WOUND HEALING 0039-6109/97 $0.00 + .20 THE ENHANCEMENT OF WOUND HEALING WITH HUMAN SKIN ALLOGRAFT Robert J. Spence, MD, FACS, and Lesley Wong, MD, FACS Wound healing is a complex and organized response by the body to tissue injury and loss of integrity. Many factors influence the progress of wound healing, but none so profoundly as whether the wound is open or closed. A closed wound heals generally undisturbed along a well-established temporal sequence of the normal repair process de- scribed by Schilling.26 In the absence of foreign bodies and microorgan- isms, inflammation, edema, and subsequent scar formation are minimal. An open wound, on the other hand, is affected by a host of outside influences that invariably prolong the wound healing process and result in more inflammation, edema, and scarring than normal closed wound healing. Whereas clean incisional wounds can be easily closed, contaminated wounds, wounds with tissue loss that cannot be closed primarily, and chronic wounds are generally not closed and suffer the effects of being open. It follows that wound healing would be enhanced if these wounds could be closed. This article describes how skin allograft biologic dress- ings bestow the benefits of wound closure on those wounds frequently not closed in practice. HISTORY Clinical Use of Skin Allograft Clearly, the most difficult type of skin wound early physicians were required to manage was the skin loss of thermal burn injury. It seems From The Johns Hopkins Medical School, Baltimore, Maryland SURGICAL CLINICS OF NORTH AMERICA VOLUME 77 * NUMBER 3 JUNE 1997 731
Transcript
WOUND HEALING 0039-6109/97 $0.00 + .20
THE ENHANCEMENT OF WOUND HEALING WITH
HUMAN SKIN ALLOGRAFT Robert J. Spence, MD, FACS, and Lesley Wong, MD, FACS
Wound healing is a complex and organized response by the body to tissue injury and loss of integrity. Many factors influence the progress of wound healing, but none so profoundly as whether the wound is open or closed. A closed wound heals generally undisturbed along a well-established temporal sequence of the normal repair process de- scribed by Schilling.26 In the absence of foreign bodies and microorgan- isms, inflammation, edema, and subsequent scar formation are minimal. An open wound, on the other hand, is affected by a host of outside influences that invariably prolong the wound healing process and result in more inflammation, edema, and scarring than normal closed wound healing.
Whereas clean incisional wounds can be easily closed, contaminated wounds, wounds with tissue loss that cannot be closed primarily, and chronic wounds are generally not closed and suffer the effects of being open. It follows that wound healing would be enhanced if these wounds could be closed. This article describes how skin allograft biologic dress- ings bestow the benefits of wound closure on those wounds frequently not closed in practice.
HISTORY
Clinical Use of Skin Allograft
Clearly, the most difficult type of skin wound early physicians were required to manage was the skin loss of thermal burn injury. It seems
From The Johns Hopkins Medical School, Baltimore, Maryland
SURGICAL CLINICS OF NORTH AMERICA
VOLUME 77 * NUMBER 3 JUNE 1997 731
732 SPENCE & WONG
logical that physicians dealing with this difficult problem, particularly before the advent of antibiotics, attempted to substitute other tissue for lost skin.
Baronioz first found that skin could be grafted from one part of a sheep to another in 1803. Surprisingly, it was 66 years before Reverdinz5 reported the first human skin graft. Reverdin’s first autograft was a small, extremely thin epidermal graft. Shortly thereafter, George David Pollockz3 reported placing a small piece of his own skin along with pieces of his patient’s skin on his patient’s burn wound. He described how both grafts appeared to take, but his skin subsequently disappeared from the healing wound. This first reported case of the use of a human skin allograft (HSA) was followed by a better known case by Girdner13 in 1881 in which a large bum wound was treated with human cadaveric skin. Again, after initial take of the skin, he reported its loss through an ”erysipelatous inflammation.”
The transplantation of allograft skin (also called homografts and isografts) was attempted by many others following Girdner’s report. Virtually all reported initial take and subsequent loss of the grafts from what we understand now is rejection of foreign tissue after vasculariza- tion by the host. Most were willing to relegate allograft transplantation to fable and mythology until Bettman4 asked and answered the question: What is the condition of the wound and the patient while the allograft is in place? The answer was that the wounds were ”healed for the time being and free from infection. The patient is rid of these areas of sepsis.” He went on to describe the great benefits two children with 60% and 80% burns, respectively, obtained from temporary allograft skin from the parents. They survived what were almost certainly fatal injuries at the time.
Allograft skin was not used routinely in the treatment of burn injuries until Brown and his associates6 in St. Louis began using it in their bum unit. Around the time of Brown’s report, allograft skin was introduced as routine therapy for bum patients at Brooke Army Hospi- tal.’ The 10-year experience with its use at Brooke was reported by Zaroff et aP5 in 1966. In that article, Zaroff and colleagues listed the benefits realized by the patients treated with the allograft skin (Table 1).
Allograft Skin Banking
The storage of allograft for use at a later time is an essential element in its routine clinical use in wounds. Although Carrelg had written about the banking of tissue in 1912 and Went~cher~~ experimented with the storage of sheepskin graft as early as 1903, the banking of human tissue had to await the development of reliable refrigeration in the 1930s. The first blood bank was established at Cook County Hospital in 1937, with subsequent creation of other tissue banks. W e b ~ t e r ~ ~ was the first to report the clinical use of skin grafts refrigerated for significant lengths of time. The maximal length of storage that yielded viable grafts under
THE ENHANCEMENT OF WOUND HEALING WITH HUMAN SKIN ALLOGRAFT 733
Table 1. BENEFITS OF ALLOGRAFT SKIN
1. Limitation of infection and keeping the bed mechanically clean 2. Decrease in water, electrolyte, and protein loss 3. Decrease in energy requirements secondary to the calories necessary for the
large obligatory loss of free water through the open wound 4. Reduction of pain, allowing exercise and ambulation, and decrease in the
incidence of contractures 5. Conservation of autograft 6. Improvement in appetite and general welfare 7. Improvement in psychological outlook of the patient
From Zaroff LI, Mills W, Duckett JW, et al: Multiple uses of viable cutaneous homografts in the burned patient. Surgery 59:368, 1966; with permission.
these conditions was 21 days. In search of a way to store tissue for longer periods, Strumia and H ~ d g e ~ ~ reported in 1945 the viable autografting of skin that had been frozen. This was almost immediately called into question by Baxter and Entin3; in 1948, they discovered that skin was killed by ice crystal formation upon freezing. It is thought that the healing Strumia and Hodge observed with the application of previously frozen skin was the result of the beneficial effects of nonviable biologic dressing on wounds that healed secondarily.
Only by a chance observation in 1949 did Polge et a122 discover a cryopreservative that made the freezing of tissues in the viable state possible. While trying numerous diluents in which to freeze sperm in the viable state, they were surprised to find that only a saline solution yielded viable sperm when thawed. On closer examination, they found glycerol present in the saline as a preservative. When they subsequently tried solutions of glycerol, they found it to be the active cryopreserva- tive agent.
Although cell suspensions were frozen in the viable state soon after this discovery, it was 1964 before Lehr and his colleague^^^ reported freezing rat skin in the viable state after exposure to a glycerol solution and the subsequent “take” of the autograft when reapplied to the rat. It was not until 1968 that Cochranel’ reported the first clinical use of skin autografts that had been frozen and thawed prior to being used in the viable state. Only then were the first skin banks for the frozen storage of skin established by Bondoc and Burke5 for the Burn Unit at the Massachusetts General Hospital and by Trier and SelPl for the US Navy at the Bethesda Naval Hospital.
Allograft Basic Science
While clinical trials using HSA were under way, basic research was being performed to elucidate the mechanisms that made biologic dressings superior to conventional dressings. Eade’* noted a significant reduction of the number of bacteria under biologic dressings compared
734 SPENCE & WONG
with conventional gauze dressings. Wood34 discovered that phagocytes in the wound used the fibrin matrix established between a biologic dressing and the wound to trap bacteria, allowing phagocytosis of the bacteria without antibody production or opsonins. These observations, repeated by others, seem to be well established.8, 30
Upon further investigation of the effects of skin allograft on wounds, ODonaghue and ZaremzO found that skin allograft stimulates neovascularization of the wound. This stimulation of neovascularization and the actual vascularization of the viable allograft (the ”take”) make viable allograft the most ideal biologic dressing (autograft would not be considered a “dressing”).
The stimulation of neovascularization and other positive effects generally seen with the use of grafts has led to speculation about the presence of cytokines at the cut surface of grafts. Cultured epithelial allografts have been used to enhance chronic wound healing and may allow investigation into the mechanism of action. Leigh and Purkis16 and Phillips et alZ1 have successfully treated refractory chronic leg ulcers with cultured epithelial autografts. Using monoclonal antibodies and chromosomal probes, they determined that cultured allograft cells do not ultimately survive but are replaced by the recipient’s own epithelial cells. The cultured allografts seem to provide a potent stimulus to healing. It was postulated that soluble growth factors contribute to the re-epithelialization noted with each successive placement of allograft (serial allografting). An epidermal cytokine network has been estab- lished, and many different mediators involved in the early inflammatory phase and later phases of fibroblast proliferation and angiogenesis have been isolated.l7, l8
The concept of using allograft skin to provide a ”dose pack” of growth factors has been postulated in which the grafts may not simply be a tissue replacement but may be used as a pharmacologic agent.14 In a recent study, Rennekampff et alZ4 measured various cytokines from cryopreserved allograft skin, autologous cultured epithelial sheets, and human keratinocytes cultured to single-layer confluence on Hydroderm polyurethane membranes. Cytokines were found associated with all three types of wound dressings, with the cultured epithelial sheets releasing the greatest quantity.
Allograft Use in Nonburn Traumatic Wounds
In 1966, Morris et all9 reported that skin allograft promoted the healing of infected ulcers. Shortly thereafter, the same group reported the beneficial effects of skin allograft placed in heavily contaminated wounds as a ”physiologic primary cl~sure.”~
Working at Brooke Army Hospital with wounded soldiers from the Vietnam War, Shuck et alZ7, 28 reasoned that the benefits seen in large bum wounds also would be seen if biologic dressings of allograft skin were used in nonburn traumatic wounds. Their clinical trial bore this out
THE ENHANCEMENT OF WOUND HEALING WITH HUMAN SKIN ALLOGRAET 735
and was reported in 1969 and 1972. These reports stimulated our use of allograft skin in traumatic nonbum wounds seen in our clinical practice at the Maryland Institute for Emergency Medical Systems in the early 1980s. During that time, dramatic improvements in the wounds and the patients’ conditions were realized. Some of these form the basis of this report.
Skin Allograft and Human Immunodeficiency Virus (HIV)
With the growth of HIV and AIDS awareness in the mid 1980s, controversy arose regarding the use of allograft skin in non-life-saving situations. Some bum units discontinued the use of allograft skin com- pletely. The transmission of HIV with HSA remained a theoretical possi- bility until 1987, when Clarke’O reported a case of HIV transmission with fresh HSA. This report appeared to bring the use of allograft skin in non-life-saving situations to a complete halt, along with our thoughts of reporting our nonburn traumatic wound experience in the literature.
However, no case of HIV transmission by properly cryopreserved and banked HSA from properly screened donors has ever been reported. Clarke’s case involved fresh allograft taken from an unscreened donor and placed on a newly d6brided bum wound. Therefore, the risk of HIV transmission via skin allograft from properly screened donors and properly cryopreserved tissue remains theoretical. Theoretically this risk should also be substantially less than the risk of transmission through banked blood, as the number of potentially HIV-bearing cells is much less than in banked blood.
TECHNIQUE
Briefly, H S A biologic dressing should be applied as i f it were autograft. The goal is to get the allograft to take just as if it were an autograft, albeit temporarily.
The wound should be prepared to enhance the vascularity of its interface with the graft and to reduce bacterial contamination and ne- crotic debris. This preparation can be performed sharply, if necessary, but my preferred method is scrubbing the wound with a surgical scrub brush containing a povidone-iodine or chlorhexidine scrub solution, followed by a saline rinse and compression for hemostasis.
In the operating room, anesthesia is usually no problem. However, HSA biologic dressing can, and frequently is, applied at the bedside. In this situation, I have found that application for 20 minutes of a gauze sponge soaked with 10% lidocaine solution results in adequate topical anesthesia to allow preparation of the wound. I have not used a topical eutectic mixture of local anesthetics, as I am not sure of its effect on the wound with regard to its ability to take a graft.
736 SPENCE & WONG
Once the wound is prepared and draped to provide as sterile a field as possible, the allograft is either applied as a sheet or meshed at a ratio of 1.5:l. On clean wounds with good hemostasis, I use the allograft as a sheet. On wounds with questionable hemostasis and in contaminated or chronic wounds, I often apply the HSA meshed but unexpanded. This, of course, allows for drainage, but it also may increase the quantity of cytokines released by the graft into the wound, further enhancing the effect.
The graft is tailored to fit the wound. Excess allograft overlying the epithelialized wound margins obviously does not adhere and is a fre- quent nidus of purulence. Once tailored, the graft is fixed in place with sterile wound tapes (e.g., Steri-Strips), and a firm outer dressing is placed. The first layer is a nonadherent layer, followed by a sterile gauze layer wet with an antibiotic or antiseptic solution (e.g., oxychlorasene). A dry outer wrap is then placed. If the graft is near a joint, the joint is splinted.
The dressing is first taken down at 3 days after application in contaminated wounds. In sterile wounds, the dressing may be left intact for a week or more. In patients with depressed immunologic capacity, such as severe bum patients, the allograft is often in place for several weeks before any signs of rejection develop. In patients with normal immunity, the allograft undergoes rejection 2 to 3 weeks after applica- tion. HSA in these patients is strictly a biologic dressing that can be removed relatively easily at 3 to 5 days. At 3 days, good adherence of the graft often gives one enough information to proceed with autograft- ing. When the graft is removed, the wound bed displays uniformly good capillary bleeding that stops easily with compression with moist saline or dilute epinephrine-saline compresses. If the allograft is not adhering, it can be changed for another piece immediately. If purulence is present, wet-to-dry dressings with a topical antiseptic solution for 1 or 2 days often prepare the wound for another allograft application.
ALLOGRAFT BENEFITS IN WOUND HEALING
The benefits of HSA as a biologic dressing in burn wounds, origi- nally outlined by Zaroff et al,35 are listed in Table 1. Our clinical experi- ence, along with that of Shuck et al,27, 28 suggests that similar benefits are seen in nonburn traumatic wounds as well. These benefits have led to some well-defined clinical situations in which HSA biologic dressings enhance wound healing and wound management (Table 2). Case histo- ries illustrate these situations and further expand the understanding of these advantages.
Case 1
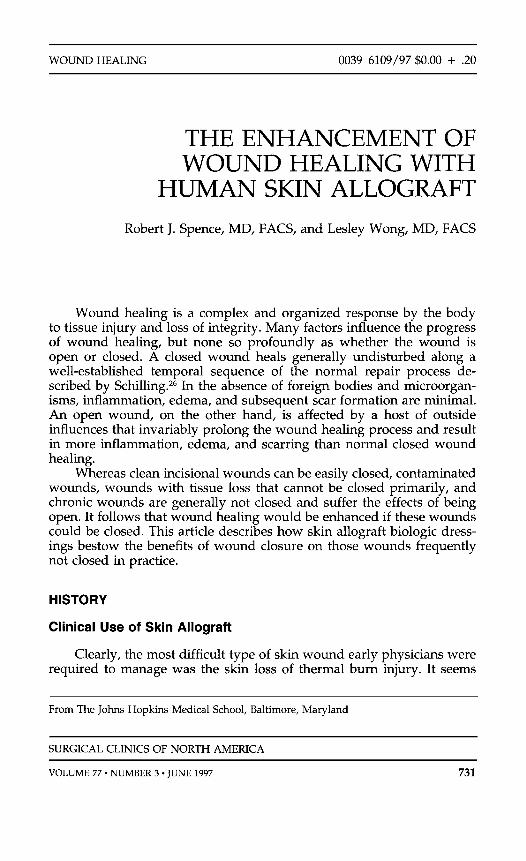
A 4-year-old child was transferred to the University of Maryland Hospital after falling under a riding lawn mower. She sustained multiple fractures and a huge longitudinal wound of her leg (Fig. 1A). An immediate operation was
THE ENHANCEMENT OF WOUND HEALING WITH HUMAN SKIN ALLOGRAFT 737
Table 2. INDICATIONS FOR ALLOGRAFT SKIN BIOLOGIC DRESSINGS
Physiologic closure of early wound Testing of wound for autograft take Preparation and enhancement of wound for autograft take Temporary closure of life-threatening, massive wounds (e.g., burns, necrotizing
fasciitis)
performed to dkbride her wound and close it with HSA (Fig. 1B). She was returned to the operating room twice for re-examination, dkbridement, and replacement of HSA dressings under general anesthesia. Between trips to the operating room, her dressings were not disturbed and the child did not complain of pain.
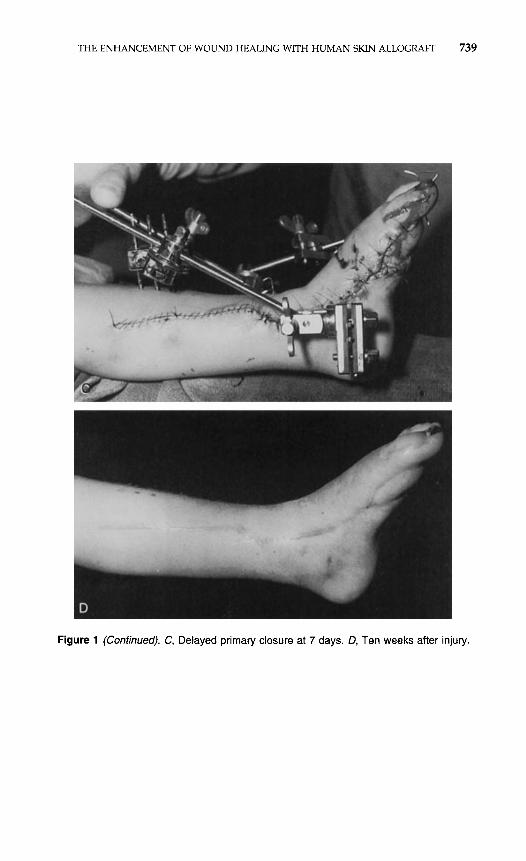
On the seventh post-injury day, her wound was clean and had no remaining nonviable tissue, no granulation tissue, and minimal swelling. A delayed pri- mary closure was therefore performed (Fig. 1C). The wound healing was uncom- plicated, and it was possible to discharge the patient 10 days after her injury. She remained healed and did well in follow-up (Fig. 1D).
Allograft skin maintained the wound as physiologically closed from just a few hours after injury until the time of reconstruction. This resulted in minimal pain, maintenance of a pristine wound, rapid resolution of edema, and early wound closure with assurance of no infection. The HSA began adhering to the wound, indicating the absence of necrotic tissue and infection. The absence of granulation tissue throughout the course of treatment and particularly at the time of wound closure was very beneficial. It adds credence to the suggestion that granulation tissue is a response to bacteria and other noxious substances that come in contact with an open wound. HSA dressings prevent such contact.
These benefits were particularly significant in this child. There were a minimum of dressing changes under anesthesia, no dressing changes while she was awake, and minimal pain from the wound after closure with HSA. All this minimized the trauma of the experience.
Similar enhancement of wound healing is achievable in fasciotomy wounds as well as traumatic wounds. This common, initially surgically sterile wound closed immediately with allograft skin can frequently be closed secondarily after resolution of the edema that occurs after HSA wound closure. This is preferable to using a patient autograft initially with its attendant donor site and other problems.
Case 2
An 89-year-old retired man was referred after a Mohs’ histographic surgical excision of a large basal cell carcinoma of his lateral face. The surgery had been completed 4 days prior to his visit. He had a 10 X 7 cm granulating wound extending from his left ear to the lateral orbital rim and covering virtually all of his lateral temporal and zygomatic regions. His wound was cleaned, and an HSA dressing was placed. The patient was discharged to return in 3 days for reconstruction of his lateral face.
The patient was admitted to the hospital 2 days later. The HSA dressing was adherent over the entire wound, with the exception of the superior margin, where purulence was present under approximately 1 cm of the allograft (Fig. 2A). This margin was dkbrided and cleansed. The following day the patient was
738 SPENCE & WONG
Figure 1. A, Case 1: left lower extremity wound at initial exploration. 8, Wound closed with human skin allograft.
THE ENHANCEMENT OF WOUND HEALING WITH HUMAN SKIN ALLOGRAFT 739
Figure 1 (Continued). C, Delayed primary closure at 7 days. D, Ten weeks after injury.
740 SPENCE & WONG
Figure 2. A, Case 2: human skin allograft adherent to skin cancer excision site. 6, Full- thickness autografl vascularized at 3 days (note blanching). C, Note poorer vascularity along superior margin not covered by HSA.
THE ENHANCEMENT OF WOUND HEALING WITH HUMAN SKIN ALLOGRAFT 741
taken to the operating room, where the superior margin was excised and a full- thickness autograft from his neck and shoulder was used to close the wound. The allograft was removed just prior to placing the autograft, revealing a clean, richly vascular bed.
The dressing was removed from the full-thickness autograft on the third postoperative day. The autograft was found to be not only adherent but also completely vascularized, as demonstrated by the visible capillaries that blanched with pressure and refilled (Fig. 2B). The superior margin was the only aspect of the autograft that looked like a typical 3-day-old full-thickness skin graft, still white and poorly vascularized (Fig. 2C). The patient went on to heal completely with a good cosmetic result.
This case demonstrates HSA’s remarkable ability to prepare an open wound for either delayed primary closure or autograft closure. Allograft cleans the wound to some degreezsB and stimulates neovas~ularization?~ The mechanism of this action is uncertain, but some biochemical interaction between the wound bed and the cut surface of the graft clearly stimulates the wound. The action of growth factors is likely, in addition to the previously documented interaction of macrophages with fibrin. Clearly, allograft skin wound delay in wounds with poor hemostasis before placing large important autografts may have added benefits besides the hemostasis.
Case 3 A 44-year-old woman presented with a chronic open wound of the dorsum
of her right foot, which first occurred after relatively minor trauma 5 years previously. Several split-thickness autografts had been attempted at other hospi- tals, but none completely healed before failing. The patient did not have diabe- tes mellitus.
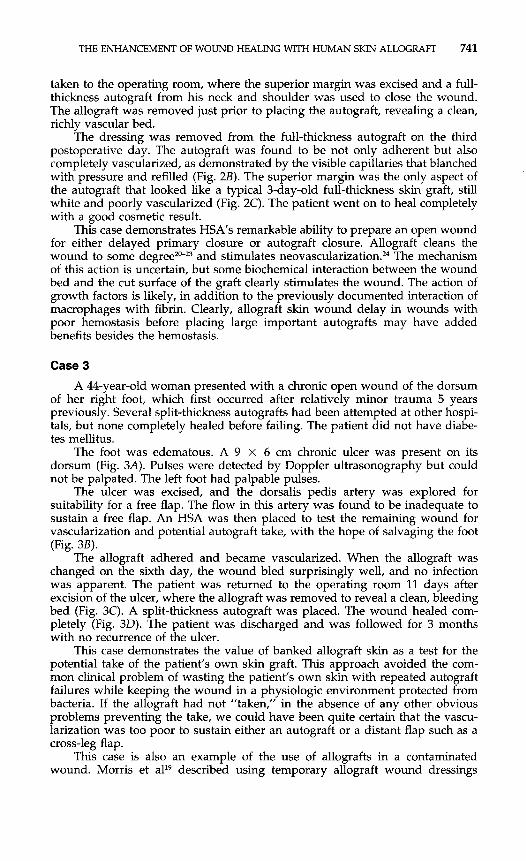
The foot was edematous. A 9 X 6 cm chronic ulcer was present on its dorsum (Fig. 3A). Pulses were detected by Doppler ultrasonography but could not be palpated. The left foot had palpable pulses.
The ulcer was excised, and the dorsalis pedis artery was explored for suitability for a free flap. The flow in this artery was found to be inadequate to sustain a free flap. An HSA was then placed to test the remaining wound for vascularization and potential autograft take, with the hope of salvaging the foot (Fig. 3B).
The allograft adhered and became vascularized. When the allograft was changed on the sixth day, the wound bled surprisingly well, and no infection was apparent. The patient was returned to the operating room 11 days after excision of the ulcer, where the allograft was removed to reveal a clean, bleeding bed (Fig. 3C). A split-thickness autograft was placed. The wound healed com- pletely (Fig. 30). The patient was discharged and was followed for 3 months with no recurrence of the ulcer.
This case demonstrates the value of banked allograft skin as a test for the potential take of the patient’s own skin graft. This approach avoided the com- mon clinical problem of wasting the patient’s own skin with repeated autograft failures while keeping the wound in a physiologic environment protected from bacteria. If the allograft had not ”taken,” in the absence of any other obvious problems preventing the take, we could have been quite certain that the vascu- larization was too poor to sustain either an autograft or a distant flap such as a cross-leg flap.
This case is also an example of the use of allografts in a contaminated wound. Morris et all9 described using temporary allograft wound dressings
742 SPENCE & WONG
Figure 3. A, Case 3: chronic wound of right foot before excision. B, Human skin allograft applied to the ulcer excision site.
in contaminated abdominal wounds, obviating repeated dressing changes and ensuring sterility before closing the wound secondarily.
Along with burn wounds, another awesome wound a surgeon must manage is that resulting from necrotizing fasciitis. These wounds, like burn wounds, are best treated with early closure after infection and necrosis are controlled by debridement. Allograft does this rapidly, at the bedside if necessary, and still allows the surgeon to inspect the wound to rule out further necrosis. Inspection can be done with the knowledge that if the allograft must be disturbed, it can be replaced easily with the same or another piece of allograft.
DISCUSSION
HSA and comparable biologic dressings close the wound . . . tempo- rarily. The patient and the wound are deceived into believing that the
THE ENHANCEMENT OF WOUND HEALING WITH HUMAN SKIN ALLOGRAFT 743
Figure 3 (Continued). C, Clean, bleeding ulcer excision site after HSA is removed. D, Wound completely healed 1 month later.
wound is closed. Clinical experience supported by basic science suggests that application of HSA can enhance the healing of wounds that would normally be left open because of significant tissue loss, contamination, chronicity, or questionable secondary closure or closure with autograft.
HSA can be an invaluable tool in the management of severe trau- matic wounds. In patients with severe burn wounds, the problems of resuscitation and early infection have been resolved adequately by advances in fluid management, monitoring, and antibiotics. The current challenge is how best to remove all the destroyed skin early, to cover the resulting wound, and to obtain optimal function of the replaced skin. HSA plays a key role in this challenge when autograft donor sites are limited. Even when extensively burned patients are grafted with their own epidermal cells grown in tissue culture, they must be covered and kept alive with skin allograft while their cells are being cultured. In fact, cultured epidermal autografts (CEA) take better and provide better wound coverage when HSA is first placed on the wound and the CEA is placed over de-epithelialized HSA.
Similarly, the greatest challenge for those dealing with nonburn traumatic wounds is how to manipulate a very large or otherwise
744 SPENCE & WONG
problematic wound to heal most quickly and with the least morbidity to the patient. We have demonstrated in this article how HSA can be used for this purpose.
The experience with a large number of trauma patients at the Maryland Institute for Emergency Medical Systems Shock Trauma Cen- ter provided ample experience with nonburn wounds. We applied les- sons learned from burn wound care with biologic dressings to patients with these wounds. The cases illustrate various ways that allograft skin is of value in these patients. All the benefits ascribed to allograft by Zaroff et a135 in burn patients are seen in this set of patients. We agree with Shuck et alZ7, 28 and others that HSA also enhances wound healing in nonburn traumatic wounds. We have found that HSA can be used to manipulate the wound: In a new wound, early closure with HSA keeps it fresh without bacterial colonization and granulation tissue and with much faster resolution of associated edema. In contaminated wounds, HSA cleans the wound and tests for autograft take potential. In chronic wounds, it prepares a wound for autograft take and results in much faster vascularization of subsequent autograft. HSA closes all wounds to which it adheres, conferring the benefits of wound closure generally.
Research is beginning to delineate the biochemical nature of the phenomenon seen with HSA application. Clearly, cytokines are involved at the interface between cut graft surface and the wound. New products using cultured cells, either alone or in conjunction with artificial wound coverings, may well replace HSA in their ability to deliver cytokines to the wound if this is the primary goal. HSA currently has the advantage of apparently adhering to the wound and vascularizing more quickly than these other products. HSA appears to resist infection better than these products as well.
The risk of HIV transmission via HSA remains a concern. However, such transmission via properly cryopreserved tissue from a properly screened donor has never been reported but remains a theoretical possi- bility, most likely with a theoretical risk substantially less than the risk from blood transfusion. We believe that certain wounds derive such great benefit from allograft application that HSA from a tissue bank that follows the American Association of Tissue Banks skin banking guide- lines can be safely applied to a patient with a non-life-threatening wound. Certainly, wound closure with either HSA or a wound cover containing human cells releasing cytokines is indicated in many wounds that are a problem simply due to failure to close.
References
1. Artz CP, Becker Jh4, Sako Y, et al: Postmortem skin homografts in the treatment of
2. Baronio G: In Degli Innesti Animali. Milano, 1804 3. Baxter H, Entin MA: Experimental and clinical studies of reduced temperatures in
4. Bettman AG: Homogeneous Thiersch grafting as a life saving measure. Am J Surg
5. Bondoc CC, Burke J F Clinical experience with viable frozen human skin and a frozen
extensive burns. Arch Surg 71:682, 1955
injury and repair in man. Plast Reconstr Surg 3:303, 1948
39:156, 1938
skin bank. Ann Surg 174:371, 1971
THE ENHANCEMENT OF WOUND HEALING WITH HUMAN SKIN ALLOGRAFT 745
6. Brown JB, Minot PF, Randall P: Postmortem homografts as ‘biological dressings’ for
7. Burke JF, Bondoc CC: A method of secondary closure of heavily contaminated wounds
8. Burleson R, Eiseman 8: Mechanisms of antibacterial effect of biological dressings. Ann
9. Carrel A: The preservation of tissues and its application of surgery. JAMA 59:523,1912 10. Clarke JA: HIV transmission and skin grafts [letter]. Lancet 1:983, 1987 11. Cochrane T The low temperature storage of skin: A preliminary report. Br J Plast
Surg 21:118, 1968 12. Eade GG: The relationship between granulation tissue, bacteria, and skin grafts in
burned patients. Plast Reconstr Surg 22:42, 1958 13. Girdner J H Skin-grafting with grafts taken from the dead subject. Med Record
20119, 1881 14. Kirsner RS, Falanga V, Eaglestein WH: Biology of skin grafts: Grafts as pharmacologic
agents. Arch Dermatol 129:481, 1993 15. Lehr HB, Berggren RB, Lotke PA, et al: Permanent survival of preserved skin auto-
grafts. Surgery 56:742, 1964 16. Leigh IM, Purkis PE: Cultured skin grafted leg ulcers. Clin Exp Dermatol 11:650452,
1986 17. Luger TA, Schwarz T: Evidence for an epidermal cytokine network. J Invest Dermatol
95:100S, 1990 18. McKenzie RC, Sauder DN: The role of keratinocyte cytokines in inflammation and
immunity. J Invest Dermatol95:105S, 1990 19. Morris PJ, Bondoc C, Burke J F The use of frequently changed skin allografts to
promote healing in the non-healing infected ulcer. Surgery 66:13, 1966 20. ODonaghue MN, Zarem HA: Stimulation of neovascularization-comparative efficacy
of fresh and preserved skin grafts. Plast Reconstr Surg 48:474, 1971 21. Phillips TJ, Kehinde 0, Green H, et al: Treatment of chronic skin ulcers with cultured
epidermal allografts. J Am Acad Dermatol 21:191, 1989 22. Polge C, Smith AU, Parkes AS Revival of spermatozoa after vitrification and dehydra-
tion at low temperature. Nature 164:666, 1949 23. Pollock GD: Cases of skin grafting and skin transplantation. Trans Clin SOC Lond
4:37, 1871 24. Rennekampff HO, Kiessig V, Loomis W, et al: Growth peptide release from biologic
dressings: A comparison. J Burn Care Rehabil 17522, 1996 25. Reverdin JL: Greffe epidermique. Bull SOC Imperiale Chir Paris 493, 1869 26. Schilling J: Wound healing. Surg Clin North Am 56:859, 1976 27. Shuck JM, Bedeau GW, Thomas PR Homograft skin for the early management of
extensive burns and denuded areas. Ann Surg 138:618,1953
98:472, 1969 29. Strumia MM, Hodge CC: Frozen human skin grafts. Ann Surg 121:860, 1945 30. Teh BT Why do skin grafts fail? Plast Reconstr Surg 63:323, 1979 31. Trier WC, Sell KW: United States Navy Skin Bank. Plast Reconstr Surg 41:543, 1968 32. Webster J P Refrigerated skin grafts. Ann Surg 120:421, 1944 33. Wentscher J: Ein weiterer Beitrag zur Uberlebensfahigkeit der menschlichen Epider-
34. Wood WB: Phagocytosis, with particular reference to encapsulated bacteria. Bacteriol
35. Zaroff LI, Mills W, Duckett JW, et a1 Multiple uses of viable cutaneous homografts in
miszellen. Deutsche Zeitschr Chir 70:21, 1903-04
Rev 24:41,1960
the burned patient. Surgery 59:368, 1966
Address reprint requests to Robert J. Spence, MD, FACS
The Johns Hopkins Bayview Medical Center 4940 Eastern Avenue Baltimore, MD 21224