1 The development of a new speciality training programme in obstetrics and gynaecology in the UK Oliver Jones, MA ODE, BSc (Hons), Education Projects Manager * , Wendy Reid, FRCOG, Chair, RCOG Curriculum Committee 2007–2010 Royal College of Obstetricians and Gynaecologists, London, UK Keywords: curriculum programme GMC good medical practice workplace–based assessment learning outcomes competencies knowledge criteria clinical competency professional skills and attitudes In 2004, the Royal College of Obstetricians and Gynaecologists (RCOG) established a working group of experienced Fellows, Members, trainees and educationalists, who were responsible for writing and coordinating the development of a new curriculum in obstetrics and gynaecology. The curriculum would underpin the new 7-year speciality training programme. In December 2006, the UK Postgraduate Medical Education and Training Board approved the curriculum. In August 2007, the new Speciality Training and Education programme in Obstetrics and Gynaecology was launched. The curriculum forms the backbone of the 7-year speciality training programme in obstetrics and gynaecology. The pro- gramme is divided into three levels of training: basic, intermediate and advanced. The programme is competency-based rather than being focussed on time periods or the number of hours or number of procedures required to progress through the programme. Successful progress is achieved by meeting the requirements at designated waypoints defined within the programme. The curriculum outlines not only the knowledge and technical clinical skill requirements, but also the professional skills and attitudes that must consistently be adopted by health-care professionals in a modern health service. The curriculum was originally benchmarked against the General Medical Council’s Good Medical Practice criteria: (1) Good clinical care; (2) Good medical practice; (3) Successful relationships with patients; * Corresponding author. E-mail address: [email protected](O. Jones). Contents lists available at ScienceDirect Best Practice & Research Clinical Obstetrics and Gynaecology journal homepage: www.elsevier.com/locate/bpobgyn 1521-6934/$ – see front matter Ó 2010 Elsevier Ltd. All rights reserved. doi:10.1016/j.bpobgyn.2010.06.001 Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701
Transcript
Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701
Contents lists available at ScienceDirect
Best Practice & Research ClinicalObstetrics and Gynaecology
The development of a new speciality training programme inobstetrics and gynaecology in the UK
Oliver Jones, MA ODE, BSc (Hons), Education Projects Manager *,Wendy Reid, FRCOG, Chair, RCOG Curriculum Committee 2007–2010Royal College of Obstetricians and Gynaecologists, London, UK
Keywords:curriculumprogrammeGMCgood medical practiceworkplace–based assessmentlearning outcomescompetenciesknowledge criteriaclinical competencyprofessional skills and attitudes
1521-6934/$ – see front matter � 2010 Elsevier Ltdoi:10.1016/j.bpobgyn.2010.06.001
In 2004, the Royal College of Obstetricians and Gynaecologists(RCOG) established a working group of experienced Fellows,Members, trainees and educationalists, who were responsible forwriting and coordinating the development of a new curriculum inobstetrics and gynaecology. The curriculum would underpin thenew 7-year speciality training programme. In December 2006, theUK Postgraduate Medical Education and Training Board approvedthe curriculum. In August 2007, the new Speciality Training andEducation programme in Obstetrics and Gynaecology waslaunched.The curriculum forms the backbone of the 7-year specialitytraining programme in obstetrics and gynaecology. The pro-gramme is divided into three levels of training: basic, intermediateand advanced. The programme is competency-based rather thanbeing focussed on time periods or the number of hours or numberof procedures required to progress through the programme.Successful progress is achieved by meeting the requirements atdesignated waypoints defined within the programme.The curriculum outlines not only the knowledge and technicalclinical skill requirements, but also the professional skills andattitudes that must consistently be adopted by health-careprofessionals in a modern health service. The curriculum wasoriginally benchmarked against the General Medical Council’sGood Medical Practice criteria:
(1) Good clinical care;(2) Good medical practice;(3) Successful relationships with patients;
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701686
(4) Working with colleagues;(5) Teaching and training;(6) Probity;(7) Health.
� 2010 Elsevier Ltd. All rights reserved.
The concept of a curriculum
A curriculum is a constantly ever-evolving reference, which informs users of defined criteriarequired to meet an overall outcome. In the case of the obstetrics and gynaecology curriculum, thereference aims to produce an individual competent to perform independently to the required standardof a consultant obstetrician and gynaecologist. There are many factors, which determine whethera curriculum is fit for purpose, but an agreed definition of the end point is crucial and is the greatestchallenge in an ever-evolving health service. In 2005, the Royal College of Obstetricians and Gynae-cologists (RCOG) commissioned a working party to establish the future service requirements of theconsultant in obstetrics and gynaecology.2 In parallel, the new curriculum was developed with anaspiration to produce the future consultants that the UK National Health Service (NHS) requires. Theparticular challenge of higher training was recognised and the RCOG commissioned aworking party toaddress this phase of training.3
The journey through a training programme needs to be standardised, yet be flexible. In an evalu-ation of different types of curricula known in the educational literature, the Postgraduate MedicalEducation and Training Board (PMETB) highlighted the following descriptions.4
A paper-based version of a curriculumA statement of purpose that includes the aims, content experiences and materials. This is also
known as a ‘planned’ or ‘formal’ curriculum.
A curriculum in actionA curriculum on paper is actually put into real-life practice. This is known as the ‘received’
curriculum.
A curriculum-user’s experienceAn outline of what curriculum users do, how they learn and practise in real life and what they
interpret to be important for new progress. This is the ‘informal’ curriculum.
A hidden curriculumAn outline of the behaviours, knowledge and performances that learners infer to be important from
the formal curriculum: an ‘informal’, ‘unplanned’ and ‘perceived curriculum’.
Interpretation of a curriculum
For the obstetrics and gynaecology curriculum, trainees and trainers will construct their owninterpretation of how to deliver a curriculum based on their own experiences. To this end, based ontheir own requirements, previous experiences and the way they know that opportunities and mile-stones will be presented throughout a training programme in a particular unit, a programme will becrafted for trainees. All adult learners attain competencies differently and at different rates; hence,although a curriculum is a standardised guide, if all of these factors are taken into consideration,PMETB’s 2006 definition of a curriculum is functional:
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701 687
“A statement of the intended aims and objectives, content, experiences, outcomes and processes of aneducational programme including:� A description of the training structure (entry requirements, length and organisation of the
programme including its flexibilities and assessment system)� A description of expected methods of learning, teaching, feedback and supervision”.5
A curriculum enables future trainees to observe the scope of the profession before application togeneralist roles of subspecialist roles. In addition, it develops a professional model that is reflexive,collective, developmental and process-orientated such that it can be followed and referred to bytrainees and consultants wishing to continue their professional development. The curriculum also actsas a guide to high-level requirements, which enables the public to see the expertise acquired bypractitioners and the level of care that they can expect from the profession.
The introduction of PMETB and MMC
National changes in postgraduate medical education, with the advent of the PMETB5 and theevolution of NHS Modernising Medical Careers (MMC),6 were addressed by the RCOG througha number of working parties formed in 2005, and also influenced by the study of a working partytasked with evaluating the core logbook in 2002.7
The MMC principles state that speciality training curricula should underpin a programme, which iscarefully designed to deliver nationally agreed standards. All speciality curricula should be defined bythe domains of General Medical Council (GMC) Good Medical Practice and the management of thecontent and delivery of the curriculum.1 The curriculummanagement and ongoing development of thecurriculum is audited annually by the PMETB. The process is managed by ensuring that the PMETBStandards for Curricula and Assessment8 are adhered to and the appropriate evidence is collected forreview.
In the modern obstetrics and gynaecology programme, educational progression is assessed by anannual review of the documented acquisition of competencies in the curriculum, for both clinical andprofessional competencies. Competencies are benchmarked and referenced against average time scaleswithin a programme to measure satisfactory progress at designated waypoints.
The RCOG convened two working parties in 2004, the Basic and Advanced Specialist TrainingWorking Parties.3,9 The working parties were responsible for reviewing and evaluating the existingcore logbook and special skills modules and for planning and conducting the development of the newcurriculum, in keeping with NHS MCC principles.
The curriculum structure and proposed content were agreed upon by the Basic and Advancedworking parties, the Specialist Training Committee, the Education Board and, finally, by the Council ofthe RCOG in 2006.10 The curriculum was implemented in August 2007, following approval by thePMETB.
Following the introduction of the new speciality training and education curricula, the TookeReport11 questioned the concept and function of MMC and the structure of medical education. Becauseof the enquiry, the creation of a new body, NHS Medical Education England (NHS: MEE), was proposed.NHS: MEE would relate to the revised medical workforce advisory machinery and act as the profes-sional interface between policy development and implementation on matters relating to postgraduatemedical education and training.
From a logbook to a curriculum
Review of the core logbook, 2002
The curriculum in obstetrics and gynaecology evolved from the output of the obstetrics andgynaecology Core Logbook Working Party,7 which produced the first logbook of competencies witha rating against competency levels enabling trainees to demonstrate progress.
The working party identified that postgraduate training needed a reference document, whichwould provide all trainees with a broad understanding of what the competencies in obstetrics and
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701688
gynaecology were and which would assure that trainees and their core training competencies could beacquired flexibly. To allow every trainee to have opportunities to access comprehensive training for theacquisition of all skills required and to achieve a level of competency whereby they become equippedfor independent professional practice, it was identified that the logbook would evolve from a syllabusinto a curriculum.12 The aim was to integrate the knowledge criteria and to specify the practical skillsand attitudes required for professional practice. In addition, it was recognised that systems forassessing these competencies would be required in line with the standards arising from the PMETB.8
The ultimate aimwas to ensure that trainees would become equipped for independent professionalpractice following completion of all logbook requirements, and the way progress would be measuredwould be to create a system to rate the development and the increasing professional responsibility ofthe trainee. The syllabi for the Part 1 and Part 2 MRCOG examinations were reviewed and clearlydefined the core knowledge required for specialist training, and the logbook would providea comprehensive andmandatory list of the skills to be acquired during core training across the iterative7-year programme. All skill requirements were reviewed, definitions were updated and advice wasprovided for trainers assessing the trainees for each module. Skills, that needed to be evaluatedrepeatedly throughout the programme, were also identified.
A five-point scale was deemed to be fit for purpose to demonstrate progress, as was the modularorganisation of relevant clinical skills. It was agreed that certain skills would be best acquired at formaltraining days or sessions and these were highlighted as compulsory requirements of relevant mod-ules. All of the skill targets in the core logbook were to be compulsory and trainees would need to berated at level 5 in order to achieve the Certificate of Completion of Specialist Training (CCST) at the endof the training programme.
Level description explanation
1. Observer: Observes the procedure performed by a colleague2. Assistant: Assists a colleague in performing the procedure3. Directly supervised: Performs the entire procedure under direct senior supervision4. Indirectly supervised: Performs the entire procedure with indirect senior supervision5. Independent: Performs the entire activity without the need for supervision
A review of training
Basic and advanced specialist training working parties, 2004–07
All members of the two working parties and the coordinated writing groups were clinical andeducational supervisors and included trainee representation. All members of working parties wereguided and supported by the Education Development Officer. The Education Development Officer’srole (as a non-clinical educationalist) was to provide educational expertise and to coordinate thegroups to develop a realistic, deliverable structure in the clinical setting. The expertise from trainersand senior trainees who were aware of current opportunities and developments in practice (includingtime constraints) was paramount, in addition to implementing conclusions drawn by the work of ‘TheFuture Role of the Consultant’ Working Group.2
The Basic and Advanced Specialist Training Working Parties designed the new curriculum to buildon the skill requirements in the logbook but to more comprehensively address required levels ofprofessionalism, attitudes and different types of competencies by introducing a series of workplace-based assessments. It was important that the curriculum would be less of a checklist and list ofrequirements, and more of an interface between trainees and trainers to inculcate clinical competency,professional skills, attitudes and reflective learning. The potential for workplace-based assessment wasto be fed throughout the entire curriculum to coordinate uniform, structured learning sessions and
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701 689
encourage a culture of documenting the acquisition of competencies for clinical, educational andprofessional competencies, as required by the MMC.
The acquisition of knowledge and skill and the consistent maintenance of performance would beachieved by the incremental acquisition of competencies. The level at which skills should normally beacquired is included in the relevant module (and sub-modules) of the curriculum. This model is basedon Miller’s triangle of learning, which runs from “knows”, to “knows how”, to “shows how” and “does”(Fig. 1). Different levels of skills are required by the end of different stages in training. The waypointsare those needed by the end of the first 2 years of training (the end of basic training), those required tobe completed before the start of advanced training (by the end of intermediate training) and thoseskills needed by the completion of training for the award of the certification of completion of training(CCT) following 2 years of advanced training.
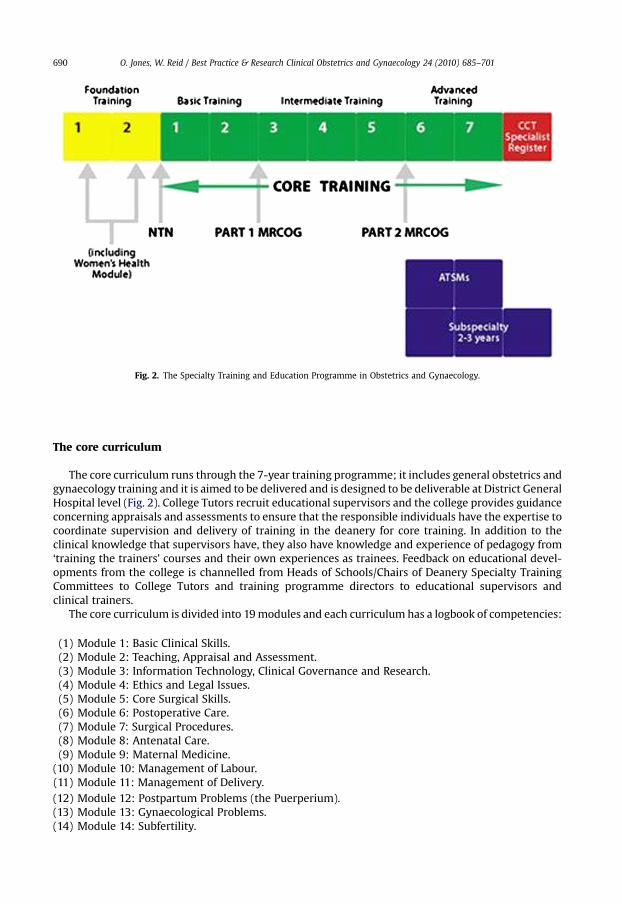
Fig. 2. The Specialty Training and Education Programme in Obstetrics and Gynaecology.
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701690
The core curriculum
The core curriculum runs through the 7-year training programme; it includes general obstetrics andgynaecology training and it is aimed to be delivered and is designed to be deliverable at District GeneralHospital level (Fig. 2). College Tutors recruit educational supervisors and the college provides guidanceconcerning appraisals and assessments to ensure that the responsible individuals have the expertise tocoordinate supervision and delivery of training in the deanery for core training. In addition to theclinical knowledge that supervisors have, they also have knowledge and experience of pedagogy from‘training the trainers’ courses and their own experiences as trainees. Feedback on educational devel-opments from the college is channelled from Heads of Schools/Chairs of Deanery Specialty TrainingCommittees to College Tutors and training programme directors to educational supervisors andclinical trainers.
The core curriculum is divided into 19modules and each curriculum has a logbook of competencies:
(10) Module 10: Management of Labour.(11) Module 11: Management of Delivery.(12) Module 12: Postpartum Problems (the Puerperium).(13) Module 13: Gynaecological Problems.(14) Module 14: Subfertility.
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701 691
(15) Module 15: Women’s Sexual and Reproductive Health.(16) Module 16: Early Pregnancy Care.(17) Module 17: Gynaecological Oncology.(18) Module 18: Urogynaecology and Pelvic Floor Problems.(19) Module 19: Professional Development.
These modules were selected as representing the core subjects required in the preparation of alltrainees for the profession of obstetrics and gynaecology.
To progress through a curriculum module, competencies are gained by the trainees first observing,then performing under supervision and repeating until competent to perform independently.
Eachmodule follows the pattern of curricula developed for the core curriculum, based on the GMC’sGood Medical Practice guidelines.13 The aims and objectives of each module are defined and theexpected skills and expertise will be assessed and documented as evidence for the annual review ofcompetence progression (ARCP).
The sequencing is established by working through the modules, starting from the most basic andprogressing to the most complex; however, significant clinical requirements are reiterated in severalmodules for reinforcement. Within modules, the logbook is structured to indicate the degree ofcompetency expected (e.g., from initial observation, to performing procedures under supervision toindependent practice). The logbook colour codes competences so that trainees/trainers can clearly seethe expected progression for each skill through the entire programme. Three colours are used torepresent competences, which are to be achieved by the end of basic, intermediate or advancedtraining. Competencies may be acquired before the set level (see Fig. 3).
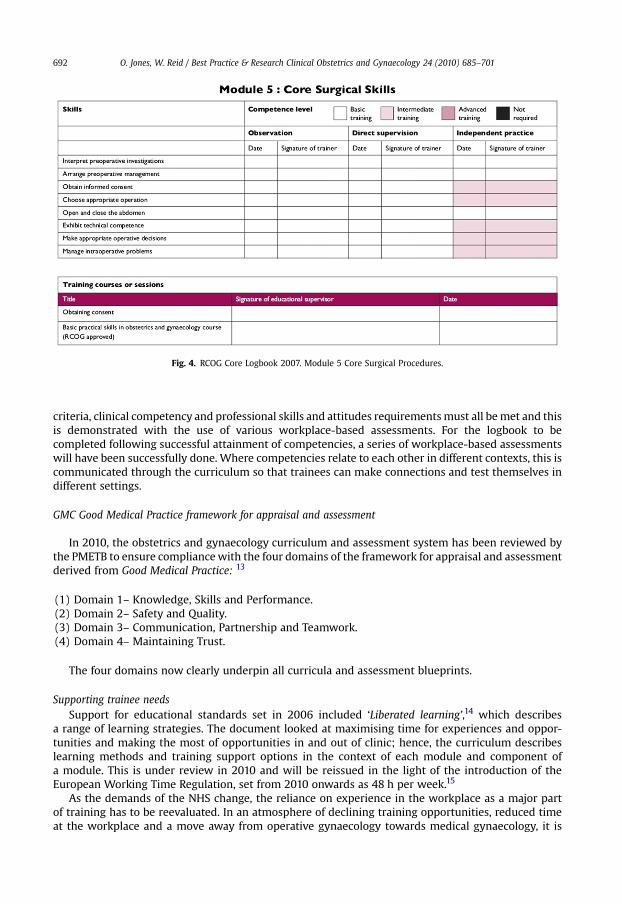
The knowledge, skills and attitudes are presented throughout the curriculum, but presented incontext, in the relevant module and alongside the relevant learning outcome, in the context of therelevant clinical situation (see Figs. 4, 5).
The curriculum as an interface
The curriculum blends theoretical and practical learning and workplace-based assessment optionsthroughout. It ensures that trainees understand practice, follow recommended processes to gainconfidence, gain competence and then be assessed. The trainees’ knowledge, skills, competency andprofessional skills and attitudes are tested in every context throughout the curriculum in the relevantcontext. Each curriculum module has a logbook but, unlike the 2002 core logbook, the knowledge
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701692
criteria, clinical competency and professional skills and attitudes requirementsmust all bemet and thisis demonstrated with the use of various workplace-based assessments. For the logbook to becompleted following successful attainment of competencies, a series of workplace-based assessmentswill have been successfully done. Where competencies relate to each other in different contexts, this iscommunicated through the curriculum so that trainees can make connections and test themselves indifferent settings.
GMC Good Medical Practice framework for appraisal and assessment
In 2010, the obstetrics and gynaecology curriculum and assessment system has been reviewed bythe PMETB to ensure compliancewith the four domains of the framework for appraisal and assessmentderived from Good Medical Practice: 13
(1) Domain 1– Knowledge, Skills and Performance.(2) Domain 2– Safety and Quality.(3) Domain 3– Communication, Partnership and Teamwork.(4) Domain 4– Maintaining Trust.
The four domains now clearly underpin all curricula and assessment blueprints.
Supporting trainee needsSupport for educational standards set in 2006 included ‘Liberated learning’,14 which describes
a range of learning strategies. The document looked at maximising time for experiences and oppor-tunities and making the most of opportunities in and out of clinic; hence, the curriculum describeslearning methods and training support options in the context of each module and component ofa module. This is under review in 2010 and will be reissued in the light of the introduction of theEuropean Working Time Regulation, set from 2010 onwards as 48 h per week.15
As the demands of the NHS change, the reliance on experience in the workplace as a major partof training has to be reevaluated. In an atmosphere of declining training opportunities, reduced timeat the workplace and a move away from operative gynaecology towards medical gynaecology, it is
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701 693
essential that training time becomes more focussed. Both the quality of training opportunities andthe use of these opportunities need to be maximised. By defining the knowledge, skills and atti-tudes required in detail within the context of learning, the trainer and trainee will have a greaterunderstanding of the continuing needs of the trainee. The Conference of Postgraduate MedicalEducation Deans (COPMeD) document ‘Liberated Learning’ describes the wide range of learningstrategies that can be used to help trainers maximise the time and opportunities available. Work-based experiential learning may be found in almost every clinical encounter. It may be in theconsulting room, at the bedside, in a clinic or in the operating theatre. It may be lengthy or brief,and take in many domains of medicine. Learners should learn actively, rather than be treated as‘passive’ trainees. A strong interface between trainee and trainer to inculcate reflective practice isimportant.
Learning can be:(1) Patient based: This includes activities such as ward rounds, topic-based bedside teaching,
outpatient clinics, special units (e.g., endoscopy) and theatre sessions.(2) Classroom based: This encompasses activities such as formal teaching sessions, clinical meetings,
journal club and theory and practical training courses.(3) Self-directed learning: Learning can take place in obstetrics and gynaecology through activities
such as reading books and journals, reflective analysis and open-, distance- and e-learning. TheRCOG has produced an e-learning programme called StratOG.net, which supports the curriculumand is referenced throughout in the relevant context. The resource includes theory, case-basedlearning, self-assessment and reflective learning so that trainees can continually learn and test theknowledge criteria of the curriculum.
(4) ‘Off-the-job’ education: Apart from the self-directed learning materials stated above, every traineehas the opportunity of study leave in which to undertake reflective learning or to take up relevantcourses either locally or at the RCOG. Work on topics such as audit and keeping a diary/portfolio ofactivities are required as part of the learning process.
The programme accepts that individual trainees have different learning styles, will learn at differentrates and will favour some learning activities over others; hence, the curriculum makes recommen-dations; however, every curriculum has a ‘hidden’ element to allow the trainee and their trainer decideto follow the curriculum in their own context.
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701694
Portfolio-based learning
From undergraduate study onwards, trainees will be responsible for maintaining a portfolio, whichrecords and presents the evidence required to demonstrate that the curriculum requirements havebeen met at all levels.
Specifically, in terms of all the standards for Curricular and assessment systems,8 a trainee’s portfolio/e-portfolio will:
� Record progression by including records of regular workplace-based assessments;� Provide evidence of appraisal and feedback on performance in posts;� Provide evidence of induction and elements of educational supervision (learning agreements,logbook and portfolio) and progress meetings;
� Provide evidence of career discussions;� Provide evidence of participation in audit;� Provide evidence of attendance at educational meetings and activities;� Contribute to meeting the standards of the curriculum (the logbook competences);� Provide evidence of autonomous and reflective thinking;� Record evidence of learning experiences and reflection of their value in achieving curricularoutcomes;
� Record evidence of assessment and progress in assessment (examination achievements);� Record evidence of feedback on learning and assessment; and� Provide uniform documentation on trainees’ progress.
Workplace-based assessment, examinations and the ARCP process
All of the workplace-based assessments in obstetrics and gynaecology are formative and traineesshould retain all of their previous workplace-based assessments in their portfolio so that educationalsupervisors can evaluate their training experiences and their progression. This applies to the MiniClinical Evaluation Exercise (Mini-CEX), Case-based discussions (CbD) and Objective StructuredAssessments of Technical Skills (OSATS). To introduce such a change in evolving training and educationto be competency-based rather than time- and ‘number-based’ has been challenging and the intro-duction of competency-based learning and transparency in workplace-based assessment has, and willcontinue, to drive a cultural change in training.
The RCOG has developed best practice in workplace-based assessment videos, which have beenintroduced to show the effectiveness of workplace-based assessment and how trainees and trainersshould maximise workplace-based assessments as structured learning episodes rather than as formalassessments. The scenarios have been written by trainees based on the positive and negative experi-ences that they have had. Of course, a significant degree of judgement is involved in workplace-basedassessment, and with judgement comes disagreement.
In the 2009 PMETB trainees survey,16 around two-thirds of trainees reported that they had beensubjected to undermining behaviour at some point in their training, and the risk with workplace-basedassessment and multi-source feedback is that judgements are so transparent that effective commu-nication should be delivered by experienced trainers, if the chances of disagreement are to be mini-mised. The challenge to train trainers in obstetrics and gynaecology is vast because training is deliveredby individuals other than obstetricians and gynaecologists; hence, the RCOG has developed a series ofvideos demonstrating how best to provide effective feedback and to highlight what could be consid-ered to be undermining behaviour in the workplace. The videos are freely available on the RCOGwebsite, and again, the feedback and concern expressed by trainees has been used constructively toscript and produce this informative and enlightening series of video-based scenarios.
At all stages, clinical and educational supervisorswill be expected to follow trainee progress throughworkplace-based assessment documentation,which cannowbemonitoredonline remotely, at any timeusing ePortfolio systems. All workplace-based assessments include assessment criteria and points foractions and personal development planning. Case-based discussions assess knowledge and provide anopportunity to advise trainees on learning options, which they will need to coordinate independently,
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701 695
but which can be followed up in a structured way. The onus for learning is on the trainee, but expertadvice and guidance is provided by the trainer. Effective management of trainees is also essential toensure trainees know the limit of their competency, which is fundamental to ensure patient safety.
Professional skills and attitudes are presented throughout the entire curriculum in the context of thesubject of curriculummodules. A trainee’s performance andprofessional conduct ismeasuredbyclinicalsupervisors not only in all non-technical workplace-based assessments, but also as part of the multi-source feedback process. Along with multi-source feedback, appraisals and workplace-based assess-ments, successful completion of the logbook requirements inform the summative process: the ARCP.
Workplace-based assessment continues to challenge the RCOG and it still remains to be seenwhether it can assess all areas of competency and performance, or more importantly, whether it canallow early identification of trainees in difficulty, which was previously not possible using alternativeassessment methods. A challenge for the RCOG in 2009 related to trainees’ overall competency,compared with their competency when working at night in a very different atmosphere with supportin terms of colleagues and resources in a hospital. This remains a challenge and the development ofassessment criteria to measure a trainee’s response and leadership skills at night rather than duringnormal working hours remains a challenge for the RCOG Curriculum and Assessment committees.
1. The Part 1 MRCOG Examination is placed at the end of basic training, ST2, before entry intointermediate training, as it is felt that aspiring clinicians should have a firm knowledge base ofbasic and clinical sciences upon which to build their clinical experience and practice. The Part 2MRCOG Examination is placed at the end of intermediate training (ST5), before entry into advancedtraining, as it is felt to be the correct point for the last major examination testing broad obstetricand gynaecological clinical knowledge, skill and competency before CCT status is achieved.Trainees have flexibility as to when they attempt their postgraduate examinations but the guid-ance is designed to enhance their likelihood of success.
2. The combination of satisfactory ARCP and examinations at relevant waypoints constitutes thesummative assessments, which must be completely satisfied to progress through the trainingprogramme.
Reflective learning
It is vital that trainees reflect upon cases; the case-based discussion forms the basis for this in a one-to-one formative workplace-based assessment with a clinical or educational supervisor. However, it isthe trainees’ responsibility to reflect on their experiences and ensure that they progress with anongoing personal development plan by following the constructive feedback from workplace-basedassessments. Trainees must manage a reflective diary of their clinical and theoretical experiences. Arequirement of the ARCP is to provide evidence of regular reflective learning through writing. Therequirement for reflective learning is underpinned throughout the ‘Evidence/Assessment’ column ofthe whole curriculum, especially where it is considered to be particularly important.
When trainees do not have an opportunity to observe rare clinical presentations and to developtheir competencies, it would not be beneficial to remove these rare occurrences from the curriculumand logbook. Trainees and trainers are aware that in such circumstances, trainees need not be seen toobserve or do the relevant procedure to be successfully assessed and to progress through training.Instead, alternative training methods should be used (drills, simulation and e-learning) and case-baseddiscussion assessments should be completed until all requirements of the assessment are met, in linewith Miller’s triangle in “knowing” and “knowing how”, even if an opportunity of “showing” and“showing how” is not possible in vivo (Fig. 3).
Advanced training
Advanced training has been designed to prepare senior trainees in obstetrics and gynaecology forthe diversity in clinical practice that future consultants will be expected to provide. Advanced trainingtakes place in years 6 and 7, after approximately 5 years of basic and intermediate training. AdvancedTraining Skills Modules (ATSMs) cover all areas of current and future practice and have been designed
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701696
by specialist societies and, although trainees in years 6 and 7 will continue with core training, alltrainees, excepting the minority who will undertake subspeciality training, will undertake at least twoATSMs that will enhance their service capability in the relevant areas of their choice, and as needed bythe service.
The Future Role of the Consultant2 recognised, for example, the reduction in traditional surgicalgynaecology and expanded roles within medical, outpatient-based gynaecology, for example, usingminimal access surgery. With this in mind, the curriculum has evolved to enable the ‘generalist’obstetrician and gynaecologist to have a concrete basis of both the obstetrics and the gynaecologyrequired for safe emergency-care provision. The emphasis driving advanced training is for the ATSMsto provide sufficient experience in specific areas so that trainees are skilled at a level required forconsultant practice.
As previously noted, a curriculum enables future trainees to view the scope of the professionbefore application and, in addition, a curriculum acts as a source for career planning and asa component of the ARCP process for planning training needs. Trainees recognise that collectinga wide range of unrelated training experiences is not realistic and will not enhance their employ-ability. Trainees and their supervisors need to look at how ATSMs should be grouped together toproduce a coherent training strategy and to prepare them for particular job roles at consultant level.Components of ATSMs are also currently being grouped to produce ATSM ‘packages’ which include,for example, surgery modules with the gynaecological oncology module. This ensures that wheretraining opportunities are competitive, trainees are not disadvantaged by having to register for andcomplete entire secondary ATSMs when only a small component complements the requirements oftheir primary ATSM choice.
Each ATSM follows the same format as the core curriculum, based on the GMC’s Good MedicalPractice13 guidelines. The aims and objectives of each module are defined as are the expected skills andexpertise to be assessed and documented as evidence for ARCP, in addition to meeting the require-ments of the core curriculum.
The ATSM logbook does not include colour codes as the average time for completion of an ATSM is 1year, although trainees typically follow two ATSMs simultaneously for the 2-year duration of advancedtraining.
Subspeciality training
Subspeciality training programmes are undertaken by a small number of trainees and therecruitment is coordinated so that they will undertake the subspeciality training programme at anapproved centre.
Subspeciality trainees are required to complete all basic and intermediate core curriculum modulerequirements. At the end of ST5, entry to an approved subspeciality programme is competitive andmaybe to either a 2- or 3-year programme, depending on research requirements. Subspeciality trainees arerequired to complete all subspeciality training curriculum and logbook requirements (includingachieving the generic competencies common to each subspeciality) to achieve a CCT in the relevantsubspeciality:
� Maternal and Foetal Medicine.� Reproductive Medicine.� Urogynaecology.� Gynaecological Oncology.� Sexual and Reproductive Health.
The Subspeciality Training Programme Supervisor (STPS) will coordinate the subspeciality trainingprogramme and will be the clinician responsible for its supervision. This includes ensuring allcomponents of the curriculum are included in the programme and that the trainee’s portfolio isaccurate and up to date. The logbook will be informed by supporting evidence from workplace-basedassessments. The subspeciality trainee’s supervisor will be responsible for coordinating four appraisalsper training year, in the same way as this is coordinated for core training.
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701 697
Once registered as a subspeciality trainee, the RCOG Advanced Training Coordinator will arrangethe midterm and final review for the subspeciality trainee, as appropriate. A typical review meetingwill review the trainee’s portfolio including logbooks, appraisals, workplace-based assessments andmulti-source feedback. The panel in attendance at a review will include the trainee, supervisor,STPS and a STPS or supervisor in the subspeciality from another Deanery. Efforts are made toensure that the same panel will be in attendance for the midterm and final review for a particulartrainee.
The STPS, in collaboration with the RCOG College Tutor and Deanery STC/Head of School,will be responsible for ensuring the subspeciality trainee has an annual ARCP (includingappropriate team observations), and the results of this are available to the assessors undertakingmid-term and final reviews. The STPS is also responsible for ensuring the Chair of theDeanery STC/Head of School is aware of any concerns identified by assessors at the midterm andfinal review.
Implementation management and evaluation
The curriculum is continually being revised and can only be as viewed as an incomplete project;hence, the Curriculum Committee was established in 2007 under the chair of Professor Wendy Reid,FRCOG. The committee was commissioned to manage the in-process evaluation of the curriculum toensure its ongoing fitness for purpose. The terms of reference of the Curriculum Committee are asbelow. The Curriculum Committee:
� Is responsible for the regular, systematic review of all the modules of the core, advanced, sub-speciality and academic curricula. The group will decide the structure for these reviews. This willbe part of a continuous feedback mechanism from trainers, trainees, patients and otherstakeholders.
� Commissions further curricular elements such as ATSMs, as requested by the Specialty EducationAdvisory Committee or Education Board. The committee may not have the relevant expertise, butleads and supports the individuals providing the professional input; for example, specialistsocieties.
� Provides evidence of review and quality control required by the PMETB annually. The committeeworks to review the standards defined by the PMETB and to ensure ongoing compliance.
� Ensures that all elements of the curriculum are coherent with particular emphasis on therelationship between the core, intermediate, advanced, ATSMs and subspecialty trainingrequirements.
� Responds to requests for elements of the curriculum to be changed in accordance with changes inpractice and changes to guidelines that reflect modern developments in the UK.
� Works with the RCOG Assessment Sub-Committee to ensure competencies in the curriculum areassessed by valid, reliable and deliverable assessment tools.
The Specialty Education Advisory Committee (SEAC) is responsible for the content, structure anddelivery of the Specialty Training and Education Programme and advises on the eligibility of doctors forthe award of the CCT. Remit of the SEAC:
� To receive recommendations from the Curriculum Committee concerning revisions to theSpecialty Training and Education Programme;
� To roll out curriculum revisions to the trainees ensuring appropriate mechanisms are in place fortransitional arrangements;
� To work closely with the Chairs of the Deanery Specialty Training Committees and Heads ofSchools concerning issues relating to the new Specialty Training and Education Programme and tomonitor the effectiveness of the programme;
� To ensure quality management of the training programme;� To liaise with the Trainees’ Committee concerning feedback from the Trainee Evaluation Form.
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701698
The College hold and annual College Tutors’ meeting and Senior Staff Conference and interactiveworking group sessions, attended by tutors who deliver the curriculum in units of varying sizesthroughout the UK.
The College website is maintained throughout the year to inform training providers of develop-ments in the curriculum. Curriculum and training support is offered by the Education Projects Manageror the Postgraduate Training Department at any time to individuals or units, as required. The Collegeaims to maintain a close relationship with trainees and trainers and communication regularly reachesthe Curriculum Committee through [email protected]. Queries from trainees and supervisors arediscussed at the College Curriculum Committee, which meets thrice a year.
There is an aspiration to have a curriculum delivery lead for each deanery, which, although not yetformalised, is established through web-based communication. For advanced trainees during years 6and 7, each deanery has a Director of ATSMs and a Preceptor for each ATSM. The College also coor-dinates a ‘Directors of ATSMs’ forum to address issues specific to ATSMs, including content, deliveryand workforce requirements. The post of the ATSM Officer at the College has been the lead contactsince 2007 for trainees, ATSM directors and specialist societies to ensure that content and deliverabilityissues are progressed and resolved for these relatively new modules.
Lay-person involvement
Responding tonational policychanges is key to improvinga service, but theCollege alsohas aproactiveConsumers’ Forum of non-clinicians, who contribute to the activities of all committees, not least theCurriculum Committee and training-related committees. The Consumers’ Forum aims to support andprovide a resource for the RCOG to deliver a professional service that meets the needs and aspirations ofwomen as well as to support effective communication between professionals and the public.
The Consumers’ Forum ensures consumer perspectives inform and influence practice throughcontributing to:
� RCOG reports;� RCOG research;� RCOG assessment;� RCOG guidelines;� Responses to consultation papers;� RCOG curriculum development and training and assessment;� RCOG meetings;� RCOG links with other bodies;� RCOG working parties/study groups;� RCOG committees and boards;� Information for the public;� Standards: quality, management and audit; and� Training: minimum competencies; and accreditation.
Lay role players award a limited number of marks in Part 2 MRCOG Oral Assessment. In addition,although not yet a component of the Specialty Training and Education Programme, patientinvolvement in multi-source feedback is conducted in some obstetrics and gynaecology settings andthe Assessment Sub-Committee is currently conducting research into the validity of questionnaires.
An external psychometrician/educational consultant is also consulted for each College examinationdiet on standard setting and error measurement. College educationalists have expertise in medicaleducation concepts, PMETB and GMC requirements.
Responding to service issuesRegistration for ATSMs may be regulated to ensure controlled entry to areas where fewer numbers
of doctors are required. Several ATSMs are undertaken by very few trainees; hence, the recruitment iscoordinated as a national process, for example, advanced laparoscopic surgery for the excision of
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701 699
benign disease. Certain ATSMs may only be delivered in specific units; hence, trainees may need toarrange out-of-programme training to gain specialist skills in ATSMs such as paediatric and adolescentgynaecology and vulval disease. This fulfils the aspiration of the Advanced TrainingWorking Party thatATSMs would inform future workforce planning and vice versa.
To drive excellence and to take remedial action where the service is failing to produce suitablyskilled obstetricians and gynaecologists, the curriculum has been realigned on occasion. Whereultrasound training was becoming difficult to access, the College introduced core ultrasoundtraining to support the need for a uniform standard of ultrasound training of all trainees. Whereaccess to sexual and reproductive health-care experience has been difficult and completing theDiploma of Sexual and Reproductive health-care has been optional, the Curriculum Committee hassupported the launch of a more easily accessible online Diploma in Sexual and Reproductive health-care, coordinated by the Faculty of Sexual and Reproductive health-care. The curriculum compe-tencies in this important area must remain, yet the mode by which experiences and competenciesare achieved may not always be possible in clinical practice for all trainees. However, a significantcomponent of the diploma can be achieved to an equivalent standard using e-learning ande-assessment tools.
The College has developed a ‘basic practical skills’ package, which is a standard, franchised packagerun by the College throughout the UK. The College aims to embed practical skills and simulatedtraining into the curriculum further not only to ensure patient safety, but also to structure trainingand ensure more protected, controlled training opportunities for trainees. Trainees must first observeprocedures, then perform skills under supervision until such time as they are competent to performthem independently. If they can practise procedures and techniques, trainees are more likely torespond positively to their training experience and the quality of obstetricians and gynaecologists willimprove.
In 2010, in response to the Chief Medical Officer’s Report,17 the College appointed a Director ofSimulation and Simulation Advisory Board to conduct a scoping exercise to ascertain themost effectiveway to further integrate practical skills courses and simulation into the curriculum. The inclusion ofpractical skills, and then the development of courses to include leadership skills and the competency tomanage human factors in a challenging, yet controlled environment, will be a challenge for allspecialties, and the College is learning from industries such as the aviation industry.
Curriculum developments
Medical leadership competency framework
In 2009, the College coordinated a working group meeting to address the integration of the NHSInstitute for Innovation and Improvement Medical Leadership Framework. The inclusion of thesecompetences (for every speciality) aims to ensure that trainees in all specialities further develop thegeneric and leadership competencies achieved at Foundation level. The competencies will be inte-grated throughout the 19 core modules, and the current core module 19: ‘Professional development’will be added to significantly and be renamed ‘Developing professionalism’. This project aims todevelop practitioners’ medical leadership competencies and to help create organisational cultureswhere practitioners are more engaged in management and leadership of health to improve services forpatients across the UK.18
Generic competency framework
The College is kept informed of projects coordinated by the AcademyofMedical Royal Colleges and istypically offered the opportunity to provide feedback on drafts of competency frameworks such as theAcademy of Medical Royal Colleges Generic Competency Framework. The Curriculum Committeereviews such frameworks, which include generic competencies, in which all health-care professionalsneed to be proficient or which need to be embedded into continuing professional development pro-grammes to ensure maintenance of knowledge. Examples of topics are safe prescribing, infectioncontrol, child protection, environmental hazards, health promotion and public health.
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701700
Proposed ATSM in ‘Leading a sexual assault and domestic violence service’
Sexual assault and domestic violence are crimes, but the consequences are a health issue. TheBritish Crime Survey shows that a woman’s lifetime risk of sexual assault is 1 in 20. Once assaulted,victims perceive their health to be poor; usually, by the second year following the assault, 50% havebecome ‘heavily embedded’ in the health-care system.19 The College is cognisant of the effects of sexualassault on women’s health and, consequently, has sponsored many initiatives to improve the care ofvictims. The Department of Health now wishes to develop a career structure for Sexual OffencesExaminers (SOEs). This will be multidisciplinary, and, in 2010, the College Curriculum Committee isdeveloping an ATSM to improve the service by creating a programme, which will train obstetriciansand gynaecologists to manage a service to provide for the victims of sexual assault and domesticviolence and support the Department of Health work. In addition, the concept of modular credentialingand, for example, offering the ATSM to general practice (GP) trainees wishing to follow the module aspart of the GP Speciality training and education programme is currently being investigated. This wouldbe the first ATSMmodule, which would be approved for a speciality training and education programmeother than obstetrics and gynaecology.
Annual review
Three years since the introduction of the obstetrics and gynaecology curriculum, the RCOG has metthe requirements of each annual review by the regulator and, in 2010, the RCOG Specialty Training andEducation Programmewas again approved andmet the revised standards of the PMETB Framework forCurriculum and Assessment. An education and training programme will continue to evolve, and thework of the curriculum and training committees continues. The RCOG has a robust quality-assurancesystem of committees in place to manage feedback offered by trainers and trainees and to ensure thatfollowing certification, trainees are practising competently and safely.
Practice points
� A curriculum forms the backbone of a programme. In contemporary medical education, itshould address knowledge criteria, clinical competencies and professional skills andattitudes.
� All UK curricula are underpinned by the four domains of GMC Good Medical PracticeFramework for Appraisal and Assessment.
� A curriculum is a reference document but successful implementation requires structuredtraining, successful governance of training and accessible learning support resources.
Research agenda
� The effectiveness of workplace-based assessment to assess trainees following a competency-based training and education programme.
� The integration of practical skills and simulation into the curriculum.� The feasibility of trainees pursuing a 7-year programme following the introduction of theEuropean Working Time Regulation and the 48-h working week.
References
1. GMC. Good medical practice. UK: General Medical Council, 2004.2. RCOG. The future role of the consultant. London: RCOG, 2005.3. RCOG. Advanced specialty training working party report. London: RCOG, 2005.
O. Jones, W. Reid / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 685–701 701
4. PMETB. Definitions of curricula and specialist qualification. London: PMETB, 2004.5. PMETB a definitions of curricula. London: Department of Health, 2006.6. Modernising medical careers. UK: National Health Service, 2007.7. RCOG. Core logbook working party. London: RCOG, 2002.8. PMETB. Standards for curricula and assessment. London: PMETB, 2008.9. RCOG. Basic specialty training working party report. London: RCOG, 2005.
10. RCOG Council. Curriculum agreement. London: RCOG, 2006.11. The Tooke Report. The final report of the independent inquiry into modernising medical careers. MMC inquiry. London: Tooke,
2007.12. Ledger WL & Murphy MG. Curriculum and syllabus. The MRCOG: a guide to the examination. London: RCOG Press, 2007.13. GMC. Framework for appraisal and assessment. Domains of good medical practice. UK: General Medical Council, 2006.14. Conference of Postgraduate Medical Education Deans (COPMED). Liberated learning. London: COPMED, 2006.15. Department of Health. European working time regulation. London: Department of Health, 2009.16. PMETB. Annual trainees survey. London: PMETB, 2009.17. Department of Health. Safer medical practice: machines, manikins and polo mints. 150 years of the annual report of the chief
medical officer: on the state of public health 200. Chief medical officer’s report. London: Department of Health, 2009.18. The NHS institute for innovation and improvement medical leadership competency framework. NHS, 2009.19. Kershaw C, Budd T, Kinshott G, et al. The 2000 British crime survey: England and Wales. Home office statistical bulletin 18/