38
Systemic Complications of LA Shashank Trivedi (110301192)
| Date post: | 17-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | shashank-trivedi |
| View: | 244 times |
| Download: | 17 times |

Systemic Complications of
LAShashank Trivedi
(110301192)
What is Local Anesthesia?
Local Anesthesia has been defined as…
“Loss of sensation in a circumscribed area of the body caused by depression of excitation in nerve endings or inhibition of the conduction process in peripheral nerves.”

Complications of LALocal Complications
1. Needle breakage2. Paresthesia3. Facial nerve paralysis4. Trismus5. Soft tissue injury6. Hematoma7. Pain/Burning on injection8. Infection9. Edema10. Sloughing of tissues11. Post anesthetic intraoral
lesions
Systemic Complications
1. Overdose reactions-LA Toxicity-Vasoconstrictor Toxicity
2. Allergy3. Idiosyncrasy

Principles of Systemic Complication
Principle 1:“No drug ever exerts a single action.”
Principle 2:“No clinically useful drug is entirely devoid of toxicity.”
Principle 3:“The potential toxicity of a drug rests in the hands of the user.”

LA Toxicity
Overdose Reactions

Definition
It refers to the symptoms manifested as a result of overdosage or excessive administration of the solution.

Etiology Large dose of drug Accidental intravenous injection High concentration of a drug Unusually slow detoxification as a result of
severe liver disease Slow elimination as a result of Kidney
problem Use of highly toxic drugs whose margin of
safety is narrow Injection of solution in a highly vascular
area without the addition of vasoconstrictor substance
Clinically
Cerebral Cortex1. Talkative2. Restlessness3. Apprehensive4. Excited5. Convulsive
Medulla1. Lethargy2. Sleepiness3. Unconscious
Early CNS Stimulation Symptoms

Clinically
Cerebral Cortex1. Blood Pressure2. Pulse rate3. Respiratory rate4. Nausea5. Vomiting
Medulla1. Blood pressure2. Pulse rate3. Heart rate4. Respiratory
depression5. Unconsciousness
Late CNS Depression Symptoms
Death usually occur due to respiratory depression and hypoxia and its subsequent
effect on the Cardiovascular system

Prevention
Pre-analgesic evaluation of the patient Use the weakest possible concentration Use vasoconstrictor whenever possible Use the least possible volume Aspirate before injection Slow injection Monitor the patient carefully after injection
TreatmentP…Position
A…Airway
B…Breathing
C…Circulation
D…Definitive care
Treatment Mild Stimulation
Moderate Stimulation
Convulsion phase
Depression Phase
1. No treatment2. Stop further injection
1. IV injection of barbiturates0.2% solution of sodium thiopentalSecobarbital
2. Oxygen inhalation

Treatment Mild Stimulation
Moderate Stimulation
Convulsion phase
Depression Phase
Anticonvulsant IV/IM-Coramine(150-450 mg IV)-Midazolam or Diazepam(100 mg IV)-Wyamine(7.5 mg IV)1. Artificial Respiration
2. IV Fluids3. Sympathomimetic drugs

Vasoconstrictor Toxicity

Clinical FeaturesSigns1. Sharp elevation in
BP,primarily systolic.2. Elevated heart rate.
3. Possible cardiac dysrhythmias(premature ventricular contractions/ventricular tachycardia/ventricular fibrillation)
Symptoms1. Fear/anxiety2. Tenseness3. Restlessness4. Throbbing headache5. Tremor6. Perspiration7. Weakness8. Dizziness9. Pallor10. Respiratory difficulty11. Palpitations

Management Most instances of Epinephrine overdose are of
short duration that require little or no formal management.However,the reaction may be prolonged and some management is desirable.
1. Terminate the procedure: if possible,remove the source of epinephrine.Stopping the injection of LA does not remove epinephrine that has been deposited;however,release of endogenous epinephrine and norepinephrine from the adrenal medulla and nerve endings is lessened once the anxiety-inducing stimulus is eliminated.
2. Basic management follows the usual P-A-B-C-D algorithm.

Management3. Definitive care(D)1. Reassure the patient that the signs and
symptoms are transient and will subside shortly.2. Monitor vital signs and administer Oxygen.
BP and heart rate should be checked every 5 minutes during the episode.
3. Hyperventilation can be seen in an apprehensive patient,this is a contraindication for the administration of oxygen.
4. Recovery: Permit the patient to remain in the dental chair as long as necessary to recover.
Do not discharge the patient if any doubt remains about his/her ability to provide self-care.

Allergy

Definition Allergy is a hypersensitive state,acquired
through exposure to a particular allergen,re-exposure to which produces a heightened capacity to react.
Allergic reactions cover a broad spectrum of clinical manifestations ranging from mild and delayed responses occurring as long as 48 hours after exposure to the allergen,to immediate and life threatening reactions developing within seconds of exposure.

Predisposing Factors Allergic response to LA include
dermatitis,bronchospasm and Systemic Anaphylaxis.
The most frequently encountered are localized dermatologic reactions.
Hypersensitivity to the ester type LA-Procaine,Propoxycaine,Benzocaine,Tetracaine,and related compounds such as Procaine Penicillin G and Procainamide is more frequent.
Allergic reactions have been documented for the various contents of the dental LA cartridge.

Contents of LA Cartridge
INGREDIENTLocal Anesthetic AgentVasoconstrictor(Epinephrine)Sodium metabisulfiteMethylparaben
Sodium Chloride
Sterile water
Allergens in LA Sodium bisulfite allergy:
People who are allergic to bisulfites(most often steroid-dependent asthmatics) may develop a severe response(bronchospasm).In presence of documented sulfite allergy,it is suggested that a LA solution without a vasopressor(“Plain Local Anesthetic”)should be used.No cross allergenicity is present between sulfites and sulfa type drugs.
Latex Allergy:The thick plunger at one end and the thin diaphragm at the other end of the cartridge,through which the needle penetrates contained LATEX.A study reveals that latex allergen can be released into the local anesthetic solution as the needle penetrates the diaphragm.Dental cartridges presently available in US and Canada are latex free.
Topical Anesthetic Allergy:Topical anesthetics possess the potential to induce allergy. The incidence of allergy to Esters is greater than Amides. The degree of allergic response depends on the site of application,dose and systemic absorption.

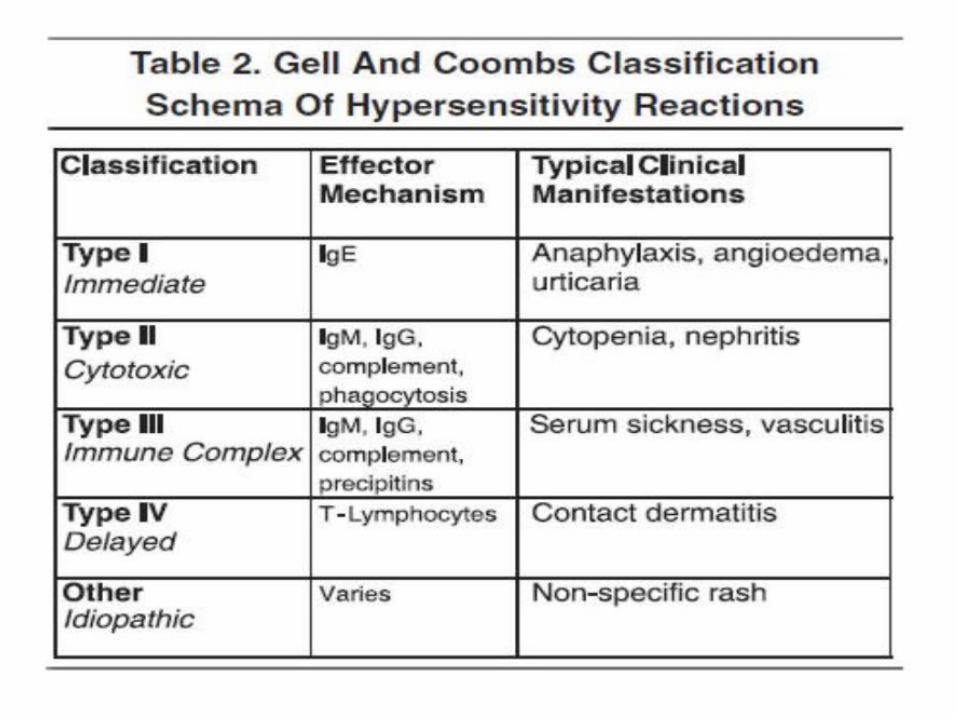
Clinical Manifestations Immediate reactions develop within seconds to
hours of exposure.They include Type I,II, and III hypersensitivity reactions.
With delayed reactions,clinical manifestations develop hours to days after antigenic exposure(Type IV).
Immediate reactions,particularly Type I anaphylaxis are significant.Organs and tissues involved in immediate allergic reactions include skin,CVS,Respiratory system, and GI system.
Generalized anaphylaxis involves all these systems.
Type I reactions may involve only one system,in which case they are referred to as localized allergy.Eg:Bronchospasm,Urticaria.

Signs and Symptoms DERMATOLOGIC REACTIONS:
The most common allergic reaction associated with LA administration consists of urticaria and angioedema.Intense itching(pruritis) is frequently present with urticaria.
Allergic skin reactions,if sole manifestation of an allergic response,normally are not life threatening;however,those that occur rapidly after drug administration may be the first indication of a more generalized reaction to follow.


Signs and Symptoms RESPIRATORY REACTIONS:
Clinical signs and sypmtoms of allergy may solely be related to the respiratory tract,or respiratory tract involvement may occur along with other systemic responses.Signs and symptoms of bronchospasm,the classic respiratory allergic response,include the following:-Respiratory distress-Dyspnea-Erythema-Cyanosis-Diaphoresis-Tachycardia-Increased anxiety-Use of accessory muscles of respiration
Laryngeal edema(life threatening emergency) is a swelling of the soft tissues surrounding the vocal apparatus with subsequent obstruction of the airway.

Signs and Symptoms Generalized Anaphylaxis:
This is an acutely life threatening allergic reaction.Clinical death can occur within a few minutes.Generalized anaphylaxis can develop after administration of an antigen by any route but is more common after parenteral administration.Time of response is variable,but the reaction typically develops rapidly,reaching maximum intensity within 5-30 minutes.It is extremelt unlikely that this reaction will ever be noted after administration of Amide local anesthetic.Signs and symptoms of generalized anaphylaxis occur as follows:Skin Reactions Smooth muscle spasm of GIT/Genitourinary/Bronchospasm
Cardiovascular collapse Respiratory distress
In fatal anaphylaxis,respiratory and cardiovascular disturbances predominate and are evident early in the reaction.


Management of Skin Reactions
Delayed Skin Reactions: (developing 60 minutes or more post exposure)P-A-B-C:Position the conscious patient comfortably.A,B,C are assessed as adequate.Definitive care:-Oral histamine blocker:50mg diphenhydramine or 10mg chlorpheniramine-If still in dental office,the patient should remain in the office under observation for 1 hour before discharge to ensure that the reaction does not progress.-Obtain medical consultation,if necessary,to determine the cause of reaction.A complete list of all the drugs and chemicals administered to or taken by the patient should be compiled for use by the allergy consultant.-If drowsiness occurs after oral histamine blocker administration,the patient should not be permitted to leave the dental office unescorted.

Management of Skin Reactions
Immediate Skin Reactions: (developing within 60 minutes post exposure)P-A-B-C:Position the conscious patient comfortably.A,B,C are assessed as adequate.Definitive care:-Administer parenteral histamine blocker:50mg diphenhydramine or 10mg chlorpheniramine-Monitor and record vital signs every 5 minutes for 1 hour.-Observe the patient a minimum of 60 minutes for evidence of recurrence.Discharge in the custody of a responsible adult if any parenteral drugs have been given.-Prescribe an oral histamine blocker for 3 days.-Fully evaluate the patient’s reaction before further dental care is provided.-If,at any time during this period,uncertainty exists as to the condition of the patient,activate emergency medical services.
Management of Respiratory Reactions
Bronchospasm:P-A-B-C:Position the patient comfortably.Most persons experiencing respiratory distress prefer to be seated upright to varying degrees.ABC are assessed.Airway is patent,although patient is exhibiting respiratory distress.C is assessed as adequate.Definitive care:-Terminate treatment.-Administer oxygen.-Administer epinephrine IM.-Activate emergency medical services.-on recovery,administer histamine blocker.

Management of Respiratory Reactions
Laryngeal Edema:P-A-B-C:Position the unconscious patient supine.ABC are assessed.If airway is maintained and the victim’s chest is making spontaneous respiratory movements but no air is being exchanged,immediate and aggressive treatment is mandatory to save the victim’s life.Definitive care:-Administer epinephrine IM.-Activate emergency medical services.-Administer oxygen-Maintain the airway.-Administer Histamine blocker IM/IV and corticosteroid IM/IV-Perform cricothyrotomy if the preceding steps have failed to secure patent airway.


Management of Generalized Anaphylaxis P-A-B-C:Position the unconscious patient supine.
ABC are assessed and performed as indicated.If Conscious,position the patient comfortably.
Definitive care:-Administer epinephrine:0.3mL of 1:1000-Activate emergency medical services.-Administer oxygen.-Monitor vital signs.-perform basic life support if needed.-Additional drug therapy:may be started once clinical improvement is noted.This includes the administration of Histamine blocker and corticosteroid(both IV/IM)NOTE:Epinephrine and oxygen are the only drugs that should be administered during the acute phase of the anaphylactic reaction.

Summary Systemic complications associated with Local
Anesthetic drug administration and techniques are frequently preventable.
Preliminary medical evaluation should be completed before administration of any local anesthetic.
The weakest effective concentration of local anesthetic solution should be injected at the minimum volume compatible with successful pain control.
Observe the patient both during and after local anesthetic administration for signs and symptoms of undesirable reaction.Never give an injection and leave the patient alone while doing other procedures.

Bibliography Handbook of Local Anesthesia
-Dr.Stanley F. Malamed
Image courtesy:google.com


















