72
The role of neuroimaging in dementia of the working age Nick Fox Dementia Research Centre Institute of Neurology, UCL Queen Square, London

The role of neuroimaging
in dementia of the
working age
Nick Fox Dementia Research Centre
Institute of Neurology, UCL
Queen Square, London

Overview
• Changing role of imaging
• “Working age” dementia
• Guidelines and consensus criteria
• Imaging features of the dementias
• What a scan can tell you – adding value
• A practical approach …
…..and a look to the future
Early-onset dementia. Jefferies & Agrawal APT 2009;15:380-388
The diagnosis of young-onset dementia. Rossor, Fox et al Lancet Neurology 2010;9:793-806.

Changing roles of imaging
• From excluding treatable causes
– Neoplasm, hydrocephalus, subdural
– “Yield” – 1% ?
• To making a positive diagnosis
– moving from “dementia” to a specific diagnosis
• Supporting an earlier diagnosis
– adding specificity to “MCI”
• Adding molecular information
• Research and Trials

Improving diagnosis
• National priority: “Dementia Strategy”
• Patient and carers: Alzheimer’s Society
“…it is crucial to highlight the value of
early diagnosis and intervention …”

Structural imaging for diagnosis
•Structural imaging should be used to assist in the diagnosis of dementia, to aid in the differentiation of type of dementia and to exclude other cerebral pathology
•Magnetic resonance imaging (MRI) is the preferred modality to assist with early diagnosis and detect subcortical vascular changes, although computed tomography (CT) scanning could be used

• CT and MRI may be used to exclude treatable causes of dementia.
• Multislice CT and coronal MRI may be used to assess hippocampal atrophy to support a clinical diagnosis of AD (Level B).
• FDG PET and perfusion SPECT are useful adjuncts when diagnosis remains in doubt (level B).
• Dopaminergic SPECT is useful to differentiate AD from DLB (level A).
• Follow up with serial MRI is useful in a clinical setting to document disease progression (good practice point).

Establishing the subtype diagnosis
• Diagnosis is based on clinical criteria
Imaging supportive but not required
• Alzheimer’s disease
• Dementia with Lewy bodies
• Frontotemporal dementia
• CJD
Imaging needed for vascular dementia
• Extent
• Topography
• Severity

How is imaging different in
people of working age?

“working age” is ?
Working age dementia in
the UK
• 40,000 cases (20-60K) vs 700,000 total
• Unusual causes relatively more common –
not so dominated by AD and VaD
• And so are atypical presentations of AD
• Higher proportion of
– “treatable” causes
– Genetic causes
• Some characteristic imaging features

Working age dementia
• AD 30-35%
• Vascular 10-15%
• FTD ~10-15%
• Alcohol ~10%
• DLB ~5%
• Other ~20-25%
• Other .. – HD
– PSP, CBD
– Head injury
– MS
– Epilepsy
– CJD
– Familial AD & trisomy 21
– Antibody mediated

Unusual & “treatable” causes are more common
in younger than older onset dementia
Early-onset dementia. Jefferies, and Agrawal APT 2009;15:380-388
©2009 by The Royal College of Psychiatrists

Structural imaging to assess: space occupying
lesions, vascular damage and pattern of atrophy





Gait disturbance
Cognitive impairment
Urinary difficulties


Normal pressure hydrocephalus Tight convexity CSF spaces

Changing roles of imaging
• From excluding treatable causes
• To making a positive diagnosis
– moving from “dementia” to a specific diagnosis

“No space occupying lesion. There
is involutional change likely related
to ageing and there are some
scattered white matter
hyperintensities…”
A scan is only as useful as its
interpretation …

What can you ask (look for)
beyond a surgical cause?
• Is the scan normal for age?
• Signal change?
– VaD?
• Look at basal ganglia & brain stem
• Extent of white matter change
– Other?
• Atrophy?
– Is there focal (lobar) or generalised atrophy?
– Disproportionate hippocampal atrophy?

Vascular dementia
• Stepwise progression of dementia may be a feature
but… many cases of VaD have gradual deterioration
• Focal neurological signs (e.g. aphasia, hemiparesis)
may be present but are often not
• Frontal subcortical cognitive profile with gait
abnormalities, brisk reflexes, pout
• Small vessel disease may mimic AD/DLB - insidious
onset and progression including “memory”

Large vessel (multi-infarct)
dementia
Cortico-
subcortical
occipito-temporal
infarct

Strategic infarct(s)
• THALAMIC
DEMENTIA


Subcortical VaD
• White matter predominant
• Lacunar
predominant

1 = Punctate 2 = Early Confluent 3 = Confluent
NEVER normal “Normal” Abnormal < 70
White matter lesions – Fazekas scale

Pattern of microbleeds

Not all signal change is
vascular

Baseline 6 months later
VGKC associated Limbic Encephalitis

DWI FLAIR
Prion – CJD

C
J
D

Atrophy
• Generalised? Symmetrical?
• Hippocampal atrophy > global?
• Progressive?

In AD tangles first appear in
Entorhinal Cortex and then
Hippocampus
Transentorhinal
Stages I-II
Limbic
Stages III-IV
Braak & Braak 1991

H
A
E
C
Medial temporal lobe regions
atrophy early in AD
AD
• Symmetrical atrophy with posterior
greater than anterior loss (cf FTLD)
• The medial temporal lobe and posterior
cingulate are sites of early change

In “mild” AD the hippocampus is
10-20% smaller than in controls
Seab ’88, De Leon ’89, Scheltens ’92, Soininen ’94, Jack ’99, Du ’01, Killiany ’02

Proposed criteria for AD


Time 0 18months 36months
H
Serial coronal MRI of an individual with initially mild AD

MMSE ~20/30
H/c 25% down
Sens & spec ~85%
Less sensitive in younger and milder patients
Arch Neurol 2007

Duara Neurology 2008
Visual assessment of atrophy

Spiral CT – now able to get
high resolution - atrophy
pattern similar to MRI
Wattjes M P et al. Radiology 2009
MRI CT

55 yr AD CDR =1
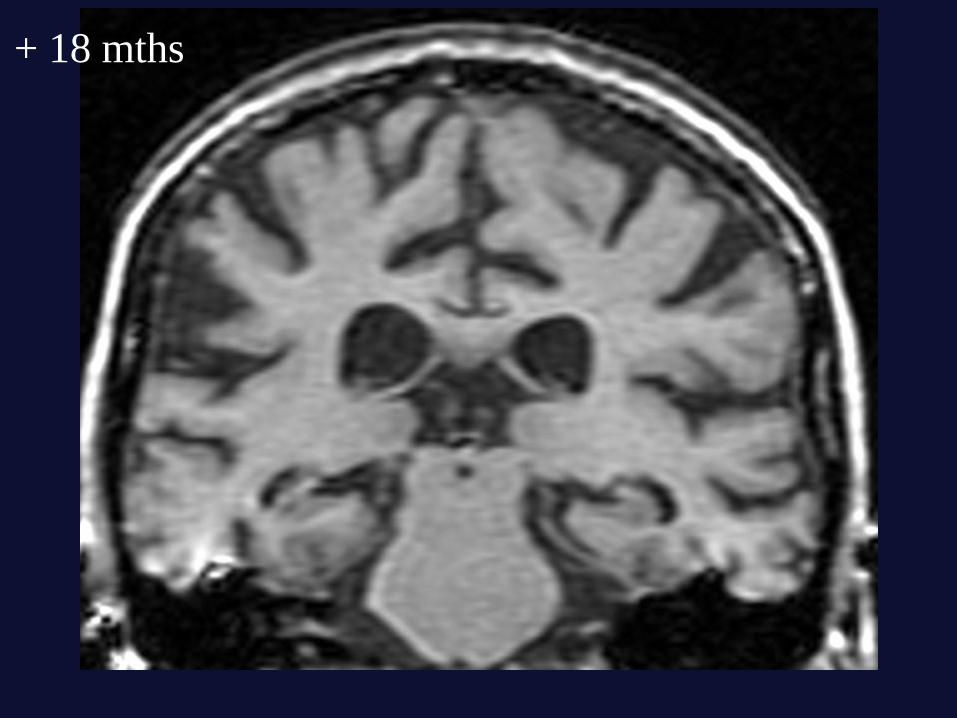
+ 18 mths

+ 36 mths

+ 42 mths
3%/yr loss

58 year old – c/o problems with vision and reading, memory not
a problem

Biparietal Alzheimer’s disease (PCA)

Symmetrical hippocampal atrophy is
characteristic of AD but also seen in
Dementia with Lewy Bodies
DLB AD PM proven

Low dopamine transporter uptake in
basal ganglia
AD DLB/PDD
Control PD
A “suggestive
feature” in
consensus criteria
for DLB (2005)
McKeith et al, 2005
O’Brien et al, 2004
Walker et al, 2002-8

Atrophy
• Focal?
• Pattern?
• Progressive?

FTD patterns…
• Behavioural variant FTD:
– Orbitofrontal or dorsolateral atrophy
• Changes in personality and social behaviour
– Right temporal (+frontal)
• Semantic dementia (svPPA):
– Ant>post; fusiform, pole
• Left: anomia, impaired comprehension & loss of word knowledge
• Right: behaviour
• Progressive nonfluent aphasia:
– Perisylvian – inf frontal
• Disrupted speech output, phonological deficits
• Cf Logopenic aphasia (AD)

Frontal

Semantic
dementia

Prosopagnosia

R L
PNFA
nfPPA

R L

Control
AD
FTLD
Jagust et al, Neurology 2007
Functional imaging: metabolic
patterns differ between diseases
FDG-PET
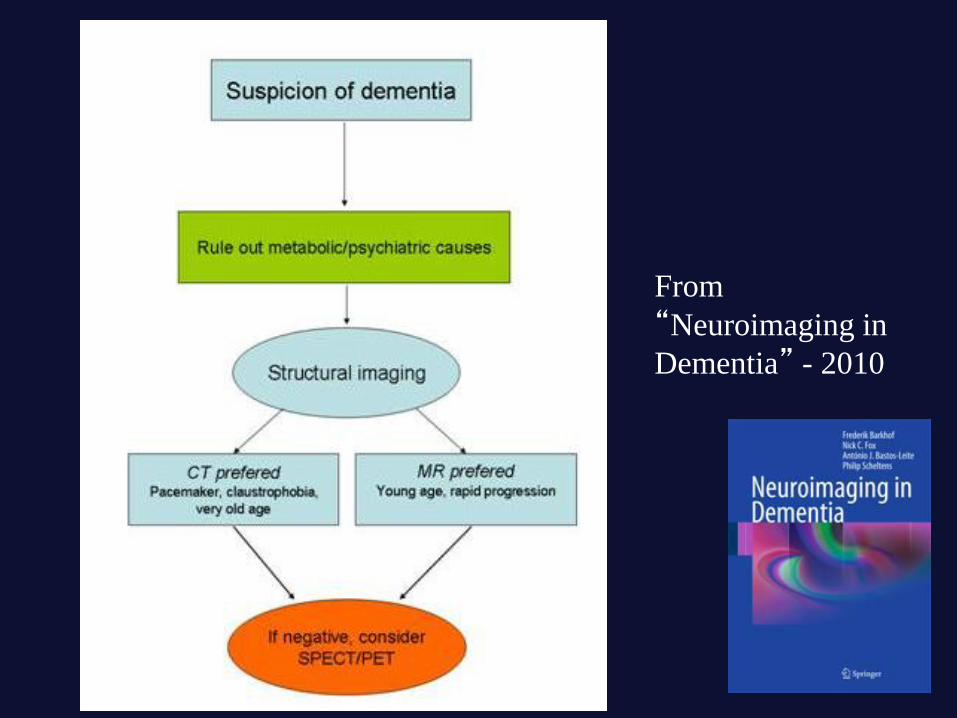
From
“Neuroimaging in
Dementia” - 2010

Research? Or the future of
clinical practice?
- an increasing range of
imaging modalities are
available

Structural imaging now can be accelerated –
retaining resolution and contrast
PM-proven AD: 1.5T MRI
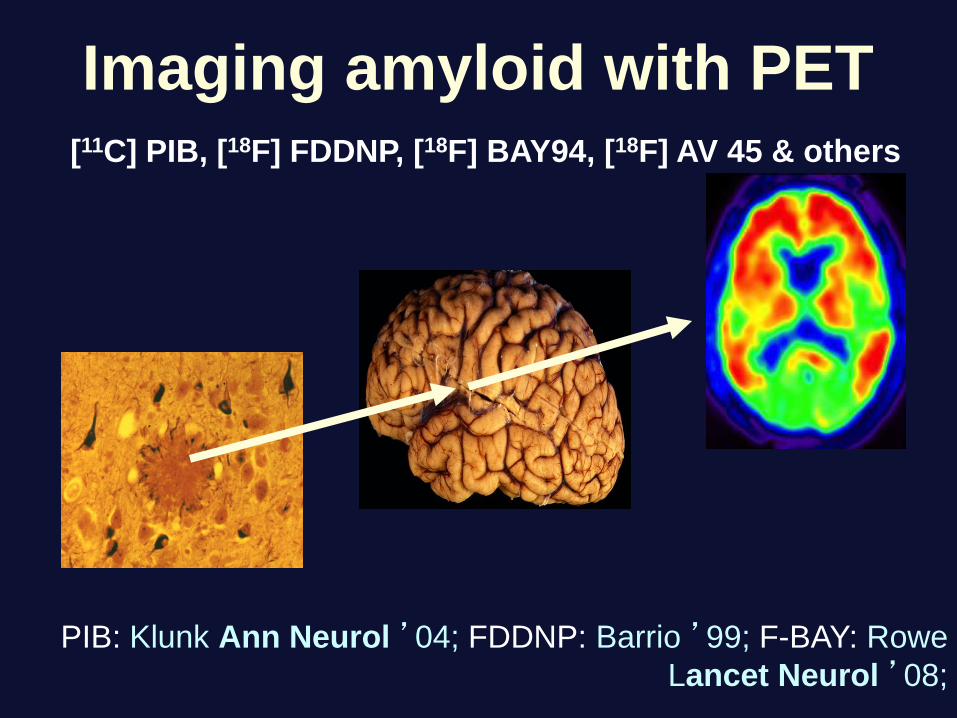
Imaging amyloid with PET
PIB: Klunk Ann Neurol ’04; FDDNP: Barrio ’99; F-BAY: Rowe
Lancet Neurol ’08;
[11C] PIB, [18F] FDDNP, [18F] BAY94, [18F] AV 45 & others

MCI non-converter MCI subject who
subsequently
converted to AD
Amyloid binding increases several
years before clinical AD
David Brooks, Hilary Archer, Aren Okello

Maruyama et al.
Neuron 2013
Tau-PET imaging with 11C-PBB3
In vitro binding to
Neurofibrillary tangles, neuropil threads and neurites in AD

How do the different
modalities associate with
each other?
Imaging posterior cortical
atrophy

Slattery CF et al Phenotypical variation in AD: insights from posterior cortical atrophy. Pract
Neurol 2014.
Profiles of atrophy, glucose metabolism and amyloid deposition in a patient with atypical AD

Ossenkoppele R, et al Annals of Neurology 2014
Tau, amyloid, and hypometabolism in a patient with posterior cortical atrophy.
Profiles of atrophy, glucose metabolism and tau deposition in a patient with atypical AD

In practice
• All patients should have structural imaging –
in working age dementia this should be MRI
• Positive predictive value for AD of
hippocampal atrophy – and
posterior>anterior gradient
• Focal atrophy syndromes and heavy
vascular burden suggest non-AD diagnoses
• Consider diffusion imaging in rapid dementia

Conclusion
• Imaging in dementia of working age is an essential part of
diagnosis
– NICE guideline
– Diagnostic criteria for AD, vascular dementia and other dementias
• Only as good as the assessment – a structured approach
can be usefully applied by a non-radiologist
• Positive contribution to the diagnosis of dementia is
possible with imaging and is even more relevant in working
age dementia
Thank you

















