Page 1
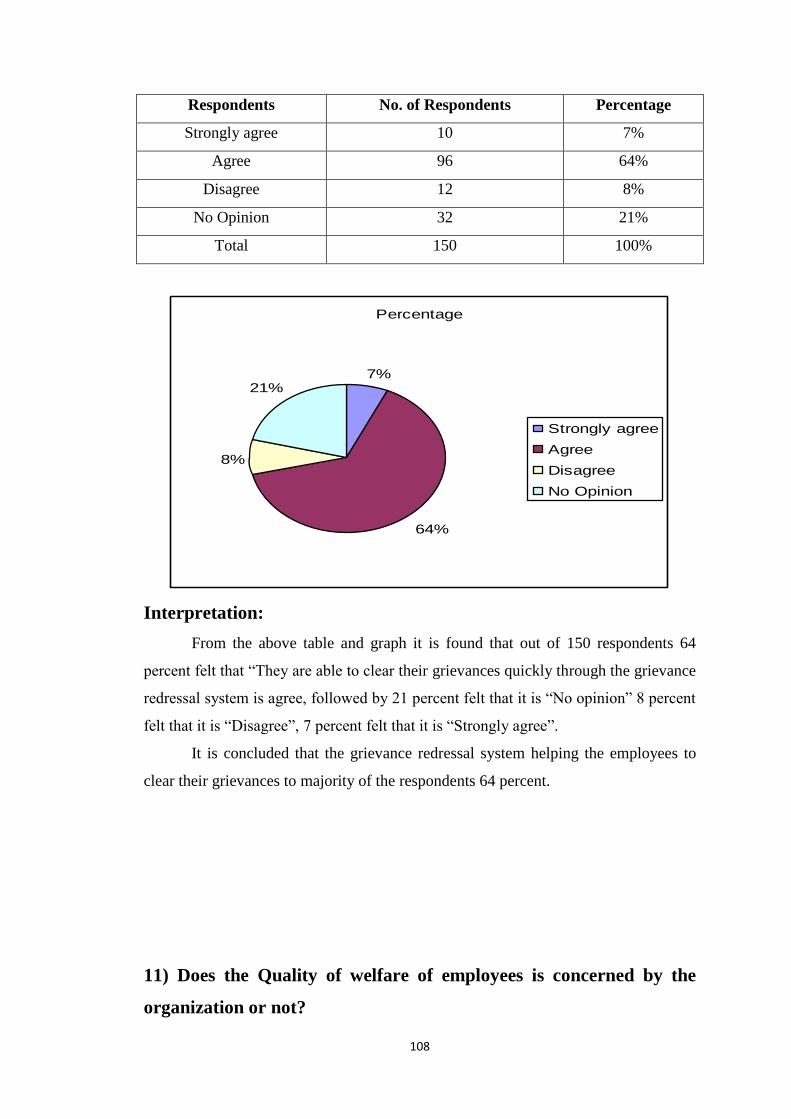
TOTAL QUALITY MANAGEMENT
(A Study With reference to CARE HOSPITAL ,HYDERABAD)
A Project report submitted to the Andhra University, Visakhapatnam in partial
l fulfillment for the award of the POST GRADUATE DEGREE
in
MASTER OF BUSINESS ADMINISTRATION
by
(Regd No.)
Under the Esteemed Guidance of
Mrs.V.V.V.PADMAJA, M.COM M.B.A,M.PHIL
Assistant Professor
DEPARTMENT OF MANAGEMENT STUDIES
SAMATA COLLEGE
(Affiliated to Andhra University and Approved by AICTE)
VISAKHAPATNAM - 530 017
2010-2012
Page 2
CERTIFICATE
This is to certify that the project work entitled “A STUDY ON TOTAL
QUALITY MANAGEMENT BASED ON STANDARD OPERATING
PROCEDURES” has been done by Mr under my guidance. It has been
compiled and submitted in partial fulfillment of the requirements for the award
of the post graduate degree in Master of Business Administration for the year
2010-2012
signature of the project guide
Station:
Date:
Page 3
3
DECLARATION
I hereby declare that the project work entitled “A STUDY ON
TOTAL QUALITY MANAGEMENT BASED ON STANDARD
OPERATING PROCEDURES” has been prepared by me in partial
fulfillment of the requirements for the degree of M.B.A. This project has
been compiled and submitted by me Under the guidance of Asst.Prof.
Mrs.V.V.V.Padmaja, Samata college and has not been submitted to any
other university or institute for the award of degree or diploma.
Place: Signature
Date:
Page 4
4
ACKNOWLEDGEMENT
I feel immense pleasure and pride of being part of SAMATA PG
COLLEGE that has nurtured me to the present state and I feel a deep sense of
gratitude towards it.
I heart fully thank Asst.Prof.V.V.V.PADMAJA. for her esteemed guidance,
valuable suggestions and continuous encouragement throughout the project.
I am profoundly thankful to DR.GURJIT SINGH MONGA (MAJOR) CHIEF
HOSPITAL ADMINISTRATOR, SRI RADHA MANOHAR H.R Manager AND
CORE H.R TEAM, NAMPALLY, HYDERBAD on providing me opportunity for
this study in their organization and for their cooperation in completion of this project
work.
I also sincerely thankful to our Director DR.B.MURALI KRISHNA & H.O.D
Ms. MADHAVI LATHA of Management studies and all other faculty members for
their continuous co-operation and guidance throughout my period of study in this
college.
I am very earnestly acknowledging my deep sense of gratitude, thankfulness to
all others those who extended their constant source of help and guidance to me in
carrying out this study and presenting this report successfully.
.
Page 5
5
INTRODUCTION
Total Quality Management (TQM) is a management approach that aims for
long-term success by focusing on customer satisfaction. TQM is based on the
participation of all members of an organization in improving processes, products,
services, and the culture in which they work.
―TQM is a process and philosophy of achieving best possible outcomes from
the inputs, by using them effectively and efficiently in order to deliver best value for
the customer, while achieving long term objectives of the organization‖
Total Quality (TQ) consists of continuous improvement activities involving
everyone in the organization—managers and workers—in a totally integrated effort
toward improving performance at every level. This improved performance is directed
toward satisfying such cross-functional goals as quality, cost, schedule, missing, need,
and suitability. TQ integrates fundamental management techniques, existing
improvement efforts, and technical tools under a disciplined approach focused on
continued process improvement. The activities are ultimately focused on increasing
customer/user satisfaction
CROSBY'S
Philip Crosby, author of Quality is Free, founded the Quality College in
Winter Park, Florida. Crosby emphasized meeting customer requirements by focusing
on prevention rather than correction. He claimed that poor quality costs about 20
percent of the revenue; a cost that could be avoided by using good quality practices.
He pushed for zero defects. His "absolutes" are: (1) quality is defined as conformance
to requirements, not goodness; (2) the system for achieving quality is prevention, not
appraisal; (3) the performance standard is zero defects, not that's close enough; and
(4) the measure of quality is the price of non-conformance, not indexes.
Page 6
6
The TQM Philosophy
Implementing a total quality management system has become the preferred
approach for improving quality and productivity in organizations. TQM, which has
been adopted by leading industrial companies, is a participative system empowering
all employees to take responsibility for improving quality within the organization.
Instead of using traditional bureaucratic rule enforcement. TQM calls for a change in
the corporate culture, where the new work climate has the following characteristics.
An open, problem-solving atmosphere;
Participatory design making
Trust among all employees (staff, line, workers, managers);
A sense of ownership and responsibility for goal achievement and problems
solving; and
Self-motivation and self-control by all employees.
The TQM approach involves more than simply meeting traditional rejection
rate standards. The end result of TQM is the efficient and effective use of all
organizational processes in providing consistent quality at a competitive price. The
TQM philosophy is a long-term endeavor that links people and processes in a system
that alters the corporate culture to become one where quality is the core aspect of
business strategy.
In cultivating the TQM philosophy, strategy implementation must involve a
focused effort on the part of every employee within the organization. It cannot be
applied successfully on a piecemeal basis. TQM requires that management, and
eventually every member of the organization, commit to the need for continual
improvement in the may work is accomplished. Business plans, strategies, and
management actions require continual rethinking in order to develop a culture that
reinforces the TQM perspective. The challenge is to develop a robust culture where
the idea of quality improvement is not only widely understood across departments,
but becomes a fundamental, deep-seated value within each function area as well.
Page 7
7
HRM as a Role Model for TQM
HRM can jumpstart the TQM process by becoming a role model. This means
that HRM has two specific tasks: ―Serving our customers, and making a significant
contribution to running the business‖. This emphasis on customer oriented service
means that the HR department must see other departments in the firm as their
customer groups for whom making continuing improvements in service becomes a
way of life.
In their efforts to achieve total quality management, HRM can demonstrate
commitment to TQM principles by soliciting feedback from its internal customer
groups on current HR services. HRM should include suggestions from its customers
in setting objective performance standards and measures. In other words, there are a
number of specific TQM principles that the HR department can model.
Applying TQM Principles in HRM.
The current emphasis on quality as a competitive strategy has produced many
views regarding the actions necessary to achieve it. Leaders in the quality movement
(Deming, Juran, Crosby, and Feigenbaum) have proposed similar approaches which
share certain themes. These themes can be summarized as five basic principles:
Focus on customers‘ needs;
Focus on problem prevention, not correction;
Make continuous improvements; seek to meet customers‘ requirements on
time, the first time, every time
Train employees in ways to improve quality and
Apply the team approach to problem solving.
To institute total quality management as a philosophy within an organization, all
employees must come to realize that satisfying customers is essential to the long-run
well-being of the firm and their jobs. No longer is the customer-driven focus
exclusive to the marketing department. But customer satisfaction can only be
achieved after first defining the customer groups. The new perspective here is that all
Page 8
8
employees exist to serve their customer groups, some internal and some external to
the firm. The human resources department has internal customers to satisfy, which
indirectly provides ultimate satisfaction to external customers.
In addition to identifying customer groups, there are other essential TQM
customer issues. Clarifying what products and services will provide maximum
customer satisfaction, measuring satisfaction, and continually monitoring and
improving the level of customer satisfaction are all fundamental to the TQM
philosophy. For the HR department, applying these TQM issues would translate into
identifying the expectations of senior management- their principal internal customer-
regarding TQM, and spearheading the TQM program‘s implementation on the basis
of those expectations. TQM in practice for HRM might also mean periodic surveys,
both formal and face-to-face; to monitor senior management‘s levels of satisfaction as
the TQM process unfolds.
The TQM approach entails identifying the wants and needs of customer
groups and then propelling the entire organization toward fulfilling these needs. A
customer‘s concerns must be taken seriously, and organizations should make certain
that its employees are empowered to make decisions that will ensure a high level of
customer satisfaction. This can be achieved by promoting an environment of self-
initiative and by not creating a quagmire of standard operating procedures and
company policies. (7) Flexibility is the key, especially in a business environment that
is diverse and constantly changing, as most are today. In modeling these aspects of
the TQM process, the HR department would need to identify human resource
concerns of other departments and undertake to continually improve its performance,
especially in any trouble areas that come to light.
Based on this ―customer first‖ orientation, organizational members are
constantly seeking to improve products or services. Employees are encouraged to
work together across organizational boundaries. Underlying these cooperative efforts
are two crucial ideas. One is that the initial contact with the customer is critical and
influences all future association with that customer. The other idea is that it is more
costly to acquire new customers than to keep the customers you already have. (7)
Exemplifying TQM here would mean that the HR department would need to train
itself, focusing on being customer-driven toward other departments.
Page 9
9
Quality improvement programs typically involve the directed efforts of quality
improvement (Q1) teams. Using teams and empowering employees to solve quality-
related issues using such tools as statistical process control (SPC) represent
fundamental changes in how many businesses operate. The Focus of SPC, also
known as statistical quality control (SQC), is defect prevention as opposed to defect
correction. Defect prevention results from continuously monitoring and improving
the process. In this context ―process‖ refers to service delivery as well as
manufacturing. To ensure that output meets quality specifications, monitoring is
performed by periodically inspecting small samples of the product. SPC alone will
not ensure quality improvement; rather, it is a tool for monitoring and identifying
quality problems.
The effective use of quality improvement teams, and the TQM system as a
whole, can be reinforced by applying basic principles of motivation. In particular, the
recognition of team accomplishments as opposed to those of individuals, and the
effective use of goal setting for group efforts, are important in driving the TQM
system. The HR department is in a position to help institutionalize team approaches
to TQM by designing appraisal and reward systems that focus on team performance.
For many companies, the philosophy of TQM represents a major culture shift
away from a traditional production-driven atmosphere. In the face of such radical
operational makeovers, a determined implementation effort is vital to prevent TQM
from becoming simply platitudinal and the team approach just another management
fad. Senior management must take the lead in overt support of TQM.
Page 10
10
NEED FOR THE STUDY
CARE hospital is a specialized service for Cardiac surgery and with many other multi
specialty services for the last 14 years with an objective to serve the patients as they
can do. It has been serving the people with its main aim ―To put the patient first‖.
CARE hospital spread over the state to serve the people.
The purpose of the quality standards to determine what aspects of quality
is needed to be evaluated. The aim of the study is to know how far the quality human
resource policies and practices making the company to be successful in building the
H.R system and employees lifetime in the organization.
Keeping in view that the hospital which is recognized by NABH (national
accreditation board for hospitals).is itself a quality control tool for the organization to
work out its operations. Instead I made an observation on human resources policy and
procedures for quality management of employees in the organization which include a
study of manpower planning, training, recruitment, performance appraisal, best
associate awards and so on
We also made an observation on the policy and procedure follow-up in the
organization towards an employee, and which quality factors influencing the
employee to do service much better.
Page 11
11
OBJECTIVES
To study the overview of CARE GROUP in General and CARE
NAMPALLY in particular
To know upto what extent does the quality practices are being implemented.
To study quality control practices that is being practiced in the organization
with particular to Human Resource Department based on standard operating
procedures.
To analyze and examine the collected data
To suggest some measures for the improvement of the quality practices.
Page 12
12
METHODOLOGY
The research process will be clearly defined to meet the objectives of the
study. The logical analysis of various aspects of the data shall be made to arrive at the
results of the study. The research process shall include the following steps like.
Unit under study: CARE is a private organization which is the hospitality services
with a work force around 800 employees. It was established in the year 1997 by
Dr.B.Somaraju and Dr.D.Prasada Rao led a team of medical professionals to set up
the first CARE Hospitals.
Sampling Unit:Various departments at CARE
Sample size:In the present study of quality of human resource practices in CARE
HOSPITALS, 150 employees were selected randomly for sampling.
Departments of this Hospital are being:
1) Human Resource
2) Marketing
3) Accounts
4) Billing
5) Purchases
6) Stores
7) Pharmacy
8) Labs
9) Quality Department
10) HID
11) Administration
Page 13
13
12) Maintenance
Sampling Method:
The basic idea of sampling is that by selecting some of the elements in a
population we may draw conclusion about the entire population. This has an
important bearing on the collection of the reliable data of the present study is to
acquire an intensive opinion about the quality of human resource practices in
CARE HOSPITALS, NAMPALLY, HYDERABAD.
Geographic Area Covered: CARE is located at Hyderabad situated in Jawaharlal
Nehru Road, Nampally.
Data Collection: Collection of data is forming both the primary and secondary
sources.
Primary Data: Data is collected through a well designed and approved questionnaire
and also interviews.
Secondary Data: It is collected from the records of the organization, profile
booklets and from HRD Dept.
Magazines
Brochures
Prospectus
Internet
Data Analysis:
For analysis and interpreting the collected data through primary data is part to
statistical techniques namely, percentage analysis and graphical analysis with bar
charts & pie charts. It is used arriving at valid reliable conclusion
Page 14
14
LIMITATIONS
Confidentiality of information is also limiting factor for analysis of data.
The whole research study was carried out in hyderabad CARE hospital only
therefore the result may not not be same in all areas or cities.
Some of the finding have been taken in the research are based on opinion
attitude,feelings,and perception of few respondent .so we cannot take it as a
granted
Page 15
15
CHAPTER-2
INDUSTRY PROFILE
a) INTRODUCTION TO INDUSTRY
All India Institute of Medical Sciences in Delhi, India
A hospital, in the modern sense of the sentence, is an institution for health
care providing patient treatment by specialized staff and equipment, and often, but not
always providing for longer-term patient stays. Its historical meaning, until relatively
recent times, was "a place of hospitality", for example the Chelsea Royal Hospital,
established in 1681 to house veteran soldiers.
Today, hospitals are usually funded by the public sector, by health
organizations, (for profit or nonprofit), health insurance companies or charities,
including by direct charitable donations. Historically, however, hospitals were often
founded and funded by religious orders or charitable individuals and leaders.
Conversely, modern-day hospitals are largely staffed by professional
physicians, surgeons, and nurses, whereas in history, this work was usually performed
by the founding religious orders or by volunteers. Today, there are
various Catholic religious orders, such as the Alexians and the Bon Secours
Sisters which still focus on hospital ministry.
There are over 17,000 hospitals in the world
ETYMOLOGY
During the middle Ages hospitals served different functions to modern
institutions, being almshouses for the poor, hostels for pilgrims, or hospital. The word
hospital comes from the Latin hospes, signifying a stranger or foreigner, hence a
guest. Another noun derived from this, hospitium came to signify hospitality that is
the relation between guest and sheltered, hospitality, friendliness, hospitable
reception. By metonymy the Latin word then came to mean a guest-chamber, guest's
lodging, an inn.[2]
Hospes is thus the root for the English words host (where the p was
dropped for convenience of pronunciation) hospitality, hospice, hostel and hotel. The
latter modern word derives from Latin via the ancient French romance word hostel,
which developed a silent s, which letter was eventually removed from the word, the
Page 16
16
loss of which is signified by a circumflex in the modern French word hotel. The
German word 'Spital' shares similar roots.
Grammar of the word differs slightly depending on the dialect. In
the U.S., hospital usually requires an article; in Britain and elsewhere, the word
normally is used without an article when it is the object of a preposition and when
referring to a patient ("in/to the hospital" vs. "in/to hospital"); in Canada, both uses
are found.
Types
Lehigh Valley Hospital in Allentown, Pennsylvania
Some patients go to a hospital just for diagnosis, treatment, or therapy and then leave
('outpatients') without staying overnight; while others are 'admitted' and stay overnight
or for several days or weeks or months ('inpatients'). Hospitals usually are
distinguished from other types of medical facilities by their ability to admit and care
for inpatients whilst the others often are described as clinics.
General
The best-known type of hospital is the general hospital, which is set up to deal
with many kinds ofdisease and injury, and normally has an emergency department to
deal with immediate and urgent threats to health. Larger cities may have several
hospitals of varying sizes and facilities. Some hospitals, especially in the United
States, have their own ambulance service.
District
A district hospital typically is the major health care facility in its region, with
large numbers of beds for intensive care and long-term care; and specialized facilities
for surgery, plastic surgery, childbirth, bioassay laboratories, and so forth.
Specialized
Types of specialized hospitals include trauma centers, rehabilitation
hospitals, children's hospitals, seniors' (geriatric) hospitals, and hospitals for dealing
with specific medical needs such as psychiatric problems (see psychiatric hospital),
certain disease categories, and so forth.
Page 17
17
A hospital may be a single building or a number of buildings on a campus.
Many hospitals with pre-twentieth-century origins began as one building and evolved
into campuses. Some hospitals are affiliated with universities for medical research and
the training of medical personnel such as physicians and nurses, often called teaching
hospitals. Worldwide, most hospitals are run on anonprofit basis by governments or
charities. Within the United States, most hospitals are nonprofit.
Teaching
A teaching hospital combines assistance to patients with teaching to medical students
and nurses and often is linked to a medical school, nursing school or university.
Clinics
Main article: Clinic
A medical facility smaller than a hospital is generally called a clinic, and often
is run by a government agency for health services or a privatepartnership of
physicians (in nations where private practice is allowed). Clinics generally provide
only outpatient services.
Departments
Resuscitation room bed after a trauma intervention, showing the highly technical
equipment of modern hospitals
Hospital departments
Hospitals vary widely in the services they offer and therefore, in the
departments they have. They may have acute services such as an emergency
department or specialist trauma centre, burn unit,surgery, or urgent care. These may
then be backed up by more specialist units such as cardiology or coronary care
unit, intensive care unit, neurology, cancer center, and obstetrics and gynecology.
Some hospitals will have outpatient departments and some will have chronic
treatment units such as behavioral health services, dentistry, dermatology, psychiatric
ward, rehabilitation services, and physical therapy.
Common support units include a dispensary or pharmacy, pathology,
and radiology, and on the non-medical side, there often are medical records
departments and/or release of information department.
Page 18
18
Broadly speaking, there are three different types of hospital in Ireland but
there is very little difference in practice between the first two types:
Health Service Executive hospitals, owned and funded by the Health Service
Executive
Voluntary public hospitals, most of whose income comes directly from the
government. Voluntary public hospitals are sometimes owned by private
bodies, i.e., religious orders. Other voluntary public hospitals are incorporated
by charter or statute and are run by boards often appointed by the Minister for
Health and Children
Private hospitals, which receive no state funding
Public health services are provided in what can broadly be termed the
public hospitals - Health Service Executive hospitals and public
voluntary hospitals. Most of these hospitals also provide private health care
but they must clearly distinguish between public and private beds.
The distinction between the broadly termed public hospitals and
private hospitals is the same, regardless of the range of services provided by
the hospitals.
Acute hospital services in Ireland exist to diagnose, treat and care for seriously
ill or injured patients. Acute hospital services are provided in Health Service
Executive hospitals, public voluntary hospitals and private hospitals. Some
hospitals are specialist - for example, maternity hospitals, psychiatric hospitals,
cancer hospitals, while others are general.
The large general and regional hospitals in Ireland provide a broad range of
services. Smaller local hospitals may not be able to cater for all illnesses and
treatments and you may have to be transferred to a larger hospital or to a specialist
hospital. Everyone living in the country and certain visitors to Ireland are
entitled to free maintenance and treatment in public beds in Health Service Executive
and voluntary hospitals. Some people may have to pay some hospital charges.
Out-patient services in public hospitals are also free of charge but some people
may have to pay an initial charge if they have not been referred by a GP.
Page 19
19
If you are in a private hospital or in a private bed in a public hospital, you
must pay for both maintenance and treatment. Your private health insurance may
cover some or all of the costs.
Normally, you must be referred by a GP in order to avail of hospital services.
There are waiting lists for non-emergency services in many areas.
Accident and Emergency/Casualty
Most general hospitals and some specialist hospitals have accident and
emergency or casualty departments which patients may attend without being referred
by a GP. If you attend without a GP referral, you will be charged €100 (January
2009). If you have to return for further visits to an out-patient clinic in relation to the
same illness or accident you should not have to pay the charge again. The following
groups do not have to pay the charge if they do not have a referral from their GP.
Medical card holders
People who are admitted to hospital as a result of attending the casualty
department (you may then be subjectto in-patient charges).
People receiving treatment for prescribed infectious diseases
Children up to six weeks of age, children suffering from prescribed diseases
and disabilities and children referred for treatment from child health clinics
and school health examinations
People who are entitled to hospital services because of EU Regulations.
Women receiving maternity services.
Long-stay patients
Sometimes people become long-stay patients in acute hospitals. There is no
clear definition of the distinction between acute and long stay. Some
district hospitals and geriatric hospitals have designated long-stay beds.
Page 20
20
History
Early examples
View of the Askleipion of Kos, the best preserved instance of an
Asklepieion.
A physician visiting the sick in a hospital, German engraving from 1682
In ancient cultures, religion and medicine were linked. The earliest
documented institutions aiming to provide cures were Egyptian temples. In ancient
Greece, temples dedicated to the healer-god Asclepius, known
as Asclepieia (Greek:Ασκληπιεία, sing. Asclepieion Ασκληπιείον), functioned as
centers of medical advice, prognosis, and healing.[3]
At these shrines, patients would
enter a dream-like state of induced sleep known as "enkoimesis" (Greek: ενκοίμησις)
not unlike anesthesia, in which they either received guidance from the deity in a
dream or were cured by surgery. Asclepeia provided carefully controlled spaces
conducive to healing and fulfilled several of the requirements of institutions created
for healing. In the Asclepieion of Epidaurus, three large marble boards dated to 350
BC preserve the names, case histories, complaints, and cures of about 70 patients who
came to the temple with a problem and shed it there. Some of the surgical cures listed,
such as the opening of an abdominal abscess or the removal of traumatic foreign
material, are realistic enough to have taken place, but with the patient in a state of
enkoimesis induced with the help of soporific substances such as opium. The worship
of Asclepius was adopted by theRomans. Under his Roman name Æsculapius, he was
provided with a temple (291 BC) on an island in the Tiber in Rome, where similar
rites were performed.
According to the Mahavamsa, the ancient chronicle of Sinhalese royalty,
written in the sixth century A.D., King Pandukabhaya of Sri Lanka (reigned 437 BC
to 367 BC) had lying-in-homes and hospitals (Sivikasotthi-Sala) built in various parts
of the country. This is the earliest documentary evidence we have of institutions
specifically dedicated to the care of the sick anywhere in the
world. Mihintale Hospital is the oldest in the world. Ruins of ancient hospitals in Sri
Lanka are still in existence in Mihintale, Anuradhapura, and Medirigiriya.
Institutions created specifically to care for the ill also appeared early in India.
King Ashoka is said to have founded at least eighteen hospitals ca. 230 B.C., with
Page 21
21
physicians and nursing staff, the expense being borne by the royal treasury. Stanley
Finger (2001) in his book, Origins of Neuroscience: A History of Explorations Into
Brain Function, cites an Ashokan edict translated as: "Everywhere King Piyadasi
(Asoka) erected two kinds of hospitals, hospitals for people and hospitals for animals.
Where there were no healing herbs for people and animals, he ordered that they be
bought and planted However Dominik Wujastyk of the University College
Londondisputes this, arguing that the edict indicates that Ashoka built rest houses (for
travellers) instead of hospitals, and that this was misinterpreted due to the reference to
medical herbs.
Roman Empire
The Romans created valetudinaria for the care of sick slaves, gladiators, and soldiers
around 100 B.C., and many were identified by later archeology. While their existence
is considered proven, there is some doubt as to whether they were as widespread as
was once thought, as many were identified only according to the layout of building
remains, and not by means of surviving records or finds of medical tools.
Medieval Islamic world
This section may contain inappropriate or misinterpreted citations that do not
verify the text. Please help improve this article by checking for inaccuracie
Bimaristan
Further information: Medicine in medieval Islam
In the medieval Islamic world, the word "bimaristan" was used to indicate a hospital
establishment where the ill were welcomed, cared for and treated by qualified staff.
The public hospital in Baghdad was opened during the Abbasid Caliphate of Harun
al-Rashid in the 8th century. The first hospital in Egypt was opened in 872 and
thereafter public hospitals sprang up all over the empire from Islamic Spain and
the Maghribto Persia..
Colonial America
The first hospital founded in the Americas was the Hospital San Nicolás de
Bari [Calle Hostos] inSanto Domingo, Distrito Nacional Dominican Republic.
Fray Nicolás de Ovando, Spanish governor and colonial administrator from 1502–
Page 22
22
1509, authorized its construction on December 29, 1503. This hospital apparently
incorporated a church. The first phase of its construction was completed in 1519, and
it was rebuilt in 1552. Abandoned in the mid-eighteenth century, the hospital now lies
in ruins near the Cathedral in Santo Domingo.
Modern era
In Europe the medieval concept of Christian care evolved during the sixteenth
and seventeenth centuries into a secular one, but it was in the eighteenth century that
the modern hospital began to appear, serving only medical needs and staffed with
physicians and surgeons.
b) INDUSTRY SCENARIO IN INDIA
1. Healthcare Scenario - India
2. Current Healthcare Landscape
103,000 crores / annum spend on healthcare
5.2 % of GDP
86,000 crores is the healthcare delivery market
17,000 crores is the retail pharma market
This spending matches that of other developing countries as a
percentage of GDP but is low on a per capita basis
Therefore,it lags behind other developing countries on key health
indicators like life expectancy,infant mortality & morbidity
3. Share of different payors
100%=86,000 crores
Private providers capture 64 % of 86,000 crores
4. Breakup of government spend
100%=17,000 crores
5. Secondary & Tertiary Care Government spend utilization among various strata
of society
Page 23
23
100%=10,000 crores
Poorest 40 % receive only 20 % of govt. spend on secondary & tertiary
care
6. Distribution of private hospitals by bed size
100%= 35,000 – 45,000 pvt hospitals & nursing homes
Avg. size of hospital = 22 beds
7. Key findings of current private spending
Private spending on healthcare delivery 69,000 crores
61 % of this is spend on OPD services = 44,000 crores
Indicates low levels of affordability & a disease pattern dominated by
infections
39 % on IPD services = 25,000 crores
85 % of IPD spend is in 5 areas : cardio,cancer,accidents,infections &
maternity
Urban Indians & the rich account for a disproportionate share of the
spend
8. Key findings of current private IPD spending
Private IPD spending , 100%=25,000 crores 4250 17 5,800 Maternity 5500 22
4,100 Infections 4750 19 9,700 Accidents 3250 13 29,600 Cancer 3500 14
29,600 Cardio Value of total private IPD market -crores % of total private IPD
market Rs.per inpatient treatment Disease segment
9. Healthcare spending by income segment 100 % = 1 bn 69,000 25,000 44,000
Higher share of rich :
higher price/treatment
hospitilisation 24,000 Rs
compared to avg.8000 Rs
higher treatment rate
(50 % higher than avg.)
Page 24
24
10. Healthcare spending – urban vs rural 100 % = 1 bn 69,000 25,000 44,000
Higher share of urban :
higher proportion of rich
households (20 %
compared to 2%)
better access & treatment
rates
11. Road Ahead - 2012
Private spending on healthcare delivery 156,000 crores because of
increase population will lead to increase treatments
change in socio-economic mix will lead to 8 % increase in treatment
rate & 30 % increase in avg.price paid
Change in prices – 26 % increase in price per treatment
Change in mix of diseases – 50 % increase in prevalence of lifestyle
diseases will lead to 12% increase in treatment rate & 7 % in price
This would lead to a change in GDP from 5.2%to 6.2%
Richest 15%will account for 50% of all private healthcare spending &
60% of inpatient spend
Private spending would increase by another 39,000 crores if the
insurance is likely to impact on middle-income households approx. 350
million in 2012 leading to achieving GDP spending to 7.5% & private
spending on healthcare delivery to 195,000crores
c) FUTURE FOCUS:
a) Costly disposables in the next 10 years.
b) Cost of angiogram below Rs7,5
c) Cost of angioplasty below Rs.40,000
d) Cost of stent below Rs.75,000
e) A day stay in ICCU to be below Rs.3,000
Page 25
25
d) NATIONAL HEALTH POLICY
National Health Policy Government Of India Ministry Of Health & Family Welfare
New Delhi 1983
Introduction
The Constitution of India envisages the establishment of a new social order
based on equality, freedom, justice and the dignity of the individual. It aims at the
elimination of poverty, ignorance and ill-health and directs the State to regard the
raising of the level of nutrition and the standard of living of its people and the
improvement of public health as among its primary duties, securing the health and
strength of workers, men and women, specially ensuring that children are given
opportunities and facilities to develop in a healthy manner.
Since the inception of the planning process in the country, the successive Five
Year Plans have been providing the framework within which the States may develop
their health services infrastructure, facilities for medical education, research, etc.
Similar guidance has sought to be provided through the discussions and conclusions
arrived at in the Joint Conferences of the Central Councils of Health and Family.
Welfare and the National Development Council. Besides, Central legislation has been
enacted to regulate standards of medical education, prevention of food adulteration,
maintenance of standards in the manufacture and sale of certified drugs, etc.
While the broad approaches contained in the successive Plan documents and
discussion in the forums referred to in para 1.2 may have generally served the needs
of the situation in the past, it is felt that an integrated, comprehensive approach
towards the future development of medical education, research and health services
requires to be established to serve the actual health needs and priorities of the country.
It is in this context that the need has been felt to evolve a National Health Policy.
Our heritage
India has a rich, centuries-old heritage of medical and health sciences. The
philosophy of Ayurveda and the surgical skills enunciated by Charaka and Shusharuta
Page 26
26
bear testimony to our ancient tradition in the scientific health care of our people. The
approach of our ancient medical systems was of a holistic nature, which took into
account all aspects of human health and disease. Over the centuries, with the intrusion
of foreign influences and mingling of cultures, various systems of medicine evolved
and have continued to be practised widely. However, the allopathic system of
medicine has, in a relatively short period of time, made a major impact on the entire
approach to health care and pattern of development of the health services
infrastructure in the country.
Progress achieved
During the last three decades and more, since the attainment of Independence,
considerable progress has been achieved in the promotion of the health status of our
people. Smallpox has been eliminated; plague is no longer a problem; mortality from
cholera and related diseases has decreased and malaria brought under control to a
considerable extent. The mortality rate per thousand of population has been reduced
from 27.4 to 14.8 and the life expectancy at birth has increased from 32.7 to over 52.
A fairly extensive network of dispensaries, hospitals and institutions providing
specialised curative care has developed and a large stock of medical and health
personnel, of various levels, has become available. Significant indigenous capacity
has been established for the production of drugs and pharmaceuticals, vaccines, sera,
hospital equipments, etc
The existing picture
In spite of such impressive progress, the demographic and health picture of the
country still constitutes a cause for serious and urgent concern. The high rate of
population growth continues to have an adverse effect on the health of our people and
the quality of their lives. The mortality rates for women and children are still dis-
tressingly high; almost one third of the total deaths occur among children below the
age of 5 years; infant mortality is around 129 per thousand live births. Efforts at
raising the nutritional levels of our people have still to bear fruit and the extent and
severity of malnutrition continues to be exceptionally high. Communicable and non-
communicable diseases have still to be brought under effective control and eradicated.
Page 27
27
Blindness, Leprosy and T.B. continue to have a high incidence. Only 31% of the rural
population has access to potable water supply and 0.5% enjoys basic sanitation.
Medical and Health Education
It is also necessary to appreciate that the effective delivery of health care
services would depend very largely on the nature of education, training and appro-
priate orientation towards community health of all categories of medical and health
personnel and their capacity to function as an integrated team, each of its members
performing given tasks within a coordinated action programme. It is, therefore, of
crucial importance that the entire basis and approach towards medical and health
education, at all levels, is reviewed in terms of national needs and priorities and the
curricular and training programmes restructured to produce personnel of various
grades of skill and competence, who are professionally equipped and socially moti-
vated to effectively deal with day-to-day problems, within the existing constraints.
Towards this end, it is necessary to formulate, separately, a National Medical and
Health Education Policy which (i) sets out the changes required to be brought about in
the curricular contents and training programme of medical and health personnel, at
various levels of functioning; (ii) takes into account the need for establishing the
extremely essential inter-relations between functionaries of various grades; (iii)
provides guidelines for the production of health personnel on the basis of realistically
assessed manpower requirements; (iv) seeks to resolve the existing sharp regional
imbalances in their availability; and (v) ensures that personnel at all levels are socially
motivated towards the rendering of community health services.
Page 28
28
HRM PRACTICES IN SERVICE-BASED ORGANIZATIONS:
Human resource management (HRM) practices are being increasingly treated
as dependent rather than independent variables. Whereas in the past researchers
focused almost exclusively on how changes in HRM practices affect employee
performance or satisfaction, researchers are now beginning to ask how organizational
conditions shape HRM practices (e.g., design, staffing, performance appraisal,
compensation, and training and development). Examples of organizational conditions
hypothesized to impact HRM practices include strategy (Hambrick and Snow 1987;
Snow and Hrebiniak 1980; Olian
and Rynes 1984; Lawler 1984; Hambrick and Mason 1984; Gupta and
Govindarajan 1984a, b; and Miller, Kets de Vries and Toulouse 1982),
organizational life cycle stage (Kochan and Chalykoff 1987; Kerr 1982, 1985),
technological change, union presence, internal labor markets and even whether or not
an organization has a personnel department (Osterman 1984; Pfeffer and Cohen 1984;
Cohen and Pfeffer 1986). Consistent with this line of research investigating the
relationship between organizational conditions and HRM practices, this article
focuses on HRM practice in service-based organizations.
The role behavior theory perspective (Naylor, Pritchard and Ilgen 1980)
provides useful insights for understanding and explaining inter-organizational
differences in HRM practices and consequent organizational behaviors. Application
of the perspective is built on two fundamental assumptions: (1) HRM practices are a
primary means for defining, communicating and rewarding desired role behaviors and
(2) desired role behaviors are a function of organizational characteristics.
Page 29
29
HRM PRACTICES FOR MANAGERIAL AND HOURLY
EMPLOYEES IN SERVICE-BASED AND MANUFACTURING
FIRMS
The U.S. economy can be carved into a large number of industry sectors, but
the distinction between manufacturing-based and service-based industries is one of
the most basic. Service organizations have been described as differing from
manufacturing organizations in three ways: (1) their "products" are intangible rather
than tangible; (2) customers are actively involved in the production of services; and
(3) the consumption of services occurs simultaneously with their production (Bowen
and Schneider 1988; Daft 1986; Mills and Margulies 1980; Mills and Moberg 1982;
Larsson and Bowen 1989).
The intangible nature of services means that performance is difficult for
supervisors to monitor directly, so employees must be trusted to monitor their own
performance. The fact that customers are actively involved in the service production
process means service providers must be sensitive to clients' needs; they must monitor
these needs and use the cues they receive from clients to guide their job behaviors.
Because of these characteristics of service jobs, service organizations should be more
likely than manufacturers to include both employee input and client input as sources
of performance appraisal information (Mills and Morris 1986).
The simultaneity of the production and consumption processes also has
implications for HRM practices (Schneider and Schecter 1991). For example, quality
control cannot be achieved by the inspect-and-correct method commonly used in
manufacturing plants. Instead, quality control occurs at the point of service delivery
(Gronroos 1990; Heskett, Sasser and Hart 1990). In order to maintain control over
quality, service organizations are likely to seek ways of controlling the process of
service production rather than the outputs (Mills and Moberg 1982). They may invest
more resources to train new recruits, with the objective of socializing them to be
effective monitors of their own service production behaviors (Bowen and Schneider
1988). They could also revise their personnel selection system (Schneider and
Schecter 1991). Another way to gain more control over performance would be to use
performance appraisal results in making compensation decisions. Job design practices
Page 30
30
could also be used to enhance service quality. Enriched jobs should encourage
selfmonitoring because employees then feel a greater sense of responsibility for their
performance and they are more aware of their significance to the firm (Hackman and
Oldham 1980).
This line of reasoning implies that the following practices would be more
prevalent in service-based firms:
Job designs that are "enriched," in that they are characterized by
Autonomy, variety and interdependence;
Employee input into performance appraisals;
Client input into performance appraisals;
Use of performance appraisal results to assess training needs;
Extensive training of new employees, with emphasis on performance on
their current jobs; and
Use of performance appraisal results in determining compensation.
It should be noted here that in comparing service-based and manufacturing firms,
these predicted differences would be found for both managerial employees and lower-
level employees. However, the differences are likely to be greater for lower-level
employees whereas differences in the tasks performed by service-based employees
and manufacturing employees are particularly pronounced.
HRM PRACTICES FOR MANAGERIAL AND HOURLY
EMPLOYEES IN SERVICE ORGANIZATIONS
A large literature addresses the nature of the managerial position. According to
this literature, the jobs of managers comprise several roles. Mintzberg (1973), for
example, described 10 managerial roles clustered into three categories: interpersonal,
informational and decisional. While allowing for differences in situations, taken
together, these 10 roles characterize the job of manager as being linked with others,
taking some risks, focusing on results and process, managing the activities and jobs of
others, dealing with unpredictable events and monitoring the environment of the
group or unit being managed. Jacques' (1989) concept of the time span of discretion
adds another distinguishing feature to this picture of managerial jobs. The time span
Page 31
31
of discretion refers to the length of time it takes for results of a contribution to become
known. For managers, this time span is usually relatively long.
Using the Mintzberg role distinctions and Jacques' time span of discretion,
managerial jobs can be compared and contrasted with hourly or nonmanagerial jobs.
While managerial and non-managerial jobs are similar in that both are remunerated
and are important to organizational effectiveness, managerial jobs are generally filled
with more unpredictability, risk-taking, results-orientation, interdependence and a
longer time span of discretion, in comparison to hourly jobs. These differences may
diminish, however, as service organizations reduce layers of management,
decentralize and push more responsibility down to lower organizational levels.
Organizations use their HRM practices to encourage the behaviors needed to
successfully carry out the managerial role. Given that the managerial role is different
from the roles of lower-level employees in organizations, it is reasonable to expect
that organizations would use somewhat different human resource management
practices for the two groups of employees. Specifically, given the nature of the
managerial role as previously described, it is probable that compared to hourly
employees in service-based organizations; managers would be more likely to be
influenced by the following practices:
Jobs with greater skill variety and responsibility;
Performance appraisals that focus on results;
Performance appraisals that focus on projects that take a longer period of time;
Compensation schemes based on company-wide bonuses;
Training that is provided for longer-term and broader skill development; and
More training hours per year.
HRM PRACTICES FOR MANAGERIAL AND HOURLY EMPLOYEES IN
EFFECTIVE AND INEFFECTIVE SERVICE-BASED FIRMS
The general hypothesis that predicts major differences in human resource
practices used in the manufacturing and service industries follows from a
deterministic view of the relationship between environments and organizational forms
Page 32
32
(Hannan and Freeman 1977). Thus, for example, population ecologists would point to
the different niches that are the relevant environments for these two industry sectors
and argue that the characteristics of the two environments dictate the forms of the
organizations that populate them (Aldrich 1979).
Models that emphasize the role of managerial decision-making and choice
represent an alternative perspective for generating hypotheses about how
organizations are likely to differ in their management practices. The strategic choice
perspective assumes that organizations face numerous design options and that the
form of management an organization adopts represents decisions made by
management. These may be made within some constraints, however, such as the
constraints related to operating within the manufacturing or service industry (see
Hrebiniak and Joyce 1985). A strategic choice perspective recognizes that multiple
design options are often available to organizations, but does not necessarily assume
that all options are equally effective within a given environment (e.g., Porter 1980,
1985). Thus, inappropriate managerial
decisions can create organizational practices that are less than optimal, in which case
organizational effectiveness is likely to suffer. When applied to the issue of human
resource management systems, this view of organizational adaptation leads to the
prediction that when organizations operating within a given industry sector are
compared, those that are more effective will be the organizations that have adopted
HRM practices consistent with the demands of the industry.
Based on the previous discussion and the literature, several differences would
be expected between the human resource practices in more effective service firms in
comparison to less effective service firms. Specifically, the more effective the service
firm the more likely that-
Job designs will be characterized by skill variety and autonomy;
Employees will have input into their performance appraisals;
Clients will have input on appraisals; ,
Performance appraisal results will be used in determining training needs;
There will be a great deal of training of new employees; and
Performance appraisal results will be used in compensation decisions.
Page 33
33
CHAPTER-3
COMPANY PROFILE
A. GENERAL PROFILE OF CARE HOSPITALS
Care foundation is a registered nonprofit society with the mandate of making
quality health care affordable and accessible to all through appropriate use of
technology. The foundation has been established by a group of medical scientists and
technologies with the stated mission of making advanced comprehensive healthcare
affordable and accessible to all. The foundation is a non-profit organization and is
registered as a society under Andhra Pradesh Society Act 1365 Falsie.
The patron of the foundation is renowned cardiologist Padmashri
Dr.B.Somaraju and the chairman of the foundation is Prof.P.Krishnam Raju. The
foundation implements its mission of making advanced technology based care
affordable and accessible to common man under a three dimensional programme.
Conducting research & imparting specialized education.
Developing cost effective medical products, and
Providing health care to people from the economically weaker
sections of the society and those living in rural areas.
In 1997, when Dr.B.Soma Raju and Dr.D.Prasada Rao led a team of medical
professionals to set up the first CARE Hospital, it signaled the dawn of a new era in
medical care. At the heart of this movement was a burning desire to practice
medicine with compassion, concern and care, with a single minded objective the
recovery of the patient. Today, with Multi-Specialty Hospital across the state, and a
reputation for humanization and selfless service of the highest order, CARE Hospital
enjoys an unbelievable amount of goodwill. A million smiles will bear testimony to
that.
VISIONARIES
1. Dr.B.Soma Raju
Chairman & Managing Director
Page 34
34
Sri Dr.B.Soma Raju, MD, DM in Cardiology and renowned cardiologist in
India and Abroad.
He headed the department of Cardiology at NIMS during which time he
brought modern Cardiac care into the country.
He developed indigenous stent along with Dr.Abdul Kalam, President of India
(Named Kalam-Raju Stent)
He was honored by Government of Indian with Padmashree Award towards
his outstanding contribution in the field of Medicine in the year 2001.
He is the Chairman & Managing Director of QCIL
2. Dr.N.Krishna Reddy
Director & CEO
MD Internal Medicine from PGIMER, Chandigarh.
DM-Cardiology from GB Pant Hospital, New Delhi.
Asst.Professor at NIMS-introduced Tran esophageal echocardiography and
Dobutamine Echocardiography.
A key team member in development & evaluation of indigenous coronary
stents, beginning with ―Kalam-Raju‖ stent.
A principal investigator for 5 ongoing National Trials
The team leader for ongoing development of drug-eluding stents.
He is a Consultant Cardiologist and the Director & Chief Executive Officer of
QCIL
The organization was incorporated with the main objective of running all
kinds of hospitals, dispensaries nursing homes, clinical laboratories carrying out
medical research, education and train medical students nursing professionals, hospital
administrator, grant diplomas or recognitions as the company may deem fit and to
render professional consultancy and advice to any individual firm, company, Govt etc.
in the fields of research and development relating to medical, pharmaceutical and
chemical industries.
Page 35
35
BOARD OF DIRECTORS
Dr.B.Soma Raju, Chairman and Managing Director
Dr.N.Krishna Reddy, Chief Executive Officer
Mr.D.Suresh
Dr.A.Rajgopala Raju, Whole-time Director
Mr.C.Rama Krishna
Mr.Rajeev Amrish Agarwal
Mr.John Michael Lind
Dr.G.N.Rao, Director
COMPANY SECRETARY
Mr.N.Anjaneyulu
GROWTH
The care foundation was established with the noble objective of
providing needed research in cardiology, to achieve indigenization of the fast growing
range of hard ware products, devices and disposables in the field to provide excellent
academics at different levels and to strive to bring down the ever bargaining cost of
cardiac health care under the able leadership of its founder, chairman Dr.B.Soma
Raju. The care foundation has relentlessly pursued those objectives and can now look
back with some satisfaction on the work done towards this end in the first few years
of its experience.
Quality Care India Limited (QCIL) was an inevitable off shoot of the zeal to
achieve the above mentioned objective. And it has the purpose of giving a practical
shape to this pursuit. The care hospital Nampally, Hyderabad is the first of the project
of Quality Care India Limited established in July 1997 in leased premises the Hospital
needs little to be said in its praise as the direction it has then and its achievements are
now very well known, the immense credibility it has established is just a reflection of
this, Dr.B.SOMA RAJU is himself, the chairman of Quality Cares India Limited and
the care hospital and Dr.B.Prasada Rao, the Vice-Chairman the governing board of
the hospital has Dr.B.Soma Raju, and Mr.D.Suresh as its directors.
Page 36
36
The care hospitals stated with 200 beds. It has never shrinked from its
responsibility of looking after the economically deprived sections of the population.
It is to the credit of the hospital that nearly 20% of accommodation is allocated under
general ward category where the tariffs are highly subsidized.
The hospital has so far been an exclusive cardiac care hospital with few
supporting departments such as internal medicine and Pulmonology; it has on its
panel specialists from all the branches who visit on call.
The hospital runs on extremely busy intensive coronary care unit attending to
all cardiac emergencies. The unit is staffed with an in house cardiologist around the
clock, supported by juni9or doctors, an anesthetist, a large number of technicians and
nursing staff and others. Laboratory services are available continuously, Emergency
services such as primary angioplasty for a person with developing heart attack are
performed at all times of day or night.
Care hospitals felt the need to introduce other specialities that could serve the
population with the same professional competence and commitment as cardiac team
with this in view neurology and other neurology services were being started at CARE
NAMPALLY from October 2000. PROF. J.M.K.MURTHY who is a well known
neurologist and acclaimed expert on seizure disorders is heading the neurology unit.
Continuing on the path to achieve the objective the group has established a super
specialty hospital at BANJARA HILLS, HYDERABAD. This has brought under one
roof highly qualified, competent and dedicated professionals who would provide the
care and service to people. CARE foundation started a research and development
institution, cardio vascular devices and disposables to develop cardiac devices and
disposables.
THE CARE MODEL
They operate on physician driven model. This means that all the main
constituents of the CARE movement, the promoters, administrators and service
providers are physician. The center of the cARE model is the patient and the
overriding motive of all care‘s activities is to provide quality medical care at an
affordable cost. Technology training and team work from the every core of the
CARE model which also emphasizes a comprehensive and continuous education and
Page 37
37
training of every individual involved in the patient care. Every effort will be taken to
ensure that their growth is decided by the patients needs and not one decided by their
corporate requirements.
The base of the logo represents a level field provided to everybody.
The column consisting of beam represents the multi-disciplinary teams of
CARE Hospitals.
The person on the pedestal is a professional like a physician/nurse/health care
professional supported by excellence.
The person trying to climb the apex of the pedestal is a patient suffering from
illness or a student seeking knowledge and skills.
The rectangular box refers to a well-defined framework within which the
hospital functions.
FUNDAMENTAL REASON FOR EXISTENCE
To make quality medical care affordable and accessible considering quality,
cost, access.
Timeless unchanging core values.
Putting the patient first above ones own interest.
CORE PRINCIPLE
Putting the Patient first; above our own interests.
MISSION
To provide the best and cost-effective care, accessible to every patient through
integrated clinical practice, education and research.
VISION
To evolve as a unique university-based health-centre where the quest for new
knowledge would continuously yield more effective and more compassionate care for
all.
Page 38
38
To nurture a new generation of professionals of life-long commitment,
dedication, knowledge, skills, wisdom and values.
To strive for public trust and maintain medicine‘s humane and noble place
amongst professions.
To be globally competitive in healthcare and related businesses integrating
local culture and ethos.
OBJECTIVES
Upgrade its education and Research wing on par with the international
standards and consequently develop health care solutions for under developed
and developing areas.
Register a phenomenal growth by adding 5000 beds in the next five years.
Offer unique platform to various partners and collaborators, both national and
international to innovate in health care delivery systems, coverage systems
like microfinance/micro insurance, medical education and research.
Develop healthcare solutions for underdeveloped and developing countries.
To develop comprehensive healthcare delivery model that suits our
population.
To develop centers of excellence in medical specialties.
To compromise the obsolete and seek excellence through effective and up-to-
date technology and service.
Undertake clinical practice through high-end education and research.
Create a web of PCD clinics, corporate health plans, and associates program to
leverage the use of technology and gain access to remote areas.
POLICIES
Sensitivity to pain and suffering shall be accorded highest priority to every
employee.
Same treatment for same illness, irrespective of ability to pay.
Tests will be done only when medically necessary
Selection of all employees shall be on the basis of merit.
Compulsory continuous medical education to lab health care personnel.
Page 39
39
All departments shall be run by full time consultants.
Round the clock availability of cardiologists, C.T.Surgeon‘s neurologists,
anesthetists, labs and technicians.
VALUES AND PRINCIPLES Practice Practice medicine as an integrated team of compassionate, physicians,
scientists and allied health professionals.
Education Learn to serve through training and education of physicians, nurses
and allied health professionals.
Research Conduct basic and clinical research programs to improve patient care
and to benefit society
Mutual Respect Treat everyone with respect and dignity
Commitment to
Quality
Continuously improve all processes that support patient care,
education and research
Work Atmosphere Foster teamwork, personal responsibility, integrity, innovation, trust
and communication, and celebrate success
Societal
Commitment
Support the society we live in and assist patients with limited financial
resources
Finances Allocate resources within the context of a system rather than its
individual entities
Page 40
40
MILESTONES OF CARE
GROWTH OF CARE
Page 41
41
ACHIEVEMENTS:
First team to conduct an angioplasty in India (1985).
First team to perform Balloon Valvoplasty in India.
First team to develop the coronary heart stent (Kalam-Raju) in Asia.
First team to do the Beating Heart Surgery in India (1999)
First team to perform the cardiac MRI in India
Quality care India Ltd., is amongst the top five health care providers in India
and no.one in the State of Andhra Pradesh. It presently comprises of 14 hospitals
with five facilities located in the city at Hyderabad, two each in Vizag and Pune and
one each in Vijayawada, Nagpur, Surat, Raipur and Bhubaneswar.
It is the first concern to launch telemedicine services linking district
government hospitals.
Academic Programmes:
Care Institute of Medical Sciences.
Care School/College of Nursing.
Indira Gandhi National Open University (14th
November)
Netaji Subash Open University (NSOU) courses clinical research.
Care Learning Centre: 5th
January, 2005 .
Existing Hospitals
1. Hyderabad
CARE Nampally
CARE Banjara
CARE Secunderabad
CARE Remedy
CARE Musheerabad
CARE Clinic, Srinagar Colony
2. Lokamanya CARE & Galaxy Care, Pune.
3. Ganga CARE, Nagpur.
4. Ramakrishna CARE, Raipur.
5. Aditya CARE, Bhubaneswar.
6. Visakha CARE Unit I & II, Visakhapatnam.
7. Pinamaneni CARE, Vijayawada.
Page 42
42
8. CARE Surat.
Upcoming Hospitals:
9. AOC CARE, Secundarabad
The best interest of their patient is the only interest they consider. They at
CARE, combine an emphasis on the pure science of medicine with a keen
appreciation for each person‘s humanity. Their caring staff, advanced medical care,
accessibility and efficiency is what make them different from others-the preferred
choice of the international patient. Every employee devotes the necessary attention to
ensure that every patient‘s visit to CARE is convenient and worthwhile. The culture
at CARE bears testimony to the fact that:
―They are dedicated to the needs of their patients. They serve with a special
attitude, special care so that all patients gain the maximum benefit from their visit to
CARE.
―It uses a collaborative approach where each physician can call on the
expertise of medical specialists and sub specialists. This team work helps physicians
arrive at an accurate diagnosis and the most effective course of treatment. Each
patient benefits from the experience and skills of many physicians. CARE continues
to offer superior value with an efficient, streamlined approach to medical care that
emphasizes accurate diagnosis and effective treatments.
―It is patient centered organization and focus on one thing the needs of the
patient. The needs of the patient come first.
―It provides the best care to every patient through integrated clinical practice,
education and research‖.
―Comprehensive evaluation with timely, efficient assessment and treatment.
Availiability of the most advanced, innovative diagnostic and therapeutic technology
and techniques.
―The CARE organization recognizes the importance of good communication
with the patient‘s personal doctor. Upon the patient‘s return home, CARE physicians
send all pertinent medical information to the home doctor to assist in continued good
care. It functions cooperatively to bring skilled, compassionate care to patients from
around the world.
Page 43
43
MEDICAL SPECIALITIES IN CARE
Specialities:
1. Anesthesiology and Pain management
2. Bio Chemistry
3. Blood Bank and Transfusion medicine
4. Cardiology
5. Cardio-Thoracic Surgery
6. Clinic Pathology
7. Critical Care
8. Dental
9. Dermatology
10. Dialysis
11. Dietetic and Nutrition
12. ENT
13. Emergency Surgery
14. Endocrinology
15. Gastro Entomology
16. General Surgery
17. Gynecology
18. Hand & Micro Surgery
19. Hepatology
20. Hoematology
21. Imageology
22. interventional Radiology
23. Internal Medicine
24. Laparoscopy
25. Microbiology
26. Medical Oncology
27. Nephrology
28. Neurology and Neuro Surgery
29. Nuclear Medicine
30. Orthopaedicies and Trauma
31. Opthalmology
Page 44
44
32. Pain Management
33. Pediatrics
34. Pediatric Surgery
35. Phyiothearphy
36. Plastic & Cosmetic Surgery
37. Psychiatry
38. Pulmonology
39. Rheumatology
40. Robotic Surgery
41. Surgical Oncology
42. Urology
43. Vascular Surgery.
ORGANIZTION STRUCTURE
In structure, we see patients, are at high priority, at quality care the main
criteria is putting the patient first above ones own interest‖. They are treated as Elite
Group of the organization.
The next preference is given to doctors and nurses; they are the people who
give emotional support and satisfaction to the patients. The more comfort they give
the more satisfied is the patient, here the nurses play a very important and vital role,
they look after every aspect of the patient starting with their food to their medicines,
for this they have to be very patient, humble and pleasing.
PATIENT
Doctors and Nurses
Paramedics and House Keepers
Departmental Manager
Support Manager
Directors
Page 45
45
The next comes Paramedics and Housekeeping, the more cleanliness the more
attractive the hospital, so the housekeeping people play a crucial role in attracting the
people to opt the hospital. Pharmacist is one who delivers the prescribed medicines
given by the physician, the more pro active they are the more willingness to buy the
medicines from within the premises. Next comes the Departmental manager, who
looks after the departments, its functions and the procedures to be followed. He is the
person who is responsible for all activities to be carried for attaining the objectives
ORGANIZATIONAL HIERARCHY
GENERAL MANAGER
DEPUTY GENERAL MANAGER
CHAIRMAN
VICE-CHAIRMAN
BOARD OF DIRECTORS
HOSPITAL ADMINISTRATOR
MANAGER
ASSISTANT MANAGER
SUPERVISOR
REGULAR STAFF
Page 46
46
FUTURE PLANS
a) Costly disposables in the next 10 years
b) Cost of angiogram below Rs.7,5
c) Cost of angioplasty below Rs.40,000
d) Cost of stent below Rs.75,000
e) A Day stay in ICCU to be below Rs.3,000
B.FUNCTIONAL PROFILE:
PRODUCTION
Production Mix:- It is min of all multi specialties services in the hospital.
Production is nothing but it related to patient CARE service to the patients.
Marketing:-
As they are service providers they following the direct service.
Patient Doctor
Products:-
It refers to the specialties that are provided by the organization.
Price:-
Price is based on the service received by the patients.
Place:-
Place is not a criteria patients from various places visit the hospital for the
services provided by the hospital.
Promotion:-
1. Medical Camps
2. Publicity
3. Advertisement in journals, magazines, TV & Other media.
Page 47
47
CHAPTER-4
CONCEPTUAL PROFILE
A.THEORETICAL ASPECTS OF THE CONCEPT
HUMAN RESOURCE MANAGEMENT (HRM) ISSUES IN TQM
IMPLEMENTATION
Wilkinson et al. (1992) claim that the ‗hard‘ and ‗soft‘ aspects in TQM programmes
are interdependent elements. Similarly, this is supported by Rees (1995) who
identified valid linkages between them. The hard aspect is referred to as generally
quantifiable quality tools and techniques, such as total quality control, just-in-time
production, six-sigma and zero defect performance measurement, and task-based team
working. Meanwhile, the soft or more qualitative aspect of a TQM programme
consists of the use of HRM policies and activities to generate employee commitment
to quality, and the dissemination of management vision and ideology that may
reinforce the maxims of quality working culture, attitudinal change, continuous
improvement, and customer orientation.
As the origin of quality management lies within the operation and production fields,
manufacturing firms may tend to place emphasis on the hard and quantifiable
measurement aspects. In contrast, service-oriented organizations, which have a greater
degree of employee-customer interaction, should concentrate on the more qualitative
and softer aspects of working culture, customer care and personal interactions.
However, the managerial approach towards various aspects of ‗soft‘ issues in quality
management must continue to search for more quantifiable measurement of
performance outcomes. On the other hand, while modern management allows greater
employee discretion, autonomy and empowerment as the benefits of a TQM
programme, closer monitoring and tighter management control are still needed to go
hand-in-hand.
Miller and Cardy (2000) suggest that HRM need to respond in a creative way to TQM
and reengineering in organisational changes. The research constructs used are
staffing, training, performance appraisal, mentoring compensation, and social support.
Furthermore, Dale and Cooper (1993) highlight the importance of concern for people
issues in TQM. The HR activities that they relate to quality improvement processes
are the role of the senior managers, motivating middle managers, training and
Page 48
48
education team building, employee involvement at work, and handling people
resistance in quality change management.
The above evidence indicates significant relationships between HRM elements and
TQM implementation. The following section elaborates on literature on HR issues,
including people resistance, managerial roles, management commitment, and the
behavioral and cultural issues in relation to TQM implementation.
QUALITY HRM CLIMATE
In this study, variable items that would form a research construct of quality working
climate involving the employee involvement and commitment elements. Therefore,
the scope of discussion will cover literature review related to employee involvement,
employee commitment, and other perspectives of quality HRM in TQM
implementation. Most of the literature selected is on the service organisation context,
with a sample of some manufacturing and mixed (service and manufacturing)
organisations also included
Employee Commitment in Quality Initiatives
Employee commitment to organizational initiatives is always important, as they are
the people who are going to perform the quality mission in daily operations. They are
also the front-liners who are directly interacting with customers. Customers‘
evaluation and perception to determine whether they are satisfied with the service
provided or not would be the main indicators of quality and excellent performance.
Therefore, this section aims to present evidence from previous study on the significant
impact of employee commitment to quality working environment. Most of the
researches done in the selected literature are in a service-oriented context, including
public and private organizations.
The review is intended to identify the variables research constructs used in
investigating employee commitment with respect to quality initiatives.
The Hogan Personality Inventory (HPI) was used by Cran (1994) to assess the
validity of employee longer-term attitudinal commitment and work performance in
service-orientation organizations involved in a TQM initiative. Training effectiveness
on personality change could lead to attitudinal change on work commitment to fulfill
their job requirements. The personality attribute, which was used to study the
relationships between personality and employee commitment, seems to be narrowly
and intrinsically motivated. In contrast, some external factors, such as management
Page 49
49
support, leadership role and recognition, were discovered to have significant influence
on the results.
Meanwhile, Taylor (1995) defines commitment as more than accepting responsibility
for an activity, or even being engaged in pursuit of a quality objective. It involved
both attitudes and behaviours of all organisational members. Taylor‘s research
adopted the Mowday et al. (1982) constructs on attitudinal commitment, which
include:
1. Strong belief in and internalisation of the organisation‘s goals and
values.
2. Preparedness to expend considerable effort on behalf of the
organisation.
3. Strong desire to maintain organisational membership.
Meanwhile, Boshoff and Tait (1996) used organisational commitment as an
intervening variable in a study on service quality. An empirical test was conducted on
SERVQUAL model involving frontline employees‘ own perception of service quality,
and the service quality their supervisor believe they should deliver (Parasuraman et
al., 1988). The hypothesised antecedent variables used under Gap 1 to affect
organisation commitment are role conflict, role ambiguity, goal setting, upward
communication, downward communication, and performance feedback. The
hypothesised antecedent factors that will affect organisational commitment under Gap
3 are the initiating structure, job satisfaction, and teamwork Commitment in quality
management programmes must include a recalibration of organization-wide thinking for
high quality work methods combined with excellent results. Meanwhile, commitment to
quality assurance is oriented towards the assurance of product and service quality based
on quality techniques and guidelines for operational
1. INTRODUCTION OF HUMAN RESOURCE MANAGEMENT:
HRM is the management of employees, skills, knowledge, abilities, talents,
aptitudes, creative abilities etc. Employee in HRM is treated not only as economic
man but also as social and psychological man. Thus, the complete man is viewed
under this approach. Employee is treated as a resource. Employees are treated as a
profit centre and therefore, invert capital for HRD and future utility.
Page 50
50
NATURE AND SCOPE OF HR’s:
People in any organization manifest themselves, not only through individual
sections but also through GP interactions. When individual come to work place, they
come with not only technical skills, knowledge etc., but also with their personal
feelings, perception, desires, motives, attributes, values etc, therefore, employee
management in an organization does mean management of not only technical skills
but also other factors of the human resources.
MEANING OF HR’s MANAGEMENT:
Different terms are used to denote HR‘s management. They are labour
management, labour managesment relations, employee, employer relations and
industrial relations.
Personnel Administration, Personnel Management, Human Capital
Management, Human Asset Management, and the like. Though these terms can be
differentiated widely, the basic nature of distinction lies in the scope of coverage and
evolutionary stage.
In simple sense, human resources management means employing people their
resources, utilizing maintaining and compensating their service in tune with the job
and organizational requirements.
DEFINITIONS:
―HRM is a process consisting of four functions, acquisition, development,
motivations and maintenance of HR‘s‖.
Robbin & Decenzo
HRM has been defined as a strategic and coherent approach to the
management of an organization most valued assets the people working these, who
individual and collectively contributes to the achievement of its goals.
Armstrong (1999)
OBJECTIVES OF HRM:
The basic aims & objectives of HRM are to help the relization of the
organizational goals.
To ensure effective utilization of human resources. All other organizational
resources will be efficiently utilized by the human resources.
To ensure respect of human beings by providing various services and welfare
facilities to the personnel.
Page 51
51
To ensure reconciliation of individual group goals with those of the
organization in such a manner that the personnel feel a sense of commitment
and loyalty towards it.
To identify and satisfy the needs of individuals by offering various monetary
and non-monetary rewards.
To achieve and maintain high morale among employees in the organization by
securing better human relations.
To establish and maintain an adequate organizational structure of relationships
among all the members of an organization by dividing of tasks with in the
organization into functions, positions, and jobs, and by defining clearly the
responsibility, accountability, authority for each job and its relation with other
jobs in the organization. HRM tries to improve morale by providing adequate
training to workers and by achieving for itself knowledge of human nature
which is ―the totality of motives that cause human actions‖.
Functions of HRM:
The function of HRM can be broadly classified in to two categories.
(I) Managerial functions and
(II) Operative functions
I.Managerial Functions:
Managerial functions of personnel management involve planning, organizing,
directing and controlling. All these functions influence the operative functions.
(i) Planning: It is a pre-determined course of action. Planning is determination
of personal is determination of personnel programmes and changes in advance that
will contribute to the organizational goals.
(ii) Organizing: An organization is a means to an end. It is essential to carry
out the determined course of action.
(iii) Directing: The next logical function after completing planning and
organizing is the execution of the plan. The basic function of personnel management
at any level is motivating, commanding, leading and activating people. The willing
and effective cooperation of employees for the attainment of organizational goals is
possible through proper direction.
(iv) Controlling: After planning, organizing and directing the various
activities of thepersonnel management, the performance is to be verified in order to
Page 52
52
know that personnel functions are performed in conformity with the plans and
directions. Controlling also involves checking, verifying and comparing of the actual
with the plans, identification of deviation if any and correcting of identified
deviations. Thus, action and operation and adjusted to pre-determined plans and
standard through control.
II.Operative Functions:
The operative functions of personnel management are related to specific
activities of personnel management viz., employement, development, compensation
and relations. All these functions are interacted by managerial functions. Further
these functional are to be performed in conjunction with management functions.
(i) Employment: It is first operative function of Human Resources Management
Employment is concerned with securing and employing the people possessing
required kind and level of human resource necessary to achieve the organizational
objectives. It covers the functions such as job analysis, huamn resource planning ,
recruitment, selection, placement, induction and internal mobility.
a. Job analysis: It is the process of study and collection of information relating to
the operations and responsibilities of a specific job.
b. Human Resource Planning: It is a process for determination and assuring that
the organization will have an adequate number of qualified persons, available
at proper times, performing jobs which would provide satisfaction for the
individual involved.
c. Recruitment: It is the process of searching for prospective employees and
stimulating them to apply for jobs in an organization.
d. Selection: It is the process of ascertaining the qualaifications, experience, skill,
knowledge etc. of an applicant with a view to a appraising his/her suitability to
a job appraising.
e. Placement: It is the process of assigning the selected candidate with the most
suitable job in terms of job requirements. It is matching of employee
specification with job requirements.
Page 53
53
f. Induction and Orientation: Induction and orientation are the techniques by
which a new employee is rehabilitated in the changed surrounding and
introduced to the practices, policies, purpose and people etc., of organization.
II. Human Resources Development: It is the process of improving, Moulding and
chnaging the skills, knowledge, creative ability, aptitude, attitude, values,
commitment etc., based on present and future job and organizational requirements.
This function includes:
a. Performance Appraisal
b. Training
c. Management Development
d. Career Planning and Development
e. Internal Mobility.
f. Transfer.
g. Promotion
III.Compensation:
It is the process of providing adequate, equitable and fair remuneration to the
employees. It includes
1. Job evaluation.
2. Wage and salary
3. Administration.
4. Incentives,
5. Bonus,
6. Fringe benefits
7. Social security measures etc.
IV. Human Relations:
Practicing various human resources policies and programmes like
employment, development and compensation and interaction among employees create
a sense of relationship between the ilndividual workers and management, among
workers and trade unions and management.
V. Effectiveness of Human Resources Management:
Effectiveness of various personnel and practices can be measured or evaluated
by means of organizational health and human resources accounting etc.
1. Organizational Health.
Page 54
54
2. Human Resource Accounting.
HUMAN RESOURCE DEVELOPMENT:
Human Resource Development assumes significance in view of the fast
changing organizational environments and need of the organization to adopt new
techniques in order to respond to the enviornment changes.
The Concept of Human Resource Development:
The concept of HRD was formally introduced by Leonard Nadler in 1969 in a
Conference organized by the American Society for Training and Development.
Leonard Nadler defines HRD as, ―those learning experiences which are organized, for
a specific time, and desined to bring about the possibility of behavioral change‖.
Among the Indian authors T.Venkateswara rao worked extensively on HrD.
He defined HrD in the organizational context as, ―a process by which the employees
of an organiztion are helped in a continuous.
HRD from organizational point of view is a process in which the employees of
an organization are helped/motivated to acquire and develop technical, managerial
and behavioral knowledge skills and abilities, and mould the value, beliefs, attitude
necessary to perform present and future roles by realizing highest human potential
with a view to contribute positively to the organizational, group, individual and social
goals.
Functions of HRD Managers
1. Role Analysis
2. Human Resource Planning.
3. Recruitment
4. Selection
5. Placement
6. Induction and Orientation.
7. Performance Appraisal
8. Training
9. Management Development
10. Career planning and Development.
11. Organizational Development.
12. Compensation.
13. Social and Cultural Programmers.
Page 55
55
14. Workers, participation in Management.
15. Quality Circles.
16. Employee Counseling.
17. Team work.
18. Communication policies.
19. Monetary Rewards.
20. Non-Monetary Rewards.
21. Employee Benefits
HRM SUB-SYSTEM
FINANCE
MRKTG
HRM
PROD’N
SYSTEMS
Page 56
56
RESPONSIBILITIES OF HRM
The responsibilities are not distinct or compartmentalized. They are inter-related.
KEY ISSUES/CHALLENGES OF HRM
1. ENVIRONMENT CHALLENGES
Rapid change
Rise of the interest
Globalization
Workforce diversity
2. ORGANIZATIONAL DIVERSITY
Competitive position
Down sizing
Decentralization
Restructuring
Self managed work teams
Small business
Organizational culture
Technology, Outsourcing
3. INDIVIDUAL CHALLENGES
Job Insecurity
Matching
ATTRACTION
ADJUSTMENT SELECTION
ASSESSMENT RETENTION
DEVELOPMENT &
MOTIVATION
Page 57
57
People and Organization
Ethical dilemmas & Social Responsibility
Productivity
Empowerment and Bran drain.
Definition of HRM Policy
A policy is a plan of action. Brewster and Richbell defined HRM policies as,
―a set of proposals and actions that act as a reference point for managers in their
dealings with employees‖ ―Personnel policies constitute guides to action. They
furnish the general standards or basis on which decisions are reached their genesis lies
in an organisation‘s values, philosophy, concepts and principles‖ personnel policies
guide the course of action intended to accomplish personnel objectives. The
following example helps to understand the personnel policy clearly.
Example: One of the prtdonnrl objectives of Indian Railways is to provide
equal employment opportunities to the people of minority sections.
Personnel policy of Indian Railway relating to the above objectives is to till 15
per cent and 7.5 per cent of the vacancies from those candidates belonging to
scheduled castes and scheduled tribes respectively.
HRM Procedure:
Policies are general instructions whereas procedures are specific applications.
A procedure is a well thought out course of action. It prescribes the specific manner
in which a piece of work is to be done. Procedures are called ‗action guidelines‘.
They are generally derived from policies. Where policies define a broad field,
procedures show a sequence of activities within that area. The emphasis is on
chronological, step-by-step sequence of required actions. For instance, a student is
required to complete several itemised steps in order to register him/herself for courses
in a university. The basic purpose of a procedure is to spell out clearly the ways one
is to go about doing something.
Pay policy of Andhra Bank:
The bank believes in paying at least the prevailing scale of salary for similar
work in comprable organizations. The bank also believes in giving consideration to
significant changes in the cost of living.
Page 58
58
The procedure is – Fix the pay of clerk,s cashiers, typists equal to the lowest
pay given by any public sector bank in the country. Fix the pay of officers according
to the recommendations of the Pillai Committee.
Human Resource Planning:
E.W.Vetter viewed human resource planning as ―a process by which an
organization should move from its current manpower position to its desired
manpower position. Through planning, management strives to have the right number
and right kind of people at the right places at the right time, doing things which result
in both the orgnization and the individual receiving maximum long-run-benefit‖.
Degree of Uncertainty and the Length of Planning Period.
Short planning period Long planning period
(uncertainty/instability) (certainty/stability)
Many new competitors Strong competitive position
Rapid changes in social and Evolutionary, social, policitical
Economic conditions and technological change
Unstable products/service demand Stable demand patterns
Patterns
Small organizational size, poor Strong management prcatices
Management practices.
Process of Human Resource Planning
Process of Human Resources Planning consists of the following steps:
(1) Analysing organizational plans.
(2) Demand Forecasting: Forecasting the overall human resource requirements in
accordance with the organizational plans.
(3) Supply Forecasting: Obtaining the data and information about the present
inventary of human resources and forecast the future changes in the human
resource inventory.
(4) Estimating the net human resource requirements.
(5) In case of future surplus, plan for redeployment, retrenchment and lay-off.
(6) In case of future deficit, forecast the future supply of human resources from
all sources with reference to plans of other companies.
(7) Plan for recruitment, development and internal mobility if future supply is
more than or equal to net human resource requirements.
Page 59
59
(8) Plan to modify or adjust the organizational plan if future supply will be
inadequate with reference to future net requirements.
Recent Implications:
Most of the organizations, before 1990s employed human resources without
human resources planning. This was acute in the public sector whose objective was
creation of employment opportunities. The absence of human resources planning
before 1990s led to the folllowing implications in Indian companies.
(i) Overstaffing: Most of the organizations are found to be overstaffed
compared totheir counterparts in other countries.
(ii) VRS/Golden-handshake: The absence of human resources planning led to
overstaffing. Consequently, most of the organizations announced
VRS/Golden-handshake programmes in order to reduce the consequences
of overstaffing.
(iii) Delayering and Downsizing: Most of the organizations delayered their
organizations and announced down sizing programmes to rectify the
consequences of overstaffing.
Now, we shall discuss the recent trends in HRP.
Recent Trends in HRP
Outsourcing: Most of the organizations started to plan for outsourcing human
resources rather than HRP in order to:
Reduce the cost of human resources
Avoid the difficulties in human resources management and
Reduce the negative implications of overstaffing.
Many organizations outsourced the canteen, housekeeping, sales, book-
keeping, accounts, receivables and employee welfare operations.
Contingency clause in HRP: Most of the software companies have been
implementing time bound projects. Similarly, fast delivery has been the vital
strategy of many manufacturing companies. Hence, most of these companies
plan for contingency human resources in order to ensure that no project is
delayed due to human factor.
Recruitment Definitions:
Edwin B.Flippo defined recruitment as ―the process of searching for
prospective emloyees and stimulating them to apply for jobs in the organization‖.
Page 60
60
Process of Recruitment:
Process of Recruitment consists of three sub-systems in recruitment viz.,
sources of recruitment, techniques of recruitment to attract the candidates and
stimulating the candidates to apply. Fig. 5.1 presents the recruitment process.
(a) Finding out and developing the sources where the required number and kind of
employees are/will be avialable.
(b) Developing suitable techniques to attract the desirable candidates and
employing the techniques to attract candidates.
(c) Stimulating as many candidates as possible and asking them to apply for jobs
irrespective of number of candidates required. Management has to attract
more candidates in order to increase selection ratio (i.e. number of
applications per one job vacancy) in order to select the most suitable
candidates out of the total candidates available and due to lower yield ratio.
Recruitment is positive as it aims at increasing the number of applicants and
selection is somewhat negative as it selects the suitable candidates in which
process the unsuitabe candidates are automatically eliminated. Though, the
function of recruitment seems to be easy, a number of factors make
performance of recruitment a complex one.
Modern Sources and Techniques of Recruitment
A number of modern recruitment sources and techniques are being used by the
corporate sector in addition to traditional sources and techniques. These sources and
techniques include walk in and consult in, head-hunting, body-shopping, business
alliances, and tele-recruitment.
(i) Walk-in: The busy organizations and the rapid changing companies do not
find time to perform various functions of recruitment. Therefore, they
advise the potential candidates to attend for an interview directly and
without a prior application on a specified date, time and at a specified
place. The suitable candidates from among the interviewees will be
selected for appointment after screening the candidates through tests and
interviews.
(ii) Consult-in:- The busy and dynamic companies encourage the potential job
seekers to approach them personally and consult them regarding the jobs.
Page 61
61
The companies select the suitable candidates from among such candidates
through the selection process.
(iii) Head-hunting:- The companies request the professional organiztions to
search for the best candidates particularly for the senior executive
positions. The professional organizations search for the most suitable
candidates and advise the company regarding the filling up of the
positions. Head-hunters are also called search consultants.
(iv) Body Shopping:- Professional organisations and the hi-tech training
institutes develop a pool of human resources for the possible employment.
The prospective employers contact these organizations to recruit the
candidates. Otherwise, the organizations themselves approach the
prospective employees to place their human resources. These professional
and training institutions are called body shoppers and theseactivities are
known as body shopping. The body shopping is used mostly for computer
professionals.
(v) Business Alliances: Business alliances like acquisitions, mergers, and
take-overs help in getting human resources. In addition, the companies do
also have alliances in sharing their human resources on ad-hoc basis.
It does mean that, the company with surplus human resources offers the services of
their employees to other needy organizations.
(vi) E-Recruitment: The technological revolution in telecommunication helped
the organiztions to use internet as a source of recruitment. Organizations
advertise the job vacancies through the world wide web (www) internet.
The job seekers send their applications through e-mail or internet.
Alternatively, job seekers place their CVs in the world wide web/internet,
which can be drawn by the prospective employmers depending upon their
requirements.
Meaning and Definition:
After identifying the sources of human resources, searching for prospective
employees and stimulating them to apply for jobs in an organisation, the management
has to perform the function of selecting the right employees at the right time. The
obvious guiding policy in selection is the intention to choose the best qualified and
suitable job candidate for each unfilled job. The objective of the selection decision is
Page 62
62
to choose the individual who can most successfullyperform the job from the pool of
qualified candidates. The selection procedure is the system of functions and devices
adopted in a given company to ascertain whether the candidates specifications are
matched with the job specifications and requirements or not. The selection procedure
cannot be effective until and unless.
1. Requirements of the job to be filled, have been clearly specified (job analysis,
etc.,)
2. Employee specifications (physical, metal social, behavioural, etc.) have been
clearly specified
3. Candidates for screening have been attracted.
Thus, the development of job analyses, human resource planning and recuitment
are necessary prerequisites to the selection process. A breakdown in any of these
processes can make even the best selection system ineffective.
Written Examination
Preliminary Interview
Business games
Tests
Final Interview
Medical Examination
Reference Checks
Line Manager’s Decision
Job Offer Employment
Development Bases for Selection
Application/Resume/CV/Bio-data Job Analysis
Human Resources Plan
Recruitment
Assess the Fit between the
Job and the Candidate
Page 63
63
Induction is the process of receiving and welcoming on employee when he first joins
a company and giving him the basic information he needs to settle down quickly and
happily and start work‖
i) About the company
ii) About the Department
iii) About the Superiors, Subordinates, etc.,
Meaning:
Performance appraisal is a method of evaluating the behaviour of employees
in the workspot, normally including both the quantitative and qualitative aspects of
job performance.
Methods of Performance Appraisal
Trait Methods Behavioural Methods Results Methods
1. Graphic Rating Scales 1. Behavioural Checklist
Method
1.Productivity Measures
2.Ranking Methods 2. Critical Incident Method 2.Balanced Scorecard
3. Paired Comparison
Method
3. Behaviourally Anchored
Rating Scales
3. Human Resource
Accounting
4. Forced Distribution
Method
4.Behavioural Observation
Scales
4.Management by
Ojectives
5.Checklist Methods
(a) Simple Checklist
(b) Weighted Checklist
(c) Forced Choice
Method
5. Assessment Centre
6. Essay/Free Form
Appraisal
6. Psychological Appraisal
7.Group Appraisal
8. Confidential Reports
Page 64
64
Dale S. Beach define training as the oragnised procedure by which peole learn
knowledge and/or skill for a definite purpose.
Training Stages
The ILO described ‗fringe benefits as ―Wages are often augmented by special
cash benefits, bythe provision of medical and other services or by payments inkind,
that forms part of the wage for expenditure on the goods and services. In addition,
workers commonly receive such benefits as holidays with pay, low cost meals, low
rent housing etc. Such additions to the wage proper are sometimes referred to as
fringe benefits. Benefits that have no relation to employment or wages should not be
regarded as fringe benefits eventhough they may constitute a significant part of the
worker‘s total income‖.
Stage-1
Needs Assessment
Organisational
Analysis
Departmental
Analysis
Job Analysis
Employee
Analysis
Stage-2
Program Design
Insturctional
Objective
Learning Principles
Teaching Principles
Training Principles
Content Design
Stage-3
Implementation
On the job methods
Off the job methods Characterstics of the
instructors Conduct the
program
Stage-4
Evaluation
Reactions
Learning
Job Behaviour
Organization
Ultimate Value
Page 66
66
Grievance Procedure
Jucius defines a grievance as ― any discontent or dissatisfaction, whether
exposed or not, whether valid or not, arising ut of anything connected with the
company which an employee thinks, believes or even feels to be unfair, unjust or
inequitable‖.
The Open door policy
Open door policy which requires effort and willingness from the individual‘s
superior. In otherwords, there should be a general invitation to all employees to walk
in at any time and speak over their grievances.
Page 67
67
Meaning and Definitions
Discipline refers to a condition or attitude, prevailing among the employees,
with respect to rules and regulatins of an organization. Discipline in the broadest
sense means – orderliness, the opposite of confusion. It does mean a strict and
technical observance of rigid rules and regulations. It simply means working,
cooperating and behaving in a normal and orderly way, as any responsible person
would expect an employees to do‖.
DISCLPINE:
Progressive discipline is a process for dealing with job-related behavior that
does not meet expected and communicated performance standards. The primary
purpose for progressive discipline is to assist the employee to understand that a
performance problem or opportunity for improvement exists.
The process features increasingly formal efforts to provide feedback to the
employee so he or she can correct the problem. The goal of progressive discipline is
to improve employee performance.
The process of progressive discipline is not intended as a punishment for an
employee, but to assist the employee to overcome performance problems and satisfy
job expectations. Progressive discipline is most successful when it assists an
individual to become an effectively performing member of the organization.
Failing that, progressive discipline enables the organization to fairly, and with
substantial documentation, terminate the employment of employees who are
ineffective and unwilling to improve.
Typical steps in a progressive discipline system may include these.
Counsel the employee about performance and ascertain his or her
understanding of requirements. Ascertain whether there are any issues
contributing to the poor performance, that are not immediately obvious to the
supervisor. Solve these issues, if possible.
Verbally reprimand the employee for poor performance.
Page 68
68
Provide a written verbal warning in the employee's file, in an effort to improve
employee performance.
Provide an escalating number of days in which the employee is suspended
from work. Start with one day and escalate to five.
End the employment of an individual who refuses to improve.
Disciplinary Procedure
Disciplinary procedures in India industries comprise of the following stages:
(1) Issuing a Letter of Charge to the employee Calling upon him for Explanation:
When the management of the establishment comes to conclusion that an act
of misconduct committed by an employee warrants disciplinary action, the
concerned employee should be issued a charge-sheet. The charge-sheet
should indicate the charges of indiscipline or misconduct clearly and
precisely. Explanation should also be called from the delinquent employee
and for that sufficient time should be given to the employee. Serving of the
charge-sheet may be either personally or by post.
(2) Consideration of the Explanation:- When the delinquent employee admits, in
an unqualified manner, about his misconduct, there is no need for conducting
any enquiry further. Besides, when the employer is satisfied with the
explanation given by the delinquent employee. On contrary, when the
management is not satisfied with the employee‘s explanation, there is need
for serving a show-cause notice.
(3) Show-cause Notice: In the show-cause notice, the employer provides another
chance to the employee to explain his conduct and rebut the charges made
against him. Show-cause notice is issued by the manager, who decides to
punish the employee. Besides, a notice of enquiry should be sent to the
employee and this should indicate clearly the name of the enquiring officer,
time, date and place of enquiry into the misconduct of the employee.
(4) Holding of a Full-fledged Enquiry: The enquiry should be in conformity with
the principles of natural justice, that is, the delinquent employee must be
given a reasonable opportunity of being heard. The enquiry officer should
record his findings in the process of an enqury. He may also suggest the
nature of disciplinary action to be taken.
Page 69
69
The important steps in domestic enquiry are: preparing and serving the charge-
sheet, supervison in grave cases. Obtain reply to charge-sheet, selecting enquiry
officer conducting enquiry proceedings, holding of enquiry in the free environment
recording findings, subitting equiry officers‘s report to the disciplinary authority,
decision of the disciplinary authority, communication of the order of punishment.
(5) Considering the Enquiry Proceedings and Findings and Making Final Order
of Punishment: When the misconduct of an employee is proved, the manager
may take disciplinary action against him. While doing so, he may give
consideration to the employee‘s previous record, precedents, effects of this
action on other employees, consulting others before awarding punishment
rate No inherent right to appeal has been provided unless the law provides it.
In case the employee feels the enqury is not proper and action unjustified, he
must be given a chance to make an appeal.
(6) Follow-up: After taking disciplinary action, there should be proper follow-up.
The disciplinary action should not make the employee repeat his mistake.
HUMAN RESOURCE AUDIT
An audit is a review and verification of completed transactions to see whether
they represent a true state of affairs of the business or not. Thus, an audit is an
examination and verification of accounts and records. Human Resource (HR) audit
refers to an examination and evaluation of policies, procedures and practices to
determine the effectiveness and efficiency of HRM. In essence, HR audit refers to:
(i) The measureent of the effectiveness of human resource management‘s
mission, objectives, strategies, policies, procedures, programmes and
activities; and
(ii) The determination of what should or should not be done in the future as a
result of such measuremet.
AREAS OF HR AUDIT
The areas of HR audit include:
(i) Mission statement relating to human resource management.
(ii) Objectives, goals and strategies of human resource management
(iii) Accomplishment of human resource management.
(iv) Progammes of human resource management including the detailed
practices and procedures.
Page 70
70
(v) Human resource management policies
(vi) Human resource management philosophy, its practices and values.
(vii) Responses of employees, trade unions and government to the practices and
achievements.
(viii) Role of human resources in total quality management.
(ix) Role of human resources management in achieving organization‘s mission,
objectives, goals and strategies.
ATTENDANCE MANAGEMENT
Managing Employee Attendance
One basic ingredient to success in the workplace is to ensure that staff are
consistently attending work. As an administrator, you can positively, proactively and
consistently encourage this by communicating, keeping records to spot trends or
trouble spots, and promoting health and wellness with your staff.
There are existing attendance management programs in place for CUPE 116
and CUPE 2950 staff, but there are common threads to both, and principles that can
be applied to all staff, no matter the employment group.
For more information on the development of the attendance management
program with regards to CUPE 116, please read the 2008 HR Memo on the CUPE
116 Attendance Management Program. If you manage CUPE 116 staff, please ensure
that you review the CUPE 116 Attendance Management Guidelines, and the letter to
CUPE 116 employees regarding the program.
Communicate
Share information with your staff about your standards for attendance and
expectations about the employee’s responsibility regarding attendance and
absenteeism. (Employee responsibilities include making sure they call their supervisor
to report absences, attending to personal business outside of business hours, and
scheduling medical and dental appointments outside of work hours, if possible.)
Page 71
71
Increase their awareness of the importance of being at work regularly and
consistently, and how their attendance relates to their contribution to the success of
your team.
Acknowledge good attendance and coach employees who are having difficulty
with attendance to find solutions.
Promote Wellness
One way to decrease the use of sick time and encourage attendance at work is
to promote health, wellness and safety.
In some cases, absenteeism may be a symptom of something else going on in
an employee’s life.
UBC has supports in place to promote wellness, both for individuals and
organizations:
Health Safety and Environment has a number of programs in place, including
workplace safety and injury prevention, health promotion, and a graduated
return to work program
the Employee and Family Assistance Program (EFAP), provided by Human
Solutions, is a confidential counseling service for employees and their families
If you need support with attendance management in your area, contact your HR
Advisor.
Keep Records
Keep accurate records of your staff’s attendance. With good records, you will
be able to see if there is excessive use of sick time, and be able to spot any patterns of
absenteeism
Reporting Sick Leave Statistics to Human Resources
UBC is committed to managing absenteeism and since 2001, has worked with
many Administrators in the departments and faculties to collect data on paid sick
leave taken by staff.
Page 72
72
Currently, the University does not have the technical capability to report sick
leave on an individual basis via PeopleSoft. Therefore, Human Resources must rely
on departments and faculties to report their data (requested by employment group and
month).
UBC HR compiles data on sick leave usage and uses it for the following purposes:
included in the ―Time Loss Management‖ report presented to the Executive
and the Board of Governors, providing a snapshot of the health of our staff
and faculty and including statistics on the usage of sick leave (staff only),
Income Replacement Plan, Employee and Family Assistance Program and the
Return to Work Program
used by HR Advisory Services in conjunction with departments to benchmark
data on sick leave and design attendance management programs (once
implemented, the data is used to assess how effective the programs are in
managing absenteeism)
Introduction to Attendance Management
(Created January 1987 and last edited March 2010)
The management of workplace attendance is an important aspect of
supervision in the workplace.
The cost of absenteeism is greater than the direct payment of wages and
benefits paid durance the absence. Organizations must also consider the indirect costs
of staffing, scheduling, re-training, lost productivity, diminished moral, turnover, and
opportunity cost. The indirect costs often exceed the direct cost of absenteeism.
Each occurrence of absence costs the employer an average of $2,500, which
includes both direct and indirect costs (based on 9 days absent out of 250 working
days and an average payroll of $35,000).
Effective supervisory efforts to manage attendance will affect a relatively
small percentage of employees, but will result in substantial savings, increased
productivity and morale.
Page 73
73
Definition of Absenteeism
Absenteeism is the failure of employees to report for work when they are
scheduled to work. Employees who are away from work on recognized holidays,
vacations, approved leaves of absence, or approved leaves of absence would not be
included.
Causes of Absenteeism
The causes of absenteeism are many and include:
serious accidents and illness
low morale
poor working conditions
boredom on the job
lack of job satisfaction
inadequate leadership and poor supervision
personal problems (financial, marital, substance abuse, childcare eldercare
etc.)
poor physical fitness
inadequate nutrition
transportation problems
the availability of income protection plans
stress
excessive workload
employee discontent
Cost of Absenteeism
Absenteeism may have repercussions, which include:
Decrease in Productivity
employees may be carrying an extra workload, or supporting new or
replacement staff
employees may be required to train and orientate new or replacement workers
staff morale and employee service may suffer
Page 74
74
Financial Costs
overtime or agency cost for replacement workers
cost of self-insured income protection plans
premium costs may rise for insured plans
Administrative Costs
staff time is required to secure replacement employees or to re-assign the
remaining employees
staff time is required to maintain and control absenteeism
Do You Have An Absenteeism Problem?
Many organizations allocate 3% of their labour budget for absenteeism based
on an average of eight (8) working days missed per employee annually. Since the rate
of absenteeism varies by industry, division and department it is best to compare to the
most relevant benchmark available.
Sources of Absenteeism Statistics
Labour Reports, Workers' Compensation Board Statistics and Statistics Canada
provide paid sick leave statistics.
Trends in Absenteeism
Surveys indicate the following generalities in absenteeism:
The higher the rate of pay and the greater the length of service of the
employee, the fewer the absences
As an organization grows, there is a tendency towards higher rates of
absenteeism
Women are absent more frequently than men
Single employees are absent more frequently than married employees
Younger employees are absent more frequently than older employees
Older employees are absent for longer periods of time than younger
employees
Page 75
75
Unionized organizations have higher absenteeism rates than non-unionized
organizations
Understanding Absenteeism
The definition, causes, affects on productivity, and costs of absenteeism are
quite clear. The challenge is to develop methods that support attendance and control
absenteeism, in such a way as not to create mistrust, costly administrative procedures
and systems avoidance. Traditional methods of absenteeism control exclusively
utilizing disciplinary procedures have proven to be ineffective. It is almost impossible
to create a fair disciplinary procedure, because even well run disciplinary systems,
which treat similar actions with consistent repercussions, are usually seen as unfair.
This perception is common, because discipline alone neither identifies nor addresses
the root causes of absenteeism. Every employee who takes time off in defiance of
company regulations has reasons, which they believe justifies their actions. Unless a
management attendance program identifies and addresses the causes of employee
absenteeism, it will be ineffective and viewed as unfair. Traditional disciplinary
programs alone can, at best, give the illusion of control. It is no secret that there are
ways to beat even the best systems. The fear of discipline often only increases the
desire to avoid management systems.
If absenteeism is to be controlled, the physical and emotional needs of
employees must be addressed. In a 1985 study on "Rates of Absence among Nurses"
it was found that 50% of absenteeism could be controlled through attending to
employees’ physical and emotional needs.
Purpose of Attendance Management
The purpose of attendance management is to develop a willingness on the part of
all employees to attend work regularly, and to assist them in motivating their co-
workers to attend work regularly. This can be done through;
1. addressing the physical and emotional needs of employees
2. communicating the attendance goals of the organization so employees can
understand and identify with them
3. dealing with cases of excessive absenteeism effectively and fairly to produce
deterrence.
Page 76
76
Successful administration of an attendance management program requires
managers and supervisors to be aware of, and to create work environments in which
the following can be actualized;
1. The greater the extent to which individuals identify with the goals of the
organization and care what happens to it, the greater their motivation to be
regular in attendance.
2. The more that people find their jobs meaningful to them, the greater their
motivation to be regular in attendance.
3. As employees’ workloads increase due to the absence of a co-worker, peer
pressure is exerted on the absent co-worker to attend work on a regular basis.
4. The more people like working for the organization, the higher their motivation
to attend regularly. Recognition of good employee attendance helps improve
attendance.
5. Employees will have a lower absence ratio if they feel free to discuss their on-
the-job problems with their immediate supervisor.
6. Employees with a low absence ratio feel confidence and have supportive
relationships in their workplace. Low absence ratio employees are found to be
more satisfied with their opportunity for promotion and upgrading.
Commitment to Attendance
This paper provides the information necessary to begin an effective attendance
management program, which will yield long-term results. This paper is intended to be
a guide rather than an instruction manual or policy. To make an attendance
management program truly successful, it will require insight into the special dynamics
present in your work place. It will require two-way communication, as both the needs
of the employees and of management must be met if good attendance is to be
achieved. Attendance is the responsibility of everyone, especially those who directly
manage the human resources of your organization.
Attendance is not only an expectation; employers have the right to receive
good attendance. Each and every employee has a contractual obligation to attend
work regularly. All levels of management must believe in, be committed to, and
communicate their expectations of good attendance. If a specific number of sick days
Page 77
77
are considered acceptable per employee, at best that will be the result. Employees will
live up to the expectations that you set for them. Expectations must be clear to both
management and employees in order for an attendance management program to get
maximum results. Goals must be tangible. Attendance expectations must be clearly
communicated and followed.
Income Protection
A common misconception about income protection plans is that they are a
entitlements, like vacation benefit, and as such, should be fully utilized. The
reality is that income protection plans are a form of insurance. The sole and
only purpose of pay for sick leave is to assist in protecting employees against
loss of income in the event of an unavoidable absence due to sickness or a
non-work related injury. Use of income protection plans for any other purpose
negates their intent and, therefore, is inappropriate. Communicating the true
intent of income protection plans and our commitment to maintaining this
original intent is an essential aspect of attendance management.
25 Ways to Reward Employees (Without Spending a Dime)
Your firm's employees work hard (well, most of them). And in a world where
corporations like to boast about running "lean and mean," it may seem nearly
impossible to compensate employees for doing good work without breaking the
budget.
1. Flex those hours. If there's one free reward that rises above the rest, it's
flexible work schedules. Nearly every expert we contacted suggested flex time as a
perk that offers the most gain with the least pain.
―Give a little latitude in determining work schedules and to take time for
family or personal issues (such as doctor’s appointment and banking errands),‖
advised Richard Martin, president of Alcera Consulting Inc. ―As long as the employee
is deserving and doesn’t abuse the privilege, this can go a long way to building
trusting and mature relationships with key workers.‖
2. Send a handwritten note. Supervisors should ask top brass to write a
personal note to employees who deserve recognition, advised Cindy Ventrice, author
Page 78
78
of "Make Their Day! Employee Recognition That Works." For example,
AdvancedMD CEO Jim Pack handwrites his thank-you notes to employees on a $2
bill. ―In three years of doing this, only one employee has asked if he could spend it,‖
said company spokesman John Pilmer.
3. Make work fun. ―During a business coaching engagement, I found
employee morale to be way down,‖ said Terri Levine, president of The Coaching
Institute. ―We created a weekly event to boost morale. One week we asked everyone
to bring in a baby picture, post it on a wall, then pick which person matched each
picture. Everyone was having fun and socializing while productivity went from 58
percent to 72 percent — all in the same week.‖
4. Help them connect. Introducing employees to key suppliers, customers or
someone in senior management can help make an employee's career, says Ventrice —
and it won't cost you a thing.
5. Lose the shoes. Kaerie Ray, an account executive with the Echo Media
Group public relations firm, said implementing a ―no-shoes policy‖ can make
employees feel right at home with each other, which translates into increased
productivity. (But she suggests keeping the footwear handy in case clients come in.)
―It's great to be in an office where employees are more concerned about doing quality
work than what shoes or jewelry they have on,‖ she said. ―We get so much done.‖
6. Send them to the showers. (As in parties, not lathering and rinsing.)
―Every birth and wedding deserves a shower,‖ said Ray. ―Echo employees always
leave early on shower days, and the food is on the house. No need to make up the
time.‖
7. Reward effort as well as success. Even if their ideas sometimes fail, you
want employees to keep producing them, said Alan Weiss, president of the Summit
Consulting Group Inc. ―When I consulted with the CEO of Calgon, we created an
annual award for 'the best idea that didn't work' and presented a loving cup at the
annual awards dinner. This stimulated innovation and positive behavior, not
'winning.'‖
Page 79
79
8. Give them a free pass. Levine suggests giving out a certain number of free
days off to employees to use as they see fit. ―Employees get a few of these a year and
can use them as they like,‖ she said. ―They don't have to pretend to be sick. They can
go to the beach, read a book, play with their kids ... it doesn't matter.‖
9. Dole out cream and sugar. During the busiest times of the year, executives
at the Cigna Group push coffee carts around the office, serving drinks and
refreshments to their colleagues, noted Steve Harrison, author of "The Manager's
Book of Decencies: How Small Gestures Build Great Companies." As they serve,
executives coach and encourage colleagues and hear about real consumer issues.
10. Blow out the candles. Cisco Systems Inc.'s CEO John Chambers hosts a
monthly hour-long birthday breakfast for any employee with a birthday that month,
says Harrison. ―Employees are invited to ask him anything. They feel recognized, and
he gains loyal employees who share their ideas.‖
11. Spread the love. Ask co-workers to write something they truly like or
admire about an employee on a scrap of paper, then frame them along with a
photograph of the employee, suggested David Russell, author of "Success With
People – A Complete System for Effectively Managing People in Any Organization."
12. Offer a swap. Giving your best employees a chance to pick their own
projects or trade tasks with a colleague empowers and rewards them at the same
time, said Harrison.
13. Applaud their efforts — literally. If someone has done something
really worthwhile, have your entire staff give them a standing ovation at the next
meeting, suggested Sharlyn Lauby, president of HR consulting firm ITM Group
Inc.
something truly special, along with the details of what they did to earn their place
on the wall.
14. Say it with flowers. Professor Linda M. Lopeke, principal
ofSmartStartCoach.com, sayid she used to reward top employees by bringing in
flowers from her garden and arranging them in a spectacular crystal vase on their
desks. ―Everybody knew what having the custody of the flowers meant,‖ she said.
―Surprisingly, even the men competed fiercely for custody of the flowers.‖ In the
Page 80
80
winter, she'd substitute a showpiece display of floating glass fish.
15. Walk it as you talk it. The City of Dallas sponsored a walkathon
where employees set goals for walking a certain number of steps each day,
offering a free gym membership to those who walked the farthest. Not only did
they get more fit, they turned their daily walks into traveling staff meetings, says
city spokeswoman Danielle McCelland.
―Group members were able to update one another on projects, solicit team
input and improve their fitness,‖ she said. ―The organized program ended after
three weeks, but the work group still holds their traveling staff meetings two
months later.‖
16. Pass the bucks. Handing out monopoly money that can be redeemed
for gifts and other goodies may not be strictly free, but it pays off handsomely in
the long run. For example, associates at BankAtlantic can pass out ―WOW!
Bucks‖ to colleagues who've done something outstanding, said bank vice
president Gregory Dalmotte. The bucks can eventually be traded in for real goods.
―There's a clear correlation that words of encouragement have created associates
who perform at a higher level,‖ he says.
17. Share the memories. ―My team created a scrapbook chronicling the
impact I'd had on their company and gave it to me on my last day in the office,‖
said Lopeke. ―People who’d worked on my teams wrote testimonials and creative
graphics highlighting some our team successes. It's the best gift I ever received in
my 40-year career.‖ 18. Elect them to the Wall of Fame. Several experts
suggested setting aside a public space inside your firm and placing photos of
employees who've accomplished something truly special, along with the details of
what they did to earn their place on the wall.
19. Create your own "Club Med." Set aside a quiet space or unused
office in your building where employees can meditate, chill out, nap or otherwise
re-center themselves, said John Putzier, author of "Get Weird! 101 Innovative
Ways to Make Your Company a Great Place to Work."
Page 81
81
20. Stoke their passion. ―Great employees are not mercenaries,‖ said
Dr. Richard Chang, CEO of Richard Chang Associates Inc., a performance-
improvement consultancy. ―They don’t just want to enjoy their work, they want to
be passionate about it ... if you want your employees to feel valued and inspire
their passion on your behalf, encourage them to make their own decisions. You
can have systems in place to control the implementation of ideas, but you must be
certain not to compromise the enthusiasm, creativity and hard work that make
them possible in the first place.‖
21. Give them a place to park it. Reserve the best parking spot for
employees who've done something truly worthwhile, said Lopeke. And if it's next
to the CEO's Lexus so the employee can chat him or her up on the way into work,
so much the better.
22. Remember the spouses. Independent management consultant Nan
Amish recalled one time when she had 16 employees trapped in a hotel lobby on a
Sunday night, waiting for the ballroom to open so they could set up a trade-show
booth. ―I bought flowers at a farmers market, a nice $6 bouquet of roses for each
person,‖ she said. ―I told them to take them home to their significant others,
apologizing for me taking them away from their families on a Sunday. The next
day I got thank-yous from most of them. One wife sent a letter saying I could keep
her husband until Friday.‖
23. Publicize their successes. ―We like to publicly recognize employees
so the whole company can share in their accomplishments,‖ noted Scott Ragusa,
president of contract businesses for staffing firm The Winter, Wyman Companies.
―Each week, nominations for our quarterly 'Clutch' award are shared with the
whole company. The Clutch nominations are a way to recognize our
administrative and nonmanagerial professional staff members who have come
through in the clutch in supporting their departments or the firm.‖
24. Let them phone it in. Telecommuting programs can relieve stress
and make workers feel more appreciated, as well as more productive. ―Reward the
employee by starting with one day of telecommuting, then add additional days as
Page 82
82
performance heightens,‖ suggested Brian Margarita, president of IT staffing
firm TalentFuse Inc. ―Having the option to cart the kids to soccer practice, visit
the beach during the afternoon or cut out early to avoid traffic congestion is
becoming more important than working an 80-hour week for a larger paycheck.‖
25. Remember the secret words. ―The two most underused words in
corporate America that get the highest ROI (return on investment) and ROT
(return on your time) are the simple words 'thank you,'‖ noted Michael Guld,
president of the Guld Resource Group author of "The Million Dollar Media Rep:
How to Become a Television and Radio Sales Superstar."
While telling your employees you appreciate them should be obvious,
added Amish, no one does it enough or is specific enough about what the
employee did. ―So when you share your appreciation, be specific about what you
really liked, so they not only feel appreciated but can do it again.‖
CONTRACT LABOUR
PRELIMINARY
1. Short title, extent, commencement and application – (1) This Act may be called the
Contract Labour (Regulation and Abolition) Act, 1970.
(2) It extents to the whole of India.
(3) It shall come into force on such date as the Central Government may, by
notification in the official Gazettee, appoint and different dates may be appointed for
different provisions of this Act.
(4) It applies
(a) to every establishment in which twenty or more workmen are employed or were
employed on any day of the preceding twelve months as contract labour.
(b) to every contractor who employs or who employed on any day of the preceding
twelve months twenty or more workmen:
Page 83
83
Provided that the appropriate Government may, after giving not less than two
months‘ notice of its intentin so to do, by notification in the Official Gazettee, apply
the provisins of this Act to any establishment or contractor employing such number of
workmen less than twenty as may be specified in the notification.
(5)(a) It shall not apply to establishments in which work only of an intermittent or
casual nature is performed.
(b) If a question arises whether work performed in an establishment is of an
intermittent or casual nature, the appropriate Governent shall decide that question
after consultation with the Central Board or as the case may be, a State Board, and its
decision shall be final.
2. Definitions – (1) In this Act, unless the context otherwise requires –
(a) ―appropriate Government‖ means
(i) in relation to an establishment in respect of which the appropriate Government
under the Industrial Disputes Act, 1947 (14 of 1947), is the Central Government the
Central Governent.
(ii) in relation to any other establishment, the Government of the State in which that
other establishment is situate.
Prelinary:
Short title, extent, commencement and application
Definitions
The Advisory Boards:
Central Advisory Board
State Advisory Board
Power to constitute committees
Registration of Establishments Employing Contract Labour
Appointment of registering officers
Registration of certain establishments
Revocation of registration in certain cases
Effect of non-registration
Page 84
84
Prohibition of employment of contract labour
Licensing of Contractors
Appointment of licensing officers
Licensing of contractors
Grant of licences
Revocation, suspension and amendment of licences
Appeal
Welfare and Health of Contract Labour
Canteens
Rest-rooms
Other facilities
First-aid-facilities
Liability of principal employer in certain cases
Responsibility for payment of wages
Penalties and Procedure
Obstructins
Contravention of provisions regarding employment of contract labour.
Other offences
Offences by compan
B.APPLICATION OF THE CONCEPT IN THE
COMPANY
The CARE Hospital was implementing quality Management activities of
Human Resource Department through standard operating procedures which include
individual policy & procedure for each activity in the organization:
POLICY & PROCEUDRE:
1) Policy & procedure for Manpower planning.
2) Policy & Procedure for Recruitment
3) Policy & Procedure for Induction
4) Policy & Procedure for Training & Development
5) Policy & Procedure for Performance appraisal
Page 85
85
6) Policy & Procedure for Disciplinary action
7) Policy & Procedure for Grievance handling
8) Policy & Procedure for addressing Employee health needs
9) Policy & Procedure for Maintenance, reviewing, updating, removal of personnel records.
10) Policy & Procedure for collecting, verifying & evaluating, credentials of medical
professionals and nursing staff.
11) Policy & Procedure on service rules
12) Policy & Procedure for leave
13) Policy & Procedure for Best Associate Award Deputation.
14) Policy & Procedure for Transfer
15) Policy & Procedure for Tours & Travels.
16) Policy & Procedure for Compensation.
17) Policy & Procedure for availing, canteen facility
18) Policy & Procedure for hostile facility/guest house facility.
19) Policy & Procedure for Attendance Management
20) Policy & Procedure for Trainees & Apprentices
21) Policy & Procedure for Implementation of Contract Labor
22) Policy & Procedure for Resignation/Separation/Exit.
23) Policy & Procedure for In charge Attendance
24) Policy & Procedure for Implementation of Trainee apprentices
25) Policy & Procedure for HR Audit.
STANDARD OPERATING PROCEDURE
POLICY FOR MANPOWER PLANNING:
Objective:-
1.1 To identify and plan for Human Resources in accordance with the business
plans of the Organization?
1.2 To ensure a lean and effective organization.
Policy Contains:
1) Scope
2) Definition
3) Responsibility
4) Accountability
5) Internal Customers
Page 86
86
6) Date of Commencement
7) Policy & Procedure
8) 8.1) Annual human Resource Plan.
8.2) Budgeting
8.3) Human Resource Inventory Reports & Monitoring.
8.4) Human Resource Technology Platform.
9) Annexure
9.1) Manpower plan
9.2) HR Inventory report
Policy for recruitment:
1) Objective: To lay down policy in order to meet the manpower requirements of
QCIL with personnel who possess the necessary qualifications, skills, aptitude and are
suitable as per organization needs.
1.1) To streamline the Recruitment process
1.2) To ensure that we always hire the right people at Right role at Right time, and
also to thrive a strong employer branding to attract the best talents available in
the industry.
2) Scope
3) Manpower requisition form (MRF)
a) Approval of MRF
b) Recruitment Approval martyr.
4) Sources of Recruitment
5) Preference of in Recruitment
6) Eligibility of Internal candidates
7) Age limits for employment
8) Manpower Budgets
9) Manpower Indent
10) Selection process
11) Offer letter
12) Appointing Authority
13) Conclusion
Policy for Induction:
1.0) Objective
Page 87
87
1.1) To ensure that the new inducts have a professional introduction to the
organization to the organization and their work area.
1.2) To facilitate smooth entry into the organization and ensure that associates get
accustomed to the organization culture, get familiarized with systems and processes
which facilitate them to acquire necessary knowledge and skills and enables them to
function effectively from the start of their employment.
2.0) Scope
3.0) Process owner(s)
4.0) Policy and procedure
4.1) Documentation & Induction
4.2) Induction Training
5.0) Conclusion.
Policy for Training:
1) Objective:To enunciate the types of training to be conducted for competency
building of associates and the purpose and methodology of training intervention
2) Scope
3) Purpose
4) Training Cycle
4.1) Need Analysis
4.2) Training Design & development
4.3) Evaluation of the training
4.4) Types of training intervention
4.5) Training staff
Training and Development
Research Content Implement &Delivery
Design Development
AGM(1) Sr.Manager(1) Manager(1)
Asst.Manager(1) Manager (1) Asst.Manager(1)
Sr.Executive (1)
4.6) Training allowance
4.7) Conclusion
Policy for disciplinary action
Page 88
88
1)Objective:
1.1) To guide associates to follow work place discipline
1.2) To take necessary actions in case of indiscipline.
2) Scope
3) Disciplinary action
4) Misconduct in General items.
5) Industrial Employment (standing orders) Act 1946
6) Natural Justice
7) Management of discipline
8) Warning
9) Show cause notice
10) Charge Sheet
11) Suspension
Policy for Grievances:
1) Objective:
1.1) This lays down the procedure for handling all personnel related grievances.
1.2) The policy is for the aid of all departmentally Branch heads to address grievances
projected by associates and systematically finding solutions for the same. In
particular it should aid the HR department in redressing grievances.
1.3) To ensure that associate grievances are handled opportunity and as without delay.
2) Scope
3) Definitions
4) Responsibility
5) Accountability
6) Internal customers
7) Date of commencement
8) Policy and procedure
Policy on employee health needs:
1) Objective
1.1) It is QCIL‘s objective, under the health policy, to provide coverage for Wealth
Care to its emplyees and his/her dependants by hospitalization Insurance policy.
2) Scope
3) Definition
4) Responsibility
Page 89
89
5) Accountability
6) Internal customers
7) Date of commencement
8) Policy & procedure
Policy for credentialling and prrivielaging:
1) Objective:
1.1) To define hospital policy and procedure for credentiating privileging of
physicians and nurses.
2) Scope
3) Definition
4) Respnsibility
5) Accountability
6) Internal customers
7) Date of Commencement
8) Policy and procedure
Policy for service rules:
1) Objective:
1.1) To guide associates so that the business conduct is consistent with the
organizations ethical standards.
1.2) To improve the understanding of the organizations ethical standard among
customers, suppliers, and others outside the organization.
2) Scope
3) Definition
4) Shared responsibilities.
5) Accountability
6) Internal customers
7) Date of commencement
8) Policy & Procedure
8.1) Compliance with the law
8.2) Environment
8.3) Government contracting
8.4) Safety and Health
8.5) Customer and supplier relations
8.6) Business courtesis
Page 90
90
8.7) Business inducement
8.8) Conflicts of interest
8.9) Protection and use of assets
8.10) Internal conytrols
8.11) Reporting integrity
8.12) Electronic information
8.13) Travel and Entertainment
8.14) Inside information
8.15) Competitive intelligence
8.16) Political contributions
8.17) Valucing individual diversity.
Policy for Award:
1.1) Objective: To lay down policy for identification nominating and awarding
associates who perform efficiently.
2) Scope
3) Definition
4) Responsibility
5) Accountability
6) Internal customers
7) Date of Commencement
8) Policy and procedure
8.1) Types of award
8.1.1) Best Associate Award
8.1.2) Annual Star Achieves award
8.2) Periodicity of award
8.3) Best Associate award
Policy of Deputation: (Shift from Original place of works)
1.1) Objective: To lay down policy on deputation allowance
2) Scope
3) Definition/Keywords
4) Responsibilities
5) Accountability
6) Internal customer
7) Date of Commencement
Page 91
91
8) Policy & Procedure
8.1) Eligibility
8.2) Approval
8.3) Procedure for compensation.
Policy for Transfer:
1) Objective: To lay down policy for effectively transfer associates from one
established to the other within QCIL.
2) Scope
3) Definition
4) Responsibilities
5) Accountability
6) Internal customers
7) Rate of commencement
8) Policy & Procedure
8.1) Purpose of transfer
8.2) Procedure
8.2.1) Permanent Transfer
8.2.2) Fares
8.2.3) Class of travel
8.2.4) Conveyance of Household goods & portage charges.
8.2.5) Setting allowances and other expenditure
8.2.6) Temporary transfer
Policy for travel allowance:
1) Objective: To lay down policy for eligibility and authorization of various
allowances during official tours/visits by associates of CARE Hospitals.
2) Scope
3) Definitions
4) Responsibilities
5) Accountability
6) Internal Customer
7) Date of commencement
8) Policy and procedure.
8.1) Grades
8.2) Classification of cities/towns.
Page 92
92
8.3) Travel
8.4) Lodging
8.5) Boarding
8.6) Journey allowance
8.7) Conveyance
8.8) Other incidentals
Policy for Compensation:
1) Objective: To attract potential candidates and retain the right talent by
compensating with salary and remuneration as a means for organizations
effectiveness.
2) Scope
3) Definition
4) Responsibility
5) Accountability
6) Internal Customers
7) Date of commencement
8) Policy
1) Gross salary HRA - 25%
2) Allowances - 45%
Policy cateen facility:
1) Objective: To provide the associates basic canteen facilities.
2) Scope
3) Definition
3.1) Patient relation executive (PRG)
4) Responsibilities
5) Accountability
6) Internal customer
7) Rate of commencement
8) Policy
8.1) 80% subsidy – nursing
8.2) 50% subsidy – junior, middles, senior management
Page 93
93
8.3) Free meal to contract staff
8.4) Midnight snakcs.
9) Procedure for availing break fast and lunch facilities.
10) Procedure for availing canteen facilities by guests or visitors.
Policy for hostel:
1) Objective: To provide guest house facility/hostel occ. to staff in the guest
house/hostels at various locations.
2) Scope
3) Definition
4) Responsibility
5) Accountability
6) Date of comencement
7) Policies
7.1) Guest house
7.2) Hostel Accommodation.
7.3) Other rules and regulations to follow in the guest house
7.4) changes in the policy
Policy for attendance Management:
1) Objective:
1.1) The objective of this policy is to provide the guidelines of how to run time office
for effective results.
1.2) To provide guidelies of what reports to be generated and their prescribed formats
and other functions to be monitoried.
2) Scope
3) Definition
4) Responsibility
5) Accountability
6) Internal customers
7) Date of commencement
8) Policy
8.1) Procedure for capturing data.
8.2) Procedure for posting the data.
8.3) Procedure for generation of Associates attendance.
8.4) Procedure for generation of late coming associates list.
Page 94
94
8.5) Procedure for generation of easily going associte list.
8.6) Procedure for generation of associates list.
8.7) Procedure for abseatees.
8.8) Procedure for Weekly/monthly attendance.
8.9) Procedure for consideration of associate leave balances.
8.10) Procedure for head count
8.11) Procedure for late deductions
8.12) Procedure for Permissions.
8.13) Procedure for monitoring time office operations.
Annexure:- Attendance Management report.
Policy Implement Apprentices Act:
1) Object: To ensure that this procedure is implemented as per the apprentices Act,
1961.
2) Scope
3) Definition
4) Responsibility
5) Accountability
6) Internal customers
7) Date of commencement
8) Policy
8.1) Training & Other requirements.
Policy for Exit:
1) Objective: To render fain and equitable treatment to an associate who is leaving the
organization. The organiztions and the associates interest will be upheld in a
respectable manner.
2) Scope
3) Definition
4) Responsibility
5) Accountability
6) Internal customers
7) Date of commencement
8) Policy
8.1) 1st month prior notice and other rules
8.2) Reasons for termination
Page 95
95
8.3) Procedure for termination
8.4) Procedure for Exit interview
8.5) Full in Final settlement
Annexure:
1) Exit interview
2) No Dues Certificate
3) F & F Settlement
Policy in-charge allowance:
1) Purpose: To provide in-charge allowance to associates working in logistics
deprtment.
2) Scope
3) Procedure
1) Eligibility
2) Pharmacy Aides
3) Monthly allowance
4) Changes in the policy (Every 1 year review)
Policy of contractor:
1) Objective: To ensure streamlined management of outsourced contract services
manpower, in particular adherence to government statuettes. The governing law is
contract labour (R&A) Act 1970 and subsequent amendaments, as well as respective
state Government G.O‘s on contract labour (R&A) Act 1970 as amended from time to
time.
2) Scope
3) Definition
4) Responsibility
5) Accountability
6) Internal customers
7) Date of commencement
8) Policy procedure for appointment for contracts.
9) Annexures forms.
Policy for HR Audit:
Objective: To periodically and systematically review of all aspects of functionering of
HR Department. So as to strong their core HR processes and ensure that SOP‘s and
Government regulations are adhered. HR audit is not a review of the HR associates
Page 96
96
performance. It is explicitly aimed to improve department functioning and is not a
fault finding mechnism. This is an annual audit of HR system that is besides other
internal/external auditors appointed by the company.
2) Scope
3) Definitions
4) Responsibility
5) Date of comencement: April, 2009
6) Importance of Audit
7) Audit procedure
8) Subject covered under Audit
9) Methodology (once in a year)
10) Auditor
11) Conclusion
12) Annexure: Check list
Policy for leave:
1) Objective: To document policy guidelines on availing of leave.
2) Scope
3) Definition
4) Responsibilities
5) Accountability
6) Internal customer
7) Date of commencement
8) Policy and procedure
8.1) Earned Leave
8.2) Causal Leave
8.3) Sick Leave
8.4) Maternity Leave
8.5) Special leave
8.6) Compensatory off
8.7) Fixed holidays
Procedure to avail leave
Accumulation/Encashment of leave records.
Table for Leave:
Page 97
97
Sl.No. Name of the Shift Working Hours
1 A 8 to 5
2 B 2 to 8
3 C 8 to 8
4 Night Shifts 10-7,11-4,9-6
Leave Administration:
CARE Hospitals has a procedure for a granting of leave if want leave has an
application from (it is printed form supplied by the company) to fill up the application
and mentioned the cause of the leave. This application submits to Head of the
department, then put forward to personal officer. The was final authority to grant
leave.
Leaves Trainee Permanent
Casual Leave 12 12
Sick Leave - 12
Earned Leaves - 15 (per annum)
In addition special leaves are granted. Compensatory pay-off is also an
additional benefit. Encashment of leave facility is provided, any casual leave not
exceed 3 days at a time. Sick leave is exceeds 3 days ‗Doctor‘ to be certified the sick
leave.
Policy for maintanance, reviewing, updating, removal of personal records.
1. Objective:
1.1 to establish procedures and responsibilities for the maintanance of employees
personnel records and personnel files.
1.2 The personnel records of CARE Associates shall maintained by respective unit
human resource department. These personnel files are maintain in individual file
folders in HR department.
2. Scope
3. Defintion
4. Responsibility
5. Accountability
6. Internal customers
7. Date of commencement
Page 98
98
8. Policy and procedure
DATA ANALYSIS AND INTERPRETATION
1) What is the quality of awareness being created to you regarding the
quality standards?
Respondents No. of Respondents Percentage
Yes 135 90%
No 15 10%
Total 150 100%
Page 99
99
Interpretation:-
From the above table it is found that out of 150 respondents 90 percent of the
respondents felt that ―CARE quality officer is creating awareness to them regarding
the quality standards‖ is yes, followed by 10 percent respondents felt that No.
It is concluded that CARE quality officer has been creating awareness
regarding the quality standards to majority of the respondents 90 percent.
2) How much percentage did your organization employee additional
staff since total quality management?
Respondents No. of Respondents Percentag
High 12 8%
Medium 94 62%
Low 44 30%
Total 150 100%
Percentage
90%
10%
Yes
No
Page 100
100
Interpretation:-
From the above table and graph it is found that out of 150 respondents 62
percent felt that ―Organization employee additional staff since total quality
management‖ is medium followed by 30 percent felt that it is low, 8 percent felt that
it is high.
It is concluded that organization is to an normal range. Employed additional
staff for the quality management activities.
3) What other benefits does your organization gain with total quality
management?
Respondents No. of Respondents Percentage
Improve Productivity 32 21%
Increase Market Share 16 11%
Better Team work 82 55%
Improve Image 20 13%
Percentage
8%
62%
30%
High
Medium
Low
Page 101
101
Total 150 100%
Interpretation:-
From the above table and graph it is found that out of 150 respondents 55
percent felt that ―Organization gains with total quality management‖ is Better team
work followed by 21 percent felt that it is ―Improve productivity‖, 11 percent felt that
it is ―Increase market share‖ 13 percent felt that it is ―Improve image‖
It is concluded that overall total quality management benefits the organization
gains in all aspects to majority of respondents supported it.
4) How far does manpower planning system is helping you to meet
the demand?
Respondents No. of Respondents Percentage
Good 72 48%
Very Good 14 9%
Percentage
21%
11%
55%
13%Improve
Productivity
Increase Market
Share
Better Team work
Improve Image
Page 102
102
Satisfactory 64 43%
Total 150 100%
Interpretation:-
From the above table and graph it is found that out of 150 respondents 48
percent felt that ―Manpower planning system is helping organization to meet the
demand‖ is ―Good‖, followed by 43 percent felt that it is ―Satisfactory‖, 9 percent felt
that is ―Very good‖.
It is concluded that manpower planning system of the organization is helping
them to meet their adequate demand.
5) Does the recruitment procedure of assessment are qualitative and
accurate?
Respondents No. of Respondents Percentage
Good 110 73%
Percentage
48%
9%
43% Good
Very Good
Satisfactory
Page 103
103
Very Good 16 11%
Excellent 0 0%
No Opinion 24 16%
Total 150 100%
Interpretation:-
From the above table and graph it is found that out of 150 respondents 73
percent felt that ―The recruitment procedure of assessment qualitative and accurate‖ is
―Good‖, followed by 16 percent ―no opinion‖ 11 percent felt that it is ―Very good‖.
It is concluded that recruitment procedure of the organization is qualitative in
assessing the ―right people for the right job‖.
6) Are you well oriented towards the culture of the organization? If
so how good was the induction training?
Respondents No. of Respondents Percentage
Good 64 43%
Percentage
73%
11%
0%
16%
Good
Very Good
Excellent
No Opinion
Page 104
104
Very Good 52 35%
Satisfactory 34 22%
Total 150 100%
Interpretation:-
From the above table and graph it is found that our of 150 respondents 43
percent felt that the statement ―Employees are well oriented towards the culture of the
organization through induction training procedure is ―Good‖ followed by 35 percent
felt it is ―Very good‖, 22 percent felt that it is ―Satisfactory‖.
It is concluded that induction training procedure is helping the employees to
be well oriented towards the culture of the organization to majority respondents
supported the 43 percent.
7) Does the training and development system helping the trainees to
gain more insights in enhancing their skills?
Respondents No. of Respondents Percentage
Good 72 48%
Percentage
43%
35%
22%
Good
Very Good
Satisfactory
Page 105
105
Excellent 30 20%
Satisfactory 48 32%
Total 150 100%
Interpretation:-
From the above table and graph it is found that out of 150 respondents 48
percent felt that the statement ―Training and development system helping the trainees
to gain mare insights in enhancing their skills is good followed by 32 percent felt that
it is ―satisfactory‖, 20 percent felt that it is ―Excellent‖.
It is concluded that training and development policy of the organization helps
trainees to gain more insights to enhance their skills for organizational growth.
8) Does the present appraisal system change the employees attitude
towards work?
Respondents No. of Respondents Percentage
Percentage
48%
20%
32%
Good
Excellent
Satisfactory
Page 106
106
Strongly agree 18 12%
Agree 68 45%
Disagree 28 19%
No Opinion 36 24%
Total 150 100%
Interpretation:-
From the above table and graph it is found that out of 150 respondents 45
percent felt that the statement ―Appraisal system changes the employees attitude
towards work is Agreed‖ followed by 24 percent felt it is ―No Opinion‖, 19 percent
felt that it is ―Disagree‖, 12 felt that it is ―Strongly agree‖.
It is concluded that the performance appraisal system change the employees
attitudes towards work environment to majority of the supported it 45 percent.
9) Does the Disciplinary system of the organization helping the
employees to be legality at work?
Respondents No. of Respondents Percentage
Percentage
12%
45%19%
24%
Strongly agree
Agree
Disagree
No Opinion
Page 107
107
Yes 144 96%
No 6 4%%
Total 150 100%
Interpretation:
From the above table and graph it is found that out of 150 respondents 96
percent felt that ―Disciplinary system of the organization helping the employees tobe
legal at work is ―yes‖ followed by 4 percent felt that it is ―no‖.
It is concluded that the disciplinary system is helping the employees to be
much legal at their working norms. To majority of the respondents 96 percent.
10) Are you able to clear your grievances quickly through the
grievance redressal system?
Percentage
96%
4%
Yes
No
Page 108
108
Respondents No. of Respondents Percentage
Strongly agree 10 7%
Agree 96 64%
Disagree 12 8%
No Opinion 32 21%
Total 150 100%
Interpretation:
From the above table and graph it is found that out of 150 respondents 64
percent felt that ―They are able to clear their grievances quickly through the grievance
redressal system is agree, followed by 21 percent felt that it is ―No opinion‖ 8 percent
felt that it is ―Disagree‖, 7 percent felt that it is ―Strongly agree‖.
It is concluded that the grievance redressal system helping the employees to
clear their grievances to majority of the respondents 64 percent.
11) Does the Quality of welfare of employees is concerned by the
organization or not?
Percentage
7%
64%
8%
21%
Strongly agree
Agree
Disagree
No Opinion
Page 109
109
Respondents No. of Respondents Percentage
A little true 44 29%
Some what true 62 41%
True to a great Extent 44 30%
Total 150 100%
Interpretation:
From the above table and graph it is found that out of 150 respondents 41
percent felt that ―Quality of welfare of employees is concerned by the organization is
some what true‖, followed by 29 percent felt that it is ―A little true‖, 30 percent felt
that it is ―True to a great extent‖
It is concluded that the quality of welfare of employees is concerned by the
organization to a majority of the respondents 41 percent.
12) How do you feel about the award and reward system?
Percentage
29%
41%
30%A little true
Some what true
True to a great
Extent
Page 110
110
Respondents No. of Respondents Percentage
Good 88 59%
Very Good 10 7%
Satisfactory 52 34%
Total 150 100%
Interpretation:
From the above table and graph it is found tht out of 150 respondents 59
percent felt that ―The award and reward system was good‖, followed by 34 percent
felt that it is ―Satisfactory‖, 7 percent felt that it is very good.
It is concluded that the award and rewared system helping the ―Employees to
work better to majority of the respondents 59 percent.
Percentage
59%
7%
34%
Good
Very Good
Satisfactory
Page 111
111
13) Is the compensation system clear or not?
Respondents No. of Respondents Percentage
Strongly Agree 8 5%
Agree 104 70%
Disagree 8 5%
No Opinion 30 20%
Total 150 100%
Interpretation:
From the above table and graph it is found that out of 150 respondents 70
percent felt that the compensation system is clear or not is agree, followed by 20
percent ―no opinion‖, 5 percent felt that it is ―strongly agree‖, 5 percent felt that it is
―Disagree‖.
It is concluded tht the compensation system followed by the organization is
agreed by the employees to majority of the respondents 70 percent.
Percentage
5%
70%
5%
20%
Strongly Agree
Agree
Disagree
No Opinion
Page 112
112
14) How best is the feedback regarding the total quality standards in
the organization?
Respondents No. of Respondents Percentage
A little true 82 21%
Somewhat true 68 45%
True too great extent 16 11%
Very true 34 23%
Total 150 100%
Interpretation:
From the above table and graph it is found that out of 150 respondents 45
percent felt that ―The feedback system regarding the total quality standards in the
organization as ―some what true‖, followed by 23 percent felt that ―very true‖ 21
percent felt that it is ―A little true‖, 11 percent felt that it is ―True to a great extent‖.
It is concluded that the organization is receiving the best feedback regarding
their quality standards to majority of the respondents 45 percent.
Percentage
21%
45%
11%
23% A little true
Some what true
True too great
extent
Very true
Page 113
113
15) Overall, do you think that TQM brings positive effect to your
organization?
Respondents No. of Respondents Percentage
Yes 138 92%
No 12 8%
Total 150 100%
Interpretation:
From the above table and graph it is found that out of 150 respondents 92
percent felt that ―The total quality management brings positve effect to their
organization is yes‖ followed by 8 percent felt that it is ―No‖.
It is concluded that the organization is bringing their positive effect by
implementing the total quality management to majority of the respondents 92 percent.
Percentage
92%
8%
Yes
No
Page 114
114
16) Are the terms and conditions regarding transfer procedure were
clear or not?
Respondents No. of Respondents Percentage
A Little True 36 24%
Some What true 62 41%
True to a great Extent 16 11%
Very True 36 24%
Total 150 100%
Interpretation:
From the above table and graph it is found that out of 150 respondents 41
percent felt that ―The terms and conditions regarding transfer procedure were clear or
not is supported as somewhat true‖ followed by 24 percent felt that is ―Very true‖ 24
felt that it is ―A little true‖, 11 percent felt that it is ―True to a great extent‖.
It is concluded that the organization transfer procedure were clear and an
objected to majority of the respondents 41 percent.
Percentage
24%
41%
11%
24% A Little True
Some What true
True to a great
Extent
Very True
Page 115
115
17) To what extent is the verifying and evaluating credentials of
medical professionals and nursing is justified?
Respondents No. of Respondents Percentage
A little true 20 12%
Somewhat true 52 34%
True to great extent 28 18%
Very true 54 36%
Total 150 100%
Interpretation:
From the above table and graph it is found that out of 150 respondents 36
percent felt that ―Verifying and evaluating credentials of medical professionals and
nursing of it is justified as ―Very true‖ followed by 34 percent felt that it is ―some
what true‖ 18 percent felt that it is ―True to a great extent‖ 12 percent felt that is ―A
little true‖.
It is concluded that credentials are verified and evaluated correctly to majority
of the respondents 36 percent.
Percentage
12%
34%
18%
36%
A little true
Some what true
True to great
extent
Very true
Page 116
116
18) Does the exit interview giving an opportunity to the organization
to realize their strengths and weakness?
Respondents No. of Respondents Percentage
Yes 142 95%
No 8 5%
Total 150 100%
Interpretation:
From the above table and graph it is found that out of 150 respondents 95
percent felt that ―The Exit interview giving an opportunity to the organization to
realize their strengths and weakness is ―yes‖ , followed by 5 felt that is ―No‖.
It is concluded that the exit interview is helping the organization to realize
their strengths and weakness to majority of the respondents 95 percent.
Percentage
95%
5%
Yes
No
Page 117
117
19) Does the organization realizing the health needs of the employees
through qualitative aspects?
Respondents No. of Respondents Percentage
Yes 122 81%
No 28 19%
Total 150 100%
Interpretation:
From the above table and graph it is found that out of 150 respondents 81%
felt that the organization realizing the health needs of the employees through
qualitative aspects is ―Yes‖ followed by 19 percent felt that it is ―No‖.
It is concluded that organization is realizing the health needs of the employees
through qualitative criteria.
Percentage
81%
19%
Yes
No
Page 118
118
20) Does the service rules helping you to be confirming to the quality
standards of the organization?
Respondents No. of Respondents Percentage
Yes 130 87%
No 20 13%
Total 150 100%
Interpretation:
From the above table and graph it is found that out of 150 respondents 87
percent felt that the service rules helping you to be confirming to the quality standards
of the organization is ‗Yes‘ followed by 13 percent felt that it is ―No‖.
It is concluded that the service rules helping employees to be confirming to the
quality standards of the organization to majority of the respondents 87 percent.
Percentage
87%
13%
Yes
No
Page 119
119
FINDINGS
The CARE quality officer is creating awareness to employees regarding the
quality standards.
The standard operating procedure helping the employees to perform or work
much better through standard procedure.
The policies designed helping the employees to work committed towards the
welfare of the organization.
The rewards/Awards system helps to motivate employees to work better.
The grievance system helps the employees to clear up their grievances and
find a solution for their grievances.
The feedback system is well conducted in the premises of all the employee to
educate them and creating on opportunity for an employee to develop himself.
Page 120
120
CHAPTER-6
SUGGESTIONS
1. Standard operating procedures can be much more frequently reviewed
and revised for more clarity, understandability and usefulness. Since
most of them need much better improvements in their quality of work
life.
2. Both quantity and quality performance factors have to be considered in
construction of SOP‘s (Standard Operating Procedures)
3. Much concentration is needed while conducting the exit interviewers
to realize organizational weakness.
4. Health needs of employees should be recognized much better.
5. Therefore present standard operating procedures may be restructured,
reoriented and repositioned to benefit both organization and
employees.
Page 121
121
ANNEXURE-1 QUALITY (HUMAN RESOURCE) MANAGEMENT PRACTICES
QUESTIONNAIRE
Dear Sir/Madam,
I, K.PRANEETH doing project in CARE under the guidance of Asst.Professor
Mrs.Padmaja. I am conducting a survey on quality practices of Human Resources
Department through study of SOP‘s at CARE Nampally‘s and I would be grateful, if
you could, kindly spare your valuable time to fill this questionnaire.
Employee name: Designation:
Please kindly tick mark your answers
1) Do the care quality officer is creating awareness to you regarding the quality
standards?
A) Yes B) No
2) Did your organization employee additional staff since TQM?
A) High B) Medium C) Low
3) What other benefits does your organization gain with TQM?
A) Improve productivity B) Increase market share
C) Better teamwork D) Improve image
4) How far your manpower planning system is helping you to meet the demand?
A) Good B) Very Good C) Satisfactory
5) Does the recruitment procedure of assessment qualitative and accurate?
A) Good B) Very Good C) Excellent D) No opinion
6) Are you well oriented towards the culture of the organization? If so how good was
the Induction training?
A) Good B) Very good C) Satisfactory
7) Does training & development system helping the trainees to gain more insights in
enhancing their skills?
A) Good B) Excellent C) Satisfactory
8) Does the present appraisal system change the employee‘s attitude towards work?
A) Strongly agree B) Agree C) Disagree D) No opinion
9) Disciplinary system of the organization is helping the employees to be legality at
work?
Page 122
122
A) Yes B) No
10) Are you able to clear your grievances quickly through the grievance redressal
system?
A) Strongly agree B) Agree C) Disagree D) No opinion
11) Quality of welfare of employee‘s is concerned by the organization or not?
A) A little true B) Somewhat true C) True to a great extent
12) How do you feel about the award and reward system?
A) Good B) Very good C) Satisfactory
13) Does the compensation system is clear and fair?
A) Strongly agree B) Agree C) Disagree D) No opinion
14) How best is the feedback regarding the total quality standards in the organization?
A) A little true B) Somewhat true C) True to a great extent
D) Very true
15) Overall, do you think that TQM brings positive effect to your organization?
A) Yes B) No
16) The terms and conditions regarding transfer procedure were clear or not?
A) A little true B) Somewhat true C) true to a great extent
D) Very true
17) To what extent is the verifying and evaluating credentials of medical professionals
and nursing justified?
A) A little true B) Somewhat true
C) True to a great extent D) Very true
18) Does the exit interview giving an opportunity to the organization to realize their
strengths & weakness.
A) Yes B) No
19) Does the organization realizing the health needs of the employees through
qualitative aspects?
A) Yes B) No
20) Does the service rules helping you to be confirming to the quality of the
organization?
A) Yes B) No.
Page 123
123
BIBLIOGRAPHY
1. Human Resource Management
P.Subba Rao
2. Human Resource Management.
… Robert L.Mathis and John H.Jackson
3. Labour Laws
… P.L.Mehtha
4. Industrial Relations
… Aruna Monappa
… TATA MC Graw-Hill Publishing House.
5. Project Report Writing
… M.K.Rampal, S.L.Gupta
… Galgotia Publishing Company
www.google.com
www.carehospitals.com
www.hrm.com