78
The Republic of Malawi Ministry of Health P.O BOX 30377 LILONGWE 3, MALAWI THE MALAWI COVID-19 VACCINE DEPLOYMENT PLAN The Expanded Programme of Immunization (EPI) 02 February 2021
The Republic of Malawi
Ministry of Health
P.O BOX 30377
LILONGWE 3,
MALAWI
THE MALAWI COVID-19 VACCINE DEPLOYMENT PLAN
The Expanded Programme of Immunization (EPI)
02 February 2021

2 | Page
Executive Summary
The vaccine deployment plan remains a strategic document which helps with the roll out of
COVID19 vaccine and ensures a clear roadmap for resource mobilization which includes extra
doses of the COVID19 vaccines. The deployment plan will provide a stepwise approach to
building confidence to the COVAX team, WHO, UNICEF and Gavi including multilateral and
bilateral partners that vaccine doses and resources are being put to good use and more lives will
be saved from this pandemic. Malawi is a member of the COVAX facility arrangement.
Malawi has a population of 18,898,441 (NSO 2021) in which 58% are those above 15years of age.
The COVAX Facility arrangement will target 20% of the country’s population, which is 3,779688.
The MAITAG recommended that the target of 20% will comprise of health workers, social
workers, the elderly, and people with comorbid health conditions such as diabetes, hypertension
and those with HIV/ AIDS, mentally ill and disabled including the humanitarian groups like
refugees. The immunization program will adopt and modify the WHO micro planning tools for
covid-19 vaccination.
The Malawi Government will engage in bilateral and multilateral discussions with relevant
partners to lobby for additional vaccines beyond the 20% from the COVAX facility. The Pharmacy
Medicines and Regulatory Authority, a member of the WHO and AVAREF has already put in
place the mechanisms for expedited approvals of the new vaccine. It will also rely on stringent
regulatory authorities, the WHO Emergency Use Listing (EUL). The manufacturer
indemnification is already approved and submitted to the COVAX team
COVID-19 vaccine introduction will be planned and coordinated under the Ministry of Health new
vaccine introduction structures. The structures include The EPI Sub Technical Working Group
(EPI-TWG), the National Task Force (NTF), the Malawi Immunization Technical Advisory Group
(MAITAG) and the District Task Force at subnational level. The country will mobilize funds and
identify funding mechanisms to support the roll out of the vaccine at national and subnational
levels. The Ministry of Finance, MoH and partners will ensure availability of resources with
support from the Presidential Task force and the office of the COVID19 coordinator at the office
of President and Cabinet (OPC).
3 | Page
The country has cold chain capacity to as much as 45% volume space following the successful
Cold Chain Equipment Optimization from Gavi. We have an available transport and logistics
system across all districts such that vaccines will be deployed without delays.
A comprehensive Communication, Social Mobilization and Risk Communication Plan to increase
knowledge and positive attitudes, and ultimately demand for the COVID-19 Vaccine has been
developed. This will be coupled with community engagement so that misinformation is corrected
and myths dispelled. The target groups have been segmented to ensure that no group is left without
information that facilitates informed choice for equity and access. The country shall use multiple
channels of communication including Interpersonal Communication (Face to Face Orientation,
interactive SMS’s, and community dialogues), Mass media (radio/TV programs & spots) and
Community Mobilization (Theatre for Development).
The National Vaccine Deployment Plan is costed at MWK1, 224,265,790.08 ($1,654,413.23) in
order to be operationalized. The demand creation and Social Mobilization is going to cost
MWK1000000000.00 in the first one year including 20% target population by the COVAX
Facility. These resources will be mobilized through the Malawi Government in collaboration with
its partners and NGOs. This cost excludes procurement of vaccines doses for the remaining 60%
of the total target population
Finally a robust paper based monitoring and evaluation has been planned which includes registers
and vaccination cards with special identity marks will be designed to monitor performance and
impact. A vaccine safety committee at both National and district level will be engaged to monitor
Adverse Events Following Immunization. A toll free number will be used to communicate any
safety concerns.

4 | Page

5 | Page
Contents
Executive Summary 2
List of Figures 8
List of Tables 9
Acknowledgements 10
Abbreviations 12
1.0 Introduction 15
1.1 Background 15
1.2 Health care services in Malawi 15
1.3 COVID-19 disease burden in Malawi 16
1.5 COVID-19 vaccine introduction 20
1.6 Lessons learned from influenza A H1N1 and other relevant vaccines 20
1.7 Goal and Objectives of COVID-19 Vaccine Deployment and Vaccination Plan 21
1.7.1 Goal 21
1.7.2 Objectives 21
2.0 Regulatory Preparedness 22
2.1 Pharmacy and Medicine Regulatory Authority (PMRA) expedited review procedure 22
2.1.2 Importation 23
2.1.3 Lot release 23
2.1.4 Risk management plan and safety surveillance 23
3.0. Planning and Coordination of the vaccine introduction 24
3.1 Development of a COVID-19 vaccine deployment Plan (NDVP) 27
3.2 Meetings 27
3.3 Microplanning 27
Resource Mobilization and funding 28
5.0 Identifications of target groups 29
5.1 Priority groups for COVID-19 Vaccination 30
5.2 Vaccination of populations outside the 20% priority target group 34
6.0 Vaccine delivery strategies 34
6.1 Health and social workers 34
6.2 Comorbid patients 35
6.3 The elderly 35

6 | Page
6.4 Refugees, Asylum seekers and Internally Displaced Persons (IDPs) 35
6.5 Mapping of eligible persons 36
6.6 Vaccination Supervision. 36
6.7 Infection prevention 36
7.0 Preparation of Supply Chain and Management of Health Care Waste 36
7.1 Strengthening Supply chain and human resource capacity 39
7.1.1 Vaccine Procurement 39
7.1.2 Distribution 40
7.1.3 Effective Vaccine Management Assessment (EVMA) 41
7.1.4 Human Resource capacity for Vaccine handling 41
7.1.5 Vaccine Stock Control and Accountability 42
7.2 Waste Management and reverse logistics 42
8.0 Human resource management and training 43
8.1 Training 44
9.0 Vaccine acceptance and uptake (Demand creation) 45
9.1 community engagement 45
9.2 Demand creation 46
9.3 Participants groups/target audiences 49
9.3.1 The primary audience 49
9.3.2 The secondary audience 49
9.3.3 The tertiary audience 50
9.4 Channels of Communication 50
9.5 Risk Communication strategy 52
9.6 Campaign Positioning 59
9.7 Phased Implementation of Risk and Crisis Communication 60
9.8 Monitoring, Evaluation and Documentation 61
9.9 Coordination 61
10.0 Vaccine safety monitoring 62
11.0 Immunization monitoring systems 66
12.0 COVID-19 vaccination Surveillance 67
13.0 Post Introduction Evaluation (PIE) 68
14.0 Lessons Learnt 68
Annexes 70

7 | Page
Annex 1 Risk Communication and Crisis plan 70
Annex 2 Proposed Set of Core Indicators for Monitoring & Evaluation 73
Annex 3 Timeline of Activities 76
Annex 3 demand creation and social mobilization and community engagement budget 78

8 | Page
List of Figures
Figure 1Distribution of COVID19 cases over time ....................................................................18
Figure 2 Map showing distribution of COVID19 cases in Malawi .............................................19
Figure 3 Coordination Flow Diagram ........................................................................................25
Figure 4 Age and sex distribution of COVID-19 deaths in Malawi as of 17 Jan 2021 ................31
Figure 5 Proportion of Age Groups According to Malawi Population and Housing National
Census 2018 ..............................................................................................................................31
Figure 6 Figure 7Malawi AEFI reporting workflow and timelines .............................................65

9 | Page
List of Tables Table 1 Malawi COVID-19 Situation by 25th January, 2021.................................................................. 17
Table 2 Summary of target and priority group ........................................................................................ 33
Table 4 Demand creation objectives ...................................................................................................... 48
Table 5 Summary of the different media and platforms to be used. ......................................................... 51
Table 6 Summary of Risk Communication Strategy ............................................................................... 52
Table 7 Proposed Crisis Responses on Anticipated Issues ...................................................................... 54
Table 8 Table 6 Risk and crisis communication phased implementation table ........................................ 60
10 | Page
Acknowledgements
The development of a National Vaccine Deployment Plan had been a huge task where only
massive commitment could help. The COVID-19 situation has made it very difficult and the work
very tedious, however the EPI-Sub Technical Working Group deserves a pat on their back. We
would therefore acknowledge the following contributors individually but also at partnership level;
MOH: Dr Storn Kabuluzi (DPHS-Chair Sub-TWG), Dr. Mike Nenani Chisema (DDPHS-EPI),
Mrs. Temwa Mzengeza Phiri, Mrs. Brenda Mhone, Mr. Mphatso Mtenje, Mr. Dennis Mwagomba,
Mr. Evans Mwendo Phiri, Mrs. Rhoda Chado, Mrs. Doreen Ali, Mrs. Janet Guta, Dr Annie Mwale,
Dr Jones Kaponda Masiye, Mr Mabvuto Thomasi, Mr. Alvin Chidothi Phiri, Mrs Pakwanja Twea,
Mr. Humphreys Nsona, Mr. Williams Lapukeni, Dr. Lawrence Nazimera, Captain Regina
Chigona(MDF) PMRA: Mr. Mphatso Kawaye, Mrs. Cecilia Sambakunsi and Mr. Anderson
Ndalama. OPC: Dr. Bridon Mbaya (COVID-19 Coordinator) COM: Dr Atupele Kapito Tembo,
Dr Juliana Kanyengambeta Mubanga (DHSS, Mchinji) Mr Davie Kulemera (CMST) Dr Sandy
Chiume Kayuni (KCH)
Partners and their representatives include WHO: Dr Susan Kambale, Dr Boston Zimba and Dr
Randy Mungwira, UNICEF: Dr Ghanashyam Seth, Mr. Steve Macheso, Mr. Chancy Mauluka,
JSI: Mrs. Hannah Hausi, Mr. Patrick Omar Nicks MLW; Dr Donnie Mategula PATH; Mr.
Rouden Nkisi ONSE: Simon Ntopi, Village Reach: Matthew Ziba UNHCR: Dr Kingsley
Ojeikere MHEN: Mr George Jobe World Bank: Dr Collins Zamawe USAID: Mrs Chifundo
Kuyeli
Colleagues please receive our heart-felt thanks to the wonderful contributions made to the whole
process with a special mention of partners like JSI, WHO and UNICEF.
,

11 | Page

12 | Page
Abbreviations
AEFI Adverse Events Following
AESI Adverse Event of special Interest
CCPF Chipatala Cha Pa Foni
CHAM Christian Health Association of Malawi
cMYP Comprehensive Multi Year Plan
CCEOP Cold Chain Equipment Optimization platform
CSOs Civil society Organizations
DVS District Vaccine Store
EMA European Medical Agency
EU European Union
EHP Essential Health Care Package
EPI Expanded Programme on Immunization
EVMA Effective Vaccine Management Assessment
FDA Food and Drug Administration
GBV Gender Based Violence
GVAP Global Vaccine Action Plan

13 | Page
HES Health Education Services
HIV Human Immuno-deficient Virus
HSSP Health Sector Strategic Plan
HSIS Health System and immunization Strengthening
HPV Human Papilloma Virus
KAP Knowledge, Attitude and Practices
KCH Kamuzu Central Hospital
MAITAG Malawi Immunization Technical Advisory Group
M & E Monitoring and Evaluation
MISA
MOH
Media Institute of Southern Africa
Ministry of Health
MOU Memorandum of Understanding
NTF National Task Force
NDVP National Vaccine deployment Plan
NGO Non-Governmental Organizations
NVS National Vaccine Store

14 | Page
PLWHIV People Living With HIV
PPE Personal Protective Equipment
PMRA Pharmacy Medicine Regulatory Authority
PHIM Public Health Institute of Malawi
POE Point of Entry
PIE Post Introduction Evaluation
RVS Regional Vaccine Store
SMT Stock Management Tool
SOP’s Standard Operating Procedures
SLA’s Service Level Agreements
VAR Vaccine arrival Report
VVM Vaccine Viral Monitor
WHO World Health Organization

15 | Page
1.0 Introduction
1.1 Background
Malawi is a landlocked country, located in sub-Saharan Africa. It is bordering Tanzania to the
north, Mozambique to the east and south, and Zambia to the west. The country has an area of 118,
500 sq. km, of which one-fifth is water surface, largely dominated by Lake Malawi. According to
National Statistical Office (NSO) 2018 projections, the country’s population in 2021 is 18,898,441
and most people live in the rural areas (84%). The country is divided into 29 health districts located
in three geographical regions: Northern, Central and Southern regions. (Malawi COVID-19
contingency plan, 2020).
1.2 Health care services in Malawi
In Malawi health care services are delivered by both the public and the private sectors. The public
sector includes all facilities under the MoH, Ministry of Local Government and Rural
Development, the Ministry of Forestry, the Police, the Prisons, and the Army. The private sector
consists of private for profit and private not for profit providers, mainly Christian Health
Association of Malawi (CHAM). The public sector provides services free of charge while the
private sector charges user fees for its services. There are currently 977 health facilities in Malawi
comprising 113 hospitals, 466 health centers, 48 dispensaries, 327 clinics, and 23 health posts.
These health facilities are managed by the government (472), CHAM (163), Private (214), NGOs
(58) and company (69) {Malawi SPA- 2013-14}. CHAM is a not for profit health services provider
and is the biggest partner for the MoH. It provides health services and trains health workers through
its health training institutions. CHAM facilities charge user fees for other medical services.
However, the Government of Malawi established Service Level Agreements (SLAs) with CHAM
facilities regarding the government-funded provision of free maternal and child health services
(Health Sector Strategic Plan (HSSP), 2011-2016).
In line with the HSSP III, health services are delivered at different levels: namely: primary,
secondary, and tertiary. These different levels are linked to each other through an elaborate referral
system that has been established within the health system. At the primary level, services are
delivered through health posts, dispensaries, maternity, health centers and community and rural

16 | Page
hospitals. At community level, health services are provided by a community-based cadre, HSAs.
District hospitals constitute the secondary level of health care. They are referral facilit ies for both
health centers and rural hospitals. They also service the local town population offering both in-
patient and out-patient services. CHAM hospitals also provide secondary level health care. The
provision and management of health services has since been devolved to Local governments
following the Decentralization Act (1997). The tertiary level comprises central hospitals: these
provide specialist referral health services for their respective regions. Specialist hospitals offer
very specific services such as obstetrics and gynecology. There are currently 4 central hospitals in
the country.
1.3 COVID-19 disease burden in Malawi
The country registered its first COVID-19 case on 2nd April 2020 and is currently experiencing a
second wave of the COVID-19 pandemic. As of 25 January 2021, a total of 19, 987 confirmed
COVID-19 cases and 518 deaths were reported in Malawi. Of these cases 1,951 are imported and
18,036 are locally transmitted. The case fatality rate so far is at 2.6%. See Table 1 below for details
on 25th January and Figure 1 for distribution of cases since April 2020.

17 | Page
Table 1 Malawi COVID-19 Situation by 25th January, 2021
Parameter Statistic
Cumulative confirmed cases 19, 987
Number of active cases 12,479
New confirmed cases in the past 24 hours 592
Cumulative deaths 518
Cumulative recoveries 6, 780
Cases lost to follow-up 134
Cases still under investigation for the outcome 76
Cumulative samples tested 130, 006

18 | Page
Figure 1Distribution of COVID19 cases over time
The cases are spread across the whole country, but more in cities of Blantyre, Lilongwe and
Mzuzu, see map below.

19 | Page
Figure 2 Map showing distribution of COVID19 cases in Malawi

20 | Page
1.5 COVID-19 vaccine introduction
The introduction of COVID-19 vaccine is one of the preventive measures adopted by the
country to prevent and control COVID-19 pandemic. This has been the long-term management
and control of COVID-19 globally. It also aligns with the comprehensive Multi-Year Plan
(cMYP) for 2017-2021 which outlines the priorities of the immunization programme, which
includes new vaccine introduction. Globally the introduction aligns with the Global Vaccine
Action Plan (GVAP) goal number 4 “Develop and Introduce new and improved vaccines and
technologies”. The country was approved to participate in the COVAX facility arrangement
which is working on ensuring equitable distribution and access of COVID-19 vaccines
regardless of economic status among the countries across the globe. The facility will work to
procure and distribute vaccines targeting 20% of the total population with other support
launched in the Technical Assistance plan and the Cold Chain Equipment support. It is expected
that countries will work to provide for operational cost as well as looking for more resources to
procure more doses to Carter for the remaining 80% populace. The country is engaging other
potential donors to support with the procurement of more vaccines and funding the operational
costs.
1.6 Lessons learned from influenza A H1N1 and other relevant vaccines
The country has provided life course vaccines which targeted other populations besides infants
e.g., H1N1 in 2010, Cholera vaccine from 2013 and Human Papilloma Virus (HPV) vaccine from
2019. The following lessons were learnt which will be applied to the COVID-19 vaccine to reach
out to more targeted populations:
● Collaboration and coordination amongst key ministries and cooperating partners are key
for the successful vaccine delivery.
● Timely availability of data capturing tools is critical for data management and timely
reporting.
● Timely communication to the public via newspaper and radios press is key to creation of
high vaccine demand.
● Timely quantification, procurement and delivery of vaccines & injection devices contribute
to the successful implementation of HPV vaccination.
● Capacity building is key to quality service delivery.
21 | Page
● Some high-risk individuals in the priority groups refused to get the vaccine, however, some
individuals demanded the vaccine even if they were not in the prioritized groups.
● Identification of eligible individuals, based on the set priority groups, is critical to avoid
vaccinating non eligible individuals to ensure adequacy of the already inadequate vaccines.
● The strategy deployed should ensure that more targeted individuals are reached.
1.7 Goal and Objectives of COVID-19 Vaccine Deployment and Vaccination Plan
1.7.1 Goal
To contribute to the reduction of COVID-19 morbidity and mortality in Malawi through an
efficient and effective vaccination program.
1.7.2 Objectives
1. To facilitate timely availability of COVID-19 vaccines in Malawi without compromising
proper regulatory decision-making.
2. To establish effective planning, monitoring and evaluation of COVID-19 vaccine
introduction readiness and deployment.
3. To identify and prioritize target populations for COVID-19.
4. To ensure available and efficient vaccination delivery strategies which ensures equity in
COVID-19 vaccine access and protects the vulnerable.
5. To procure and provide adequate quantities of COVID-19 vaccine and injection materials
of the right quality at the right time to all delivery points.
6. To create demand for COVID-19 vaccine through effective communication and
community engagement to increase acceptance and uptake for equitable vaccine access.
7. To provide for a clear plan for vaccine safety and monitoring of adverse events following
immunization and help to build and sustain public confidence in COVID-19 vaccination
and immunization in general.
8. To establish a monitoring and evaluation system to measure the performance of COVID-
19 vaccination including Post Introduction evaluation (PIE).

22 | Page
9. To stand in as a tool that Identifies and mobilizes resources for the rolling out of COVID-
19 vaccination.
2.0 Regulatory Preparedness
The objective is to facilitate the timely access of COVID-19 vaccines in Malawi while adhering to
the existing regulatory structures. The Pharmacy and Medicines Regulatory Authority (PMRA) is
a designated institution in Malawi with a mandate to regulate medicines including vaccines.
PMRA licenses all medicines that are marketed in Malawi and vaccines that are provided both in
public and private facilities. The process is easier if the product has received authorization by a
WHO listed country’s NRA. (https://www.who.int/medicines/regulation/sras/en/). This also
applies to all the vaccines that have received WHO prequalification including those that have
received WHO Emergency Use Listing (EUL
2.1 Pharmacy and Medicine Regulatory Authority (PMRA) expedited review
procedure
2.1.1 Registration
PMRA is able to conduct expedited review of the products which include vaccines. The process
usually takes approximately 15 days especially in an emergency setting. For the product to undergo
expedited review, it depends on the registration of the product. For the vaccine that has received
approval from WHO listed country’s NRA PMRA requires; evidence of registration in the
manufacturing country, assessment report from the NRA that approved the vaccine and lot release
information from the manufacturing country. The same process occurs if the product that has
received WHO prequalification or WHO Emergency Use Listing.
While the product that has received authorization from NRA from the country that is not listed by
WHO, the PMRA endeavors to conduct a comprehensive review. This involves requesting for the
full dossier and conducting a full evaluation. In an emergency setting, they involve an expedited
process which takes approximately 90 days. If the product is approved in a country that has a
working agreement with MPRA, the PMRA will rely on the assessment report from that country’s
NRA.

23 | Page
There are times that PMRA participates in joint evaluation with other regional NRAs. For instance,
PMRA has ever participated in joint evaluation with AVAREF when they were evaluating RTS,
S vaccine for pilot use. There are no plans to have a joint review with AVAREF on COVID-
19 vaccines. Sometimes the country’s NRA conducts joint evaluation with ZAZIBONA, which is
the regulatory authority of a group of countries within the SADC region. PMRA has been invited
to participate in joint evaluation with ZAZIBONA on one of the COVID-19 vaccines.
2.1.2 Importation
When the product has been procured, it is the duty of the procuring institution to arrange with
the clearing agent. In most instances, the vaccines that have WHO PQ or WHO EUL, UNICEF
procures and ensures that they have identified the clearing agent. PMRA provides import licenses
to the procuring institution, in this case to UNICEF.
2.1.3 Lot release
The country does not have the capacity to conduct lot release. It relies on the lot release data from
the manufacturing country. This is documented in the import license that PMRA provides to the
procuring institution when they are importing the vaccine (the guideline is still in draft form but
this is the practice). The manufacturer of the COVID-19 candidate that the country will receive
will have to provide the lot release so that it is included in the import license to be issued by PMRA.
2.1.4 Risk management plan and safety surveillance
The PMRA put in place measures which ensure that all the activities that market authorization
holders planned as part of their risk management plans are implemented. Also, they continue
monitoring the safety of the vaccine in routine use. There is a medicines safety and quality
monitoring committee that works hand in hand with EPI when there are issues regarding the safety
of the vaccine.
No regulatory challenges are expected during authorization of COVID-19 vaccine?. Considering
the accelerated nature of the COVID-19 vaccine, an enhanced safety surveillance program will be
necessary. PMRA has now implemented a functional pharmacovigilance system. PMRA-Malawi
is now the 135th Member of the WHO International Drug Monitoring Program.
24 | Page
Using the Reliance approach, 15 working days are adequate for the Medicines Committee to meet
and consider the registration of the product. Please note that the Ministry of Health sits in this
committee of the Board of Directors. The national regulator or authority has clarified the
requirements and documents needed for regulatory approvals of COVID-19 vaccines which
include; Product Dossier from manufacturer and Product sample from manufacturer while the
requirements and documents needed to import COVID-19 vaccines include; Import permit from
PMRA and summary lot protocols for lot release from the manufacture. The current average time
to issue an import permit or reject is 2 days.
The waiver for lot release is available and, in that case, goods are immediately allowed entry into
the country if there is available a valid import permit (Max 1 day). The normal regulatory approach
to new vaccine registration before introduction is only through product dossier review (either
locally or relying on dossier review reports from stringent regulatory authorities such as USFDA
or EMA or WHO prequalification). For biological products e.g. vaccine, testing is a very
challenging venture and usually only done when a product quality problem is identified after
introduction (e.g. when severe AEFIs are observed). The capacity to test biological products is
also quite limited in this part of Africa
3.0. Planning and Coordination of the vaccine introduction
Planning and coordination are a critical element of COVID-19 vaccine introduction. This function
shall ensure that adequate support and funding for COVID-19 vaccine are secured and utilized
prudently. The objectives include ensuring strong linkages across all the stakeholders for resource
mobilization, efficient allocation and utilization of resources and robust governance and
coordination across all relevant stakeholders.

25 | Page
Figure 3 Coordination Flow Diagram
COVID-19 vaccine introduction will be planned and coordinated through existing immunization
structures of the EPI program. The structures include The EPI Sub Technical Working Group (EPI
TWG), National Task Force (NTF) and the Malawi Immunization Technical Advisory Group
(MAITAG). EPI TWG is the equivalent of the Immunization Coordinating Committee (ICC),
which ultimately reports to the Essential Health Care package (EHP) Technical Working Group
of the MoH. It is responsible for planning, coordination, implementation, and monitoring of the
roll out of the COVID-19 vaccine. The EPI sub-TWG is a multidisciplinary platform with
representation from the MOH, other sectors, development partners, implementing partners,
academia, and Civil Society Organizations (CSOs), Non-Governmental Organizations (NGOs),
among others. Decisions to introduce a vaccine are made by the sub TWG after discussing the
burden of the disease and advantages of the vaccine, which follows consultation of the Malawi
Immunization Technical Advisory Group (MAITAG) for advice to the Ministry. Based on
Ministry of Health
Malawi Immunization
Technical Advisory Group
EPI sub Technical Working
Group
EPI District Task Force
National Task Force

26 | Page
MAITAG advice, the senior management of the ministry approves or rejects the introduction of a
vaccine.
The EPI sub TWG discussed the introduction of COVID-19 vaccine in the country and it was
approved. Afterwards MAITAG was engaged for advice and they recommended the introduction
and proposed the priority target group for the vaccine based on the local and international data
which was available. Finally, the Ministry of Health approved the introduction of COVID-19
vaccine in the country.
As a way of operationalizing and integration into existing processes, the COVID-19 vaccine roll
out activities will be included in the COVID-19 response plan as one of the strategies to be used
for the prevention and control of the pandemic. The Presidential task force will provide oversight
to the implementation of the vaccine deployment plan aided by the Ministry of Health and the
COVID19 Coordinating office at the Office of the President and Cabinet.
The NTF under the EPI sub TWG has been established to coordinate the actual implementation of
COVID-19 vaccine introduction. This task force includes stakeholders from CSOs, the private
sector, development partners, and NGOs and Malawi government and public services departments.
The NTF will guide on issues of:
Service Delivery.
Vaccine, Cold Chain & Logistics
Demand Generation & Communication.
Monitoring and Evaluation.
Determination of eligibility and proof of Vaccination.
Monitoring Vaccination impact
Monitoring vaccine safety
At subnational level, a replica structure called the District Task Force (DTF) will be established to
coordinate and guide implementation of district level activities. See the diagram below:
Six key activities to strengthen planning and coordination for COVID-19 vaccination, include;
conduct meetings across EPI governance structures (Sub-TWG, MAITAG, NTF, DTF, SMT and
EHP), develop a National Vaccine Deployment Plan ( NDVP), prepare detailed budgets for all

27 | Page
preparatory activities and actual vaccination, mobilize resources for the operationalization of the
vaccination, develop micro plans, conduct supportive supervision (pre-introduction and during
introduction) and conduct post mortem meetings and documentation of lessons learnt.
3.1 Development of a COVID-19 vaccine deployment Plan (NDVP)
A COVID-19 vaccine introduction plan has been developed by the EPI program with support from
partners. This is in line with the guidelines provided by WHO and MAITAG. The EPI sub TWG
drafted the NDVP which has been approved by the senior management of the ministry before
submission to COVAX.
3.2 Meetings
The sub TWG meets frequently to make decisions on the way forward on the introduction of
COVID-19 vaccines. The frequency of MAITAG meetings also increased to assist with the
decisions on target groups and vaccine candidates to be used in the country, as evidence unfolds.
NTF and DTF meetings will also roll out to guide on the planning and implementation of
preparatory activities at zonal and district level respectively.
3.3 Microplanning
The microplanning will be done by adapting the existing micro planning tool for Supplementary
Immunization Activities (SIA). The variables will include facility catchment population, priority
target groups, supply chain and logistics requirements, and prevention materials items like masks,
handwashing facilities and sanitizers.
Estimation of frontline health care workers and the social workers will be done by using the Human
Resource staff return which will be made available by the public Human resources offices. These
target numbers will provide the basis for calculation of logistic and supply requirements for the
delivery of the vaccines. The elderly will be estimated by using the 5% estimate of the total
population. The adapted micro planning tool will be sent out to the districts for population by
health facility and then aggregated at district level. 4.0 Resources and Funding
The COVID-19 vaccine introduction will require resources which include human resource and
capacity building, vaccines, cold chain equipment and funds for operational activities. These
activities will include training of health workers, supervision, printing of guidelines, monitoring

28 | Page
tools, communication materials and incentives for vaccinators. The vaccine and CCE requests
were submitted to Gavi for support with the vaccines and cold chain equipment procurement.
Resource Mobilization and funding
The National Vaccine Deployment Plan is costed at MWK1, 224,265,790.08 ($1,654,413.23) in
order to be operationalized. The demand creation and Social Mobilization is going to cost
MWK1000000000.00 in the first year of rolling out COVID-19 vaccine including 20% of target
population by the COVAX Facility. The country will mobilize funds and identify funding
mechanisms to release and distribute funds to lowest levels for operations. This cost is with
exception of procurement of doses beyond the COVAX Facility. (See Annex 2 and 3)
WHO and UNICEF are providing both technical and budgetary support in planning and
preparing the delivery of the vaccines. Malawi is erecting additional two cold rooms at the national
vaccine store with support from UNICEF under Gavi HSIS funding. John Snow Inc. is equally a
core partner supporting with technical assistance to the preparatory activities. We have been
assured of more resource mobilization in the country to facilitate the introduction.
Other potential funding sources are:
Loans (WB, AU)
Donations
Government contribution
COVAX facility
COVID-19 response budget
Bilateral and multilateral organizations
While looking at issues of resources and funding, the following points have to be considered in
order to ensure a successful vaccine introduction;
Estimation of financial and human resources needed to conduct the deployment and
vaccination operations in the designated points and in the required number of days.
Identification of funding mechanisms in collaboration with relevant stakeholders.

29 | Page
Finalization of the cost micro-plans for vaccination including plans for other relevant
components such as demand generation, risk communications and safety surveillance and
establishing a mechanism to release and distribute funds to lowest levels for operations.
A deliberate resource mobilization strategy will be developed to facilitate the execution of the
deployment plan but also increase transparency and accountability to the Malawi citizenry. Both
the public and the private including the faith based organization will be reached out in order to
mobilize resources and reduce any inequalities in the distribution of the vaccines. Where possible,
revolving funds will be introduced to facilitate acquisition of extra doses for all the people in the
country at the earliest time possible and beyond COVAX arrangement.
The Malawi government through the Ministries of Health and Finance will be engaging the
Bilateral and Multilateral and development banks in discussion for the possibility of grants and
loans. The loans will focus both procurement of extra doses and providing for the operation costs
so that no vaccines sit idle without use.
The EPI program will ensure leveraging of resources from the existing Health Systems
Strengthening Grant Gavi support. The areas include vaccine collection and distribution,
conducting National and district Task force meetings since Malawi will conduct IPV and HPV
routinization around this year 2021. We will also be conducting the Measles Rubella
supplementary immunization activities in October 2021, all these will provide an opportunity for
resource leveraging.
5.0 Identifications of target groups
Target group identification is aimed at getting the eligible groups for COVID-19 vaccination in an
equitable manner through prioritizing the recipient groups. This is in anticipation that the initial
supply will not be adequate to reach the whole population. It is therefore important to prioritize
groups to receive the initial vaccine supply from COVAX facility as well as subsequent vaccines
that will be made available to the country. The identification and prioritization is based on COVID-
19 morbidity and mortality data as stipulated below.

30 | Page
5.1 Priority groups for COVID-19 Vaccination
In the first phase, the COVAX Facility will target 20% of the country’s population, which is
3,779688 (NSO, 2021 population projection). The COVID_19 has hit every country in the world
and this has pressed a lot of demand than the suppliers would handle and prioritization becomes
key in protecting the high risk groups. The MAITAG agreed to prioritize health workers and social
workers, the elderly, and people with comorbid health conditions such as diabetes, hypertension
and HIV that increase the risk of developing severe COVID-19 disease and death. A buffer will
also be set aside for humanitarian deployment. The first 3% within the initial 20% phase will target
health workers. The decision was based on the WHO recommendation to target groups based on
local epidemiologic information and an assessment of risk factors but also vaccine supply situation
in the country. Health workers include all health professionals and supporting staff providing care
to the patients in hospitals, community health workers and other support staff within the hospital
settings in direct contact with clients during service provision. This will include all health workers
in both public and private facilities. These will comprise 3% of the population. However, in case
of short supply of the vaccine, the priority will be health workers who are in hospitals that are
treating COVID-19 patients. These will comprise 2% of the health workers.
The social workers to be targeted in the first phase will include the police, soldiers, and prison
warders, who according to their work, are always in direct contact with groups of people and
mostly difficult to keep social distance. These comprise 2.4% of the population.
Although all age groups are at risk of contracting COVID-19 disease, older people are at increased
risk of developing severe illness and even death, if they contract the disease due to physiological
changes that come with ageing and potential underlying health conditions. The elderly who will
be targeted are those above 60 years since COVID-19 data for the first wave, Figure 3 below, has
shown that this is the age category that has most of the deaths.
The other priority group to be considered will be those who are mentally ill and disabled as they
can hardly understand and follow the COVID19 preventive measures despite not falling into any
of the categories. The country NVDP will ensure that the prioritization and targeting processes

31 | Page
will be ongoing as we continue to monitor the epidemiological trends of the disease and the
availability of the vaccine doses.
Figure 4 Age and sex distribution of COVID-19 deaths in Malawi as of 17 Jan 2021
The Projected population of >60yrs is 944,922, which is 5% of the population [1], see Figure 4
below. Additional age groups will be added as the vaccine supply situation improves.
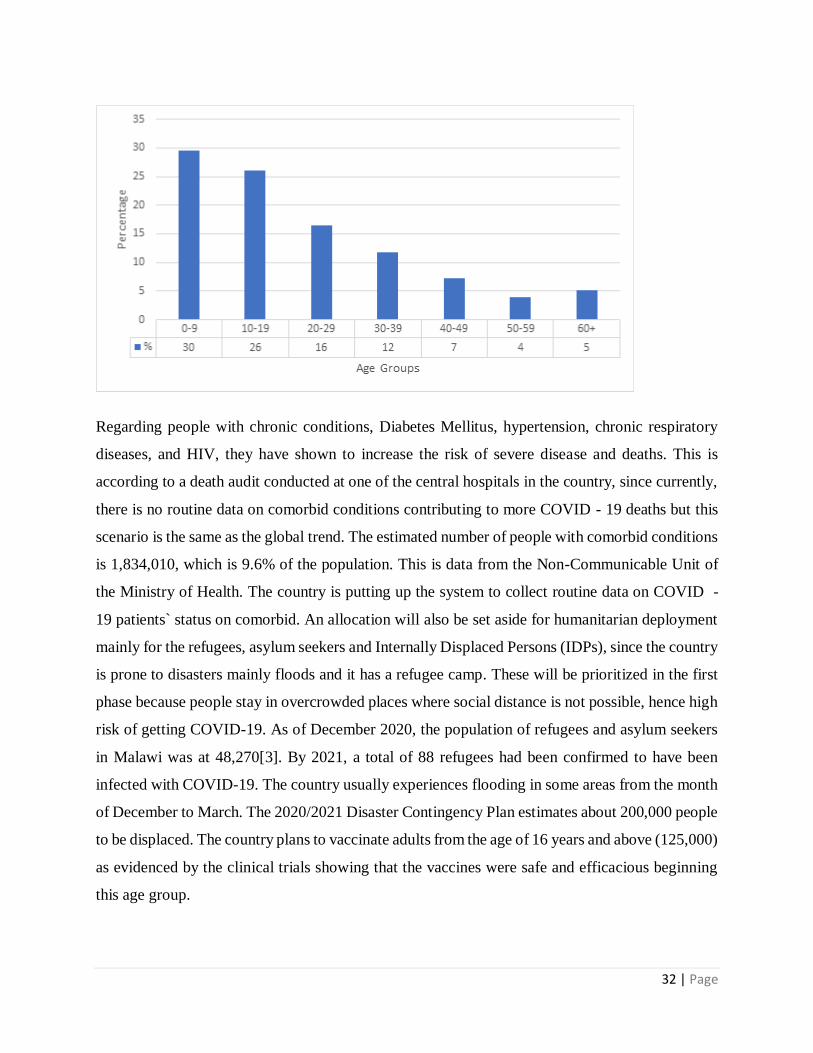
Figure 5 Proportion of Age Groups According to Malawi Population and Housing National
Census 2018
32 | Page
Regarding people with chronic conditions, Diabetes Mellitus, hypertension, chronic respiratory
diseases, and HIV, they have shown to increase the risk of severe disease and deaths. This is
according to a death audit conducted at one of the central hospitals in the country, since currently,
there is no routine data on comorbid conditions contributing to more COVID - 19 deaths but this
scenario is the same as the global trend. The estimated number of people with comorbid conditions
is 1,834,010, which is 9.6% of the population. This is data from the Non-Communicable Unit of
the Ministry of Health. The country is putting up the system to collect routine data on COVID -
19 patients` status on comorbid. An allocation will also be set aside for humanitarian deployment
mainly for the refugees, asylum seekers and Internally Displaced Persons (IDPs), since the country
is prone to disasters mainly floods and it has a refugee camp. These will be prioritized in the first
phase because people stay in overcrowded places where social distance is not possible, hence high
risk of getting COVID-19. As of December 2020, the population of refugees and asylum seekers
in Malawi was at 48,270[3]. By 2021, a total of 88 refugees had been confirmed to have been
infected with COVID-19. The country usually experiences flooding in some areas from the month
of December to March. The 2020/2021 Disaster Contingency Plan estimates about 200,000 people
to be displaced. The country plans to vaccinate adults from the age of 16 years and above (125,000)
as evidenced by the clinical trials showing that the vaccines were safe and efficacious beginning
this age group.

33 | Page
Table 2 below summarizes the numbers, proportions and strategies for the priority target
populations in order of priority.
Table 2 Summary of target and priority group
Target population (in
order of priority)
Number of
additional
individuals to be
vaccinated
Priority targeted
delivery strategy for
this population
Total cumulative % of
vaccines as a
percentage of
population
1. Front line
Health care
workers
( bedside and
COVID19
attendants)
377969 (2%) Workplaces 2%
2. Other health
workers (other
wards,
vaccinators)
188,985 (1%) Workplace 3%
3. Social workers 302,375 (1.6 %) Workplaces 4.6%
4. Population with
Comorbid
conditions
1,814,250 (9.5%) Health facilities 14.1%
5. The Elderly
(>60 years)
944,922 (5%) Health facilities and
communities
19.1%
6. Humanitarian
deployment
173,270 (0.9%) In camps 20%

34 | Page
5.2 Vaccination of populations outside the 20% priority target group
The Malawi Government is engaged in bilateral discussions with relevant groups to lobby for
additional vaccines beyond the 20% from the COVAX facility. As more and more vaccines
become available, the second phase, which will vaccinate beyond the 20%, will reach the
remaining priority groups such as essential workers (teachers/ lecturers), the new cohort of the
elderly from the age of 40 years, social employment groups unable to social distance (commercial
sex workers, vendors and individuals working at supermarkets, shops, financial institutions like
banks), people living in squatter areas, prisoners and travelers.
The third phase will include age groups of high risk to transmit disease (16 to 49 years). The
priority groups will continue to be assessed till everyone eligible is reached with the vaccine in the
subsequent phases.
The country is planning to introduce the COVID-19 vaccine in March 2021 for phase 1
implementation. The introduction will be countrywide since the COVID-19 cases are distributed
in all the districts in the country. The subsequent phases will be at a four months interval, with the
second phase coming in August 2021 and the third phase in January 2022. However the phases
will be determined as more vaccine doses become available on a daily basis.
6.0 Vaccine delivery strategies
This section outlines the delivery strategies that will ensure good accessibility and utilization of
the COVID-19 vaccine including the hard to reach areas. Table 2 above also shows the strategy to
be used for each priority group. This will highlight issues of access by each target group,
supervision, and infection prevention.
6.1 Health and social workers
These health workers shall be reached and vaccinated at their workplaces. At each health facility
a COVID-19 vaccination point shall be available for the entire day to enable all health workers at
the institution and social workers in that area access the service. This arrangement will enable
health workers to get vaccinated whilst ensuring that services are not disrupted. We have engaged

35 | Page
the Human Resources Management offices to provide health and social workforce data through
stuff return aggregates and physical counting of the employees. This data will facilitate supply
chain and logistics including management of the delivery strategy so that each and every frontline
worker is reached with information and the actual vaccine. The health workers will be registered
on the day of actual immunization. A vaccine data card will be provided to each vaccinated
individual so they can produce when they come back for their second dose and for their record.
6.2 Comorbid patients
COVID-19 vaccination shall be integrated with the health services such as Non-Communicable
Diseases (NCD) clinics in both public and high volume private health facilities and immunization
outreach clinics will also be used to ensure that all persons with comorbid conditions are reached
and vaccinated. Health facilities will provide numbers of comorbid patients in their microplans
and these are expected to be vaccinated in health facilities (NCD clinics) where they normally
access their treatments and at outreach clinics where routine immunizations are conducted. Days
will be set aside for their vaccinations or integrated during their special clinics, where possible.
The vaccine carriers and cold boxes will be used to transport vaccines to the outreach sites while
the fridges will keep vaccines at the static clinic.
6.3 The elderly
Vaccination stations for COVID-19 vaccine shall be set up in hospitals, health centers, clinics both
public and private near the Outpatient Care department to ensure that all the elderly easily access
the services. In addition to existing immunization sites such as static and outreach clinics,
temporary sites will be used to reach out and vaccinate the elderly in areas that are far from the set
routine immunization sites. The number of elderly persons in each health facility will be estimated
by using a 5% percent estimate of the catchment population
6.4 Refugees, Asylum seekers and Internally Displaced Persons (IDPs)
In Malawi all documented refugees and Asylum seekers reside at Dzaleka refugee camp in Dowa.
COVID-19 vaccination sites shall be arranged and set up at Dzaleka refugee camp health center

36 | Page
including outreach sites within the camp to reach out those that cannot easily make it to the health
center.
6.5 Mapping of eligible persons
We shall rely on available data to map out for the elderly and those that are handicapped otherwise
the majority will be expected to come for vaccination at the nearest static or outreach clinic.
6.6 Vaccination Supervision.
District and National supervisors will conduct supportive supervision during vaccination. This will
aim at ensuring quality service provision.
6.7 Infection prevention
All vaccination sites will follow immunization protocols (SOPs) for COVID-19 infection
prevention measures which are used in all immunization sessions to ensure continuation of
immunization services. These include use of PPEs by all vaccinators, social distance, hand
washing, and use of sanitizers. The EPI program with guidance from WHO has developed a
Standard Operating Procedure which is currently being used for routine Immunization amidst
COVID - 19 pandemic, as such COVID-19 vaccination will use the same SOPs. The overall
gazetted COVID-19 restrictions and IPC guidelines developed by the Quality Department of the
Ministry of Health will equally be used.
7.0 Preparation of Supply Chain and Management of Health Care Waste
The Malawi immunization supply chain is a constellation of four levels of vaccine and axillary
storage facilities, processes, transport, and human resource. National Vaccine Stores (NVS) is the
primary store for vaccine and injection materials. The country uses both pull and push strategies
to move vaccines from National Vaccine stores to service delivery points. The supply chain
arrangement is meant to ensure that all delivery points have reliable supply of vaccine and injection
materials at the right time and in adequate quantities.
In Malawi, Vaccines enter the country through the Kamuzu International Airport in Lilongwe and
are readily moved to NVS for inspection and storage. Injection materials are shipped by sea and

37 | Page
enter the country through Malawi’s main entry borders of Mwanza and Dedza districts. The
injection materials are then transported to the NVS warehouse for inspection and storage. Vaccine
and injection materials are collected from the NVS to regional stores. Districts collect vaccines
and injection materials from the regional stores. The districts keep vaccines for a month, during
which vaccines are distributed to all the health centers where they are provided to beneficiaries.
The NVS has a net positive storage capacity of 57,144 liters and negative storage capacity of 10,
256 liters. The negative cold chain storage capacity requirement for routine vaccines at National
vaccine stores is at 5,691.42 liters and the positive storage is at 31,575.99 liters, representing 55%
occupancy proportion for both negative and positive storage. The regional stores in the North and
Southern Region, have positive storage volume of 19,048 liters and negative storage capacities of
10,256 liters and the central regional store has 9,524 liters. The cold chain capacity currently
available is adequate to accommodate and support roll out of new vaccines, including COVID-19
vaccine. The COVID-19 vaccine will require 36725 liters including a buffer of 5% should we
manage to get doses enough for the 20% population. The MoH is adding two Walk in Cold rooms
at the National Vaccine store equivalent to 19048litres. This is with support from UNICEF.
The country is implementing the 5-year GAVI supported Cold Chain Equipment Optimization
Platform (CCEOP), a strategy that supports countries to procure vaccine cold chain equipment.
Through the grant, the country has procured and installed 106 (69 replacements and 37 extension)
and 203 (105 replacements and 98 extension) Solar Directed Drive (SDD) refrigerators in 2018
and 2020 respectively, and in 2021, a total of 260 refrigerators will be procured and installed. The
2021 implementation will install equipment at District Vaccine Stores (DVS) and various health
facilities to increase the cold chain space, this is in addition to equipping facilities which have
never had any Cold Chain Equipment (CCE). It is anticipated that this effort will increase the cold
chain space at district level.
Table 3 Summary Table of Point of Entry, Cold Chain Capacity of in-country fallback facilities

38 | Page
Storage
Condition
Airport of Entry (Kamuzu
International Airport) (L)
National
Vaccine Stores
(L)
Regional
Vaccine
Stores
District
Stores (L)
+2 to +8 16,900 57,144 47,620 26,759
-15 to -25 0 10, 256 20,512 1,604
Dry store
space
0 846 m3 108 m3
Existing vaccine cold chain equipment including the refrigerators at service delivery points shall
be used for storing COVID-19 vaccine. It is anticipated that the country shall obtain COVID-19
vaccine candidates that conform to current available cold chain conditions of +2-+8 degrees
Celsius. However, as more candidates become available, vaccines that can be kept at -15 to -25
degrees Celsius can also be accepted however we do not have negative storage beyond the National
Vaccine Store and makes it difficult to accommodate ultra-cold chain vaccines. Malawi has also
submitted a Cold Chain Equipment request to the COVAX facility for consideration. We would
like to expand our National vaccine stores and Regional vaccine stores with additional two Walk
in Cold Rooms and one WICR at the central and Northern Regional vaccine stores. We have also
asked for support for remote temperature control gadgets and extra cold boxes and vaccine carriers
to supplement our cold chain equipment. This will support us in the long-term should we have
COVID-19 vaccine routinized or any future pandemics of similar nature and magnitude.
The National Vaccine Store and the Regional Vaccine Stores uses remote temperature monitoring
devices as well as onsite monitoring mechanism using available Fridge Tag 2 and freeze Tag 2
while the districts and health centers use track through the use Fridge Tag 2 to record and monitor
temperatures. These have been very essential during transportation at all tier levels across the

39 | Page
country. We expect to benefit from this temperature monitoring technologies even for the COVID-
19 vaccines which among others may be without Vaccine Vial Monitor.
7.1 Strengthening Supply chain and human resource capacity
7.1.1 Vaccine Procurement
Vaccine and injection materials are procured through UNICEF and documentation for the same is
shared with the Ministry of Health/EPI prior to delivery of vaccines and injection materials. A
local clearing agent, is responsible for receiving and clearing vaccines and injection materials at
the point of entry, and transportation to the NVS. There are no notable challenges with this
available contractor as such we are confident of the continuation of similar services for COVID-
19 vaccines. The current Memorandum of Understanding (MoU) between the Ministry of Health
and Allied Freight shall be used to clear and transport COVID-19 vaccines and injection materials
from port of entry to the NVS.
Like any other vaccines, it is expected that upon arrival of COVID-19 vaccines, the country will
ensure that:
Pre-advice is shared with all relevant stakeholders before the arrival of vaccines and
injection materials.
Clearing agent has arranged for customs clearing and transportation from point of entry to
NVS.
Staff at national vaccine stores are ready to inspect and receive the vaccines and injection
materials
Vaccine arrival report is prepared and submitted to the UNICEF country office within 3
days following receipt of vaccines and our recent assessment on VAR had been above 95%
on time.
The WHO Stock Management Tool is being adapted to include COVID-19 vaccine, an Excel
based tool, is used to manage vaccine and axillary stocks, including stock control, tracking and
issuing. The SMT is available and used at NVS, the regional stores and the district vaccine stores.
The health facilities use the vaccine/injection materials stock management books that have all the
elements to track vaccine/injection materials transaction, including stock management of the

40 | Page
stocks. In addition, the system uses the requisition/request form, dispatch forms and the vaccine
arrival report. Accountability during distribution is all a critical element area that shall be
prioritized for the COVID-19 vaccine. During distribution, each batch of vaccine shall be
accompanied by the dispatch form, and upon arrival the receiving stores shall prepare and provide
the arrival report. The VAR is a tool that provides feedback on the status and quantities of vaccines
received. As the roll out continues, subsequent issues will depend on the requesting facilities to
provide the storage facility the requisition form of the vaccine and ancillaries
required.
7.1.2 Distribution
Vaccine cold boxes and carriers are used to maintain cold chains during distribution. Freeze tags
are placed in the vaccine box/carriers to enable vaccine handlers detect if vaccines are exposed to
freezing, so that necessary steps are taken to ensure that only potent vaccines are provided to
beneficiaries. The COVID-19 vaccine has no Vaccine Vial Monitors (VVM) to check vaccine
potency hence prudence in temperature monitoring.
The Malawi EPI, through the GAVI Health System and Immunization Strengthening (HSIS) grant
procured seven vaccine transportation trucks. The trucks are positioned at NVS and the regional
Stores and these help with distribution of vaccines and injection materials from the NVS to the
regional stores. Through the same grant, each district was provided with vehicles to assist vaccine
collection and distribution.
Vaccines and injection materials are transported using the trucks that the country with support
from GAVI procured for transportation of vaccine and injection materials. Vaccines are loaded in
cold boxes for transportation to different tier levels. The cold boxes are conditioned properly to
ensure that recommended conditions are maintained during transportation of the vaccines. Freeze
tags are put in the cold boxes to assist the officers to detect if the vaccines were exposed to freezing
during transportation.
COVID -19 vaccines shall be transported in cold boxes, freeze indicators shall also be placed in
the cold boxes to ensure that vaccine potent and we have enough quantities. The NVS and the

41 | Page
regional stores have already prepared space for storing covid-19 vaccine. The same shall also be
prepared at DVS.
7.1.3 Effective Vaccine Management Assessment (EVMA)
Malawi conducted the last EVMA in 2016 of which the primary, district and regional levels scored
above 80% for all the nine criteria. The National level scored 98% for vaccine arrival, 86% on
temperature, 100% on capacity, 835 on equipment, 100% on maintenance, 98% on stock
management, 93% on distribution, 96% on vaccine management and 96% on information and
support functions. However, some gaps were identified including lack of periodic temperature
record reviews, lack of alarms for some of the cold rooms at NVS, absence of fire management
protocols and extinguishers at all levels.
The country has been implementing some activities in the EVMA improvement plan since 2016
including institutionalizing temperature record reviews and installation of voltage regulators for
cold rooms at NVS, Regional Vaccine Store (RVS) and refrigerators at DVS. The country has
delayed conducting EVMA, as the one planned in 2020 was postponed to 2021 due to COVID-19
restrictions.
7.1.4 Human Resource capacity for Vaccine handling
The national and regional stores have officers who are responsible for managing vaccines and
axillaries, the cold chain equipment and accounting for the commodities. The district EPI
coordinators oversee vaccination activities in the district including management of vaccines at
district vaccine stores. They are supported by the cold chain technicians who repair cold chain
equipment and distribute vaccines. Although these teams can manage routine vaccines, there is a
need to build their capacity to adequately manage COVID-19 vaccines.
Malawi is a beneficiary of the Gavi Health System Strengthening grant now in year 3. Despite the
COVID-19 Challenges, the EPI program continues to conduct Vaccine Management training
targeting 9000 HSAs. So far one-third of the target number has been reached with the training. We
believe the objectives of this training will extend to COVID-19 vaccines.

42 | Page
We are expecting that the EPI team together with its partners will be responsible for training of
the health workers and the volunteers with regards to supply chain and logistics. These topics will
also be included in the facilitators manual and trainers slide deck for COVID-19 vaccines.
7.1.5 Vaccine Stock Control and Accountability
Stock control and accountability is one of the critical responsibilities of the immunization program.
There are several tools that help vaccine stock control and helps to account for the doses that the
country prepares and administers to the beneficiaries. The tools include the WHO Stock
Management Tool (SMT), vaccine and injection dispatch forms, the Vaccine Arrival Reports
(VAR), Vaccine Request forms and Vaccine and injection material stock books. The dispatch
forms are used during the shipping of vaccines and axillaries from one point to another in the
supply chain. Upon receipt of the commodities, documentation is done in the VAR, SMT (at NVS,
RVS and DVS) and Vaccine and injection materials stock books at health facilities. The batch
numbers and VVM status is documented in the tools to enable accountability and quality
monitoring. This process has been mainstreamed for all vaccines in the supply chain and it shall
also apply to COVID-19 vaccines, except for VVM.
Key elements to be addressed for successful COVID-19 deployment include:
Develop SOPs and share with all vaccine storage facilities.
Complete furnishment of the NVS to increase capacity.
Procure refrigerators to distribute to both districts and health facilities to increase storage
capacity, as the rolling out of the vaccine proceeds.
Develop new guidelines for management of COVID-19 wastes
Revise the distribution plan for vaccines, injection material to include COVID-19 vaccine
and axillaries and PPEs.
7.2 Waste Management and reverse logistics
Vaccination campaigns are known to generate wastes. Types of wastes include sharps, infectious
non-sharp wastes and IPC materials wastes e.g. gloves, masks, used syringes, and other injection
materials that have negative effects on communities and the health workers. The risk from wastes
generated during campaigns increases when temporary sites are opened in communities. Waste

43 | Page
management ensures that we do not pose any risk to both humans and the environment while
vaccinating the people. It is important that wastes are properly and categorically managed. The
EPI through the supply chain coordination team will facilitate collection of different wastes from
the vaccination sites to the designated incineration and disposal sites.
The NVS generates significant quantities of wastes from secondary packaging and packs that help
maintain the right conditions during transportation of vaccine and injection materials. These wastes
are shipped to pharma grade environmentally friendly incinerators located at Kamuzu Central
Hospital (KCH) in the central region and Queen Elizabeth Central Hospital in the south where they
are properly incinerated and disposed of. In addition, all waste generated at service delivery points
including used syringes and vials are largely disposed of by incineration at the district hospital
level. We are planning to use the same structures to dispose of waste that will be generated during
the management of COVID-19 vaccine.
The EPI program will be responsible for ensuring that all vaccines and vaccine devices which have
been used are recalled back to the National Vaccine stores. These will be reallocated or should
they show signs of not being potent, then disposal will be planned with nearest incineration facility.
A budget has been set aside to support this process and it is a common practice even during
supplementary immunization activities SIA.
8.0 Human resource management and training
Availability of human resources is critical in the introduction of the new vaccine. The EPI
Programme is under the directorate of Preventive Health services in the Ministry of Health. At
National level, the programme is managed by the EPI Programme manager and assisted by his
deputy. In addition, there are officers responsible for Routine immunization, cold chain, supply
chain, surveillance for both diseases, and AEFI and Monitoring and Evaluation.
The country has five zones and in all the zones there are Routine immunization officers responsible
for the zone. In two zones where there are cold-rooms, we have Zonal Immunization Supply
Officers managing the cold rooms and supplies. There are 29 District EPI Coordinators managing
EPI services in districts and these are assisted by their deputies and district Cold Chain
Technicians.

44 | Page
About 80% of vaccinations in Malawi are done by the cadre of Health Surveillance Assistants.
Few nurses mainly Community Health Nurses and some clinicians also provide immunization
services. During vaccination sessions, the vaccinators are assisted by volunteers who support with
crowd control, and other integrated interventions e.g. growth monitoring. The COVID-19
vaccination will be handled by Health surveillance Assistants as usual who will be supervised by
the Community Health nurses, Public Health Officers at district including other cadres who will
be designated to undertake the supervisory role depending on training and availability. At the
health facility level, Nurses will be expected to vaccinate all the health and social workers at their
health facilities. The EPI coordinator at district level will be expected to coordinate all the activities
including management of supply chain and logistics.
All Health Promotion Officers will be expected to carry out demand creation activities in the
districts with support from the Health Education services unit of the Ministry of health. They will
be assisted by the Community Health Coordinator at district level who will be responsible for
community engagement activities which includes reaching to opinion leaders in order to facilitate
demand creation and dispel myths and misconception as well as misinformation.
The volunteers will be responsible for supporting the vaccinator including document management
and filing. They will also ensure clients are observing COVID-19 preventive measures and do any
other duty as assigned but not technical work.
8.1 Training
Training of Health workers is key to the successful introduction of any new vaccine in the
country. The country will develop a training plan to prepare for COVID-19 vaccine introduction
that includes key groups of participants, number of participants, training materials required. The
dates of training and key training partners and allocation of resources and overall planning.
National facilitators will train the District trainers who will carry out cascade training for health
workers and volunteers in their respective districts and central hospitals. The training will be
both in-person and virtual depending on Internet and network connectivity challenges, budgetary
constraints, and technical know-how on the use of virtual platforms for conducting
meetings/workshops.
45 | Page
Training materials are essential tools for successful implementation of every training in the
introduction of new vaccines. In preparation of the COVID-19 vaccine introduction, different
training materials such as field manual, operational manual and training decks will be developed,
printed, and distributed in all the districts to guide training and used as reference materials. These
guidelines are being developed by adapting the generic materials provided by WHO. National
supervisors will supervise the district training sessions and district trainers will supervise the
orientation of community health volunteers to ensure high quality of training at all levels.
It is expected that the COVID-19 training will be rolled out immediately as the National Vaccine
Deployment Plan is submitted which is the third week of February prior to arrival of the first
consignment of the COVID-19 vaccines. The WHO has provided training materials which have
already been adapted in readiness for the trainings. WHO will support the printing of the training
manuals and slide decks for both facilitators and vaccinators.
Other materials to be used during the training include, COVID-19 tally books, registers, ID cards
and AEFI forms. These documents are under development with support from JSI, WHO and
UNICEF.
9.0 Vaccine acceptance and uptake (Demand creation)
9.1 community engagement
Community engagement is very crucial when introducing interventions in the community. More
so when Malawi will be introducing the new COVID-19 vaccine, the communities should be
properly engaged for successful implementation. All stakeholders including leaders - political,
religious, and traditional and community structures should be involved at onset during the
planning, implementation and evaluation phases. Communities should be empowered to assist in
making decisions and to implement and manage the introduction of the vaccine.
Community engagement activities will be done countrywide and some to targeted communities.
The target populations for the vaccine includes the health workers, elderly, social workers and
persons with comorbidities. Community engagement is complex, hard work, and requires to be
done on a continuous basis. The following are the interventions to be carried out;

46 | Page
1. Development of operational guide for community engagement on COVID-19 response
using COVID 19 vaccine
2. Orientation of HSAS and other community Health workers on the operational guide for
community engagement on COVID 19 vaccine
3. Engagement with community leaders, block leaders, religious leaders, political leaders
on COVID 19 vaccine introduction and implementation including their roles
4. Engagement with community structures (CHAGS, VHCs, HCMCs, HMCs, VDCs,
ADCs) on COVID 19 vaccine introduction and implementation including their roles
5. Engagement with the Civil Society on COVID 19 vaccine including their roles to
support implementation
6. Monitor COVID-19 vaccine implementation using the community Health register
7. Review meetings with communities on implementation of COVID 19 vaccine
8. Community dialogue meetings during implementation
The community structures and stakeholders will be utilized by;
Promotion messaging
Engaging in rumour and misinformation identification and mitigation Arranging
community dialogue meetings as appropriate
Mitigating social and psychosocial impact as well as stigma and discrimination associated
with COVID-19 vaccine
Normalizing reactions of fear and anxiety associated with the uncertainty
and eventuality of COVID-19 vaccine
Giving key messages on the necessity of supportive family/caregiver
networks
9.2 Demand creation
Introducing a new vaccine is always a challenge, often due to inadequate knowledge, prevalence
of false information and general fear around adoption of new ideas and information. Since early
2020, there has been general hesitancy around COVID-19 vaccine on social media. By end
December 2020, the overall tone of immunization content was trending negatively in the region,

47 | Page
including Malawi. Around 40% of content had a negative tone, with only 8% of articles and posts
displaying positive sentiments.
There has been resistance from religious sectors and doubts/concerns in the general population
about effectiveness and safety of COVID-19 vaccines. These include false claims that the vaccine
will cause infertility and that its promotion and/or uptake is diabolical/sinful. Other fears relate
to the fact that the vaccine has been developed over a short period of time; thus, its safety has not
been scientifically proven outside clinical trials. On the other hand, some Anti-vaccine groups have
disseminated news that the vaccine is a political agenda by the West to wipe out the African
population.
Pandemic fatigue is increasing, as a result in part due to the stress caused by uncertainty, lower
risk perceptions and reduced trust in government responses. By September 2020, according to
rapid assessment activities conducted by UNICEF, HC4L and MEIRU, knowledge of COVID-19
was over 90% while self-efficacy to practice the recommended behaviors trailed over 70%.
However, risk perception was low at around 40%.
The College of Medicine, with support from UNICEF and FCDO, conducted a KAP survey in
November 2020. Qualitative results indicated that most participants highlighted that COVID-19 is
a threat to humankind because of its transmission through air, spreads fast, it is deadly more deadly
than other known diseases and it has no cure. However, some reported that they are not afraid
because they are following preventive measures. Others indicated that there is nothing to fear about
COVID-19 because God is bigger than COVID-19 (they trust God and they would not be at risk).
Participants highlighted several social problems being faced by communities due to COVID-19.
Some highlighted loss of business and decreased economic activities as major concerns. Other
participants reported closure of schools as a critical problem facing the youth, while others were
much concerned with isolation.
Majority of participants indicated that they get information from radio, TV, and health workers.
Others reported that they get information from church leaders and at funerals. Participants reported

48 | Page
getting trusted information regarding COVID-19 from health workers. However, it was also noted
that radio, television, and social media plays a critical role in informing people regarding COVID-
19.
Almost all participants had adequate knowledge regarding preventive measures of spread of
COVID-19 19. Participants highlighted hand washing, use of masks, sanitizers and observing
social distance as common preventive measures. Almost all participants understand the need to
keep preventive measures in place, participants highlighted that reduction in COVID-19 cases can
be the only reason to lift the measures that have been put in place.
In recommendation the team observed, among other processes, that there is need to strengthen
interpersonal communication and community engagement which should include engagement of
religious leaders, community leaders and health workers to raise risk perception and debunk
rumors. In addition, partners need concerted effort from all response pillars to respond to the
socioecological effects of COVID-19 e.g. missed employment, which has a bearing on reducing
risk perception and adoption of recommended practices. The recommendations have been utilized
to share the current risk and crisis communication, and social mobilization plan on COVID-19
vaccine, which includes risk communication.
The demand creation strategy intends to ensure a high level of COVID-19 vaccine acceptance and
uptake among most-at-risk populations and the public. Demand creation strategies will be drawn
under the objectives stipulated in the Table 4 below.
Table 3 Demand creation objectives
COVID-19 Vaccine COVID-19
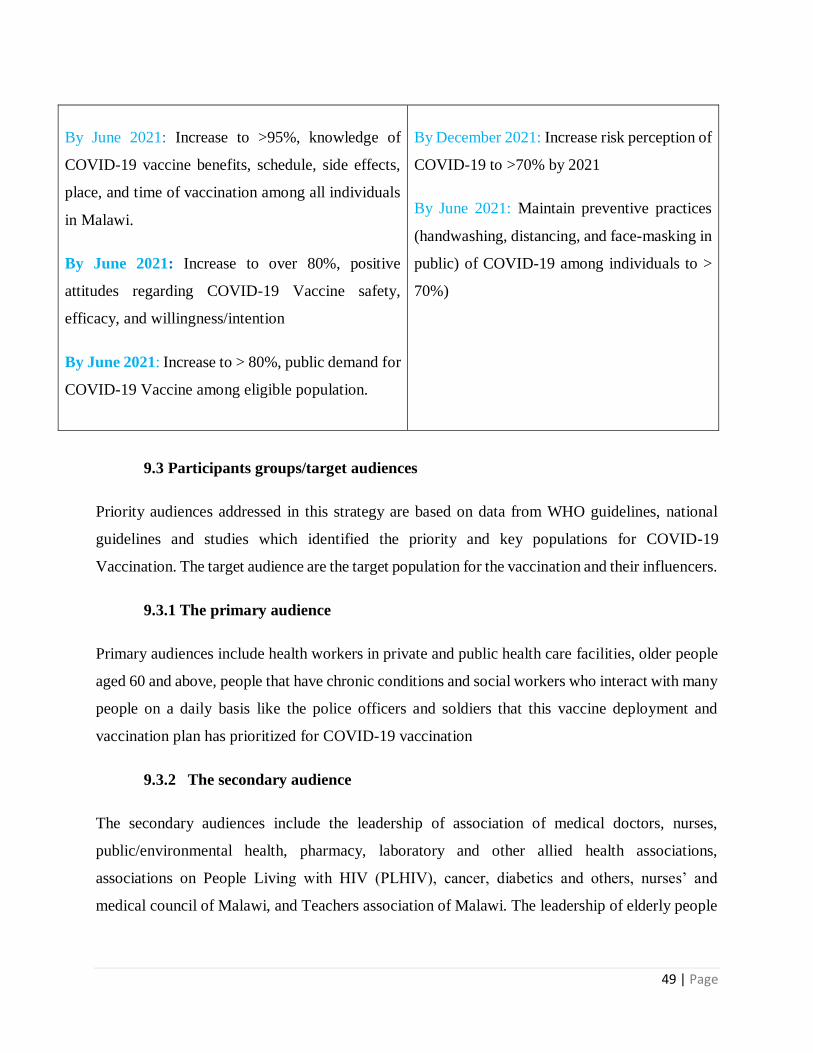
49 | Page
By June 2021: Increase to >95%, knowledge of
COVID-19 vaccine benefits, schedule, side effects,
place, and time of vaccination among all individuals
in Malawi.
By June 2021: Increase to over 80%, positive
attitudes regarding COVID-19 Vaccine safety,
efficacy, and willingness/intention
By June 2021: Increase to > 80%, public demand for
COVID-19 Vaccine among eligible population.
By December 2021: Increase risk perception of
COVID-19 to >70% by 2021
By June 2021: Maintain preventive practices
(handwashing, distancing, and face-masking in
public) of COVID-19 among individuals to >
70%)
9.3 Participants groups/target audiences
Priority audiences addressed in this strategy are based on data from WHO guidelines, national
guidelines and studies which identified the priority and key populations for COVID-19
Vaccination. The target audience are the target population for the vaccination and their influencers.
9.3.1 The primary audience
Primary audiences include health workers in private and public health care facilities, older people
aged 60 and above, people that have chronic conditions and social workers who interact with many
people on a daily basis like the police officers and soldiers that this vaccine deployment and
vaccination plan has prioritized for COVID-19 vaccination
9.3.2 The secondary audience
The secondary audiences include the leadership of association of medical doctors, nurses,
public/environmental health, pharmacy, laboratory and other allied health associations,
associations on People Living with HIV (PLHIV), cancer, diabetics and others, nurses’ and
medical council of Malawi, and Teachers association of Malawi. The leadership of elderly people

50 | Page
in Malawi, pensioners’ association of Malawi, religious groupings, Malawi interfaith association,
Pentecostal churches of Malawi and traditional leaders
9.3.3 The tertiary audience
Members of parliament, health right activists, Malawi Health Equity Network, Media Institute of
Southern Africa (MISA) in Malawi and the media fraternity constitute the tertiary audience. These
will be reached to lobby for message dissemination through their bodies.
9.4 Channels of Communication
The media plays a significant role in ensuring significant public awareness. The country shall use
multiple media and platforms for better message consumption and coverage.
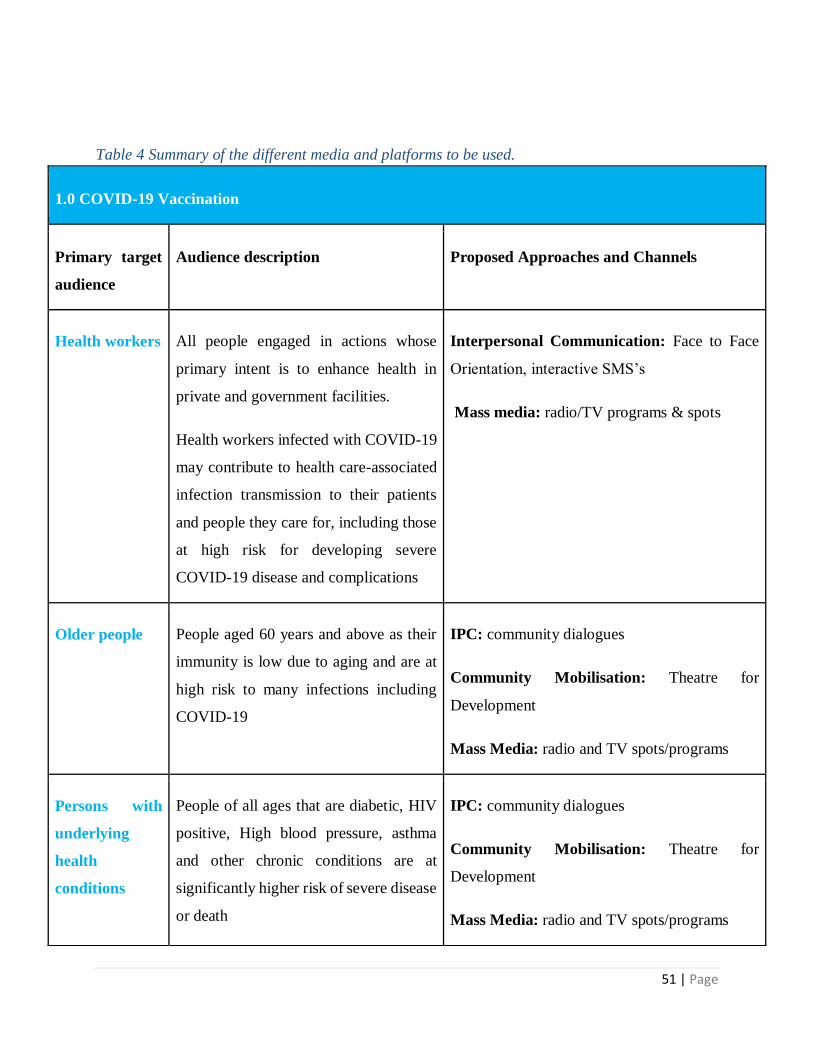
51 | Page
Table 4 Summary of the different media and platforms to be used.
1.0 COVID-19 Vaccination
Primary target
audience
Audience description Proposed Approaches and Channels
Health workers All people engaged in actions whose
primary intent is to enhance health in
private and government facilities.
Health workers infected with COVID-19
may contribute to health care-associated
infection transmission to their patients
and people they care for, including those
at high risk for developing severe
COVID-19 disease and complications
Interpersonal Communication: Face to Face
Orientation, interactive SMS’s
Mass media: radio/TV programs & spots
Older people People aged 60 years and above as their
immunity is low due to aging and are at
high risk to many infections including
COVID-19
IPC: community dialogues
Community Mobilisation: Theatre for
Development
Mass Media: radio and TV spots/programs
Persons with
underlying
health
conditions
People of all ages that are diabetic, HIV
positive, High blood pressure, asthma
and other chronic conditions are at
significantly higher risk of severe disease
or death
IPC: community dialogues
Community Mobilisation: Theatre for
Development
Mass Media: radio and TV spots/programs

52 | Page
9.5 Risk Communication strategy
Crisis communication for the COVID-19 vaccine has been designed to provide guidance and easy
to follow steps to support the community in preparation for, management of rumors,
misconceptions and other associated vaccine AEFI with some of the following scenarios:
Side effects: soreness at the site of injection, fatigue, headache, and muscle pain.
Suspicion about poor vaccine quality.
Actual event arising from vaccine: Loss of trust of the current and subsequent vaccines.
Vaccine replacement/recall.
Table 5 Summary of Risk Communication Strategy
COVAX scenario
Development of side
effects: soreness at the site
of injection, fatigue,
headache, and muscle pain:
COVAX scenario:
Other adverse effects e.g.
fainting or death
COVAX scenario
Developing COVID-19
symptoms after vaccination
Key message:
It is normal to experience side
effects within 24 to 48 hours
after immunization
Key message:
There can be other effects
not related to COVAX,
which can happen when one
has taken the vaccine
Key message:
COVAX reduces the risk of
getting infected. Always follow
recommendations to avoid
vaccination if you are already
infected

53 | Page
1. Supporting message
Seek prompt medical
attention if side effects
continue or if you are
concerned about their severity
1. Supporting message
COVAX does not increase
people’s risk to other life
threatening conditions
1. Supporting message
It is rare for a person who is
vaccinated to develop COVID-
19 symptoms
COVAX scenario:
Suspect poor vaccine quality
COVAX scenario:
· Actual
event arising from vaccine:
Loss of trust of the current
and subsequent vaccines
COVAX scenario:
· Vaccine
replacement/recall:
Demand explanations,
apology and
compensations.
Key message:
All vaccines including COVAX
are tested and found to be safe for
use.
Key message:
Many children in Malawi
safely receive the vaccines.
There are times when a single
or few doses might have
problems. The good news is
that a large number of the
population is protected
Key message:
Government can
recall/replace a vaccine if
it is proven that it have
detrimental effect on the
lives of people.

54 | Page
1. Supporting message
To protect lives some vaccines
are developed quickly e.g. the
Ebola vaccine and COVAX.
These are still tested for safety
1. Supporting message
COVAX is safe. Government
can recall/replace a vaccine if it
is proven that it have
detrimental effect on the lives
of people.
1. Supporting
message
When you have issues with
our services seek advice
from the nearest health
facility.
Table 6 Proposed Crisis Responses on Anticipated Issues
Issue Scenario Serious-
ness
(low,
medium,
high)
Crisis activities Preventive
actions e.g.
training etc.
New study New findings
showing that
COVAX has lower
efficacy
High
Ministerial
statement
Panel discussion
by experts (live)
Health worker
trainings
Media
orientations

55 | Page
Production and
dissemination of
fact sheets
Community
sensitizations
Vaccine
reaction
(AEFI/AE)
Development of
other side effects (
normal and
abnormal)
Medium
High
Investigation and
prompt feedback
Follow up/close
supervision
Holding statement
(MoH Hq)
Health worker
trainings
Community
sensitization
Surveillance
and supervision

56 | Page
Vaccine
recall
(suspensio
n)
Product quality
related issues
Program related
immunization error
High
Review
communication
materials
(Question and
answers, fact
sheet, press
statement, holding
statement
Investigation
(within 24 hours
after an AESI
report)
Press statement
Holding
statement
Community
meeting
Press briefing
Training health
workers on
malaria vaccine
& related AESIs
Community
meetings
Media briefing

57 | Page
(Question and
answers, fact
sheet)
Media
report and
rumour
AEFIs/AESIs High
Medium
Media briefing
Press release
Public
announcements
Community
awareness
meetings
Community
engagement
Media briefing
Training health
workers & PROs
Press conference
Community
awareness
meetings
Community
engagement

58 | Page
Vaccine
replacemen
t
Suspect poor
vaccine quality-
affect uptake
Loss of trust of the
current and
subsequent
vaccines
Demand
explanations,
apology and
compensations.
High
Media briefing
Press release
Public
announcements-
holding statements
Press conference
Community
awareness
meetings
Community
engagement
Training of
health workers,
Media & PROs
Press conference
Community
awareness
meetings
Community
engagement

59 | Page
9.6 Campaign Positioning
Communication and social mobilization interventions will be implemented in three phases with
different levels of intensity. Phase 1 will include inception activities, e.g., rapid assessment, and
accelerated high-intensity interventions on debunking rumors and providing accurate information
on the vaccination. In addition, RCCE interventions will intensify motivation to increase risk
perception of COVID-19. Phase 2 will continue with community engagement while taking into
consideration emerging issues, e.g. AEFIs and crisis communication, while continuing to collect
insights and conduct communication, community engagement and social mobilization. Finally
Phase 3 will mainly involve evaluation and replanning. The table below illustrates:

60 | Page
9.7 Phased Implementation of Risk and Crisis Communication
Table 7 Table 6 Risk and crisis communication phased implementation table
Intervention Phase 1 Phase 2 Phase 3
Rapid Assessment √ √
Regular collection of
insights
√ √ √
Review crisis
communication plan √ √
Public risk
communication:
Awareness &
debunking rumours
√ √ √
Community
engagement and
social mobilization
√ √ √
Advocacy √ √
AEFI & regular
monitoring and
response
√
Crisis communication √

61 | Page
Review and
replanning
√
9.8 Monitoring, Evaluation and Documentation
Monitoring tools will be adapted from the COVID-19 vaccination monitoring framework and be
utilized for data collection at national, district and community levels, see Annex 2 for the
indicators. An online dashboard will be created for i) District health Promotion Officers and ii)
national partners (CSOs, iNGOs and government partners) to fill data on reach and provide insights
collected from the field as well as recommendations that will be discussed in RCCE meetings. To
ensure that there is regular situation analysis, other digital platforms will be utilized e.g. U-report,
929 platform (Chipatala cha pa Foni). M&E tools/platforms will include:
o National-level data collection forms
o District-level data collection forms
o Community-level data collection forms
o Online dashboard ( national and district)
o U-report templates
o CCPF (Chipatala cha pa Foni)
o Formal Survey by academia
o Talk walker ( Online Social Listening)
9.9 Coordination
Coordination mechanisms through COVID-19 RCCE Committees will be strengthened at national,
district and community levels to increase participation of partners. The committees will be chaired
by the Deputy Director of HES, District Health Promotion Officer and facility Health promotion
focal person respectively, and the responsibilities at national and district will be:
● Mapping interventions
● Monitoring implementation

62 | Page
● Coordinating monitoring and evaluation activities e.g. joint monitoring, coordinating
partners conducting rapid assessment
● Providing guidance for leveraging resources
● Providing guidance for strategic approaches
At community Level the committee will be responsible for:
o Mapping interventions
o Monitoring implementation by community agents
o Coordinating monitoring and evaluation activities e.g. joint monitoring, coordinating
partners, monitoring, and reporting AEFIs.
In order to ensure that all the above objectives have been achieved, the following will be
undertaken; Conduct baseline research and evaluation, development of COVID-19 vaccine social
mobilization and crisis communication strategy, develop communication products for various
groups (media briefs, IPC for frontline workers, print materials, community mobilization guides,
advocacy kits), conduct district level social mobilization community engagement and
interpersonal communication by frontline workers, conduct media briefings, produce and air
communication products on COVID-19 vaccine, conduct advocacy meetings on COVID-19
vaccine and monitor implementation of communication activities, rumors, myths and
misconceptions.
10.0 Vaccine safety monitoring
Quality vaccines and safe immunization practices are important to successful immunization
programmes. Vaccines are largely used to protect individuals from acquiring deadly infectious
diseases which are preventable. Vaccines are safe and effective. However, no vaccine is 100% safe
and adverse reactions may occur which are mostly mild and self-limiting. Vaccines rarely cause
serious reactions and most of these serious reactions are coincidental to vaccination.
Adverse events following immunization (AEFI) surveillance is important in monitoring safety of
vaccines. AEFIs, if not properly handled, may confuse the public to the extent of compromising
the success of immunization programmes. AEFIs occur during routine immunizations, campaigns
and/or when new vaccines are introduced.

63 | Page
Another essential component of vaccine safety surveillance is the detection and reporting of
Adverse Events of Special Interests (AESIs). This is a list of conditions set by experts to pay
special attention. The conditions would come from the events that have been detected in the
product of similar characteristics or and potential signals that were detected in the clinical trials.
Malawi will utilize its experience and lessons learnt with RTS, S AESI surveillance to conduct
similar active surveillance for selected AESIs of covid-19 vaccines.
The broad objective is to ensure that there is adequate monitoring and appropriate management of
AEFIs during the introduction of Covid vaccination. Including training of health care workers on
identification, management and reporting of suspected anaphylaxis and ensuring availability of
adrenaline AEFI kits at all vaccination sites.
Pharmacovigilance during the implementation of this deployment and vaccination plan shall be
guided by the following specific objectives:
To ensure that health workers are adequately trained on both common and rare
AEFIs
To ensure that vaccinators and health workers can detect, manage and report AEFIs
including those that may be due to COVID-19 vaccine.
To strengthen the existing structures of AEFI review and causality assessments so
that there is capacity to timely identify and characterize all AEFIs including those
that may appear in patients that received COVID-19 vaccine.
Malawi has a functional AEFI surveillance system. Since 2019, Malawi has been reporting more
than 10/100,000 cases which is an indicator of a functional AEFI surveillance system according to
the Global Vaccine Action Plan (GVAP). All the districts have AEFI reporting forms and AEFI
investigation forms. Furthermore, 11 out of 29 administrative districts have district investigational
teams. The guidelines are in place, the reporting and investigational tools have been distributed,
and line-list is generated and shared every quarter. Roles and responsibilities are clearly identified,
and training have been conducted at all levels and also in progress. Also, the country has a well
established national AEFI committee with expertise from diverse backgrounds already trained in
generic causality assessment. The committee, in coordination with the Intercountry Support team

64 | Page
(IST) is also being trained to undergo Covid vaccine specific challenges on causality assessment.
This committee is called the Medicines Safety and Quality Monitoring Committee, under
Pharmacy Medicine Regulatory Authority.
The country will continue training more health care workers in AEFI surveillance. Also, it will
utilize lessons learnt from RTS, S vaccine implementation in training and strengthening district
investigation teams in all the districts. These teams will be able to conduct investigation of all
AEFIs that warrant investigations and be able to provide feedback to the concerned communities.
Equally important is the training of health promotion officers in vaccine safety and crisis
communication. This will form an essential component of vaccine safety surveillance.
In addition, EPI will work closely with PMRA to ensure that the activities mentioned by the
vaccine manufacturers as part of their risk management plan are successfully implemented. AEFI
reporting will use the already existing structures as shown in figures 7 below

65 | Page
Figure 6 Figure 7Malawi AEFI reporting workflow and timelines

66 | Page
11.0 Immunization monitoring systems
Monitoring of COVID-19 vaccine uptake will be integrated into the routine immunization system.
During the vaccination session, WHO recommended tally sheets will be adapted to record doses
given. Vaccination registers will be used for recording recipient details i.e. name, village, date of
birth, and doses given i.e. first and second doses. Every vaccinated person will be given an ID
card, which will also act as a reminder card for the second dose. Summary sheets will be used for
consolidating data at every vaccination point, and the facility summaries will be reported
immediately using specifically designed excel base tools At the district level, data will be
aggregated in the excel tool disaggregated by gender and priority group, and sent to the national
level immediately. The national level will have a command center which will receive and
aggregate the data, analyze, interpret for action and give feedback to districts. The data will also
be shared with local and external partners.
The country has designed and developed COVID-19 vaccine M&E tools to be used for recording,
aggregation, and reporting data. These are micro-planning tools, registers, vaccination ID cards,
tally sheets which will be segregated by gender, target group, etc. These tools have been developed
by the national level team through adaptation of the generic WHO COVID-19 materials and other
materials from previous vaccine introduction. Health workers will be oriented on the use of the
revised tools for them to be able to use them for data collection and timely reporting.
Monitoring framework with a set of recommended indicators among which will be on coverage,
acceptability, disease surveillance, AEFI surveillance. These indicators include; Percentage of
health workers vaccinated monthly with the first dose of COVID-19 vaccine by district, Sex and
age(<60 and >60); Monthly drop out of COVID-19 vaccine (dose 1- dose 2) by district; Proportion
of districts with stock out of COVID-19 vaccine in a month; COVID-19 vaccine wastage rate by
district by month; Number of cases with minor or serious AEFIs associated with COVID-19
vaccine reported by district by month and Number of COVID-19 reported cases in the vaccinated
target group with number of doses received and interval from first to second dose. After the
vaccination exercise, the district will review the tally sheets and aggregate the data by target group
and report to the national command center, where data will be aggregated by gender and priority
target groups in order to understand the successes or challenges within each group.

67 | Page
12.0 COVID-19 vaccination Surveillance
Malawi has detailed guidelines on how to implement surveillance strategies for COVID-19. The
main aim is to ensure that public health authorities rapidly identify and manage cases whilst
preventing further spread of the virus, thereby limiting associated morbidity and mortality.
Surveillance data helps to guide COVID-19 interventions including vaccination by providing
evidence for prioritizing high risk groups such as the elderly and those with comorbidities,
including those to be targeted for COVID-19 vaccines beyond the initial 20%. The objectives of
covid-19 surveillance are; Enable rapid detection, isolation, testing and management of cases;
Identify, follow-up and quarantine contacts; Monitor trends of COVID-19; Identify risk factors
for infection and disease transmission and guide development and implementation of targeted
control measures and vaccine implementation. Specifically, the vaccine programme will conduct
surveillance for AEFI for COVID-19 vaccine, early detection of infection and severe disease in
the vaccinated population and virus transmission dynamics following infection post vaccination.
In order to achieve the above objectives, the following disease surveillance strategies will be
implemented as part of the already existing surveillance system: Community Active Case finding,
Health Facility Active Case Finding- for both health workers and clients, Testing all travelers on
entry into the country and conduct follow-up visits up to 14 days, Testing of all truck drivers
entering the country, Testing all entrant essential personnel , Routine screening and testing health
workers managing COVID-19 cases, Isolation of all confirmed cases and quarantine of their
contacts, Intensified Contact Tracing and testing of all primary contacts and Sentinel and Mortality
surveillance in select facilities.
Surveillance system is currently being conducted in all the health facilities and the same system
will be maintained during COVID-19 vaccine introduction. A generic case-based surveillance
form is available for use in the surveillance manual of all immediately notifiable priority diseases
including COVID-19. The form also collects information on vaccination status of individuals for
vaccine preventable conditions, see Annex 3. The Public Health Institute of Malawi (PHIM) and
EPI have adapted the case-based form to collect information on COVID-19 vaccination status and
will include the vaccination status variable in the line list reporting template.
68 | Page
Effectiveness or impact studies for the new covid-19 vaccine will be conducted by PHIM and EPI
in collaboration with academia and research institutions and any other stakeholders assessed to
have the technical expertise to conduct such studies. A proposed study looking at sero-
immunology among individuals receiving COVID-19 vaccine in urban and rural cohorts of
Malawi with ongoing work with Malawi Epidemiology Intervention Research Unit, will assess the
immune response, in vitro neutralizing antibody properties and susceptibility post COVID-19
vaccination. Another study will be a quasi-experimental design and will be conducted to assess
differences in infection/re-infection rates and severity of COVID-19 disease between those
receiving the vaccine and those not vaccinated for COVID-19. These studies will follow the ethical
guidance of in-country IRB, the National Health Sciences Research Committee and will be
monitored by the National Regulatory Authority.
13.0 Post Introduction Evaluation (PIE)
Post introduction evaluation assesses the impact of a new vaccine introduction on the country's
immunization system, including the vaccination performance during introduction. The country has
been conducting PIEs for all the new vaccines it has introduced before. The evaluation is conducted
6 to 12 months after the introduction.
The PIE will also be conducted for COVID-19 vaccine after 1 month from the first phase of
introduction to get lessons that can inform the rest of the phases. Due to the travel restrictions, the
country team will conduct the PIE by adapting the generic WHO PIE materials. Districts will be
sampled for data collection on all components of immunization. The data will be analysed and a
report written with key findings and recommendations.
14.0 Lessons Learnt
COVID-19 vaccine has been introduced in the world in a unique way due to the short time taken
from trials to manufacturing up to the actual vaccination. There has been a lot of misinformation
in social media even before the vaccine is introduced in the country. The country will be getting
lessons during the introduction through supervisory visits, the PIE and general feedback from the
community. After the vaccination, the country will pull together all these in a documentation which
will guide the follow-on phases and even share the lessons with other countries.

69 | Page
References
[1] Kanyuka MM. 2018 MALAWI POPULATION AND HOUSING CENSUS. 18.
[2] Malawi_2009_STEPS_Report.pdf,
https://www.who.int/ncds/surveillance/steps/Malawi_2009_STEPS_Report.pdf (accessed
31 January 2021).
[3] Country - Malawi, https://data2.unhcr.org/en/country/mwi (accessed 31 January 2021).

70 | Page
Annexes
Annex 1 Risk Communication and Crisis plan
Target audience Justification Channel of communication
Teachers, Police
officers, soldiers,
drivers, sex
workers,
hospitality staff
These are workers whose nature of their
job demands interaction with a lot of
people and most of the times cannot
adhere to physical distancing; social
employment groups.
Interpersonal Communication: Face to
Face Orientation, interactive SMS’s
Mass media: radio/TV programs & spots
People around
borders Point of
Entries (/POEs)
(general
populations)
They are at high risk as they get exposed
to travelers.
Mass communication: leaflets, banners,
radio programs/spots
Community Mobilisation: community
dialogues/meetings/theatre
Travelers They are highly exposed to COVID-19
during travel
Mass communication: leaflets, banners
General
population
They have low risk perception due to
misconceptions and myths
IPC: community dialogues
Community Mobilisation: Theatre for
Development
Mass Media: radio and TV spots/programs

71 | Page
Children &
Young People
Children are particularly vulnerable to
the socio-economic impacts and, in some
cases, by pandemic
Mitigation measures e.g. school closures.
They may not be able to access
appropriate information or understand
the recommended behaviors and suffer
from the psychosocial impacts of the
pandemic. There may also be disruptions
in care due to the socio-economic
impacts
IPC: interactive guides
Mass Media: comic books, animations
The homeless They may live isolated from society and
not have a network of family and friends
to share information.
They may be more focused on surviving
and obtaining food than accessing
official public health information and
may be suspicious or fearful of
government services.
IPC: Guides for child protection frontline
workers
GBV Survivors Gender-based violence (GBV) increases
during every type of emergency,
including disease outbreaks. Care and
support for GBV survivors may be
disrupted, including safety, security, and
justice services.
IPC: Victim support materials (integrated
with COVID-19 messages)

72 | Page
People with
disabilities
Youth
Even under normal circumstances,
people with disabilities are less likely to
access health care, education, and
employment and to participate in the
community. They are more likely to live
in poverty, experience higher rates of
violence, neglect, and abuse, and are
among the most marginalized in any
crisis-affected community. They are
often excluded from decision-making
spaces and have unequal access to
information on outbreaks and
availability of services, especially those
who have specific communication needs.
Act as influencers and help in
information dissemination. Some are
active drivers of the pandemic, therefore
need to participate in prevention and
control.
IPC: Special materials for PwDs e.g.
Braille, sign language
Entertainment education: TV/radio
programs
Community/social mobilisation:
utilisation of youth platforms e.g. National
Youth Council at national and district levels,
youth clubs
New media: WhatsApp, FB etc.

73 | Page
Annex 2 Proposed Set of Core Indicators for Monitoring & Evaluation
Outcome (Impact) Indicators
1. % of fully immunized persons segregated by Sex and age.
2. % of individuals who believe that all eligible persons should take the COVID-19
vaccine
3. % of beneficiaries and/or their parents who are willing to be vaccinated (or give
consent to be vaccinated).
4. %age of individuals practicing recommended behaviors to prevent and control COVID-
19
Outputs and Interim Outcomes Indicators
Knowledge, Awareness, Perception of Risk, Acceptance and Trust
1. % of individuals who have heard about the COVID-19 vaccine and know what it is
meant for.
2. % of individuals who know what measures should be taken if they have been in
contact with someone who has COVID-19
3. % of persons who believe they are at high/low/no risk of getting COVID-19.
4. % of persons per eligible population group who agree to take the COVID-19 vaccine
for preventing COVID-19.
5. % of all eligible persons who intend to give consent for COVID-19 vaccination (in the
future)
6. % of people who agree that they would consent to their child/relative receiving the
COVID-19 vaccine
7. % of eligible persons who believe that the COVID-19 vaccines are safe
8. % of eligible persons who believe that the COVID-19 vaccine is effective in preventing
COVID-19

74 | Page
Coverage with Equity
11. % of eligible persons who took their first dose/all doses of COVID-19 vaccine.
12. % of eligible persons segregated by gender who were fully immunized with all doses
of COVID-19 vaccine in hard to reach areas.
Vaccination Experience and Frontline Worker Commitment
13. % of beneficiaries and/or their parents who reported that the vaccination experience
was positive
14. % of beneficiaries and/or their parents who had, or agreed to, proactively promote
COVID-19 vaccination in their communities or among their peers.
15. % of front-liners who ensured that >90% of all eligible persons in their designated
catchment area were reached with messages/interventions
Establishing COVID-19 Vaccination as a Norm
16. % of beneficiaries and/or their parents who believe that their community or peer group
expects all eligible persons to take COVID-19 vaccination.
Media Support and Commitment
18. % of positive and supportive COVID-19 vaccine reports in the media compared to
negative reports.
Input and Process Indicators: Coordination, Planning, and Operations
National Level
1. # of Communication Sub-committee or Working Group meetings that took place
75 | Page
2. # of communication and social mobilization activities or events planned compared to
# of activities or events implemented
3. # of planned communication materials/products produced on COVID-19 vaccine
4. # of planned communication materials/products disseminated on COVID-19 vaccine
(distributed or broadcast)
5. # of parents/guardians of eligible persons who had been reached by COVID-19 vaccine
key messages (heard on broadcast media or through interpersonal communication by
front-line workers, etc.)
6. # of community leaders (at village/community level) who had been reached by
COVID-19 vaccine key messages (heard on broadcast media or through interpersonal
communication by front-line workers, etc.)
District Level
7. # of districts with communication and community engagement micro-plans (including
specific plans for reaching all beneficiaries in the hotspots)
8. # of communication and social mobilization activities or events planned compared to
# of activities or events implemented
9. # of frontline health-workers trained or sensitized versus # planned
10. # of planned locations per district that received IEC materials in a timely manner.
11. # of districts who reported sufficiency of communication resources (funds, fuel, IEC
materials, front-liners)
12. # of districts who conducted sensitization and engagement activity in each of the
GHVs
13. # of reports of rumors, misinformation, or AEFIs
14. # of reports of rumors, misinformation, or AEFIs that were resolved within 72 hours.
15. % of individuals who know how to provide feedback about decision making processes
which affect them

76 | Page
Annex 3 Timeline of Activities
FUNDING
Start End 1 2 3 4 5 6
1 Development of NDVP, budgets and timelinesEPI-
TWG(NCC)DONE 20/12/2020 09/02/2021
WHO/UNICEF/JS
I3 National Task Force Meeting NTF CHAIR in progress 16/02/2021 ongoing GLOBAL FUND
4 Sub committees' meetings NTF in progress 16/02/2021 ongoing not secured
5 Development of IEC materials and Review of
communication strategy including Risk and Crisis HEU in progress 11/02/2021 28/02/2021 UNICEF
6 Development of publicity materials HEU in progress 11/02/2021 28/02/2021 UNICEF
7 Printing of social mobilization Materials HEU in progress 11/02/2021 28/02/2021 UNICEF
8 Press conference HEU TO BE DONE 01/03/2021 23/04/2021
9 Briefing of media personnel HEU in progress 02/03/2021 31/03/2021 TREASURY
10 Advance Publicity HEU TO BE DONE 01/03/2021 ongoing WORLD BANK
11 Development of operational guide and training deck EPI in progress 15/02/2021 28/02/2021 WHO
12Finalization of training guides, Data monitoring and
Microplanning toolsEPI
in progress01/03/2021 05/03/2021
WHO
13 Development of data monitoring tools (including
C0VID vaccine)EPI in progress 15/02/2021 19/02/2021 UNICEF
14 Procurement/ mobilization of PPE EPI In progress 01/02/2021 28/02/2021 MoF/MoH
15 Airing of Radio/ TV slots HEU 01/03/2021 on going UNICEF
16 Printing of training guides and data monitoring tools EPI 15/02/2021 05/03/2021 WHO/UNICEF
17 Distribution of logistics to districts EPI 05/03/2021 31/03/2021 GLOBAL FUND
18 Training of District Trainers on COVID vaccine
IntroductionNTF 01/03/2021 12/03/2021 MoF/MoH
19 Briefing of DEC/DDC members DTF 01/03/2021 03/03/2021 MoF/MoH
20 Briefing of District Taskforce Members NTF 01/03/2021 12/03/2021 MoF/MoH
21 DTF meetings DTF 14/03/2021 30/03/2020 MoF/MoH
22 Briefing of Supervisors EPI 03/03/2021 04/03/2021 MoF/MoH
23 Briefing of vaccinators DTF 03/03/2021 04/03/2021 GLOBAL FUND
24 NTF Supervision during briefing of vaccinators DTF 03/03/2021 03/03/2021 MoF/MoH
25 Distribution of logistics to health facilities DTF 10/03/2021 16/03/2021 GLOBAL FUND
26 Facility microplanning DTF 05/03/2021 13/03/2021 MoF/MoH
27 Briefing of local leaders DTF 05/03/2021 06/03/2021 MoF/MoH
28 Briefing of Volunteers DTF 05/03/2021 06/03/2021 not secured
29 Micro planning Meeting EPI 10/03/2021 21/03/2021 not secured
30 Forecasting and Establishment of Traceability of
VaccinesEPI 23/03/2021 on going not secured
31Operational Research EPI/PHIM/
COM/PAR 01/03/2021 on going not secured
32 National Launch of COVID-19 vaccine NTF 08/03/2021 0ne time off MoF/MoH
33 NTF supervision on actual days NTF 26/03/2021 ongoing MoF/MoH
34 District level supervision on actual days DTF 26/03/2021 ongoing MoF/MoH
35 Injection materials wastes incineration DTF 01/03/2021 ongoing MoF/MoH
36 Data analysis at district level DTF 10/05/2021 ongoing MoF/MoH
37 Report writing NTF 30/06/2021 05/08/2021 MoF/MoH
38 Post -Introduction Evaluation (PIE) NTF 01/10/2021 30/10/2021 WHO/UNICEF
COVID 19 VACCINATION TIMELINE2021
S/No Main ActivitiesResponsib
leStatus

77 | Page
Annex 4 Budget
Table 1: Budget Summary
Item Description COST (MWK) US$ Funding support
Development of training guides 10,943,344.00 14,788.30 WHO/UNICEF
Finalization of training guides 8,548,008.00 11,551.36 WHO
Development of data monitoring tools (including C0VID 13,888,344.00 18,768.03 UNICEF
Printing of training guides and procurement of other 15,156,600.00 20,481.89 WHO
Press conference 590,280.00 797.68 MIN. OF FINANCE
Micro planning Meeting 92,260,300.00 124,676.08 MIN. OF FINANCE
Review and Finalization of Microplanning Tools 31,532,447.20 42,611.42 MIN. OF FINANCE
Mapping of target population for COVID-19 vaccine 97,528,000.00 131,794.59 MIN. OF FINANCE
Training of District Trainers on COVID vaccine 64,166,440.00 86,711.41 MIN. OF FINANCE
Briefing of District Taskforce Members 73,371,280.00 99,150.38 MIN. OF FINANCE
Briefing of Supervisors 49,906,348.00 67,441.01 MIN. OF FINANCE
Briefing of DEC/DDC members 24,992,182.00 33,773.22 MIN. OF FINANCE
Briefing of Vaccinators 82,643,494.00 111,680.40 MIN. OF FINANCE
Briefing of Volunteers 19,680,000.00 26,594.59 MIN. OF FINANCE
Briefing of local leaders 59,040,000.00 79,783.78 MIN. OF FINANCE
NTF Supervision during briefing of vaccinators 39,891,840.00 53,907.89 MIN. OF FINANCE
Distribution of logistics to districts 8,010,000.00 10,824.32 GLOBAL FUND
Distribution of logistics to health facilities 29,310,000.00 39,608.11 GLOBAL FUND
Incentives for vaccinators during Actual days 120,000,000.00 162,162.16 MIN. OF FINANCE
Incentives for volunteers during Actual days 13,120,000.00 17,729.73 MIN. OF FINANCE
NTF supervision on actual days 13,100,000.00 17,702.70 MIN. OF FINANCE
District level supervision on actual days 79,760,952.00 107,785.07 MIN. OF FINANCE
National Taskforce meetings 24,065,360.00 32,520.76 GLOBAL FUND
District planning meetings 45,836,978.88 61,941.86 MIN. OF FINANCE
Injection materials wastes incineration 8,206,492.00 11,089.85 MIN. OF FINANCE
Report writing 14,479,100.00 19,566.35 MIN. OF FINANCE
Clearing costs of vaccine and injection materials 4,420,000.00 5,972.97 MIN. OF FINANCE
Post -Introduction Evaluation (PIE) 33,702,160.00 45,543.46 WHO/UNICEF
Procurement of PPE 146,115,840.00 197,453.84 MIN. OF FINANCE
Grand Total 1,224,265,790.08 1,654,413.23
COVID-19 VACCINE INTRODUCTION BUDGET, 2021-22

78 | Page
Annex 3 demand creation and social mobilization and community engagement budget
MK US$
1 Development of Risk Crisis and Communication Strategy 20,137,232
2 Development of COVID-19 vaccine communication materials 6,767,504
3 Pre-Testing of COVID-19 vaccine materials 15,700,032
4 Printing of Publicity materials 34,300,000
5 Conduct Regional Press Briefings 19,939,716
6 Conduct Regional Media Tours 24,009,732
7 Media press releases on COVID-19 Vaccine 126,000,000
8 Advance Publicity 178,585,120
9 Hoisting of banners in strategic places in cities and districts 79,800,000
10Production of Radio and TV, Radio Programs, PSAs and Jingles
in different languages
123,000,000
11Airing of Radio and TV, Radio Programs, PSAs, Jingles and Live
Panel Discussions
1,015,126,680
12 Briefing of local leaders 139,334,328
13 Briefing of religious leaders 209,334,328
14 Conduct Door to Door meetings by HWs in 29 districts 195,865,600
15 Engagement with Civil Society 13,293,144
16 Strengthen the online presence 143,600,000
17 Virtual National Launch of COVID-19 VACCINE by H.E. 500,000
18Monitoring of Communication interventions with district task
teams
33,716,184
Grand Total 2,379,009,600 3,050,012
DEMAND CREATION BUDGET FOR 2021-22 COVID-19 VACCINE

















