TESTING A CONCEPTUAL MODEL OF VOCAL TREMOR: RESPIRATORY AND LARYNGEAL CONTRIBUTIONS TO ACOUSTIC MODULATION by Jordon LeBaron A thesis submitted to the faculty of The University of Utah in partial fulfillment of the requirements for the degree of Master of Science in Speech-Language Pathology Department of Communication Sciences and Disorders The University of Utah December 2016
Transcript
TESTING A CONCEPTUAL MODEL OF VOCAL TREMOR: RESPIRATORY
AND LARYNGEAL CONTRIBUTIONS TO ACOUSTIC MODULATION
by
Jordon LeBaron
A thesis submitted to the faculty of The University of Utah
in partial fulfillment of the requirements for the degree of
Master of Science
in
Speech-Language Pathology
Department of Communication Sciences and Disorders
respectively (p = .026). A significant difference was also found between voicing
conditions for modulation rate of fo (p = .049) and SPL (p < .001). The rates of
modulation during AMV were slower (fo = 2.8 (+ .8) Hz; SPL = 2.1 (+ .7) Hz) than
for vibrato (fo = 5.1 (+ .7) Hz; SPL = 5 (+ .6) Hz). However, laryngeal kinematic
and acoustic fo and SPL magnitude patterns did not differ between voicing
conditions. Outcomes support predicted contributions of the respiratory system
to voicing modulation; however, the larynx appears interactive with the
respiratory and other speech structures during voicing.
TABLE OF CONTENTS
ABSTRACT ...........................................................................................................iii LIST OF FIGURES ...............................................................................................vii LIST OF TABLES ..................................................................................................ix ACKNOWLEDGEMENTS ......................................................................................x INTRODUCTION ...................................................................................................1
Background .....................................................................................................1 Statement of Purpose .....................................................................................14
Qualitative Analysis of Results .......................................................................42 Respiratory System Contributions to Acoustic Modulation .............................42 Phonatory System Contributions to Acoustic Modulation ...............................44 Vocal Tract Movements by Condition .............................................................47
Vertical Laryngeal Movement ....................................................................47 Pharyngeal Movement ..............................................................................48
Respiratory System Contributions to Acoustic Modulation .............................50 Laryngeal Contributions to Acoustic Modulation ............................................52 Application of Current Findings to Vocal Tremor ............................................55 Limitations ......................................................................................................56 Conclusion ......................................................................................................58
1 Barkmeier-Kraemer and Story (2010) Conceptual Model of Vocal Tremor .......7
2 Lengthwise (A) and medial/lateral (B) oscillation directions within the Phonatory System ..............................................................................................8
3 LabChart Pro display of simultaneously recorded laryngeal images and acoustic and respiratory signals .......................................................................18
4 A comparison of signals rated for each voicing condition (i.e., vibrato and AMVT). A. A comparison of signals rated for the vibrato condition from the two subjects rated with 44% expert agreement from S03 (a-c) and S04 (d-f) and signals with 100% expert agreement from S05 (g-i) versus. B A comparison of signals rated for the AMVT condition with 67% expert agreement from S10 (a-c) and 100% expert agreement from S05 (d-f) ............................................27 5 Example of determining rate for respiratory kinematic oscillation. Each arrow marks the peak of each modulation cycle displayed in the 2-s window. A total of 11 peak-to-peak cycles are shown in the 2-s window giving a 5.5 Hz respiratory kinematic rate ........................................................29
6 Example of measuring extent of respiratory kinematic oscillation. The minimum and maximum values associated with summated rib cage and abdominal movements in the figure represent the original data points. The original data points were corrected before extent was calculated. After adjustment for the sloping values, the relative %VC extent was calculated as described above ...............................................................................................29
7 Example of fo (top line) and SPL (bottom line) plot of vibrato within Praat. Arrows have been added to the signal to indicate the beginning of the
8 Example of fo (top line) and SPL (bottom line) plot of vibrato within Praat. Arrows have been added to the signal to indicate the maximum and minimum points of cycle 3 (fo) and cycle 8 (SPL) ............................................................32
viii
9 An example of laryngeal imaging measures for the first end point of one laryngeal oscillatory cycle. Each panel displays A) the image analyzed, B) the anatomical referent line measure, C) the relative measure of vocal fold length, and D) the relative measure of interarytenoid distance associated with the first end point of one laryngeal oscillation cycle. B. Example of laryngeal imaging measures for the second end point of one laryngeal oscillatory cycle. Each panel displays A) the image analyzed, B) the anatomical referent line measure, C) the relative measure of vocal fold length, and D) the relative measure of interarytenoid distance associated with the second end point of one laryngeal oscillation cycle ........................................................................36
10 Kinematic extent comparisons between voicing conditions (i.e., AMVT and vibrato) ..........................................................................................................45 11 Kinematic extent comparisons between voicing types (i.e., AMVT and vibrato) ..........................................................................................................45
12 Acoustic extent comparisons between voicing conditions (i.e., AMVT and vibrato) ..........................................................................................................46
13 Acoustic rate comparisons between voicing conditions (i.e., AMVT and vibrato) .........................................................................................................46
LIST OF TABLES
Tables 1 Speech structures reported to exhibit tremor ....................................................4
2 Barkmeier-Kraemer and Story (2010) summary of conceptual model of vocal tremor ................................................................................................................9 3 Aims of this study ...........................................................................................15
4 Percent agreement between expert judges and intended production condition .........................................................................................................26
5 Intrarater reliability determined using intraclass correlations .........................40
Lester, Barkmeier-Kraemer, & Story, 2013) (see Table 1). The latter structures
may be most frequently associated with vocal tremor due to their ease of
observation during endoscopic evaluation. However, tremor has also been
identified in other structures such as the soft palate (Sulica & Louis, 2010) and
respiratory musculature (Tomoda et al., 1987). Although the majority of literature
addressing vocal tremor has focused on the larynx, approximately 25% of those
with vocal tremor exhibit tremor in structures outside of the larynx, or within the
vocal tract (Bové et al., 2006). Although prior studies have noted tremor affecting
4
Table 1. Speech structures reported to exhibit tremor.
Study Subjects
Methods Speech Structures Studied with Tremor
Sulica, L., & Louis, E. D. (2010). Clinical characteristics of essential voice tremor: A study of 34 cases. The Laryngoscope, 120(3), 516-528.
N=34 with ET
Vocal Tremor Scoring System (VTSS) for laryngeal and pharyngeal movement, Washington Heights Inwood Genetic Study of Essential Tremor (WHIGET) rating scale for arm tremor, Voice Handicap Index (VHI) for voice disability rating.
Larynx, Pharynx, Palate, Tongue
Finnegan, E. M., Luschei, E. S., Barkmeier, J. M., & Hoffman, H. T. (2003). Synchrony of laryngeal muscle activity in persons with vocal tremor. Archives of Otolaryngology–Head & Neck Surgery, 129(3), 313-318.
Ackermann, H., & Ziegler, W. (1991). Cerebellar voice tremor: an acoustic analysis. Journal of Neurology, Neurosurgery & Psychiatry, 54(1), 74- 76.
N=1 with Cerebellar tremor
Acoustic analysis from voice recordings
Larynx only
Gamboa, J., Jiménez-Jiménez, F. J., Nieto, A., Cobeta, I., Vegas, A., Ortí-Pareja, M., García-Albea, E. (1998). Acoustic voice analysis in patients with essential tremor. Journal of Voice, 12(4), 444-452.
N=56 (28 with ET; 28 control)
Acoustic analysis from voice recordings
Larynx, Vocal Tract (articulators)
Jiang, J., Lin, E., & Hanson, D. G. (2000). Acoustic and Airflow Spectral Analysis of Voice Tremor. Journal of Speech, Language & Hearing Research, 43(1), 191.
N=10 (5M, 5F) neuro-logical disease showing signs of VT
Lester, R. A., Barkmeier-Kraemer, J., & Story, B. H. (2013). Physiologic and Acoustic Patterns of Essential Vocal Tremor. Journal of Voice, 27(4), 422-432.
N=1 with EVT Rigid videostroboscopy, acoustic analysis, simulation using computer model
Larynx, Vocal Tract (articulators)
Adler, C. H., Bansberg, S. F., Hentz, J. G., Ramig, L. O., Buder, E. H., Witt, K., Edwards, B. W., Krein-Jones, K., & Caviness, J. N., (2004). Botulinum toxin type A for treating voice tremor. Archives of Neurology, 61(9), 1416-1420.
N=13 with VT Video laryngostroboscopy, acoustic analysis
Larynx
Bové, M., Daamen, N., Rosen, C., Wang, C. C., Sulica, L., & Gartner-Schmidt, J. (2006). Development and Validation of the Vocal Tremor Scoring System. The Laryngoscope, 116(9), 1662-1667.
N=10 with VT Transnasal videostroboscopy, acoustic analysis
Larynx
6
speech structures in individuals with vocal tremor, none of these studies
compared the contribution of oscillating speech structures to the final acoustic
output.
To better elucidate the impact of tremor on voice and speech, improved
understanding of the contribution of speech structures on the associated acoustic
signal needs to be prospectively studied. To date, attempts to characterize vocal
tremor by neurogenic disorder has not been successful due to the range of
acoustic patterns demonstrated using primarily fo and SPL rate patterns, in some
cases comparing measures across pitch productions. However, literature
addressing tremor in the limbs has systematically studied the rate, extent, and
conditions under which tremor occurs to classify and diagnose different forms of
tremor. The impact of tremor on functional movements during everyday activities
is considered by neurologists to be the symptoms that bring patients to the clinic.
Similarly, patients with vocal tremor complain of speech and voice problems, but
analysis of the acoustic correlates of the symptoms does not provide insight into
the underpinnings of vocal tremor physiology and its influence on the speech
mechanism. To address the physiologic underpinnings of vocal tremor, a
conceptual model was developed by Barkmeier-Kraemer and Story (2010) (see
Figure 1).
The conceptual model of vocal tremor proposes that tremor oscillation
originating from structures of the respiratory, phonatory, and articulatory systems
will contribute hypothesized patterns of acoustic modulation during voice
production (see Figure 1). For example, tremor oscillations within the respiratory
system are hypothesized to result in acoustic modulation of sound pressure level
7
Figure 1. Barkmeier-Kraemer and Story (2010) Conceptual Model of Vocal Tremor
(SPL) during phonation due to subglottal pressure changes associated with
rhythmic compression and expansion movements of the thoracic cavity due to
tremor affecting muscles of the rib cage, diaphragm, or abdomen (see Figure 1).
Oscillation of the articulatory structures is hypothesized to result in acoustic
modulation of the formant frequencies (i.e., resonant frequencies). The latter is
based upon a model of speech production developed by Brad Story (Story,
1995). This model renders the oral and pharyngeal cavities lined by associated
articulators to behave as a resonating chamber that filters the sound produced at
the level of the larynx by varying length, diameter, and shape. This resonating
chamber is referred to as the vocal tract. If an articulator associated with any
portion of the vocal tract oscillates (e.g., the base of tongue and posterior
Phonatory System Oscillation:
- Vocal fold length changes
o Results in fo
modulation
- Abductory/Adductory vocal
fold movements
o Results in SPL
modulation
Articulatory System
Oscillation:
- Diameter and length
changes in the vocal
tract
- Results in F1 and F2
modulation
Respiratory System
Oscillation:
- Subglottal
Pressure
changes
- Results in SPL
modulation
8
oropharyngeal wall region), the result is oscillation of diameter due to alternation
of constriction and dilation of the vocal tract, or length changes occurring due to
vertical oscillation of the larynx (see Figure 1). Finally, tremor causing oscillation
within the phonatory system is hypothesized to result in two different, or
combined acoustic modulations: 1) lengthwise oscillation of the vocal folds is
hypothesized to predominantly result in modulation of fundamental frequency (fo),
and 2) medial/lateral oscillations of the vocal folds (i.e., oscillation causing
abduction/adduction of the vocal folds) is hypothesized to predominantly result in
modulation of SPL (see Figure 2). Thus, the conceptual model of vocal tremor
offers specific predictions regarding acoustic patterns resulting from tremor
affecting each of the speech mechanism systems to explain the range of vocal
tremor acoustic patterns described in the literature.
The Conceptual Model of Vocal Tremor was developed to help frame
future research investigating characteristics of tremor affecting the speech
Figure 2. Lengthwise (A) and medial/lateral (B) oscillation directions within the Phonatory System
B A
9
mechanism and associated acoustic patterns. For a summary of the model, see
Table 2. To date, testing of this model has primarily been completed using case-
based studies and simulation of tremor within isolated speech mechanism
systems.
One example combined case-based testing of vocal tremor and simulation
of vocal tremor is a study by Lester and colleagues (Lester, et al., 2013). This
study evaluated acoustic patterns in an individual observed to present with
lengthwise vocal fold oscillation during sustained phonation as determined using
stroboscopic imaging. Although lengthwise vocal fold oscillation was
hypothesized within the Conceptual Model of Vocal Tremor to result in a
predominance of acoustic modulation of fo, SPL modulation extent was found to
predominate. Reevaluation of the original stroboscopic evaluation identified that
the laryngeal vestibule appeared to also oscillate in a lengthwise direction
associated with vocal fold lengthwise oscillation. Further investigation was
completed with consideration that the laryngeal vestibule may serve as part of
the vocal tract acting as a resonating chamber and contribute to the acoustic
Table 2. Barkmeier-Kraemer and Story (2010) Summary of Conceptual model of vocal tremor.
Speech Mechanism System Affected by Tremor Hypothesized Acoustic Modulation
Respiratory System oscillation of thoracic cavity compression and expansion
Sound Pressure Level (SPL)
Phonatory System 1: Vocal fold length oscillation Fundamental Frequency (fo)
Phonatory System 2: Medial/lateral vocal fold oscillation
Sound Pressure Level (SPL)
Articulatory System oscillation of diameter and/or length of the vocal tract
Formant Frequencies (F1 and F2)
10
patterns predicted for the vocal tract resulting in formant modulation and
subsequent SPL modulation. Acoustic analysis of the vocal tract formants
supported that the case under study demonstrated formant modulation consistent
with the idea that the laryngeal vestibule contributed to vocal tract oscillation. To
further test the idea of the laryngeal vestibule as a component of the vocal tract
for this individual case, an analysis-by-synthesis approach was utilized. That is,
the acoustic characteristics from the case voice recordings were used to model
acoustic modulation patterns resulting from oscillation originating within the
larynx alone compared to the larynx plus the vocal tract. Systematic analysis of
varied possible conditions of laryngeal and vocal tract oscillation patterns and
associated acoustic patterns demonstrated that the Conceptual Model of Vocal
Tremor helped elucidate the location of tremor within and outside of the vocal
folds of one individual and supported that the laryngeal vestibule resonating
chamber contributed to acoustic modulation patterns as predicted for the vocal
tract (Lester et al., 2013).
Although the case example described above was helpful for testing the
Conceptual Model of Vocal Tremor, general testing on groups of individuals with
vocal tremor has not yet been completed. One reason for this arises due to
difficulty successfully identifying individuals representing tremor isolated within
each system of the speech mechanism. Thus, the question arises whether a
human demonstration of volitional oscillation within one subsystem of the speech
mechanism could be used as a surrogate approach to test the Conceptual Model
of Vocal Tremor (Barkmeier-Kraemer & Story, 2010).
One possible approach to studying vocal tremor acoustic patterns
11
associated with oscillation of speech mechanism structures is to study volitional
modulation of the voice, or vibrato. Western classical singing proponents
consider vibrato to be the “quasi automatic” result of correct singing technique,
used by singers to produce an aesthetically pleasing singing voice (Sundberg,
1994). Vibrato shares many similar acoustic features to vocal tremor such as
rate and extent of fo and SPL (Anand, Shrivastav, Wingate, & Chheda, 2012;
Anand, Wingate, Smith, & Shrivastav, 2012). Similar to vocal tremor, typical
vibrato rate is between 4-7 Hz (Anand, Widgate, et al., 2012; Guzman et al.,
*This production condition did not meet accuracy criteria and was subject to review by the authors.
27
A.
B.
Figure 4. A comparison of signals rated for each voicing condition (i.e., vibrato and AMVT). A. A comparison of signals rated for the vibrato condition from the two subjects rated with 44% expert agreement from S03 (a-c) and S04 (d-f) and signals with 100% expert agreement from S05 (g-i) versus. B. A comparison of signals rated for the AMVT condition with 67% expert agreement from S10 (a-c) and 100% expert agreement from S05 (d-f).
28
Respiratory Kinematic Analysis
Respiratory oscillation movements were analyzed during the same time
frame analyzed for the audio recordings to compare simultaneous respiratory
kinematic and acoustic patterns.
Respiratory Kinematic Oscillation Rate
The rate of respiratory kinematic oscillation was determined by identifying
peak-to-peak or trough-to-trough patterns of the modulating waveform per
second from the summated rib cage and abdominal voltage signal (see Figure 5).
The rate of oscillation was determined from the number of cycles recorded
per second (Hz).
Respiratory Kinematic Measure Adjustments for Slope
Given that participants sustained phonation while producing vibrato or
AMVT, the lung volume continually decreased across the recorded trials. Thus,
adjustments to the respiratory measures were needed to reduce, or eliminate the
changing lung volume effect on measures obtained over the duration of the
recording. To achieve this, the mean slope of each signal was calculated for
each 2-s segment and factored in to each maximum and minimum value
obtained to adjust for the slope (see Figure 6). The mean slope of the entire
signal was multiplied by the time point associated with the maximum or minimum
value within the 2-s signal and then added to the value measured at the peak
and valley values of the modulating respiratory kinematic signal. Note that the
time point value is based on a 0-2 s time interval, rather than the timestamp of
the entire recording. For example, the 2-s window in Figure 6 took place at
29
Figure 5. Example of determining rate for respiratory kinematic oscillation. Each arrow marks the peak of each modulation cycle displayed in the 2-s window. A total of 11 peak-to-peak cycles are shown in the 2-s window giving a 5.5 Hz respiratory kinematic rate.
Figure 6. Example of measuring extent of respiratory kinematic oscillation. The minimum and maximum values associated with summated rib cage and abdominal movements in the figure represent the original data points. The original data points were corrected before extent was calculated. After adjustment for the sloping values, the relative %VC extent was calculated as described above.
30
timestamp 48-50 s. Therefore, a timestamp of 48.783 s for the data point would
be equal to an adjusted time point value of 0.783 s. The equation used to adjust
the kinematic %vital capacity (%VC) measures to eliminate the slope
effects is shown in equation 1 below: y corrected = y original + [mean slope * time point max/min] (1) Thus, with reference to the values displayed in Figure 6, the following
calculations were completed to obtain the adjusted maximum and minimum
Acoustic modulation patterns of fo and SPL were measured from the
middle 2-s portion of each recorded trial. The fo and SPL values within each
selected acoustic segment for analysis were displayed in Praat (Boersma &
Weenink, 2015; v 5.4.09) for analysis of rate and extent of modulation.
Acoustic Modulation Rate
The 2-s segments of fo and SPL modulation were analyzed for rate by
counting the number of peak-to-peak or trough-to-trough fo and SPL modulation
cycles displayed and dividing by 2-s to record rate of modulation in Hertz
(cycles/s) (see Figure 7). The number of fo and SPL modulation cycles per
s was determined for the signals displayed in Figure 7 with the following equation 3:
32
Figure 7. Example of fo (top line) and SPL (bottom line) plot of vibrato within Praat. Arrows have been added to the signal to indicate the beginning of the cycle. Rate (Hz) = (Number of cycles) / (time (s)) (3)
Rate for fo (top signal) is 9.5 cycles / 2-s = 4.8 Hz
Rate for SPL (bottom signal) is 9.5 cycles / 2-s = 4.8 Hz
Acoustic Modulation Extent
The extent of fo and SPL modulation for each cycle was determined by
measuring the maximum and the minimum values from the peak and valley
portions of each cycle (see Figure 8). The maximum and minimum values were
identified by importing the 2-s portion of the acoustic files being analyzed into
Praat. The modulation cycles were identified using the peak to peak or trough to
trough analysis (see Figure 8). Each cycle was then highlighted by dragging the
cursor across one cycle. Then, functions were completed within Praat to
calculate the maximum and minimum values of fo and SPL (i.e., get minimum
pitch, get maximum pitch, get minimum intensity, and get maximum intensity).
The respective values were then entered into an MS Excel spreadsheet for
calculation of the extent values.
33
Figure 8. Example of fo (top line) and SPL (bottom line) plot of vibrato within Praat. Arrows have been added to the signal to indicate the maximum and minimum points of cycle 3 (fo) and cycle 8 (SPL). fo Extent Measures
Calculation of fo extent was completed by subtracting the minimum fo value
from the maximum fo value and dividing the resulting value by the sum of the
maximum and minimum fo values of that cycle and multiplying by 100 to
determine a percentage value. This was repeated for all fo modulation cycles
within the selected segment of each trial as shown in the equation 4 below for Figure 8: Extent = (fo Max - fo Min) / (fo Max + fo Min) * 100 (4)
The extent of SPL modulation was determined from the maximum and
minimum dB SPL values associated with SPL modulation (see Figure 8). SPL
values were converted to a linear scale, Pascals, so that the same calculation
method used for fo extent could be performed for SPL extent. Using the values
shown in Figure 8 below, the following equation 5 offers an example of one cycle
of SPL modulation extent calculation:
34
SPL Extent = (SPL Max – SPL Min) / (SPL Max + SPL Min) * 100 (5)
Figure 8 Extent SPL = (.017 Pa - .016 Pa) / (.017 Pa + .016 Pa) * 100 = 3.03%
Laryngeal Imaging Kinematic Analysis
Frame by frame analysis of laryngeal oscillatory movements was
completed to determine the predominant pattern of laryngeal movement
associated with each voice modulation condition (vibrato vs. AMVT). Laryngeal
oscillation movements were analyzed from a similar or the same 2-s duration
segment as the respiratory kinematic and acoustic signals for each experimental
trial. Adjustments in the portion of the endoscopic recording were made if
pharyngeal or laryngeal postures occluded views of the vocal folds. During the
latter situations, the 2-s segment analyzed was shifted earlier or later as needed
to assure continuous views of the vocal folds for kinematic analysis. Given the
subjective impression that laryngeal movements remained continuous during all
trials, it was not expected that analysis from a shifted time segment would impact
measurement outcomes. The maximum and minimum range of vocal fold
movement in the anterior/posterior (i.e., lengthwise) and medial/lateral (i.e.,
abductor/adductor) directions was measured to determine laryngeal oscillation
rate and extent for comparison to acoustic and respiratory kinematic modulation
patterns. The endoscopic video recordings for each subject were imported into
QuickTime to select each of the mid-portion 2-s segments analyzed for the
acoustic and respiratory kinematic signals. The maximum and minimum
movement frames associated with each laryngeal movement cycle within the
analyzed segment were copied and imported into ImageJ (October, 2015) for
35
measurement.
Laryngeal Oscillation Rate
Laryngeal oscillation rate was determined by recording the number of
laryngeal oscillatory cycles obtained during the 2-s segment analyzed for
each trial divided by 2 s to determine the rate in Hertz (cycles/s).
Laryngeal Oscillation Extent
Extent of laryngeal oscillation was measured by identifying image frames
displaying the minimum and maximum displacement of laryngeal structures/vocal
folds during the predominant direction of oscillation (i.e., lengthwise versus
abduction/adduction). The lens to larynx distance varied during recordings,
requiring image measures to be normalized by creating a ratio of distance (unit =
pixels) between laryngeal movement measures and an anatomical measure
observed to remain constant (e.g., width of the epiglottis apex). Referent Anatomical Distance Measures
Individual frames judged to exhibit the maximum displacement end points
of laryngeal oscillation were selected and saved for analysis within ImageJ
software (Rasband, 2015). The referent anatomical distance between two
constant and clearly identifiable locations measuring the interarytenoid distance
was measured for each maximum and minimum cyclic displacement image (see
Figure 9, Part A and B). This was accomplished by drawing a line between the
two referent image points using the ImageJ line tool and recording the length of
the line in pixels.
36
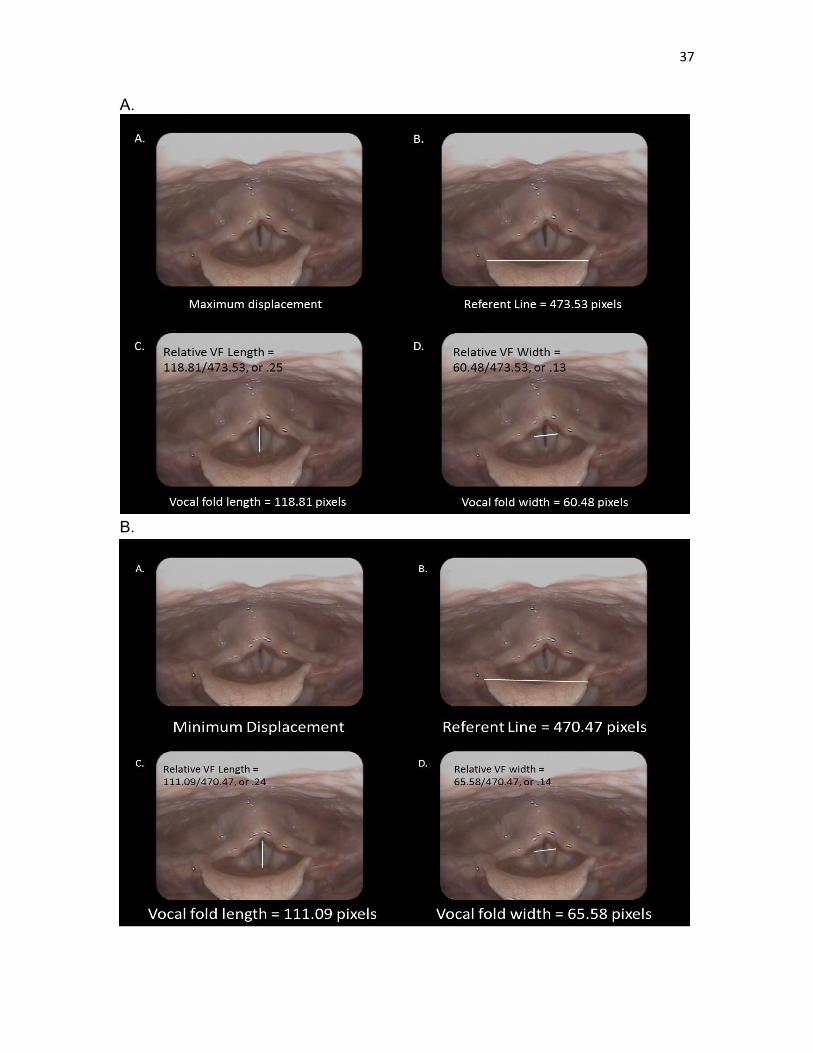
Figure 9. An example of laryngeal imaging measures for the first end point of one laryngeal oscillatory cycle. Each panel displays A) the image analyzed, B) the anatomical referent line measure, C) the relative measure of vocal fold length, and D) the relative measure of interarytenoid distance associated with the first end point of one laryngeal oscillation cycle. B. Example of laryngeal imaging measures for the second end point of one laryngeal oscillatory cycle. Each panel displays A) the image analyzed, B) the anatomical referent line measure, C) the relative measure of vocal fold length, and D) the relative measure of interarytenoid distance associated with the second end point of one laryngeal oscillation cycle.
37
A.
B.
38
Laryngeal Lengthwise Extent Measures
The length of the vocal folds during maximum and minimum laryngeal
cyclic movements was measured by drawing a line from the anterior commissure
(or most anterior visible portion of the vocal folds) and posterior commissure (or
most visible posterior point on the vocal folds) and recording the number of pixels
associated with the length. The magnitude, or extent, of lengthwise vocal fold
movement during the laryngeal movement cycle associated with vibrato or AMVT
was determined by dividing the vocal fold length measure (in pixels) by the
standard referent distance (in pixels) (see Figure 9). The extent of lengthwise
change was determined using the following equation (6) for
*Signifies measures that are significantly different between voicing conditions. Table 7. Vibrato voicing condition descriptive statistical summary for individual subjects.
*Signifies measures that are significantly different between voicing conditions.
Ackermann, H., & Ziegler, W. (1991). Cerebellar voice tremor: an acoustic analysis. Journal of Neurology, Neurosurgery & Psychiatry, 54(1), 74-76. Adler, C. H., Bansberg, S. F., Hentz, J. G., Ramig, L. O., Buder, E. H., Witt, K.,
Edwards, B. W., Krein-Jones, K., Caviness, J. N., (2004). Botulinum toxin type A for treating voice tremor. Archives of Neurology, 61(9), 1416-1420.
Anand, S., Shrivastav, R., Wingate, J. M., & Chheda, N. N. (2012). An acoustic-
perceptual study of vocal tremor. Journal of Voice, 26(6), 811-817. Anand, S., Wingate, J. M., Smith, B., & Shrivastav, R. (2012). Acoustic
parameters critical for an appropriate vibrato. Journal of Voice, 26(6), 819-825.
Barkmeier-Kraemer, J., Lato, K., & Wiley, K. (2011). Development of a speech treatment program for a client with essential vocal tremor. Seminars in Speech and Language, 32(1), 43-57.
Barkmeier-Kraemer, J., & Story, B. (2010). Conceptual and clinical updates on
vocal tremor. ASHA Leader, 15(14), 16-19. Boersma, Paul & Weenink, David (2015). Praat: doing phonetics by computer
[Computer program]. Version 5.4.09, Retrieved 2 June 2015 from http://www.praat.org/
Bové, M., Daamen, N., Rosen, C., Wang, C.-C., Sulica, L., & Gartner-Schmidt, J.
(2006). Development and validation of the vocal tremor scoring system. The Laryngoscope, 116(9), 1662-1667.
Brown, JR & Simonson, J (1963). Organic voice tremor. A tremor of phonation.
Neurology, 13, 520-525. Cohen, S. M., Jacobson, B. H., Garrett, C. G., Noordzij, J. P., Stewart, M. G.,
Attia, A., Cleveland, T. F. (2007). Creation and validation of the singing voice handicap index. Annals of Otology, Rhinology & Laryngology, 116(6), 402-406.
Dalvi, A., & Premkumar, A. (2011). Tremor: etiology, phenomenology, and
Dromey, C., & Smith, M. E. (2008). Vocal tremor and vibrato in the same person: acoustic and electromyographic differences. Journal of Voice, 22(5), 541-545.
Dromey, C., Warrick, P., & Irish, J. (2002). The influence of pitch and loudness
changes on the acoustics of vocal tremor. Journal of Speech, Language & Hearing Research, 45(5), 879.
Farinella K. A., Hixon T. J., Hoit J. D., Story B. H., Jones P. A. (2006). Listener
perception of respiratory-induced voice tremor. American Journal of Speech Language Pathology, 15(1):72-84.
Finnegan, E. M., Luschei, E. S., Barkmeier, J. M., & Hoffman, H. T. (2003).
Synchrony of laryngeal muscle activity in persons with vocal tremor. Archives of Otolaryngology–Head & Neck Surgery, 129(3), 313-318.
Gamboa, J., Jiménez-Jiménez, F. J., Nieto, A., Cobeta, I., Vegas, A., Ortí-Pareja,
M., García-Albea, E. (1998). Acoustic voice analysis in patients with essential tremor. Journal of Voice, 12(4), 444-452.
Gurey, L., Sinclair C., & Blitzer, A. (2013). A new paradigm for the management
of essential vocal tremor with botulinum toxin. Laryngoscope, 123(10), 2497-2501.
Guzman, M. A., Dowdall, J., Rubin, A. D., Maki, A., Levin, S., Mayerhoff, R., &
Jackson-Menaldi, M. C. (2012). Influence of emotional expression, loudness, and gender on the acoustic parameters of vibrato in classical singers. Journal of Voice, 26(5), 675.
Howes, P., Callaghan, J., Davis, P., Kenny, D., & Thorpe, W. (2004). The
relationship between measured vibrato characteristics and perception in Western operatic singing. Journal of Voice, 18(2), 216-230.
Hsiao, T.-Y., Solomon, N. P., Luschei, E. S., & Titze, I. R. (1994). Modulation of
fundamental frequency by laryngeal muscles during vibrato. Journal of Voice, 8(3), 224-229.
Jacobson, B. H., Johnson, A., Grywalski, C., Silbergleit, A., Jacobson, G.,
Benninger, M. S., & Newman, C. W. (1997). The voice handicap index (vhi) development and validation. American Journal of Speech- Language Pathology, 6(3), 66-70.
Jiang, J., Lin, E., & Hanson, D. G. (2000). Acoustic and Airflow Spectral Analysis
of Voice Tremor. Journal of Speech, Language & Hearing Research, 43(1), 191.
63
Kendall, K. A., & Leonard, R. J. (2011). Interarytenoid muscle botox injection for treatment of adductor spasmodic dysphonia with vocal tremor. Journal of Voice, 25(1), 114-119.
Kirkpatrick, A. (2008). Teaching methods for correcting problematic vibratos:
using sustained dynamic exercises to discover and foster healthy vibrato. Journal of Singing, 64(5), 551-556.
Kotby, M., & Fex, B. (1998). the accent method: behavior readjustment voice
therapy. Logopedics Phoniatrics Vocology, 23(1), 39-43. Kotby, M., Shiromoto, O., & Hirano, M. (1993). The accent method of voice
therapy: Effect of accentuations on FO, SPL, and airflow. Journal of Voice, 7(4), 319-325.
Lederle, A., Barkmeier-Kraemer, J., & Finnegan, E. (2012). Perception of vocal
tremor during sustained phonation compared with sentence context. Journal of Voice, 26(5), 668-669.
Lester, R. A., Barkmeier-Kraemer, J., & Story, B. H. (2013). Physiologic and
acoustic patterns of essential vocal tremor. Journal of Voice, 27(4), 422-432.
Louis, E. D., & Machado, D. G. (2015). Tremor-related quality of life: A
comparison of essential tremor vs. Parkinson's disease patients. Parkinsonism & Related Disorders, 21(7), 729-735.
Lowell S. Y., Barkmeier-Kraemer J. M., Hoit J. D., Story B. H. (2008).
Respiratory and laryngeal function during spontaneous speaking in teachers with voice disorders. Journal of Speech, Language, and Hearing Research, 51(2):333-49.
Lundy, D. S., Roy, S., Xue, J. W., Casiano, R. R., & Jassir, D. (2004).
Spastic/spasmodic vs. tremulous vocal quality: motor speech profile analysis. Journal of Voice, 18(1), 146-152.
Pettersen, V., & Westgaard, R. H. (2005). The activity patterns of neck muscles
in professional classical singing. Journal of Voice, 19(2), 238-251. Prame, E. (1994). Measurements of the vibrato rate of ten singers. The Journal
of the Acoustical Society of America, 96(4), 1979-1984. Ramig, L. A., & Shipp, T. (1987). Comparative measures of vocal tremor and
vocal vibrato. Journal of Voice, 1(2), 162-167. Rasband, W.S., ImageJ, U. S. National Institutes of Health, Bethesda, Maryland,
USA, Retrieved from http://imagej.nih.gov/ij/, 2015
64
Schneider, S. A., & Deuschl, G. (2015). Medical and surgical treatment of tremors. Neurologic Clinics, 33, 57-75.
Seashore, C. E. (1931). The natural history of the vibrato. Proceedings of the
National Academy of Sciences of the United States of America, 17(12), 623-626.
Story, B. H. (1995). Physiologically-based speech simulation using and
enhanced wave-reflection model of the vocal tract. (Unpublished doctoral dissertation). University of Iowa, Iowa City, IA.
Sulica, L., & Louis, E. D. (2010). Clinical characteristics of essential voice tremor:
A study of 34 cases. The Laryngoscope, 120(3), 516-528. Sundberg, J. (1994). Acoustic and psychoacoustic aspects of vocal vibrato. STL-
QPSR, 35(2-3), 045-068. Taha, J. M., Janszen, M. A., & Favre, J. (1999). Thalamic deep brain stimulation
for the treatment of head, voice, and bilateral limb tremor. Journal of Neurosurgery, 91(1), 68-72.
Titze, I. R., Story, B., Smith, M., & Long, R. (2002). A reflex resonance model of
vocal vibrato. The Journal of the Acoustical Society of America, 111(5), 2272-2282.
dysregulation of voluntary expiratory muscles. Neurology, 37(1), 117-122. Warrick, P., Dromey, C., Irish, J., Durkin, L., Pakiam, A., Lang, A. (2000).
Botulinum toxin for essential tremor of the voice with multiple anatomical sites of tremor: a crossover design study of unilateral versus bilateral injection. Laryngoscope, 110(8), 1366-74.
Watson, A. H. D., Williams, C., & James, B. V. (2012). Activity patterns in
latissimus dorsi and sternocleidomastoid in classical singers. Journal of Voice, 26(3), 95-105.
Wolraich, D., Marchis-Crisan, C.V., Redding, N., Khella, S.L., & Mirza, N. (2010).
Laryngeal tremor: co-occurrence with other movement disorders. Otorhinolaryngology, 72, 291–294.