The Neglected Child Patrick Ayre email: [email protected]web: http://patrickayre.co.uk Graham Hopkins email: [email protected]http://www.rightthing.co.uk/ With Elli Mackenzie and Adrian Pleater
“One third of long-term cases examined on this inspection were characterised by drift and delay, resulting in failure to protect children from continued neglect and poor planning in respect of their needs and future care”.
Family history not attended to
Lack of focus on the child
Little evidence of long term support to enable lasting change
Non-compliance not addressed
LSCBs lacked data and strategic plan
Sir Walter Monckton
“I have pointed out where I think that the two authorities failed separately in their duty to take adequate care of these two children. There was also a lamentable failure of communication of material facts between the two.”
Sir Walter Monckton – “Report on the circumstances which led to the boarding out of Dennis and Terence O’Neill…”
May 1945
Terry O’Neill
NEGLECT
Neglect is the persistent failure to meet a child’s basic physical and/or psychological needs, likely to result in the serious impairment of the child’s health or development. Neglect may occur during pregnancy as a result of maternal substance abuse. Once a child is born, neglect may involve a parent or carer failing to: provide adequate food, clothing and shelter protect from physical and emotional harm or danger ensure adequate supervision ensure access to medical care or treatment.
It may also include neglect of, or unresponsiveness to, a child’s basic emotional needs.
NEGLECT
Neglect is the persistent failure to meet a child’s basic physical and/or psychological needs, likely to result in the serious impairment of the child’s health or development. Neglect may occur during pregnancy as a result of maternal substance abuse. Once a child is born, neglect may involve a parent or carer failing to: provide adequate food, clothing and shelter protect from physical and emotional harm or danger ensure adequate supervision ensure access to medical care or treatment.
It may also include neglect of, or unresponsiveness to, a child’s basic emotional needs.
NEGLECT
Neglect is the persistent failure to meet a child’s basic physical and/or psychological needs, likely to result in the serious impairment of the child’s health or development. Neglect may occur during pregnancy as a result of maternal substance abuse. Once a child is born, neglect may involve a parent or carer failing to: provide adequate food, clothing and shelter protect from physical and emotional harm or danger ensure adequate supervision ensure access to medical care or treatment.
It may also include neglect of, or unresponsiveness to, a child’s basic emotional needs.
NEGLECT
Neglect is the persistent failure to meet a child’s basic physical and/or psychological needs, likely to result in the serious impairment of the child’s health or development. Neglect may occur during pregnancy as a result of maternal substance abuse. Once a child is born, neglect may involve a parent or carer failing to: provide adequate food, clothing and shelter protect from physical and emotional harm or danger ensure adequate supervision ensure access to medical care or treatment.
It may also include neglect of, or unresponsiveness to, a child’s basic emotional needs.
NEGLECT
Parents who neglect their children basically just don’t know any better because of their own poor upbringings. If we send them to a family centre for Parental Skills training, all will be well.
NEGLECT
Parents who neglect their children basically just don’t know any better because of their own poor upbringings. If we send them to a family centre for Parental Skills training, all will be well.
IF ONLY!!....
NEGLECT
So neglected children who come into care may be a bit thin, a bit dirty, badly in need of seeing a doctor or dentist, maybe a bit wild.
But we can place them with foster carers for a bit of looking after, a bit of TLC, a bit of structure and everything will be fine. The children will absolutely love it and will immediately start to thrive. Simple really!
NEGLECT
So neglected children who come into care may be a bit thin, a bit dirty, badly in need of seeing a doctor or dentist, maybe a bit wild.
But we can place them with foster carers for a bit of looking after, a bit of TLC, a bit of structure and everything will be fine. The children will absolutely love it and will immediately start to thrive. Simple really!
IF ONLY!!....
Neglect
Behavioural
Constant hunger
Constant tiredness
Frequent lateness or non-attendance at school
Destructive tendencies
Neglect
Low self-esteem
Neurotic behaviour
No social relationships
Running away
Compulsive stealing or scavenging
Neglect
Physical
Poor personal hygiene
Poor state of clothing
Emaciation, pot belly, short stature
Poor skin and hair tone
Untreated medical problems
Significant harm
Harm is defined by Children Act 1989:
ill-treatment (including sexual abuse and, by implication, physical abuse)
impairment of health (physical or mental) or development (physical, intellectual, emotional, social or behavioural)
The child's basic needs
basic physical care
affection
security
stimulation of innate potential
guidance and control
responsibility
independence
Why do parents neglect?
We need to understand the interaction between:
3 Ns: Nurture, Nature, Now
Circumstantial factors and fundamental factors
Why do parents neglect?
Circumstantial Poverty
Particular relationships
Lack of skill/knowledge
Temporary illness
Lack of support
Environmental factors
Fundamental
Lack of parenting capacity
Deep seated attitudinal/behavioural/ psychological problems
Long term health issues
Entrenched problematical drug /alcohol use
Forms of neglectHowe identifies 4 types of neglect
Emotional neglect
Disorganised neglect
Depressed or passive neglect
Severe deprivation
Each is associated with different effects and implications for intervention
(Howe, D (2005) Child Abuse and Neglect, Basingstoke: Palgrave Macmillan)
Emotional neglect Sins of commission and omission
‘Closure’ and ‘flight’: avoid contact, ignore advice, miss appointments, deride professionals, children unavailable
However, may seek help with a child who needs to be ‘cured’
Intervention often delayed
Associated with avoidant/defended patterns of attachment
Emotional neglect: parents Can’t cope with children’s demands:
avoid/disengage from child in need; dismissive or punitive response
Children provided for materially but there is a failure to connect emotionally
More rules; everyone has a role and knows what to do.
Parents may feel awkward & tense when alone with their children.
Emotional neglect: children
When attachment behaviour rejected: Learns that caregiver’s physical and emotional
availability is reduced when emotional demands are made;
Caregiver most available when child is showing positive affect, being self-sufficient, undemanding and compliant;
Reverse roles, “false brightness” to care for/ reassure parent.
Emotional neglect: children
Frightened, unhappy, anxious, low self-esteem
Withdrawn, isolated, fear intimacy and dependence
Precocious, ‘streetwise’, self-reliant
Emotional neglect: children
May show compliance to dominant caregivers but anger and aggression in situations where they feel more dominant.
May learn that power and aggression are how relationships work and you get your needs met
Behaviour increasingly anti-social and oppositional
Brain development affected: difficulties in processing and regulating emotional arousal
Disorganised neglect Classic ‘problem families’
Thick case files
Can annoy and frustrate but endear and amuse
Chaos and disruption
Reasoning minimised, affect is dominant
Feelings drive behaviour and social interaction
Worker may feel agenda co-opted by family’s immediate needs
Disorganised neglect: carers Feelings of being undervalued or emotionally
deprived in childhood so need to be centre of attention/affection
Demanding and dependant with respect to professionals
May be regarded as overwhelmed but amenable to services
Crisis is a necessary not a contingent state
Associated with ambivalent/coercive patterns of attachment
Disorganised neglect: carers
Cope with babies (babies need them) but then…
Parental responses to children
– unpredictable and insensitive (though not necessarily hostile or rejecting).
– driven by how the parent is feeling, not the needs of the child
Lack of ‘attunement’ and ‘synchronicity’
Disorganised neglect: children Anxious and demanding
Infants: fractious, fretful, clinging, hard to soothe
Young children: attention seeking; exaggerated affect; poor confidence and concentration; jealous; show off; go to far
Teens: immature, impulsive; need to be noticed leads to trouble at school and in community
Neglectful parents feel angry and helpless: reject the child; to grandparents, care or gangs
Depressed neglect
Classic neglect
Material and emotional poverty
Homes and children dirty and smelly
Urine soaked matresses, dog faeces, filthy plates, rags at the windows
A sense of hopelessness and despair (can be reflected in workers)
Depressed neglect: carers Often severely abused/neglected: own parents
depressed or sexually or physically abusive
May seem unmotivated, mild learning disability
Learned helplessness in response to demands of family life;
Stubborn negativism; passive-aggressive Have given up both thinking and feeling
Depressed neglect: carers Listless and unresponsive to children’s needs
and demands, limited interaction
Lack of pleasure or anger in dealings with children and professionals
No smacks, no shouting, no deliberate harm but no hugs, no warmth, no emotional involvement
No structure; poor supervision, care and food
Depressed neglect: children
Younger the child, more debilitating the effects
Lack interaction with parents required for mental and emotional development
Infant: Incurious and unresponsive; moan and whimper but don’t cry or laugh
At school: isolated, aimless, lacking in concentration, drive, confidence and self-esteem but do not show anti-social behaviour
Severe deprivation
Eastern European orphanages, parents with serious issues of depression, learning disabilities, drug addiction, care system at its worst
Children left in cot or ‘serial caregiving’
Combination of severe neglect and absence of selective attachment: child is essentially alone
Severe deprivation: children Infants: lack pre-attachment behaviours of smiling,
crying, eye contact
Children: impulsivity, hyperactivity, attention deficits, cognitive impairment and developmental delay, aggressive and coercive behaviour, eating problems, poor relationships
Inhibited: withdrawn passive, rarely smile, autistic-type behaviour and self-soothing
Teach parents to engage emotionally with their children.
Must be highly structured as neither parent or child know how to interact normally & spontaneously.
Fear of affect – need clear rules & roles
Disorganised neglect: case management
Logic would argue for warding off crises for a while so that families can be taught to organise their lives, but…
Family may want to have needs met, but cannot delay gratification or trust logic and planning;
Without intense demands associated with crises, have no way of being important to others;
Will CREATE new crises.
Disorganised neglect: case management
Feelings must be addressed
Need a structured, predictable environment with no surprises where:
– There are rewards for clear, direct, and undistorted communication of feelings and accurate cognitive information about future outcomes
– Family can learn the value of compromise
Teach parents how to use cognitive information to regulate feelings (without denying them)
Depressed neglect: case management
Involves much more than teaching appropriate parenting
All family members must learn that their behaviour has predictable and meaningful consequences
Teach that it helps to share feelings with empathetic others.
Depressed neglect: case management Our standard approaches don’t work Threats / punitive approaches particularly
ineffective:– Parents don’t believe they can change so don’t
even try.– Even most reasonable pressure results in “shutting
down” / blocking out all info. Parent education – may be ineffective because
judgment impaired and gains not transferable.
Depressed neglect: case management
These families need: Long term involvement Supportive approach Responsiveness to family’s signals and needs BUT these need to be balanced with a
recognition of the children’s needs. (How long is too long? How much is too much?)
Depressed neglect: infants and children
Must experience responsive and stimulating environments that also provide human comfort for a few hours each day.
The longer the child is exposed to helplessness, the more intense and longer the intervention needed to remedy the situation.
Depressed neglect: parents
Must learn appropriate ways to show their feelings– Practice smiling, laughing, soothing– May be mechanical at first– Genuine feelings will emerge with repetition
As parents learn to show their feelings, the child’s responsiveness will increase; virtuous spiral
Severe deprivation: case management
Highly unlikely to be in the child’s best interests to remain in the environment which caused the harm;
It is probable that the child and new carers will require substantial therapeutic and emotional support;
Significant challenges often persist despite a move to a caring and predictable environment.
Chronologies
Chronologies:
as a
matter
of
fact
Hamzah Khan
11 September 1970
Amanda Hutton is born
1986/87
Hutton begins her long relationship with Aftab Khan, Hamzah’s father.
13 February 1989
Tariq Khan born - Hutton and Khan’s first child.
…and so begins the pattern of avoiding contact with health services.
28 May 1996
First record of police being called to a domestic violence incident involving Hutton being attacked by Khan.
Early 2005
Hutton misses an ultrasound scan at hospital arranged for Hamzah
June 17, 2005Hamza Khan born. Nothing reported to cause concern
June 23, 2005 Hamzah seen by a midwife at home. Nothing to cause concern
July 7, 2005 Hamzah is seen by health visitor for “birth visit”. Nothing to cause concern
6 October 2005 Hutton discusses options for getting away from Aftab Khan with PC Whittaker, an experienced domestic violence officer with West Yorkshire Police. 11 October 2005Hutton is diagnosed with post-natal depression. She is prescribed anti-depressants.
October 2005Health visitor sees Hutton after three unsuccessful attempts. Health Visitor says the door was slammed in her face.
24 December 2005Hutton’s mother dies.
15 February 2006The health visitor again attempts to visit Hutton and leaves a calling card
August 2006
Following further attempts by the health visitor to see Hutton. Health visitor contacts the social services – child protection team - for advice
October 2005Health visitor sees Hutton after three unsuccessful attempts.
15 February 2006The health visitor again attempts to visit Hutton and leaves a calling card
August 2006Following further attempts by the health visitor to see Hutton. Health visitor contacts the social services
August 2006
A registrar of births visits Hutton at home and notes Hutton had a “puffed up” eye and smelt of alcohol.
7 September 2006Hutton goes to her GP – needs drink to cope 19 September 2006 Hamzah is registered with a GP 15 months after his birth but never attends the practice or gets any of his jabs. 23 November 2006 - A social worker attends Hutton’s house and speaks to her.
December 2006
One of the children reports domestic violence to police, saying both Hutton and Khan have assaulted him.
Police try and arrange accommodation with Children’s Social Care who are unable to find a placement. The child returns home.
Shortly after this Amanda Hutton calls police for help but by the time they arrive, Aftab Khan has left the house.
February 2007Amanda Hutton attends A&E with bruising and chest pains following an assault at home. She says she has separated from Aftab Khan.
She would attend A&E on three further occasions – once being taken there by ambulance after it had been called to the house by one of the children.
22 February 2007 Hutton attends GP surgery for last time
April 2007Hutton’s social worker contacts health visitor to say Hutton has had a “change of heart”
May 2007Older child makes another complaint of physical and emotional abuse. Social Care Services interpret this as “teenage angst”.
He is accommodated for two nights in an emergency accommodation but returns home to the family.
May to November 2007Appointments are made for a range of immunisations for Hamzah. Not one is kept.
7 December 2007 Police call to Hutton’s house after a “dropped” 999 call. Hutton also requests to see a specific police officer whom had previously supported her. But by the time the officer makes contact Hutton says she no longer wants to meet.
13 June 2008Hutton and her family are the subject of a Multi-Agency Risk Assessment Conference (MARAC). A health visitor contacts school about attendance issues with some of Hutton’s children August 2008 Another MARAC discusses Hutton’s refusal to engage with an organisation that supports women affected by domestic violence
4 December 2008
Aftab Khan assaults Hutton.
A police officer visits and notes nothing of concern relating to children in the house. The police officer told the court she had a list of all the children in her notebook but could not remember whether this meant she had actually seen all of them.
This incident leads to Khan’s only conviction for attacking Hutton and the couple split.
9 December 2008
Aftab Khan is interviewed by police about the incident on 4 December. He admits assault. But he also raises concerns about the welfare of Hamzah – says police should check on him as he is being neglected. Khan claims he will contact social services.
December 2008
Hutton and all her children except Qaiser, who is now 22, move house in Bradford following her split from Khan. A judge grants a no-contact order, forcing Aftab Khan to stay away from Hutton
January 2009Another MARAC meeting hears that Hutton is now working with a domestic violence support charity. Notes that Hamzah has not seen a GP since birth.
19 January 2009A worker for a domestic abuse support charity visits Hutton in her new home and reports nothing of concern.
17 February 2009PC Whittaker visits Hutton at home in connection with the ongoing prosecution of Aftab Khan.
16 March 2009Hutton and her children move to a larger house in Bradford.
21 April 2009A different police officer conducts a “welfare check” on Hutton’s house after some of the children are not picked up after school.
9 June 2009Aftab Khan given a community order by magistrates after admitting battery following the incident on 4 December 2008.
September 2009Hamzah would normally have started school (although there is no legal requirement until his fifth birthday in June 2010). Hutton answers questions about his absence by claiming he is in Portsmouth with an Uncle
October 2009The children and Amanda Hutton are removed from the register of the GP practice.
14 December 2009Hutton said Hamzah has been taken ill but describes him as poorly rather than seriously unwell. 15 December 2009Hamzah dies at a time unknown while Hutton is at Morrison’s supermarket. At 11.05pm a call is made from Hutton’s phone to Pizza Hut. At 11.07pm a call is made from Hutton’s phone to the Spicy Delight Indian take-away.
2010
Correspondence in 2010 between health visitors, early childhood services, children’s social care and education centres on the difficulties in seeing the children. The health visitor realises that the younger children have not been in contact with health services or registered with a GP.
Amanda Hutton again says the children are living elsewhere.
11 March 2011
One of Hutton's neighbours alerted social services to her concerns about the family.
21 September 2011Uniformed police officers gain access to Amanda Hutton’s home. Hamzah’s decomposed body is found in a cot in Hutton’s bedroom.
Five of his siblings, aged between five and 13, are removed from the house, which is described as being in “appalling squalor”.
6 March 2013
Hutton is charged with the manslaughter of Hamzah.
24 July 2013Hutton admits child cruelty in respect to five of her children and preventing the burial of a corpse at Bradford Crown Court. Her son, Tariq, admits preventing the burial of a corpse. • 18 September 2013 Hutton goes on trial at Bradford Crown Court accused of manslaughter. • 30 September 2013Hutton is brought to court by police but is too drunk to give evidence and her defence is delayed.
October 2014
Hutton is convicted of manslaughter and is sentenced to 12 years in prison, and three years for child cruelty – to run concurrently.
Capturing chronic abuse
Judging the quality of care is an essential component of any assessment but how well do we do it?
Judgements subjective and prone to bias
Intangible: Difficult to capture and compare
High threshold for recognition
Neglect is a pattern not an event
The pattern of neglect: atypical
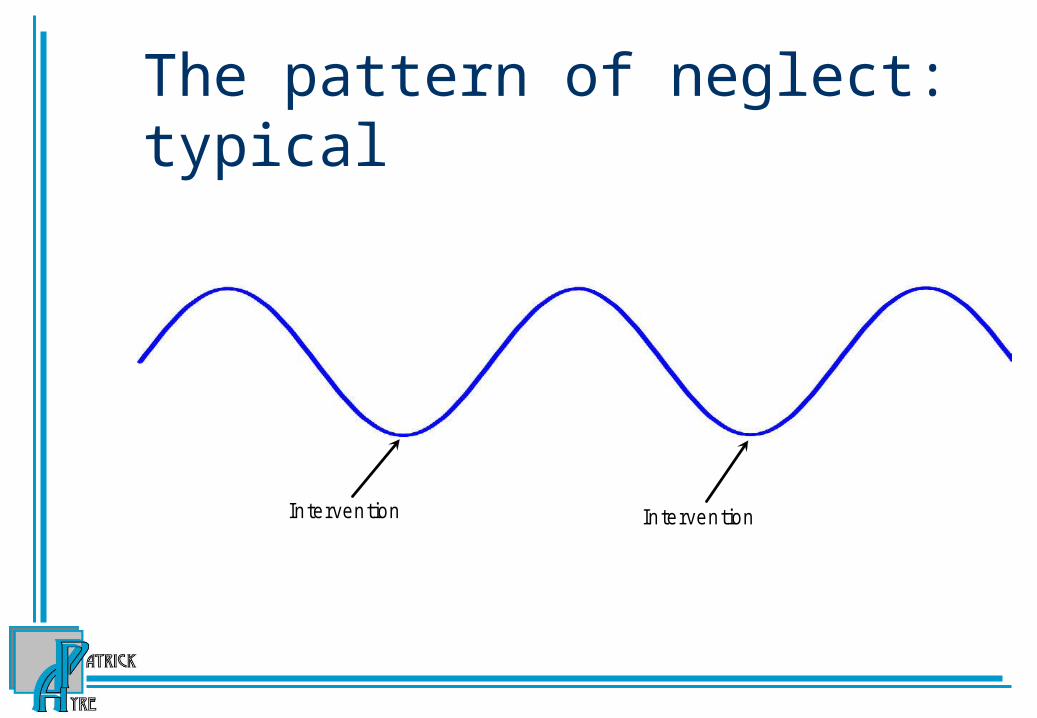
The pattern of neglect: typical
Intervention Intervention
The pattern of neglect
'G ood enough' level
Intervention Intervention
The pattern of neglect
Intervention Intervention
'G ood enough' level
Intervention ceases
The pattern of neglect
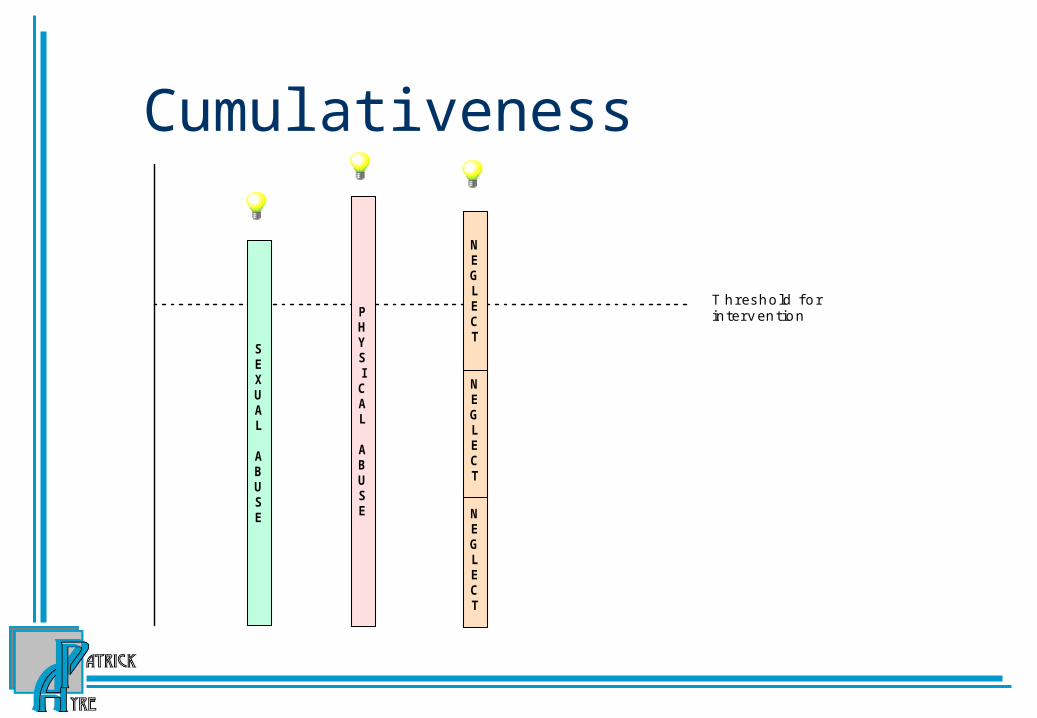
Cumulativeness
T h r es h o ld f o rin te r v en tio n
SEXUAL
ABUSE
PHYSICAL
ABUSE N
EGLECT
NEGLECT
NEGLECT
Failure of cumulativeness
T h r es h o ld f o rin te r v en tio n
SEXUAL
ABUSE
PHYSICAL
ABUSE
NEGLECT
NEGLECT
NEGLECT
NEGLECT
What’s the problem?
Chronic abuse and the principle of cumulativenessFiles very long and badly structured
Patterns missed and ‘chronic abuse’ overlooked
The problem of proportionality
Acclimatisation (case, agency and geographical)
More assessment issues Picking out the important from a mass of data Interpretation Decoyed by another problem False certainty; undue faith in a ‘known fact’ Discarding information which does not fit First impressions/assumptions Too trusting/insufficiently critical Distinguishing fact/opinion
Department of Health (1991) Child abuse: A study of inquiry reports, 1980-1989,
HMSO
Assessment Pitfalls
When faced with an aggressive or frightening family, professionals are reluctant to discuss fears for their own safety and ask for help
Attention is focused on the most visible or pressing problems and other warning signs are not appreciated
Parents’ behaviour, whether co-operative or uncooperative, is often misinterpreted
Not enough weight to information from family friends and neighbours
Not enough attention is paid to what children say, how they look and how they behave
In Cleaver, H, Wattam, C and Cawson, P Assessing Risk in Child Protection, NSPCC, 1998
Child centred assessment
The purpose of assessment is to understand what it is like to be that child or young person (and what it will be like in the future if nothing changes)
Assessment pitfalls
Rule of optimism
Start again syndrome
Natural love
Cultural relativism
Too much
not enough
Brain development
At birth our brains are only 25% developed By age 3, a child’s brain has reached almost 90%
of its adult size and has accomplished 80% of its total development.
The growth in each region of the brain largely depends on receiving stimulation.
This stimulation provides the foundation for learning.
Experience Affects the Structure of the Brain
Brain development is “activity-dependent” Every experience excites some neural
circuits and leaves others alone Neural circuits used over and over
strengthen, those that are not used are dropped resulting in “pruning”
Poor integration of hemispheres and underdevelopment of the orbitofrontal cortex
Difficulty regulating emotion, Lack of cause-effect thinking, Inability to recognize emotions in others, Inability to articulate own emotions, Incoherent sense of self and
autobiographical history Lack of conscience.
Other physiological issues
Serotonin: emotional stability and feeling good
Malnutrition: cognitive and motor delays, anxiety, depression, social problems, and attention problems
MyelinationSensitive periods (infancy & attachment)
Emotional development
Sensitive period for emotional development: up to 18 months
Shaped primarily by the way in which the prime carer interacts with the child
Emotional deficits harder to overcome once the sensitive window has passed.
How often do we intervene assertively at this point?
Building a child
Building a child is like building a house, each new level built on the one below. If the lower levels are unsound, no amount of tinkering with the upper floors will make it stable.
A final thought
“We are guilty of many errors and many faults but the worst of our crimes is abandoning our children, neglecting the fountain of life. Many of the things we need can wait. The child cannot. Right now is the time his bones are being formed, his blood is being made, and his senses are being developed. To him we cannot answer 'Tomorrow.' His name is 'Today.'”