25
Bermans J. Iskandar Pediatric Neurosurgery University of Wisconsin, Madison ASAP Austin 2010
| Date post: | 31-Dec-2015 |
| Category: |
Documents |
| Upload: | wade-fulton |
| View: | 50 times |
| Download: | 4 times |

Bermans J. Iskandar
Pediatric Neurosurgery
University of Wisconsin, Madison ASAP Austin 2010

Chiari Type I Tonsillar descent >5mm below the plane of the foramen magnum.
No associated brainstem herniation or supratentorial anomalies
Low frequency of hydrocephalus and syringomyelia
Chiari Type II Caudal descent of the vermis, brainstem, and fourth ventricle.
Associated with myelomeningocele and multiple brain anomalies
High frequency of hydrocephalus and syringohydromyelia
Standard
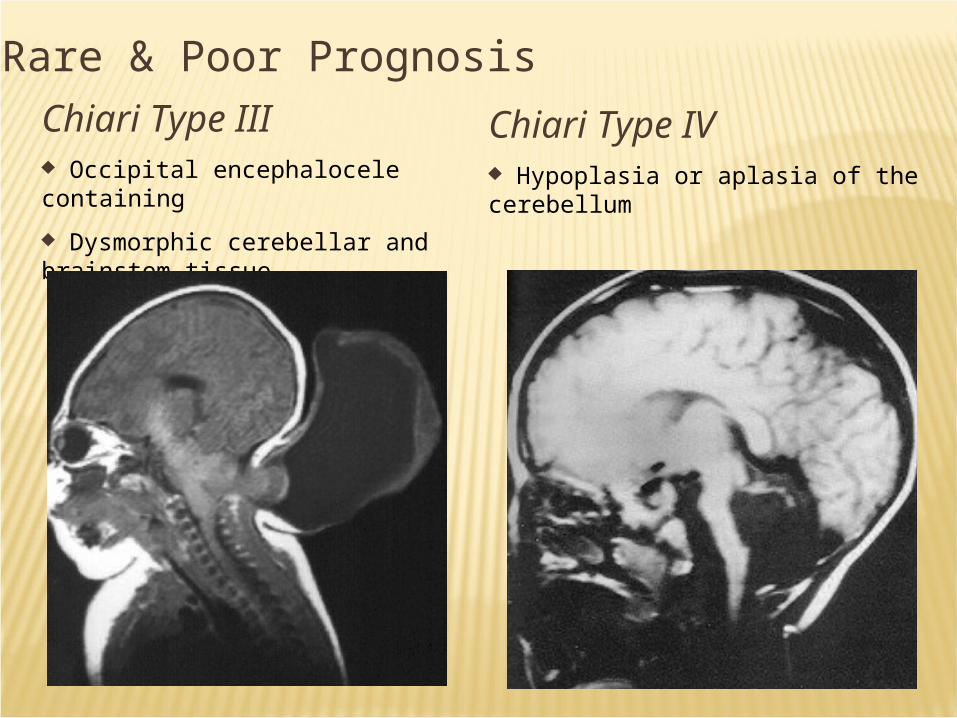
Chiari Type IV Hypoplasia or aplasia of the cerebellum
Chiari Type III Occipital encephalocele containing
Dysmorphic cerebellar and brainstem tissue
Rare & Poor Prognosis

New & Controversial
Chiari Zero Idiopathic syringomyelia that responds to craniocervical decompression
Chiari 1.5 Descent of tonsils & medulla
Behaves like Chiari I
JNS:Peds 2004 JNS 1998

Diagnosis made on MRI Treatment: posterior fossa
decompression. If the syrinx does not
resolve: Re-explore the posterior fossa
and expand the decompression
Consideration of subtle craniocervical instability
Consideration of benign intracranial hypertension
Consideration of shunting the syrinx directly

8 year old boy with headaches Syrinx 1 cm tonsillar descent

30 year-old with 1.5 cm tonsillar descent and severe symptoms
Posterior fossa decompression fails LP monitoring reveals elevated ICP VP shunt Symptoms resolve


10 year-old who underwent serial lumbar punctures for a mild viral meningitis
Develops lower cranial nerve symptoms
MRI reveals new tonsillar herniation

12 year-old with Chiari I, syringomyelia, and basilar invagination
Posterior fossa decompression
Symptoms and syrinx don’t resolve until craniocervical fusion a year later
Likely Etiology In utero CSF leak through the
myelomeningocele opening, causing caudal traction on brain structures
Clinical Presentation Infants: usually asymptomatic Children: signs of lower brainstem
compression: stridor, apnea, dysphagia, aspiration

Chiari II: leading cause of death in spina bifida patients in the recent past
30% of patients: brainstem symptoms by age 5 (1/3 of these die)
Most dangerous period: 2-3 months of age (sometimes up to 2 years)

Current understanding VP shunt malfunction most likely
cause of deterioration, rather than the Chiari
Ventricle size may not change Number of Chiari II decompressions
has decreased significantly since more aggressive shunt revisions

Fluid-filled cavity within the spinal cord
Other nomenclature
Hydromyelia Syringohydromyelia Spinal cord cyst

Dissociated sensory loss
Central cord syndrome
Brainstem symptoms and signs
Scoliosis Chronic pain

Spinal MRI will show a dilated cavity with the same intensity of CSF.
A complete brain and spinal MRI with and without Gadolinium is needed to determine the primary pathology.
Cine MRI may also help in diagnosing abnormal CSF flow patterns. So far results have been conflicting.
Rarely, myelography may help to sort some of the more difficult cases.

Asymptomatic patients with small syrinx cavity and no obvious etiology are best managed with watchful waiting and serial imaging
Large syrinx: Treat the cause of the syrinx, not the syrinx itself

The syrinx may be the result Tethered cord from the
myelomenigocele repair scar Chiari II malformation Ventricular shunt malfunction.
Location of the syrinx within
the spinal cord may help to dictate the treatment Lumbar syrinx ??tethered
cord release Cervical syrinx ?? VP shunt
revision Check the shunt first!

Diagnosis by MRI Treatment:
Tethered cord release
If syrinx is large, it is often drained at the same surgery

Diagnosis made on MRI Treatment: Dissection of the arachnoid
scar (often difficult or impossible) Goal: Reestablish normal CSF flow Difficulties: If the arachnoiditis is so
diffuse that it becomes impossible to achieve a good dissection, shunt the syrinx to the pleural or peritoneal cavities

Post-traumatic syrinx is difficult to treat successfully
Possible causes Arachnoiditis and blockage of
flow causing expansion of the cord, or
Atrophy long term after cord contusion
Treatment: arachnoidal dissection, or syrinx shunt into the pleura or peritoneum

Diagnosis made on MRI High protein content Treatment:
Tumor resection It is rare to have to
shunt the syrinx in these situations.

In a large percentage of patients, the syrinx has no identifiable cause
Difficult to treat If large, syrinx shunting Rarely, posterior fossa decompression
(Chiari zero) It is so far impossible to predict which
patient with idiopathic syringomyelia would respond to posterior fossa decompression

Chiari decompression Excellent outcome
Spina bifida Excellent outcome when shunt is functional
Arachnoiditis Focal – fair prognosis Diffuse – poor, need to shunt the syrinx
Trauma Poor outcome for syringomyelia and pain
Tumor: Excellent outcome for syringomyelia Overall Prognosis depends on tumor grade
Standard basic definitions Complicating factors: hydrocephalus,
pseudotumor cerebri, instability, etc. Treatment controversies
When to treat What to do When to do it
Goals: Recognize basic concepts; recognize controversial areas; be prepared to bring these points up with your physician

















