The Risk of Injury to the Anterior Tibial Artery in thePosterolateral Approach to the Tibia Plateau:
A Cadaver Study
Nima Heidari, MBBS, MRCS(Eng), MSc, FRCS(Tr&Orth),* Surjit Lidder, BSc(Hons), MBBS, MRCS(Eng),†Wolfgang Grechenig, MD,‡ Norbert P. Tesch, MD,§ and Annelie M. Weinberg, MDk
Background: Posterolateral tibial plateau shear fractures oftenrequire buttress plating, which can be performed through a postero-lateral approach. The purpose of this study was to provide accuratedata about the inferior limit of dissection.
Methods: Forty unpaired cadaver adult lower limbs were used. Theanterior tibial artery was identified because it coursed through theinterosseous membrane. The perpendicular distance from the lateraljoint line and fibula head to this landmark was measured.
Results: The anterior tibial artery coursed through the interosseousmembrane at 46.36 9.0 mm (range 27–62 mm) distal to the lateral tibialplateau and 35.7 6 9.0 mm (range 17–50 mm) distal to the fibula head.
Conclusions: Displaced posterolateral tibial plateau fracturesrequire anatomic reduction and stabilization with a buttress plate.This can be achieved by gaining access to the posterolateral tibialcortex. The distal limit of this dissection can be as little as 27 mmdistal to the lateral tibial plateau. Dissection in this region should becarried out with caution.
INTRODUCTIONFractures of the tibial plateau are uncommon with those
affecting the posterolateral tibial plateau accounting forapproximately 7%.1 Operative fixation through an anterolat-eral approach has been described; however, there is a biome-chanical advantage of a posterolateral plate position. Severalapproaches have been described for the posterolateral tibialplateau2–8 with authors deliberating over the merits of each.
The extent of distal dissection through the posterolateralapproach is often stated as 5 cm from the tibial plateau wherethe anterior tibial artery perforates through the interosseousmembrane5; however, no published anatomic studies supportthis measurement. This study aims to provide accurate dataabout the safe inferior limit of dissection for the posterolateralapproach by providing measurements of the anterior tibialartery from the lateral joint line and fibula head to where itpierces the interosseous membrane.
MATERIALS AND METHODSForty unpaired, white adult lower limbs (20 left and 20
right) preserved using the method of Thiel were used for thisstudy.9 None of the limbs had signs of previous injury, abnor-mality, or disease. The mean age of the donors had been 71years (range, 44–84 years) at the time of death.
Each lower limb was dissected using the posterolateralapproach to the proximal tibia, as described by Frosch et al.7
The skin and superficial fascia were removed from the kneeleaving the deep fascia intact. First, the common peronealnerve was identified on the posterior border of biceps fem-oris (Fig. 1). It was followed from the apex of the poplitealfossa to the fibular neck. The lateral border of the lateralhead of gastrocnemius muscle was identified from its originon the posterior aspect of the lateral femoral condyle distally(Fig. 2). The anatomic plane between it and the soleus mus-cle was developed by blunt dissection. This brought thetendon of the popliteus muscle and the belly of the soleusmuscle along its fibular attachment into view (Fig. 3). In thisplane, care must be taken to identify and ligate the infero-lateral genicular branch of the popliteal artery. Once this wasdone, the popliteus muscle was mobilized subperiosteallyeither proximally or its tendon divided between stay-suturesso that it could be repaired during closure (Fig. 4). Thesoleus muscle was released from its origin on the posterioraspect of the fibula and retracted medially. This brought theanterior tibial vessels into view (Fig. 5). Occasionally, mus-cular branches of the popliteal artery require ligation for themuscle to be mobilized more easily. Care must be takenwhen releasing the soleus from the medial border of fibulabecause the attachment is quite fibrous at this locationand vigorous tissue handling can injure the anterior tibialvessels. Just distal to the inferior border of popliteus, the ante-rior tibial artery courses anteriorly and pierces the interosseous
Accepted for publication August 30, 2012.From the *Department of Trauma and Orthopaedics, Royal London Hospital,
London, United Kingdom; †Department of Trauma and Orthopaedics,Eastbourne District General Hospital, East Sussex, United Kingdom;‡Department of Traumatology, Medical University of Graz, Graz, Austria;§Institute of Anatomy, Medical University of Graz, Graz, Austria; andkDepartment of Pediatric and Adolescent Surgery, Medical University ofGraz, Graz, Austria.
The authors have no financial disclosures or conflicts of interest to declare.Reprints: Mr Nima Heidari, MBBS, MRCS(Eng), MSc, FRCS(Tr&Orth), Depart-
ment of Trauma and Orthopaedics, Royal London Hospital, Whitechapel,London E1 1BB, United Kingdom (e-mail: [email protected]).
membrane. This defines the most distal limit of this dissection.Once the anterior tibial artery was identified as it coursedthrough the interosseous membrane, a posterior arthrotomywas performed locating the joint line (Fig. 6). Perpendicularmeasurements were made from the posterior limit of the artic-ular surface of the lateral tibial plateau and fibula head (Fig. 7)to the position where the anterior tibial artery pierced theinterosseous membrane. All distances were measured usinga Vernier caliper and recorded in millimeters.
RESULTSThe anterior tibial artery coursed through the inteross-
eous membrane at 46.36 9.0 mm (range 27–62 mm) distal tothe lateral tibial plateau and 35.7 6 9.0 mm (range 17–50 mm) distal to the fibula head. In 6 of the 40 (15%) speci-mens, the distance from the lateral tibial plateau to the perfo-ration of the anterior tibial artery was 27–35 mm. In 13 of 40(32.5%), the distance was 36–45 mm. In 13 of 40 (32.5%),
the distance was 46–55 mm, and in the last 8 of 40 (20%), thedistance was 56–62 mm.
There was no difference between right- or left-sidedknees [anterior tibial artery distal to lateral tibial plateau;right: 44.8 6 8.5 mm (range 30–60 mm), left: 47.8 69.3 mm (range 27–62 mm); and distal to fibula head; right:34.4 6 8.6 mm (range 18–49 mm), left: 37.0 6 9.3 mm(range 17–50 mm)] (Fig. 8).
DISCUSSIONPosterolateral tibial plateau fractures are uncommon.
They are caused by a valgus and axial compressive force,with the knee in flexion. This results in a shearing forceexerted on the posterolateral tibial plateau by the lateralfemoral condyle. Isolated posterolateral plateau injuries aredifficult to asses radiographically on anteroposterior views andfull assessment of the fracture morphology requires
FIGURE 1. Posterior aspect of the right knee with skin andsuperficial fascia removed. Biceps femoris muscle (b), commonperoneal nerve (c), lateral head of gastrocnemius muscle (g)and soleus muscle (s).
FIGURE 2. The lateral border of the lateral head of gastroc-nemius muscle (g) was identified from its origin on the pos-terior aspect of the lateral femoral condyle distally andcommon peroneal nerve (c) exposed distally in the soleusmuscle (s). Biceps femoris muscle (b).
Heidari et al J Orthop Trauma � Volume 27, Number 4, April 2013
222 | www.jorthotrauma.com � 2013 Lippincott Williams & Wilkins
a computed tomography.10 Most tibial plateau fractures arepartial articular OTA type B and involve the anterolateral(Schatzker type I-III) or posteromedial (Schatzker type IV)quadrants.11 Posterolateral tibial plateau injuries may occurin isolation or in combination with posteromedial or antero-lateral tibial plateau fractures. Anatomic reduction of theseintra-articular fractures is advocated to reduce painful intra-articular malunions.12 Up to 26% of reduced fractures maystill have an articular step and angular deformity.7
For isolated posterolateral tibial plateau fractures,a buttress plate affords optimal biomechanical fixation.A number of approaches have been described for theoperative reduction and fixation of isolated or combinedposterolateral tibial plateau fractures.3,5,7,13 When there isa combination of posteromedial and posterolateral shearfractures, an extensile posteromedial approach has beendescribed.10 To avoid injury to the neurovascular bundle inthe popliteal space, Luo et al10 suggested that all the dissec-tion from medial to lateral should be performed beneath thepopliteus muscle in the proximal part of the approach.
Normal anatomic variation in the popliteal artery and itsbranches can, however, provide a challenge during this sur-gical dissection. The anterior tibial artery branches quiteproximally from the popliteal artery trunk at the proximalborder of popliteus muscle in 2.3% of the cases.14 In a further0.9% of the cases, the peroneal artery arises from the highbranching anterior tibial artery.14 In an unknown proportionof these anatomic variants, the anterior tibial artery lies deepto the popliteus muscle, in direct contact with the posteriortibial cortex.14
The rarity of these injuries means that the results offixation of these fractures are restricted to small caseseries.13 Frosch et al7 described a posterolateral approachwithout fibula osteotomy. This technique permits minimalfracture fragment dissection with preservation of the pos-terolateral ligaments.
With all of the techniques described, however, thedistal limit of dissection is the location that the anteriortibial artery perforates the interosseous membrane. Thisdistance has not been previously described with reference to
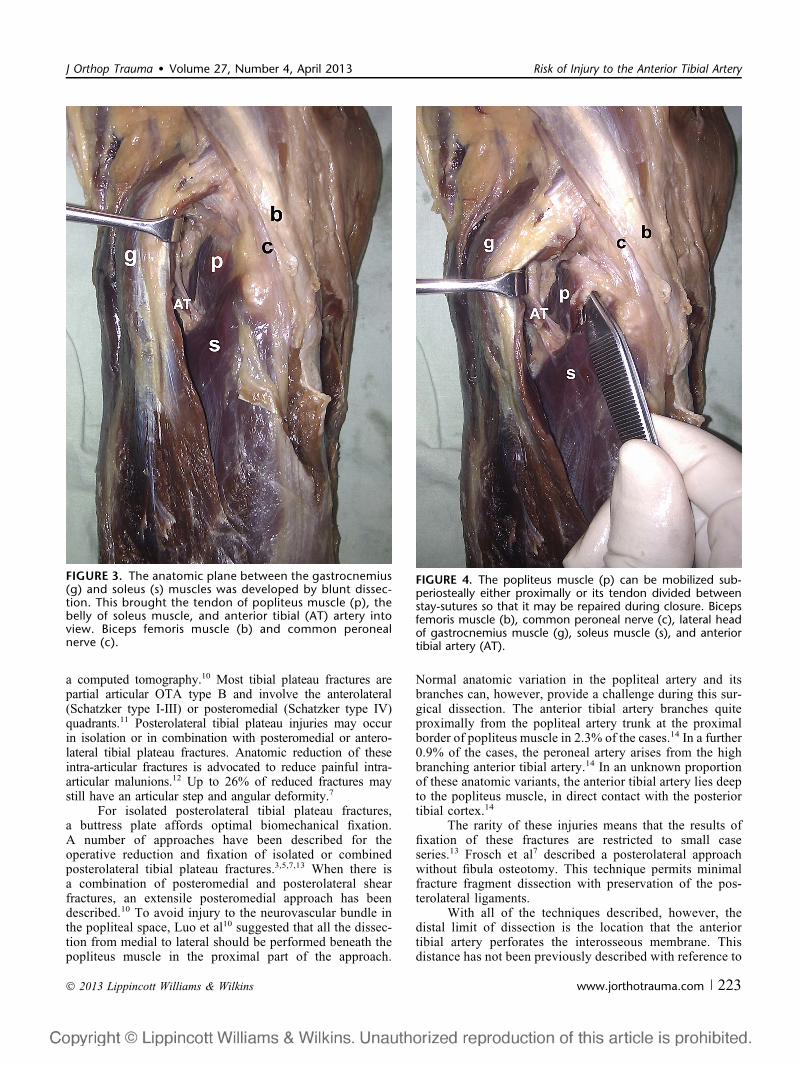
FIGURE 3. The anatomic plane between the gastrocnemius(g) and soleus (s) muscles was developed by blunt dissec-tion. This brought the tendon of popliteus muscle (p), thebelly of soleus muscle, and anterior tibial (AT) artery intoview. Biceps femoris muscle (b) and common peronealnerve (c).
FIGURE 4. The popliteus muscle (p) can be mobilized sub-periosteally either proximally or its tendon divided betweenstay-sutures so that it may be repaired during closure. Bicepsfemoris muscle (b), common peroneal nerve (c), lateral headof gastrocnemius muscle (g), soleus muscle (s), and anteriortibial artery (AT).
J Orthop Trauma � Volume 27, Number 4, April 2013 Risk of Injury to the Anterior Tibial Artery
� 2013 Lippincott Williams & Wilkins www.jorthotrauma.com | 223
anatomic data. The anterior tibial artery supplies themuscles of the anterior compartment of the leg and theoverlying skin.15 Iatrogenic injury to it at the level of tri-furcation can result in ischemic necrosis of the muscles ofthis compartment and skin loss. This cadaveric study showsthat the safe zone of distal exposure through which fracturemanipulation and safe application of a buttress plate can beperformed maybe as little as 27 mm distal to the lateraltibial plateau. This was the case in 1 of the 40 specimensinvestigated for this study, but in a further 5, the distance ofthe lateral tibial plateau to the perforation of the anteriortibial artery was less than 35 mm. In these challengingcases, a proximal fibular osteotomy as described byLobenhoffer et al3 can be performed. However, this doesnot necessarily improve the distal extent of the dissectionand carries with it the associated risks of injury to the
common peroneal nerve and further compromise of thealready injured posterolateral corner soft tissues. There isalso a small risk of nonunion of this osteotomy. Luo et al10
have described an extensile posteromedial approach wherethe posterolateral cortex of the proximal tibia can beexposed by subperiosteal dissection deep to the popliteusmuscle. These authors also caution against dissecting toofar distally and laterally toward the interosseous membranebecause the anterior tibial artery may be damaged. Addition-ally, ultrasonography studies have shown that in up to 6% ofcases, the anterior tibial artery has a more proximal origin.16
It originates proximal to the popliteus muscle and passesbeneath it in contact with the posterior tibial cortex, leavingit unprotected during elevation of the popliteus muscle fromthe posterior tibial cortex.
In conclusion, dissection in this region should becarried out with caution. A good understanding of the surgicalanatomy of this region and the morphology of the fracture areessential for a successful outcome.
FIGURE 5. The soleus muscle (s) is released from its originon the posterior aspect of the fibula (f) and retractedmedially. The anterior tibial (AT) vessels are brought intoview. Biceps femoris muscle (b), common peroneal nerve(c), lateral head of gastrocnemius muscle (g), and poplitealmuscle (p).
FIGURE 6. The anterior tibial (AT) artery was identified as itcoursed through the interosseous membrane. The poplitealmuscle (p) is reflected medially to identify the lateral tibialplateau (t). Biceps femoris muscle (b), common peronealnerve (c), lateral head of gastrocnemius muscle (g), fibula (f),and soleus muscle (s).
Heidari et al J Orthop Trauma � Volume 27, Number 4, April 2013
224 | www.jorthotrauma.com � 2013 Lippincott Williams & Wilkins
REFERENCES1. Partenheimer A, Gosling T, Muller M, et al. Management of bicondylar
fractures of the tibial plateau with unilateral fixed-angle plate fixation[Article in German]. Unfallchirurg. 2007;110:675–683.
3. Lobenhoffer P, Gerich T, Bertram T, et al. Particular posteromedial andposterolateral approaches for the treatment of tibial head fractures [Arti-cle in German]. Unfallchirurg. 1997;100:957–967.
4. Alpert JM, McCarty LP, Bach BR Jr. The posterolateral corner of the knee:anatomic dissection and surgical approach. J Knee Surg. 2008;21:50–54.
5. Chang SM, Zheng HP, Li HF, et al. Treatment of isolated posteriorcoronal fracture of the lateral tibial plateau through posterolateralapproach for direct exposure and buttress plate fixation. Arch OrthopTrauma Surg. 2009;129:955–962.
6. Trickey EL. Rupture of the posterior cruciate ligament of the knee.J Bone Joint Surg Br. 1968;50:334–341.
7. Frosch KH, Balcarek P, Walde T, et al. A new posterolateral approachwithout fibula osteotomy for the treatment of tibial plateau fractures.J Orthop Trauma. 2010;24:515–520.
8. Tao J, Hang DH, Wang QG, et al. The posterolateral shearing tibialplateau fracture: treatment and results via a modified posterolateralapproach. Knee. 2008;15:473–479.
9. Thiel W. The preservation of the whole corpse with natural color [Articlein German]. Ann Anat. 1992;174:185–195.
10. Luo CF, Sun H, Zhang B, et al. Three-column fixation for complex tibialplateau fractures. J Orthop Trauma. 2010;24:683–692.
11. Chang SM. Selection of surgical approaches to the posterolateral tibial plateaufracture by its combination patterns. J Orthop Trauma. 2011;25:e32–e33.
12. Stevens DG, Beharry R, McKee MD, et al. The long-term functionaloutcome of operatively treated tibial plateau fractures. J Orthop Trauma.2001;15:312–320.
13. Solomon LB, Stevenson AW, Baird RP, et al. Posterolateral transfibularapproach to tibial plateau fractures: technique, results, and rationale.J Orthop Trauma. 2010;24:505–514.
14. Mauro MA, Jaques PF, Moore M. The popliteal artery and its branches:embryologic basis of normal and variant anatomy. AJR Am J Roentgenol.1988;150:435–437.
15. Attinger CE, Evans KK, Bulan E, et al. Angiosomes of the foot and ankleand clinical implications for limb salvage: reconstruction, incisions, andrevascularization. Plast Reconstr Surg. 2006;117:261S–293S.
16. Tindall AJ, Shetty AA, James KD, et al. Prevalence and surgical signif-icance of a high-origin anterior tibial artery. J Orthop Surg (Hong Kong).2006;14:13–16.
FIGURE 7. Vascular anatomy of the posterior left knee. Pop-liteal artery (P), lateral superior genicular artery (a), medialsuperior genicular artery (b), lateral inferior genicular artery(c), medial inferior genicular artery (d), anterior tibial (AT)artery. Perpendicular measurements from lateral joint line (A)and fibula head (B) to anterior tibial artery.
FIGURE 8. Bar graph and diagram showing perpendiculardistance of anterior tibial artery perforating the interosseousmembrane (X) from the lateral tibial plateau.
J Orthop Trauma � Volume 27, Number 4, April 2013 Risk of Injury to the Anterior Tibial Artery
� 2013 Lippincott Williams & Wilkins www.jorthotrauma.com | 225