Tetrabenazine Tetrabenazine Prestwick Pharmaceuticals, Inc. Prestwick Pharmaceuticals, Inc. New Drug Application 21- New Drug Application 21- 894 894 Peripheral and Central Nervous System Peripheral and Central Nervous System Drugs Advisory Committee Meeting Drugs Advisory Committee Meeting Beltsville, Maryland Beltsville, Maryland December 6, 2007 December 6, 2007 Review of Safety Review of Safety Lourdes Villalba, M.D. Lourdes Villalba, M.D. Division of Neurology Drug Products (DNP) Division of Neurology Drug Products (DNP) Center for Drug Evaluation and Research Center for Drug Evaluation and Research
Transcript
TetrabenazineTetrabenazinePrestwick Pharmaceuticals, Inc.Prestwick Pharmaceuticals, Inc. New Drug Application 21-894New Drug Application 21-894
TetrabenazineTetrabenazinePrestwick Pharmaceuticals, Inc.Prestwick Pharmaceuticals, Inc. New Drug Application 21-894New Drug Application 21-894
Peripheral and Central Nervous System Drugs Peripheral and Central Nervous System Drugs Advisory Committee MeetingAdvisory Committee MeetingBeltsville, MarylandBeltsville, MarylandDecember 6, 2007December 6, 2007
Review of SafetyReview of SafetyLourdes Villalba, M.D. Lourdes Villalba, M.D. Division of Neurology Drug Products (DNP)Division of Neurology Drug Products (DNP)
Peripheral and Central Nervous System Drugs Peripheral and Central Nervous System Drugs Advisory Committee MeetingAdvisory Committee MeetingBeltsville, MarylandBeltsville, MarylandDecember 6, 2007December 6, 2007
Review of SafetyReview of SafetyLourdes Villalba, M.D. Lourdes Villalba, M.D. Division of Neurology Drug Products (DNP)Division of Neurology Drug Products (DNP)
Center for Drug Evaluation and ResearchCenter for Drug Evaluation and Research
2
OverviewOverview
• Limitations of safety database• Safety in study 004 and other studies
• Small – 111 unique subjects with HD in Prestwick’s studies
• Flexible-dose design – Titration up to “desired” effect, maximum dose of
100 mg/day, or “intolerable” AEs over 7 weeks• At the investigator’s discretion
• Complex disease– Some of AEs associated with TBZ difficult to
distinguish from underlying disease • Depression; dysphagia & bradykinesia in late HD
• Small – 111 unique subjects with HD in Prestwick’s studies
• Flexible-dose design – Titration up to “desired” effect, maximum dose of
100 mg/day, or “intolerable” AEs over 7 weeks• At the investigator’s discretion
• Complex disease– Some of AEs associated with TBZ difficult to
distinguish from underlying disease • Depression; dysphagia & bradykinesia in late HD
4
NDA DatabaseNDA Database NDA DatabaseNDA DatabaseProtocol Design N
TBZ/Pla
TBZ dose(mg/day)
Sites
Prestwick’s sponsored studies
004
007
R, DB, PC, 12 wks
OL extension, 80 wks
54/30
75/0
12.5 – 100
12.5 – 200
16
16
005
006
R, DB, PC, staggered withdrawal, 5 days OL extension, 48 wks
30-24
29/0
Up to 150
Up to 150
1
1
Other data (Baylor studies)
Chorea – 011
Non-chorea
OL, dose titration
OL, compassion. use up to several years
1621
2802
12.5 – 200
12.5 - 200
1
1R= randomized; DB= double-blind; PC= placebo-controlled; OL= open label; N= patients randomized to TBZ. 1 Available for 98 patients with HD chorea and 47 with non-HD chorea. 2 Available for 247 patients. Total number of patients with HD exposed to TBZ in Prestwick-sponsored studies: 111.
Healthy subjects in clinical pharmacology studies (n=259) are not included.
5
TBZ Safety - Study 004 (I)TBZ Safety - Study 004 (I)TBZ Safety - Study 004 (I)TBZ Safety - Study 004 (I)
TBZ
N=54 n (%)
PlaceboN=30 n (%)
Death (suicide) 1 (1.9) 0
Non-fatal Serious AEs Breast cancer Fall/ subarachnoid hemorrhage Restlessness (Suicidal ideation/ paranoid psychosis)
3 (5.6) 0
Discontinuations due to AEs1 5 (9.2) 0
Dose reduction or stopping upward titration due to AEs
28 (52.0) 1 (3.3)
n= Number of patients with AE. 1 Death & Serious AEs plus one case of akathisia.
6
TBZ Safety - Study 004 (II)TBZ Safety - Study 004 (II)TBZ Safety - Study 004 (II)TBZ Safety - Study 004 (II)
AEs that led to dose reduction or stopping upward titration
TBZN=54 n (%)
PlaceboN=30 n (%)
All Sedation Akathisia Depression Parkinsonism Restlessness Anxiety Other
28 (52)1
15 (28) 5 (9) 3 (6) 4 (7) 2 (4) 2 (4)
2 (4)2
1 (3) 0 0 0 0 0 0
1 (3)3
n= number of patients with AE. 1 Some patients had more than one event. 2 Other: one fatigue, one diarrhea. 3 Dizziness.
7
AEs of InterestAEs of InterestAEs of InterestAEs of Interest
• Akathisia, parkinsonism, depression and dysphagia
– Recognized as a potential drug-related AE?
– Dose related?• Response to dose reduction?
– Effects on Total Chorea Scores (TCS)?
• Akathisia, parkinsonism, depression and dysphagia
– Recognized as a potential drug-related AE?
– Dose related?• Response to dose reduction?
– Effects on Total Chorea Scores (TCS)?
8
AE of Interest in Study 004AE of Interest in Study 00411AE of Interest in Study 004AE of Interest in Study 00411
TBZ (N=54)n (%)
Placebo (N=30)n (%)Sponsor FDA2
Akathisia 5 (9) 7 (13) 0
Parkinsonism 5 (13) 8 (15) 0
Depression 8 (15) 10 (19) 0
Dysphagia 1 (2) 2 (4) 1 (3)
1 Source: Adverse event & concomitant medication listings and UH file (Comments in the UHDRS dataset, submitted 9/05). One patient may have had more than one adverse event.
2 Cases not included in sponsor’s analyses: Two cases of akathisia, one of parkinsonism and one dysphagia recorded in UH file but not listed in AE listing; two additional cases from AE listings consistent with parkinsonism; one retrospective diagnosis of depression in patient who committed suicide; one case of depression/paranoid psychosis/suicidal ideation. Discrepancy points to difficulty in ascertainment and coding.
9
AE of Interest in Studies 007 & 006AE of Interest in Studies 007 & 006AE of Interest in Studies 007 & 006AE of Interest in Studies 007 & 006
007 (multi-center)
(N= 75)
006 (single-center)
(N= 29)Sponsor
nFDAn (%)
Sponsorn
FDAn (%)
Akathisia 15 15 (20) - -
Parkinsonism 2 2 (3) 3 3 (10)
Depression1 24 26 (35) 9 10 (35)
Dysphagia2 3 6 (8) 3 3 (10)N= patients on TBZ. 1As per medication file 2 additional patients in 007 and one in 006 changed their antidepressant regimen (dose increased, antidepressant added or switched) to treat depression, but were not recorded in AE listings. 3 Three additional cases of choking in the AE listing for study 007.
10
AE of Interest in Studies 004, 007 AE of Interest in Studies 004, 007 & 006 - FDA Analysis& 006 - FDA Analysis
AE of Interest in Studies 004, 007 AE of Interest in Studies 004, 007 & 006 - FDA Analysis& 006 - FDA Analysis
004 (N=54)
n
007 (N= 75)
n
006 (N= 29)
n
All
(N=111)Eventsa Patients(%)
Akathisia 7 15 - 22 20 (18)
Parkinsonism 8 2 3 13 13 (12)
Depression 10 26 10 51 44 (40)
Dysphagia 2 6 3 11 11 (10)N= patients on TBZ (total does not add up because some patients in 004 rolled into 007). n= patients with event. a Events. A patient may have the same event twice.
11
Akathisia, Study 004 (n=7)Akathisia, Study 004 (n=7)Akathisia, Study 004 (n=7)Akathisia, Study 004 (n=7)
• Known to occur with other dopamine antagonists
• Sponsor identified 5 cases
• FDA identified 2 additional cases of Akathisia– ID# 236. Listed as restlessness in AE file; recorded as
akathisia in UH file 1 – ID# 267. Not listed in AE listing; mild akathisia recorded
in UH file 1
• All on TBZ
• Known to occur with other dopamine antagonists
• Sponsor identified 5 cases
• FDA identified 2 additional cases of Akathisia– ID# 236. Listed as restlessness in AE file; recorded as
akathisia in UH file 1 – ID# 267. Not listed in AE listing; mild akathisia recorded
in UH file 1
• All on TBZ 1“UH” file containing United Huntington’s Disease Research Score UHDRS) values and investigators’ comments, submitted September 2005. There were 4 additional cases of “restlessness” in the AE listings.
12
ID# TCSa
Db 0AE Dose reduction (DR):
Yes/No Outcome: Rd, Ce, WDf, NAg
TCSAfter AEh
TCSD 84i
(dose)D Onset (dosec)
DEnd
208 12 D 59 (100)
D 92 No. R after C
12 16 (100)
229 14 D 19 (50)
D 88 No. R after C
12 15 (100)
246 13 D 43 (100)
D 71 Yes. Early WD, D 50R after WD
6 NA
248 11 D 63 (75)
D 63 Yes. R with DR. Recurred (007)
11* 9 (37.5)
Akathisia, Study 004 (I)Akathisia, Study 004 (I)
aTCS= Total Chorea Score (Baseline dose= 0). bD= relative day. cTBZ dose in mg/day. dResolved. eC= study completion. fWD= withdrawal. gNA= not available. hTCS at next available visit. iApproximate day for 12 week visit. Source: Sponsor’s tables. * 248 had TCS on day 21 (50 mg/d)= 6.
13
ID# TCSa
D 0b AE Dose reduction (DR):
Yes/No Outcome: Rd, Ce, WDf, NAg
TCSAfter AEh
TCSD 84i
(dose)Onset (dosec)
End
279 11 D 36 (75)
D 38 Yes R with DR. Recurred (007)
8 9(37.5)
236 20 40 (50)
D 55 Yes j
R with DR10j 10
(37.5)
267 19 51(62.5)
- Nok Dose ↓ for sedation & depression.Outcome of akathisia NA
12 8(50)
Akathisia, Study 004 (II)Akathisia, Study 004 (II)
aTCS= Total Chorea Score (Baseline dose= 0). bD= relative day. cTBZ dose in mg/day. dR=Resolved, eWD= withdrawal. fNA= not available. g TCS at next available visit. Italics= not included in sponsor’s analysis. j236, coded as restlessness in AE file but recorded as akathisia in UH file. TCS on Day 21 (50 mg/d)= 11. k267 Akathisia not in AE listing.
14
Summary of Akathisia in Study 004 Summary of Akathisia in Study 004 (n= 7, all TBZ)(n= 7, all TBZ)
Summary of Akathisia in Study 004 Summary of Akathisia in Study 004 (n= 7, all TBZ)(n= 7, all TBZ)
• Median Dose at onset (mg/d) 75 (range, 50-100)
• Median Time to onset (days) 43 (range,19-59)
• Led to dose reduction (DR) or withdrawal (WD)
n= 4a n= 1
• Outcome Resolved after DR“ after completion“ after withdrawal Not available
• Patients with drop in TCS ≥3 at Week 12 2 out of 7
Additionally, there were 4 cases of restlessness. Some cases of restlessness may be difficult to distinguish from akathisia.
15
ID# TCSa
D 0b AE Dose Reduction (DR):
Yes/No Outcome: Rd, Ce, WDf,NAg
TCSAfter AEh
TCSD 84i
(dose)Onset (dosec)
End
213 19 D 48(87.5)
D 98 Yes. [Hospitalized multiple medsj]. R when TBZ stopped but recurred when TBZ restarted. WD for suicidal ideation & psychosis on D 71.
10 NA
217 13 D 52 (100)
D 75 Yes. R with DR 6 8 (87.5)
238 14 D 48 (100)
D 68 Yes. R with DR 7 8(75)
275 15 D 7(37.5)
D 7 No. R without DR 10 4(100)
Restlessness, Study 004 (II)Restlessness, Study 004 (II)
aTCS= Total Chorea Score (Baseline dose= 0). bD= relative day. cTBZ dose in mg/day. dDR= dose reduction. eResolved, fC= completed. gD= withdrawal. hNA= not available. i TCS at next available visit. J Week 12 approximate day. j Patient 213 received klonopin, restoril, aprazolam, lorazepam, beta blockers, bupropion, secobarbital and mirtazapine. Based on BARNES’ scores, the sponsor agrees all 4 cases are consistent with akathisia.
16
Parkinsonism, Study 004 (n=8)Parkinsonism, Study 004 (n=8)Parkinsonism, Study 004 (n=8)Parkinsonism, Study 004 (n=8)
• Known to occur with dopamine antagonists; also manifestation of late HD
• Sponsor identified 5 cases
• FDA identified 3 additional cases– ID# 231, “Bradykinesia worse” 1 – ID# 233, “Stiffness when walking”2
– ID# 240, “Decreased dexterity, coordination abnormal, balance difficulty” (along with dysphagia, dysarthria and insomnia) 2
• All on TBZ
• Known to occur with dopamine antagonists; also manifestation of late HD
• Sponsor identified 5 cases
• FDA identified 3 additional cases– ID# 231, “Bradykinesia worse” 1 – ID# 233, “Stiffness when walking”2
– ID# 240, “Decreased dexterity, coordination abnormal, balance difficulty” (along with dysphagia, dysarthria and insomnia) 2
• All on TBZ
1 Source: UH file. 2 Source: AE listings.
17
ID# TCSa
D 0b AE Dose reduction (DR):
Yes/No Outcome: Rd, Ce, WDf, NAg
TCSAfter AEh
TCSD 84i
(dose)Onset (dosec)
End
203 13 D 17 (50)
D 90 No. Intensity ↑ to severe D 32 (TBZ 75mg/d). Dose ↓ for sedation. Intensity ↓ mod. D 56. R after C
7 9 (37.5)
207 16 D 28(62.5)
D 29 Yes. R with DR. 12 3(25)
224 10 D 25 (62.5)
- Yes. Ongoing at entry in 007; lost to FU on D 7 (admitted to NH facility)
7 7 (50)
236 20 D 18 (50)
D 45 No. Dose ↓ to 37.5 mg/d because of disorientation & sedation on D 23. R with DR.
11 10 (37.5)
263 10 D 50(87.5)
D 71 (Yes) R with DR. 0 4 (50)
Parkinsonism, Study 004 (I)Parkinsonism, Study 004 (I)
18
ID# TCSa
D 0b AE Drug Reduction (DR):
Yes/No Outcome: Rd, Ce, WDf,Nag
TCSAfter AEh
TCSD 84i
(dose)Onset (dosec)
End
231 19 D 36(75)
- No. “Bradykinesia worse” recorded in UH file. Dose ↓ for depression. Outcome NA (not recorded as AE)
9
12(50)
233 20 D 36(75)
- No. “Stiffness when walking” and sedation. Outcome NA*
19
22 (87.5)
240 15 D 29(75)
D 50 Yes. “Coordination abnorm., balance difficulty”, also fatigue, dysphagia, dysarthria & insomnia. Most events R with DR on D 50.
18
17 (50)
Parkinsonism, Study 004 (II)Parkinsonism, Study 004 (II)
aTCS= Total Chorea Score (Baseline dose= 0). bD= relative day. cTBZ dose in mg/day. dR=Resolved, eWD= withdrawal. fNA= not available. gTCS at next available visit. h Approximate day for 12 week visit. *No ending date for event; “safer with rolling walker” on D 63; TBZ up to 125mg/d in 007 without reported AE of parkinsonism.
19
Summary Parkinsonism in Study 004Summary Parkinsonism in Study 004 (n= 8) (n= 8)
Summary Parkinsonism in Study 004Summary Parkinsonism in Study 004 (n= 8) (n= 8)
• Median Dose at onset (mg/d) 62.5 (range, 50 - 87.5)
• Median Time to onset (days) 28 (range, 17 – 36)
• Led to dose reduction (DR) or Withdrawal
n= 4a n= 0
• Outcome Resolved after DRResolved after CompletionNot available
n= 4 (1 day – 3 wks) n= 1 (6 days) n= 3 (1 lost to FU, 1 no end date for AE, 1 not in AE listing)
• Patients with drop in TCS ≥3 at Wk 12 6 out of 8
a Additionally, 3 underwent dose reduction because of other AEs (depression, sedation and disorientation).
20
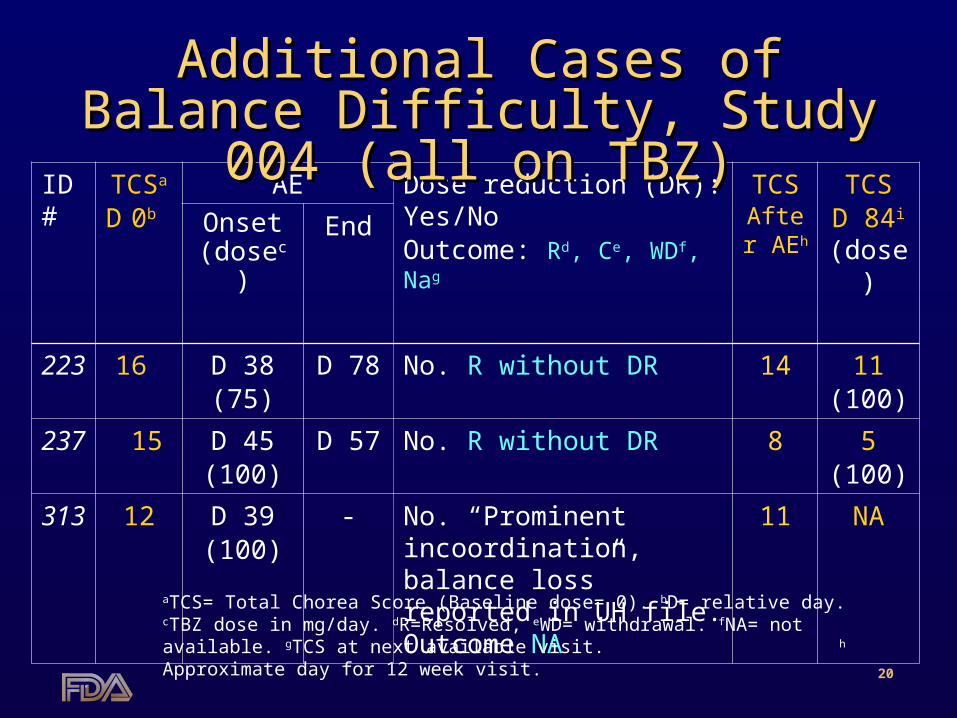
ID# TCSa
D 0b AE Dose reduction (DR):
Yes/No Outcome: Rd, Ce, WDf, Nag
TCSAfter AEh
TCSD 84i
(dose)Onset (dosec)
End
223 16 D 38(75)
D 78 No. R without DR 14 11(100)
237 15 D 45(100)
D 57 No. R without DR 8 5(100)
313 12 D 39(100)
- No. “Prominent incoordination, balance loss” reported in UH file. Outcome NA
11 NA
Additional Cases of Balance Additional Cases of Balance Difficulty, Study 004 (all on TBZ)Difficulty, Study 004 (all on TBZ)
aTCS= Total Chorea Score (Baseline dose= 0). bD= relative day. cTBZ dose in mg/day. dR=Resolved, eWD= withdrawal. fNA= not available. gTCS at next available visit. h Approximate day for 12 week visit.
21
Potential Extrapyramidal Potential Extrapyramidal Symptoms (EPS) in study 004Symptoms (EPS) in study 004
Potential Extrapyramidal Potential Extrapyramidal Symptoms (EPS) in study 004Symptoms (EPS) in study 004
AE Verbatim Term TBZ N=54n (%)
PlaceboN=30n (%)
Akathisia (includes 2 in UH file)Bradykinesia (includes 1 in UH file)Slowness of movement Parkinsonism Stiffness when walkingDystoniaBalance & gait unsteady Poor coordination/gait unsteady Decreased dexterity/off balanceProminent incoordinat. balance loss
Patients with any
7 2a
21 11 1111
17 (32)
0000010000
1(3)
a One patient had both akathisia and bradykinesia
22
Depression/Worsening DepressionDepression/Worsening Depression Study 004 (n=10)Study 004 (n=10)
Depression/Worsening DepressionDepression/Worsening Depression Study 004 (n=10)Study 004 (n=10)
• Sponsor identified 8 cases • FDA identified 2 more cases
– ID# 271. Retrospective diagnosis based on signs of depression prior to suicide1
– ID# 213. Patient discontinued for depression, suicidal ideation/psychosis, received treatment with mirtazapine2
• Although depression is prevalent in patients with HD, there were no treatment-emergent cases on placebo.
• Biological plausibility for increased risk of depression with TBZ (↓ dopamine, serotonin & norepinephrine)
• Sponsor identified 8 cases • FDA identified 2 more cases
– ID# 271. Retrospective diagnosis based on signs of depression prior to suicide1
– ID# 213. Patient discontinued for depression, suicidal ideation/psychosis, received treatment with mirtazapine2
• Although depression is prevalent in patients with HD, there were no treatment-emergent cases on placebo.
• Biological plausibility for increased risk of depression with TBZ (↓ dopamine, serotonin & norepinephrine)
Depression, Study 004 (I)Depression, Study 004 (I)
aTCS= Total Chorea Score (Baseline dose= 0). bD= relative day. cTBZ dose in mg/day. dDR= dose reduction. eResolved, fC= completion gWD= withdrawal. hNA= not available. iTCS at next available visit. jApproximate day for 12 week visit. * AD= Antidepressant regimen. ** Δ= AD started, dose increased, switched, added.
24
ID# TCSa
D 0b AE Dose reduction (DR):
Yes/No Outcome: Rd, Ce, WDf,
NAg
AD* TCSAfter AEh
TCSD 84i
(dose)Onset (dosec)
End
244 12 D 50(37.5)
D 91 No. R after C Δ** 11 10(37.5)
251 10 D 31(75)
D 62 Yes. R with DR and Δ** .
Δ** 3 2(12.5)
267 19 D 51(62.5)
D 58 Yes. Also had mild akathisia. R with DR. Suicide attempt in 007.
Same 14 8(50)
274 12 D 737.5
D 33 No. R with Δ**
Δ** 12 8(62.5)
Depression, Study 004 (II)Depression, Study 004 (II)
aTCS= Total Chorea Score (Baseline dose= 0). bD= relative day. cTBZ dose in mg/day. dDR= dose reduction. eResolved, fC= completion gWD= withdrawal. hNA= not available. iTCS at next available visit. jApproximate day for 12 week visit. * AD= Antidepressant regimen. ** Changed= AD started, dose increased, switched, added to prior Rx.
25
ID# TCSa
D 0b AE Dose reduction (DR):
Yes/No Outcome: Rd, Ce, WDf,
NAg
AD* TCSAfter AEh
TCSD 84i
(dose)Onset (dosec)
End
271 22 D 50(87.5)
- No. Retrospective Dx in patient who committed suicide.
None 14 NA
213 19 D 69(12.5)
72 No. Dose had been ↓ for restlessness. Early WD b/c suicidal ideation, depression, psychosis & paranoid reaction on D 71.* R with Δ**
Δ** 9 NA
Depression, Study 004 (III)Depression, Study 004 (III)
aTCS= Total Chorea Score (Baseline dose= 0). bD= relative day. cTBZ dose in mg/day. dResolved, eC= completion fWD= withdrawal. gNA= not available. hhCS at next available visit. iApproximate day for 12 week visit. * AD= Antidepressant regimen. ** Δ= initiated mirtazapine for indication of depression. Patients ID 271 & 213 had no history of depression.
26
Summary Depression in Study 004Summary Depression in Study 004(n= 10)(n= 10)
Summary Depression in Study 004Summary Depression in Study 004(n= 10)(n= 10)
• Median Dose at onset (mg/d) 62.5 (range, 25 – 100)
• Median Time to onset (days) 50 (range, 4 – 82)
• Dose reduction (DR) for depression• Change in AD regimena
n= 3n= 5
• Outcomeb –Resolved with DR– “ after completion– “ after early WD– “ with AD treatment– “ with DR and AD treatment– Did not resolve
n= 2 (1 to 2 wks)
n= 2 (1 wk) n= 1c
n= 3d n= 1n= 1e
• Patients with drop in TCS ≥3 at Wk 12 5 out of 10
a AD= antidepressant medication started, increased, added or switched. b Two recurred in 007. c Early withdrawal because of fall and SA hemorrhage (resolved 4 weeks after WD) d Suicidal ideation resolved with AD treatment (mirtazapine). e One patient committed suicide.
27
Dysphagia in Study 004Dysphagia in Study 004Dysphagia in Study 004Dysphagia in Study 004
• Associated with TBZ at doses >100 mg/day
• In study 004 sponsor identified one case on TBZ and one on placebo.
• FDA identified one additional case – ID# 224: “occasional choking” not listed as AE but
recorded in UH file (on TBZ).
• Associated with TBZ at doses >100 mg/day
• In study 004 sponsor identified one case on TBZ and one on placebo.
• FDA identified one additional case – ID# 224: “occasional choking” not listed as AE but
recorded in UH file (on TBZ).
28
ID# TCSa
D 0b AE Dose reduction (DR):
Yes/No Outcome: Rd, Ce, WDf, Nag
TCSAfter AEh
TCSD 84i
(dose)Onset(dosec)
End
240 15 D 23(62.5)
61 Yes. R with DR. Also had dysarthria, balance diff. & lethargy. Did not enter 007
17 17(25)
224 10 D 32(50)
- No.j
Outcome NA. Ongoing. Lost to FU on D 7 of 007
7 7(50)
273 16 D 96Placebo
96 No. R same day. Preceded by dyspepsia, N,V,Dk & ulcerative stomatitis
14 14Placebo
Dysphagia in Study 004Dysphagia in Study 004
aTCS= Total Chorea Score (Baseline dose= 0). bD= relative day. cTBZ dose in mg/day. dResolved, eC= completion fWD= withdrawal. gNA= not available. hTCS at next available visit. iApproximate day for 12 week visit. j Choking recorded in UH file but not AE listing. k N, V, D= nausea, vomiting, diarrhea.
29
Dysphagia in 004Dysphagia in 004Dysphagia in 004Dysphagia in 004
• Small database, few cases• Can not rule out detrimental effect of
TBZ on dysphagia
• Small database, few cases• Can not rule out detrimental effect of
TBZ on dysphagia
30
Outcome for AE of InterestOutcome for AE of InterestStudies 004, 007 & 006Studies 004, 007 & 006
Outcome for AE of InterestOutcome for AE of InterestStudies 004, 007 & 006Studies 004, 007 & 006
• Recognized as a potential drug-related AEs by the investigator?
• Dose related?
• Effects on Total Chorea Scores (TCS)?
• Recognized as a potential drug-related AEs by the investigator?
• Dose related?
• Effects on Total Chorea Scores (TCS)?
31
Outcome for AE of InterestOutcome for AE of InterestStudies 004, 007 & 006Studies 004, 007 & 006
Outcome for AE of InterestOutcome for AE of InterestStudies 004, 007 & 006Studies 004, 007 & 006
• Recognized as a potential drug-related AE?– Not always
• Dose response for toxicity?– Strong suggestion of a dose response
• Dose at onset of first event were (mg/day) ≥ 50 (akathisia), ≥ 62.5 (parkinsonism), ≥ 25 (depression) & ≥ 50 (dysphagia)
• Response to dose reduction or discontinuation?– Yes, in general (unclear for depression & dysphagia)
• Total Chorea Scores after dose reduction?– In general, patients who had responded before
developing the AE maintained a drop in TCS ≥3 from baseline (if they did not discontinue TBZ).
• Recognized as a potential drug-related AE?– Not always
• Dose response for toxicity?– Strong suggestion of a dose response
• Dose at onset of first event were (mg/day) ≥ 50 (akathisia), ≥ 62.5 (parkinsonism), ≥ 25 (depression) & ≥ 50 (dysphagia)
• Response to dose reduction or discontinuation?– Yes, in general (unclear for depression & dysphagia)
• Total Chorea Scores after dose reduction?– In general, patients who had responded before
developing the AE maintained a drop in TCS ≥3 from baseline (if they did not discontinue TBZ).
32
Does TBZ 50 mg/day have a better Does TBZ 50 mg/day have a better benefit/risk profile than 100 mg/day? benefit/risk profile than 100 mg/day?
Is there a need to increase the dose Is there a need to increase the dose to the point that toxicity develops?to the point that toxicity develops?
Does TBZ 50 mg/day have a better Does TBZ 50 mg/day have a better benefit/risk profile than 100 mg/day? benefit/risk profile than 100 mg/day?
Is there a need to increase the dose Is there a need to increase the dose to the point that toxicity develops?to the point that toxicity develops?
33
Number of Responders (TCS drop of Number of Responders (TCS drop of ≥≥3) 3) at Week 12, by doseat Week 12, by dose
Source: Listing 1.2 Appendix 4 of Complete Response (Feb 2007)
34
TCS Median Change (TCS Median Change (±±SE) from Baseline SE) from Baseline Over Time By Responder Status at Week 12Over Time By Responder Status at Week 12TCS Median Change (TCS Median Change (±±SE) from Baseline SE) from Baseline
Over Time By Responder Status at Week 12Over Time By Responder Status at Week 12
-9
-8
-7
-6
-5
-4
-3
-2
-1
0
1
Del
ta T
CS
Wk 3 Wk 7 Wk 12
Responder
Non responder
35
TCS Median Change (TCS Median Change (±±SE) from SE) from Baseline Over Time Baseline Over Time
in Responders at Week 12in Responders at Week 12
TCS Median Change (TCS Median Change (±±SE) from SE) from Baseline Over Time Baseline Over Time
in Responders at Week 12in Responders at Week 12
AE Requiring
dose reduction
-10
-9
-8
-7
-6
-5
-4
-3
-2
-1
0
Responder > 50-100 mg/d
Responder ≤ 50 mg/d
Wk 3 Wk 7 Wk 12
Del
ta T
CS
36
Does TBZ 50 mg/day have a better Does TBZ 50 mg/day have a better benefit/risk profile than 100 mg/day? benefit/risk profile than 100 mg/day?
Is there a need to increase the dose Is there a need to increase the dose to the point that toxicity develops? to the point that toxicity develops?
Does TBZ 50 mg/day have a better Does TBZ 50 mg/day have a better benefit/risk profile than 100 mg/day? benefit/risk profile than 100 mg/day?
Is there a need to increase the dose Is there a need to increase the dose to the point that toxicity develops? to the point that toxicity develops?
• Can not be answered in this database
37
Other Safety IssuesOther Safety IssuesOther Safety IssuesOther Safety Issues
• Sedation– Clearly dose related
• Falls – No reduction as compared to placebo in 004
• Hyperprolactinemia – Observed in clinical trials
• Can the risk for depression and other adverse events be minimized?
• Are there actions, in addition to appropriate patient and prescriber labeling, that the sponsor could undertake to insure that tetrabenazine could be given safely?
• Can the risk for depression and other adverse events be minimized?
• Are there actions, in addition to appropriate patient and prescriber labeling, that the sponsor could undertake to insure that tetrabenazine could be given safely?
41
TBZ SummaryTBZ SummaryTBZ SummaryTBZ Summary• HD is a complex disease
• TBZ is effective in reducing TCS in patients with HD
• Safety profile consistent with other dopamine antagonists.
• Major Issues: –Depression/suicidality–Extrapyramidal symptoms
• Difficult to recognize AEs as being drug-related
• HD is a complex disease
• TBZ is effective in reducing TCS in patients with HD
• Safety profile consistent with other dopamine antagonists.
• Major Issues: –Depression/suicidality–Extrapyramidal symptoms
• Difficult to recognize AEs as being drug-related
42
AcknowledgementsAcknowledgementsAcknowledgementsAcknowledgements– Office of Surveillance & Epidemiology, RiskMAP Review Team
• Mary Willy • Claudia Karwoski • Joyce Weaver • Mary Dempsey
– Division of Neurology Drug Products• Alice Hughes • Susan Daugherty• Elizabeth McNeil• John Feeney
43
Depression Depression Baseline Risk Factors in Study 004Baseline Risk Factors in Study 004
Depression Depression Baseline Risk Factors in Study 004Baseline Risk Factors in Study 004
Measurement TBZN=54
PlaN=30
Patients with Past Hx of depression (%) 34 (63%) 14 (47%)
Yes, Q 38 of UHDRS (%) 8 (15%) 2 (7%)
Mean HAM-D score ± SD (range)
4.5 ± 3.4 (0-14)
5.1 ± 3.9 (0-14)
Antidepressant use at baseline
30 (56%) 20 (67%)
Q 25 of UHDRS (%) 0 0
HAM-D: 17-item Hamilton Depression scale; UHDRS: Unified Huntington’s Disease Rating Scale. Question 38: “Does the investigator believe the patient is depressed?”. Q 25: suicidal ideation.
44
Depression Depression Patients with recurrent eventPatients with recurrent event
Depression Depression Patients with recurrent eventPatients with recurrent event
ID 1st episode 2nd episode
Onset(day/dose)
Action Resol(day)
Onset(day/dose)
Action Resol(day)
4-231* 24 (62.5) DR 40 24 (62.5) DR 32
4-267* 51 (62.5) DR 58 125 (62.5) DR+AD WD1
7-209 145 (62.5) DR+AD 359 535 (25) AD Ongoing
7-252 2 (12.5) AD 44 183 (25) AD 237
7-266 56 (75) AD 169 337 (50) AD Ongoing
7-288 50 (50) DR+AD 182 355 (50) AD 5802
7-291 42 (87.5) DR 71 210 (75) None 5962
DR= Dose reduction. AD= change in antidepressant regimen. WD= withdrawal. * Second episode occurred in study 007. 1TBZ WD on D 463 because of worsening depression. Psychosis with depressive features started on D 466. Event resolved on day 473. 2 Resolved after Week 80 (2-3 weeks after study completion date).
45
Narrative of Subject Who Narrative of Subject Who Committed Suicide in Study 004Committed Suicide in Study 004
Narrative of Subject Who Narrative of Subject Who Committed Suicide in Study 004Committed Suicide in Study 004
• ID# 447-271. 40 y.o. male randomized to TBZ. Reported suicidal ideation in the past. No concomitant meds at the time of enrollment. Baseline TCS= 22.
• At week 3 (TBZ 62.5 mg/d), TCS= 14. Total HAM-D score was 0, including 0 suicidal thoughts.
• At week 7 (TBZ 87.5 mg/d), TCS was stable. HAM-D score was 1 due to early morning awakening.
• After this visit the patient decided to stop working because of his disability. Subsequently, his mood and behavior changed dramatically. He spent most of his time in his room at home and sometimes did not come out for meals. He committed suicide. The investigator judged that the AE was possibly related to study drug.
• ID# 447-271. 40 y.o. male randomized to TBZ. Reported suicidal ideation in the past. No concomitant meds at the time of enrollment. Baseline TCS= 22.
• At week 3 (TBZ 62.5 mg/d), TCS= 14. Total HAM-D score was 0, including 0 suicidal thoughts.
• At week 7 (TBZ 87.5 mg/d), TCS was stable. HAM-D score was 1 due to early morning awakening.
• After this visit the patient decided to stop working because of his disability. Subsequently, his mood and behavior changed dramatically. He spent most of his time in his room at home and sometimes did not come out for meals. He committed suicide. The investigator judged that the AE was possibly related to study drug.
46
Narrative of Subject With Narrative of Subject With Suicidal Ideation in Study 004Suicidal Ideation in Study 004
Narrative of Subject With Narrative of Subject With Suicidal Ideation in Study 004Suicidal Ideation in Study 004
• ID# 447-213. 62 y.o. male randomized to TBZ. No prior history of depression. No concomitant meds at the time of enrollment. Baseline TCS= 19.
• At week 3 (TBZ 50 mg/d), TCS= 15.
• At week 7 (TBZ 100 mg/d), TCS= 10.
• On Day 49 had restlessness, TBZ was suspended & patient hospitalized. On D 56 he recovered from the event and re-started TBZ, 12.5 mg/day. Three weeks later, TBZ was not effective to control the chorea. He developed depression and suicidal thoughts, with symptoms of psychosis and paranoia, requiring hospitalization. Treated with mirtazapine, lorazepam and olanzapine. TBZ was d/c on Day 71. Symptoms resolved on Day 72. He was discharged on Day 79, to a nursing home facility. The event was considered by the investigator to be unrelated to TBZ.
• ID# 447-213. 62 y.o. male randomized to TBZ. No prior history of depression. No concomitant meds at the time of enrollment. Baseline TCS= 19.
• At week 3 (TBZ 50 mg/d), TCS= 15.
• At week 7 (TBZ 100 mg/d), TCS= 10.
• On Day 49 had restlessness, TBZ was suspended & patient hospitalized. On D 56 he recovered from the event and re-started TBZ, 12.5 mg/day. Three weeks later, TBZ was not effective to control the chorea. He developed depression and suicidal thoughts, with symptoms of psychosis and paranoia, requiring hospitalization. Treated with mirtazapine, lorazepam and olanzapine. TBZ was d/c on Day 71. Symptoms resolved on Day 72. He was discharged on Day 79, to a nursing home facility. The event was considered by the investigator to be unrelated to TBZ.
47
Rate of Depression Rate of Depression Patients with HDPatients with HD
Rate of Depression Rate of Depression Patients with HDPatients with HD
Study/Duration N1 PYRs2 Number of events
Rate per 100 PYRs
TBZ in Prestwick’s studies
004/ 12 wks 54 12.2 10 82.0
007/ Up to 80 wks 75 96.8 26 26.9
006/ 48 wks 29 25.5 10 35.3
No TBZ
CARE-HD3
Up to 3 years347 817.0 93 11.4
N= patients randomized. 2 Person years of exposure. CARE-HD: Non-Prestwick study with baseline characteristics similar to those in the Prestwick’s studies, with the following treatment arms: Remacemide, Co Q10, both, or placebo.
48
Rate of DysphagiaRate of Dysphagia in Patients with HD in Patients with HD
Rate of DysphagiaRate of Dysphagia in Patients with HD in Patients with HD
Study/Duration N1 PYRs2 Number of events
Rate per 100 PYRs
TBZ in Prestwick’s studies
004/ 12 wks 543 12.2 2 16.4
007/ Up to 80 wks 75 96.8 6 6.2
006/ 48 wks 29 25.5 3 11.8
No TBZ
CARE-HD4
Up to 3 years347 817.0 32 3.9
N= patients randomized. 2 Person years of exposure. 3 Placebo: 1 case, 14.3 per 100 PYRs. 4CARE-HD: Non-Prestwick study with baseline characteristics similar to those in the Prestwick’s studies, with the following treatment arms: Remacemide, Co Q10, both, or placebo.