23
The financing dimension in SHA 2011 A focus on the Revenue of Schemes Patricia Hernandez WHO HA Geneva
The financing dimension in SHA 2011
A focus on the Revenue of Schemes
Patricia Hernandez WHO HA Geneva
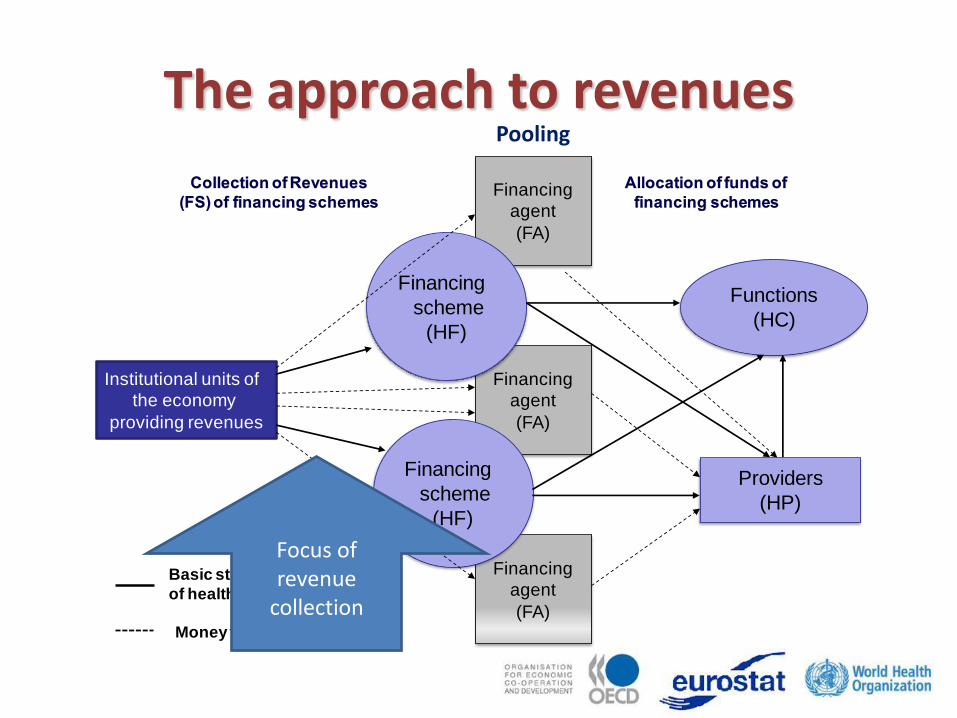
The approach to revenues
Financing
agent
(FA)
Financing
agent
(FA)
Institutional units of
the economy
providing revenues
Financing
agent
(FA)
Providers
(HP)
Functions
(HC)
Financing
scheme
(HF)
Financing
scheme
(HF)
Basic structural relationships
of health financing
Money flow
Pooling
Focus of revenue
collection

Revenues of health financing schemes (FS)
• Revenues vs. Expenditures – Revenue is an increase in the funds of a financing
scheme
– Expenditure is the amount spent by the institutional units providing resources.
• FS classification highlights the sources and the mechanisms of revenue raising for each financing scheme.
• PG tracked Financing Sources = expenditure by entities; whereas SHA 2011 track Revenues linked to expenditure by financing schemes.

Classification of revenues of financing schemes (First digit)
FS.1Transfers from government domestic revenue (allocated to
health purposes)
FS.2 Transfers distributed by government from foreign origin
FS.3 Social insurance contributions
FS.4 Compulsory prepayment (other than FS.3)
FS.5 Voluntary prepayment
FS.6 Other domestic revenues n.e.c.
FS.7 Direct foreign transfers
Reporting items
FS.RI.1 Institutional units providing revenues to financing schemes
FS.RI.2 Total foreign revenues (FS.2 +FS.7)
FS Related
items
FSR.1 Loans
FSR.2 Aid in kind at donor value
Memorandum items
SNA based
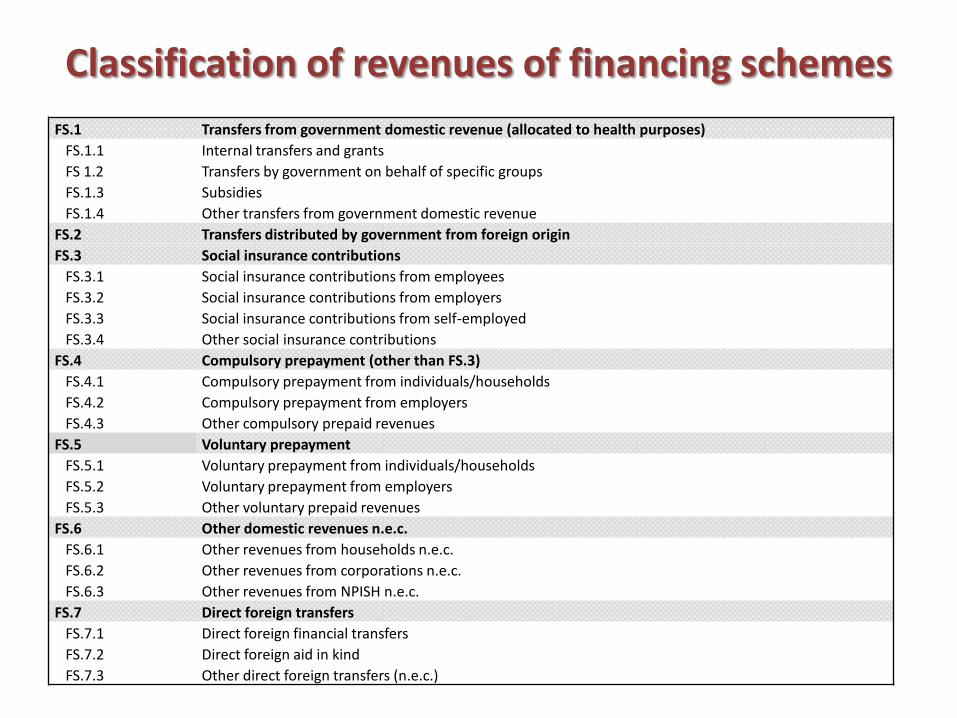
Classification of revenues of financing schemes
FS.1 Transfers from government domestic revenue (allocated to health purposes)
FS.1.1 Internal transfers and grants
FS 1.2 Transfers by government on behalf of specific groups
FS.1.3 Subsidies
FS.1.4 Other transfers from government domestic revenue
FS.2 Transfers distributed by government from foreign origin
FS.3 Social insurance contributions
FS.3.1 Social insurance contributions from employees
FS.3.2 Social insurance contributions from employers
FS.3.3 Social insurance contributions from self-employed
FS.3.4 Other social insurance contributions
FS.4 Compulsory prepayment (other than FS.3)
FS.4.1 Compulsory prepayment from individuals/households
FS.4.2 Compulsory prepayment from employers
FS.4.3 Other compulsory prepaid revenues
FS.5 Voluntary prepayment
FS.5.1 Voluntary prepayment from individuals/households
FS.5.2 Voluntary prepayment from employers
FS.5.3 Other voluntary prepaid revenues
FS.6 Other domestic revenues n.e.c.
FS.6.1 Other revenues from households n.e.c.
FS.6.2 Other revenues from corporations n.e.c.
FS.6.3 Other revenues from NPISH n.e.c.
FS.7 Direct foreign transfers
FS.7.1 Direct foreign financial transfers
FS.7.2 Direct foreign aid in kind
FS.7.3 Other direct foreign transfers (n.e.c.)

Classification of revenues of financing schemes
Memorandum items Reporting items
FS.RI.1 Institutional units providing revenues to financing schemes
FS.RI.1.1 Government
FS.RI.1.2 Corporations
FS.RI.1.3 Households
FS.RI.1.4 NPISH
FS.RI.1.5 Rest of the world
FS.RI.2 Total foreign revenues (FS.2 +FS.7)
FS Related items
FSR.1 Loans
FSR.1.1 Loans taken by government
FSR.1.2 Loans taken by private organisations
FSR.2 Aid in kind at donor value
Key indicators
• CHE by revenue of scheme
– Transfers from Government current expenditure
(internal and external origin)
– Social insurance contributions
– Prepayment (compulsory and voluntary)
– Other domestic revenue
– Direct foreign transfers (in cash and in kind)
Key indicators (ctd) • CHE by origin of the revenue: Memorandum
Items: institutional units – Government current expenditure (internal and external)
– Corporations – Households – NPISH – RoW
• CHE by revenue for schemes: cross-classified HF – Government schemes & Compulsory health insurance – Voluntary schemes – Oops – ROW

Structure of the classification
• The classification refers to the mechanism directly channeling the resources to the scheme
– e.g. transfers by government from foreign origin
• Additional layers can be added to existing categories when needed
Example:
• FS.1.1 Internal transfers and grants – FS 1.1.2 Internal transfers and grants from general
revenues
– FS.1.1.3 Internal transfers and grants from earmarked tax

Multiple financing paths example of government flows
Revenue-Expenditure
• FS may show discrepancies between revenues received and payments made
• Although a difference can be estimated for revenue and expenditure, the full assessment of a financial condition of a scheme results of more information (EU and GFS rules)
• Important to identify the revenue used – The RMNCH and other initiatives require revenue
amounts related to the expenditure by schemes
– "how was the burden of the expenditure distributed?"

Public – Private mix
• "Compulsory" revenues are treated as governmental. – "Compulsory" reflects a public intervention resulting
in a regulated financial structure – Compulsory = public intervention
• "Voluntary" implies a discretionary use of resources, out of regulation, out of government direct intervention – Private decision on use of resources – It involves both public and private resources – Voluntary = non - governmental

• From the perspective of financing scheme:
– participation in a scheme is compulsory or voluntary
• From the perspective of the revenue:
– payment of revenue is compulsory or voluntary
• In SHA 2011 ownership is not the basis of analysis
Public – Private in SHA 2011
The role of foreign resources
• Most resources are released by agencies acting as residents (SNA): – A focus on local health, staying one year or more
– With cooperation and interaction with MoH (Paris agreements)
• Foreign agencies without minimal or not interacting nationally, are not residents: RoW
• Example: – WHO HQ – WHO country office

About loans • Loans are not a real increase of the funds
(they have to be repaid + they have a cost), they are reported as memorandum item
• Loans are recorded only on the amount used during the accounting period
• Debt forgiven as well as low interest loans (concessional and other quasi-grants) are recorded as RoW (FS.7)

About transfers • In kind transfers are included and valued at
current market prices. E.g. foreign technical assistance. The viewpoint of originators can be recorded below the line.
• Conditional health cash transfers are recorded as governmental, because recipient households cannot make a discretionary use of them
• Non conditional health transfers are excluded. They are recorded when spent / used by households on health care.

General Government – Public Sector
• Government = GFS public sector includes public corporations & other non budgetary entities
• National labels may not be equivalent to those in SHA 2011: – One "insurance" can nest several schemes – A label "insurance" can represent a governmental scheme
• NPIs are classified as part of government based on criteria (not only one, not all needed):
– Government appoints officers – Contractual agreements with government – Degree of financing by government – Other provisions (discretionary use of funds for other purposes) – Risk exposure

Coverage of the Government Sector reflected in reports
Source: GFS 2011 manual

Data Collection issues • Preparatory work for SHA 2011 framework • Data may still be collected from financing agents
• when there is third party involvement: shift from agent (SHA 1.0) to scheme (SHA 2011).
• Only health components are kept, and should be treated by scheme
• Surveys and other instruments need to be adjusted – added complexity and detail to the surveys/records to
cover from revenues to allocation, fund management and agents involved
– special effort to cover more relevant funds (size, role) – need of detail to allow the consolidation of flows.

Intermediation
• Agencies with no active role between allocation resources to health and paying for health services may operate, frequently to transfer resources
• Their intervention frequently involves an overhead or transaction costs important to capture
• Accounting for them is proposed based on documented reports or allocation based on administration costs
Estimation issues • Earmarked revenue is recorded directly to schemes.
• Non-earmarked revenue of government is allocated through a budgetary decision
• Non earmarked revenue has to be registered considering information available. – In the absence of any additional information, one
approach is to assume the same distribution of the health system spending: all spending had a revenue
– Or same distribution of allocation on health as in the state budget as a whole: e.g. foreign revenue non earmarked for health
Keep in mind the objectives: e.g. to identify distribution of the burden of revenue used

Guidelines / References
In addition to SHA 2011, PG, SHA 1.0
• Some revenue guidelines on the IMF Government Finance Statistics Manual (including compilation guide for developing countries)
Exercise
• Identify the revenue modalities existing in your country and mark those more relevant
• Continue the exercise for schemes and list the related revenue types for each scheme
• Identify their potential data sources
• Which revenues can be considered public, which private and which are external?
















