Cambridge CB2 2QQ, UK E Reid CLINICAL FEATURES The principal clinical feature of pHSP is, by definition, the presence of a progressive spastic paraplegia. Often this is of insidious onset and the abnormal gait is frequently noticed by rela- tives before the affected person becomes aware of it. 8 9 Age at onset may range from early childhood, with delayed motor milestones and "clumsiness", to adult life.5 8 9 Age at onset is not consistent between families, although it is consistent within some families.5 8 9 There is also considerable variation in disease severity. Affected subjects may range from entirely asymptomatic (10-20% of cases) to chair- bound (1 0-1 5% of cases).5 8 9 Although severity tends to increase with disease duration, consid- erable variation is present even when people who have been affected for the same length of time are compared.5 8 Urinary symptoms are common, and 50% of patients may be affected by urinary frequency, urgency, or hesitancy.5 8 9 15-17 Anal sphincter disturbances have been reported but are rare.7 Erectile impotence may occur, although its frequency is unknown.6 Physical examination findings are typical of a spastic paraplegia. However, the degree of hypertonicity is often out of proportion to weakness, and is frequently the most disabling feature.5 Weakness and hypertonicity are usu- ally restricted to the legs, although there have been occasional reports of mild upper limb weakness, and upper limb hyperreflexia is common. 8 Pes cavus is present in 30-50% of cases.5 8 Mild upper limb incoordination may occur and mild distal amyotrophy is well recognised, though rare.5 Unexpected physical signs may be found; ankle jerks are absent and Babinski reflexes plantar in a small proportion of patients.5 8 9 Additional neurological abnor- malities, indicating involvement of systems other than the motor tracts, are frequent. A significant proportion of patients (20-65%) have diminished vibration sense, and a small number have diminished joint position sense.5 89 Subclinical sensory abnormalities affecting these and other modalities may be present in the majority of cases.'8 Attempts have been made to subclassify autosomal dominant pHSP on the basis of clinical features. Harding5 found a bimodal distribution of age of onset and used this to divide families into type I, with age of onset predominantly below 35 years, and type II, with age of onset predominantly over 35 years. Subjects from type II families had a disorder which progressed more rapidly and was more commonly associated with somatosensory and urinary sphincter disturbances than subjects from type I families. Muscular weakness predominated in type II families, while hyper- tonicity was more marked in type I families. However, there was considerable overlap be- tween these two groups and subsequent studies have not consistently supported the concept of two distinct types of pHSP.8 9 No consistent clinical differences are apparent between fami- lies with different inheritance patterns. PATHOLOGY Pathological reports for pHSP are scant and have usually described patients with long 499
Transcript
JMed Genet 1997;34:499-503
Syndrome of the month
Pure hereditary spastic paraplegia
Evan Reid
The hereditary spastic paraplegias are a groupof neurological conditions which are character-ised by the presence of progressive spasticity,predominantly affecting the legs. They may besubclassified into pure and complicated formsbased on the presence of additionalneurological or non-neurological features.(YMed Genet 1997;34:499-503)
Keywords: pure hereditary spastic paraplegia; differen-tial diagnosis; molecular genetics
Pure hereditary spastic paraplegia(pHSP)The first clear description of pHSP was byStrumpell in 1880,2 who reported a family inwhich two brothers were affected by a lateonset spastic paraplegia. Autosomal dominantinheritance was likely, since their mother was"a little lame". Subsequent reports havedescribed autosomal dominant, autosomalrecessive, and X linked recessive patterns ofinheritance.' 3-12 Autosomal dominant inherit-ance accounts for approximately 70-80% offamilies, with autosomal recessive inheritancebeing responsible for most of the remainder.5 8
X linked recessive inheritance is very rare.
PREVALENCE
Pure hereditary spastic paraplegia is the mostcommon form of hereditary spastic paraplegia(HSP). '3 A rigorously conducted epidemiologi-cal study in the Cantabria region of Spain sug-gested a prevalence for pHSP of 9.6 per100 000.14
CLINICAL FEATURESThe principal clinical feature of pHSP is, bydefinition, the presence of a progressive spasticparaplegia. Often this is of insidious onset andthe abnormal gait is frequently noticed by rela-tives before the affected person becomes awareof it. 8 9 Age at onset may range from earlychildhood, with delayed motor milestones and"clumsiness", to adult life.5 8 9 Age at onset isnot consistent between families, although it isconsistent within some families.5 8 9 There isalso considerable variation in disease severity.Affected subjects may range from entirelyasymptomatic (10-20% of cases) to chair-bound (10-15% of cases).5 8 9Although severitytends to increase with disease duration, consid-erable variation is present even when peoplewho have been affected for the same length of
time are compared.5 8 Urinary symptoms arecommon, and 50% of patients may be affectedby urinary frequency, urgency, orhesitancy.5 8 9 15-17 Anal sphincter disturbanceshave been reported but are rare.7 Erectileimpotence may occur, although its frequency isunknown.6
Physical examination findings are typical of aspastic paraplegia. However, the degree ofhypertonicity is often out of proportion toweakness, and is frequently the most disablingfeature.5 Weakness and hypertonicity are usu-ally restricted to the legs, although there havebeen occasional reports of mild upper limbweakness, and upper limb hyperreflexia iscommon. 8 Pes cavus is present in 30-50% ofcases.5 8 Mild upper limb incoordination mayoccur and mild distal amyotrophy is wellrecognised, though rare.5 Unexpected physicalsigns may be found; ankle jerks are absent andBabinski reflexes plantar in a small proportionof patients.5 8 9 Additional neurological abnor-malities, indicating involvement of systemsother than the motor tracts, are frequent. Asignificant proportion of patients (20-65%)have diminished vibration sense, and a smallnumber have diminished joint positionsense.5 8 9 Subclinical sensory abnormalitiesaffecting these and other modalities may bepresent in the majority of cases.'8Attempts have been made to subclassify
autosomal dominant pHSP on the basis ofclinical features. Harding5 found a bimodaldistribution of age of onset and used this todivide families into type I, with age of onsetpredominantly below 35 years, and type II,with age of onset predominantly over 35 years.Subjects from type II families had a disorderwhich progressed more rapidly and was morecommonly associated with somatosensory andurinary sphincter disturbances than subjectsfrom type I families. Muscular weaknesspredominated in type II families, while hyper-tonicity was more marked in type I families.However, there was considerable overlap be-tween these two groups and subsequent studieshave not consistently supported the concept oftwo distinct types of pHSP.8 9 No consistentclinical differences are apparent between fami-lies with different inheritance patterns.
PATHOLOGYPathological reports for pHSP are scant andhave usually described patients with long
499
500
standing disease. The principal pathologicalfinding is of axonal degeneration involving theterminal ends of the longest fibres of the corti-cospinal tracts and dorsal columns. Thespinocerebellar tracts are involved to a lesserdegree. The cell bodies of the degeneratingfibres are apparently normal; the process hasbeen described as "dying back" of the nervefibre endings. There is no evidence of primarydemyelination and no abnormality of peri-pheral nerves, dorsal roots, or dorsal root gan-glia has been reported.'9
DIFFERENTIAL DIAGNOSIS AND INVESTIGATIONSThe diagnosis of pHSP in a family where sev-eral members have typical clinical features isrelatively straightforward. Standardneurological investigations should be usedselectively to exclude alternative diagnoses.Magnetic resonance imaging may show spinalcord atrophy, particularly in the cervicalregion."3 Peripheral nerve conduction studiesare almost always normal.5 20 21 Cervical soma-tosensory evoked potentials and central motorconduction studies are abnormal in the major-ity of cases, although unfortunately do not pro-vide a means for early detection of affectedfamily members."-4 Interestingly, brain stemauditory evoked potentials and visual evokedp.otentials are abnormal in a minority of cases.9
Other genetic conditions to be considered inthe differential diagnosis include dopa respon-sive dystonia, which should actively be ex-cluded in families where age of onset is earlyand sensory signs are absent, particularly ifthere is marked diurnal variation of spasticity.Dramatic and sustained improvement of symp-toms occurs with small doses of L-dopa.'5 Theclinical picture should allow exclusion of thespinocerebellar syndromes and Machado-Joseph disease, in which ataxia is a much moreprominent feature. Adult onset forms ofadrenoleucodystrophy, Krabbe's leucodystro-phy, and metachromatic leucodystrophy mayrarely present with spastic paraplegia, and canbe detected with appropriate biochemicaltests.26 Atypical Friedreich's ataxia should alsobe considered, since a proportion of patientshomozygous for the frataxin gene triplet repeatexpansion have retained or exaggerated lowerlimb reflexes and upgoing plantar responses.27The differential diagnosis is more extensive
in sporadic cases of spastic paraplegia and, inaddition to the above, includes structural spinalcord lesions, intracranial parasagittal spaceoccupying lesions, multiple sclerosis, myelopa-thies associated with deficiencies of vitaminB12 or E, and abetalipoproteinaemia. Infectiveconditions including tertiary syphilis, HTLV1infection causing tropical spastic paraparesis,and the myelopathy associated with the ac-quired immune deficiency syndrome should beconsidered, although the clinical picture wouldbe not entirely typical of pHSP."6
DIAGNOSIS IN AT RISK FAMILY MEMBERS
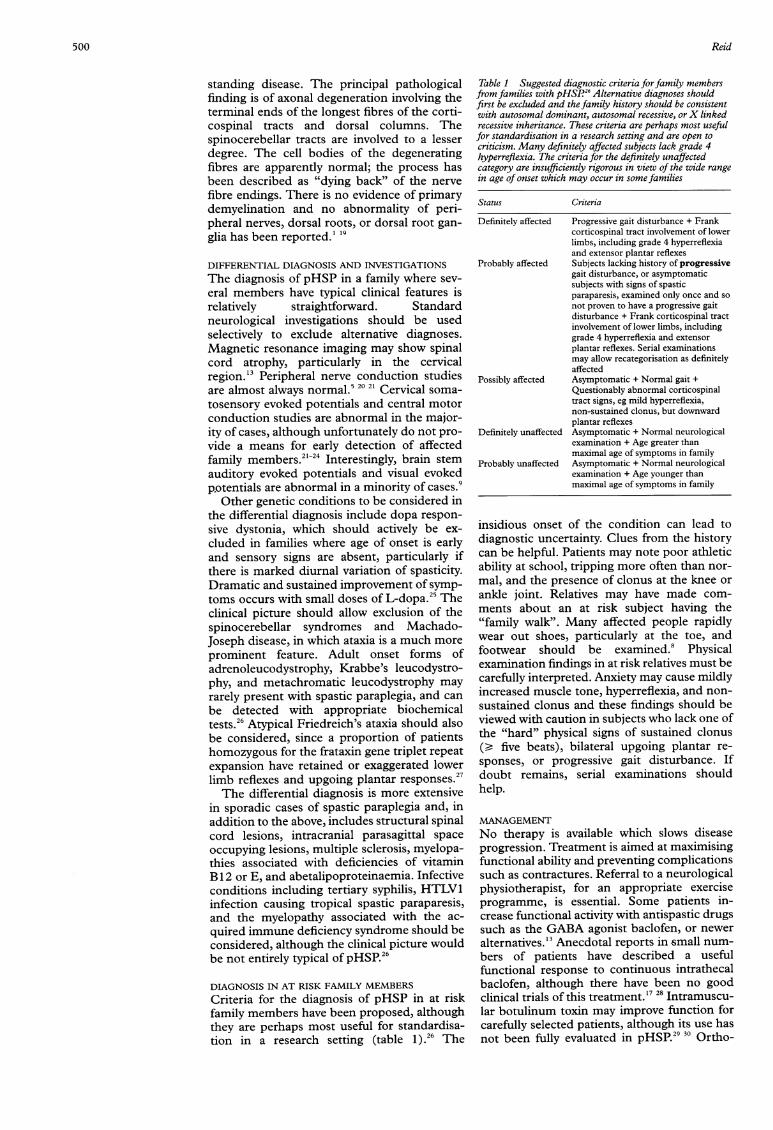
Criteria for the diagnosis of pHSP in at riskfamily members have been proposed, althoughthey are perhaps most useful for standardisa-tion in a research setting (table 1).26 The
Table 1 Suggested diagnostic criteria forfamily membersfrom families with pHSP.2' Alternative diagnoses shouldfirst be excluded and the family history should be consistentwith autosomal dominant, autosomal recessive, orX linkedrecessive inheritance. These criteria are perhaps most usefulfor standardisation in a research setting and are open tocriticism. Many definitely affected subjects lack grade 4hyperreflexia. The criteria for the definitely unaffectedcategory are insufficiently rigorous in view of the wide rangein age of onset which may occur in some families
Status Criteria
Definitely affected Progressive gait disturbance + Frankcorticospinal tract involvement of lowerlimbs, including grade 4 hyperreflexiaand extensor plantar reflexes
Probably affected Subjects lacking history of progressivegait disturbance, or asymptomaticsubjects with signs of spasticparaparesis, examined only once and sonot proven to have a progressive gaitdisturbance + Frank corticospinal tractinvolvement of lower limbs, includinggrade 4 hyperreflexia and extensorplantar reflexes. Serial examinationsmay allow recategorisation as definitelyaffected
Possibly affected Asymptomatic + Normal gait +Questionably abnormal corticospinaltract signs, eg mild hyperreflexia,non-sustained clonus, but downwardplantar reflexes
Definitely unaffected Asymptomatic + Normal neurologicalexamination + Age greater thanmaximal age of symptoms in family
Probably unaffected Asymptomatic + Normal neurologicalexamination + Age younger thanmaximal age of symptoms in family
insidious onset of the condition can lead todiagnostic uncertainty. Clues from the historycan be helpful. Patients may note poor athleticability at school, tripping more often than nor-mal, and the presence of clonus at the knee orankle joint. Relatives may have made com-ments about an at risk subject having the"family walk". Many affected people rapidlywear out shoes, particularly at the toe, andfootwear should be examined.8 Physicalexamination findings in at risk relatives must becarefully interpreted. Anxiety may cause mildlyincreased muscle tone, hyperreflexia, and non-sustained clonus and these findings should beviewed with caution in subjects who lack one ofthe "hard" physical signs of sustained clonus(D five beats), bilateral upgoing plantar re-sponses, or progressive gait disturbance. Ifdoubt remains, serial examinations shouldhelp.
MANAGEMENTNo therapy is available which slows diseaseprogression. Treatment is aimed at maximisingfunctional ability and preventing complicationssuch as contractures. Referral to a neurologicalphysiotherapist, for an appropriate exerciseprogramme, is essential. Some patients in-crease functional activity with antispastic drugssuch as the GABA agonist baclofen, or neweralternatives."' Anecdotal reports in small num-bers of patients have described a usefulfunctional response to continuous intrathecalbaclofen, although there have been no goodclinical trials of this treatment."7 28 Intramuscu-lar botulinum toxin may improve function forcarefully selected patients, although its use hasnot been fully evaluated in pHSP.29 30 Ortho-
Reid
Pure hereditary spastic paraplegia
paedic surgery, usually release of contracturesand tenotomies, may rarely have a role, butrequires very careful assessment of the likelyconsequences of the procedure on gait.
GENETIC COUNSELLING
The often late onset ofpHSP and the variabil-ity of age of onset within families showingdominant inheritance means that it may beimpossible to reassure clinically normal youngadults who are at 50% prior risk of havinginherited the disease gene. The data ofHarding5 on type I families indicate that theclinically normal offspring ofan affected parenthave, at the age of 20, a 24% chance of havingthe abnormal gene, and at the age of 45, a 9%chance of having inherited the abnormal gene(table 2).5 It should be emphasised that thesedata are only applicable to families in which theage of onset for the condition is predominantlyunder 35 years. The risk figures are almost cer-tainly overestimates, since they are derivedfrom an age at onset of symptoms cumulativefrequency curve. The degree of reductionwhich can be made when an at risk patient hasno signs is unknown. Predictive testing may befeasible for at risk subjects from large familieswhere definite linkage is established.The frequent occurrence of asymptomatic
subjects means that every effort should bemade to examine both parents of sibs withapparently recessive pHSP. If both parents are
normal, recessive inheritance is most likely.Non-penetrance (only a few well documentedcases exist8 13) or gonadal mosaicism in a parentare alternative possibilities. If both parents ofaffected sibs cannot be examined, empiricalfigures derived by Harding5 (and only applica-ble to type I families) indicate a 1/6 chance thatone parent was affected. The risks to theoffspring of the affected sibs are therefore 1/12.No empirical figures are available for the risksto offspring of apparently sporadic cases, wherein addition to non-penetrance in a parent a newdominant mutation is a possibility.Although X linked inheritance cannot be
excluded in many families, it would appear tobe rare and only a few convincing pedigreeshave been described." 12 Those obligate carrierfemales examined have been almost alwaysnormal neurologically and none has had clearcut signs of spastic paraplegia." 12 However,because X linked pedigrees are so sparse andbecause examination findings in carrier fe-males have not always been reported, it is diffi-cult to be certain that carrier females neverhave definite signs of spastic paraplegia." 12
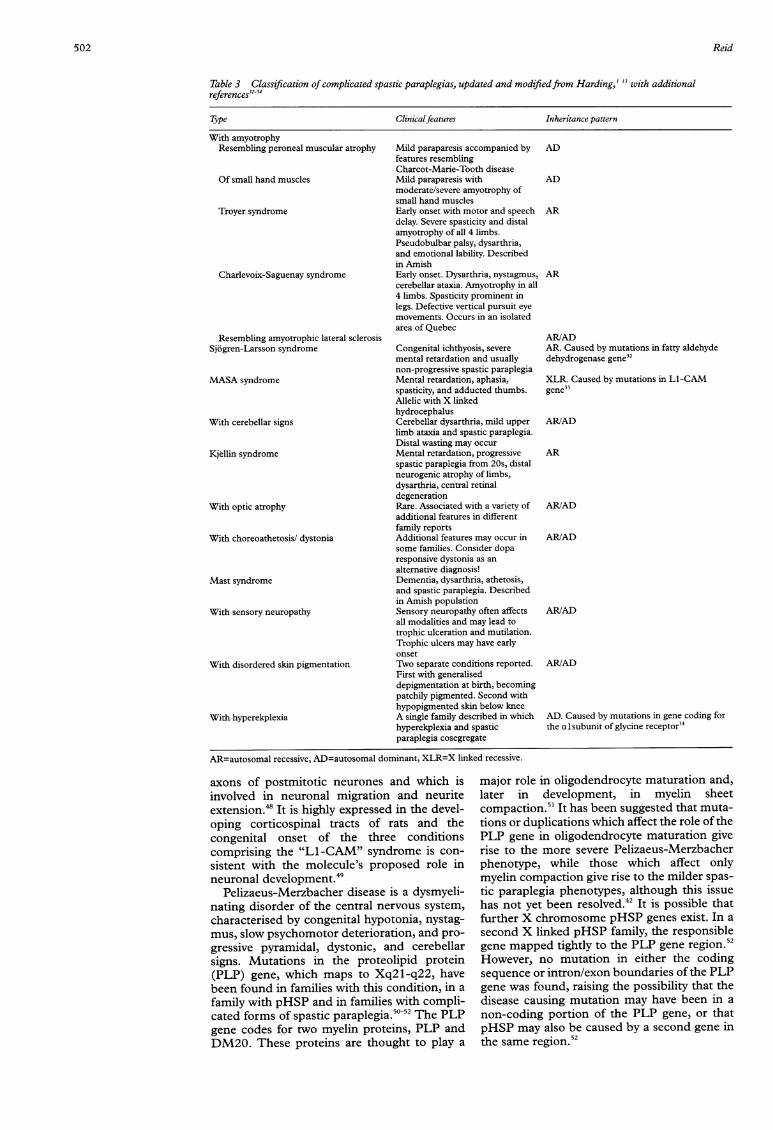
Complicated HSPComplicated HSP consists of a large numberof rare conditions, which tend to be inheritedin an autosomal recessive fashion. They havebeen well reviewed by Bundey3' and byHarding,'3 whose proposed classification isgiven in table 3.
Molecular genetics ofHSPThree autosomal dominant genes causingpHSP have been mapped, on chromosomes 2p,14q, and 15q (to regions of 4 cM, 7 cM, and 7
cM respectively).35-38 Linkage results have beenpublished in complete form for 34 families.35-42Strong evidence of linkage to one of the threeknown loci has been found in approximatelyhalf of these families, with weaker evidence oflinkage being found in a proportion of theremainder. Of those families showing evidenceof linkage, most are linked to chromosome2,35 36 40-42 with small numbers showing linkageto chromosomes 14 (three families)36 37 39 and15 (one family).38 Linkage to all three loci hasbeen excluded in a number of families, stronglysuggesting the existence of at least one furtherlocus.43 44 Anticipation has been postulated tooccur for a proportion of the families where thedisease gene maps to chromosome 235 40 41 45and to chromosome 14,3 suggesting theintriguing possibility that the underlying ge-netic abnormality might involve a trinucleotiderepeat expansion, as has been described forseveral other neurodegenerative conditions.There may be some correlation between
genetic locus and clinical phenotype, althoughassessment of this is hampered by scanty clini-cal details in mapping reports. All three of thefamilies showing linkage to the chromosome 14locus had a very early mean age at onset, under10 years old.36 37 3 On the other hand, familiesshowing linkage to chromosome 2 have consid-erable inter- and intrafamilial variation inage of onset, corresponding to both types I andII of Harding, and further weakening theargument that these types of pHSP aredistinct.35 36404 In none of these families wasthe mean age of onset as early as thechromosome 14 linked families. The singlefamily showing linkage to chromosome 15 hada unimodal age of onset (mean 22 years) andwas characterised by the relative severity of thecondition, with approximately 30% of itsmembers being chairbound.38A gene for autosomal recessive pHSP has
been mapped to the pericentric region of chro-mosome 8 in three consanguineous and one
non-consanguineous Tunisian families.46 Againthere is evidence of locus heterogeneity, withlinkage to chromosome 8 markers beingexcluded in a fifth consanguineous Tunisianfamily. The clinical picture was homogeneousin all five families, with an early age of onset(between 1 and 20 years), loss of vibrationsense and proprioception, and bladder sphinc-ter disturbance in all affected members.46While X linked spastic paraplegia is rare, it is
important because its molecular pathology ismore completely understood than that of theother forms. Mutations in the gene encodingthe neural cell adhesion molecule LI (Li-CAM) at Xq28 are responsible for a compli-cated form of spastic paraplegia, in whichparaplegia is accompanied by mental retarda-tion and absence of the extensor pollicis longusmuscle.33 Different mutations in the same geneare responsible for the MASA syndrome (men-
tal retardation, aphasia, shuffling gait, ad-ducted thumbs) and X linked hydrocephalus.33The same LI-CAM mutation may result ineither an X linked hydrocephalus phenotype or
a MASA phenotype.47 LI-CAM is a cellsurface glycoprotein which is expressed on the
Table 2 Risks ofhavingdisease gene for clinicallynormal offspring of affectedsubjects, based oncumulative age of onsetcurve for autosomaldominant pHSP1 For usewith families in which ageof onset is predominantlyunder 35years. Modifiedfrom Harding'
Risk of havingAge (y) disease gene (%)
20 2425 2230 1935 1340 1145 9
501
Reid
Table 3 Classification of complicated spastic paraplegias, updated and modifiedfrom Harding,' 13 with additionalreferences32-34
Type Clinicalfeatures Inheritance pattern
With amyotrophyResembling peroneal muscular atrophy
Mild paraparesis accompanied by ADfeatures resemblingCharcot-Marie-Tooth diseaseMild paraparesis with ADmoderate/severe amyotrophy ofsmall hand musclesEarly onset with motor and speech ARdelay. Severe spasticity and distalamyotrophy of all 4 limbs.Pseudobulbar palsy, dysarthria,and emotional lability. Describedin AmishEarly onset. Dysarthria, nystagmus, ARcerebellar ataxia. Amyotrophy in all4 limbs. Spasticity prominent inlegs. Defective vertical pursuit eyemovements. Occurs in an isolatedarea of Quebec
AR/'Congenital ichthyosis, severe AR.mental retardation and usually dehynon-progressive spastic paraplegiaMental retardation, aphasia, XLFspasticity, and adducted thumbs. geneAllelic with X linkedhydrocephalusCerebellar dysarthria, mild upper AR/Blimb ataxia and spastic paraplegia.Distal wasting may occurMental retardation, progressive ARspastic paraplegia from 20s, distalneurogenic atrophy of limbs,dysarthria, central retinaldegenerationRare. Associated with a variety of ARBAadditional features in differentfamily reportsAdditional features may occur in AR/Bsome families. Consider doparesponsive dystonia as analternative diagnosis!Dementia, dysarthria, athetosis,and spastic paraplegia. Describedin Amish populationSensory neuropathy often affects AR/!all modalities and may lead totrophic ulceration and mutilation.Trophic ulcers may have earlyonsetTwo separate conditions reported. AR/First with generaliseddepigmentation at birth, becomingpatchily pigmented. Second withhypopigmented skin below kneeA single family described in which AD.hyperekplexia and spastic theparaplegia cosegregate
'ADCaused by mutations in fatty aldehydeydrogenase gene32
R. Caused by mutations in LI-CAM.33
'AD
'AD
'AD
'AD
'AD
.Caused by mutations in gene coding foralsubunit of glycine receptor34
axons of postmitotic neurones and which isinvolved in neuronal migration and neuriteextension.48 It is highly expressed in the devel-oping corticospinal tracts of rats and thecongenital onset of the three conditionscomprising the "Li-CAM" syndrome is con-sistent with the molecule's proposed role inneuronal development.49
Pelizaeus-Merzbacher disease is a dysmyeli-nating disorder of the central nervous system,characterised by congenital hypotonia, nystag-mus, slow psychomotor deterioration, and pro-gressive pyramidal, dystonic, and cerebellarsigns. Mutations in the proteolipid protein(PLP) gene, which maps to Xq21-q22, havebeen found in families with this condition, in afamily with pHSP and in families with compli-cated forms of spastic paraplegia."1'2 The PLPgene codes for two myelin proteins, PLP andDM20. These proteins are thought to play a
major role in oligodendrocyte maturation and,later in development, in myelin sheetcompaction.51 It has been suggested that muta-tions or duplications which affect the role ofthePLP gene in oligodendrocyte maturation giverise to the more severe Pelizaeus-Merzbacherphenotype, while those which affect onlymyelin compaction give rise to the milder spas-tic paraplegia phenotypes, although this issuehas not yet been resolved.42 It is possible thatfurther X chromosome pHSP genes exist. In asecond X linked pHSP family, the responsiblegene mapped tightly to the PLP gene region.52However, no mutation in either the codingsequence or intron/exon boundaries of the PLPgene was found, raising the possibility that thedisease causing mutation may have been in anon-coding portion of the PLP gene, or thatpHSP may also be caused by a second gene inthe same region.52
502
Pure hereditary spastic paraplegia
Thus, the X linked hereditary spastic para-plegias indicate that mutations in the samegene may be responsible for both pure andcomplicated forms of HSP, as well as otherneurological conditions. In addition, they sug-gest that cell adhesion molecule genes andmyelin genes are likely candidates for otherforms of spastic paraplegia.
ConclusionKnowledge of the genetics of the hereditaryspastic paraplegias is advancing rapidly. Even-tually, an understanding of the molecularpathology underlying these conditions mayallow better genetic counselling for at risk fam-ily members, rational development of moreeffective treatments, and insight into the func-tion of the spinal cord in health and disease.
I am grateful to Dr Charles ffrench-Constant and Dr AndrewGreen for their helpful comments on the manuscript and to theMRC for their support of my work on pHSP.
1 Harding AE. The hereditary ataxias and related disorders.Edinburgh: Churchill Livingstone, 1984.
2 Strumpell A. Beitrage zur Pathologie des Ruckenmarks.Arch Psychiatr Nervenkr 1880;10:676-717.
3 Roe P. Hereditary spastic paraplegia. J Neurol NeurosurgPsychiatry 1963;26:516-19.
4 Holmes GL, Shaywitz BA. Strumpell's pure hereditaryspastic paraplegia: case study and review of the literature. JNeurol Neurosurg Psychiatry 1977;40: 1003-8.
5 Harding AE. Hereditary "pure" spastic paraplegia: a clinicaland genetic study of 22 families. J Neurol NeurosurgPsychiatry 1981;44:871-83.
6 Boustany RMN, Fleischnick E, Alper CA, et al. Theautosomal dominant form of "pure" familial spasticparaplegia: clinical findings and linkage analysis of a largepedigree. Neurology 1987;37:910-15.
8 Polo JM, Calleja J, Combarros 0, et al. Hereditary "pure"spastic paraplegia: a study of nine families. J Neurol Neuro-surg Psychiatry 1993;56: 175-81.
9 Durr A, Brice A, Serdaru M, et al. The phenotype of "pure"autosomal dominant spastic paraplegia. Neurology 1994;44:1274-7.
10 Fink JK, Sharp GB, Lange BM, et al. Autosomal dominant,familial spastic paraplegia type I: clinical and genetic analy-sis of a large North American family. Neurology 1995;45:325-31.
11 Keppen LD, Leppert MF, O'Connell P, et al. Etiologicalheterogeneity in X-linked spastic paraplegia. Am JTHumGenet 1987;41:933-43.
12 Cambi F, Tartaglino L, Lublin F, et al. X-linked pure famil-ial spastic paraparesis. Arch Neurol 1995;52:665-9.
14 Polo JM, Calleja J, Combarros 0, et al. Hereditary ataxiasand paraplegias in Cantabria, Spain. An epidemiologicaland clinical study. Brain 1991;114:855-66.
15 Cartlidge NEF, Bone G. Sphincter involvement in heredi-tary spastic paraplegia. Neurology 1973;23: 1160-3.
16 Opjordsmoen S, Nyberg-Hansen R. Hereditary spasticparaplegia with neurogenic bladder distrubances andsyndactylia. Acta Neurol Scand 1980;61:35-41.
17 Bushman W, Steers WD, Meythaler JM. Voiding dysfunc-tion in patients with spastic paraplegia: urodynamic evalu-ation and response to continuous intrathecal baclofen.Neurourol Urodyn 1993;12:163-70.
18 Schady W, Sheard A. A quantitative study of sensory func-tion in hereditary spastic paraplegia. Brain 1990;113:709-20.
19 Behan WMH, Maia M. Strumpell's familial spasticparaplegia: genetics and neuropathology. Neurol Neuro-surg Psychiatry 1974;37:8-20.
20 McLeod JG, Morgan JA, Reye C. Electrophysiological stud-ies in familial spastic paraplegia. 7 Neural NeurosurgPsychiatry 1977;40:611-15.
21 Bruyn RPM, van Dijk JG, Scheltens P, et aL Clinically silentdysfunction of dorsal columns and dorsal spinocerebellartracts in hereditary spastic paraparesis. _7 Neurol Sci1994;125:206-1 1.
22 Thomas PK, Jefferys JGR, Smith IS, et al. Spinalsomatosensory evoked potentials in hereditary spasticparaplegia. _7 Neurol Neurosurg Psychiatry 1981;44:243-6.
23 Aalfs CM, Koelman JHTM, Posthumus Meyjes FE, et al.Posterior tibial and sural nerve somatosensory evoked
potentials: a study in spastic paraparesis and spinal cordlesions. Electroetncephalogr Clin Neurophysiol 1993;89:437-41.
24 Schady W, Dick JPR, Sheard A, et al. Central motorconduction studies in hereditary spastic paraplegia. . Neu-rol Neurosurg Psychiatry 199 1;54:775-9.
25 Nygard TG, Marsden CD, Fahn S. Dopa responsivedystonia: long term treatment response and prognosis.Neurology 1991;41:174.
26 Fink JK, Heiman-Patterson T. Hereditary spasticparaplegia: advances in genetic research. Neurology 1996;46:1507-14.
27 Durr A, Cossee M, Agid Y, et al. Clinical and genetic abnor-malities in patients with Friedreich's ataxia. N Engl 7 Med1996;335: 1169-75.
28 Meythaler JM, Steers WD, Tuel SM, et al. Intrathecalbaclofen in hereditary spastic paraparesis. Arch Phys MedRehabil 1992;73:794-7.
29 Dunne JW, Heye N, Dunne SL. Treatment of chronic limbspasticity with botulinum toxin A. _7 Neurol NeurosurgPsychiatry 1995;58:232-5.
30 Cosgrove AP, Corry IS, Graham HK. Botulinum toxin inthe management of the lower limb in cerebral palsy. DevMed Child Neurol 1994;36:386-96.
31 Bundey S. Genetics and neurology. Edinburgh: Churchill Liv-ingstone, 1992.
32 De Laurenzi V, Rogers CG, Hamrock DJ, et al. Sjogren-Larsson syndrome is caused by mutations in the fatty alde-hyde dehydrogenase gene. Nat Genet 1996;12:52-7.
33 Jouet M, Rosenthal A, Armstrong G, et al. X-linked spasticparaplegia (SPG1), MASA syndrome and X-linked hydro-cephalus result from mutations in the LI gene. Nat Genet1994;7:402-7.
34 Elmslie FV, Hutchings SM, Spencer V, et al. Analysis ofGLRA1 in hereditary and sporadic hyperekplexia: a novelmutation in a family cosegregating for hyperekplexia andspastic paraparesis. _7 Med Genet 1996;33:435-6.
35 Hazan J, Fontaine B, Bruyn RPM, et al. Linkage of a newlocus for autosomal dominant familial spastic paraplegia tochromosome 2p. Hum Mol Genet 1994;3:1569-73.
36 Hentati A, Pericak-Vance MA, Lennon F, et al. Linkage of alocus for autosomal dominant familial spastic paraplegia tochromosome 2p markers. Hum Mol Genet 1994;3: 1867-71.
37 Hazan J, Lamy C, Melki J, et al. Autosomal dominant famil-ial spastic paraplegia is genetically heterogeneous and onelocus maps to chromosome 14q. Nat Genet 1993;5:163-7.
38 Fink JK, Wu CB, Jones SM, et al. Autosomal dominantfamilial spastic paraplegia: tight linkage to chromosome15q.AmJ Hum Genet 1995;56:188-92.
39 Gispert S, Santos N, Damen R, et al. Autosomal dominantfamilial spastic paraplegia: reduction of the FSP 1 candidateregion on chromosome 14q to 7 cM and locus heterogene-ity.Am _J Hum Genet 1995;56:183-7.
40 De Jonge P, Krols L, Michalik A, et al. Pure familial spasticparaplegia: clinical and genetic analysis of nine Belgianpedigrees. EurJ7 Hum Genet 1996;4:260-6.
41 Burger J, Metzke H, Paternotte C, et al. Autosomaldominant spastic paraplegia with anticipation maps to a 4cM interval on chromosome 2p21-p24 in a large Germanfamily. Humn Genet 1996;98:371-5.
42 Kobayashi H, Garcia CA, Alfonso G, et al. Molecular genet-ics of familial spastic paraplegia: a multitude of responsiblegenes. Neurol Sci 1995;137:131-8.
43 Lennon F, Gaskell PC, Wolpert C, et al. Linkage andheterogeneity in hereditary spastic paraparesis. Am _7 HumGenet Suppl 1995;57:A217.
45 Lennon F, Gaskell PC, Scott WK, et al. Genetic studies infamilial spastic paraparesis: heterogeneity results andevidence for anticipation in chromosome 2 SPG. Am _7Hum GenetSuppl 1996;59:A225
46 Hentati A, Pericak-Vance MA, Hung WY, et al. Linkage of"pure" autosomal recessive familial spastic paraplegia tochromosome 8 markers and evidence of genetic locus het-erogeneity. Hum Mol Genet 1994;3:1263-7.
47 Jouet M, Moncla A, Paterson J, et al. New domains of neu-ral cell-adhesion molecule LI implicated in X-linkedhydrocephalus and MASA syndrome. Am 7 Hum Genet1995;56: 1304-14.
48 Sonderegger P, Rathjen FG. Regulation of axonal growth inthe vertebrate nervous system by interactions betweenglycoproteins belonging to two subgroups of the immu-noglobulin superfamily.] Cell Biol 1992;119:1387-94.
49 Joosten EAJ, Gribnau AAM. Immunocytochemical localiza-tion of cell adhesion molecule LI in developing rat pyrami-dal tract. Neurosci Lett 1989;100:94-8.
50 Saugier-Veber P, Munnich A, Bonneau D, et al. X-linkedspastic paraplegia and Pelizaeus-Merzbacher disease areallelic disorders at the proteolipid protein locus. Nlat Genet1994;6:257-62.
51 Griffiths I, Montague P, Dickinson P. The proteolipidprotein gene. Neuropathol Appl Neurobiol 1995;21:85-96.
52 Cambi F, Tang XM, Cordray MS, et al. Refined geneticmapping and proteolipid protein mutation analysis inX-linked pure hereditary spastic paraplegia. Neurology1996;46:1 112-17.