PHARMACOECONOMICS AND OUTCOMES IN PAIN ANDPALLIATIVE CARE
Therapeutic Options for the Treatment of PostherpeticNeuralgia: A Systematic Review
Tina Khadem and Vanessa Stevens
ABSTRACT
Postherpetic neuralgia (PHN) is a chronic and painful condition that may result in significant disturbances tonormal activities and decreases in the quality of life for those affected. Despite the availability of several first-and second-line treatment options, many patients may experience refractory pain. The objectives of this reviewwere to summarize evidence for Food and Drug Administration (FDA)-approved and off-label therapies for thetreatment of PHN and to present gaps in the current literature for future research focus. Several agents, includ-ing pregabalin, gabapentin, and opioids, have been shown to significantly improve pain when compared withplacebo. However, evidence regarding the comparative effectiveness of these treatment alternatives is lacking.In order to choose the optimal treatment, providers should consider issues related to efficacy, safety, and tol-erability in conjunction with patient goals, preferences, and adherence issues. Evidence from randomized orobservational studies that directly compare agents with each other should help to inform treatment choices.
Postherpetic neuralgia (PHN) is the most commoncomplication following an acute herpes zoster (AHZ;shingles) infection. AHZ is a blistering skin rash thatresults from the reactivation of varicella, the viralinfection responsible for chicken pox. Following theinitial varicella infection, virus persists in an inactivestate in the ganglia of spinal cord and cranial nervesfor decades. The symptoms of AHZ typically resolveafter a few weeks, but in a proportion of patients, sen-sory nerve damage caused by the reactivation of virusresults in pain lasting more than 3 months.1 Varicellainfection is nearly universal in developed countries,
Tina Khadem, PharmD, is a postdoctoral associate with the Depart-ment of Pharmacy Practice, SUNY Buffalo School of Pharmacy and Phar-maceutical Sciences, Buffalo, New York, USA, and the Department ofPharmacy, University of Rochester Medical Center, Rochester, New York,USA. Vanessa Stevens, PhD, is research assistant professor in the Pharma-cotherapy Outcomes Research Center, Department of Pharmacotherapy,University of Utah College of Pharmacy, Salt Lake City, Utah, USA.
Address correspondence to: Vanessa Stevens, PhD, Department of Pharma-cotherapy, University of Utah College of Pharmacy, 30 S 2000 E RM 105,Salt Lake City, Utah 84112-5820, USA (E-mail: [email protected]).
resulting in a large population at risk for reactivationand the development of AHZ.2 Up to 33% of indi-viduals are affected by AHZ at some point in theirlifetime, and 10% of those go on to develop PHN.3
Symptoms of PHN include itching, burning, andstabbing, shooting, or throbbing pains. In most casesof PHN, the pain lasts for several months followingthe resolution of AHZ, but in approximately 2% ofpatients, the pain can persist for 5 years or more.4
Advanced age is an important risk factor for PHN,with nearly 75% of cases of PHN being observedamong individuals aged 60 years and older.5 PHNis a debilitating condition, often accompanied byallodynia, which is excessive pain following minorphysical stimuli. PHN patients frequently experiencesleep disturbances and other normal functions.1
Currently, the only therapies that are Food andDrug Administration (FDA)-approved for the treat-ment of postherpetic neuralgia are the lidocaineand capsaicin patches, gabapentin, and pregabalin.Therapies that are commonly used off-label or over-the-counter for PHN include tricyclic antidepres-sants (TCAs), selective serotonin reuptake inhibitors(SSRIs), opioids, antiepileptics, and nonsteroidal
1
J Pa
in P
allia
t Car
e Ph
arm
acot
her
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tex
as S
tate
Uni
v Sa
n M
arco
s on
08/
23/1
3Fo
r pe
rson
al u
se o
nly.
2 Pharmacoeconomics and Outcomes in Pain and Palliative Care
anti-inflammatory drugs (NSAIDs). Despite the va-riety of treatment options available, a proportion ofpatients remain refractory to treatment, and in gen-eral PHN patients are thought to be undertreated.1,6
There are several reviews that address various aspectsof PHN therapy,2,6 including a recent meta-analysisfocused on the percent reduction in pain scoresamong patients enrolled in randomized controlledtrails.7 The purpose of this review is to summarize theevidence for currently available therapies, includingfrom nonrandomized trials, with a focus on a broaderrange of outcomes. We also highlight areas of futureresearch focus that will improve clinicians’ ability tooptimize treatment choices.
METHODS
Literature Search
A comprehensive literature search for studies thatevaluated the treatment of postherpetic neuralgiawas conducted using the PubMed and EMBASE(MAP to preferred terminology, including sub-terms/derivatives [explosion search]) search enginesusing the key word “postherpetic neuralgia.” Thesearch was limited to English-language studies andclinical trials. Identified studies included those thatevaluated postherpetic neuralgia treatment in termsof efficacy, safety, and tolerability. The same searchwas repeated including review article types, includ-ing systematic reviews and meta-analyses, in additionto clinical trials. Bibliographies of review articles weremanually searched for additional studies for inclusionin the current review.
Studies were excluded if they were conducted inhealthy volunteers or in patients with acute herpeticpain, evaluated pharmacokinetic parameters only,evaluated the prevention of postherpetic neuralgia, orevaluated the use of herbal medications or nonphar-macologic interventions. Studies were also excludedif (1) the study concerned drugs administered in com-bination with another treatment modality other thanpharmacologic (e.g., invasive treatment, acupunc-ture, psychological interventions, etc.); (2) methodswere not adequately described with regard to studydesign, intervention, and outcomes studied; (3) re-sults reported for postherpetic neuralgia were com-bined with other neuropathic pain syndromes; (4) re-sults for the primary outcome were only presentedgraphically and specific pain scores and P values werenot reported; or (5) the study described case reportsor case series. Although studies that included otherforms of neuropathic pain (e.g., diabetic neuropathicpain) were included in this review, they were only
included if results were reported separately for eachsubgroup of neuropathic pain. Finally, studies thatevaluated the use of agents that are no longer on themarket or investigational agents that were never mar-keted, or agents that are clinically out of favor (i.e.,dextromethorphan), were not included in this review.
Recently, Edelsberg and colleagues conducted asystematic review and meta-analysis of randomizedcontrolled trials that evaluated the efficacy, safety,and tolerability data of drugs used to treat posther-petic neuralgia.7 The review focused on a single pri-mary efficacy measure including the percentage re-duction in pain intensity from baseline to study endas measured by a numeric rating scale (NRS), visualanalog scale (VAS), or other interval scales. Addition-ally, they excluded published reports if they includeddrugs administered other than orally or via transder-mal route and clinical trials that were shorter than 4weeks, among other various exclusion criteria. Thecurrent review expands on the prior work through theinclusion of nonrandomized trials and the expansionof endpoint types in randomized controlled trials.
RESULTS
Study and Patient Characteristicsof Included Trials
A total of 495 clinical trials and 213 review arti-cles were identified using the search criteria speci-fied above in the PubMed and EMBASE databases.After filtering out duplicate studies between the twodatabases, 44 studies met the prespecified criteriafor inclusion in the review. These studies were pub-lished between the years of 1982 and 2012 and aresummarized in Tables 1–3.8–51 Although the focusof this review was on patients with postherpetic neu-ralgia (PHN) and 40 studies included patients withonly PHN, four studies also included patients withadditional forms of neuropathic pain, including dia-betic neuropathic pain and acute herpetic neuralgia.However, as mentioned previously, these studies re-ported results for each subgroup of neuropathic painseparately. Of the 44 included studies, 38 were ran-domized controlled trials (RCTs) of which 7 werecrossover studies and 27 were a parallel design. Twoof the RCTs were dose-response studies and twoRCTs were open-label, noninferiority studies. Sixnonrandomized trials were included in this review,the majority of which were prospective, open-label,noncomparator studies.
Of the RCTs included, agents that were the focusof more than one trial include amitriptyline (n = 5),nortriptyline (n = 4), capsaicin (n = 6), gabapentin
Journal of Pain & Palliative Care Pharmacotherapy
J Pa
in P
allia
t Car
e Ph
arm
acot
her
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tex
as S
tate
Uni
v Sa
n M
arco
s on
08/
23/1
3Fo
r pe
rson
al u
se o
nly.
T. Khadem and V. Stevens 3
(n = 8), pregabalin (n = 7), and lidocaine (n = 8).Opioids including tramadol, a partial mu-opioid re-ceptor agonist, were the topic of three RCTs. In-travenous magnesium and oral divalproex were eachthe topic of a single RCT in which they were bothcompared with placebo. Twenty of the RCTs wereplacebo-controlled, whereas 11 included active con-trols, and 7 included both placebo and active agentsas controls. Agents studied in the six nonrandom-ized trials include capsaicin, lidocaine, epidural mor-phine, oxcarbazepine, acyclovir, and levetiracetam.Only one of these six studies was a nonrandomized,placebo-controlled study. The remaining five werenoncomparative studies and were before-and-afterstudies that evaluated patient’s pain levels at baselineand after study drug was administered.
Outcomes Evaluated
Although various outcomes were evaluated amongthe studies included in this review, they can begrouped into five general categories: mean change inpain score (n = 20), response rate (n = 10), percentmean change in pain score (n = 8), absolute painscores at endpoint (n = 3), and time-to-event (n =3). The majority of studies evaluated mean change inpain score as the primary outcome, of which morethan half used an 11-point (0–10) numeric ratingscale (NRS) where “0” represents the least amountof pain or no pain and “10” represents worst imagin-able pain. The remaining studies that evaluated meanchange in pain score as the primary outcome used ei-ther the 10 cm (100 mm) visual analog scale (VAS)or a composite neuropathic pain score. Among thestudies that evaluated response rate, a clinically sig-nificant response was defined as a reduction in painscore by at least 50% on a VAS or at least 2 points ona numeric rating scale. One study evaluated responserate defined as a subjective response to pain on a ver-bal pain scale. Studies that evaluated percent meanchange in pain score used the NRS or VAS as previ-ously described. Finally, studies that evaluated time-to-event outcomes include two studies that evaluatedtime to study exit due to lack of efficacy and one studythat evaluated time to onset pain relief.
FDA-Approved Drugs for the Treatment ofPostherpetic Neuralgia (Table 1)
Currently, only four products are FDA-approved forthe treatment of PHN. These are (1) lidocaine 5%transdermal patch; (2) capsaicin 8% transdermalpatch; (3) gabapentin; and (4) pregabalin.
Lidocaine Transdermal PatchLidocaine 5% transdermal patch was compared withboth placebo and pregabalin among PHN patientsin studies included in this review. When comparedwith placebo, lidocaine 5% patch has been shown toprovide longer pain relief.9,14 Median time to studyexit due to treatment failure (defined as a decrease inpain relief score by at least two categories on a 6-itempain relief scale for two consecutive days) was greaterthan 14 days for lidocaine 5% patch and about 4 daysfor placebo (P < .001).9 At study completion, 78%of patients preferred treatment with lidocaine patchas compared with 9.4% that preferred placebo patch(P < .001). Similar results were seen in another studythat evaluated time-to-exit due to lack of efficacy, butresults were not significant in the full-analysis popula-tion or the per-protocol population studied.14 A thirdstudy that evaluated lidocaine 5% patch comparedwith a vehicle placebo patch assessed the effects oflidocaine patch on distinct neuropathic pain qualitiescommon to all neuropathic pain conditions, includ-ing PHN, by using a neuropathic pain scale (NPS).Only patients who reported moderate-to-severe painon the NPS (defined as a score ≥4/10 reported for atleast 6 of the 10 individual NPS items) at the time ofenrollment were included in the analysis. At week 3,the lidocaine patch improved all assessed pain qual-ities to a greater extent than the placebo patch. Thedifference (lidocaine minus placebo) in the mean re-duction in neuropathic pain (from baseline to week3) was 7.6 (P = .043).
Lidocaine 5% transdermal patch was also com-pared with pregabalin in an open-label, noninferior-ity study.13,15 Results were initially reported in thefull-analysis population where the percent of patientswith at least a 2-point reduction in pain score or whoachieved an overall score of 4 or less at week 4 was66.4% with the lidocaine patch and 61.5% with pre-gabalin (P = .002).13 Similar results were observedin the per-protocol population (82.1% lidocaine vs.65% pregabalin; P value not reported), and addi-tional analyses were conducted to assess the benefitsof combining both drugs in patients not respondingto either single agent.15 During combination treat-ment, mean pain scores improved along with allody-nia severity and quality of life. Patients who receivedpregabalin in addition to their existing lidocaine treat-ment demonstrated a mean decrease in the Short-Form McGill Pain Questionnaire (SF-MPQ) pain in-tensity from combination phase baseline by 27.8 ±21.6 points, whereas those who received lidocaine inaddition to their existing pregabalin treatment sawa decrease by 33.7 ± 22.75 points (no P values re-ported). Combination treatment was generally welltolerated.
Topical CapsaicinTwo of the included studies examined the effec-tiveness of topical capsaicin for the treatment ofPHN.16,17 Both of these studies compared the useof capsaicin 0.075% cream versus a vehicle placebocream, applied topically up to four times per day for6 weeks. Similar results were observed in these twostudies, where subjects treated with capsaicin 0.075%noted a statistically significant decrease in pain by15–30% and those given placebo actually noted anincrease in pain intensity of 1–5%. As these two stud-ies have demonstrated, patients achieved only mod-est pain relief with the low-concentration cream andrequired many applications per day. Additionally, be-cause capsaicin is a natural irritant found in hot pep-pers, common effects include burning and erythemawhen applied topically as an analgesic. The high-concentration transdermal capsaicin 8% patch alsoproduces a burning sensation, but only requires onesingle application for 60 minutes every 3 months.In studies that evaluated capsaicin 8% transdermalpatch, the patch site was pretreated with a topiclocal anesthetic, such as lidocaine cream, for 60minutes prior to administering the patch. The com-parator arm in these studies was treated with 0.04%capsaicin patch in order to produce the same burn-ing or tingling sensation on the skin but without pro-ducing a therapeutic effect of the high concentration.The absolute difference (capsaicin 8% minus con-trol) in pain intensity (baseline to endpoint) rangedfrom 6.6% to 28.3%.18–22 In the study that demon-strated the largest difference in absolute pain intensityof 28.3%, patients treated with capsaicin 8% patchsaw a 32.7% reduction in pain intensity during the4-week randomized study compared with 4.4% re-duction in the group treated with the 0.04% controlpatch (P = .003).19 An additional 34.1% reduction inpain intensity was observed in nine subjects who con-tinued in the open-label extension study (95% confi-dence interval [CI], 15.6–52.7%).
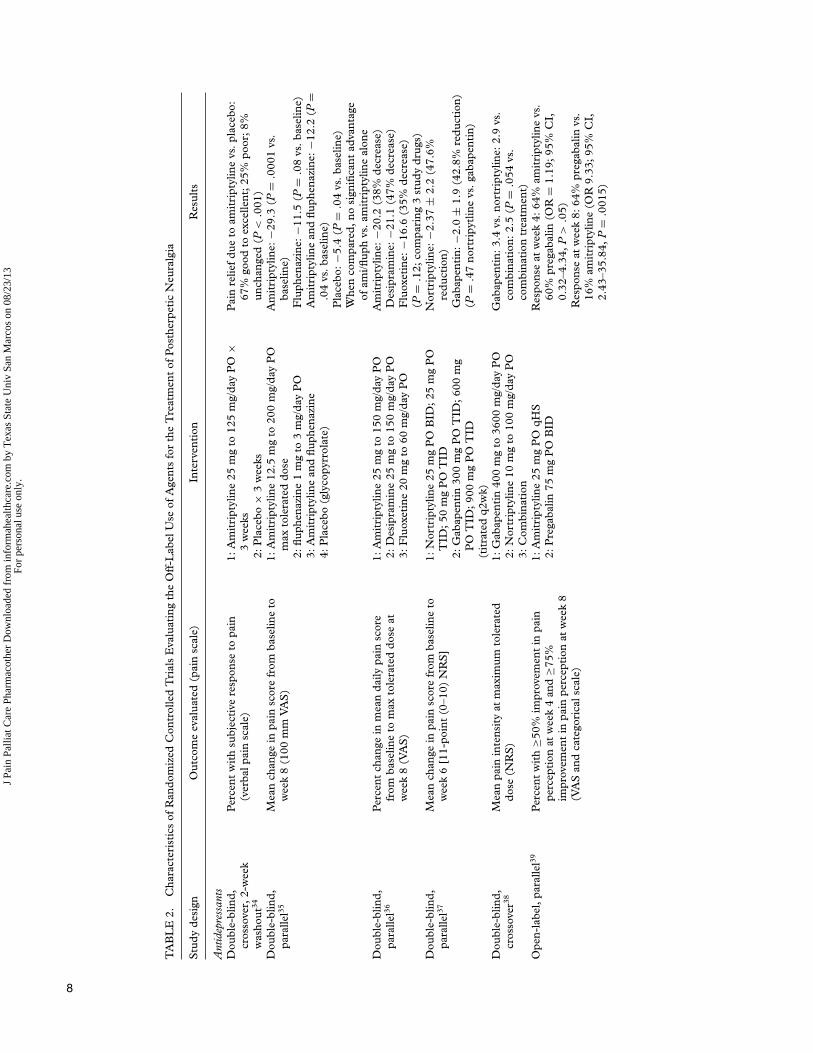
GabapentinoidsGabapentin and pregabalin are both FDA-approvedfor the treatment of neuropathic pain, includingPHN. They appear to have the same mechanismsof action, and have been shown to provide supe-rior pain relief compared with placebo. Among theincluded studies, doses of gabapentin were as highas 3600 mg/day and were often titrated to effect tothe maximum tolerated dose for the individual pa-tient. When compared with placebo, the difference(gabapentin minus placebo) in the percentage reduc-tion in pain intensity (from baseline to endpoint) var-ied from 11.5% (gabapentin extended-release [ER]1800 mg once daily vs. placebo; P = .089) to 25.6%
(gabapentin titrated to maximum tolerated dose upto 3600 mg/day vs. placebo; P < .001).23,30 Therewere no significant differences between gabapentinand nortriptyline, a tricyclic antidepressant (TCA)that is often used off-label for the treatment of neu-ropathic pain.37,38 Pregabalin has been shown to pro-vide significantly superior pain relief when comparedwith placebo and, similar to gabapentin, providedgreater pain relief at higher doses.25,26,28 In a 13-week,randomized, double-blind, placebo-controlled study,pregabalin provided significant, dose-proportionalpain relief at week 13 based on the last 7 days ofpatients’ daily pain diaries.28 The difference fromplacebo in mean pain scores for pregabalin 150,300, and 600 mg/day was −0.88 (95% CI, −1.53to −0.23; P = .0077), −1.07 (95% CI, −1.70 to−0.45; P = .0016), and −1.79 (95% CI, −2.43 to−1.15; P = .0003), respectively. Weekly mean painscores and sleep interference significantly improvedas early as week 1, and pregabalin’s effects were sus-tained throughout the study period.
Drugs Used Off-Label for the Treatmentof Postherpetic Neuralgia (Table 2)Antidepressant AgentsTricyclic antidepressants have been specifically stud-ied in patients with PHN but are not FDA-approvedfor this indication. Among the TCAs, amitriptylinehas been studied the most for PHN. When comparedwith placebo in a randomized, double-blind crossoverstudy, 67% of patients treated with amitriptyline re-ported “good to excellent” pain relief on a verbalpain scale (P < .001).34 The median reported dose ofamitriptyline was 75 mg and did not produce a signif-icant antidepressant effect in most patients, althoughthis falls within the FDA-approved dosing range of50 to 300 mg per day for depression. Amitriptylineappeared to produce greater pain relief from base-line compared with fluphenazine or a combinationof amitriptyline plus fluphenazine, with a difference(study drug minus placebo) in mean reduction in painscore of −23.9, −6.1, and −6.8, respectively.35 Nosignificant advantage was seen for combination ther-apy compared with amitriptyline alone. When com-pared with desipramine and fluoxetine, the percentreduction in mean daily pain score from baselineto maximum tolerated dose at week 8 was similar,with no significant differences among the three studydrugs.36 Amitriptyline has also been compared withpregabalin in a recent randomized, open-label com-parative study. Satisfactory improvement was definedas at least 50% improvement in pain perception atweek 4 and at least 75% improvement in pain per-ception at week 8 as measured by visual analog scale
10 Pharmacoeconomics and Outcomes in Pain and Palliative Care
and categorical scale.39 The percentage of patientswith satisfactory improvement at week 4 was greaterin the amitriptyline group compared with the prega-balin group, but was not statistically significant (64%vs. 60%, respectively; odds ratio [OR] = 1.19; 95%CI, 0.32–4.34; P > .05). At week 8, 64% of patientsin the pregabalin group had satisfactory improvementcompared with 16% of patients in the amitriptylinegroup (OR = 9.33; 95% CI, 2.43–35.84; P = .0015).Although the rate of side effects was 1.6 times lower(OR = 1.64; 95% CI, 0.46–5.97) in the pregabalingroup than in the amitriptyline group, no patients dis-continued treatment due to side effects. The authorsof this study offer no further conclusions as to whythere was such a large difference in the percentage ofpatients who demonstrated satisfactory improvementat week 8 among the two treatment groups. Instead,they reference a study that demonstrated long-termtreatment with pregabalin may beneficial in patientswith PHN.
Nonsteroidal Anti-inflammatory Drugsand OpioidsWhen taken orally, nonsteroidal anti-inflammatorydrugs (NSAIDs) are generally not effective for treat-ing neuropathic pain. The only study identified forinclusion in this review that evaluated the use ofNSAIDs compared a topical aspirin mixture, in-domethacin mixture, and diclofenac mixture withplacebo in a double-blind crossover study.40 Thegreatest difference versus placebo was seen in the as-pirin group and only aspirin was statistically supe-rior to placebo. Opioids, on the other hand, havebeen shown to be particularly effective in treat-ing PHN when taken orally. Oxycodone, morphine,methadone, and tramadol, a partial opioid receptoragonist, have all demonstrated to be significantly su-perior to placebo.41–43 Morphine and methadone didnot demonstrate significant differences when com-pared with nortriptyline and desipramine.42
Other Antiepileptic AgentsIn addition to gabapentin and pregabalin de-scribed above, various antiepileptic agents havebeen evaluated for the use of neuropathic pain,but only one study met inclusion for this re-view. In an 8-week randomized, double-blind,placebo-controlled trial, patients treated withoral valproic acid 1000 mg/day had significantpain relief compared with patients treated withplacebo where VAS results decreased from 70.17 ±9.21 to 31.27 ± 29.74 (P < .0001).44 Valoproic acidwas generally well tolerated except in one patientwho developed severe vertigo after treatment for10 days.
Although it is not used clinically for the treatmentof PHN, intravenous magnesium sulfate has beenstudied in a small study of seven patients who pre-viously did not respond to therapy with anticonvul-sants and TCAs.45 Patients were randomly assignedto receive magnesium or placebo in a crossover de-sign with a 1-week washout period in between. Dur-ing intravenous administration of magnesium, painscores were significantly lower for magnesium com-pared with placebo at 20 and 30 minutes (P = .017)but not at 10 minutes. Intravenous magnesium wasconsidered to be safe, well tolerated, and effective inthese patients with PHN.
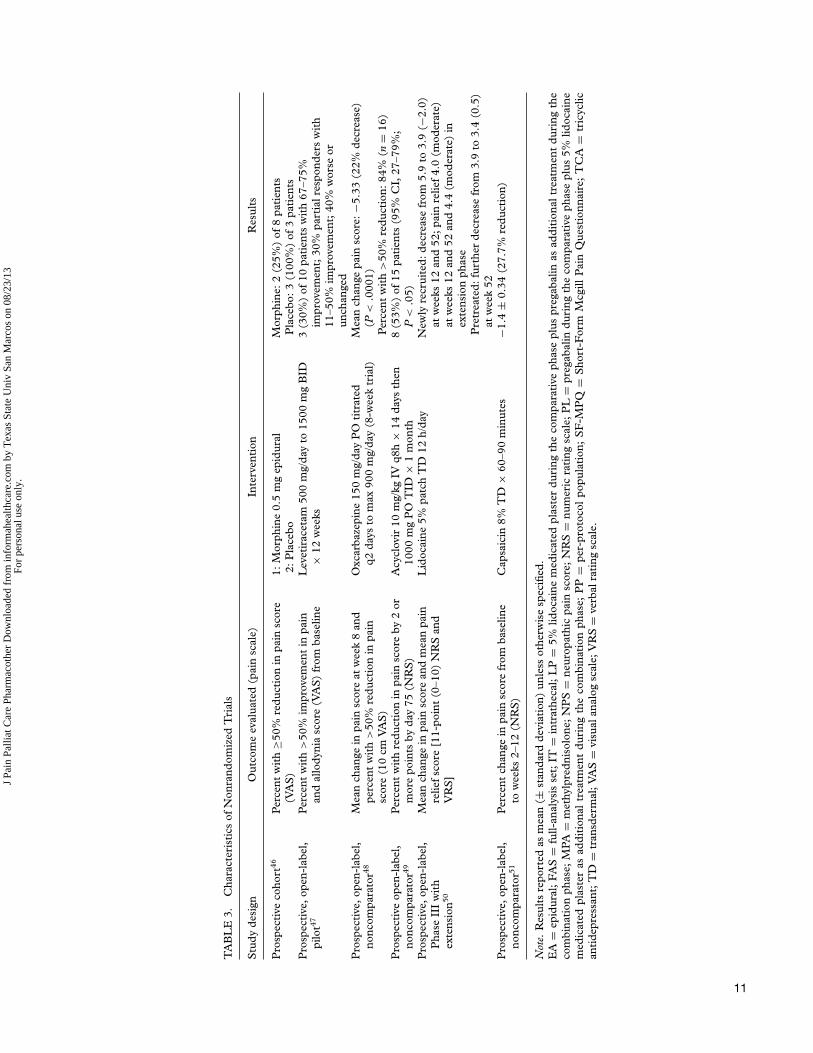
Evidence From Nonrandomized Studies(Table 3)The majority of studies evaluating treatment of PHNare randomized controlled trials. Surprisingly, PHNalone was not a topic of any retrospective cohort stud-ies or case-control studies. This is likely due to thefact that case-control studies are often used to evalu-ate risk factors associated with a disease, rather thandifferences in treatment. The lack of retrospective co-hort studies may be due to the limitation in retro-spectively identifying patients with a specific diagno-sis of postherpetic neuralgia as opposed to a moregeneral diagnosis of neuropathic pain in the medi-cal record. The few nonrandomized studies identifiedin this review were prospective, open-label, noncom-parator trials that evaluated the use of a single agentin PHN patients at baseline and posttreatment.47–51
One prospective cohort study with 11 patients wasidentified that evaluated the effectiveness of epidu-ral morphine as compared with placebo and foundthat epidural morphine produced more side effectsthan pain relief when administered to patients withPHN.46
Because PHN is a complication of varicella-zostervirus reactivation, there is some speculation thatlow-grade viral ganglionitis contributes to pain. Asa result, if chronic pain reflects active infection, an-tiviral therapy may play a role in relieving pain fromPHN.49 In a prospective, open-label trial conductedat a tertiary care university hospital, 15 patients withmoderate to severe PHN were given intravenousacyclovir 10 mg/kg every 8 hours for 14 days,followed by oral valacyclovir 1000 mg three timesdaily for 1 month.49 About 53% of patients reportedimprovement on a numeric rating scale for pain, asdefined by a decrease of 2 or more points on thescale. The authors concluded that the study demon-strated clinical improvement in most of the patients,warranting further investigation in larger, random-ized, double-blind, placebo-controlled trials. Similar
Journal of Pain & Palliative Care Pharmacotherapy
J Pa
in P
allia
t Car
e Ph
arm
acot
her
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tex
as S
tate
Uni
v Sa
n M
arco
s on
08/
23/1
3Fo
r pe
rson
al u
se o
nly.
TA
BL
E3.
Cha
ract
eris
tics
ofN
onra
ndom
ized
Tri
als
Stu
dyde
sign
Out
com
eev
alua
ted
(pai
nsc
ale)
Inte
rven
tion
Res
ults
Pro
spec
tive
coho
rt46
Per
cent
wit
h≥5
0%re
duct
ion
inpa
insc
ore
(VA
S)
1:M
orph
ine
0.5
mg
epid
ural
2:P
lace
boM
orph
ine:
2(2
5%)
of8
pati
ents
Pla
cebo
:3(1
00%
)of
3pa
tien
tsP
rosp
ecti
ve,o
pen-
labe
l,pi
lot47
Per
cent
wit
h>
50%
impr
ovem
ent
inpa
inan
dal
lody
nia
scor
e(V
AS
)fr
omba
selin
eL
evet
irac
etam
500
mg/
day
to15
00m
gB
ID×
12w
eeks
3(3
0%)
of10
pati
ents
wit
h67
–75%
impr
ovem
ent;
30%
part
ialr
espo
nder
sw
ith
11–5
0%im
prov
emen
t;40
%w
orse
orun
chan
ged
Pro
spec
tive
,ope
n-la
bel,
nonc
ompa
rato
r48M
ean
chan
gein
pain
scor
eat
wee
k8
and
perc
ent
wit
h>
50%
redu
ctio
nin
pain
scor
e(1
0cm
VA
S)
Oxc
arba
zepi
ne15
0m
g/da
yP
Oti
trat
edq2
days
tom
ax90
0m
g/da
y(8
-wee
ktr
ial)
Mea
nch
ange
pain
scor
e:−5
.33
(22%
decr
ease
)(P
<.0
001)
Per
cent
wit
h>
50%
redu
ctio
n:84
%(n
=16
)P
rosp
ecti
veop
en-l
abel
,no
ncom
para
tor49
Per
cent
wit
hre
duct
ion
inpa
insc
ore
by2
orm
ore
poin
tsby
day
75(N
RS
)A
cycl
ovir
10m
g/kg
IVq8
h×
14da
ysth
en10
00m
gP
OT
ID×
1m
onth
8(5
3%)
of15
pati
ents
(95%
CI,
27–7
9%;
P<
.05)
Pro
spec
tive
,ope
n-la
bel,
Pha
seII
Iw
ith
exte
nsio
n50
Mea
nch
ange
inpa
insc
ore
and
mea
npa
inre
lief
scor
e[1
1-po
int
(0–1
0)N
RS
and
VR
S]
Lid
ocai
ne5%
patc
hT
D12
h/da
yN
ewly
recr
uite
d:de
crea
sefr
om5.
9to
3.9
(−2.
0)at
wee
ks12
and
52;p
ain
relie
f4.
0(m
oder
ate)
atw
eeks
12an
d52
and
4.4
(mod
erat
e)in
exte
nsio
nph
ase
Pre
trea
ted:
furt
her
decr
ease
from
3.9
to3.
4(0
.5)
atw
eek
52P
rosp
ecti
ve,o
pen-
labe
l,no
ncom
para
tor51
Per
cent
chan
gein
pain
scor
efr
omba
selin
eto
wee
ks2–
12(N
RS
)C
apsa
icin
8%T
D×
60–9
0m
inut
es−1
.4±
0.34
(27.
7%re
duct
ion)
Not
e.R
esul
tsre
port
edas
mea
n(±
stan
dard
devi
atio
n)un
less
othe
rwis
esp
ecifi
ed.
EA
=ep
idur
al;
FA
S=
full-
anal
ysis
set;
IT=
intr
athe
cal;
LP
=5%
lidoc
aine
med
icat
edpl
aste
rdu
ring
the
com
para
tive
phas
epl
uspr
egab
alin
asad
diti
onal
trea
tmen
tdu
ring
the
com
bina
tion
phas
e;M
PA=
met
hylp
redn
isol
one;
NP
S=
neur
opat
hic
pain
scor
e;N
RS
=nu
mer
icra
ting
scal
e;P
L=
preg
abal
indu
ring
the
com
para
tive
phas
epl
us5%
lidoc
aine
med
icat
edpl
aste
ras
addi
tion
altr
eatm
ent
duri
ngth
eco
mbi
nati
onph
ase;
PP
=pe
r-pr
otoc
olpo
pula
tion
;S
F-M
PQ
=S
hort
-For
mM
cgill
Pai
nQ
uest
ionn
aire
;T
CA
=tr
icyc
lican
tide
pres
sant
;TD
=tr
ansd
erm
al;V
AS
=vi
sual
anal
ogsc
ale;
VR
S=
verb
alra
ting
scal
e.
11
J Pa
in P
allia
t Car
e Ph
arm
acot
her
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tex
as S
tate
Uni
v Sa
n M
arco
s on
08/
23/1
3Fo
r pe
rson
al u
se o
nly.
12 Pharmacoeconomics and Outcomes in Pain and Palliative Care
results were seen in a randomized, double-blind,placebo-controlled study, but due to inadequatesample size this study was terminated early.52
Safety Data—Side Effects and Tolerability
No serious adverse events were reported in the studiesincluded in this review. This is consistent with mostrandomized controlled trials of drugs used for neuro-pathic pain due to the strict monitoring used in ran-domized controlled trials in general that minimizesthe potential inappropriate use of drugs. Therefore,safety and tolerability is reported in terms of the mostfrequently reported adverse events among the studiesincluded in this review.
Among studies that included safety data, themost common side effects observed were consis-tent depending on the agent and/or drug class stud-ied. The most common side effects observed withgabapentin and pregabalin, both of which act on theγ -aminobutyric acid (GABA) receptor, were dizzi-ness and somnolence. Tricyclic antidepressants as adrug class were most commonly associated with drymouth. Transdermal agents, including lidocaine andcapsaicin, were very well tolerated and generally pro-duced application site reactions, particularly localizedtingling sensation and erythema with capsaicin. Over-all, agents were well tolerated at the doses studied, al-though variation in dosage ranges used should be con-sidered. Due to individualized responses to the agentssuch as gabapentin, pregabalin, or the TCAs, dosesare often titrated to maximum effect while maintain-ing an acceptable level of side effects. With regard tothe use of transdermal lidocaine, the extent of the af-fected area may determine the number of lidocainepatches used at any one time.
DISCUSSION
Among the randomized controlled trials evaluatingneuropathic pain, postherpetic neuralgia has been thefocus of most behind that of diabetic neuropathy.Nevertheless, most systematic reviews of postherpeticneuralgia treatment have ignored the heterogeneity ofoutcome measures used to evaluate efficacy and havecombined results across clinical trials of broad classesof drugs with various mechanisms of action testedin patients with different types of neuropathic painsyndromes.7 Similar to the meta-analysis conductedby Edelsberg et al.,7 we attempted to evaluate the ef-ficacy, safety, and tolerability of drugs that have beenstudied in PHN patients alone due to the possibil-ity there may be considerable variation in the relativeimportance of different mechanisms of neuropathic
pain. Although our purpose of focusing on PHNalone was to minimize heterogeneity involved withcomparing data across multiple neuropathic pain syn-dromes, our conclusions are limited by the quality ofthe studies included in our review. Such limitationsinclude small sample size, heterogeneity in study de-sign of RCTs, and variety of outcomes evaluated andpain scales used. Additionally, comparing placebo-controlled studies with studies comparing two activeagents may not provide very meaningful conclusions.However, we felt it necessary to include these studiesin order to grasp a better understanding of what hasbeen trialed as potential treatment of PHN, includ-ing nonrandomized studies that may be the subjectof further investigation in well-designed, randomizedcontrolled clinical trials.
Gabapentin is one of the FDA-approved agentsfor PHN and has shown to be an effective treat-ment option. It appears to be dose dependent, wherehigher doses up to 3600 mg/day produced a largerreduction in pain intensity.23 In an open-label, dose-response study, gabapentin doses of 200, 400, and600 mg/day, each given for 3 days, produced clini-cally and statistically significant responses, with thehigher dosage providing a greater decrease in painscore.27 Gabapentin is rapidly absorbed when admin-istered orally, although bioavailability may decrease athigher doses due to saturation in the transport mech-anism that mediates absorption of the drug. Dosesmust be individualized based on pain response whilemaintaining an acceptable side effect profile.
Lidocaine 5% transdermal patch and capsaicin 8%transdermal patch are options when local, topicaltherapy is preferred. Although never compared head-to-head for the treatment of PHN, each have beenshown superior when compared with placebo. The li-docaine patch seems to be better tolerated than thecapsaicin patch, but requires more frequent applica-tion. Both topical agents commonly produce applica-tion site reactions, with capsaicin being more irritat-ing and severe, often requiring a numbing agents suchas lidocaine prior to application. However, a singleapplication of capsaicin 8% for 60 minutes has shownto provide relief for up to 12 weeks. Lidocaine patchesmay be cut and applied to several areas, and remainat the application site for 12 hours per day.
Although the majority of studies evaluating theuse of TCAs for the treatment of PHN studiedamitriptyline, evidence and clinical experiencessuggest that nortriptyline and desipramine may bebetter tolerated.53,54 One of the major limitationsof using TCAs is their side effect profile. The mostcommon side effect noted in the included studieswas dry mouth, although other side effects includefatigue, dizziness, sedation, constipation, urinary
Journal of Pain & Palliative Care Pharmacotherapy
J Pa
in P
allia
t Car
e Ph
arm
acot
her
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tex
as S
tate
Uni
v Sa
n M
arco
s on
08/
23/1
3Fo
r pe
rson
al u
se o
nly.
T. Khadem and V. Stevens 13
retention, and palpitations. Less common but po-tentially more severe side effects include blurredvision and QTc prolongation and therefore shouldbe used with caution in elderly patients and in thosewith a history of cardiac arrhythmias. Therapeuticmonitoring of serum blood concentrations may berequired. Opioids are considered to be as efficaciousas TCAs and are also generally reserved as second-or third-line agents. Although effective in treatingPHN, the development of tolerance and concernsof misuse and abuse often prevent opioids frombeing used as first-line agents. Opioids also have thepotential to produce unwanted side effects, includingsedation and constipation. These are of particularconcern in the elderly population who primarilysuffer from PHN. Therefore, if used, low dosesshould be initiated and titrated to effect, at whichpoint can then be converted to long-acting agents.
Valproic acid provided significant pain relief in pa-tients with PHN with very little incidence of adversereactions. However, because of the relatively smallsamples size of the study, further investigation in alonger trial in a larger group of patients is warranted.Levetiracetam and oxcarbazepine were also studiedin small noncomparative trials but require furtherinvestigation.
Although not routinely used, magnesium and ke-tamine have both been studied assuming that theN-methyl-D-aspartate (NMDA) receptor is involvedin the control of PHN. The NMDA receptor mayplay a role in the mechanisms underlying centralsensitization (wind-up) in the spinal cord, which isimportant for the establishment of several chronicneuropathic pain states.55 A centrally positioned mag-nesium ion blocks the NMDA receptor in its inactivestate. However, afferent activity in nociceptor fibersdislodges this central magnesium ion from the recep-tor, allowing calcium influx into the cell.45 Ketaminealso blocks the NMDA receptor and has been shownto reduce neuropathic pain and allodynia in patientswith chronic PHN.56,57 However, side effects of ke-tamine have limited its use in clinical practice.
Treatment of PHN can be very challenging forboth the patient and clinician. The FDA-approvedagents are often considered as possible first-lineagents, whereas opioids and antiepileptic agentsmay be considered second-line agents due to theirunlabeled indications. Although the FDA requiresdemonstration of efficacy in each neuropathic painsyndrome for label indication, there is a generalconsensus in the pain management community thatdrugs effective for the management of one type ofneuropathic pain syndrome, e.g., PHN, may also beuseful in another, e.g., diabetic peripheral neuropa-thy (DPN). Of note, TCAs are considered drugs of
choice for the treatment of neuropathic pain basedon number-needed-to-treat (NNT) analyses.58–61 Ina recent Cochrane Review, results demonstrated therewas no top-tier evidence for amitriptyline in treatingneuropathic pain or fibromyalgia.62 Despite the lackof solid evidence for a beneficial effect, the authors ofthis review suggested that the results of these stud-ies must be balanced against decades of successfultreatment in many patients with neuropathic pain orfibromyalgia.
Among the various antidepressants, only the TCAsand one serotonin and norepinephrine reuptakeinhibitor (SNRI), duloxetine, have evidence of con-sistent analgesic activity in neuropathic pain. Dulox-etine is FDA-approved for DPN and fibromyalgia,but not for PHN. The other two commercially avail-able SNRIs in the United States, venlafaxine andmilnacipran, are approved only for depression and fi-bromyalgia, respectively, in the United States. Mil-nacipran is also approved as an antidepressant inEurope. Fluoxetine, a selective serotonin reuptake in-hibitor (SSRI), has been studied in PHN patientsbut is not approved for the treatment of neuropathicpain.36 In randomized controlled trials, fluoxetinedemonstrated no significant difference from placebowhen controlled for the effect of mood.63
In patients with PHN intractable to first- andsecond-line pharmacologic therapies, adjunctivetherapies such as invasive modalities with spinalcord stimulation, acupuncture, and psychologicalinterventions could be considered, although theevidence for their effectiveness is outside of the scopeof this review. With regard to pharmacologic therapy,there were two studies identified that evaluated theuse of lidocaine plus methylprednisolone given viaintrathecal route for the treatment of intractablePHN.8,10 These both provided significant painrelief and may be considered by clinicians as alast-line treatment option in patients with intractablePHN.
CONCLUSIONS
The current systematic review has provided a sum-mary of agents evaluated among PHN patients. Aspreviously discussed, there are several limitations incomparing the data provided in these studies and ad-ditional studies are warranted. Specifically, studiescomparing agents with each other such as lidocaineversus pregabalin, gabapentin, or capsaicin may bebeneficial, since these agents have already been shownto be effective when compared with placebo. Addi-tionally, longitudinal observational studies would beparticularly useful in capturing the long-term risks
14 Pharmacoeconomics and Outcomes in Pain and Palliative Care
and benefits of these agents. Although the results ofthe nonrandomized studies are interesting, further in-vestigation of these agents is warranted. Nevertheless,important conclusions can be taken away from thisreview. There are several agents shown to be effec-tive in treating PHN, and these must be chosen basedon individuals’ goals of therapy and preferences. Forexample, the capsaicin 8% patch may be preferableto one who has a small localized area of neuropathicpain and would like to try the single application patchevery 12 weeks. However, if the area is more exten-sive and/or severe, the lidocaine 5% patch or systemictherapy with one of the FDA-approved agents may bemore advantageous. Oral antidepressants includingthe TCAs may be an option for patients who can ben-efit from the antidepressant effects as well. Opioidsmay be particularly useful in patients who are havingacute, severe pain in the inpatient setting and thensubsequently transitioned to an agent that is moreappropriate for long-term use, such as pregabalin orgabapentin. Finally, some may require a combina-tion of treatments, including those with intractablePHN who may require invasive therapy. Regard-less of the agent chosen, side effects and limitationsshould also be considered to provide safe and effectivetherapy.
Declaration of interest: The authors report no con-flicts of interest. The authors alone are responsible forthe content and writing of the paper.
REFERENCES
[1] Philip A, Thakur R. Post herpetic neuralgia. J Palliat Med.2011;14:765–773.
[2] Nalamachu S, Morley-Forster P. Diagnosing and managingpostherpetic neuralgia. Drugs Aging. 2012;29:863–869.
[3] Ragozzino MW, Melton LJ, 3rd, Kurland LT, Chu CP, PerryHO. Population-based study of herpes zoster and its sequelae.Medicine. 1982;61:310–316.
[4] Watson P. Postherpetic neuralgia. Am Fam Physician.2011;84:690–692.
[5] Yawn BP, Saddier P, Wollan PC, St Sauver JL, Kurland MJ, SyLS. A population-based study of the incidence and complicationrates of herpes zoster before zoster vaccine introduction. MayoClinic Proc. 2007;82:1341–1349.
[6] Saks GM. Unmet need in the treatment of postherpetic neural-gia. Am J Manag Care. 2013;19(1 Suppl):S207–S213.
[7] Edelsberg JS, Lord C, Oster G. Systematic review and meta-analysis of efficacy, safety, and tolerability data from randomizedcontrolled trials of drugs used to treat postherpetic neuralgia.Ann Pharmacother. 2011;45:1483–1490.
[8] Kikuchi A, Kotani N, Sato T, Takamura K, Sakai I,Matsuki A. Comparative therapeutic evaluation of intrathecalversus epidural methylprednisolone for long-term analgesia inpatients with intractable postherpetic neuralgia. Region AnesthPain Med. 1999;24:287–293.
[9] Galer BS, Rowbotham MC, Perander J, Friedman E. Topicallidocaine patch relieves postherpetic neuralgia more effectivelythan a vehicle topical patch: results of an enriched enrollmentstudy. Pain. 1999;80:533–538.
[10] Kotani N, Kushikata T, Hashimoto H, et al. Intrathecal methyl-prednisolone for intractable postherpetic neuralgia. N Engl JMed. 2000;343:1514–1519.
[11] Galer BS, Jensen MP, Ma T, Davies PS, Rowbotham MC. Thelidocaine patch 5% effectively treats all neuropathic pain qual-ities: results of a randomized, double-blind, vehicle-controlled,3-week efficacy study with use of the neuropathic pain scale. ClinJ Pain. 2002;18:297–301.
[12] Amjad M, Mashhood AA. The efficacy of local infiltration of tri-amcinolone acetonide with lignocaine compared with lignocainealone in the treatment of postherpetic neuralgia. J Coll PhysiciansSurgeons Pakistan. 2005;15:683–685.
[13] Baron R, Mayoral V, Leijon G, Binder A, Steigerwald I,Serpell M. 5% lidocaine medicated plaster versus pregabalin inpost-herpetic neuralgia and diabetic polyneuropathy: an open-label, non-inferiority two-stage RCT study. Curr Med Res Opin.2009;25:1663–1676.
[14] Binder A, Bruxelle J, Rogers P, Hans G, Bosl I, Baron R.Topical 5% lidocaine (lignocaine) medicated plaster treatmentfor post-herpetic neuralgia: results of a double-blind, placebo-controlled, multinational efficacy and safety trial. Clin Drug In-vest. 2009;29:393–408.
[15] Rehm S, Binder A, Baron R. Post-herpetic neuralgia: 5% lido-caine medicated plaster, pregabalin, or a combination of both?A randomized, open, clinical effectiveness study. Curr Med ResOpin. 2010;26:1607–1619.
[16] Bernstein JE, Korman NJ, Bickers DR, Dahl MV, Millikan LE.Topical capsaicin treatment of chronic postherpetic neuralgia. JAm Acad Dermatol. 1989;21(2 Pt 1):265–270.
[17] Watson CP, Tyler KL, Bickers DR, Millikan LE, Smith S,Coleman E. A randomized vehicle-controlled trial of topicalcapsaicin in the treatment of postherpetic neuralgia. Clin Ther.1993;15:510–526.
[18] Backonja M, Wallace MS, Blonsky ER, et al. NGX-4010, ahigh-concentration capsaicin patch, for the treatment of pos-therpetic neuralgia: a randomised, double-blind study. LancetNeurol. 2008;7:1106–1112.
[19] Backonja MM, Malan TP, Vanhove GF, Tobias JK. NGX-4010, a high-concentration capsaicin patch, for the treat-ment of postherpetic neuralgia: a randomized, double-blind,controlled study with an open-label extension. Pain Med.2010;11:600–608.
[20] Webster LR, Tark M, Rauck R, Tobias JK, Vanhove GF. Ef-fect of duration of postherpetic neuralgia on efficacy analyses ina multicenter, randomized, controlled study of NGX-4010, an8% capsaicin patch evaluated for the treatment of postherpeticneuralgia. BMC Neurol. 2010;10:92.
[21] Webster LR, Malan TP, Tuchman MM, Mollen MD,Tobias JK, Vanhove GF. A multicenter, randomized, double-blind, controlled dose finding study of NGX-4010, a high-concentration capsaicin patch, for the treatment of postherpeticneuralgia. J Pain. 2010;11:972–982.
[22] Irving GA, Backonja MM, Dunteman E, et al. A multi-center, randomized, double-blind, controlled study of NGX-4010, a high-concentration capsaicin patch, for the treat-ment of postherpetic neuralgia. Pain Med. 2011;12:99–109.
[23] Rowbotham M, Harden N, Stacey B, Bernstein P, Magnus-Miller L. Gabapentin for the treatment of postherpeticneuralgia: a randomized controlled trial. JAMA. 1998;280:1837–1842.
Journal of Pain & Palliative Care Pharmacotherapy
J Pa
in P
allia
t Car
e Ph
arm
acot
her
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tex
as S
tate
Uni
v Sa
n M
arco
s on
08/
23/1
3Fo
r pe
rson
al u
se o
nly.
T. Khadem and V. Stevens 15
[24] Rice AS, Maton S. Gabapentin in postherpetic neuralgia:a randomised, double blind, placebo controlled study. Pain.2001;94:215–224.
[25] Dworkin RH, Corbin AE, Young JP Jr , et al. Pregabalin forthe treatment of postherpetic neuralgia: a randomized, placebo-controlled trial. Neurology. 2003;60:1274–1283.
[26] Sabatowski R, Galvez R, Cherry DA, et al. Pregabalin reducespain and improves sleep and mood disturbances in patientswith post-herpetic neuralgia: results of a randomised, placebo-controlled clinical trial. Pain. 2004;109:26–35.
[27] Jean WH, Wu CC, Mok MS, Sun WZ. Starting dose ofgabapentin for patients with post-herpetic neuralgia—a dose-response study. Acta Anaesthesiol Taiwanica. 2005;43:73–77.
[28] van Seventer R, Feister HA, Young JP Jr, Stoker M, VersavelM, Rigaudy L. Efficacy and tolerability of twice-daily prega-balin for treating pain and related sleep interference in posther-petic neuralgia: a 13-week, randomized trial. Curr Med Res Opin.2006;22:375–384.
[29] Stacey BR, Barrett JA, Whalen E, Phillips KF, Rowbotham MC.Pregabalin for postherpetic neuralgia: placebo-controlled trial offixed and flexible dosing regimens on allodynia and time to onsetof pain relief. J Pain. 2008;9:1006–1017.
[30] Irving G, Jensen M, Cramer M, et al. Efficacy and tolerabil-ity of gastric-retentive gabapentin for the treatment of posther-petic neuralgia: results of a double-blind, randomized, placebo-controlled clinical trial. Clin J Pain. 2009;25:185–192.
[31] Jensen MP, Chiang YK, Wu J. Assessment of pain quality ina clinical trial of gabapentin extended release for postherpeticneuralgia. Clin J Pain. 2009;25:286–292.
[32] Wallace MS, Irving G, Cowles VE. Gabapentin extended-release tablets for the treatment of patients with postherpeticneuralgia: a randomized, double-blind, placebo-controlled,multicentre study. Clin Drug Invest. 2010;30:765–776.
[33] Backonja MM, Canafax DM, Cundy KC. Efficacy ofgabapentin enacarbil vs placebo in patients with posther-petic neuralgia and a pharmacokinetic comparison with oralgabapentin. Pain Med. 2011;12:1098–1108.
[34] Watson CP, Evans RJ, Reed K, Merskey H, Goldsmith L, WarshJ. Amitriptyline versus placebo in postherpetic neuralgia. Neu-rology. 1982;32:671–673.
[35] Graff-Radford SB, Shaw LR, Naliboff BN. Amitriptyline andfluphenazine in the treatment of postherpetic neuralgia. Clin JPain. 2000;16:188–192.
[37] Chandra K, Shafiq N, Pandhi P, Gupta S, Malhotra S.Gabapentin versus nortriptyline in post-herpetic neuralgia pa-tients: a randomized, double-blind clinical trial–the GONIPTrial. Int J Clin Pharmacol Ther. 2006;44:358–363.
[38] Gilron I, Bailey JM, Tu D, Holden RR, Jackson AC, HouldenRL. Nortriptyline and gabapentin, alone and in combinationfor neuropathic pain: a double-blind, randomised controlledcrossover trial. Lancet. 2009;374:1252–1261.
[39] Achar A, Chakraborty PP, Bisai S, Biswas A, Guharay T. Com-parative study of clinical efficacy of amitriptyline and prega-balin in postherpetic neuralgia. Acta Dermatovenerol Croatica.2012;20:89–94.
[40] De Benedittis G, Lorenzetti A. Topical aspirin/diethyl ethermixture versus indomethacin and diclofenac/diethyl ether mix-tures for acute herpetic neuralgia and postherpetic neural-gia: a double-blind crossover placebo-controlled study. Pain.1996;65:45–51.
[41] Watson CP, Babul N. Efficacy of oxycodone in neuropathicpain: a randomized trial in postherpetic neuralgia. Neurology.1998;50:1837–1841.
[42] Raja SN, Haythornthwaite JA, Pappagallo M, et al. Opioidsversus antidepressants in postherpetic neuralgia: a randomized,placebo-controlled trial. Neurology. 2002;59:1015–1021.
[43] Boureau F, Legallicier P, Kabir-Ahmadi M. Tramadol inpost-herpetic neuralgia: a randomized, double-blind, placebo-controlled trial. Pain. 2003;104:323–331.
[44] Kochar DK, Garg P, Bumb RA, et al. Divalproex sodium in themanagement of post-herpetic neuralgia: a randomized double-blind placebo-controlled study. QJM. 2005;98:29–34.
[45] Brill S, Sedgwick PM, Hamann W, Di Vadi PP. Efficacy ofintravenous magnesium in neuropathic pain. Br J Anaesth.2002;89:711–714.
[46] Watt JW, Wiles JR, Bowsher DR. Epidural morphine for pos-therpetic neuralgia. Anaesthesia. 1996;51:647–651.
[47] Rowbotham MC, Manville NS, Ren J. Pilot tolerability andeffectiveness study of levetiracetam for postherpetic neuralgia.Neurology. 2003;61:866–867.
[48] Criscuolo S, Auletta C, Lippi S, Brogi F, Brogi A. Ox-carbazepine monotherapy in postherpetic neuralgia unrespon-sive to carbamazepine and gabapentin. Acta Neurol Scand.2005;111:229–232.
[49] Quan D, Hammack BN, Kittelson J, Gilden DH. Improve-ment of postherpetic neuralgia after treatment with intra-venous acyclovir followed by oral valacyclovir. Arch Neurol.2006;63:940–942.
[50] Hans G, Sabatowski R, Binder A, Boesl I, Rogers P, BaronR. Efficacy and tolerability of a 5% lidocaine medicated plas-ter for the topical treatment of post-herpetic neuralgia: re-sults of a long-term study. Curr Med Res Opin. 2009;25:1295–1305.
[51] Webster LR, Peppin JF, Murphy FT, Lu B, Tobias JK, VanhoveGF. Efficacy, safety, and tolerability of NGX-4010, capsaicin8% patch, in an open-label study of patients with peripheral neu-ropathic pain. Diabetes Res Clin Pract. 2011;93:187–197.
[52] Surman OS, Flynn T, Schooley RT, et al. A double-blind,placebo-controlled study of oral acyclovir in postherpetic neu-ralgia. Psychosomatics. 1990;31:287–292.
[53] Watson CP, Vernich L, Chipman M, Reed K. Nortriptyline ver-sus amitriptyline in postherpetic neuralgia: a randomized trial.Neurology. 1998;51:1166–1171.
[54] Dworkin RH, O’Connor AB, Backonja M, et al. Pharmacologicmanagement of neuropathic pain: evidence-based recommen-dations. Pain. 2007;132:237–251.
[55] Woolf CJ, Thompson SW. The induction and maintenance ofcentral sensitization is dependent on N-methyl-D-aspartic acidreceptor activation; implications for the treatment of post-injurypain hypersensitivity states. Pain. 1991;44:293–299.
[56] Hoffmann V, Coppejans H, Vercauteren M, Adriaensen H. Suc-cessful treatment of postherpetic neuralgia with oral ketamine.Clin J Pain. 1994;10:240–242.
[57] Eide PK, Jorum E, Stubhaug A, Bremnes J, Breivik H. Relief ofpost-herpetic neuralgia with the N-methyl-D-aspartic acid re-ceptor antagonist ketamine: a double-blind, cross-over compar-ison with morphine and placebo. Pain. 1994;58:347–354.
[58] Collins SL, Moore RA, McQuayHj, Wiffen P. Antidepressantsand anticonvulsants for diabetic neuropathy and postherpeticneuralgia: a quantitative systematic review. J Pain SymptomManage. 2000;20:449–458.
[59] Hempenstall K, Nurmikko TJ, Johnson RW, A’Hern RP, RiceAS. Analgesic therapy in postherpetic neuralgia: a quantitativesystematic review. PLoS Med. 2005;2:e164.
[62] Moore RA, Derry S, Aldington D, Cole P, Wiffen PJ. Amitripty-line for neuropathic pain and fibromyalgia in adults. CochraneDatabase Syst Rev. 2012;(12):CD008242.
[63] Max MB, Lynch SA, Muir J, Shoaf SE, Smoller B, Dubner R.Effects of desipramine, amitriptyline, and fluoxetine on pain indiabetic neuropathy. N Engl J Med. 1992;326:1250–1256.