Page 1
©2013 Children's Mercy. All Rights Reserved. 09/13©2013 Children's Mercy. All Rights Reserved. 09/13
The Drug Exposed Neonate; The Drug Exposed Neonate; Now What?Now What?
Neonatal Abstinence Syndrome (NAS)Neonatal Abstinence Syndrome (NAS)
Betsy Knappen APRN, BSN, Betsy Knappen APRN, BSN, Jodi Jackson MDJodi Jackson MD
Page 2
©2013 Children's Mercy. All Rights Reserved. 09/13
Page 3
©2013 Children's Mercy. All Rights Reserved. 09/13
3
©2013 Children's Mercy. All Rights Reserved. 09/13
Is NAS a Real Problem?Is NAS a Real Problem?
Over the last decade, there has been increasing public health, medical, and political attention paid to the parallel rise in two trends
– Increase in the prevalence of prescription opioid abuse
– Increase in the incidence of neonatal abstinence syndrome (NAS)
Increase in the prevalence of NAS
– 1.20 per 1,000 U.S. hospital births in 2000
– 3.39 per 1,000 U.S. hospital births in 2009
Page 4
©2013 Children's Mercy. All Rights Reserved. 09/13
Finnegan ScaleAre you familiar with the
scale?A.A. YesYes
B.B. NoNo
Yes No
0%0%
Page 5
©2013 Children's Mercy. All Rights Reserved. 09/13
Finnegan ScaleWhat is your comfort level
with using the scale?A.A. Not at allNot at all
B.B. SomewhatSomewhat
C.C. NeutralNeutral
D.D. ComfortableComfortable
E.E. Very ComfortableVery Comfortable
Not at a
ll
Somewhat
Neutral
Comfo
rtable
Very Com
forta
ble
0% 0% 0%0%0%
Page 6
©2013 Children's Mercy. All Rights Reserved. 09/13
Percentage of Mother-Baby Nurses Reporting Discomfort with Elements of NAS Scoring Before and
After Education
Page 7
©2013 Children's Mercy. All Rights Reserved. 09/13
7
©2013 Children's Mercy. All Rights Reserved. 09/13
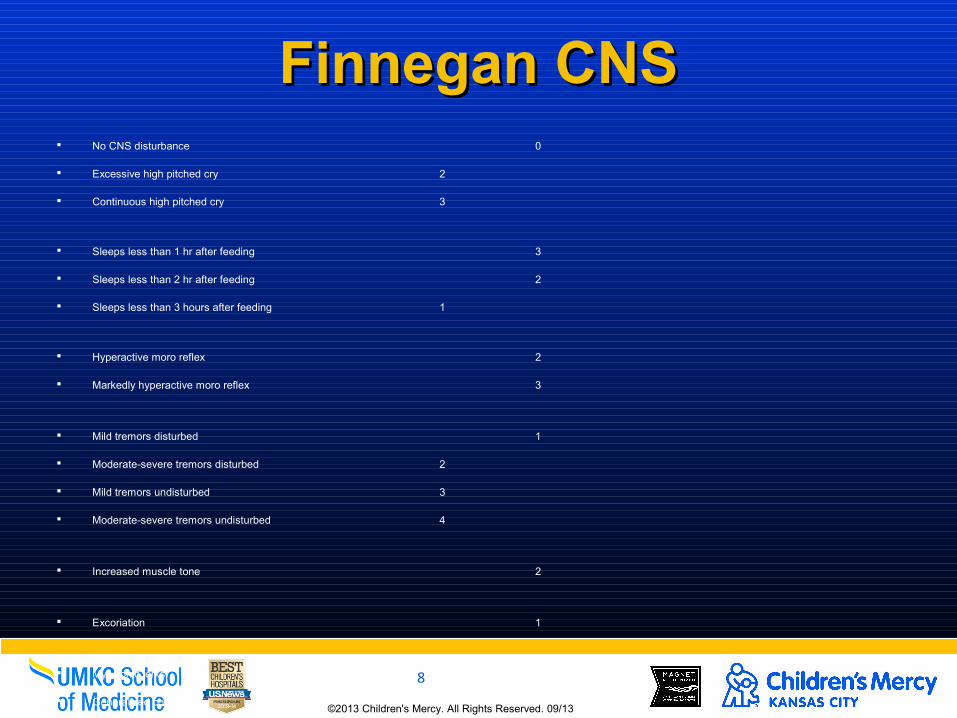
Elements of the Finnegan Elements of the Finnegan ScaleScale
Opioid receptors are concentrated in the CNS and the gastrointestinal tract, the predominant signs and symptoms of pure opioid withdrawal reflect:
– CNS irritability
– Autonomic over-reactivity
– Gastrointestinal tract dysfunction
Page 8
©2013 Children's Mercy. All Rights Reserved. 09/13
8
©2013 Children's Mercy. All Rights Reserved. 09/13
Finnegan CNSFinnegan CNS No CNS disturbance 0
Excessive high pitched cry 2
Continuous high pitched cry 3
Sleeps less than 1 hr after feeding 3
Sleeps less than 2 hr after feeding 2
Sleeps less than 3 hours after feeding 1
Hyperactive moro reflex 2
Markedly hyperactive moro reflex 3
Mild tremors disturbed 1
Moderate-severe tremors disturbed 2
Mild tremors undisturbed 3
Moderate-severe tremors undisturbed 4
Increased muscle tone 2
Excoriation 1
Myoclonic jerks 3
Generalized convulsions 5
Page 9
©2013 Children's Mercy. All Rights Reserved. 09/13
9
©2013 Children's Mercy. All Rights Reserved. 09/13
Finnegan Finnegan Metabolic/Vasomotor/RespMetabolic/Vasomotor/Resp
No Disturbance 0
Sweating 1
Fever less than 101° F (99-100.8, 37.2-38.2 C) 1
Fever greater than 101° F (38.4C) 2
Frequent yawning (3-4x/exam period) 1
Mottling 1
Nasal stuffiness 1
Sneezing (3-4x/exam period) 1
Nasal flaring 2
RR > 60/min 1
RR > 60/min with retractions 2
Page 10
©2013 Children's Mercy. All Rights Reserved. 09/13
10
©2013 Children's Mercy. All Rights Reserved. 09/13
Finnegan GIFinnegan GI
No GI disturbance 0
Excessive sucking 1
Poor feeding 2
Regurgitation 2
Projectile vomiting 3
Loose stools 2
Watery stools 3
Adapted from L.P. Finnegan (1986)
Page 11
©2013 Children's Mercy. All Rights Reserved. 09/13
Which is the First Line Treatment for NAS?
A.A. MorphineMorphine
B.B. PhenobarbPhenobarb
C.C. FentanylFentanyl
D.D. Low LightsLow Lights
E.E. Skin to Skin Skin to Skin HoldingHolding
F.F. SwaddlingSwaddlingM
orphine
Phenobarb
Fenta
nyl
Low Li
ghts
Skin to
Skin Holding
Swaddlin
g
0% 0% 0%0%0%0%
Page 12
©2013 Children's Mercy. All Rights Reserved. 09/13
12
©2013 Children's Mercy. All Rights Reserved. 09/13
Comfort MeasuresComfort Measures
Initial treatment
– Minimizing environmental stimulation
Light
Sound
– Decreasing Auto-stimulation
Swaddling
Positioning
responding to infant’s cues
frequent feedings
non-nutritive suck
clustering of cares
(Hudak & Tan, 2012; Jansson & Velez, 2012)
Page 13
©2013 Children's Mercy. All Rights Reserved. 09/13
13
©2013 Children's Mercy. All Rights Reserved. 09/13
When to use Pharmacologic When to use Pharmacologic TreatmentTreatment
The Rule of 24:
– When 2-3 consecutive scores = 24
3 Consecutive scores of 8-11
2 Consecutive scores 12 or higher
Page 14
©2013 Children's Mercy. All Rights Reserved. 09/13
Page 15
©2013 Children's Mercy. All Rights Reserved. 09/13
15
Opioid/Unknown/Poly
Morphine When pharmacologic treatment begins, patient will be started on scheduled dosing, no prns will be used
- Start morphine if Score of 24 Rule is met. - Start course based on highest score in the last 24 hours.
Initial Dose Score Frequency/Route: Every 3 hours PO
8-10 0.05 mg/kg/dose
11-13 0.08 mg/kg/dose
14-16 0.11 mg/kg/dose
>16 0.17 mg/kg/dose
Morphine Dose Escalation
If Score of 24 Rule is met after initiation, increase dose by 20%. Dose may continue to be increased by 20% every 12 hours (3-4 doses) if Score of 24 Rule is met.
Page 16
©2013 Children's Mercy. All Rights Reserved. 09/13
16
©2013 Children's Mercy. All Rights Reserved. 09/13
Pharmacologic TreatmentPharmacologic Treatment
Allow infant to stabilize 24 hours on a dose that controls symptoms prior to initiation of weaning.
If symptoms are not controlled on a total daily dose > 1 mg/kg/day, consider adding a second line medication (clonidine).
16
Page 17
©2013 Children's Mercy. All Rights Reserved. 09/13
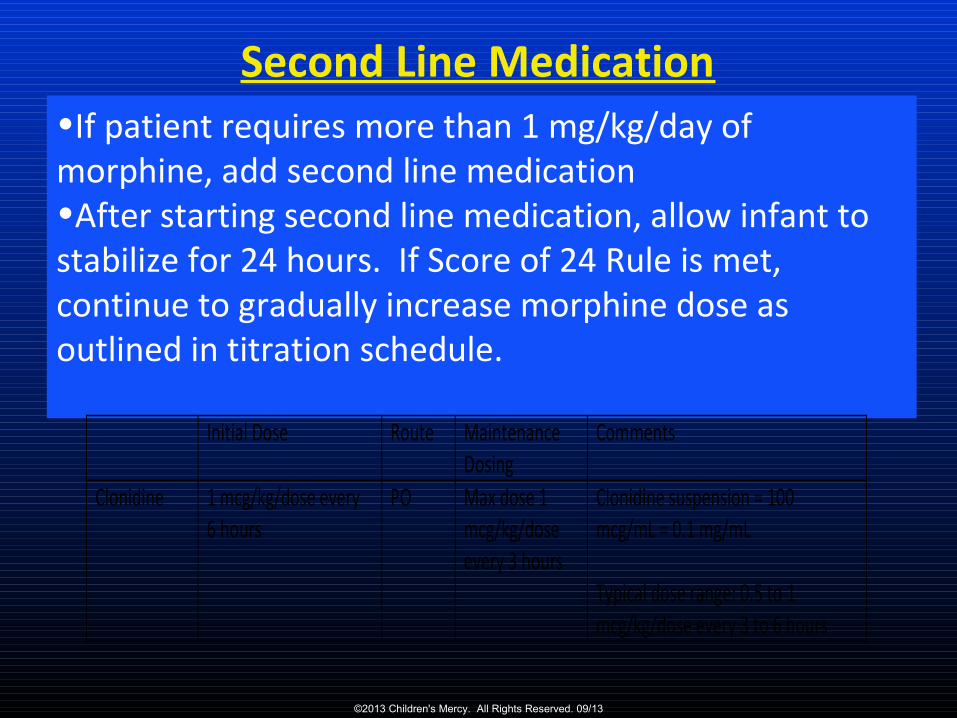
•If patient requires more than 1 mg/kg/day of morphine, add second line medication•After starting second line medication, allow infant to stabilize for 24 hours. If Score of 24 Rule is met, continue to gradually increase morphine dose as outlined in titration schedule.
Second Line Medication
Initial Dose Route Maintenance Dosing
Comments
Clonidine 1 mcg/kg/dose every 6 hours
PO Max dose 1 mcg/kg/dose every 3 hours
Clonidine suspension = 100 mcg/mL = 0.1 mg/mL Typical dose range: 0.5 to 1 mcg/kg/dose every 3 to 6 hours
Page 18
©2013 Children's Mercy. All Rights Reserved. 09/13
18
©2013 Children's Mercy. All Rights Reserved. 09/13
Weaning Pharmacologic Weaning Pharmacologic TreatmentTreatment
“Stable NAS score” is defined as all NAS scores < 8 in the preceding 24 hours
Allow 24-48 hours between medication weans
After discontinuing tx continue NAS scoring
Discharge infant when scores < 8 for at least 48 hours
18
Page 19
©2013 Children's Mercy. All Rights Reserved. 09/13
19
©2013 Children's Mercy. All Rights Reserved. 09/13
Morphine Only When NAS scores are stable, IF doses are: < 0.1 mg/kg/dose then wean dose by 20%** ≥ 0.1 mg/kg/dose then wean dose by 10%** -Allow 24 hours between morphine weans; Consult pharmacist after 2 dose changes When morphine dose reaches 0.02 mg/kg/dose every 3 hours, change frequency to every 6 hours Discontinue morphine when infant has tolerated a dose of 0.02 mg/kg/dose every 6 hours for 24-48 hours.
Morphine and Clonidine
When NAS scores are stable, IF doses are: < 0.1 mg/kg/dose then wean dose by 20% ≥ 0.1 mg/kg/dose then wean dose by 10% -Allow 24-48 hours between morphine weans; Consult pharmacist after 2 dose changes When morphine has reached ~ 0.05 mg/kg/dose, hold morphine wean and decrease clonidine by 25% daily until discontinued Resume decreasing morphine dose per pharmacist weaning schedule and discontinue morphine when infant has tolerated 0.02 mg/kg/dose for 24-48 hours.
** Percent is calculated from the original morphine dose at the start of weaning
This part of the wean has been most difficult, it is still being revised
Page 20
©2013 Children's Mercy. All Rights Reserved. 09/13©2013 Children's Mercy. All Rights Reserved. 09/13
Betsy Knappen APRN, BSN, Betsy Knappen APRN, BSN, Kim Mason RN, BSN, Andrea Vance RN, BSN, Kim Mason RN, BSN, Andrea Vance RN, BSN,
Jodi Jackson MDJodi Jackson MD
Improving Care of the Infant at Risk for Neonatal Abstinence Syndrome through
a Standardized Family Centered Protocol and Nursing Education
Page 21
©2013 Children's Mercy. All Rights Reserved. 09/13
21
©2013 Children's Mercy. All Rights Reserved. 09/13
METHODMETHOD Oct 1, 2013: NAS Protocol Trialed
– Mandatory NICU admit for high risk infant stopped
– Infants admitted to Mother-Baby unit
– NAS scoring per NICU RN
Dec 1, 2013: Mother-Baby education completed
– Infants scored and cared by Mother-Baby RN
– Transferred to NICU when Tx needed
Jan, 2014: Joined the iNICQ Collaborative
– PDSA QI process utilized for ongoing projects
– Begun standardized education program for NICU nurses
– NAS Scoring competency/reliability for NICU/Mother-Baby
Page 22
©2013 Children's Mercy. All Rights Reserved. 09/13
22
©2013 Children's Mercy. All Rights Reserved. 09/13
MEASURESMEASURES Outcome Measure:
– Infants at risk for NAS avoiding NICU admit and Tx Initial: month blocks pre/post protocol for NICU admission/ Tx
Ongoing: Quarterly review admission/ Tx ; run chart
Process Measures: – Nurses attending education, impact on
competency/comfort
Initial: comfort with NAS; Likert scale self report before/after
Ongoing: measure of reliably with competency evaluation
Validation of all scores > 8 by second observer
Page 23
©2013 Children's Mercy. All Rights Reserved. 09/13
Location of Care During Hospitalization
Infants Requiring Pharmacological Treatment
Page 24
©2013 Children's Mercy. All Rights Reserved. 09/13
24
Page 25
©2013 Children's Mercy. All Rights Reserved. 09/13
25
©2013 Children's Mercy. All Rights Reserved. 09/13
NAS scoring indicated after NAS scoring indicated after deliverydelivery
Morphine
Codeine
Hydrocodone (Lortab, Vicodin)
Oxycodone (Percocet, Oxycontin)
Methadone
Suboxone
Heroin
Tramadol
Benzodiazepines: Ativan, Xanax, Valium, Clonaxepam (Klonopin)
Polysubstance use- combination of medications (ie: mood stabilizer with an antidepressant or antipsychotic)
Page 26
©2013 Children's Mercy. All Rights Reserved. 09/13
26
©2013 Children's Mercy. All Rights Reserved. 09/13
NAS scoring not indicated after delivery NAS scoring not indicated after delivery (warrants close observation)(warrants close observation)
CNS depressant:
– Alcohol, Marijuana, K2
Hallucinogens:
– Cocaine, LSD, Methamphetamines, PCP, Phenylisopropylamines (Esctasy)
SSRI:
– Celexa, Lexapro, Prozac, Paxil, Zoloft, Luvox
SSRI/Norepiphrine Reuptake Inhibitor:
– Cymbalta
Mood Stabilizer:
– Lithium, Lamictal ?
Antipsychotics:
– Seroquel, Abilify, Latuda, Risperdal, Invega, Zyprexa, Geodon, Saphris, Fanapt, Haldol
Anxiety:
– Vistaril, Buspar
Page 27
©2013 Children's Mercy. All Rights Reserved. 09/13
27
©2013 Children's Mercy. All Rights Reserved. 09/13
Kim Mason RN, BSN; Betsy Knappen, APRN, BSN; Dawn Caspers, BS
Pharm, Jodi Jackson, MD
Standardized Approach to Educating Families at
Risk for Neonatal Abstinence Syndrome
Page 28
©2013 Children's Mercy. All Rights Reserved. 09/13
28
©2013 Children's Mercy. All Rights Reserved. 09/13
MeasuresMeasures
Outcome Measure
– Number of families at-risk for NAS who were provided education and material prior to admission
Secondary outcome:
– Number of families at-risk for NAS who are provided education and material after admission, but prior to giving birth, or after delivery (but within 24 hours)
Process Measures
– Completion of consult checklist
Balancing Measures
– Number of “urgent” unscheduled consultations required
Page 29
©2013 Children's Mercy. All Rights Reserved. 09/13
Page 30
©2013 Children's Mercy. All Rights Reserved. 09/13
30
©2013 Children's Mercy. All Rights Reserved. 09/13
Lessons LearnedLessons Learned
A key barrier in disseminating information to families prior to delivery is identification of at-risk families.
– Need for improved identification of at-risk patients
– Communication with primary care doctors regarding institutional program
– Improved collaboration with community programs
– Need to develop a mechanism to measure and quantify
– Parent-reported satisfaction with the process
Page 31
©2013 Children's Mercy. All Rights Reserved. 09/13
31
©2013 Children's Mercy. All Rights Reserved. 09/13
Breast Feeding PolicyBreast Feeding Policy
Circumstance to encourage, discourage and equivocal
The encouragement and support of BF depends on:
– Maternal drug use
– Maternal alcohol use
– Substance abuse treatment history
– Any medical and psychiatric issues
– Any medication needs
– Infants health status, in utero or post-partum
– The presence or absence and adequacy of maternal family and community support, post-partum follow up, treatment for substance abuse as needed
(Academy of Breastfeeding Medicine (ABM) Clinical Protocol #21)
Page 32
©2013 Children's Mercy. All Rights Reserved. 09/13
• CMH SCC
Our Next Initiative
Page 33
©2013 Children's Mercy. All Rights Reserved. 09/13
33
©2013 Children's Mercy. All Rights Reserved. 09/13
Thank You for Your Thank You for Your Attention.Attention.
Questions?







































![Jaundice in Neonate[1]](https://static.documents.pub/doc/80x56/577cdf6d1a28ab9e78b136c3/jaundice-in-neonate1.jpg)





