Department of Anaesthesia and Intensive Care Department of Clinical Pharmacology Helsinki University Central Hospital University of Helsinki Finland Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies Erik Samuel Litonius ACADEMIC DISSERTATION To be publicly discussed, with the permission of the Faculty of Medicine of the University of Helsinki, in the lecture hall of Töölö Hospital on August 31, 2012 at 12 noon. Helsinki 2012
Transcript
Department of Anaesthesia and Intensive Care
Department of Clinical Pharmacology
Helsinki University Central Hospital
University of Helsinki
Finland
Treatment of acute intoxication with intravenous lipid emulsion –
animal and human studies
Erik Samuel Litonius
ACADEMIC DISSERTATION
To be publicly discussed, with the permission of the Faculty of Medicine of the University of Helsinki, in the lecture hall
of Töölö Hospital on August 31, 2012 at 12 noon.
Helsinki 2012
Supervised by
Professor Per H. RosenbergDepartment of Anaesthesiology and Intensive CareHelsinki University Central HospitalHelsinki, Finland
Reviewed by
Professor Hannu KokkiDepartment of Anaesthesia and Operative ServicesKuopio University HospitalUniversity of Eastern FinlandKuopio, Finland
and
Professor Kalle HoppuPoison Information CentreHUSLABHelsinki, Finland
To be discussed with
Professor Dag JacobsenDepartment of Acute MedicineOslo University Hospital, UllevålOslo, Norway
ISBN 978-952-10-8167-5 (paperback)ISBN 978-952-10-8168-2 (PDF)http://ethesis.helsinki.fiUnigrafia OyHelsinki 2012
“Science is the great antidote to the poison of enthusiasm and superstition.”
Adam Smith (1723-1790), The Wealth of Nations
To my wife Anna.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 4 –
TABLE OF CONTENTS
LIST OF ORIGINAL PUBLICATIONS 6
ABBREVIATIONS 7
ABSTRACT 9
SAMMANFATTNING 10
YHTEENVETO 11
INTRODUCTION 12
REVIEW OF THE LITERATURE 14 Local anaesthetic systemic toxicity 14 Intravenous lipid emulsion as treatment for severe intoxication 15 Pharmacokinetics of drug distribution 18 Pharmacologic properties of drugs studied 21 Current evidence supporting the use of intravenous lipid emulsion
as treatment for severe intoxication 24
AIMS OF THE STUDY 43
MATERIALS AND METHODS 44 Animal studies (I-III, V) 44 Human study (IV) 47 Preparation of POPC-POPG liposome dispersion 48 Partial filling electrokinetic capillary chromatography 48 Sample handling 48 Statistical analyses 50
RESULTS 51 Study I 51 Study II 53 Study III 54 Study IV 56 Study V 58
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 5 –
DISCUSSION 62 Main findings 62 Experimental model vs. clinical situation 62 Lipid solubility requirement for entrapment 64 Lipid sink or lipid subway? 65 Animal models 66 Other mechanisms for the therapeutic effect of intravenous lipid
emulsion in local anaesthetic-induced myocardial depression 68 Intravenous lipid emulsion for CNS or cardiac toxicity of local
anaesthetics 68 Possible adverse effects of the intravenous lipid emulsion
treatment for severe intoxication 69 Limitations of the studies 69
CONCLUSIONS 71
IMPLICATIONS FOR FUTURE STUDIES 72
ACKNOWLEDGEMENTS 74
REFERENCES 76
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 6 –
LIST OF ORIGINAL PUBLICATIONS
This thesis is based on the following original articles, which are referred to in the text by their Roman numerals.
Intravenous lipid emulsion sequesters amiodarone in plasma and eliminates its hypotensive action in pigs. Niiya T, Litonius E, Petäjä L, Neuvonen PJ, Rosenberg PH. Ann Emerg Med;56(4):402-408, 2010.
Intravenous lipid emulsion only minimally influences bupivacaine and mepivacaine distribution in plasma and does not enhance recovery from intoxication in pigs. Litonius E, Niiya T, Neuvonen PJ, Rosenberg PH. Anest Analg;114(4):901-906, 2012.
No antidotal effect of intravenous lipid emulsion in experimental amitriptyline intoxication despite significant entrapment of amitriptyline. Litonius E, Niiya T, Neuvonen PJ, Rosenberg PH. Basic Clin Pharmacol Toxicol;110(4):378-383, 2012.
Effect of intravenous lipid emulsion on bupivacaine plasma concentration in humans. Litonius E, Tarkkila P, Neuvonen PJ, Rosenberg PH. Anaesthesia;67(6):600-605, 2012.
In vitro and in vivo entrapment of bupivacaine by lipid dispersions. Litonius E, Lokajova J, Gebrenegus Y, Neuvonen PJ, Holopainen JM, Rosenberg PH, Wiedmer SK. J Chromatograph A; In Press, http://dx.doi.org/10.1016/j.chroma.2012.07.013
The original publications are reproduced with the permission of the copyright holders.
I.
II.
III.
IV.
V.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 7 –
ABBREVIATIONS
ACLS Advanced cardiac life support
ADR Adrenaline (epinephrine)
ASA American Society of Anesthesiologists physical status classification
ATR Atropine
AVP Vasopressin
CI Confidence interval
CNS Central nervous system
C.O. Cardiac output
CPR Cardiopulmonary resuscitation
CVP Central venous pressure
DOPA Dopamine
ECG Electrocardiography
EtCO2 End-tidal carbon dioxide
Hg Mercury
IC50 Halv maximal inhibitory concentration
ILE Intravenous lipid emulsion
IM Intramuscular
INS Insulin
IQR Interquartile range
IV Intravenous
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 9 –
ABSTRACT
Drug overdoses are the most common intoxications requiring hospitalisation. Severe toxicity can also occur during regional anaesthetic procedures due to inadvertent intravascular injection or rapid absorption of large doses of local anaesthetic. In severe cases, the outcome may be the death of the patient, despite the best currently available treatment. Recently, a rapidly administered large dose of lipid emulsion has been proposed as a treatment alternative based on encouraging results from animal studies and published case reports of its successful use. The mechanism by which lipid emulsion mitigates intoxication is thought to be the entrapment of lipophilic drugs into a “lipid sink” formed by the lipid emulsion in plasma.
This thesis consists of a series of studies on the entrapment effect of lipid emulsion on lipophilic drugs. The drugs studied are amiodarone (octanol:water distribution logP 7.24), bupivacaine (logP 3.31), mepivacaine (logP 2.16), and amitriptyline (logP 5.10). An anaesthetized pig model of intoxication was used in four of the studies, allowing evaluation of the effect of lipid therapy on the recovery from severe intoxication. A study comparing the entrapment of bupivacaine by a commercially available lipid emulsion to the experimental POPC/POPG lipid dispersion in pigs was performed after in vitro experiments suggesting that POPG/POPG dispersion had superior entrapment capability. In addition, a human study of the effect of lipid emulsion on the pharmacokinetics of a non-toxic intravenous dose of bupivacaine was also performed.
When a toxic dose of amiodarone was infused concurrently with lipid emulsion in a pig model, amiodarone was highly entrapped and its hypotensive adverse effect prevented. Lipid emulsion infusion following severe amitriptyline intoxication entrapped amitriptyline for the duration of the infusion, but improved neither the pigs’ recovery nor survival compared to placebo. When pigs were infused with the lipid emulsion following severe bupivacaine or mepivacaine intoxication, no significant entrapment occurred and no improvement of recovery compared to placebo was detected. The POPC/POPG lipid dispersion did not cause superior entrapment of bupivacaine compared to Intralipid® in pigs. In human volunteers, lipid emulsion compared to placebo decreased the context-sensitive half-life of a non-toxic dose of bupivacaine from 45 minutes to 25 minutes, but did not affect free plasma concentrations.
In summary, this thesis found little evidence for the current clinical use of lipid emulsion for the treatment of severe intoxications in the models used. Only in the case of amiodarone was a clear effect of lipid emulsion shown. This suggests that only extremely lipophilic substances are affected significantly by lipid emulsion in this setting.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 10 –
SAMMANFATTNING
Medicinöverdos är den vanligaste orsaken till förgiftning som kräver sjukhusvård. Förgiftningstillstånd kan också uppkomma vid regionalanestesi ifall lokalbedövningsmedlet oväntat injiceras direkt i blodomloppet eller absorberas ovanligt snabbt. Svåra förgiftningsfall kan leda till patientens död trots den bästa behandling. Baserat på uppmuntrande resultat från djurförsök och fallbeskrivningar har man nyligen velat lansera en ny vårdmetod som går ut på att snabbt injicera en stor dos intravenös fettemulsion. Den tänkta mekanismen är att fettemulsionen binder fettlösliga läkemedel i en ”fettreservoar” som bildas av fettemulsionen i plasma.
Denna avhandling består av en serie studier av fettemulsionens bindningseffekt på fettlösliga läkemedel. Läkemedlen som studerats är amiodaron (oktanol:vatten-distributions-logP 7.24), bupivakain (logP 3.31), mepivakain (logP 2.16) och amitriptylin (logP 5.10). En förgiftningsmodell med sövd gris användes i fyra av studierna. Modellen gör det möjligt att bedöma fettbehandlingens effekt på återhämtningen från svår förgiftning. Efter att in vitro-experiment antytt att den experimentella fettdispersionen POPC/POPG borde ha betydligt kraftigare bindningseffekt på fettlösliga läkemedel än en kommersiell fettemulsion, utfördes en jämförelsestudie mellan dessa i grisar förgiftade med bupivakain. Dessutom utfördes en humanstudie på fettemulsionens effekt på farmakokinetiken hos en icke-giftig dos bupivakain.
Amiodaron bands kraftigt av fettemulsion då denna gavs samtidigt med läkemedlet i en grismodell. Blodtryckssänkningen som orsakas av amiodaron uteblev också. Fettemulsionen band tydligt amitriptylin så länge fettemulsionsinfusionen pågick, men förbättrade inte grisarnas återhämtning eller överlevnad jämfört med placebo. Då intravenös fettemulsion gavs åt grisar efter att de förgiftats med bupivakain eller mepivakain bands ingetdera läkemedlet till signifikant grad och ingen förbättring av återhämtningen skedde. POPC/POPG-dispersionen band inte bupivakain till en signifikant högre grad än en kommersiell fettemulsion i grisar. Hos frivilliga försökspersoner förkortade fettemulsion en icke-giftig bupivakaindos kontext-känsliga halveringstid från 45 minuter till 25 minuter, men påverkade inte den fria bupivakainkoncentrationen i plasma.
Denna avhandling fann alltså få bevis för det nuvarande kliniska bruket av fettemulsion som behandling vid svåra förgiftningar i de använda modellerna. Endast i fallet amiodaron kunde en tydlig effekt visas. Detta antyder att endast extremt fettlösliga läkemedel kan påverkas signifikant av fettemulsion i detta sammanhang.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 11 –
YHTEENVETO
Lääkeyliannos on tavallisin syy sairaalahoitoa vaativille myrkytysoireille. Vaikea myrkytys voi myös syntyä laajoihin puudutuksiin liittyen, mikäli paikallispuudutetta ruiskutetaan vahingossa suonensisäisesti tai jos puudute imeytyy epätavallisen nopeasti verenkiertoon. Vakavasta puudutemyrkytyksestä kärsivä potilas voi kuolla parhaasta mahdollisesta hoidosta huolimatta. Puudutemyrkytyksen uudeksi hoidoksi on viimeaikaisten eläinkokeiden ja tapausselostusten perusteella esitetty nopeata rasvaemulsion suonensisäistä antamista. Rasvaemulsion vaikutusmekanismiksi on esitetty rasvaliukoisten lääkkeiden sitoutumista emulsion muodostamaan ”rasva-altaaseen” plasmassa.
Tämä väitöskirja koostuu sarjasta tutkimuksia, joissa tarkastellaan rasvaemulsion kykyä sitoa rasvaliukoisia lääkkeitä. Tutkitut lääkkeet ovat amiodaroni (oktanoli:vesi-jakautumis-logP 7.24), bupivakaiini (logP 3.31), mepivakaiini (logP 2.16) ja amitriptyliini (logP 5.10). Neljässä tutkimuksessa myrkytysmallina käytettiin nukutettuja porsaita. Näin arvioitiin rasvaemulsion vaikutusta vakavasta puudutemyrkytyksestä toipumiseen. Verrattiin myös kokeellisen POPC/POPG-rasvadispersion ja kaupallisen rasvaemulsion kykyä sitoa bupivakaiinia nukutetuilla porsailla. Lisäksi tutkittiin rasvaemulsion vaikutusta ei-myrkyllisen suonensisäisen bupivakaiiniannoksen farmakokinetiikkaan vapaaehtoisilla koehenkilöillä.
Kun porsaalle infusoitiin myrkyllinen annos amiodaronia yhtä aikaa rasvaemulsion kanssa, rasvaemulsio sitoi suuren määrän amiodaronia ja esti amiodaronin verenpainetta laskevan sivuvaikutuksen. Vakavan amitriptyliinimyrkytyksen jälkeen rasvaemulsio sitoi amitriptyliiniä rasvaemulsioinfuusion aikana, mutta ei parantanut porsaiden toipumista tai selviytymistä myrkytyksestä. Kun porsaille infusoitiin rasvaemulsiota vakavan bupivakaiini- tai mepivakaiinimyrkytyksen jälkeen, mitään merkitsevää sitomista ei havaittu, eikä rasvaemulsio vaikuttanut porsaiden toipumiseen myrkytyksestä. Kaupalliseen rasvaemulsioon verrattuna POPC/POPG-rasvadispersio ei sitonut bupivakaiinia paremmin nukutetuissa porsaissa. Vapaaehtoisissa koehenkilöissä rasvaemulsio lyhensi ei-myrkyllisen bupivakaiiniannoksen kontekstiherkkää puoliintumisaikaa 45 minuutista 25 minuuttiin. Tällä ei kuitenkaan ollut vaikutusta vapaaseen bupivakaiinipitoisuuteen.
Yhteenvetona voidaan todeta, että tämä väitöskirja ei käytetyssä koemallissa löytänyt tukea rasvaemulsion nykyiselle kliiniselle käytölle vakavien myrkytysten hoitoon. Ainoastaan amiodaronin tapauksessa havaittiin rasvaemulsiolla selvä vaikutus. Tämä viittaa siihen, että rasvaemulsio vaikuttaa tässä yhteydessä ainoastaan äärimmäisen rasvaliukoisiin aineisiin.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 12 –
INTRODUCTION
Severe intoxication is a major cause of death, especially in the young adult population (Hepp et al. 2011). In suicide cases, the cause of death is often one of the patient’s own prescriptions taken as an overdose (Vuori et al. 2003; Jonsson et al. 2004).However, nine out of ten deaths due to intoxication occur outside the hospital, and 82% of these are declared dead on scene without treatment (Bjornaas et al. 2010). If the patient reaches the hospital alive, even severe symptoms of intoxication prove transient, and 90% of patients can be discharged within 24 hours of hospitalization, with only 3.5% of these patients requiring treatment in the intensive care unit (Lapatto-Reiniluoto et al. 1998).
Iatrogenic local anaesthetic intoxication is a feared complication of regional anaesthetic techniques. It occurs most commonly with epidural block (33% of reported cases), axillary blocks (17%), and interscalene blocks (13%), probably due to the large doses of local anaesthetic used and the considerable vascularity of the injection sites (Di Gregorio et al. 2010). Despite the best treatment currently available, severe local anaesthetic intoxication can be fatal (Di Gregorio et al. 2010).
The idea that intravenous lipid emulsion could be used to affect the pharmacokinetics of a drug in circulation was first introduced fifty years ago. It was shown that rats infused lipid emulsion after an injection of the barbiturate thiopental emerged more rapidly from anaesthesia than rats infused the same volume of fat-free solution (Russell & Westfall 1962). Other early studies were published on the effect of lipid emulsion on chlorpromazine availability in rabbits (Krieglstein et al. 1974), and the effect of lipid emulsion on the elimination of phenytoin (Straathof et al. 1984). Although the studies show some effect of lipid emulsion, this did not kindle more widespread interest in the subject.
The serendipitous discovery of the apparently shielding effect of a large intravenous dose of lipid emulsion against bupivacaine toxicity in rats triggered renewed interest in the field (Weinberg et al. 1998). Additional experimental animal and isolated heart studies were performed (Weinberg 2002; Cave & Harvey 2009a), and although efficacy and safety had not been established by clinical trials, clinicians soon applied lipid therapy to seemingly hopeless cases of severe intoxication (Rosenblatt et al. 2006).
Following the case reports of successful treatment and encouraging results of animal studies, clinical adoption of lipid therapy has been advocated strongly by its proponents despite the limited evidence of its efficacy in man (Neal et al. 2010; Cave et al. 2010). One of the main arguments for the rapid adoption of this treatment despite the lack of evidence, is that many therapies in the emergency setting (e.g. dantrolene for malignant hyperthermia) are applied without controlled randomized studies supporting their use (Picard & Meek 2006; Di Gregorio et al. 2009). In most of these cases, knowledge of the mechanisms of
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 13 –
interaction between the pathologic state and the treatment allow inference of efficacy. For lipid therapy, this mechanism is thought to be the entrapment of lipophilic drugs into a
“lipid sink” formed by the enlarged lipid phase in plasma (Picard & Meek 2006).
The “lipid sink” theory of lipid therapy is mainly supported by in vitro studies of drug distribution (Bushey et al. 2011; Jamaty et al. 2010; Papadopoulou et al. 2012; Samuels et al. 2011; French, Smollin, Ruan, Wong, Drasner & Wu 2011b; Mazoit et al. 2009; Weinberg et al. 2010). Systematic studies of the effect of intravenous lipid emulsion on drug disposition in plasma in humans or animals have not been performed. Thus it has not been proved that the “lipid sink” effect actually occurs in the clinical situation. Without proof of the mechanism, inference of efficacy is impossible, and emergency use of lipid therapy cannot be considered evidence based.
This thesis examines whether intravenously administered lipid emulsion functions as a “lipid sink”, entrapping lipophilic drugs to an extent sufficient to improve recovery and survival from severe intoxication.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 14 –
REVIEW OF THE LITERATURE
LOCAL ANAESTHETIC SYSTEMIC TOXICITY
Within one year of its introduction into clinical use as a local anaesthetic, the symptoms of cocaine intoxication were described (Pilcher 1886). Local anaesthetic intoxication remains a feared complication, encountered most often when a large amount is inadvertently injected intravascularly, but can also occur due to unexpected absorption of the extravascularly injected local anaesthetic into the circulation from well-vascularized tissues. The injected dose of local anaesthetic may also be high enough to cause toxicity, even when absorbed at the expected rate. Fortunately, improved safety measures, such as the use of ultrasonography to guide the injection, and the use of safer local anaesthetics, such as ropivacaine, have made serious intoxications more rare (Weinberg et al. 1998; Drasner 2010). Intoxications occur in 1-2‰ of performed blocks (Mulroy 2002; Barrington et al. 2009).
The clinical symptoms of local anaesthetic systemic toxicity are numbness of the lips and tongue, disorders of hearing and vision, and a sensation of a metallic taste. In severe intoxication, these symptoms are followed by tremors progressing to generalized seizures, followed by loss of consciousness, respiratory arrest, and finally circulatory collapse (Weinberg et al. 2006; Di Gregorio et al. 2010). The aforementioned progression of symptoms occurs when the local anaesthetic plasma concentration rises gradually due to absorption from the extravascular space. When the local anaesthetic is injected directly into circulation, the first sign of toxicity may be circulatory collapse. Cardiovascular toxicity is caused by a variety of effects, the main effect being the blocking of fast sodium channels in cardiac myocytes. This interferes with impulse conduction the heart, and is reflected in the electrocardiogram (ECG) by increases in PR interval and QRS duration (Clarkson & Hondeghem 1985). Bupivacaine blocks inactivated cardiac sodium channels in a fast-in, slow-out fashion instead of the fast-in, fast-out fashion of drugs like lidocaine, for example, increasing its potential for cardiac toxicity (Mayr et al. 2008; Clarkson & Hondeghem 1985).
In addition to blocking sodium channels, lipophilic local anaesthetics (e.g. bupivacaine) may directly impair energy production in mitochondria. Three mechanisms have been suggested: uncoupling of oxygen consumption and adenosine triphosphate synthesis with a half maximal inhibitory concentration (IC50) for bupivacaine approximately 150 µM (Terada et al. 1990); inhibition of complex I in the respiratory chain with IC50 for bupivacaine 380 µM (Sztark et al. 1998); and inhibition of the fatty acid transport enzyme acylcarnitine transferase with IC50 for bupivacaine 260 µM (Weinberg et al. 2000). After rapid intravenous injection, however, the peak plasma bupivacaine concentration can reach approximately 100 µM (Hicks et al. 2009; Weinberg et al. 2000), thus the previously mentioned inhibitory concentrations for mitochondrial function likely remain outside those clinically encountered.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 15 –
Central to the treatment of severe local anaesthetic systemic toxicity is securing the airway to ensure adequate ventilation and oxygenation in order to prevent respiratory acidosis (Weinberg 2010). Convulsions should quickly be controlled in order to minimize oxygen consumption and the risk of developing metabolic acidosis. Both acidosis and alkalosis lower the threshold for toxicity (Candela et al. 2010; Adriani et al. 1966). Aggressive use of vasopressors to sustain coronary perfusion should expedite egression of the local anaesthetic from cardiac tissue, restoring cardiac function (Mazoit et al. 1993). Since local anaesthetics do not directly permanently damage the myocardium, there is a reasonable chance of survival even after prolonged resuscitation in cases where no other condition indicates poor prognosis (e.g. prolonged asphyxia). Due to the good prognosis, and if circulation can be maintained, even cardiopulmonary bypass is suggested (Weinberg 2010) and has been used in extreme cases (Long et al. 1989).
INTRAVENOUS LIPID EMULSION AS TREATMENT FOR SEVERE INTOXICATION
Intravenous lipid emulsion was first proposed as a treatment for local anaesthetic systemic toxicity after the observation that pre-treatment with a 20% intravenous lipid emulsion (Intralipid®; Fresenius-Kabi AB, Uppsala, Sweden) significantly raised the median lethal dose (LD50) of bupivacaine in rats (Weinberg et al. 1998). Following several case reports of human use, the first published in 2006 (Rosenblatt et al. 2006), and a few studies in animals (Weinberg 2002), recommendations for the use of intravenous lipid emulsion for treating local anaesthetic systemic toxicity have been published, although the evidence currently consists of small animal studies and case reports of human use (Neal et al. 2010; Cave et al. 2010). A systematic review of the current level of evidence for lipid treatment concluded that lipid emulsion use should only be considered when the patient remains severely cardiovascularly unstable even after maximal conventional treatment (Cave et al. 2011). The common protocol consists of an initial 1.5 ml/kg bolus of 20% Intralipid® followed by an infusion of 0.25 ml/kg/min for 30 minutes. The protocol also allows for repeated boluses in cases when there is no response to the therapy. The maximum recommended dose of 20% Intralipid®, according to the protocol, is 12 ml/kg, i.e. almost one litre in a patient weighing 80 kg. It should be noted that the rapid infusion mandated by the protocols exceeds the recommendation of the manufacturer (Fresenius-Kabi 2007). Although Intralipid® is currently the recommended lipid emulsion for the treatment of local anaesthetic systemic toxicity, several other brands that differ in composition have been used in both animal studies and case reports (Table 1).
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 16 –
Table 1. Composition of lipid emulsions used in animal studies or case reports (Russell & Westfall 1962; Granato et al. 2000; Rubin et al. 2000; B. Braun Melsungen AG 2005; Grimm 2005; Fresenius-Kabi 2007).
Com
posi
tion
(wei
ght %
)
Intr
alip
id®
Clin
Ole
ic®
Lipo
fund
in
MC
T/LC
T® (AK
A
Med
ialip
ide® )
Stru
ctol
ipid
®Iv
elip
®Li
posy
n®
III
Lipo
veno
es®
Lipo
mul
®
Soyb
ean
oil
204
1012
.820
2020
-
Oliv
e oi
l-
16-
--
--
-
Coco
nut o
il-
-10
7.2
--
--
Cott
onse
ed o
il-
--
--
--
15
Egg
phos
phat
ides
1.2
1.2
1.2
1.2
1.2
1.8
1.2
1.2
Gly
cero
l2.
52.
252.
52.
22.
52.
52.
5-
Sodi
um o
leat
e-
0.03
--
0.03
0.03
-
Long
-cha
in fa
tty
acid
s10
0 m
ol%
100
mol
%50
wt%
50 m
ol%
100
mol
%10
0 m
ol%
100
mol
%10
0 m
ol%
Med
ium
-cha
in fa
tty
acid
s-
-50
wt%
50 m
ol%
--
--
Osm
olar
ity
(mO
sm)
350
270
380
350
360
293
272
N/A
pH8.
07.
0-8.
06.
5-8.
58
7-9
8.4
6.5-
8.7
N/A
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 17 –
When used in high doses for the treatment of intoxication, lipid emulsion is hypothesised to act as a “lipid sink” (Picard & Meek 2006). The circulating liposomes are believed to expand a hydrophobic compartment in plasma, creating a significant concentration gradient, which entraps freely circulating lipophilic drugs. In turn, when free drug diffuses into the expanded lipid compartment, this creates a concentration gradient that draws drug away from the tissues into which it has been distributed. This reduction in tissue concentration would then lead to a reduced toxicity, since less drug molecules would be available to bind to receptors. The opposite mechanism is employed when liposomes are used to deliver drugs, e.g. slow-release bupivacaine (Bergese et al. 2012). In the case of liposome delivery of drugs, the drug concentration is highest in the liposomes, and the diffusion gradient favours drug egress and distribution into target tissues. For other possible mechanisms, please refer to section “Other mechanisms for the therapeutic effect of intravenous lipid emulsion in local anaesthetic-induced myocardial depression” of the Discussion.
Lipid emulsion is also employed clinically as a vehicle for intravenous delivery of drugs that are not water-soluble. In the field of anaesthesia, propofol (logP 3.77 (Tetko et al. 2001)), diazepam (logP 2.98 (Tetko et al. 2001)), and etomidate (logP 2.75 (Tetko et al. 2001)) are used. All of the three aforementioned drugs act on the central nervous system, and thus have to pass through the blood-brain barrier to act on their targets. The blood-brain barrier effectively blocks most hydrophilic drugs from entering the brain, but more lipophilic drugs pass through the barrier more effectively (Upton 2007). Counter to the proposed “lipid sink” effect, although the drugs are injected in a lipid emulsion, this does not prevent their rapid distribution (Upton 2007).
Only a few case reports or animal studies report measured drug concentrations, but in vitro studies show the tendency for lipophilic drugs to be entrapped into liposomes from plasma (Cave et al. 2011). After its introduction as a treatment for local anaesthetic systemic toxicity, intravenous lipid emulsion has been suggested to be used as a “universal antidote” for all intoxications caused by lipophilic drugs (Jamaty et al. 2010).
It has been proposed that in the rare instances of severe local anaesthetic cardiac toxicity, lipid emulsion could possibly counteract the inbition of the mitochondrial fatty acid transport enzyme acylcarnitine transferase by mass action (Weinberg et al. 2000). Whether this mechanism would have any effect on the other intoxications that lipid emulsion is thought to counteract remains unclear. No studies on the effect of lipid emulsion on acylcarnitine transferase inbition have been published.
In vitro, lipid emulsion has been shown to open voltage-gated calcium channels, increasing current through them, which would lead to increased contractility in cardiac myocytes (Huang et al. 1992). It is possible that the haemodynamic effects of intravenous lipid emulsion are partly due to this direct positive inotropy (Pennec et al. 2010).
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 18 –
It should be noted, that no human safety trials have been performed for this extremely high dose of lipid emulsion. A single study using nine rats estimated the LD50 of intravenous lipid emulsion at 67.7 ml/kg (Hiller et al. 2010). This is much higher than the total dose 9 ml/kg in the current recommendations (Neal et al. 2010; Cave et al. 2010). However, even when infused slowly as parenteral nutrition, intravenous lipid emulsion can cause pancreatitis or thromboemboli (Mirtallo et al. 2010).
PHARMACOKINETICS OF DRUG DISTRIBUTION
The treatment of severe intoxications with intravenous lipid emulsion is mainly based on the hypothesis that the lipid emulsion will beneficially alter the pharmacokinetics of the intoxicant. It is thought that a large volume of intravenous lipid emulsion will create a
“lipid sink” in plasma into which lipophilic drugs are entrapped.
In order to reach its target, a drug must cross several lipid bilayer cell membranes. Lipid bilayers consist of two lipid layers oriented oppositely, with the polar (hydrophilic) head groups oriented toward the outside of the bilayer, and the non-polar (hydrophobic) lipid tails toward the inside of the bilayer. Transport of drugs through biologic membranes occurs mostly through passive diffusion, but also by filtration, saturable carrier-mediated active transport, or rarely by endocytosis (Pazdernik & Kerecsen 2010). The more lipid soluble a drug is, the more readily it crosses membranes. Measured or predicted octanol:water coefficients are used to define the lipid solubility of drugs (see Table 2 for the predicted octanol:water partition coefficient logP and other pharmacokinetic variables for drugs significant for this thesis). Higher partition coefficient logP values indicate increasing lipophilicity. Since the value is logarithmic, a unitary increase translates to a tenfold increase in lipophilicity (Tetko et al. 2001). Nonpolar, uncharged molecules cross membranes the fastest, since they are most soluble in the thick hydrophobic layer of the membrane. Weak acids cross faster in an acidic environment, and weak bases in a basic environment, since they are less ionized in their respective environments.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 19 –
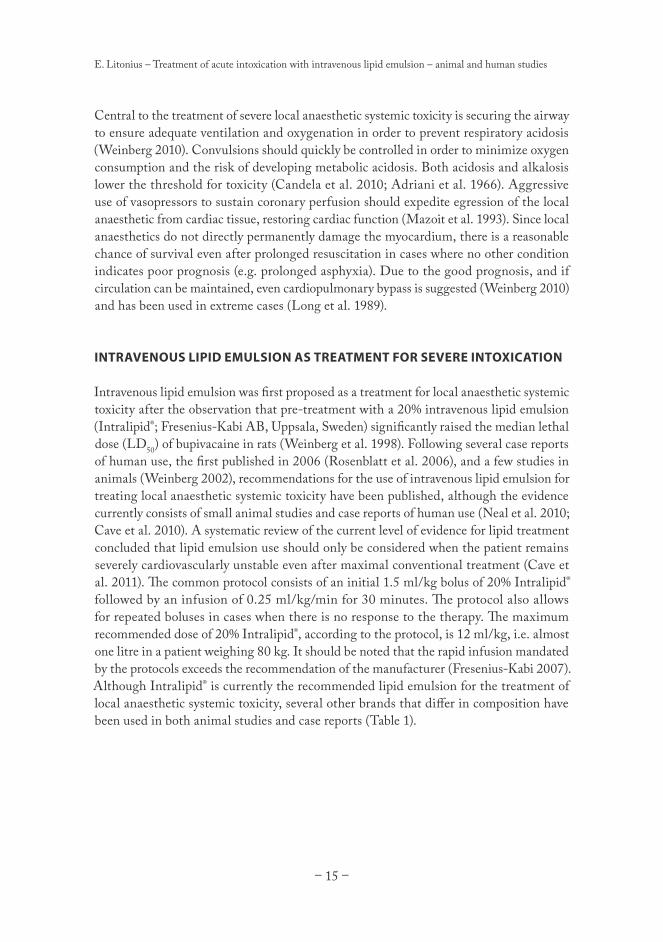
Table 2. Predicted octanol:water partition coefficient logP (Tetko et al. 2001), volume of distribution Vd (Chow et al. 1985; Russo et al. 1995; Yuen et al. 1996; Cheymol et al. 1997; Scholz 1997; Simon et al. 1998; Dony et al. 2000; Hiemke & Härtter 2000; Wójcicki et al. 2003; Ferner 2008; Ahn et al. 2008; Howland 2011a; Mylan 2011; Nelson & Lewin 2011; Anon n.d.), protein binding (Shayeganpour et al. 2005; Ferner 2008; Mylan 2011; Nelson & Lewin 2011; Schwartz & Kaufman 2011), and acid dissociation constant pKa (Andreasen et al. 1981; Motomura et al. 1993; Mashru et al. 2005; Stojanović et al. 2005; Vasskog et al. 2006; Rampono et al. 2007; Ferner 2008; Shalaeva et al. 2008; Joshi et al. 2009; Nielsen & Johansen 2009; Howland 2011b; Wishart et al. n.d.) for drugs involved in intoxication treated with intravenous lipid emulsion. Drugs examined in the present thesis are also included.
Drug logP Vd (l/kg) Protein binding pKa
Local anaesthetics
Bupivacaine 3.31 195% to albumin and alpha-1-acid
glycoprotein 8.1
Cocaine 3.08 1.96±0.292% to albumin and alpha-1-acid
glycoprotein 8.7
Ropivacaine 2.91 195% to albumin and alpha-1-acid
glycoprotein 8.2
Mepivacaine 2.16 175% to albumin and alpha-1-acid
glycoprotein 7.9
Prilocaine 1.87 240% to albumin and alpha-1-acid
glycoprotein 8.0
Lidocaine 1.81 170% to albumin and alpha-1-acid
glycoprotein 7.8
Anti-depressants
Amitriptyline 5.10 8.3 ± 2
96% to alpha-1-acid glycoprotein and other plasma
proteins
9.4
Sertraline 5.06 2098% to albumin and alpha-1-acid
glycoprotein9.47
Clomipramine 5.04 9-25 97.25% 9.3
Dosulepin 4.98 45 85% N/A
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 20 –
Drug logP Vd (l/kg) Protein binding pKa
Imipramine 4.53 21 60-95% 9.4
Doxepin 4.08 20 76% 8.96
Bupropion 3.28 18.6 84% N/A
Venlafaxine 2.69 7.5±3.7 27% 9.4
Antipsychotics
Chlorpromazine 5.18 20 >90% to albumin 9.3
Haloperidol 3.70 18 92% 8.66
Olanzapine 3.61 1000 93% 5.0 and 7.4
Quetiapine 2.93 10±4 83% 3.3 and 6.8
Cardiovascular
Amiodarone 7.24 66±44 65% to albumin, 30% to lipoprotein 5.6
Verapamil 5.32 4.7 83-92% 8.92
Diltiazem 3.09 5.3 70-80% 8.1
Carvedilol 3.05 115 98% 7.97
Propranolol 3.03 3.6 93% 9.5
Nebivolol 2.44 11.2 98% 8.22
Amlodipine 2.22 21 97.5% 8.6
Metoprolol 1.80 11 12% 9.5
Atenolol 0.57 0.7 6-16% 9.5
Other
Thiopental 3.05 2 80% 7.4
Phenytoin 2.26 0.9 90% 8.33
Lamotrigine 1.87 0.9-1.3 55% 5.7
Zopiclone 0.97 1.5 45% 6.7
Factors influencing the rate and extent of distribution of a drug include plasma protein binding, affinity to tissue proteins, acid-base status, drug transporters, and physiologic barriers, such as the blood-brain barrier (Rang, Dale & Ritter 1999a; Upton 2007). The initial phase of distribution is dependent on the free:bound drug ratio in plasma, transporters, and regional blood flow. Since the heart and brain have a much higher blood flow rate (55-550 ml/min/100 g) than muscle, connective tissue, and fat (1-5 ml/min/100 g), higher concentrations of drugs are initially found in the vital organs (Howland 2011b). However,
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 21 –
in critically ill patients, regional hypoperfusion significantly alters pharmacokinetics making drug distribution difficult to predict (Varghese et al. 2010).
The volume of distribution (Vd) is the apparent volume into which a drug is distributed after administration. It indicates how much of a drug is inside the plasma compartment. A Vd of 0.04 l/kg indicates that all administered drug remains in plasma. A Vd below 1 l/kg is considered low, especially when determining whether the drug can be removed by haemodialysis. A Vd significantly larger than 1 l/kg indicates that most of the drug resides outside the plasma compartment. Typically, the more lipophilic drugs also have a high Vd (Howland 2011b).
Several plasma proteins bind drugs. For this thesis, the most interesting proteins are α1-acid glycoprotein, which binds local anaesthetics with a high affinity but low capacity, and albumin, which binds many drugs with a low affinity but high capacity (Denson et al. 1984). Saturation of plasma protein binding capacity can increase the fraction of free drug in plasma at higher total concentrations, but the total plasma concentrations required for saturation widely exceed even the cardiotoxic 20 µg/ml (Denson et al. 1984). Acidosis, however, can significantly increase the fraction of free drug at lower plasma concentrations. For example, at a total plasma concentration of 3 µg/ml, a decrease in pH from 7.4 to 7.0 almost doubles the free plasma bupivacaine concentration from 0.054 to 0.101 µg/ml (Denson et al. 1984). Thus, prevention and prompt treatment of acidosis is a cornerstone of the management of local anaesthetic toxicity (Weinberg 2010).
PHARMACOLOGIC PROPERTIES OF DRUGS STUDIED
Bupivacaine and mepivacaine
Both bupivacaine and mepivacaine are amide-linked local anaesthetics. Their chemical structure consists of a lipophilic aromatic ring linked by an amide linkage to a hydrophilic amine (Figures 1 and 2). The amine is a weak base leading to partial ionization at physiological pH (7.35-7.45).
Figure 1. Chemical structure of bupivacaine. Figure 2. Chemical structure of mepivacaine.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 22 –
Bupivacaine has a pKa of 8.1, is 95% bound to albumin and alpha-1-acidic glycoprotein in plasma, and is significantly lipophilic with a octanol:water distribution logP of 3.31 (Tetko et al. 2001). The binding affinity of bupivacaine to alpha-1-acidic glycoprotein is decreased at lower pH (Denson et al. 1984). Bupivacaine has a steady-state volume of distribution of 1 l/kg. The minimum intravenous toxic dose of bupivacaine in humans is on average 1.6 mg/kg, although there is great inter-individual variation (Schwartz & Kaufman 2011). Mepivacaine is less lipophilic than bupivacaine with a octanol:water distribution logP of 2.16 (Tetko et al. 2001), has a pKa of 7.9 and is 75% bound to albumin and alpha-1-acidic glycoprotein in plasma, has a volume of distribution of 1 l/kg, with an average human intravenous toxic dose of 9.8 mg/kg (Schwartz & Kaufman 2011).
The mode of action of local anaesthetics is the reversible blockade of membrane bound sodium channels in conductive tissues such as nerve cells. The sodium channels have three states: open, inactive, and resting. Local anaesthetics have a high affinity for the open and inactive states, but dissociate rapidly from the resting state. Bupivacaine is an exception from this principle, since it rapidly binds to the open or inactive sodium channel, but is only slowly dissociated from the resting channel. This slow dissociation increases bupivacaine’s potency and cardiotoxicity (Clarkson & Hondeghem 1985; Mather et al. 2005). The receptor site for local anaesthetics on the sodium channels can only be reached from the intra-cellular side, meaning that the local anaesthetic must first traverse the cell membrane. This causes more lipophilic local anaesthetics to be more potent, since they traverse the cell membrane more easily (Schwartz & Kaufman 2011).
A wide range of local anaesthetics are currently used clinically. They can be infiltrated locally for small, superficial procedures, and are also employed by anaesthesiologists for neuraxial and regional anaesthesia, which enables major abdominal and limb surgery without general anaesthesia. The large doses used in regional and neuraxial anaesthesia increase the risk of toxicity (Rosenberg et al. 2004; Di Gregorio et al. 2010). The maximum safe dose varies between blocks, since injection locations vary in vascularity. The same dose of lidocaine leads to a three times higher plasma concentration when injected into the intercostal space compared to a subcutaneous injection (Rosenberg et al. 2004). Bupivacaine is considered the most toxic of the local anaesthetics in current clinical use, and its use for blocks requiring large doses is discouraged (Rosenberg et al. 2004).
Amiodarone
Amiodarone is a class III antidysrhythmic. Its chemical structure is an iodinated benzofurane (Figure 3). Its main effects is prolonging cardiac myocyte repolarization by blocking the delayed potassium rectifier current, but amiodarone also has weak α- and β-adrenergic antagonist activity and also blocks both L-type calcium channels as well as inactivated sodium channels (Nelson & Lewin 2011). Amiodarone is highly lipophilic with a octanol:water logP of 7.24 (Tetko et al. 2001), has a very large volume of distribution
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 23 –
(66±44 l/kg), and is approximately 65% bound to plasma albumin and 30% bound to plasma lipoproteins (Shayeganpour et al. 2005). Therapeutic doses prolong PR and QT intervals, and may cause sinus bradycardia or ventricular dysrhythmias. Administered intravenously as a rapid bolus, amiodarone causes hypotension, which is further potentiated by the solvent polysorbate 80 included in the routinely used formulation (Munoz et al. 1988).
Figure 3. Chemical structure of amiodarone.
Clinically, amiodarone is used to treat and prevent tachyarrhythmias (e.g. ventricular and supraventricular tachycardia) and atrial as well as ventricular fibrillation (Van Herendael & Dorian 2010). In long-term use, amiodarone has many serious adverse effects, including thyroid function disturbance, pulmonary fibrosis, liver damage, corneal microdeposits, and ataxia. In long-term use, amiodarone is typically taken perorally, but can also be administered intravenously (e.g. to combat persistent or recurring ventricular fibrillation during resuscitation from cardiac arrest). Intravenous amiodarone is the anti-arrhythmic drug of choice for local anaesthetic-induced life-threatening ventricular or supraventricular dysrhythmias (Weinberg 2002). Lidocaine, which otherwise has been recommended as a anti-arrhythmic for use during resuscitation from cardiac arrest (Boyd & Brady 2012), is not suitable for this purpose since it potentiates cardiotoxicity caused by itself or other local anaesthetics (Kyttä et al. 1991).
Acute amiodarone toxicity after an overdose is rare due its low bioavailability and large volume of distribution. The main risks are hypotension, in case of intravenous administration, or arrhythmias, if hypokalemia occurs simultaneously or other arrhythmics are present (Leatham et al. 1993).
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 24 –
Amitriptyline
Amitriptyline is a tertiary amine tricyclic antidepressant (Figure 4). It is 96% bound to plasma proteins, notably alpha-1-acidic glycoprotein, with a volume of distribution of 8.3±2 l/kg (Liebelt 2011) and a octanol:water distribution logP of 5.10 (Tetko et al. 2001). As is the case with local anaesthetics, the binding affinity of amitriptyline is decreased at lower pH (Liebelt 2011). It is metabolized into the active metabolite nortriptyline by the CYP2C9 enzyme in the liver, and exhibits enterohepatic circulation. Only 5% of amitriptyline is secreted unmetabolized by the kidneys. At therapeutic concentrations, amitriptyline and its metabolite nortriptyline inhibit presynaptic reuptake of noradrenaline and serotonin, accounting for its main antidepressant effect (Tatsumi et al. 1997).
Figure 4. Chemical structure of amitriptyline.
At toxic levels, amitriptyline blocks cardiac sodium channels resulting in an effect similar to local anaesthetic intoxication (Liebelt 2011). Sudden deterioration and tachyarrhythmias are common, with torsades des pointes occurring less frequently. The persistence of ECG changes is typical for amitriptyline intoxication, even after the patient’s condition has improved clinically (Liebelt et al. 1997). The current recommendation for treatment of amitriptyline toxicity is sodium bicarbonate to increase the binding affinity for alpha-1-acidic glycoprotein in addition to general advanced life support (Body et al. 2011; Liebelt 2011).
As an antidepressant, amitriptyline has been surpassed by the newer selective serotonin reuptake inhibitors because of their fewer adverse effects (Guaiana et al. 2009), but it continues to be used in the treatment of neuropathic pain (Saarto & Wiffen 2010). Many chronic depression patients also continue to use amitriptyline after originally initiating treatment with the drug. Amitriptyline intoxication is a major cause of suicidal death (Vuori et al. 2003; Jonsson et al. 2004).
CURRENT EVIDENCE SUPPORTING THE USE OF INTRAVENOUS LIPID EMULSION AS TREATMENT FOR SEVERE INTOXICATION
Intravenous lipid emulsion therapy for severe intoxication is a relatively young field. Although a few early studies on the pharmacokinetic effects of intravenous lipid emulsion
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 25 –
exist (Russell & Westfall 1962; Krieglstein et al. 1974; Straathof et al. 1984; Minton et al. 1987), its use as a treatment for severe intoxication was proposed as late as 1998 (Weinberg et al. 1998). Since this proposal, no randomized controlled human trials have been published. Thus, the evidence supporting this use of lipid emulsion consists only of animal studies and human case reports of varying quality (Cave et al. 2011).
The fact that lipophilic substances preferentially disperse into liposomes from water-based solutions (e.g. plasma) is easily demonstrated (Weinberg et al. 1998). When the three are mixed, and the mixture subsequently centrifuged to separate the lipid and aqueous phase, the lipophilic drug is found in the lipid phase in significantly higher concentrations than in the aqueous phase. However, this does not add much new information, since the measurement is nearly identical to the octanol:water distribution coefficient logP, by which the drug’s relative lipophilicity is measured. The interaction (i.e. entrapment potential) between lipid emulsions and drugs can also be measured efficiently in vitro using liposome electrokinetic capillary chromatography (LEKC), which requires very small amounts of analyte, enabling cost-effective testing of new lipid emulsion compositions intended for use as an entrapping agent (Muhonen et al. 2009).
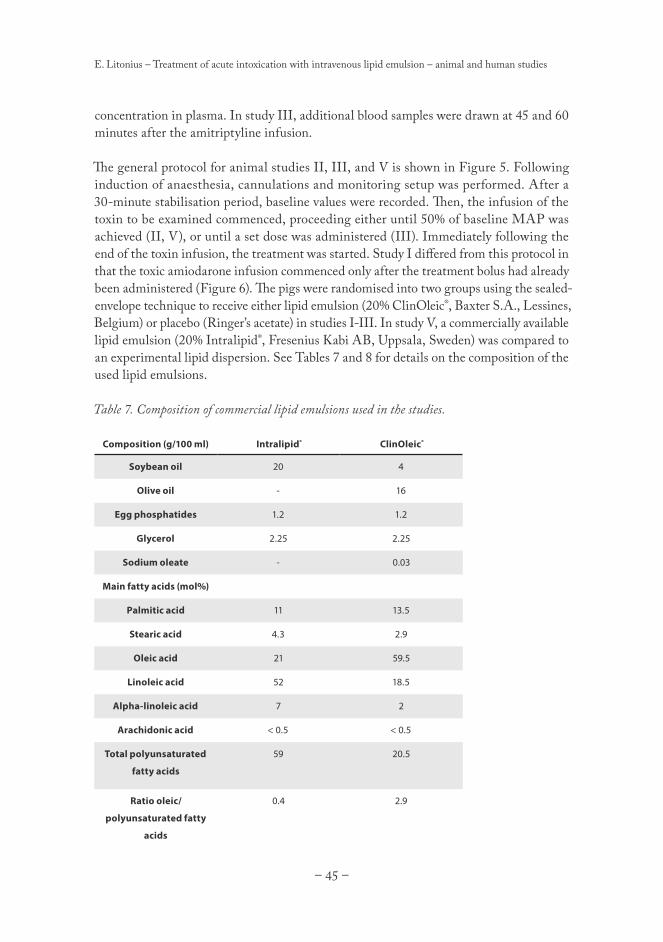
The commercially available 20% soybean oil-based lipid emulsion Intralipid® is currently recommended for the purposes of resuscitation from severe intoxication (Neal et al. 2010; Cave et al. 2010). Whether this is the optimal lipid emulsion for this purpose has not been determined. Reducing the lipid particle size from approximately 400 nm in off-the-shelf Intralipid® to approximately 100 nm greatly enhances the in vitro entrapment of bupivacaine as well as promoting recovery in a guinea pig heart model of bupivacaine intoxication (Morey et al. 2004). Altering the lipid composition of the infused liposomes may also increase their entrapment potential. In vitro, the commercially available Lipofundin®, which is a mixture of medium- and long-chain triglycerides (see Table 1), extracted more local anaesthetic from human serum than did Intralipid®, which consists purely of long-chain triglycerides (Ruan et al. 2012). By employing LEKC in an in vitro effort to optimize the liposome composition for bupivacaine entrapment, it was found that a 80%/20% mixture of 1-palmitoyl-2-oleyl-sn-glycero-3-phosphocholine (POPC) and 1-palmitoyl-2-oleyl-sn
-glycero-3-[phosphor-rac-(1-glycerol)] (POPG) had the strongest interaction (and thus entrapment potential) with bupivacaine (Lokajova et al. 2010). Whether these in vitro results can be repeated in vivo remains to be determined.
Previous studies on the use of intravenous lipid emulsion for the treatment of severe intoxication (examined in detail in the next sections) have mainly concentrated on showing improved survival or recovery from intoxication. Only a few studies report measurements of drug concentration in blood or tissue samples from whole animals (Weinberg et al. 1998; Mayr et al. 2008; Harvey et al. 2009; Hicks et al. 2009; Candela et al. 2010; Mauch et al. 2011; Li et al. 2012; Mauch et al. 2012), and before the studies presented in this thesis, no studies measuring actual drug entrapment by lipid emulsion in whole animals have
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 26 –
been published. Only one study reports both the total and free plasma concentrations of bupivacaine; in this pig study, the free plasma bupivacaine concentration was slightly, but significantly, lower at one time point during lipid emulsion treatment compared to treatment with adrenaline and vasopressin (Mayr et al. 2008).
Local anaesthetic systemic toxicity treated with intravenous lipid emulsion
AnimAl studies
There are currently 16 published controlled randomized animal studies on the treatment of local anaesthetic systemic toxicity using intravenous lipid emulsion (summarized in Table 3). Because of the large variation in treatment, timing, follow-up and end-variables, direct comparison of the studies proves difficult.
The first controlled randomized animal study of the treatment of local anaesthetic systemic toxicity using intravenous lipid emulsion was published in 1998 (Weinberg et al. 1998). When rats were pre-treated with 30% lipid emulsion, the bupivacaine dose required to cause cardiac arrest was raised almost 10-fold compared to the control group pre-treated with physiologic saline solution. Pre-treatment with smaller doses of intravenous lipid emulsion diminished the toxic response in a dose-dependent manner. Post-treatment with intravenous lipid emulsion also raised the LD50 of bupivacaine by almost 50%. A later study using dogs showed 100% survival in the group treated with lipid emulsion, with no dogs in the saline group surviving cardiac arrest caused by an intentional overdose of intravenous bupivacaine (Weinberg et al. 2003). A trial of the currently recommended intravenous lipid emulsion treatment regimen using rabbits showed 50% survival in the group treated with lipid emulsion and no survival in the group treated with saline following bupivacaine-induced cardiac arrest (Cave et al. 2009).
Four of the studies used the isolated rat heart as a model. The first study showed that adding intravenous lipid emulsion to the perfusion solution led to faster recovery from bupivacaine intoxication (Weinberg et al. 2006). In a similar setting, only the hearts perfused with solution containing lipid emulsion recovered (Chen et al. 2010). The same study showed that the speed of recovery correlated linearly with the concentration of lipid in the perfusion solution. The two aforementioned studies both show that the bupivacaine concentration in the heart reversely correlates with the concentration of lipid in the perfusion solution. In contrast, in a third study, lipid emulsion did not accelerate recovery of beating after intoxication, and only bupivacaine-intoxicated but not mepivacaine- or ropivacaine-intoxicated hearts recovered their beat rate and rate-pressure product more rapidly when perfused with solution containing lipid emulsion compared to a control solution without lipid emulsion (Zausig, Zink, Keil, Sinner, Barwing, Wiese & Graf 2009b). Lipid emulsion had a positive inotropic effect on hearts intoxicated with levobupivacaine (Stehr et al. 2007). However, lipid emulsion had no effect on pulse rate or conduction times. In contrast,
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 27 –
intravenously administered lipid emulsion was shown to cancel the cardiac electrophysiologic effects of bupivacaine in a pig study (Candela et al. 2010).
The results of studies comparing adrenaline, vasopressin or their combination with intravenous lipid emulsion are also contradictory. Studied in rats (Weinberg et al. 2008), resuscitation with intravenous lipid emulsion improved recovery from local anaesthetic systemic toxicity as measured by metabolic (serum lactate concentration, arterial blood gas samples) and hemodynamic parameters (heart rate, blood pressure). In the same study, four out of five rats resuscitated with adrenaline (30 µg/kg) developed pulmonary oedema. Another study (Di Gregorio et al. 2009) comparing resuscitation with intravenous lipid emulsion to either vasopressin alone or a combination of vasopressin and adrenaline (30 µg/kg) showed similar results: the hemodynamic, metabolic, and electrophysiologic parameters showed superior recovery in the group treated with intravenous lipid emulsion compared to the groups treated with the different vasopressors. As in the previously mentioned study (Weinberg et al. 2008), all animals treated with vasopressors developed pulmonary oedema. It should be noticed that the adrenaline dose in both of the aforementioned studies was quite large, corresponding to approximately 2 mg in a 70 kg human (twice the dose recommended for resuscitation). In a study comparing saline to lipid emulsion combined with different doses of adrenaline (Hiller et al. 2009), high doses of adrenaline (10 and 25 µg/kg) impaired survival when combined with lipid emulsion compared to lipid emulsion alone, or lipid emulsion combined with a smaller dose of adrenaline (1 and 2.5 µg/kg). A later rat study comparing a smaller adrenaline dose (10 µg/kg), either alone or combined with intravenous lipid emulsion, to either intravenous lipid emulsion alone or saline solution alone, concluded that the combination of adrenaline and intravenous lipid emulsion led to optimal survival and recovery (Li et al. 2012).
A study using a pig model compared treatment of a combined bupivacaine intoxication and asphyctic cardiac arrest with intravenous lipid emulsion to a combination of adrenaline and vasopressin (Mayr et al. 2008). In this study, contradicting the previously mentioned studies using rats (Weinberg et al. 2008; Di Gregorio et al. 2009), the vasopressor-treated group showed 100% survival while the group treated with intravenous lipid emulsion had no survivors. Metabolic parameters and coronary perfusion were both better in the vasopressor group after the start of treatment. Another pig study compared intravenous lipid emulsion to physiologic saline solution, with both groups additionally receiving adrenaline and vasopressin, as treatment for cardiac arrest induced by bupivacaine (Hicks et al. 2009). Intravenous lipid emulsion did not improve survival compared to physiologic saline solution. In addition, the surviving pigs that were treated with intravenous lipid emulsion required larger doses of noradrenaline after the return of spontaneous circulation (ROSC) to keep mean arterial pressure (MAP) above 60 mmHg. Otherwise, there were no differences between groups in hemodynamic or metabolic parameters. Bushey et al. discovered that intravenous lipid emulsion added to the normal advanced cardiac life support (ACLS) protocol did not improve the pigs’ survival from bupivacaine intoxication and asphyctic cardiac arrest (Bushey et al. 2011).
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 28 –
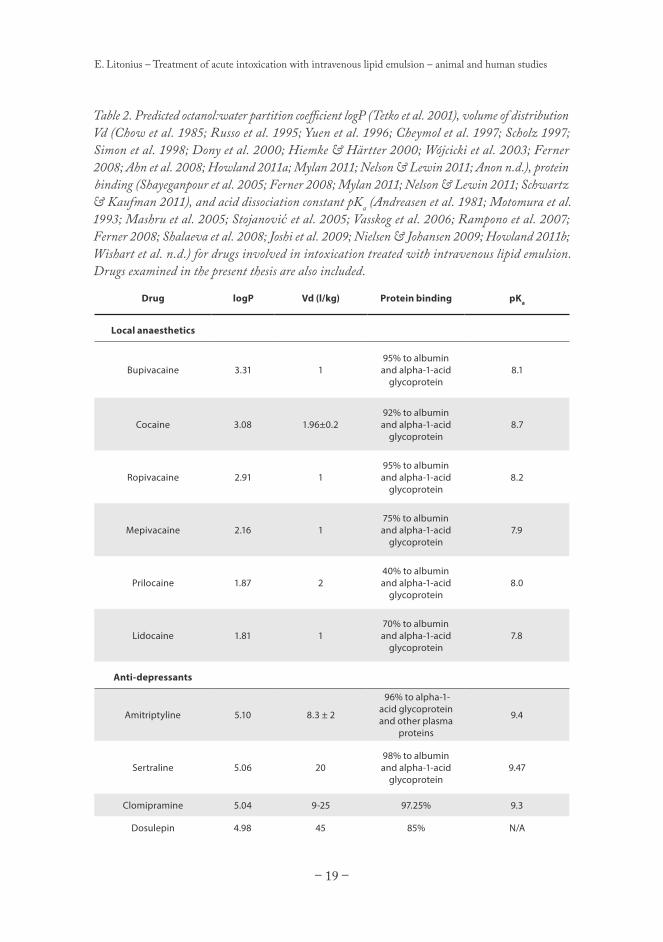
Table 3. Animal studies on the treatment of local anaesthetic intoxication with intravenous lipid emulsion. ACLS = Advanced cardiac life support, ADR = Adrenaline, AVP = Vasopressin, IV = Intravenous, KRB = Krebs-Ringer buffer, MAP = Mean arterial pressure, PSS = Physiologic saline solution, ROSC = Return of spontaneous circulation, RPP = Rate-pressure product.
Publication Model Local anaesthetic (IV)
Compared treatments (IV)
Treatment timing
Follow-up
Weinberg et al. 1998 part 1
Rat Bupivacaine 0.75% 10 ml/kg/min until cardiac arrest
1. 10%, 20%, or 30% Intralipid® 2. PSS 3 ml/kg for 5 min
5 min before bupivacaine
Until death
Weinberg et al. 1998 part 2
Rat Bupivacaine1. 15, 17.5, 20, or 22.5 mg/kg2. 10, 12.5, or 15 ml/kg
1. 30% Intralipid®
2. PSS7.5 ml/kg bolus, 3 ml/kg for 2 min
Immediately after bupivacaine
Until death
Weinberg et al. 2003
Dog Bupivacaine10 mg/kg
1. 20% Intralipid®
2. PSS4 ml/kg bolus, 0.5 ml/kg/min
10 min after cardiac arrest and open-chest heart massage
30 min
Weinberg et al. 2006
Rat heart
Bupivacaine500 µM
1. 20% Intralipid® until triglyceride concentration 1%2. KRB
Hiller et al. 2009 Rat Bupivacaine 20 mg/kg 1. PSS 5 ml/kg, 1 ml/kg/min for 2 min, 5 ml/kg at 5 min2. 30% Intralipid® 5 ml/kg, 1 ml/kg/min for 2 min, 5 ml/kg at 5 min3. Same as 2. + ADR 1 µg/kg4. Same as 2. + ADR 2.5 µg/kg5. Same as 2. + ADR 10 µg/kg6. Same as 2. + ADR 25 µg/kg
3 min after cardiac arrest
15 min
Candela et al. 2010
Pig Bupivacaine4 mg/kg
1. 20% Ivelip®
2. 20% Medialipide®
3. PSS1.5 ml/kg bolus, 0.25 ml/kg/min
30 s after bupivacaine
30 min
Chen et al. 2010 Rat heart
Bupivacaine100µM40 µM 3 min after cardiac arrest
20% Intralipid® at concentrations 0.25%, 0.5%, 1%, 2%, 4%, 8%, and 16%
1. ADR bolus at 1, 3, 5, 10 min, later every 3 min until RPP > 20% of baseline2. PSS 1 ml/kg at 1, 3, 5 min, 5 ml/kg at 10 min, then 0.5 ml/kg/min infusion3. PSS 1 ml/kg at 1, 3, 5 min. 20% Intralipid 5 ml/kg at 10 min, then 0.5 ml/kg/min infusion.4. PSS 1 ml/kg at 1, 3, 5 min. 20% Intralipid 5 ml/kg at 10 min, then 0.5 ml/kg/min infusion. ADR 10 µg/kg at 10 min.
25 min
CAse reports
Before the publication of the human study in this thesis, there have been no published randomized controlled studies on the effect of intravenous lipid emulsion on human plasma concentrations of bupivacaine or any other local anaesthetic. However, there are 29 published case reports on the use of intravenous lipid emulsion for the treatment of suspected local anaesthetic systemic toxicity (summarized in Table 4). The level of detail reported concerning the cases varies greatly, making it difficult to evaluate what effect, if any, intravenous lipid emulsion had on the patient’s recovery. One should obviously be aware of the possibility of especially severe publication bias when interpreting the impact of case reports regarding a new therapeutic modality since it can be assumed that reports of negative or poor outcome are underrepresented in the available literature (Easterbrook et al. 1991; Di Gregorio et al. 2010; De Oliveira et al. 2012).
Evaluated based on the case reports, lipid therapy for local anaesthetic intoxication seems effective. In many of the cases, return of spontaneous circulation, end of seizures, or end of central nervous system symptoms has occurred shortly after intravenous lipid emulsion infusion (Rosenblatt et al. 2006; Spence 2007; Whiteside 2008; Sonsino & Fischler 2009;
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 31 –
Charbonneau et al. 2009; Espinet & Emmerton 2009; Cordell et al. 2010; Wong et al. 2010). In most cases, some minutes elapsed between intravenous lipid emulsion infusion and recovery from intoxication (Foxall et al. 2007; Litz et al. 2008; Ludot et al. 2008; H. M. Smith et al. 2008; Markowitz & Neal 2009; Gnaho et al. 2009; Marwick, P. C. et al. 2009; Fuzaylov et al. 2010; Gallagher et al. 2010; Lin & Aronson 2010; Varela & Bums 2010; Harvey, Cave, Chanwai & Nicholson 2011a; Mizutani et al. 2011; Shih et al. 2011; Dix et al. 2011). In three cases, the time to recovery was over 10 minutes or even hours (Litz et al. 2006; McCutchen & Gerancher 2008; Warren et al. 2008). In the aforementioned three cases, it would seem unlikely that lipid emulsion actually contributed to the patient’s recovery, since the proposed mechanisms support mainly a more rapid effect as reported in the majority of published cases.
In only two reported cases was there no beneficial effect of intravenous lipid emulsion (Calenda & Dinescu 2009; Aveline et al. 2010). Even in those two cases, the patients made a full recovery, showing that severe local anaesthetic systemic toxicity is not uniformly lethal when not treated with intravenous lipid emulsion. In fact, a recent review of published cases shows that only one of 93 reported severe intoxications between 1979 and 2009 led to the death of the patient (Di Gregorio et al. 2010). Intravenous lipid emulsion was only used in seven of the 92 successfully treated intoxications.
Based on the case reports, there seems to be little difference between local anaesthetics in the efficacy of intravenous lipid emulsion. Nevertheless, in most case reports on successful resuscitation using intravenous lipid emulsion, the causative agent was the most lipophilic local anaesthetic bupivacaine. In both cases where no beneficial effect of intravenous lipid emulsion was observed, the less lipophilic ropivacaine, mepivacaine, or lidocaine had been used. This would suggest, as predicted by the proposed “lipid sink” theory, that the efficacy of lipid emulsion therapy depends on the lipophilicity of the local anaesthetic (Mazoit et al. 2009).
In many cases, intravenous lipid emulsion has been infused at approximately the same time as other treatments (Rosenblatt et al. 2006; McCutchen & Gerancher 2008; Marwick, P. C. et al. 2009; Fuzaylov et al. 2010). In the cases where no other simultaneous treatment was administered, it is still possible that intravenous lipid emulsion had no effect and the patient recovered due to distribution of the local anaesthetic into inert tissues or a delayed effect of previous medications (Spence 2007; Litz et al. 2008; Ludot et al. 2008; Whiteside 2008; Espinet & Emmerton 2009; Lin & Aronson 2010; Mizutani et al. 2011). No harmful effects of intravenous lipid emulsion have been reported, except in two cases. In one case, serum amylase concentration increased significantly (Marwick, P. C. et al. 2009), and in the other, the patient developed lung oedema (Fuzaylov et al. 2010).
Cocaine intoxication has also been treated using intravenous lipid emulsion (Jakkala-Saibaba et al. 2011). A young cocaine abuser presented with seizures and hypotensive ventricular
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 32 –
tachycardia, and was anaesthetized with thiopental and loaded with phenytoin. He was infused lipid emulsion when his circulation deteriorated, requiring increasing noradrenaline support. Sinus rhythm returned 15 minutes after the initial intravenous lipid emulsion bolus, and the noradrenaline infusion could be discontinued within 30 minutes.
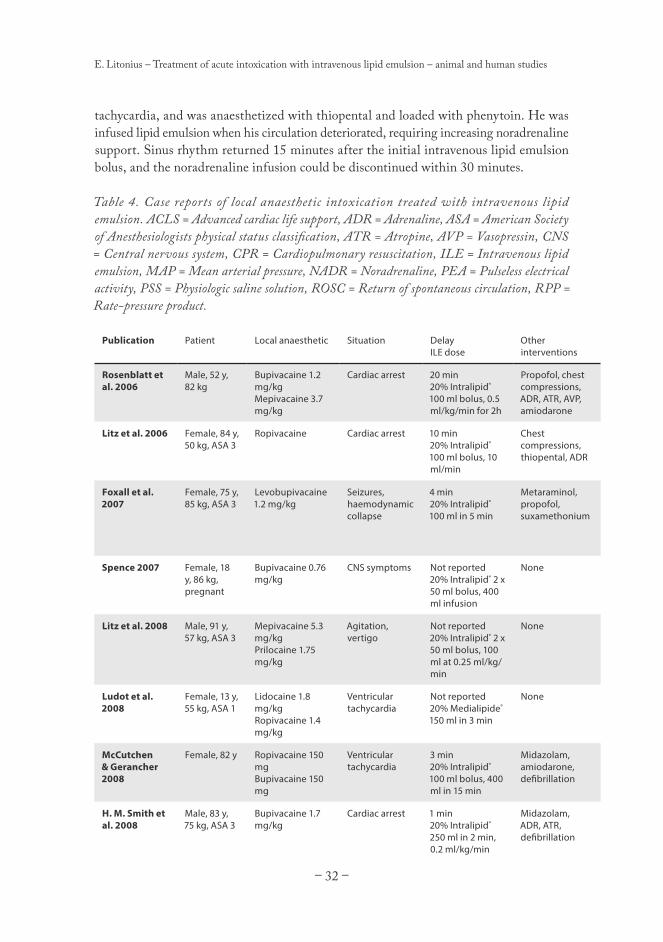
Table 4. Case reports of local anaesthetic intoxication treated with intravenous lipid emulsion. ACLS = Advanced cardiac life support, ADR = Adrenaline, ASA = American Society of Anesthesiologists physical status classification, ATR = Atropine, AVP = Vasopressin, CNS = Central nervous system, CPR = Cardiopulmonary resuscitation, ILE = Intravenous lipid emulsion, MAP = Mean arterial pressure, NADR = Noradrenaline, PEA = Pulseless electrical activity, PSS = Physiologic saline solution, ROSC = Return of spontaneous circulation, RPP = Rate-pressure product.
Publication Patient Local anaesthetic Situation Delay ILE dose
Other interventions
Rosenblatt et al. 2006
Male, 52 y, 82 kg
Bupivacaine 1.2 mg/kgMepivacaine 3.7 mg/kg
Cardiac arrest 20 min20% Intralipid® 100 ml bolus, 0.5 ml/kg/min for 2h
Cardiac arrest No delay20% Intralipid® 150 ml in 90 s, 350 ml in 30 min
ADR, chest compressions
Aveline et al. 2010
Female, 51 y, 57 kg, ASA 2
Lidocaine 7.0 mg/kgRopivacaine 1.97 mg/kg
Seizure Not reported20% Intralipid® 100 ml bolus
Midazolam
Cordell et al. 2010
Female, 17 y Bupivacaine 75 mg
Cardiac arrest Not reported3 x 100 ml bolus
ACLS, midazolam, propofol, ADR
Fuzaylov et al. 2010
Female, 13 y, 50 kg, ASA 1
Bupivacaine 0.5 mg/kg
Ventricular tachycardia
3-4 min100 ml bolus
ADR, dopamine
Gallagher et al. 2010
Male, 28 y, 56 kg
Lidocaine 10 mg/kgBupivacaine 1.9 mg/kg
PEA Not reported2 units 20% ILE
CPR, ADR, AVP, ATR, NaHCO3
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 34 –
Lin & Aronson 2010
Male, 2 d, 3.2 kg
Bupivacaine 2.5 mg/kg
Ventricular tachycardia
Not reported20% Intralipid® 1 ml/kg
CPR
Varela & Bums 2010
Female, 83 y, 70 kg, ASA 2
Bupivacaine 2.1 mg/kgRopivacaine 4.3 mg/kg
Ventricular tachycardia
5 min20% Liposyn® III 500 ml in 1 h
ATR, midazolam
Wong et al. 2010
Male, 6 y, 24 kg
Bupivacaine 0.25 mg/kg/h for 8h
Arrhythmia Not reported20% Intralipid® 20 ml bolus, 0.25 ml/kg/min 30 min
CPR, ATR, ADR
Harvey, Cave, Chanwai & Nicholson 2011a
Female, 69 y, 80 kg
Bupivacaine 1.9 mg/kgLidocaine 0.6 mg/kg
Seizures, bradycardia
8 min20% Intralipid® 100 ml bolus, 400 ml during 45 min
Midazolam, ATR, ADR, metaraminol
Mizutani et al. 2011
Male, 24 y, 66 kg
Ropivacaine 3.0 mg/kg
CNS symptoms 10 min100 ml 20% ILE in 10 min
None
Shih et al. 2011 Female, 69 y, 48.5 kg
Bupivacaine 0.77 mg/kgLidocaine 4.6 mg/kg
Bradycardia > 15 min20% Lipovenoes® 50 ml bolus
ATR, ephedrine, NaHCO3
Dix et al. 2011 Male, 57 y Lidocaine, plasma concentration 7.6 µg/ml
PEA 55 min20% Intralipid® 1 ml/kg bolus, 0.25 ml/kg/min for 30 min
ADR, amiodarone, MgSO4, calcium gluconate, NaHCO3
Jakkala-Saibaba et al. 2011
Male, 28 y Cocaine Seizures, ventricular tachycardia
Not reported20% Intralipid® 120 ml bolus, 380 ml in 20 min
Thiopental, phenytoin, NADR, NaHCO3, diazepam
Other intoxications treated with intravenous lipid emulsion
Since the lipophilicity of the drug causing the intoxication is thought to be the main determinant for the effectiveness of lipid emulsion therapy, it has been suggested to be used as a “universal antidote” for all intoxications caused by lipophilic drugs (Cave & Harvey 2009a; Weinberg 2010). As with local anaesthetic systemic toxicity, there are no randomized controlled human studies on the subject, and the recommendation is based on animal studies and human case reports.
AnimAl studies
There are 14 published randomized controlled animal studies on the treatment of intoxications, other than local anaesthetic systemic toxicity, with intravenous lipid emulsion (summarized in Table 5). As was the case with the local anaesthetic studies, these studies also vary greatly concerning the exact treatment, timing, follow-up time, and measured
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 35 –
parameters, making direct comparison of results difficult.
The first controlled randomized study on the effect of intravenously administered lipid emulsion on drug disposition aimed to shorten the time to emergence from thiopental anaesthesia in rats (Russell & Westfall 1962). The study showed that 10% and 15% intravenous lipid emulsion shortened the time to emergence significantly. There was also evidence that intravenous lipid emulsion diminished the reduction in cortical slice oxygen consumption caused by thiopental. Much later, it was shown in rats that intravenous lipid emulsion also partly reverses the respiratory depression caused by thiopental (Cave et al. 2005).
The elimination half-life of phenytoin was lengthened by both intravenous lipid emulsion and physiologic saline compared to no treatment in rats (Straathof et al. 1984).
The effect of intravenous lipid emulsion on chlorpromazine was also studied decades before the current interest in the subject. A study published in 1974 using rabbits showed that the free plasma concentration of the very lipophilic drug chlorpromazine (octanol:water logP 5.81 (Tetko et al. 2001)) decreases significantly after infusion of lipid emulsion compared to infusion of a xylitol solution (Harvey & Cave 2007). In addition, all rabbits infused intravenous lipid emulsion survived double the LD50 dose of chlorpromazine, while all the rabbits in the xylitol group perished.
Intravenous lipid emulsion treatment has also been studied in models of tricyclic antidepressant intoxication. A rabbit study showed that the MAP of animals treated with intravenous lipid emulsion recovered faster from clomipramine intoxication compared to animals treated with sodium bicarbonate or physiologic saline (Harvey & Cave 2007). There was no difference in pulse or cardiac conduction rates between groups. The same study showed that only the animals treated with intravenous lipid emulsion survived an intoxication that lowered their mean arterial pressure to 25 mmHg, even though all animals were treated with adrenaline and chest compressions in addition to the infusion. The same authors also showed that clomipramine intoxicated rabbits recovered quicker, as measured by haemodynamic parameters, when treated with a combination of lipid emulsion as intravenous infusion and as intraperitoneal dialysis compared to physiologic saline (Harvey et al. 2009). They also noted that both the plasma and the dialysate from the animals treated with lipid emulsion had a significantly higher clomipramine concentration compared to the animals treated with physiologic saline.
The LD50 dose of verapamil was almost doubled when the rats were infused lipid emulsion when compared to physiologic saline (Tebbutt et al. 2006). When dogs intoxicated with verapamil were infused lipid emulsion, mean arterial pressure, heart rate and minute volume all recovered faster than in dogs infused PSS (Bania et al. 2007). Lipid emulsion also improved survival. The optimal intravenous lipid emulsion dose for survival from
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 36 –
verapamil intoxication was determined to be 18.6 ml/kg in rats (Perez et al. 2008). The optimal hemodynamic recovery was obtained with the larger dose 24.8 ml/kg. This is a huge dose, considering that the currently recommended safe limit for lipid emulsion in this setting is 12 ml/kg, and that the blood volume of a rat is approximately 70 ml/kg. Such a large dose infused rapidly would undoubtedly raise blood pressure simply due to its volume.
Intravenous lipid emulsion has also been studied as a treatment for ß-blocker intoxication. When rats were pre-treated with intravenous lipid emulsion, the lethal dose of propranolol tended to increase, but the study had insufficient power to show statistical significance (Cave et al. 2006). It was later shown in rabbits that treating propranolol intoxication with intravenous lipid emulsion led to faster haemodynamic recovery compared to the control group (Harvey & Cave 2008). However, when treatment with intravenous lipid emulsion was compared to glucose-insulin infusion in rabbits intoxicated with propranolol, the animals treated with glucose-insulin showed a more rapid haemodynamic recovery (Harvey, Cave, Lahner, Desmet, Prince & Hopgood 2011b). Neither treatment was superior to the other in aiding survival. There was no difference in survival from atenolol intoxication when comparing intravenous lipid emulsion to physiologic saline in rabbits (Cave & Harvey 2009b), but early mean arterial pressure recovery was faster in the animals treated with intravenous lipid emulsion. However, 15 minutes later, the situation was reversed and the mean arterial pressure was higher in the rabbits treated with physiologic saline. There was no difference between the control group and the group treated with intravenous lipid emulsion in a rabbit model of metoprolol intoxication (Browne et al. 2010).
Table 5. Animal studies on the treatment of other intoxications with lipid emulsion. ILE = Intravenous lipid emulsion, INS = Insulin, IV = Intravenous, MAP = Mean arterial pressure, PSS = Physiologic saline solution, Vf = Respiration rate.
Publication Model Drug (IV) Compared treatments (IV)
Harvey, Cave, Lahner, Desmet, Prince & Hopgood 2011b
Rabbit Propranolol 40 mg/kg (PO)30 min later 0.3 mg/kg bolus and 4 mg/kg/h IV
1. 20% Intralipid® 10 ml/kg2. INS 3 IU/kg + glucose 0.5 g/kg + PSS 7 ml/kgin 5 min
MAP 50% of baseline
60 min
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 38 –
HumAn study And CAse reports
The effect of lipid emulsion on the plasma concentration of amitriptyline has been studied in four volunteers, who took amitriptyline perorally for ten days (Minton et al. 1987). On the eighth day, two of the volunteers were infused lipid emulsion and the other two volunteers physiologic saline. The infusions were repeated in reverse on the tenth day. The plasma concentration of amitriptyline tended to be 14% higher following intravenous lipid emulsion compared to physiologic saline; however, the small study lacked power to show the statistical significance.
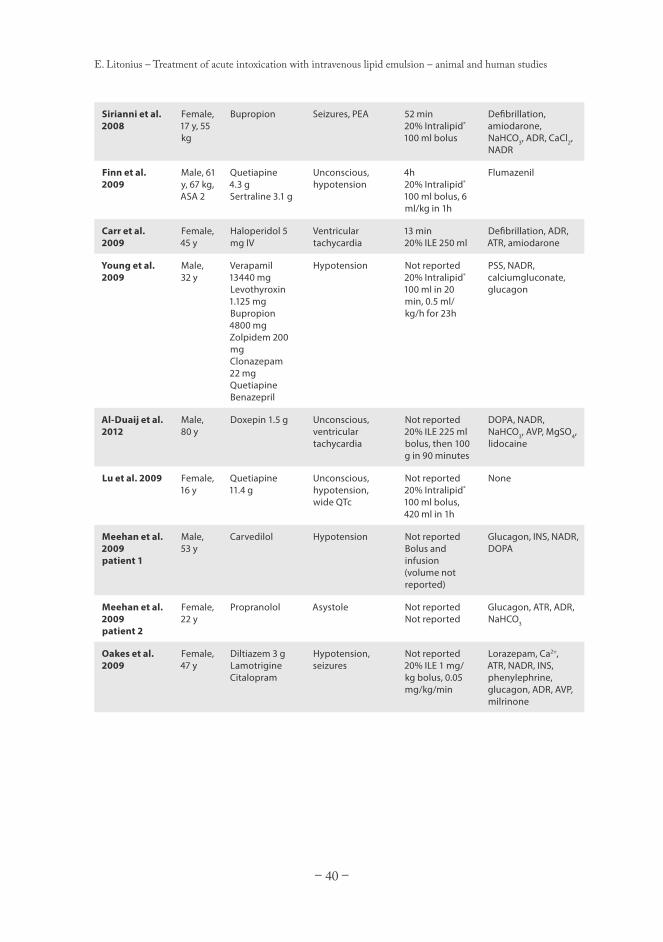
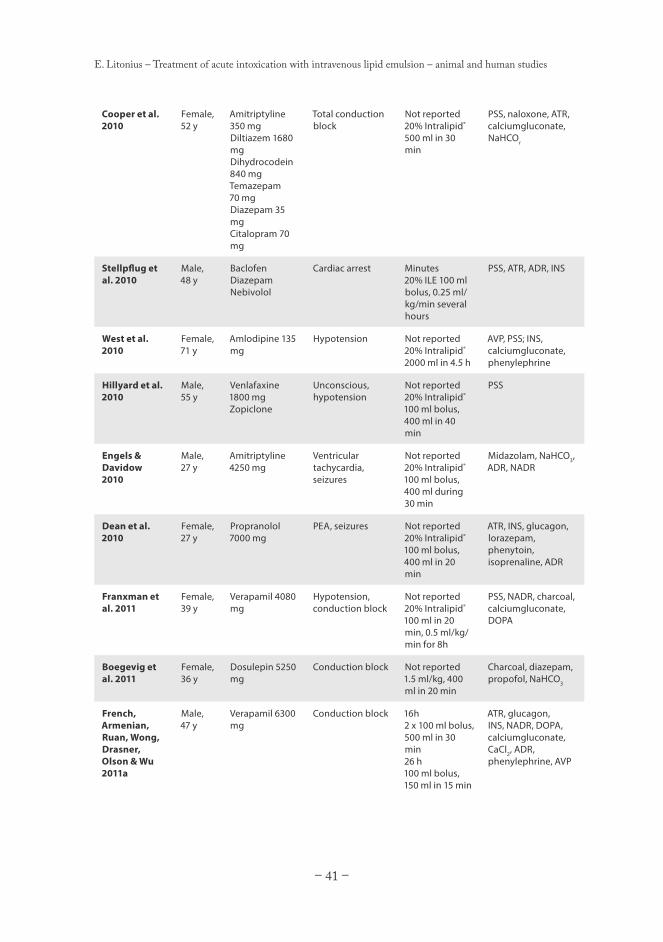
There are currently 26 published case reports on the treatment of intoxications by drugs other than local anaesthetics with intravenous lipid emulsion (summarized in Table 6). As with the case reports of local anaesthetic intoxications, these case reports are also of varying detail; some provide so little detail that it is impossible to appraise the effect of lipid emulsion.
Most of the published cases report a significant benefit of treatment with intravenous lipid emulsion. The spectrum of reported effects is quite wide. Some cases of antidepressant intoxication report an almost immediate improvement following lipid emulsion infusion (Engels & Davidow 2010; Boegevig et al. 2011; Castanares-Zapatero et al. 2012). In one case, intravenous lipid emulsion treatment, after almost an hour of unsuccessful advanced cardiac life support, led to the near immediate return of spontaneous circulation (Sirianni et al. 2008). In other cases, the patient only improved gradually several hours after intravenous lipid emulsion infusion (Hillyard et al. 2010; Livshits et al. 2011; Al-Duaij et al. 2012; Carr et al. 2012).
Similarly, in some cases of intoxication by drugs affecting the cardiovascular system, such as ß-blockers or anti-arrhythmics, the recovery was near instant or occurred within minutes after intravenous lipid emulsion infusion (Dolcourt & Aaron 2008; Meehan et al. 2009; Dean et al. 2010; Stellpflug et al. 2010; Jovic-Stosic et al. 2011; Harvey & Cave 2012). For example, the return of spontaneous circulation was achieved or the patient emerged from unconsciousness almost immediately following intravenous lipid emulsion infusion. It should be noted, that at least in one of these cases (Stellpflug et al. 2010), adrenaline had been administered immediately prior to intravenous lipid emulsion, so the recovery could more likely be due to a delayed effect of the adrenaline than due to the intravenous lipid emulsion infusion.
In other cases, the patients’ condition improved only slowly during several hours or even days, but the turning point was the intravenous lipid emulsion infusion (Harchelroad & Palma 2008; Carr et al. 2009; Oakes et al. 2009; Young et al. 2009; Cooper et al. 2010; Franxman et al. 2011; Montiel et al. 2011; French, Armenian, Ruan, Wong, Drasner, Olson & Wu 2011a; Liang et al. 2011). There was no discernable benefit of intravenous lipid
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 39 –
emulsion in a reported case of amlodipine intoxication, and the patient was administered a total dose of intravenous lipid emulsion almost five times the recommended dose (West et al. 2010). Treatment was eventually discontinued because of the poor prognosis and the patient perished. Another patient died due to a combined intoxication of verapamil and atenolol, even after showing transient improvement subsequent to intravenous lipid emulsion infusion (Dolcourt & Aaron 2008). French et al. reported a reduction in free serum verapamil following intravenous lipid emulsion infusion in samples obtained during resuscitation (French, Armenian, Ruan, Wong, Drasner, Olson & Wu 2011a).
When used to treat anti-psychotic intoxication, intravenous lipid emulsion has led to rapid patient improvement (Finn et al. 2009; Lu et al. 2009; Weinberg et al. 2009; McAllister et al. 2012). Additionally, in one case, the intoxication symptoms returned after intravenous lipid emulsion infusion was discontinued, but could be reversed by repeated intravenous lipid emulsion administration (McAllister et al. 2012).
As with the local anaesthetic intoxication case reports, interpretation of the aforementioned case reports of intravenous lipid emulsion use is complicated by the fact that the patients were treated with multiple drugs concurrently. In four cases, adverse effects were reported. In two of the cases, the patient developed pneumonia (Sirianni et al. 2008; Cooper et al. 2010). The other two patients developed more serious symptoms. One case was diagnosed with pancreatitis, renal failure, and raised levels of liver enzymes (Oakes et al. 2009). The other case had pneumonia, colitis, sepsis, transient thrombocytopenia, as well as liver and kidney failure (Livshits et al. 2011). As with the possible beneficial effects, these deleterious effects cannot directly be attributed to the intravenous lipid emulsion, since the patients were concurrently treated with several drugs. The initial intoxication and possible aspiration of gastric contents should also not be disregarded.
Table 6. Human case reports on the treatment of other intoxications with lipid emulsion. ADR = Adrenaline, ASA = American Society of Anesthesiologists physical status classification, ATR = Atropine, AVP = Vasopressin, DOPA = Dopamine, ILE = Intravenous lipid emulsion, INS = Insulin, NADR = Noradrenaline, PEA = Pulseless electrical activity, PSS = Physiologic saline solution.
Publication Patient Drug (PO) Situation Delay ILE dose
Other interventions
Dolcourt & Aaron 2008
Male, 52 y
Verapamil, metoprolol
Shock Not reported20% ILE 1.5 ml bolus, 0.25 ml/kg/min. Repeated.
PSS, Ca2+, DOPA, NADR, INS, cardiac pacing
Harchelroad & Palma 2008
Female, 46 y
Atenolol, paracetamol, ethanol
Sinus bradycardia Not reported20% ILE 1000 ml in 2h
ATR, PSS, glucagon
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 40 –
Sirianni et al. 2008
Female, 17 y, 55 kg
Bupropion Seizures, PEA 52 min20% Intralipid® 100 ml bolus
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 43 –
AIMS OF THE STUDY
The aim of the study was to examine in pigs and in humans whether an intravenously infused lipid emulsion would act as a “lipid sink” and entrap local anaesthetics and other lipophilic drugs to an extent that may prevent or treat intoxication by such drugs. Since the
“lipid sink” theory is currently the purported mechanism for lipid treatment of intoxication, studies confirming a high degree of drug entrapment would greatly encourage the clinical use of the treatment.
The specific aims were:
To evaluate to what extent intravenously infused lipid emulsion entraps amiodarone, amitriptyline, bupivacaine, and mepivacaine (I-V).
To examine whether intravenously infused lipid emulsion prevents intoxication caused by amiodarone (I).
To examine whether intravenously infused lipid emulsion enhances recovery from intoxications caused by amitriptyline, bupivacaine and mepivacaine (II, III, V).
To examine whether in vitro lipid-bupivacaine interaction measurements can predict the in vivo entrapping effect of lipid emulsions (V).
1.
2.
3.
4.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 44 –
MATERIALS AND METHODS
ANIMAL STUDIES (I-III, V)
Young landrace pigs (age approximately 3 months, weight 20-30 kg) were used for all of the animal studies. The pig is often used as a toxicological model because of its physiologic resemblance to humans (Swindle et al. 2011), and young pigs are of a size suitable for cannulas and endotracheal tubes intended for human use.
Prior to the experiment, the pigs were fasted for at least 12 hours with free access to water. In study I, the pigs were given an intramuscular (IM) injection of 15 mg/kg ketamine 20-30 minutes before the induction of anaesthesia. For the other animal studies, no premedication was employed. In studies I, II, and III, anaesthesia was induced using intravenous (IV) ketamine (400 mg, with additional 50-100 mg IV boluses as required). In study V, anaesthesia was induced using isoflurane in 21% O2 administered by mask.
Following induction, the pig’s trachea was intubated and mechanical ventilation initiated with 2% isoflurane in 21% O2. The ventilator was set as volume controlled at a frequency of 20 breaths/min, with tidal volumes adjusted to keep end-tidal CO2 (EtCO2) between 4.5 and 5.0 kPa.
Two auricular veins were cannulated for IV fluid administration. The internal jugular vein (preferably the right) was cannulated for fluid administration and central venous pressure (CVP) measurement using a introducer (Avanti®+; Cordis Corporation, Miami, FL, USA). In studies III and V, a 5F (1.67 mm external diameter) pulmonary artery catheter (Model 132F5; Edwards Lifesciences LLC, Irvine, CA, USA) for core temperature, cardiac output (C.O.), and pulmonary capillary wedge pressure (PCWP) measurements, was inserted through the introducer. A femoral artery was exposed and cannulated (Arterial Cannula with FloSwitch 20G, Becton-Dickinson, Singapore, Singapore). Continuous 5-lead ECG data was recorded for offline analysis using surface electrodes.
A 30-minute stabilisation period followed the cannulations. During this period, the pig’s core temperature was adjusted to 37.5-39.0°C using external radiant heating (OPN Ceiling Control Unit Type VII; Aragona, Sweden). Ringer’s acetate (Ringer-Acetat Baxter Viaflo®, Baxter Medical, Sweden) was infused to keep the pigs CVP at 2-8 mmHg.
Following the 30-minute stabilisation period, baseline values of heart rate, MAP, C.O. (III and V), PCWP (III and V), SpO2, and EtCO2 were recorded. The same parameters were recorded during the experiment at the same time points as blood samples were drawn. Blood samples were drawn at baseline, immediately following the toxin infusion, and 5, 10, 20, and 30 minutes later during the treatment infusion for the measurement of toxin
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 45 –
concentration in plasma. In study III, additional blood samples were drawn at 45 and 60 minutes after the amitriptyline infusion.
The general protocol for animal studies II, III, and V is shown in Figure 5. Following induction of anaesthesia, cannulations and monitoring setup was performed. After a 30-minute stabilisation period, baseline values were recorded. Then, the infusion of the toxin to be examined commenced, proceeding either until 50% of baseline MAP was achieved (II, V), or until a set dose was administered (III). Immediately following the end of the toxin infusion, the treatment was started. Study I differed from this protocol in that the toxic amiodarone infusion commenced only after the treatment bolus had already been administered (Figure 6). The pigs were randomised into two groups using the sealed-envelope technique to receive either lipid emulsion (20% ClinOleic®, Baxter S.A., Lessines, Belgium) or placebo (Ringer’s acetate) in studies I-III. In study V, a commercially available lipid emulsion (20% Intralipid®, Fresenius Kabi AB, Uppsala, Sweden) was compared to an experimental lipid dispersion. See Tables 7 and 8 for details on the composition of the used lipid emulsions.
Table 7. Composition of commercial lipid emulsions used in the studies.
Composition (g/100 ml) Intralipid® ClinOleic®
Soybean oil 20 4
Olive oil - 16
Egg phosphatides 1.2 1.2
Glycerol 2.25 2.25
Sodium oleate - 0.03
Main fatty acids (mol%)
Palmitic acid 11 13.5
Stearic acid 4.3 2.9
Oleic acid 21 59.5
Linoleic acid 52 18.5
Alpha-linoleic acid 7 2
Arachidonic acid < 0.5 < 0.5
Total polyunsaturated
fatty acids
59 20.5
Ratio oleic/
polyunsaturated fatty
acids
0.4 2.9
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 46 –
The treatment infusion was infused at the rate recommended for the clinical treatment of intoxications (Weinberg 2010); first a 1-minute bolus of 1.5 ml/kg, then a 29-minute infusion of 0.25 ml/kg/min.
Figure 5. General protocol for animal studies II, III, and V
Figure 6. Study I protocol.
Following the treatment infusion, and in study III after an additional 30-minute follow-up, the pigs were euthanized during continued anaesthesia using IV potassium chloride.
npigs
Randomization
n/2 pigs
ToxinInfusion
ILE1.5 ml/kg
1 min
ILE0.25 ml/kg/min
29 min
ToxinInfusion
Ringer1.5 ml/kg
1 min
Ringer0.25 ml/kg/min
29 minn/2pigs
S am pling t im e (m in) Baseline 0 5 10 20 30
20pigs
Randomization
10 pigs 1 min
ILE1.5 ml/kg
ILE0.25 ml/kg/minAmiodarone
20 mg/kg total dose
1 min
Ringer1.5 ml/kg
Ringer0.25 ml/kg/min10
pigs
S am pling t im e (m in) Baseline 0 5 10 20
Amiodarone20 mg/kg total dose
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 47 –
HUMAN STUDY (IV)
Eight male Caucasian volunteers aged 21-35, with a mean body weight of 77 kg (range 67-100 kg, standard deviation [SD] 10 kg), and a body mass index of 24 kg/m2 (range 21-30 kg/m2, SD 3 kg/m2), were recruited for the study. They were determined to be healthy through medical history, physical examination, and routine laboratory tests. None of the subjects used any continuous medication, but one of them was a tobacco smoker.
The experiments were performed in the post-anaesthesia care unit at Töölö Hospital (a part of Helsinki University Central Hospital, Helsinki, Finland). The volunteers were monitored during the experiment using continuous three-lead ECG, non-invasive blood pressure, and pulse oximetry via finger probe. Antebrachial superficial veins on both arms were cannulated using large-bore cannulas (minimum 17G) to ensure venous access allowing the high flow rate required (approximately 100 ml/min). One arm was set up for venous blood sampling, and the other for infusions. The arm set up for infusions and the corresponding infusors with tubing were covered to ensure blinding of both volunteers and researchers. The infusions were prepared and infusors operated by anaesthesia nurses not otherwise participating in the study.
The experiment protocol is shown in Figure 7. To minimize the number of volunteers required while ensuring sufficient statistical power, the study was conducted using a crossover protocol. Each volunteer was thus infused both lipid emulsion and placebo (Ringer’s acetate) during two separate sessions with a 2-3 week washout period.
Figure 7. Human study protocol.
After recording baseline values, all volunteers were infused 0.5 mg/kg bupivacaine IV over 20 minutes. The dose was safe (Knudsen et al. 1997), but reliably quantifiable in blood samples. Immediately following the bupivacaine infusion, the treatment infusion (lipid emulsion or placebo) commenced with a 1-minute bolus of 1.5 ml/kg. After the bolus, the treatment infusion continued at a rate of 0.25 ml/kg/min for 29 minutes. The total volume infused during the experiment was approximately 10 ml/kg.
8men
Randomization
4men
Bupivacaine0.5 mg/kg
20 min
ILE1.5 ml/kg
1 min
ILE0.25 ml/kg/min
29 min
Bupivacaine0.5 mg/kg
20 min
Ringer1.5 ml/kg
1 min
Ringer0.25 ml/kg/min
29 min4
men
Bupivacaine0.5 mg/kg
20 min
ILE1.5 ml/kg
1 min
ILE0.25 ml/kg/min
29 min
Bupivacaine0.5 mg/kg
20 min
Ringer1.5 ml/kg
1 min
Ringer0.25 ml/kg/min
29 min
Washout2-3 weeksSession 1 Session 2
S am pling t im e (m in) Baseline 0 5 10 20 30 Baseline 0 5 10 20 30
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 48 –
Heart rate and blood pressure were recorded and blood samples drawn at baseline (before the bupivacaine infusion) and 0, 5, 10, 20, and 30 minutes after the start of the treatment infusion. The volunteers were asked to report any adverse effects occurring during or after the experiments in an interview following the second session.
PREPARATION OF POPC-POPG LIPOSOME DISPERSION
Lipid vesicles were prepared from 1-palmitoyl-2-oleyl-sn-glycero-3-phosphocholine (POPC) and 1-palmitoyl-2-oleyl-sn-glycero-3-[phospho-rac-(1-glycerol)] (POPG) either by the lipid film method or by direct hydration of lipid powder with 0.9% NaCl solution. For the lipid film method, stock solutions of the lipids in chloroform (20 mM POPC and 13 mM POPG) were used. The stock solutions were mixed in appropriate proportions to obtain the composition desired. The mixture was then dried by evaporation using a stream of pressurized air. Traces of remaining solvent were removed by evacuation under reduced pressure for a minimum of 16h. The dry lipid residue was then hydrated at 60°C for 60 minutes with shaking using 0.9% NaCl solution, yielding multilamellar vesicles. The resulting dispersion could then be used either crude, or after further processing by sonication or filtration. Sonication was performed with the lipid in an ice-water bath using a microtip Branson Sonifier 250 sonicator (Branson Ultrasonic, Danbury, CT, USA). Following sonication, the lipid dispersion was centrifuged at 14 900 g at 15°C for 5 minutes to remove any metal residue left by the sonication tip.
To determine the interaction strength between bupivacaine and liposomes, a partial filling electrokinetic capillary chromatography (PF-EKC) method (Hewlett-Packard 3DCapillary Electrophoresis System; Agilent, Waldbronn, Germany) was used. Uncoated fused-silica capillaries (Polymicro Technologies, Phoenix, AZ, USA), 50 µm inner diameter (375 µm outer diameter), 30/38.5 cm (length to detector/total length) were preconditioned by rinsing for 15 min with 0.1M sodium hydroxide, for 10 min with water, and for 5 min with lipid dispersion at 940 mbar of pressure. A plug of lipid dispersion was followed by a sample plug consisting of 30 µg/ml bupivacaine and 0.5 mM thiourea in background electrolyte injected in 10 s at 15 mbar, run at 20 kV at a temperature of 37°C with UV-detection at 200 nm. The runs were repeated 3-6 times.
SAMPLE HANDLING
Following all experiments, the plasma was separated from the blood samples by centrifugation for 10 minutes at 3000 rpm (2500 g) and stored at -22°C. When all samples
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 49 –
in a study had been obtained, the frozen plasma samples were thawed for analysis.
In study I, the amiodarone concentration was measured with a Sciex API 2000 Q Trap LC/MS/MS system (Sciex Division of MDS, Toronto, Ontario, Canada) using the method described by Kollroser and Schober in 2002. (Kollroser & Schober 2002).
In study II, the bupivacaine concentration was measured with a Sciex API 2000 Q Trap LC/MS/MS system (Sciex Division of MDS, Toronto, Ontario, Canada) using the method described by Tanaka et al. in 2006. (Tanaka et al. 2006).
In study III, the amitriptyline concentration was measured with a Sciex API 2000 Q Trap LC/MS/MS system (Sciex Division of MDS, Toronto, Ontario, Canada) using the method described by Samanidou et al. in 2007. (Samanidou et al. 2007).
In study IV, the bupivacaine concentration was measured with a Sciex API 2000 Q Trap LC/MS/MS system (Sciex Division of MDS, Toronto, Ontario, Canada) using the method described by Ledger in 2003. (Ledger 2003).
In study V, the bupivacaine concentration was measured with a Sciex API 2000 Q Trap LC/MS/MS system (Sciex Division of MDS, Toronto, Ontario, Canada) using the method described by Hoizey et al. in 2005. (Hoizey et al. 2005).
The total plasma toxin concentration was measured in aliquots of all samples. This concentration measure includes all drug present in the samples, including that bound to proteins and entrapped in the lipid phase.
In studies IV and V, aliquots of samples drawn after the start of the treatment infusion were ultrafiltered using Centrifree® Ultrafiltration Devices (Millipore Ireland Ltd., Tullagreen, Carrigtwohill, Co. Cork, Ireland) centrifuged at 1260 g for 30 minutes at 25°C. The free bupivacaine concentration was measured in the ultrafiltrate. This concentration measure includes the plasma bupivacaine that is neither bound to proteins nor entrapped in the lipid phase.
In all studies, aliquots of samples drawn after the start of the treatment infusion were centrifuged at 14000 rpm (20800 g) in order to separate the lipid and aqueous fractions. The unentrapped toxin concentration was measured in the lipid poor aqueous fraction. This concentration measure excludes the plasma toxin that is entrapped in the lipid phase, but includes toxin bound to plasma proteins as well as free toxin.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 50 –
STATISTICAL ANALYSES
All data were analysed using the following statistics software:
Study I: PASW for Macintosh version 18 (SPSS Inc., Chicago, IL, USA), Prism 4 for Macintosh (GraphPad Software Inc., La Jolla, CA, USA), and StatView for PowerPC version 5.0 (SAS Institute Inc., Cary, NC, USA).
Study II: SPSS for OS X version 19.0.1 (IBM Corporation, Somers, NY, USA), and R version 2.12.1 (R Foundation for Statistical Computing, Vienna, Austria).
Study III: SPSS for OS X version 19.0.1 (IBM Corporation, Somers, NY, USA), and R version 2.12.2 (R Foundation for Statistical Computing, Vienna, Austria).
Studies IV and V: Prism for OS X version 5.0d (GraphPad Software Inc., La Jolla, CA, USA).
Variable values are presented as median with interquartile range (IQR) and range, mean with standard deviation (SD) and range, or median difference with 95 % confidence interval (CI) and range. The effect of treatment over time was evaluated using repeated measures analysis of variance (study I) with post hoc Bonferroni correction. The difference between groups at each time point was evaluated by the non-parametric Mann-Whitney U test (studies I-III), paired t-test (study IV), or unpaired t-test (study V). The Holm-Bonferroni method (Holm 1979) was used to correct for multiple comparisons (studies II, III). The context-sensitive plasma half-life of bupivacaine was estimated using non-linear regression (studies IV, V).
To estimate the required sample sizes, a power analysis was performed when planning the studies. Since no data on the effect of intravenous lipid emulsion on the plasma concentration of the drugs studied was available, groups of ten animals each were arbitrarily chosen. Limiting the risk of a Type I error at less than 0.05, while keeping the risk of a Type II error at less than 0.2, a effect size Cohen’s d of 1.3 is required for statistical significance in studies I-III and V (Faul et al. 2007). For study IV, the power analysis was based on data from study II. It was expected that a 20% difference in total bupivacaine plasma concentration between lipid emulsion and placebo (Ringer’s acetate) would be clinically significant. With parameters for Type I and Type II errors as previously mentioned, eight subjects in a crossover design proved sufficient. With this sample size, the study’s power is 87%, and the smallest detectable difference in total plasma bupivacaine concentrations is 16%.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 51 –
RESULTS
STUDY I
The aim of this study was to investigate to what extent intravenously administered amiodarone was entrapped by ILE in anesthetized pigs and whether the entrapment prevents amiodarone-induced hypotension.
Entrapment of amiodarone
The time course of the plasma amiodarone concentration in the Lipid group was significantly (P < 0.0005) different from that in the Control group (Figure 8). The plasma amiodarone concentrations increased during the continuous amiodarone infusion in both groups ending at a median of 96.8 mg/l (IQR 85.4-102.0 mg/l, range 84.2-120.0 mg/l) at 20 minutes in the Lipid group and 21.5 mg/l (IQR 18.9-22.3 mg/l, range 15.6-30.8 mg/l) at 20 minutes in the Control group, indicating significant entrapment.
Figure 8. Median amiodarone plasma concentrations. Error bars show 25th-75th percentile.
The unentrapped amiodarone concentration measured in the lipid-poor aqueous fraction (separated from the lipaemic plasma by centrifugation) was much lower than in the uncentrifuged lipaemic sample (Figure 8). After 20 minutes of concurrent amiodarone and lipid emulsion infusion, the median amiodarone concentration was 13.3 mg/l (IQR
0 5 10 200
30
60
90
120
Time (min)
Plas
ma
amio
daro
ne c
once
ntra
tion
(mg/
l) Lipid (Total)
Control (Total)Lipid (Unentrapped)
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 52 –
12.0-13.7 mg/l, range 10.5-13.9 mg/l) in the lipid-poor aqueous fraction (difference to lipaemic plasma concentration -83.6 mg/l, 95% CI -93.3 to -73.8 mg/l) indicating that most of the amiodarone remained entrapped in the lipid phase after the centrifugation.
Hemodynamic effect of intravenous lipid emulsion
The time course of MAP in the Lipid group was significantly different (P < 0.001) from that in the Control group (Figure 9). MAP in the Lipid group did not decrease during the amiodarone infusion, while MAP was 26 mmHg (95%CI 9-43 mmHg) lower in the Control group at the lowest measured point (after 10 minutes of concurrent amiodarone and Ringer infusion). There was no difference in heart rate between groups.
Figure 9. Mean arterial pressure. Amiodarone infusion from time point 1 to time point 21 min. Error bars show 25th-75th percentile.
Intravenous lipid emulsion side-effects
Within 10 minutes of the start of lipid emulsion infusion, the skin of all pigs in the Lipid group turned increasingly red. The two pigs that turned exceptionally red had SpO2 67% and 83% at the end of the experiment; the other eight Lipid pigs’ SpO2 remained within the normal range (91-100%). Haemodynamically, the two desaturated pigs did not differ from the rest, but blood gas samples taken at the end of the experiment showed hypoxemia in both pigs (PaO2 38.6 mmHg/5.15 kPa and 50.6 mmHg/6.75 kPa) and hypercapnia in one of the pigs (PaCO2 50.6 mmHg/6.75 kPa). There was no change in airway pressure in any of the pigs during the experiment.
0 5 10 20 300
25
50
75
100
Time (min)
Mea
n ar
teria
l pre
ssur
e (m
mH
g)
Lipid
Control
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 53 –
STUDY II
The aim of this study was to determine whether local anaesthetics of differing lipophilicity are entrapped by intravenous lipid emulsion to different degree, and whether this affects the hemodynamic recovery from severe local anaesthetic intoxication in a pig model.
Entrapment of bupivacaine and mepivacaine
There was no overall difference in plasma local anaesthetic concentrations between Lipid and Control groups (Figure 10). After 20 and 30 minutes of lipid emulsion infusion, the median total plasma bupivacaine concentration was 1.8 mg/L (95%CI 0.5-2.9 mg/l, P = 0.016) and 1.9 mg/l (95% CI 0.6-3.3 mg/l, P = 0.016) higher in the lipid group, respectively.
Figure 10. Median plasma bupivacaine (A) and mepivacaine (B) concentrations. * = Bupivacaine Lipid (Total) vs. Control (Total) concentration P < 0.05. Error bars show 25th-75th percentile.
Hemodynamic and electrophysiologic recovery from bupivacaine or mepivacaine intoxication
There was no overall difference in recovery of either MAP or heart rate between Lipid and Control groups (Figure 11). After 10 and 15 minutes of lipid emulsion infusion following bupivacaine intoxication, the median MAP of the Lipid group was 16 mmHg (95% CI 0-39 mmHg, P = 0.016) and 15 mmHg (95% CI 4-26mmHg, P = 0.021) higher.
Tox 5 10 20 301
10
100
Time (min)
Plas
ma
bupi
vaca
ine
conc
entr
atio
n (m
g/l)
Lipid (Total)
Control (Total)Lipid (Unentrapped)
* *
Lipid (n)Control (n)
1010 8
A
Tox 5 10 20 301
10
100
Time (min)
Plas
ma
mep
ivac
aine
con
cent
ratio
n (m
g/l)
Lipid (Total)
Control (Total)Lipid (Unentrapped)
Lipid (n)Control (n)
1010
9
B
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 54 –
Figure 11. Median MAP during treatment infusion after bupivacaine (A) or mepivacaine (B) intoxication. * = Lipid vs. Control MAP P < 0.05. Error bars show 25th-75th percentile.
In the ECG, the PQ interval and QRS width broadened at the end of the bupivacaine infusion in all pigs in comparison with baseline and returned to normal at the end of the experiment. There were no significant differences in PQ interval and QRS width between Lipid and Control groups at any point.
STUDY III
The aim of this study was to determine whether the lipophilic tricyclic antidepressant amitriptyline is significantly entrapped by intravenous lipid emulsion, and whether this affects the hemodynamic recovery from severe amitriptyline intoxication in a pig model.
Entrapment of amitriptyline by intravenous lipid emulsion
At the start of the treatment infusion following infusion of 15 mg/kg amitriptyline, the median total plasma concentration of amitriptyline was 12.1 mg/l (IQR 10.3-13.2 mg/l, range 6.4-18.4 mg/l) in the Lipid group and 12.6 mg/l (IQR 11.3-14.4 mg/l, range 8.3-17.6 mg/l) in the Control group (the concentration range after therapeutic doses is 30-300 µg/l (Bailey & Jatlow 1976)). Subsequently, the amitriptyline concentration declined steeply in both groups, remaining similar five minutes into the treatment infusion (Figure 12). During the rest of the treatment infusion, however, the total plasma amitriptyline concentrations diverged. The total plasma amitriptyline concentration continued to decline in the Control group, with a half-life of approximately 30 minutes, suggesting further distribution into
Tox 5 10 20 3015 25
30
60
90
120
Time (min)
Mea
n ar
teri
al p
ress
ure
(mm
Hg)
LipidControl
*
*
Lipid (n)Control (n)
1010 8
A
Tox 5 10 20 3015 25
30
60
90
120
Time (min)
Mea
n ar
teri
al p
ress
ure
(mm
Hg)
LipidControl
Lipid (n)Control (n)
1010
9
B
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 55 –
tissues. During the same time period, the total plasma amitriptyline concentration did not decline at all in the Lipid group. At 30 minutes, the total plasma concentration was approximately 90% higher in the Lipid group than in the Control group (P < 0.001).
Figure 12. Median plasma amitriptyline concentrations. * = Lipid (Total) vs. Control (Total) amitriptyline concentration P < 0.05. Error bars show 25th-75th percentile.
In contrast, the unentrapped amitriptyline concentration in the Lipid group samples (the concentration remaining in the lipid-poor aqueous phase of plasma after separating the lipid from the samples by centrifugation) declined in parallel with the total plasma concentration in the Control group.
At the start of the treatment infusion, the mean free amitriptyline fractions were similar in the Lipid and Control group (4.2% and 4.6%, respectively). At the end of the treatment infusion, the mean free fraction of amitriptyline was significantly lower in the Lipid group (1.1% vs. 3.0%, P = 0.014). However, the mean free concentrations at the same time point did not differ significantly (0.049 mg/l, SD 0.014 mg/l, range 0.036-0.070 mg/l in the Lipid group, 0.077 mg/l, SD 0.033, range 0.025-0.130 in the Control group, P = 0.094).
Hemodynamic and electrophysiologic recovery from amitriptyline intoxication
At the end of the amitriptyline infusion, MAP had nearly halved from baseline in both groups and subsequently recovered at a similar rate in both groups (Figure 13). The median heart rate remained constant throughout the experiment in both groups. The median C.O.
Tox 5 10 20 30 45 601
10
Time (min)
Plas
ma
amitr
ipty
line
conc
entr
atio
n (m
g/l) Lipid (Total)
Control (Total)Lipid (Unentrapped)
* *
Lipid (n)Control (n)
1010
9
*
Lipid/Ringer infusion
7 6 59 8
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 56 –
was also halved from baseline at the end of the amitriptyline infusion. Only two pigs in the Lipid group recovered baseline C.O. while five of the Control pigs achieved baseline C.O. during the experiment.
All of the pigs had various forms of cardiac arrhythmia (e.g. atrioventricular conduction block, ventricular extrasystoles, junctional beats and ventricular tachycardia) including ventricular fibrillation or asystole. There was no difference between groups in the incidence of arrhythmias.
All pigs survived the initial amitriptyline infusion. After the start of the treatment infusion, a total of five pigs in the Lipid group and two pigs in the Control group went into cardiac arrest and could not be resuscitated. The first cardiac arrests occurred 3 min. after the end of the amitriptyline infusion, but the last cardiac arrest 30 min. after the start of the treatment infusion.
Figure 13. Median mean arterial pressure during treatment and recovery after amitriptyline intoxication. Error bars show 25th-75th percentile.
STUDY IV
The aim of this study was to determine what effect lipid emulsion infusion according to the currently recommended protocol, has on the distribution pharmacokinetics of intravenously infused bupivacaine, as well as to record possible adverse effects associated with lipid emulsion infusion in healthy human volunteers.
Tox 5 10 20 30 45 600
20
40
60
80
100
Time (min)
Mea
n A
rter
ial P
ress
ure
(mm
Hg)
LipidControl
Lipid (n)Control (n)
1010
9
Lipid/Ringer infusion
6 59 8
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 57 –
Pharmacokinetics and entrapment of bupivacaine
After intravenous infusion of 0.5 mg/kg of bupivacaine in 20 minutes, the mean total plasma bupivacaine concentration was 610 (median 602, SD 137, range 447-857) µg/l before lipid emulsion infusion and 590 (median 616, SD 117, range 412-722) µg/l before Ringer infusion. The context-sensitive half-life of the total plasma bupivacaine concentration was shorter (P = 0.01) during lipid emulsion infusion (25 min, 95%CI 20-33 min) than during Ringer infusion (45 min 95%CI 32-76 min), (Figure 14). Accordingly, the mean total plasma bupivacaine at 20 and 30 minutes after the start of the treatment infusion were lower (P < 0.02) during lipid emulsion infusion (20 min mean 318 µg/l, median 308 µg/l, SD 30 µg/l, range 292-386 µg/l and 30 min mean 283 µg/l, median 280 µg/l, SD 33 µg/l, range 244-325 µg/l) than during Ringer infusion (20 min mean 429 µg/l, median 430 µg/l, SD 81 µg/l, range 293-553 µg/l and 30 min mean 358 µg/l, median 356, SD 73 µg/l, range 263-449 µg/l).
Figure 14. Plasma bupivacaine concentrations. * = Lipid (Total) vs. Ringer (Total) bupivacaine concentration P < 0.05. Error bars show standard deviation.
There were no differences in either mean free plasma bupivacaine concentrations or context-sensitive half-life of free plasma bupivacaine concentrations between lipid emulsion and Ringer infusions. The mean free bupivacaine concentration was 21 µg/l (median 21 µg/l, SD 5 µg/l, range 14-28 µg/l) before lipid emulsion infusion and 20 µg/l (median 20 µg/l, SD 4 µg/l, range 13-26 µg/l) before Ringer infusion. The context-sensitive half-life of free bupivacaine was 44 minutes (95%CI 28-97 minutes) during lipid emulsion infusion and 50 minutes (95%CI 32-116 minutes) during Ringer infusion. There was no difference in mean unentrapped and total plasma bupivacaine concentration at any point during lipid emulsion infusion.
Tox 5 10 20 30
10
100
1000
Time (min)
Plas
ma
bupi
vaca
ine
conc
entr
atio
n (µ
g/l)
Lipid (Total)
Ringer (Total)Lipid (Unentrapped)
**
Total & Unentrapped
Free
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 58 –
Adverse effects of lipid emulsion infusion
The non-toxic dose of bupivacaine had no effect on either blood pressure or heart rate, and no other signs of bupivacaine toxicity were detected during or after the experiment. All test subjects reported experiencing a soy-like taste during the lipid emulsion infusion. One subject had increased saliva secretion for approximately 24 hours after lipid emulsion infusion. The increased secretion commenced 2-3 hours after the experiment, and the saliva secreted was fatty and foamy.
STUDY V
The objective of the study was to determine whether the 80/20 mol% 1-palmitoyl-2-oleyl-sn-glycero-3-phosphocholine (POPC) and 1-palmitoyl-2-oleyl-sn-glycero-3-[phospho-rac-(1-glycerol)] (POPG) lipid dispersion would entrap bupivacaine to a greater degree than a commercial lipid emulsion (Intralipid®) in vivo. Prior studies in vitro showed a much stronger interaction between the POPC/POPG dispersion and bupivacaine than between the commercial lipid emulsion and bupivacaine.
Up-scaling the production of the POPC/POPG dispersion and verifying its entrapment efficiency compared to Intralipid®
In previous in vitro studies, the POPC/POPG dispersion had been produced by extrusion. Since the concentration and volume of dispersion required for a single experiment in the current study exceeded what is feasible to produce by extrusion, other methods (i.e. crude creation of multilamellar vesicles by hydration with shaking, or further processing by sonication or filtration) more suitable for producing the required dispersion were tested.
The POPC/POPG dispersions prepared by different methods were compared to the commercial lipid emulsion in a PF-EKC measurement of electrophoretic mobility of bupivacaine to ensure that the superior entrapment efficiency remained. The crude multilamellar and sonicated POPC/POPG dispersions had a superior entrapment efficiency to the commercial lipid emulsion, while the filtered dispersion had a similar entrapment efficiency to the commercial lipid emulsion. Since the crude multilamellar vesicle POPC/POPG dispersion had the best entrapment efficiency, this method was selected for the preparation of dispersion for the in vivo experiments.
Toxicity of the POPC/POPG dispersion
Even though all researchers were blinded to which lipid emulsion was infused, after ten experiments, of the twenty experiment series, had been performed there was a strong suspicion that the multilamellar POPC/POPG dispersion was toxic. Some of the pigs
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 59 –
went into cardiac arrest rapidly after the start of the lipid emulsion infusion, in a pattern contrary to that previously experienced in study II. The blinding was broken, and it was discovered that all three pigs infused multilamellar POPC/POPG dispersion had died, while only one of seven pigs infused Intralipid® had required resuscitation (P = 0.03).
To verify the toxicity of the multilamellar POPC/POPG dispersion, an anaesthetized pig was infused the same dose of POPC/POPG dispersion as the pigs in the study. Within five minutes of the start of the infusion, the pig’s MAP had risen from 75 mmHg to 147 mmHg, mean pulmonary artery pressure from 15 to 34 mm Hg, and PCWP from 12 to 35 mmHg. At the same time, SpO2 dropped from 97% to 84%, indicating disturbance of oxygenation. The pig survived until the end of the experiment after 30 minutes of POPC/POPG dispersion infusion. At the end, MAP had returned to baseline, but oxygenation did not improve. A similar test was performed using the commercial lipid emulsion. During this test, only a modest increase in MAP was observed, but no other hemodynamic effects occurred.
Reduction of the toxicity of POPC/POPG dispersion
Since lipid vesicles of high polydispersity and bigger size increase the risk of toxicity (Szebeni et al. 2000), the sonication procedure was refined in order to produce a POPC/POPG dispersion of lesser toxicity. The polydispersity index and particle sizes were measured using asymmetrical flow fractionation and dynamic light scattering, and it was concluded that sonication for 60 minutes after lipid film hydration produced optimal vesicles for our purposes. The resulting particle size in the sonicated POPC/POPG dispersion was smaller than in the commercial lipid emulsion (91 nm vs. 303 ± 15.6 nm). The sonicated POPC/POPG dispersion was tried in a pilot experiment, and after concluding that no severe hemodynamic adverse effects occurred, it was decided to proceed with a new randomized and blinded series.
Comparison of the in vivo entrapment efficiency of sonicated POPC/POPG dispersion and Intralipid®
At the Toxic Point, just before initiation of the lipid emulsion infusion, the mean plasma bupivacaine concentration was similar in both groups, 23.4 mg/l (median 24.3 mg/l, SD 3.9 mg/l, range 16.9-29.4 mg/l) in the POPC/POPG group, and 22.1 mg/l (median 22.3 mg/l, SD 2.3 mg/l, range 16.9-29.4 mg/l) in the Intralipid® group, P = 0.382). The mean plasma bupivacaine concentrations remained similar for the duration of the experiment (Figure 15A), ending at 8.2 mg/l (median 7.8 mg/l, SD 1.5 mg/l, range 6.6-11.4 mg/l) in the POPC/POPG group and 7.8 mg/l (median 7.0 mg/l, SD 1.8 mg/l, range 5.3-10.8 mg/l) in the Intralipid® group (P = 0.591) after 30 minutes of lipid emulsion infusion. A two-phase model of decay fit the data best (R2 = 0.869) and was used to estimate the context-sensitive half-life of the plasma bupivacaine concentration in the groups. The fast
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 60 –
and slow phase half-lives were 1.5 and 131 minutes for POPC/POPG and 1.3 and 78 minutes for Intralipid®, with no significant difference between groups (P = 0.932).
The mean concentration of free plasma bupivacaine measured five minutes after the start of lipid emulsion infusion was 1.2 mg/l (median 1.0 mg/l, SD 0.4 mg/l, range 0.8-2.0 mg/l) in the POPC/POPG group and 0.9 mg/l (median 0.9 mg/l, SD 0.4 mg/l, range 0.5-1.4 mg/l) in the Intralipid® group (P = 0.199).
Figure 15. A. Plasma bupivacaine concentration. B. Heart rate. C. Mean arterial pressure. D. Cardiac Output. Error bars show SD (unidirectional for clarity). B-D only includes data from pigs that were not injected adrenaline due to severe hypotension.
Tox 5 10 20 301
10
100
Time (min)
Plas
ma
bupi
vaca
ine
conc
entr
atio
n (m
g/l)
POPC/POPGIntralipid®
A
Tox 5 10 20 300
50
100
150
Time (min)
Hea
rt r
ate
(bpm
)
POPC/POPGIntralipid®
C
Tox 5 10 20 3050
75
100
125
150
Time (min)
Hea
rt r
ate
(bpm
)
POPC/POPGIntralipid®
B
Tox 5 10 20 300
1
2
3
4
5
Time (min)
Car
diac
Out
put
(l/m
in)
POPC/POPGIntralipid®
D
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 61 –
Hemodynamic effect of POPC/POPG dispersion compared to Intralipid®
Seven pigs out of ten in the POPC/POPG group and five pigs out of ten in the Intralipid® group were injected epinephrine during the lipid emulsion infusion due to severe hypotension (P = 0.65). These pigs were excluded from the analysis of haemodynamics because of the confounding effect of epinephrine. In the remaining pigs, hemodynamic recovery (Figure 15B-D) from bupivacaine intoxication occurred at a similar rate as indicated by heart rate (P = 0.6), MAP (P = 0.89), and cardiac output (P = 0.72).
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 62 –
DISCUSSION
MAIN FINDINGS
Intravenous lipid emulsion did not entrap all drugs studied here to the same degree, in the pig model. Amiodarone was entrapped to a high degree, resulting in attenuation of its hypotensive adverse effect (Study I). Amitriptyline was entrapped to some degree for the duration of the lipid emulsion infusion, but this possibly had a deleterious effect on survival (Study III). Most surprisingly, intravenous lipid emulsion did not entrap bupivacaine, the most lipophilic of clinically used local anaesthetics, to any significant degree, and mepivacaine even less (Study II). A similar result of no significant entrapment of bupivacaine was found in study IV on human volunteers, but in this study, intravenous lipid emulsion shortened the context-sensitive half-life of the plasma bupivacaine concentration significantly.
A beneficial effect of lipid emulsion infusion was only observed in study I, as the hypotensive adverse effect of a high dose of amiodarone was attenuated by concurrent lipid emulsion infusion. This study differs from the other studies in that the treatment infusion was begun before amiodarone administration. Pre-treatment may have enhanced entrapment, since an expanded lipid phase was already present in the circulation. Since the amiodarone preparation used contains the solvents polysorbate 80 and benzyl alcohol, which independently cause hypotension, it is also possible that the hypotensive effect attenuated by intravenous lipid emulsion was not caused by amiodarone alone, but also by one or both of these solvents. In study II, III, and V, in which the lipid emulsion was infused only after intoxication, no enhanced recovery occurred.
Despite a clear advantage in interaction (entrapment potential) measured in vitro, the experimental POPC/POPG dispersion failed to perform better than a commercial lipid emulsion in a pig model of bupivacaine intoxication (Study V). Neither entrapment of bupivacaine in plasma nor recovery from bupivacaine intoxication was enhanced by POPC/POPG dispersion compared to Intralipid®.
EXPERIMENTAL MODEL VS. CLINICAL SITUATION
The typical clinical situation in the published case reports has been refractory cardiac arrest with continuing CPR. In studies II and V, the end-point for the local anaesthetic infusion was set at 50% baseline MAP, because pilot experiments indicated that no pigs survived if the infusion was allowed to continue until asystole. Even with this precaution, some pigs died during the resuscitative phase of the experiment.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 63 –
Although the doses and infusion rates of local anaesthetics used in studies II and V led to severe intoxication within less than 10 minutes, this does not exactly mimic the common reason for an intoxication in human patients, i.e., rapid intravascular injection. The possibility that lipid emulsion would affect local anaesthetic pharmacokinetics and toxicity differently after a rapid intravascular injection cannot be excluded.
In study III, amitriptyline was administered intravenously, but in clinical intoxications, it has usually been taken orally. In that case, the amitriptyline in the gut would continue to be absorbed as long as there remained drug in the gut, often for hours after hospital admission. A patient can be admitted to hospital at any time after ingesting toxic agents, however, making modelling the entire spectrum of possible clinical scenarios difficult. In study III, intravenous amitriptyline (15 mg ⁄ kg) led to plasma concentrations comparable to those in published intoxication cases (Baselt et al. 1975; Huge et al. 2011). The intravenous amitriptyline infusion was discontinued after the set dose (15 mg/kg), and the lipid emulsion infusion started, to allow more exact measurements of the entrapment of amitriptyline by intravenous lipid emulsion without continuous and unpredictable enteral absorption confounding the interpretation. In acute intoxications, during the gastrointestinal absorption of amitriptyline, intravenous lipid emulsion could bind amitriptyline in plasma and increase its total plasma concentration. In most clinical situations, the intoxication potentially occurs several hours before any treatment can be administered. In the case reports previously mentioned (Engels & Davidow 2010; Huge et al. 2011), lipid emulsion was only administered after all other treatment options had been tried. Theoretically, intravenous lipid emulsion, administered during the post-absorption phase, could entrap some amitriptyline from tissues. Due to the high volume of distribution of amitriptyline, however, even a twofold increase in total plasma amitriptyline concentration signifies an entrapment of only roughly 1% or less of all the amitriptyline distributed into tissues and might even mean an increase in plasma concentration to cardiotoxic levels.
Because of ethical considerations, the pigs were anaesthetized for the duration of the experiment. The induction agent ketamine used in studies I-III is known to stimulate the circulation (Sinner & Graf 2008), while the maintenance agent isoflurane, used in studies I-III and V, causes cardiac depression (Eger 1981). Because ketamine was only administered for the induction of anaesthesia, we expect that its effect during the experiment was minimal. The isoflurane concentration was kept at a standardized low level for the maintenance of unconsciousness of the animal, but isoflurane probably depressed the circulation to some extent. Because all pigs in each study were anaesthetized according to the same protocol, comparison of treatment groups can be considered valid. General anaesthesia has been shown to have a significant protective effect on both the pharmacokinetics and pharmacodynamics of local anaesthetics, however. In awake sheep, CNS toxicity stimulated the heart causing malignant arrhythmias; general anaesthesia prevented this effect while instead exacerbating cardiovascular depression (Copeland, Ladd, Gu & Mather 2008a). General anaesthesia also doubled the blood concentration of local anaesthetics in sheep by
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 64 –
reducing the apparent volume of distribution, which also reduced the elimination half-life (Copeland, Ladd, Gu & Mather 2008b).
In clinical severe intoxication, the disturbance of circulation and respiration rapidly leads to acidosis. The blood pH affects the dissociation of weak bases (e.g. bupivacaine, mepivacaine, and amitriptyline) and acids (e.g. amiodarone). In acidotic conditions (pH < 7.35), weak bases are ionized to a higher degree, decreasing their lipid solubility and capacity to pass through lipid bilayers. The reverse is true for weak acids. In the case of local anaesthetics, a reduction in pH reduces the local anaesthetics’ affinity for alpha-1-acid glycoprotein, increasing the free concentration of local anaesthetic during acidosis (Denson et al. 1984). Prompt treatment of acidosis is central to the treatment of both local anaesthetic (Weinberg 2010) and amitriptyline intoxication (Blackman et al. 2001). However, in the case of local anaesthetics, it has been suggested that the influence of pH on free concentrations is not clinically significant at toxic concentrations (Denson et al. 1984), and in the case of amitriptyline intoxication, the precise mechanism by which increasing pH ameliorates toxicity is unclear (Blackman et al. 2001). The pigs studied in this thesis were anaesthetized under controlled ventilation, and did not develop acidosis as verified by arterial blood gas sampling. The lack of acidosis clearly differs from clinically encountered severe intoxications, and may have influenced the outcome of the studies. A pig study with concomitant hypoventilation and bupivacaine toxicity has found, however, that lipid emulsion led to inferior resuscitation results compared to adrenaline and vasopressin (Mayr et al. 2008). The bupivacaine concentrations measured in the study also show similarly small differences between groups as seen in study II of this thesis.
Since study IV involved human subjects, a non-toxic dose of bupivacaine was used. This meant that there were no convulsions, ECG changes, or circulatory collapse, which would affect, for instance, plasma pH or tissue perfusion. This also meant that the pharmacokinetic findings could not be correlated with any pharmacodynamic effects. At the low concentrations encountered in the study, bupivacaine is bound up to 98% to plasma proteins. At the toxic concentrations in studies II and V, as well as in clinically encountered intoxications, bupivacaine is protein bound to a lesser degree (Denson et al. 1984). This reduction in protein binding increases toxicity, but might also increase entrapment in lipid emulsion. However, in study V, no sign of the possible increased entrapment occurred, and bupivacaine was approximately 90% protein bound at a total plasma concentration of 10 mg/l.
LIPID SOLUBILITY REQUIREMENT FOR ENTRAPMENT
The results of these studies indicate that the lipid solubility of a drug has to be very high for it to be significantly sequestered by intravenous lipid emulsion. Amiodarone, which was highly sequestered in study I, has a octanol:water partition logP of 7.24 (Tetko et al. 2001),
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 65 –
and a very large volume of distribution (approximately 60 l/kg) although it is extensively bound to plasma proteins (96% binding). Amitriptyline, which was entrapped to some degree, has a octanol:water partition logP of 5.10 (Tetko et al. 2001), has a large volume of distribution (approximately 8 l/kg), and is extensively bound to plasma proteins (96% binding). Bupivacaine and mepivacaine, which were not significantly entrapped, have a octanol:water partition logP of 3.31 for bupivacaine and 2.16 for mepivacaine (Tetko et al. 2001), and a comparatively small volume of distribution (approximately 1 l/kg). Bupivacaine is 95% bound to plasma proteins, while mepivacaine is 77% protein bound.
The study results suggest that an octanol:water partition logP above 3.31 is required for significant entrapment to occur, and an even higher logP (possibly as high as 7.24) is required for a clear clinical effect. Interestingly, most of the case reports of successful resuscitation from intoxication using intravenous lipid emulsion concern intoxications by drugs with an octanol:water partition logP in the 3-5 range (e.g. bupivacaine, amitriptyline, verapamil). However, since no entrapment was shown with the most lipid soluble local anaesthetic, bupivacaine, another mechanism than entrapment might be required to explain the observed beneficial effect of intravenous lipid emulsion in cases and animal studies of local anaesthetic intoxication. A more in depth discussion of other possible mechanisms follows later in this discussion.
LIPID SINK OR LIPID SUBWAY?
Currently, the main hypothesis for the mechanism by which intravenous lipid emulsion would revive intoxicated patients and animals is the purported “lipid sink” (Weinberg et al. 1998). According to this theory, an expanded lipid phase in plasma would entrap lipophilic drugs by establishing a concentration gradient favouring the diffusion of the free lipophilic drugs from the aqueous plasma into the lipid vesicles. It is not determined what the final fate of the drug entrapped in the lipid vesicles will be. Most favourably, the lipid vesicles would aid distribution of the drug into inert tissues such as body fat, but results suggest that the vesicles in some cases act as a transporter, aiding distribution into critical tissues such as the central nervous system (Kazemi et al. 2011).
If a “lipid sink” effect occurs, the expected findings in the plasma samples would be an increased total plasma concentration of the drug when compared to placebo. This is demonstrated in studies I and III. Another example of similar phenomenons is the increased concentration of plasma digitoxin and reversal of toxicity after injection of digitoxin-specific Fab fragments (Ochs & T. W. Smith 1977) and the reversal of neuromuscular blockade with concurrent increase of plasma rocuronium concentration after infusion of the rocuronium-specific cyclodextrin sugammadex (Epemolu et al. 2003). Direct parallels between the two previously mentioned treatments and lipid emulsion infusion cannot be drawn, since both digitoxin-specific Fabs and sugammadex bind their targets by van der
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 66 –
Waals interaction, which although weak compared to molecular covalent bonds, is still much stronger than the entrapping force exerted by a polar/nonpolar concentration gradient.
The decrease in the context-sensitive half-life of total plasma bupivacaine following intravenous lipid emulsion administration that occurred in study V may support a pharmacokinetic distribution-enhancing mechanism of action in the treatment of local anaesthetic intoxication. However, there was no significant reduction in the free bupivacaine plasma concentration during lipid emulsion infusion compared with that seen during Ringer infusion. There also was no significant difference between unentrapped and total plasma concentrations of bupivacaine during lipid emulsion infusion, implying that the hypothesized ‘lipid sink’ had little or no effect on the plasma disposition of the non-toxic concentration of bupivacaine in the study. This is corroborated by the finding in study II that intravenous lipid emulsion has little or no influence on the plasma disposition of toxic levels of bupivacaine or mepivacaine. Other similar pharmacokinetic drug interactions also usually do not affect the free drug concentration except transiently (Rang, Dale & Ritter 1999b). Increased distribution could possibly even be deleterious, if the increased distribution reaches critical tissues.
Although a “lipid sink” effect was observed in study III, there were more cardiac arrests and deaths following amitriptyline intoxication in the lipid emulsion group than in the Ringer group. This suggests that intravenous lipid emulsion might not improve survival in this scenario, and calls into doubt whether the “lipid sink” caused the beneficial effects previously reported (Jamaty et al. 2010; Huge et al. 2011). In a study using rabbits (Kazemi et al. 2011), lipid emulsion actually increased the depth of anaesthesia when infused immediately after the lipophilic barbiturate thiopental (octanol:water distribution logP 3.05 (Tetko et al. 2001)). Kazemi’s finding suggests that in some situations, intravenous lipid emulsion can function as a “lipid subway”, transporting drug into critical tissues instead of as a “lipid sink” into which toxic concentrations of drug can be made to “disappear”. In study III, it is possible that the infusion of lipid emulsion and resulting entrapment that leads to a higher circulating concentration of amitriptyline perfusing the heart and other highly perfused tissues, leads to more binding of amitriptyline to receptors and increased toxicity because the entrapment in lipid vesicles is easily reversible compared to the receptor affinity of amitriptyline.
ANIMAL MODELS
A review of animal models concluded that no model can be sure to mimic the precise situation of a human local anaesthetic intoxication (Groban 2003). For studies I-III and V, the pig was chosen as a model because it is considered a good model for toxicological studies due to its human-like physiology (Swindle et al. 2011). Although the microsomal metabolism of the studied drugs most likely was not relevant due to the short time-frame
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 67 –
of the experiments, the similarity of porcine liver microsomal enzymes to human also benefits toxicological studies (Achour et al. 2011).
An additional argument for choosing the pig was that a model of local anaesthetic intoxication had been developed and used in the same laboratory for studies on the use of amrinone (Lindgren et al. 1992) or levosimendan (Aittomäki et al. 2010) as a treatment for local anaesthetic intoxication. Due to its size, a 20-30 kg pig can be cannulated with equipment intended for human use, and a normal anaesthesia ventilator with evaporator can be used.
Despite these observations, the contradictory results from the different animal models suggest that there is a significant difference between species in the efficacy of the lipid treatment. Studies in rodents and dogs show much more encouraging results than those performed in pigs. In agreement with the findings in study II, two studies on bupivacaine intoxication performed on pigs also found no beneficial effect of lipid emulsion when compared with vasopressors (Mayr et al. 2008; Hicks et al. 2009), whereas using rats (Di Gregorio et al. 2009) or dogs (Weinberg et al. 2003), lipid emulsion was superior to vasopressin and saline, respectively. In rabbits, lipid emulsion outperformed the currently considered best treatment, sodium bicarbonate, when administered in a model of chlomipramine (a tricyclic antidepressant) toxicity (Harvey & Cave 2007). In comparison, in the pig model of amitriptyline (also a tricyclic antidepressant) intoxication used in study III, even when compared to placebo, lipid emulsion failed to improve survival or recovery. Lipid emulsion was not superior, however, compared to insulin in a rabbit model of severe propranolol toxicity (Harvey, Cave, Lahner, Desmet, Prince & Hopgood 2011b).
Recently, the failure of pig models to produce results favouring lipid emulsion has been attributed to the observation that pigs exhibit a complement activation related pseudoallergy (CARPA) to certain liposomes (Szebeni 2005), and it has been suggested that pigs would not be suitable for intravenous lipid emulsion studies (Weinberg & Rubinstein 2011). Since 5-7% of humans exhibit the same possibly severe reaction (Szebeni et al. 2007), it would seem unwise to disregard a model which also accounts for this potentially severe side-effect of what is intended as an antidote for a life-threatening intoxication. It should also be considered that not all liposomes cause the reaction, and whether the currently recommended parenteral nutrition lipid emulsion does is unknown (Szebeni et al. 2011; Weinberg & Rubinstein 2011). In addition, although a pseudoallergic reaction could prevent haemodynamic recovery, CARPA has not been shown to affect entrapment.
When considering the evidence for and against intravenous lipid emulsion, one should take into account that no single animal model sufficiently reflects human physiology. Thus, regulatory bodies require proof of efficacy and safety from several species before authorizing human trials of new compounds (European Medicines Agency 2009). Currently, only rodents show a uniformly positive response to lipid emulsion, while non-rodents provide contradictory results (Jamaty et al. 2010).
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 68 –
OTHER MECHANISMS FOR THE THERAPEUTIC EFFECT OF INTRAVENOUS LIPID EMULSION IN LOCAL ANAESTHETIC-INDUCED MYOCARDIAL DEPRESSION
One possible explanation for the increase in blood pressure occurring with rapid lipid emulsion infusion would be a direct volume effect (Zausig, Graf & Zink 2009a). However, in rats that were in cardiac arrest after a 20 mg/kg IV bolus of bupivacaine, the same volume of saline solution led to ROSC in only one of five animals, compared to ROSC in all animals treated with lipid emulsion with or without a moderate dose of epinephrine (Hiller et al. 2009). This suggests that other factors than fluid resuscitation cause the increase in survival shown in the studies.
The rapidly infused lipid emulsion could provide its therapeutic effect through other mechanisms than sequestration, including a theorized reversal of bupivacaine-induced inhibition of acylcarnitine-translocase-mediated lipid substrate oxidation in cardiac mitochondria (Weinberg et al. 2000). Whether raising the amount of lipid substrate actually overcomes the inhibition of the translocase has not been shown, however. A strong direct myocardial effect of the lipid emulsion was not evident in our studies, because MAP, heart rate, and ECG variables returned to baseline at a similar rate in all treatment groups.
It has also been suggested that fatty acids may exhibit a direct positive effect on myocardial voltage-dependent calcium channels in the setting of intoxication (Pennec et al. 2010). This suggestion follows on the discovery that long-chain fatty acids activate ventricular myocyte calcium channels (Huang et al. 1992). The phosphodiesterase III inhibitor amrinone, which increases Ca2+-influx into cardiac myocytes, has been shown to significantly improve recovery from bupivacaine intoxication in pigs (Lindgren et al. 1992). This effect could be hypothesized to be of particular importance in the setting of calcium channel blocker intoxication. However, the very potent calcium sensitizing inotrope levosimendan did not enhance recovery from bupivacaine-induced cardiovascular depression in pigs (Aittomäki et al. 2010).
INTRAVENOUS LIPID EMULSION FOR CNS OR CARDIAC TOXICITY OF LOCAL ANAESTHETICS
There is still disagreement on whether lipid emulsion should be reserved for cases of severe cardiac toxicity, or whether it should be administered as soon as any symptoms of local anaesthetic intoxication are detected (Weinberg 2010; Cave et al. 2010; Neal et al. 2010). Animal studies on lipid therapy have been limited to the more severe forms of cardiac toxicity. Of the case reports, only six of the 28 reports use in the setting of CNS intoxication. Of these, five cases resolved after lipid emulsion infusion, but in one of the cases seizures continued and thiopental was administered (Calenda & Dinescu 2009). Since the plasma
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 69 –
concentration threshold for CNS toxicity to develop is much lower than for cardiac toxicity, and local anaesthetics are rapidly distributed into tissues after intravascular injection, it is conceivable that in the case of isolated CNS toxicity the patients recovery was merely due to the distribution which lowered the circulating bupivacaine concentration, and not due to lipid emulsion. In addition, the proposed alternative mechanisms of lipid therapy for cardiac toxicity are irrelevant for CNS toxicity. Thus, since there is lack of proof of both efficacy and even mechanism for lipid emulsion reversal of CNS toxicity, it seems prudent to only consider its use when developing cardiac toxicity is evident.
POSSIBLE ADVERSE EFFECTS OF THE INTRAVENOUS LIPID EMULSION TREATMENT FOR SEVERE INTOXICATION
In study IV, the volunteers reported no severe adverse effects of the lipid emulsion. Less severe side effects may have been forgotten by subjects that were infused lipid emulsion in the first experiment session in the time passing before the interview at the end of the second experiment session.
When used as parenteral nutrition, lipid emulsions are associated with cases of pancreatitis due to triglyceridemia caused by administration at a rate that supercedes the elimination rate (Mirtallo et al. 2010). Intravenous lipid emulsion can also reduce the diffusion capacity of the lungs (Greene et al. 1976), which may be of special significance in critically ill patients. Fatty acids activate coagulation factors and cause platelet aggregation (Hoak et al. 1967), leading to potentially lethal thrombosis (Connor et al. 1963). The previously mentioned CARPA reaction may also cause circulatory collapse in its more severe forms (Szebeni et al. 2000). These severe adverse effects would almost certainly not be detected in single cases of lipid emulsion use, since they would be almost impossible to distinguish from non-responsiveness to resuscitation. This leads to the dangerous situation where any successful resuscitation during which lipid emulsion has been employed is attributed to the use of the treatment, while any deaths caused by adverse effects are lost in the background of expected unresponsiveness to all treatments.
LIMITATIONS OF THE STUDIES
In study I, all blood samples were drawn during the concomitant amiodarone and lipid (or Ringer) infusions. Because of this, the highest measured concentration occurs at the final sampling point. In retrospect, a series of blood samples taken at time points after the end of the infusions, as in study III, would have provided interesting data on the continuing effect of lipid emulsion on the distribution of amiodarone.
Study IV included only eight subjects. This was remediated by using a crossover experimental
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 70 –
protocol, which increases power to a comparable level to the other studies in this thesis. The studies were designed to detect a difference in total plasma concentrations of approximately 20%, which would likely be a large enough effect to explain the rapid recovery of the patients in the case reports. However, smaller effects would not be reliably detected, and the studies were not powered to detect the much smaller changes in free plasma concentrations that might be sufficient for survival from severe intoxication. In study IV, the free bupivacaine concentration decreased more rapidly during the first five minutes of the lipid infusion than during Ringer infusion, but the free bupivacaine concentration at five minutes did not differ significantly between infusions. Using a larger number of subjects, this difference could become statistically significant. A rapid decrease in free bupivacaine concentration, within five minutes of the start of the lipid infusion, could be clinically important in the setting of an acute and severe intoxication.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 71 –
CONCLUSIONS
The aim of the study was to examine whether intravenously infused lipid emulsion would entrap lipophilic drugs to a clinically significant extent. The results show, in these models, that this may not be the case.
In pigs, amiodarone was highly entrapped by intravenous lipid emulsion: the median concentration in the control group was 78% lower than in the lipid group at the end of the experiment. Amitriptyline was clearly entrapped, with a 47% lower concentration in the control pigs. In contrast, the local anaesthetic bupivacaine was only slightly entrapped, with a 16% lower concentration in the control group, and the local anaesthetic mepivacaine was not entrapped at all. In human volunteers at non-toxic concentrations, lipid emulsion accelerated the distribution of bupivacaine. These results indicate that a drug must be highly lipophilic in order for significant entrapment to occur.
Although amitriptyline was entrapped to some degree, no enhancement of recovery from intoxication occurred. The local anaesthetics studied, especially mepivacaine, were not entrapped to any significant degree, and no enhancement of recovery from intoxication occurred.
Pre-treatment using lipid emulsion entrapped amiodarone significantly, and prevented the hypotensive effect associated with infusion of a toxic dose of amiodarone.
Although in vitro lipid-drug interaction studies showed the POPC/POPG lipid dispersion to have superior entrapment potential for bupivacaine, this effect could not be repeated in vivo.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 72 –
IMPLICATIONS FOR FUTURE STUDIES
Despite the increasing research efforts of the past years and the numerous case reports published, many issues concerning the use of lipid emulsion for the treatment of acute intoxications remain. This thesis attempted to answer some of these questions, but the results raise further interesting questions that require further study.
Whether intravenous lipid emulsion is efficacious for the treatment of acute intoxications by lipophilic drugs, especially the local anaesthetics for which it is currently recommended, remains unclear. The results presented in this thesis call into doubt whether lipid emulsion has any effect on the disposition of local anaesthetics in plasma, and thus undermine the currently proposed “lipid sink” mechanism of lipid therapy. If entrapment turns out to be a mechanistic “red herring”, the basis for deciding what intoxications, if any, should be treated using lipid emulsion needs to be re-evaluated.
Local anaesthetics at high concentrations are known to inhibit cardiac energy metabolism. Future studies should address whether this phenomenon is relevant at clinically encountered concentrations, and whether lipid emulsion can reverse the inhibition.
The currently recommended lipid emulsion dose is only based on similar use in animal studies. If the therapy is to be adopted, dose-dependence studies are required to determine the optimal dosage.
Randomized, controlled prospective human volunteer studies of lipid therapy in the setting of severe intoxication are difficult if not impossible to arrange. We lack a safety profile of lipid emulsion at the currently recommended rapidly administered high dose. Since no serious adverse effects are currently known, it would be both ethical and most accurate to perform this study using human subjects.
In the setting of emergency medicine, a possibly multicentre study of patients suffering from severe intoxication suspected to be caused by lipophilic drugs could yield a sufficient number of treatments for a prospective, controlled, and randomized study of lipid therapy to be performed.
Species differences in susceptibility to the toxicity of drugs as well as response to intravenous lipid emulsion remain a problem. Studies in rodents generally favour lipid therapy, but studies in larger mammals, especially pigs, show little or no positive effect of lipid emulsion compared to traditional treatments. A consensus on what animal model best reflects the human response to intoxication and lipid therapy needs to be established.
In vitro studies have been used to demonstrate the entrapment potential of lipid emulsion.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 73 –
As study V shows, due to the complicated nature of interactions in the whole organism, in vitro effects are not always repeatable in vivo. Great care should be exercised in inferring clinical significance from test tube projects.
Intravenous lipid emulsion therapy for severe intoxication remains an interesting possibility. Active research into the efficacy and mechanisms of the therapy will continue.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 74 –
ACKNOWLEDGEMENTS
This work was performed at the departments of Anaesthesiology and Intensive Care and Clinical Pharmacology at Helsinki University Central Hospital and the University of Helsinki between 2009 and 2012.
The work has been financially supported by the Helsinki University Hospital Research Fund, the Liv och Hälsa Foundation, Finska Läkaresällskapet, and Stiftelsen Dorothea Olivia, Karl Walter och Jarl Walter Perkléns Minne.
I am deeply grateful to my supervisor, Professor Per H. Rosenberg. It has been a privilege to work closely with you during the entire project. Your expertise in the field of anaesthesia, especially local anaesthetics, never ceases to amaze me. I value the time you have taken both to conduct experiments and discuss the work with me most highly.
I extend my gratitude to Professor Janne Backman for acting as custos at the dissertation.
For their support and counsel, I thank my thesis committee members Professor emeritus Pertti Neuvonen and Jouni Kurola. Professor Neuvonen and his lab measured the drug concentrations in all of the studies. In addition, Professor Neuvonen participated tirelessly in the preparation of the publications, sharing his knowledge and ensuring the work held to the best standard. Jouni Kurola is an inspiration in the field of prehospital medicine, and I enjoyed discussing this work with him greatly.
I also thank Professors Hannu Kokki and Kalle Hoppu, who kindly agreed to review this thesis, accommodating the slightly strained schedule this spring. To be able to draw upon the knowledge of the best experts in the field to improve one’s work is a privilege, and I am grateful.
Jennifer Rowland corrected my English and taught me the secrets of correct punctuation, while Kristina Stening did the graphical design of the thesis, making it a pleasure for the eyes. Beatrice Silén, in addition to being my favourite aunt, corrected my Swedish, which I regret to admit lacks finesse in scientific circumstances. My lovely friend and colleague Elina Jokinen kindly corrected my Finnish grammar. I am grateful to all of you for helping me make my thesis as appealing as possible for its likely quite small readership.
My sincere gratitude goes to my collaborators and co-authors. Tomohisa Niiya tirelessly worked on all aspects of the studies, sometimes spending late nights on some problem in order to dazzle us with his results in the morning. Susanne Wiedmer, Jana Lokajova, Juha Holopainen, and Gebrenegus Yohannes introduced the exciting idea of a liposome specifically prepared for the purpose of entrapment, which led to the fruitful collaboration
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 75 –
in this thesis. Markku Paloheimo generously provided equipment, and was an inspiring teacher when I began my residency rotations at the HUCH Eye and Ear Hospital. Pekka Tarkkila contributed to all stages of the volunteer study. Liisa Petäjä kindly found time in her busy schedule to perform cardiac ultrasounds when requested. Juho Heinonen made significant contributions to many parts of the work, and will find success in whichever field of medicine he chooses to apply himself to (hopefully this will be anaesthesiology!).
For their diligent work in determining the drug concentrations in the plasma samples, I thank Jouko Laitila and Eija Mäkinen-Pulli. For his assistance in understanding the statistical analysis of the results, I thank Janne Pitkäniemi. For their technical assistance and excellent ideas for the practical performance of the human study, I thank nurses Sari Pyhälä, Johanna Merenlahti, Saija Pihlamaa, and Markus Sjögren. For their technical assistance in the studies, I thank Veikko Huusko and Olli Valtanen.
I am grateful to the volunteers who participated in the study for your valuable and selfless contribution to this project. We should also not forget the pigs, of which the ultimate sacrifice for science was required.
I thank the chief physicians of the hospitals where I’ve worked during the project for their flexibility in providing me the opportunity to use some of my work hours for research. My co-workers, who were then required to pick up the slack, deserve my deepest gratitude for making this possible.
My friends deserve thanks for enduring and encouraging my work. Fellow young scientists Benjamin, Daniel, Eppu and Verneri all share my excitement for discovery. Fun times were had with Klaus, whose sense of humour is always a source of laughter (always remember to pack your bags!). For relaxation, nothing is better than a weekend spent with captain Jonas and family.
For their loving support, I thank my family. My mother’s exacting standards have pushed me to aim for excellence in all my endeavours. As far back as I can remember, my father has always been inventing something. I hope some of his spirit of discovery has rubbed off on me. My brother Henrik; thank you for all the fun we have had and will have together. A special thanks also goes out to my in-laws Iris and Antti.
Finally, I wish to thank my wife Anna, without whose love and support this work would not have been possible. You have endured endless discussion of my work, celebrated my successes, and consoled me at times of despair. I love you.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 76 –
REFERENCES
Achour, B., Barber, J. & Rostami-Hodjegan, A., 2011. Cytochrome P450 Pig Liver Pie: Determination of individual cytochrome P450 isoenzyme contents in microsomes from two pig livers using LC MS. Drug Metab Dispos, 39(11), pp.2130–2134.
Adriani, J., Zepernick, R. & Hyde, E., 1966. Influence of the status of the patient on systemic effects of local anesthetic agents. Anesth Analg, 45(1), pp.87–92.
Ahn, J.E., Cloyd, J.C., Brundage, R.C., Marino, S.E., Conway, J.M., Ramsay, R.E., White, J.R., Musib, L.C., Rarick, J.O., Birnbaum, A.K. & Leppik, I.E., 2008. Phenytoin half-life and clearance during maintenance therapy in adults and elderly patients with epilepsy. Neurology, 71(1), pp.38–43.
Aittomäki, J., Liuhanen, S., Sallisalmi, M., Salmenpera, M.T., Heavner, J.E. & Rosenberg, P.H., 2010. The effect of levosimendan on bupivacaine-induced severe myocardial depression in anesthetized pigs. Reg Anesth Pain Med, 35(1), pp.34–40.
Al-Duaij, N., George, M., O’Donnell, K. & Burns Ewald, M., 2012. Lipid Emulsion Therapy in Massive Imipramine Overdose. Clin Toxicol, 47(5), p.460.
Andreasen, F., Agerbaek, H., Bjerregaard, P. & Gøtzsche, H., 1981. Pharmacokinetics of amiodarone after intravenous and oral administration. Eur J Clin Pharmacol, 19(4), pp.293–299.
Anon, INCHEM, International Programme on Chemical Safety. Available at: http://www.inchem.org/ [Accessed May 9, 2012].
Aveline, C., Cognet, F. & Bonnet, F., 2010. Ineffectiveness of intralipid infusion for central nervous toxicity following ultrasound-guided sciatic nerve block with lidocaine-ropivacaine solution: interaction between carbamazepine, local anaesthetic and intralipid? Eur J Anaesthesiol, 27(12), pp.1070–1072.
B. Braun Melsungen AG, 2005. Lipofundin® MCT/LCT. pp.1–6.
Bailey, D.N. & Jatlow, P.I., 1976. Gas-chromatographic analysis for therapeutic concentrations of amitriptyline and nortriptyline in plasma, with use of a nitrogen detector. Clin Chem, 22(6), pp.777–781.
Bania, T., Chu, J., Perez, E., Su, M. & Hahn, I., 2007. Hemodynamic effects of intravenous fat emulsion in an animal model of severe verapamil toxicity resuscitated with atropine, calcium, and saline. Acad Emerg Med, 14(2), pp.105–111.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
Baselt, R., Wright, J. & Cravey, R., 1975. Therapeutic and toxic concentrations of more than 100 toxicologically significant drugs in blood, plasma, or serum: a tabulation. Clin Chem, 21(1), pp.44–62.
Bergese, S.D., Onel, E., Morren, M. & Morganroth, J., 2012. Bupivacaine extended-release liposome injection exhibits a favorable cardiac safety profile. Reg Anesth Pain Med, 37(2), pp.145–151.
Bjornaas, M.A., Teige, B., Hovda, K.E., Ekeberg, O., Heyerdahl, F. & Jacobsen, D., 2010. Fatal poisonings in Oslo: a one-year observational study. BMC Emerg Med, 10(1), pp.13–23.
Blackman, K., Brown, S.G. & Wilkes, G.J., 2001. Plasma alkalinization for tricyclic antidepressant toxicity: a systematic review. Emerg Med (Fremantle), 13(2), pp.204–210.
Body, R., Bartram, T., Azam, F. & Mackway-Jones, K., 2011. Guidelines in Emergency Medicine Network (GEMNet): guideline for the management of tricyclic antidepressant overdose. Emerg Med J, 28(4), pp.347–368.
Boegevig, S., Rothe, A., Tfelt-Hansen, J. & Hoegberg, L., 2011. Successful reversal of life threatening cardiac effect following dosulepin overdose using intravenous lipid emulsion. Clin Toxicol (Phila), 49(4), pp.337–339.
Boyd, T. & Brady, W., 2012. The “Code Drugs in Cardiac Arrest”—the use of cardioactive medications in cardiac arrest resuscitation. Am J Emerg Med, 30(5), pp.811–818.
Browne, A., Harvey, M. & Cave, G., 2010. Intravenous Lipid Emulsion Does Not Augment Blood Pressure Recovery in A Rabbit Model of Metoprolol Toxicity. J Med Toxicol, 6(4), pp.373–378.
Bushey, B.A., Auld, V.H., Volk, J.E. & Vacchiano, C.A., 2011. Combined lipid emulsion and ACLS resuscitation following bupivacaine- and hypoxia-induced cardiovascular collapse in unanesthetized swine. AANA J, 79(2), pp.129–138.
Calenda, E. & Dinescu, S.A., 2009. Failure of lipid emulsion to reverse neurotoxicity after an ultrasound-guided axillary block with ropivacaine and mepivacaine. J Anesth, 23(3), pp.472–473.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 78 –
Candela, D., Louart, G., Bousquet, P.J., Muller, L., Nguyen, M., Boyer, J.C., Peray, P.A., Goret, L., Ripart, J., Lefrant, J.Y. & La Coussaye, de, J.E., 2010. Reversal of bupivacaine-induced cardiac electrophysiologic changes by two lipid emulsions in anesthetized and mechanically ventilated piglets. Anesth Analg, 110(5), pp.1473–1479.
Carr, D., Boone, A., Hoffman, R., Martin, K. & Ahluwalia, N., 2012. Successful Resuscitation of a Carvedilol Overdose Using Intravenous Fat Emulsion (IFE). Clin Toxicol, 47(7), p.727.
Carr, D., Boone, A., Hoffman, R., Martin, K. & Ahluwalia, N., 2009. Successful Resuscitation of a Doxepin Overdose Using Intravenous Fat Emulsion (IFE). Clin Toxicol, 47(7), p.710.
Castanares-Zapatero, D., Wittebole, X., Huberlant, V., Morunglav, M. & Hantson, P., 2012. Lipid Emulsion as Rescue Therapy in Lamotrigine Overdose. J Emerg Med, 42(1), pp.48–51.
Cave, G. & Harvey, M., 2009a. Intravenous lipid emulsion as antidote beyond local anesthetic toxicity: a systematic review. Acad Emerg Med, 16(9), pp.815–824.
Cave, G. & Harvey, M., 2009b. Lipid emulsion may augment early blood pressure recovery in a rabbit model of atenolol toxicity. J Med Toxicol, 5(1), pp.50–51.
Cave, G., Harrop-Griffiths, W., Harvey, M., Meek, T., Picard, J., Short, T. & Weinberg, G., 2010. AAGBI safety guideline: management of severe local anaesthetic toxicity. Available at: http://www.aagbi.org/sites/default/files/la_toxicity_2010_0.pdf [Accessed September 11, 2011].
Cave, G., Harvey, M. & Graudins, A., 2011. Review article: Intravenous lipid emulsion as antidote: A summary of published human experience. Emerg Med Australas, 23(2), pp.123–141.
Cave, G., Harvey, M.G. & Castle, C.D., 2005. Intralipid ameliorates thiopentone induced respiratory depression in rats: investigative pilot study. Emerg Med Australas, 17(2), pp.180–181.
Cave, G., Harvey, M.G. & Castle, C.D., 2006. The role of fat emulsion therapy in a rodent model of propranolol toxicity: a preliminary study. J Med Toxicol, 2(1), pp.4–7.
Cave, G., Harvey, M.G. & Winterbottom, T., 2009. Evaluation of the Association of Anaesthetists of Great Britain and Ireland lipid infusion protocol in bupivacaine induced cardiac arrest in rabbits. Anaesthesia, 64(7), pp.732–737.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 79 –
Charbonneau, H., Marcou, T.A.P., Mazoit, J.-X., Zetlaoui, P.J. & Benhamou, D., 2009. Early use of lipid emulsion to treat incipient mepivacaine intoxication. Reg Anesth Pain Med, 34(3), pp.277–278.
Chen, Y., Xia, Y., Liu, L., Shi, T., Shi, K., Wang, Q., Chen, L., Papadimos, T.J. & Xu, X., 2010. Lipid Emulsion Reverses Bupivacaine-induced Asystole in Isolated Rat Hearts: Concentration-Response and Time-Response Relationships. Anesthesiology, 113(6), pp.1320–1325.
Cheymol, G., Woestenborghs, R., Snoeck, E., Ianucci, R., Le Moing, J.P., Naditch, L., Levron, J.C. & Poirier, J.M., 1997. Pharmacokinetic study and cardiovascular monitoring of nebivolol in normal and obese subjects. Eur J Clin Pharmacol, 51(6), pp.493–498.
Chow, M.J., Ambre, J.J., Ruo, T.I., Atkinson, A.J., Bowsher, D.J. & Fischman, M.W., 1985. Kinetics of cocaine distribution, elimination, and chronotropic effects. Clin Pharmacol Ther, 38(3), pp.318–324.
Clarkson, C.W. & Hondeghem, L.M., 1985. Mechanism for bupivacaine depression of cardiac conduction: fast block of sodium channels during the action potential with slow recovery from block during diastole. Anesthesiology, 62(4), pp.396–405.
Connor, W.E., Hoak, J. & Warner, E.D., 1963. Massive thrombosis produced by fatty acid infusion. J Clin Invest, 42(6), pp.860–866.
Cooper, G., Dyas, J., Krishna, C. & Thompson, J., 2010. Successful use of Intravenous Fat Emulsion in Severe Poisoning Following Ingestion of Lipid Soluble Drugs. Clin Toxicol, 48(3), p.298.
Copeland, S.E., Ladd, L.A., Gu, X.-Q. & Mather, L.E., 2008a. The Effects of General Anesthesia on the Central Nervous and Cardiovascular System Toxicity of Local Anesthetics. Anesth Analg, 106(5), pp.1429–1439.
Copeland, S.E., Ladd, L.A., Gu, X.-Q. & Mather, L.E., 2008b. The effects of general anesthesia on whole body and regional pharmacokinetics of local anesthetics at toxic doses. Anesth Analg, 106(5), pp.1440–1449.
Cordell, C.L., Schubkegel, T., Light, T.R. & Ahmad, F., 2010. Lipid Infusion Rescue for Bupivacaine-Induced Cardiac Arrest After Axillary Block. J Hand Surg, 35(1), pp.144–146.
De Oliveira, G.S., Jr., Chang, R., Kendall, M.C., Fitzgerald, P.C. & McCarthy, R.J., 2012. Publication Bias in the Anesthesiology Literature. Anesth Analg, 114(5), pp.1042–1048.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
Denson, D., Coyle, D., Thompson, G. & Myers, J., 1984. Alpha 1-acid glycoprotein and albumin in human serum bupivacaine binding. Clin Pharmacol Ther, 35(3), pp.409–415.
Di Gregorio, G., Neal, J.M., Rosenquist, R.W. & Weinberg, G.L., 2010. Clinical presentation of local anesthetic systemic toxicity: a review of published cases, 1979 to 2009. Reg Anesth Pain Med, 35(2), pp.181–187.
Di Gregorio, G., Schwartz, D., Ripper, R., Kelly, K., Feinstein, D.L., Minshall, R.D., Massad, M., Ori, C. & Weinberg, G.L., 2009. Lipid emulsion is superior to vasopressin in a rodent model of resuscitation from toxin-induced cardiac arrest. Crit Care Med, 37(3), pp.993–999.
Dix, S.K., Rosner, G.F., Nayar, M., Harris, J.J., Guglin, M.E., Winterfield, J.R., Xiong, Z. & Mudge, G.H.J., 2011. Intractable cardiac arrest due to lidocaine toxicity successfully resuscitated with lipid emulsion. Crit Care Med, 39(4), pp.872–874.
Dolcourt, B. & Aaron, C., 2008. Intravenous Fat Emulsion for Refractory Verapamil and Atenolol Induced Shock: A Human Case Report. Clin Toxicol, 46(7), pp.619–620.
Dony, P., Dewinde, V., Vanderick, B., Cuignet, O., Gautier, P., Legrand, E., Lavand’homme, P. & De Kock, M., 2000. The comparative toxicity of ropivacaine and bupivacaine at equipotent doses in rats. Anesth Analg, 91(6), pp.1489–1492.
Drasner, K., 2010. Local Anesthetic Systemic Toxicity. Reg Anesth Pain Med, 35(2), pp.162–166.
Easterbrook, P.J., Berlin, J.A., Gopalan, R. & Matthews, D.R., 1991. Publication bias in clinical research. Lancet, 337(8746), pp.867–872.
Eger, E.I.I., 1981. Isoflurane: A Review. Anesthesiology, 55(5), pp.559–576.
Engels, P.T. & Davidow, J.S., 2010. Intravenous fat emulsion to reverse haemodynamic instability from intentional amitriptyline overdose. Resuscitation, 81(8), pp.1037–1039.
Epemolu, O., Bom, A., Hope, F. & Mason, R., 2003. Reversal of neuromuscular blockade and simultaneous increase in plasma rocuronium concentration after the intravenous infusion of the novel reversal agent Org 25969. Anesthesiology, 99(3), pp.632–637.
Espinet, A.J. & Emmerton, M.T., 2009. The successful use of intralipid for treatment of
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 81 –
local anesthetic-induced central nervous system toxicity: Some considerations for administration of intralipid in an emergency. Clin J Pain, 25(9), pp.808–809.
European Medicines Agency, 2009. Note for guidance on non-clinical safety studies for the conduct of human clinical trials and marketing authorization for pharmaceuticals, ICH M3(R2).
Faul, F., Erdfelder, E., Lang, A.-G. & Buchner, A., 2007. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods, 39(2), pp.175–191.
Ferner, R.E., 2008. Post-mortem clinical pharmacology. British Journal of Clinical Pharmacology, 66(4), pp.430–443.
Finn, S.D.H., Uncles, D.R., Willers, J. & Sable, N., 2009. Early treatment of a quetiapine and sertraline overdose with Intralipid®. Anaesthesia, 64(2), pp.191–194.
Foxall, G., McCahon, R., Lamb, J., Hardman, J.G. & Bedforth, N.M., 2007. Levobupivacaine-induced seizures and cardiovascular collapse treated with Intralipid. Anaesthesia, 62(5), pp.516–518.
Franxman, T.J., Al-Nabhan, M., Cavallazzi, R.S. & Speak, A.J., 2011. Lipid emulsion therapy for verapamil overdose. Ann Intern Med, 154(4), p.292.
French, D., Armenian, P., Ruan, W., Wong, A., Drasner, K., Olson, K. & Wu, A., 2011a. Serum verapamil concentrations before and after Intralipid® therapy during treatment of an overdose. Clin Toxicol (Phila), 49(4), pp.340–344.
French, D., Smollin, C., Ruan, W., Wong, A., Drasner, K. & Wu, A.H.B., 2011b. Partition constant and volume of distribution as predictors of clinical efficacy of lipid rescue for toxicological emergencies. Clin Toxicol, 49(9), pp.801–809.
Fresenius-Kabi, 2007. Intralipid 20%, U.S. Food and Drug Administration.
Fuzaylov, G., Ying, B., Tang, Y. & Sethna, N.F., 2010. Successful resuscitation after inadvertent intravenous injection of bupivacaine in an adolescent. Pediatr Anesth, 20(10), pp.958–959.
Gallagher, C.J., Tan, J.M. & Foster, C.-G., 2010. Lipid rescue for bupivacaine toxicity during cardiovascular procedures. Heart Int, 5(1), pp.20–21.
Gnaho, A., Eyrieux, S. & Gentili, M., 2009. Cardiac arrest during an ultrasound-guided
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
Granato, D., Blum, S., Rossle, C., Le Boucher, J., Malnoe, A. & Dutot, G., 2000. Effects of parenteral lipid emulsions with different fatty acid composition on immune cell functions in vitro. Journal of Parenteral and Enteral Nutrition, 24(2), pp.113–118.
Greene, H.L., Hazlett, D. & Demaree, R., 1976. Relationship between Intralipid-induced hyperlipemia and pulmonary function. Am J Clin Nutr, 29(2), pp.127–135.
Grimm, H., 2005. A balanced lipid emulsion—A new concept in parenteral nutrition. Clinical Nutrition Supplements, 1(3), pp.25–30.
Groban, L., 2003. Central nervous system and cardiac effects from long-acting amide local anesthetic toxicity in the intact animal model. Reg Anesth Pain Med, 28(1), pp.3–11.
Guaiana, G., Barbui, C. & Hotopf, M., 2009. Amitriptyline for depression. Cochrane Database Syst Rev, (3), pp.1–128.
Harchelroad, F. & Palma, A., 2008. Efficacy and safety of intravenous lipid therapy in a beta blocker overdose. Clin Toxicol, 46(7), p.634.
Harvey, M. & Cave, G., 2012. Case report: successful lipid resuscitation in multi-drug overdose with predominant tricyclic antidepressant toxidrome. Int J Emerg Med, 5(1), p.8.
Harvey, M. & Cave, G., 2007. Intralipid outperforms sodium bicarbonate in a rabbit model of clomipramine toxicity. Ann Emerg Med, 49(2), pp.178–185.
Harvey, M., Cave, G. & Hoggett, K., 2009. Correlation of plasma and peritoneal diasylate clomipramine concentration with hemodynamic recovery after intralipid infusion in rabbits. Ann Emerg Med, 16(2), pp.151–156.
Harvey, M., Cave, G., Chanwai, G. & Nicholson, T., 2011a. Successful resuscitation from bupivacaine-induced cardiovascular collapse with intravenous lipid emulsion following femoral nerve block in an emergency department. Emerg Med Australas, 23(2), pp.209–214.
Harvey, M., Cave, G., Lahner, D., Desmet, J., Prince, G. & Hopgood, G., 2011b. Insulin versus Lipid Emulsion in a Rabbit Model of Severe Propranolol Toxicity: A Pilot Study. Crit Care Res Pract.
Harvey, M.G. & Cave, G.R., 2008. Intralipid infusion ameliorates propranolol-induced hypotension in rabbits. J Med Toxicol, 4(2), pp.71–76.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 83 –
Hepp, U., Stulz, N., Unger-Köppel, J. & Ajdacic-Gross, V., 2011. Methods of suicide used by children and adolescents. Eur Child Adolesc Psychiatry, 21(2), pp.67–73.
Hicks, S.D., Salcido, D.D., Logue, E.S., Suffoletto, B.P., Empey, P.E., Poloyac, S.M., Miller, D.R., Callaway, C.W. & Menegazzi, J.J., 2009. Lipid emulsion combined with epinephrine and vasopressin does not improve survival in a swine model of bupivacaine-induced cardiac arrest. Anesthesiology, 111(1), pp.138–146.
Hiemke, C. & Härtter, S., 2000. Pharmacokinetics of selective serotonin reuptake inhibitors. Pharmacol Ther, 85(1), pp.11–28.
Hiller, D.B., Di Gregorio, G., Kelly, K., Ripper, R., Edelman, L., Boumendjel, R., Drasner, K. & Weinberg, G.L., 2010. Safety of high volume lipid emulsion infusion: a first approximation of LD50 in rats. Reg Anesth Pain Med, 35(2), pp.140–144.
Hiller, D.B., Gregorio, G.D., Ripper, R., Kelly, K., Massad, M., Edelman, L., Edelman, G., Feinstein, D.L. & Weinberg, G.L., 2009. Epinephrine impairs lipid resuscitation from bupivacaine overdose: a threshold effect. Anesthesiology, 111(3), pp.498–505.
Hillyard, S.G., Barrera-Groba, C. & Tighe, R., 2010. Intralipid reverses coma associated with zopiclone and venlafaxine overdose. Eur J Anaesthesiol, 27(6), pp.582–583.
Hoizey, G., Lamiable, D., Robinet, A., Ludot, H., Malinovsky, J.-M., Kaltenbach, M.L., Binet, L., Boulanger, C. & Millart, H., 2005. Sensitive bioassay of bupivacaine in human plasma by liquid-chromatography-ion trap mass spectrometry. J Pharm Biomed Anal, 39(3-4), pp.587–592.
Holm, S., 1979. A simple sequentially rejective multiple test procedure. Scand J Statist, 6(2), pp.65–70.
Howland, M.A., 2011a. Digoxin-Specific Antibody Fragments. In L. S. Nelson, N. A. Lewin, M. A. Howland, R. S. Hoffman, R. S. Goldfrank, & N. E. Flomenbaum, eds. Goldfrank’s Toxicologic Emergencies. McGraw-Hill, pp. 946–951.
Howland, M.A., 2011b. Pharmacokinetic and Toxicokinetic Principles. In L. S. Nelson, N. A. Lewin, M. A. Howland, R. S. Hoffman, L. S. Goldfrank, & N. E. Flomenbaum, eds. Goldfrank’s Toxicologic Emergencies. McGraw-Hill, pp. 119–134.
Huang, J.M., Xian, H. & Bacaner, M., 1992. Long-chain fatty acids activate calcium channels in ventricular myocytes. Proc Natl Acad Sci USA, 89(14), pp.6452–6456.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
Jakkala-Saibaba, R., Morgan, P.G. & Morton, G.L., 2011. Treatment of cocaine overdose with lipid emulsion. Anaesthesia, 66(12), pp.1168–1170.
Jamaty, C., Bailey, B., Larocque, A., Notebaert, E., Sanogo, K. & Chauny, J.M., 2010. Lipid emulsions in the treatment of acute poisoning: a systematic review of human and animal studies. Clin Toxicol, 48(1), pp.1–27.
Jonsson, A., Holmgren, P. & Ahlner, J., 2004. Fatal intoxications in a Swedish forensic autopsy material during 1992-2002. Forensic Sci Int, 143(1), pp.53–59.
Joshi, S.J., Karbhari, P.A. & Bhoir, S.I., 2009. RP-LC Simultaneous Determination of Nebivolol Hydrochloride and Amlodipine Besilate in Bi-Layer Tablets. Chroma, 70(3-4), pp.557–561.
Jovic-Stosic, J., Gligic, B., Putic, V., Brajkovic, G. & Spasic, R., 2011. Severe propranolol and ethanol overdose with wide complex tachycardia treated with intravenous lipid emulsion: A case report. Clin Toxicol (Phila), 49(5), pp.426–430.
Kazemi, A., Harvey, M., Cave, G. & Lahner, D., 2011. The effect of lipid emulsion on depth of anaesthesia following thiopental administration to rabbits. Anaesthesia, 66(5), pp.373–378.
Knudsen, K., Suurkula, M.B., Blomberg, S., Sjovall, J. & Edvardsson, N., 1997. Central nervous and cardiovascular effects of i.v. infusions of ropivacaine, bupivacaine and placebo in volunteers. Br J Anaesth, 78(5), pp.507–514.
Kollroser, M. & Schober, C., 2002. Determination of amiodarone and desethylamiodarone in human plasma by high-performance liquid chromatography-electrospray ionization tandem mass spectrometry with an ion trap detector. J Chromatogr B, 766(2), pp.219–226.
Krieglstein, J., Meffert, A. & Niemeyer, D., 1974. Inf luence of emulsif ied fat on chlorpromazine availability in rabbit blood. Experientia, 30(8), pp.924–926.
Kyttä, J., Heavner, J.E., Badgwell, J.M. & Rosenberg, P.H., 1991. Cardiovascular and central nervous system effects of co-administered lidocaine and bupivacaine in piglets. Reg Anesth, 16(2), pp.89–94.
Lapatto-Reiniluoto, O., Kivistö, K.T., Pohjola-Sintonen, S., Luomanmäki, K. & Neuvonen,
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 85 –
P.J., 1998. A prospective study of acute poisonings in Finnish hospital patients. Hum Exp Toxicol, 17(6), pp.307–311.
Leatham, E.W., Holt, D.W. & McKenna, W.J., 1993. Class III antiarrhythmics in overdose. Presenting features and management principles. Drug Saf, 9(6), pp.450–462.
Ledger, R., 2003. Nonaromatic hydroxylation of bupivacaine during continuous epidural infusion in man. J Biochem Biophys Methods, 57(2), pp.105–114.
Li, B., Yan, J., Shen, Y., Li, B., Hu, Z. & Ma, Z., 2012. Association of sustained cardiovascular recovery with epinephrine in the delayed lipid-based resuscitation from cardiac arrest induced by bupivacaine overdose in rats. Br J Anaesth, 108(5), pp.857–863.
Liang, C.W., Diamond, S.J. & Hagg, D.S., 2011. Lipid rescue of massive verapamil overdose: a case report. J Med Case Rep, 5(1), pp.399–403.
Liebelt, E.L., 2011. Cyclic Antidepressants. In L. S. Nelson, N. A. Lewin, M. A. Howland, R. S. Hoffman, L. S. Goldfrank, & N. E. Flomenbaum, eds. Goldfrank’s Toxicologic Emergencies. McGraw-Hill, pp. 1049–1059.
Liebelt, E.L., Ulrich, A., Francis, P.D. & Woolf, A., 1997. Serial electrocardiogram changes in acute tricyclic antidepressant overdoses. Crit Care Med, 25(10), pp.1721–1726.
Lin, E.P. & Aronson, L.A., 2010. Successful resuscitation of bupivacaine-induced cardiotoxicity in a neonate. Pediatr Anesth, 20(10), pp.955–957.
Lindgren, L., Randell, T., Suzuki, N., Kyttä, J., Yli-Hankala, A. & Rosenberg, P.H., 1992. The effect of amrinone on recovery from severe bupivacaine intoxication in pigs. Anesthesiology, 77(2), pp.309–315.
Litz, R.J., Popp, M., Stehr, S.N. & Koch, T., 2006. Successful resuscitation of a patient with ropivacaine-induced asystole after axillary plexus block using lipid infusion. Anaesthesia, 61(8), pp.800–801.
Litz, R.J., Roessel, T., Heller, A.R. & Stehr, S.N., 2008. Reversal of central nervous system and cardiac toxicity after local anesthetic intoxication by lipid emulsion injection. Anesth Analg, 106(5), pp.1575–1577.
Livshits, Z., Feng, Q., Chowdhury, F., Amdo, T.D., Nelson, L.S. & Hoffman, R.S., 2011. Life-Threatening Bupropion Ingestion: Is There a Role for Intravenous Fat Emulsion? Basic Clin Pharmacol Toxicol, 109, pp.418–422.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 86 –
Lokajova, J., Laine, J., Puukilainen, E., Ritala, M., Holopainen, J.M. & Wiedmer, S.K., 2010. Liposomes for entrapping local anesthetics: a liposome electrokinetic chromatographic study. Electrophoresis, 31(9), pp.1540–1549.
Long, W.B., Rosenblum, S. & Grady, I.P., 1989. Successful resuscitation of bupivacaine-induced cardiac arrest using cardiopulmonary bypass. Anesth Analg, 69(3), pp.403–406.
Lu, J., Hast, H. & Erickson, T., 2009. Dramatic QTc Narrowing after Intralipid Administration in Quetiapine Overdose. Clin Toxicol, 47(7), p.740.
Ludot, H., Tharin, J.-Y., Belouadah, M., Mazoit, J.-X. & Malinovsky, J.-M., 2008. Successful Resuscitation After Ropivacaine and Lidocaine-Induced Ventricular Arrhythmia Following Posterior Lumbar Plexus Block in a Child. Anesth Analg, 106(5), pp.1572–1574.
Markowitz, S. & Neal, J.M., 2009. Immediate lipid emulsion therapy in the successful treatment of bupivacaine systemic toxicity. Reg Anesth Pain Med, 34(3), p.276.
Marwick, P. C., Levin, A.I. & Coetzee, A.R., 2009. Recurrence of cardiotoxicity after lipid rescue from bupivacaine-induced cardiac arrest. Anesth Analg, 108(4), pp.1344–1346.
Mashru, R., Sutariya, V., Sankalia, M. & Sankalia, J., 2005. Transbuccal delivery of lamotrigine across porcine buccal mucosa: in vitro determination of routes of buccal transport. J Pharm Pharm Sci, 8(1), pp.54–62.
Mather, L., Copeland, S. & Ladd, L., 2005. Acute Toxicity of Local Anesthetics: Underlying Pharmacokinetic and Pharmacodynamic Concepts. Reg Anesth Pain Med, 30(6), pp.553–566.
Mauch, J., Martin Jurado, O., Spielmann, N., Bettschart-Wolfensberger, R. & Weiss, M., 2011. Comparison of epinephrine vs lipid rescue to treat severe local anesthetic toxicity - an experimental study in piglets. Pediatr Anesth, 21(11), pp.1103–1108.
Mauch, J., Martin Jurado, O., Spielmann, N., Bettschart-Wolfensberger, R. & Weiss, M., 2012. Resuscitation strategies from bupivacaine-induced cardiac arrest. Pediatr Anesth, 22(2), pp.124–129.
Mayr, V.D., Mitterschiffthaler, L., Neurauter, A., Gritsch, C., Wenzel, V., M ºller, T., Luckner, G., Lindner, K.H. & Strohmenger, H.-U., 2008. A comparison of the combination of epinephrine and vasopressin with lipid emulsion in a porcine model of asphyxial cardiac arrest after intravenous injection of bupivacaine. Anesth Analg, 106(5), pp.1566–1571.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 87 –
Mazoit, J.-X., Le Guen, R., Beloeil, H. & Benhamou, D., 2009. Binding of long-lasting local anesthetics to lipid emulsions. Anesthesiology, 110(2), pp.380–386.
Mazoit, J.X., Orhant, E.E., Boïco, O., Kantelip, J.P. & Samii, K., 1993. Myocardial uptake of bupivacaine: I. Pharmacokinetics and pharmacodynamics of lidocaine and bupivacaine in the isolated perfused rabbit heart. Anesth Analg, 77(3), pp.469–476.
McAllister, R.K., Tutt, C.D. & Colvin, C.S., 2012. Lipid 20% emulsion ameliorates the symptoms of olanzapine toxicity in a 4-year-old. Am J Emerg Med, 30(6), pp.1012.e1–2.
McCutchen, T. & Gerancher, J., 2008. Early Intralipid Therapy May Have Prevented Bupivacaine-Associated Cardiac Arrest. Reg Anesth Pain Med, 33(2), pp.178–180.
Meehan, T., Gummin, D., Kostic, M., Cattapan, S., Waghray, R. & Bryant, S., 2009. Beta Blocker Toxicity Successfully Treated with Intravenous Fat Emulsion: A Case Series. Clin Toxicol, 47(7), p.735.
Minton, N.A., Goode, A.G. & Henry, J.A., 1987. The effect of a lipid suspension on amitriptyline disposition. Arch Toxicol, 60(6), pp.467–469.
Mirtallo, J.M., Dasta, J.F., Kleinschmidt, K.C. & Varon, J., 2010. State of the art review: Intravenous Fat Emulsions: Current Applications, Safety Profile, and Clinical Implications. Ann Pharmacother, 44(4), pp.688–700.
Mizutani, K., Oda, Y. & Sato, H., 2011. Successful treatment of ropivacaine-induced central nervous system toxicity by use of lipid emulsion: effect on total and unbound plasma fractions. J Anesth, 25(3), pp.442–445.
Montiel, V., Gougnard, T. & Hantson, P., 2011. Diltiazem poisoning treated with hyperinsulinemic euglycemia therapy and intravenous lipid emulsion. Eur J Emerg Med, 18(2), pp.121–123.
Morey, T.E., Varshney, M., Flint, J.A., Rajasekaran, S., Shah, D.O. & Dennis, D.M., 2004. Treatment of Local Anesthetic-Induced Cardiotoxicity Using Drug Scavenging Nanoparticles. Nano Lett, 4(4), pp.757–759.
Motomura, S., Wu, Z.J. & Hashimoto, K., 1993. Lacidipine, a new long-acting dihydropyridine calcium antagonist, has high vascular selectivity against all intracardiac variables. Heart Vessels, 8(1), pp.16–22.
Muhonen, J., Holopainen, J.M. & Wiedmer, S.K., 2009. Interactions between local anesthetics and lipid dispersions studied with liposome electrokinetic capillary
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 88 –
chromatography. J Chromatogr A, 1216(15), pp.3392–3397.
Mulroy, M., 2002. Systemic toxicity and cardiotoxicity from local anesthetics: Incidence and preventive measures. Reg Anesth Pain Med, 27(6), pp.556–561.
Munoz, A., Karila, P., Gallay, P., Zettelmeier, F., Messner, P., Mery, M. & Grolleau, R., 1988. A randomized hemodynamic comparison of intravenous amiodarone with and without Tween 80. Eur Heart J, 9(2), pp.142–148.
Mylan, 2011. Doxepin, Mylan New Zealand Ltd.
Neal, J.M., Bernards, C.M., Butterworth, J.F.4., Di Gregorio, G., Drasner, K., Hejtmanek, M.R., Mulroy, M.F., Rosenquist, R.W. & Weinberg, G.L., 2010. ASRA practice advisory on local anesthetic systemic toxicity. Reg Anesth Pain Med, 35(2), pp.152–161.
Nelson, L.S. & Lewin, N.A., 2011. Antidysrhythmics. In L. S. Nelson, N. A. Lewin, M. A. Howland, R. S. Hoffman, L. R. Goldfrank, & N. E. Flomenbaum, eds. Goldfrank’s Toxicologic Emergencies. McGraw-Hill, pp. 925–935.
Nielsen, M.K.K. & Johansen, S.S., 2009. Determination of olanzapine in whole blood using simple protein precipitation and liquid chromatography-tandem mass spectrometry. Journal of analytical toxicology, 33(4), pp.212–217.
Oakes, J., Piquette, C. & Barthold, C., 2009. Successful Use of Intravenous Lipid as Adjunctive Therapy in a Severe Calcium Channel Antagonist Poisoning. Clin Toxicol, 47(7), pp.755–756.
Ochs, H.R. & Smith, T.W., 1977. Reversal of advanced digitoxin toxicity and modification of pharmacokinetics by specific antibodies and Fab fragments. J Clin Invest, 60(6), pp.1303–1313.
Papadopoulou, A., Willers, J.W., Samuels, T.L. & Uncles, D.R., 2012. The use of dye surrogates to illustrate local anesthetic drug sequestration by lipid emulsion: a visual demonstration of the lipid sink effect. Reg Anesth Pain Med, 37(2), pp.183–187.
Pennec, J.-P., Guillouet, M., Rannou, F., Arvieux, C.C. & Gueret, G., 2010. Hemodynamic effects of lipid emulsion after local anesthetic intoxication may be due to a direct effect of fatty acids on myocardial voltage-dependent calcium channels. Can J Anesth, 57(10), pp.947–947.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 89 –
Perez, E., Bania, T., Medlej, K. & Chu, J., 2008. Determining the optimal dose of intravenous fat emulsion for the treatment of severe verapamiltoxicity in a rodent model. Acad Emerg Med, 15(12), pp.1284–1289.
Picard, J. & Meek, T., 2006. Lipid emulsion to treat overdose of local anaesthetic: the gift of the glob. Anaesthesia, 61(2), pp.107–109.
Pilcher, J.E., 1886. Cocaine as an anaesthetic; its status at the close of the first year of its use. Ann Surg, 3(1), pp.51–66.
Rampono, J., Kristensen, J.H., Ilett, K.F., Hackett, L.P. & Kohan, R., 2007. Quetiapine and Breast Feeding. Ann Pharmacother, 41(4), pp.711–714.
Rang, H.P., Dale, M.M. & Ritter, J.M., 1999a. Absorption and Distribution of Drugs. In Pharmacology. Edinburgh: Churchill Livingstone, pp. 61–77.
Rang, H.P., Dale, M.M. & Ritter, J.M., 1999b. Individual Variation and Drug Interaction. In Pharmacology. Edinburgh: Churchill Livingstone, pp. 746–756.
Rosenberg, P.H., Veering, B.T. & Urmey, W.F., 2004. Maximum recommended doses of local anesthetics: a multifactorial concept. Reg Anesth Pain Med, 29(6), pp.564–575.
Rosenblatt, M.A., Abel, M., Fischer, G.W., Itzkovich, C.J. & Eisenkraft, J.B., 2006. Successful use of a 20% lipid emulsion to resuscitate a patient after a presumed bupivacaine-related cardiac arrest. Anesthesiology, 105(1), pp.217–218.
Ruan, W., French, D., Wong, A., Drasner, K. & Wu, A.H.B., 2012. A Mixed (Long- and Medium-chain) Triglyceride Lipid Emulsion Extracts Local Anesthetic from Human Serum In Vitro More Effectively than a Long-chain Emulsion. Anesthesiology, 116(2), pp.334–339.
Rubin, M., Moser, A., Vaserberg, N., Greig, F., Levy, Y., Spivak, H., Ziv, Y. & Lelcuk, S., 2000. Structured triacylglycerol emulsion, containing both medium- and long-chain fatty acids, in long-term home parenteral nutrition: a double-blind randomized cross-over study. Nutrition, 16(2), pp.95–100.
Russo, H., Brès, J., Duboin, M.P. & Roquefeuil, B., 1995. Pharmacokinetics of thiopental after single and multiple intravenous doses in critical care patients. Eur J Clin Pharmacol, 49(1-2), pp.127–137.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 90 –
Saarto, T. & Wiffen, P.J., 2010. Antidepressants for neuropathic pain. Cochrane Database Syst Rev, (4), pp.1–75.
Samanidou, V.F., Nika, M.K. & Papadoyannis, I.N., 2007. Development of an HPLC method for the monitoring of tricyclic antidepressants in biofluids. J Sep Sci, 30(15), pp.2391–2400.
Samuels, T.L., Willers, J.W., Uncles, D.R., Monteiro, R., Halloran, C. & Dai, H., 2011. In vitro suppression of drug-induced methaemoglobin formation by Intralipid® in whole human blood: observations relevant to the “lipid sink theory.” Anaesthesia, 67(1), pp.23–32.
Schwartz, D.R. & Kaufman, B., 2011. Local Anesthetics. In L. S. Nelson, N. A. Lewin, M. A. Howland, R. S. Hoffman, L. R. Goldfrank, & N. E. Flomenbaum, eds. Goldfrank’s Toxicologic Emergencies. McGraw-Hill, pp. 965–975.
Shalaeva, M., Kenseth, J., Lombardo, F. & Bastin, A., 2008. Measurement of dissociation constants (pKa values) of organic compounds by multiplexed capillary electrophoresis using aqueous and cosolvent buffers. J Pharm Sci, 97(7), pp.2581–2606.
Shayeganpour, A., Jun, A.S. & Brocks, D.R., 2005. Pharmacokinetics of Amiodarone in hyperlipidemic and simulated high fat-meal rat models. Biopharm Drug Dispos, 26(6), pp.249–257.
Shih, Y.H., Chen, C.H., Wang, Y.M. & Liu, K., 2011. Successful reversal of bupivacaine and lidocaine-induced severe junctional bradycardia by lipid emulsion following infraclavicular brachial plexus block in a uremic patient. Acta Anaesthesiol Taiwan, 49(2), pp.72–74.
Simon, M.A., Vree, T.B., Gielen, M.J., Booij, L.H. & Lagerwerf, A.J., 1998. Comparison of the effects and disposition kinetics of lidocaine and (+/-)prilocaine in patients undergoing axillary brachial plexus block during day case surgery. Clin Drug Investig, 16(3), pp.241–250.
Sinner, B. & Graf, B.M., 2008. Ketamine. In J. Schüttler & H. Schwilden, eds. Modern Anesthetics. Germany: Springer Berlin Heidelberg, pp. 313–333.
Sirianni, A.J., Osterhoudt, K.C., Calello, D.P., Muller, A.A., Waterhouse, M.R., Goodkin, M.B., Weinberg, G.L. & Henretig, F.M., 2008. Use of lipid emulsion in
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 91 –
the resuscitation of a patient with prolonged cardiovascular collapse after overdose of bupropion and lamotrigine. Ann Emerg Med, 51(4), pp.412–415.
Smith, H.M., Jacob, A.K., Segura, L.G., Dilger, J.A. & Torsher, L.C., 2008. Simulation Education in Anesthesia Training: A Case Report of Successful Resuscitation of Bupivacaine-Induced Cardiac Arrest Linked to Recent Simulation Training. Anesth Analg, 106(5), pp.1581–1584.
Sonsino, D.H. & Fischler, M., 2009. Immediate intravenous lipid infusion in the successful resuscitation of ropivacaine-induced cardiac arrest after infraclavicular brachial plexus block. Reg Anesth Pain Med, 34(3), pp.276–277.
Spence, A.G., 2007. Lipid reversal of central nervous system symptoms of bupivacaine toxicity. Anesthesiology, 107(3), pp.516–517.
Stehr, S.N., Ziegeler, J.C., Pexa, A., Oertel, R., Deussen, A., Koch, T. & Hubler, M., 2007. The effects of lipid infusion on myocardial function and bioenergetics in l-bupivacaine toxicity in the isolated rat heart. Anesth Analg, 104(1), pp.186–192.
Stellpflug, S.J., Harris, C.R., Engebretsen, K.M., Cole, J.B. & Holger, J.S., 2010. Intentional overdose with cardiac arrest treated with intravenous fat emulsion and high-dose insulin. Clin Toxicol, 48(3), pp.227–229.
Stojanović, J., Marinković, V., Vladimirov, S., Veličković, D. & Sibinović, P., 2005. Determination of Carvedilol and its Impurities in Pharmaceuticals. Chroma, 62(9-10), pp.539–542.
Straathof, D.J., Driessen, O., Meijer, J.W., Van Rees, H., Vermeij, P. & Vermeij, T.A., 1984. Influence of Intralipid infusion on the elimination of phenytoin. Arch Int Pharmacodyn Ther, 267(2), pp.180–186.
Swindle, M.M., Makin, A., Herron, A.J., Clubb, F.J.J. & Frazier, K.S., 2011. Swine as models in biomedical research and toxicology testing. Vet Pathol, 49(2), pp. 344-356.
Szebeni, J., 2005. Complement activation-related pseudoallergy: A new class of drug-induced acute immune toxicity. Toxicology, 216(2-3), pp.106–121.
Szebeni, J., Alving, C.R., Rosivall, L., Bunger, R., Baranyi, L., Bedocs, P., Toth, M. & Barenholz, Y., 2007. Animal models of complement-mediated hypersensitivity reactions to liposomes and other lipid-based nanoparticles. J Liposome Res, 17(2), pp.107–117.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 92 –
Szebeni, J., Baranyi, L., Savay, S., Bodo, M., Morse, D.S., Basta, M., Stahl, G.L., Bunger, R. & Alving, C.R., 2000. Liposome-induced pulmonary hypertension: properties and mechanism of a complement-mediated pseudoallergic reaction. Am J Physiol Heart Circ Physiol, 279(3), pp.1319–1328.
Szebeni, J., Muggia, F., Gabizon, A. & Barenholz, Y., 2011. Activation of complement by therapeutic liposomes and other lipid excipient-based therapeutic products: Prediction and prevention. Adv Drug Deliv Rev, 63(12), pp.1020–1030.
Sztark, F., Malgat, M., Dabadie, P. & Mazat, J.P., 1998. Comparison of the effects of bupivacaine and ropivacaine on heart cell mitochondrial bioenergetics. Anesthesiology, 88(5), pp.1340–1349.
Tanaka, E., Nakamura, T., Inomata, S. & Honda, K., 2006. Simultaneous determination of three local anesthetic drugs from the pipecoloxylidide group in human serum by high-performance liquid chromatography. J Chromatogr B, 834(1-2), pp.213–216.
Tatsumi, M., Groshan, K., Blakely, R.D. & Richelson, E., 1997. Pharmacological profile of antidepressants and related compounds at human monoamine transporters. Eur J Pharmacol, 340(2-3), pp.249–258.
Tebbutt, S., Harvey, M., Nicholson, T. & Cave, G., 2006. Intralipid prolongs survival in a rat model of verapamil toxicity. Ann Emerg Med, 13(2), pp.134–139.
Terada, H., Shima, O., Yoshida, K. & Shinohara, Y., 1990. Effects of the local anesthetic bupivacaine on oxidative phosphorylation in mitochondria. J Biol Chem, 265(14), pp.7837–7842.
Tetko, I.V., Tanchuk, V.Y. & Villa, A.E.P., 2001. Prediction of n-octanol/water partition coefficients from PHYSPROP database using artificial neural networks and E-state indices. J Chem Inf Model, 41(5), pp.1407–1421.
Upton, R.N., 2007. Cerebral uptake of drugs in humans. Clin Exp Pharmacol Physiol, 34(8), pp.695–701.
Van Herendael, H. & Dorian, P., 2010. Amiodarone for the treatment and prevention of ventricular fibrillation and ventricular tachycardia. Vasc Health Risk Manag, 6, pp.465–472.
Varela, H. & Bums, S.M., 2010. Use of lipid emulsions for treatment of local anesthetic toxicity: a case report. AANA J, 78(5), pp.359–364.
Varghese, J.M., Roberts, J.A. & Lipman, J., 2010. Pharmacokinetics and pharmacodynamics
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 93 –
in critically ill patients. Curr Opin Anesthesiol, 23(4), pp.472–478.
Vasskog, T., Berger, U., Samuelsen, P.-J., Kallenborn, R. & Jensen, E., 2006. Selective serotonin reuptake inhibitors in sewage influents and effluents from Tromsø, Norway. J Chromatogr A, 1115(1-2), pp.187–195.
Vuori, E., Ojanperä, I., Nokua, J. & Ojansivu, R.L., 2003. Oikeuskemiallisesti todetut myrkytyskuolemat vuosina 2000 ja 2001. Suom Lääkäril, 58(35), pp.3403–3407.
Warren, J.A., Thoma, R.B., Georgescu, A. & Shah, S.J., 2008. Intravenous Lipid Infusion in the Successful Resuscitation of Local Anesthetic-Induced Cardiovascular Collapse After Supraclavicular Brachial Plexus Block. Anesth Analg, 106(5), pp.1578–1580.
Weinberg, G., 2002. Current concepts in resuscitation of patients with local anesthetic cardiac toxicity. Reg Anesth Pain Med, 27(6), pp.568–575.
Weinberg, G. & Rubinstein, I., 2011. Pig in a Poke: Species Specificity in Modeling Lipid Resuscitation. Anesth Analg, pp.1–3.
Weinberg, G., Di Gregorio, G., Hiller, D., Hewett, A. & Sirianni, A., 2009. Reversal of haloperidol-induced cardiac arrest by using lipid emulsion. Ann Intern Med, 150(10), pp.737–738.
Weinberg, G., Lin, B., Zheng, S., Di Gregorio, G., Hiller, D., Ripper, R., Edelman, L., Kelly, K. & Feinstein, D., 2010. Partitioning effect in lipid resuscitation: further evidence for the lipid sink. Crit Care Med, 38(11), pp.2268–2269.
Weinberg, G., Ripper, R., Feinstein, D.L. & Hoffman, W., 2003. Lipid emulsion infusion rescues dogs from bupivacaine-induced cardiac toxicity. Reg Anesth Pain Med, 28(3), pp.198–202.
Weinberg, G.L., 2010. Treatment of local anesthetic systemic toxicity (LAST). Reg Anesth Pain Med, 35(2), pp.188–193.
Weinberg, G.L., Di Gregorio, G., Ripper, R., Kelly, K., Massad, M., Edelman, L., Schwartz, D., Shah, N., Zheng, S. & Feinstein, D.L., 2008. Resuscitation with lipid versus epinephrine in a rat model of bupivacaine overdose. Anesthesiology, 108(5), pp.907–913.
E. Litonius – Treatment of acute intoxication with intravenous lipid emulsion – animal and human studies
– 94 –
Weinberg, G.L., Ripper, R., Murphy, P., Edelman, L.B., Hoffman, W., Strichartz, G. & Feinstein, D.L., 2006. Lipid infusion accelerates removal of bupivacaine and recovery from bupivacaine toxicity in the isolated rat heart. Reg Anesth Pain Med, 31(4), pp.296–303.
Weinberg, G.L., VadeBoncouer, T., Ramaraju, G.A., Garcia-Amaro, M.F. & Cwik, M.J., 1998. Pretreatment or resuscitation with a lipid infusion shifts the dose-response to bupivacaine-induced asystole in rats. Anesthesiology, 88(4), pp.1071–1075.
West, P.L., Mckeown, N.J. & Hendrickson, R.G., 2010. Iatrogenic lipid emulsion overdose in a case of amlodipine poisoning. Clin Toxicol, 48(4), pp.393–396.
Whiteside, J., 2008. Reversal of local anaesthetic induced CNS toxicity with lipid emulsion. Anaesthesia, 63(2), pp.203–204.
Wishart, D., Knox, C. & Law, V. eds., DrugBank, Available at: http://www.drugbank.ca/ [Accessed May 9, 2012].
Wong, G.K., Joo, D.T. & McDonnell, C., 2010. Lipid resuscitation in a carnitine deficient child following intravascular migration of an epidural catheter. Anaesthesia, 65(2), pp.192–195.
Wójcicki, J., Jaroszynska, M., Drozdzik, M., Pawlik, A., Gawronska-Szklarz, B. & Sterna, R., 2003. Comparative pharmacokinetics and pharmacodynamics of propranolol and atenolol in normolipaemic and hyperlipidaemic obese subjects. Biopharm Drug Dispos, 24(5), pp.211–218.
Yuen, K., Chan, K., Toh, W., Peh, K., Ang, H. & Ong, B., 1996. Pharmacokinetics and comparative bioavailability of two metoprolol tablet preparations. Drug Dev Ind Pharm, 22(4), pp.329–333.
Zausig, Y.A., Graf, B.M. & Zink, W., 2009a. Is it“ lipid sink,” hemodilution, or both? Crit Care Med, 37(10), p.2863.
Zausig, Y.A., Zink, W., Keil, M., Sinner, B., Barwing, J., Wiese, C.H.R. & Graf, B.M., 2009b. Lipid emulsion improves recovery from bupivacaine-induced cardiac arrest, but not from ropivacaine- or mepivacaine-induced cardiac arrest. Anesth Analg, 109(4), pp.1323–1326.