35
TINNITUS BY:DR NDUATI J. MWANGI SUPERVISOR:DR MASINDE P. 02/08/14 (b)
| Date post: | 27-Dec-2015 |
| Category: |
Documents |
| Upload: | hilary-morrison |
| View: | 220 times |
| Download: | 0 times |

TINNITUS
BY:DR NDUATI J. MWANGISUPERVISOR:DR MASINDE P.
02/08/14 (b)

outline• Introduction • Epidemiology.• Types/classification.• Etiology .• Pathophysiology.• Features/measurements.• Diagnosis & investigations• Management • Conclusion

Introduction
• Tinnire – to ring. Tinnitus - ringing in the ear.• perception of sound in absence of stimulation /no
external acoustic source.• A Conscious experience of a sound that originates in
the head of the owner.• hissing, sizzling and buzzing, pulsatile• can be persistent, intermittent, or throbbing.• Tinnitus is an element of the symptom profile of
several significant otological pathologies.

Epidemiology
• In US,37-40M i.e 12-14% americans1.• 30% of adults,6% incapacitated• Peak age-40-70Yrs• M>F higher risk(12% M over 65,only 7% F)• Whites>blacks• prevalence increases with age & with HL• > risk in low economic status.
1.Heller AJ. Classification and epidemiology of tinnitus. Otolaryngol Clin N Am 2003;36:239-248.

Types/classification
• Subjective-has a neurophysiological origin • Objective
Vascular somatosoundsMorphologicalDynamic
Myogenic sounds Patulous ET TMJ abnormality SOAEs
1.Heller AJ. Classification and epidemiology of tinnitus. Otolaryngol Clin N Am 2003;36:239-248.

Objective -Pulsatile tinnitus
• AVMs• Vascular tumors• Venous hum• Atherosclerosis• Ectopic carotid artery• Persistent stapedial
artery• Dehiscent jugular bulb• Vascular loops
•Cardiac murmurs•Pregnancy•Anemia•Thyrotoxicosis•Paget’s disease•Benign intracranial hypertension

EtiologySubjective tinnitus:-• Otological:-noise ,infections,presbycusis,menieres,
otosclerosis, neuromas,cerumen,labyrinthitis.• Trauma-neck injuries,explosions,closed head injuries.• CNS disorders-meningitis.• Metabolic disorders, auto-immune disorders• Depression, anxiety• Medications, drug abuse

Mechanisms of tinnitus
• heterogeneity in the tinnitus population-many different mechanisms.
• Little known about physiologic mechanism• Modified neural activity in central auditory
system due to peripheral auditory structures damage2
• Cochlear ;Non-cochlear mechanisms of tinnitus generation
2.Eggermont JJ, Roberts LE. The neuroscience of tinnitus. Trends Neurosci. 2004;27:676–682.

Mechanisms of tinnitus
• Hyperactive hair cells or nerve fibers• Chemical imbalance• Reduced suppressive influence of CNS

Cochlear mechanisms• Discordant damage of IHC and OHC:-IHCs more
resistant to damage.3
• modification of auditory afferent activity leading to tinnitus perception
• SOAEs-rarely correspond to the judged frequency of the tinnitus4
• Biochemical models-Endogenous dynorphins(stress) potentiate glutamate within the cochlea5
3.Hazell JWP, Jastreboff PJ. Tinnitus. I. Auditory mechanisms: a model for tinnitus and hearing impairment. J Otolaryngol 1990; 19: 1–54.Penner MJ. An estimate of the prevalence of tinnitus caused by spontaneous otoacoustic emissions. Arch Otolaryngol Head Neck Surg 1990; 115: 871–55.Sahey TL, Nodar RH. A biochemical model of peripheral tinnitus. Hear Res 2001; 152: 43–54
Non-cochlear mechanisms
• Jastreboff neurophysiological model6-auditory perceptual, emotional and reactive systems
• Increased neural activity- dorsal cochlear nucleus (DCN), IC,cortical activity.
• Analogies with pain7
– chronic pain– phantom pain:-Cortical re-organisation
6.Jastreboff PJ, Gray WC, Gold SL. Neurophysiological approach to tinnitus patients. Am J Otol 1996;17:236-240.7.Moller AR. Similarities between severe tinnitus and chronic pain. J Am Acad Audiol 2000; 11: 115–24
Pathophysiology• Modified neural activity in central auditory
system due to peripheral auditory structures damage
• Tonotopic frequency matching from periphery to cortex is altered.
• increased spontaneous firing & increased fqcy presentation of bordering neurons( plasticity)
• detrimental cortical adaptation to input deprivation from the sensory periphery
8.Kitahara M. Tinnitus Pathophysiology and Management. Igaku-Shoin: Tokyo, New York; 1998. 9.Moller AR. Pathophysiology of tinnitus. Otolaryngol Clin N Am 2003;36:249-266

Pathophysiology cont’d
• These changes lead to abnormal interaction btn auditory & other central pathways.
• Mechanism by which other symptoms e.g depression,fear & anxiety are produced.
• Coupling of auditory system with other central systems like limbic & autonomic NS6 –basis of neuro-physiological approach to tinnitus.
6.Jastreboff PJ, Gray WC, Gold SL. Neurophysiological approach to tinnitus patients. Am J Otol 1996;17:236-240.
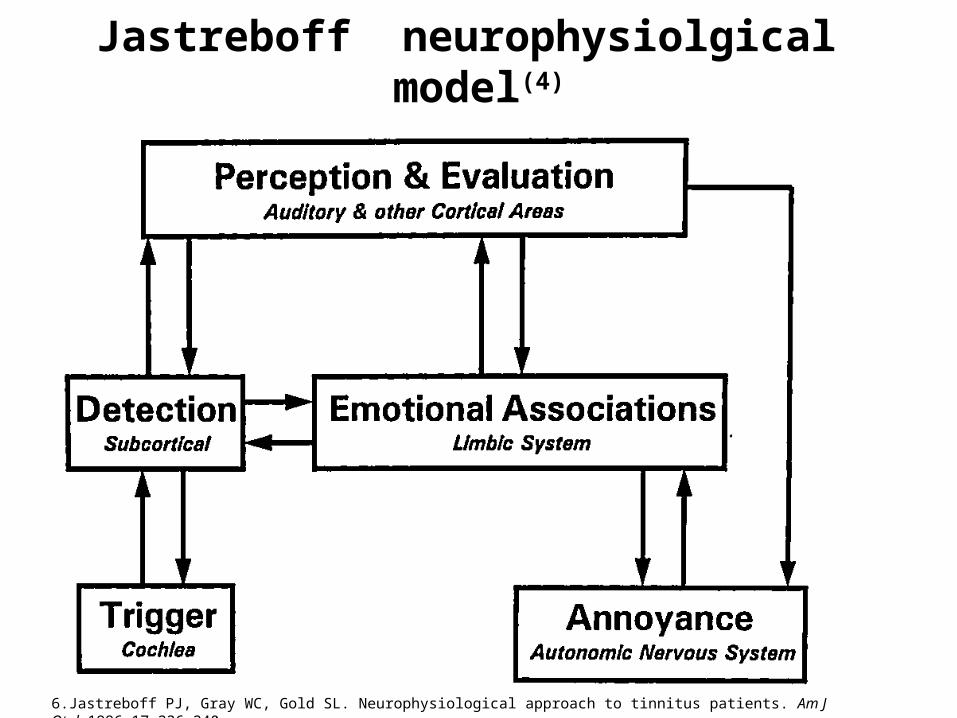
Jastreboff neurophysiolgical model(4)
6.Jastreboff PJ, Gray WC, Gold SL. Neurophysiological approach to tinnitus patients. Am J Otol 1996;17:236-240.

Neurophysiological model cont’d(4)
• Principally,auditory pathway & several non auditory systems play essential role in tinnitus.
• Stresses non auditory system dominates in determining annoyance level.
• Proposis treatment by inducing & facilitating habituation to tinnitus signal.
• Goal-to reach level though patient percieves tinnitus as unchanged,they arent aware of it &/or no annoyance occurs.
6.Jastreboff PJ, Gray WC, Gold SL. Neurophysiological approach to tinnitus patients. Am J Otol 1996;17:236-240.

Acoustic features(measurement)
• Clinically not as relevant.mainly in research.• Pitch-equate a pure tone pitch to that of
tinnitus.• Loudness-most <7 dBel• Minimum masking level-no of dBels of sound
required to cover tinnitus.• Residual inhibition(postmasking effects)-
periods of decreased or no tinnitus after masking.
Clinical measures• evaluate presence & severity of the tinnitus.• VAS assess loudness, pitch, & disturbance of the
tinnitus• Tinnitus Handicap Inventory • Tinnitus Reaction Questionnaire• Tinnitus Functional Index-severity,negative
impact,Rx-related changes
Tinnitus in children• Underestimated-no vocabulary to explain,may
consider it normal,fear to disclose(withdrawal)• Look for changes in attention,depression,poor
school performance,insomnia.• 6-13% 10 of children with normal hearing on &off• 24-29% -with hearing difficulties.• Causes-inborn,ME infections,wax, deafness,
noise,meningitis,asprin ,ET dysfunction.
10.Baguley DM, McFerran DJ. Current perspectives on tinnitus. Arch Dis Child 2002; 86: 141–3

Diagnosis/evaluation• Thorough History & PE.-etiology may be picked. History:- • noise exposure/trauma• HL & vertigo+/- dizziness,otalgia,• Quality- buzzing,rushing, roaring ,flactuating.• Trauma- head/neck• Medical history• Medications/drug use• Depression/somatoform disorders• Tinnitus handicup inventory.
11.Denk DM, Ehrenberger K. Tinnitus: causes, diagnosis, therapy Wien Med Wochenschr, 142(11-12):259-62 12..Schwaber MK. Medical evaluation of tinnitus. Otolaryngol Clin N Am 2003;36:287-292. .

Physical examination
• General exam vital.• Thorough H/N exam.• Otoscopy-wax,glomus,dehiscent jugular bulb
etc• Auscultation –bruit,venous hums• Light exercise,neck compression,valsalva
manoeuvers.• Audiometric tests-PTA ,speech, impedence
testing, OAE,

Investigations• No diagnostic modality to objectively measure
or confirm tinnitus.• FBC,ESR,U&Es..VDRL,HIV.• CT scans, angiograhy, MRI, PET,Magnetic
studies especially for pulsatile tinnitus.

Management • Various treatments –unsuccessful/unproven• Cochlea,NTs &receptors,ion channels.• Treatment methods not able to reduce or
eliminate the sensation on any consistent basis
• no drug that has been approved specifically for its treatment
• Comorbidities- hearing loss, mental health problems, or sleep disorders.
• Medical/Physiological Treatments– Pharmacological Treatment– Transcranial Magnetic Stimulation– Complementary and Alternative Medicine Therapies
• surgical treatments• Sound treatments/technologies
– Hearing Aids– Cochlear Implants– Sound Generators– Tinnitus Retraining Therapy– Neuromonics Tinnitus Treatment 13-combines acoustic stimulation with
a structured program of counseling support by a clinician
13.anley PJ, Davis PB. Treatment of tinnitus with a customized, dynamic acoustic neural stimulus: underlying principles and clinical efficacy. Trends Amplif. 2008;12:210–22.

• Psychological/behavioral treatments– Cognitive Behavioral Therapy– Biofeedback, Education, and Relaxation Therapies– Progressive Tinnitus Management
Medical • Glutamate rerceptor antagonist –caroverine, memantine,
Acamprosate• activate GABA receptors• Antidepressants-amitriptyline,nortriptyline, trimipramine • Anxiolytics-Alprazolam-• Anticonvulsants- Carbamazepine, Gabapentin• Vasodilators/vasoactive substances- Prostaglandin E1• Selective serotonin-reuptake inhibitors: fluoxetine and
paroxetine • Lidocaine IV/transtympanic.
14.Ehrenberger K. Topical administration of Caroverine in somatic tinnitus treatment: proof-of-concept study. Int Tinnitus J. 2005;11:34–7.15.Bauer CA, Brozoski TJ. Effect of gabapentin on the sensation and impact of tinnitus. Laryngoscope. 2006;116:675–8116.Baldo P, Doree C, Lazzarini R, Molin P, McFerran D. Antidepressants for patients with tinnitus. Cochrane Database of Systematic Reviews. 2006;(Issue 4):CD003853
Others • Transcranial Magnetic Stimulation 17-
• proven effect in auditory hallucinations .• Reduction of tinnitus loudness
• Complementary and Alternative Medicine Therapies• Ginkgo Biloba Extract 18- glutamate antagonist, strong
anti-oxidant • Acupuncture 19, and hyperbaric oxygen• diet modifications eg avoid high-sodium foods,
caffeine, chocolate, and other stimulants
17Kleinjung T, Vielsmeier V, Landgrebe M, Hajak G, Langguth B. Transcranial magnetic stimulation: a new diagnostic and therapeutic tool for tinnitus patients. Int Tinnitus J. 2008;14:112–8.18.Hilton M, Stuart E. Ginkgo biloba for tinnitus. Cochrane Database Syst Rev 2004;(2):CD003852. PMID: 15106224. 19.Park J, White AR, Ernst E. Efficacy of acupuncture as a treatment for tinnitus: a systematic review. Arch Otolaryngol Head Neck Surg 2000 Apr;126(4):489-92. PMID: 10772302.

Cognitive-Behavioral Therapy (CBT)
• aim- to modify harmful behaviours & thoughts using “deconditioning” technique
• reduces arousal levels via relaxation therapy &changing –ve thoughts through cognitive therapy.
• Goebel et al 20 confirm the long-term benefits of CBT for tinnitus.
20.Goebel G, Kahl M, Arnold W, Fichter M. 15 years prospective follow-up study of behavioural therapy in a large samplke of inpatients with chronic tinnitus. Acta Otolaryngol. 2006;126:70–9.
Tinnitus Retraining Therapy
• Based on neurophysiological model.• Conditioned reflexes involving connections of
auditory with limbic & ANS are retrained such that the subconscious part of auditory pathway blocks the tinnitus signal.
• Acoustic input with unimportant information is ignored(habituation)
• Inducing & sustaining habituation of conditioned reflexes removes –ve impact of tinnitus
21.Jastreboff PJ, Jastreboff MM. Tinnitus retraining therapy for patients with tinnitus and decreased sound tolerance. Otolaryngol Clin N Am 2003;36:321-33622.Phillips JS, McFerran D. Tinnitus Retraining Therapy (TRT) for tinnitus. Cochrane Database Syst Rev 2010 Mar 17;(3):CD007330. PMID: 20238353.
TRT
• Goal-train CNS to interpret tinnitus as unimportant & ignore it.
• Has 2 components:- -intensive direct counselling. -sound therapy using sound generators which
emit low level broad band noise.• Not masking-cant habituate a signal that cannot
be detected.• Jastreboff 21 reported success in over 80% of his
cases.
21.Jastreboff PJ, Jastreboff MM. Tinnitus retraining therapy for patients with tinnitus and decreased sound tolerance. Otolaryngol Clin N Am 2003;36:321-336.
Biofeedback, Education, and Relaxation Therapies
• control or habituate to the perceived ringing and the subsequent distress.
• Biofeedback therapy-listens to audio signal from EMG of frontalis muscle
• reduces perceived ringing &muscle tension• strategies to self-manage their tinnitus.• Relaxation therapies -focus pt’s attention away
from the sound;psychologically improving symptoms.
23.Seidman MD, Babu S. Alternative medications and other treatments for tinnitus: Facts from fiction. Otolaryngol Clin N Am 2003;36:359-381.

Future
• PET /fMRI help in research into the mechanisms and hence treatment of tinnitus.
• Transcranial DC Stimulation(tDCS)• Transcranial magnetic stimulation.
24..Mirz F, Pedersen CB, Ishizu K, Johannsen P, Ovesen T, Stodkilde-Jorgensen H, Gjedde A. Positron emission tomography of cortical centes of tinnitus. Hear Res 1999;134:133-144..

Conclusion
• difficult to study and treat -no objective tools to quantify and measure.
• no therapeutically successful treatment in terms of medium or long term remission
• no universally accepted therapies for managing tinnitus
• interactions among the auditory, cognitive, affective, and mental health issues.

References 1.Heller AJ. Classification and epidemiology of tinnitus. Otolaryngol Clin N Am 2003;36:239-2482.Eggermont JJ, Roberts LE. The neuroscience of tinnitus. Trends Neurosci. 2004;27:676–6823.Hazell JWP, Jastreboff PJ. Tinnitus. I. Auditory mechanisms: a model for tinnitus and hearing impairment. J Otolaryngol 1990; 19: 1–54.Penner MJ. An estimate of the prevalence of tinnitus caused by spontaneous otoacoustic emissions. Arch Otolaryngol Head Neck Surg 1990; 115: 871–55.Sahey TL, Nodar RH. A biochemical model of peripheral tinnitus. Hear Res 2001; 152: 43–546.Jastreboff PJ, Gray WC, Gold SL. Neurophysiological approach to tinnitus patients. Am J Otol 1996;17:236-240.7.Moller AR. Similarities between severe tinnitus and chronic pain. J Am Acad Audiol 2000; 11: 115–248.Kitahara M. Tinnitus Pathophysiology and Management. Igaku-Shoin: Tokyo, New York; 1998. 9.Moller AR. Pathophysiology of tinnitus. Otolaryngol Clin N Am 2003;36:249-26610.Baguley DM, McFerran DJ. Current perspectives on tinnitus. Arch Dis Child 2002; 86: 141–311.Denk DM, Ehrenberger K. Tinnitus: causes, diagnosis, therapy Wien Med Wochenschr, 142(11-12):259-62 12..Schwaber MK. Medical evaluation of tinnitus. Otolaryngol Clin N Am 2003;36:287-292
.
References 13.anley PJ, Davis PB. Treatment of tinnitus with a customized, dynamic acoustic neural stimulus: underlying principles and clinical efficacy. Trends Amplif. 2008;12:210–2214.Ehrenberger K. Topical administration of Caroverine in somatic tinnitus treatment: proof-of-concept study. Int Tinnitus J. 2005;11:34–7.15.Bauer CA, Brozoski TJ. Effect of gabapentin on the sensation and impact of tinnitus. Laryngoscope. 2006;116:675–8116.Baldo P, Doree C, Lazzarini R, Molin P, McFerran D. Antidepressants for patients with tinnitus. Cochrane Database of Systematic Reviews. 2006;(Issue 4) 17Kleinjung T, Vielsmeier V, Landgrebe M, Hajak G, Langguth B. Transcranial magnetic stimulation: a new diagnostic and therapeutic tool for tinnitus patients. Int Tinnitus J. 2008;14:112–8.18.Hilton M, Stuart E. Ginkgo biloba for tinnitus. Cochrane Database Syst Rev 2004;(2):CD003852. PMID: 15106224. 19.Park J, White AR, Ernst E. Efficacy of acupuncture as a treatment for tinnitus: a systematic review. Arch Otolaryngol Head Neck Surg 2000 Apr;126(4):489-92. PMID: 10772302.:CD00385320.Goebel G, Kahl M, Arnold W, Fichter M. 15 years prospective follow-up study of behavioural therapy in a large samplke of inpatients with chronic tinnitus. Acta Otolaryngol. 2006;126:70–9.21.Jastreboff PJ, Jastreboff MM. Tinnitus retraining therapy for patients with tinnitus and decreased sound tolerance. Otolaryngol Clin N Am 2003;36:321-33622.Phillips JS, McFerran D. Tinnitus Retraining Therapy (TRT) for tinnitus. Cochrane Database Syst Rev 2010 Mar 17;(3):CD007330. PMID: 2023835323.Seidman MD, Babu S. Alternative medications and other treatments for tinnitus: Facts from fiction. Otolaryngol Clin N Am 2003;36:359-381. 24..Mirz F, Pedersen CB, Ishizu K, Johannsen P, Ovesen T, Stodkilde-Jorgensen H, Gjedde A. Positron emission tomography of cortical centes of tinnitus. Hear Res 1999;134:133-144..

THANK YOU

















