53
Treatment of Cutaneous T- Cell Lymphoma: Focus on Relapsed/Refractory Disease This program is supported by an educational grant from Ligand and Clinical Care Options, LLC
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | imogen-anthony |
| View: | 215 times |
| Download: | 0 times |
Treatment of Cutaneous T-Cell Lymphoma: Focus on Relapsed/Refractory Disease
This program is supported by an educational grant from Ligand and Clinical Care Options, LLC
Pathophysiology and TreatmentJohn A. Zic, MDVanderbilt University Medical CenterNashville, Tennessee
Diagnosis and StagingTimothy M. Kuzel, MDNorthwestern UniversityChicago, Illinois
Treatment of Cutaneous T-Cell Lymphoma: Focus on Relapsed/Refractory Disease

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
First Description of Mycosis Fungoides
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Primary Cutaneous T-Cell Lymphoma (CTCL) Mycosis fungoides (MF)
– Most common T-Cell lymphoma of the skin
– Isolated patches, plaques, and/or tumors
Classic histopathologic features
– Superficial dermal infiltrate of malignant lymphocytes
– Cerebriform nuclei within malignant lymphocytes
– Epidermotropism (Pautrier’s microabscesses)
– Early stage lesions include reactive benign T-lymphocytes

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Histopathologic Appearance of MF
Upper dermal infiltrate of small lymphocytes with presence of Pautrier’s microabscesses in epidermis
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
TNM and B Staging of MF*
T (Skin)
– T1 Limited patch/plaque (< 10% BSA)
– T2 Generalized patch/plaque
– T3 Tumors
– T4 Generalized erythroderma
M (Viscera)
– M0 No visceral involvement
– M1 Visceral involvement
B (Blood)
– B0 Atypical circulating cells not present (< 5%)
– B1 > 5% atypical cells, < 1000 atypical cells/mm3
– B2 > 1000 atypical cells/mm3
* Staging should be done at diagnosis only and does not change with treatment effect; provides prognostic information for patients.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
TNM and B Staging of MF (continued)
N (Nodes)
– N0 No clinically abnormal nodes
– N1 Clinical abnormal node
– N2 Biopsy performed, not involved with MF
– LN0 normal; LN1 dermatopathic reactive lymph node
– LN2 dermatopathic node with atypical cells (< 6 cells/cluster)
– N3 Biopsy performed, involved with MF
– LN3 large clusters of atypical cells (> 6 cells/cluster) to partial effacement
– LN4 lymph node effacement
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
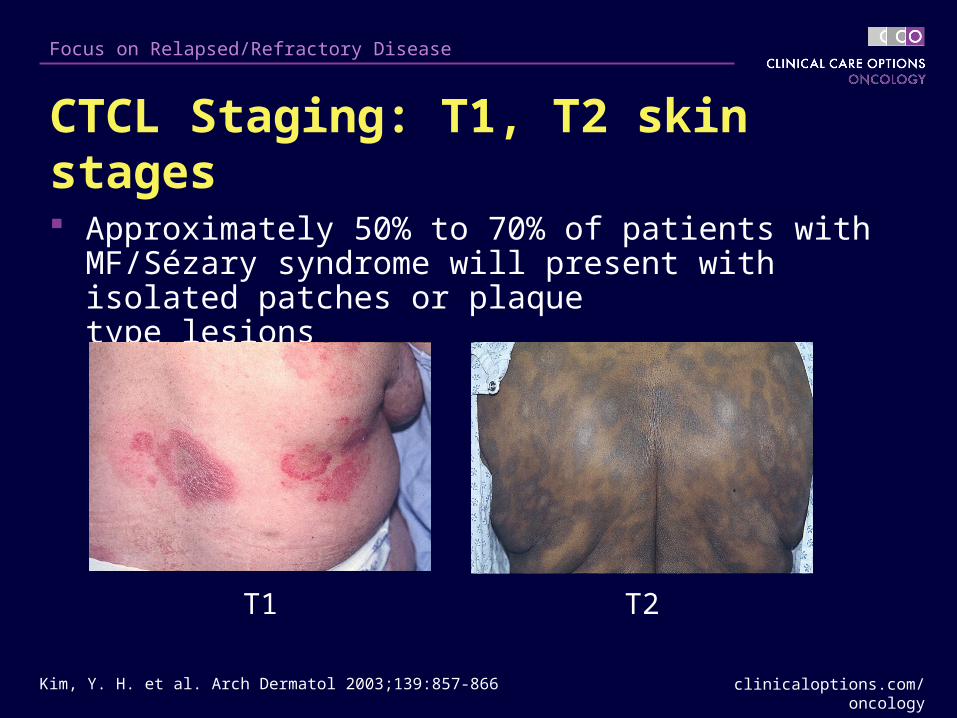
CTCL Staging: T1, T2 skin stages
Approximately 50% to 70% of patients with MF/Sézary syndrome will present with isolated patches or plaque type lesions
T1 T2
Kim, Y. H. et al. Arch Dermatol 2003;139:857-866
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
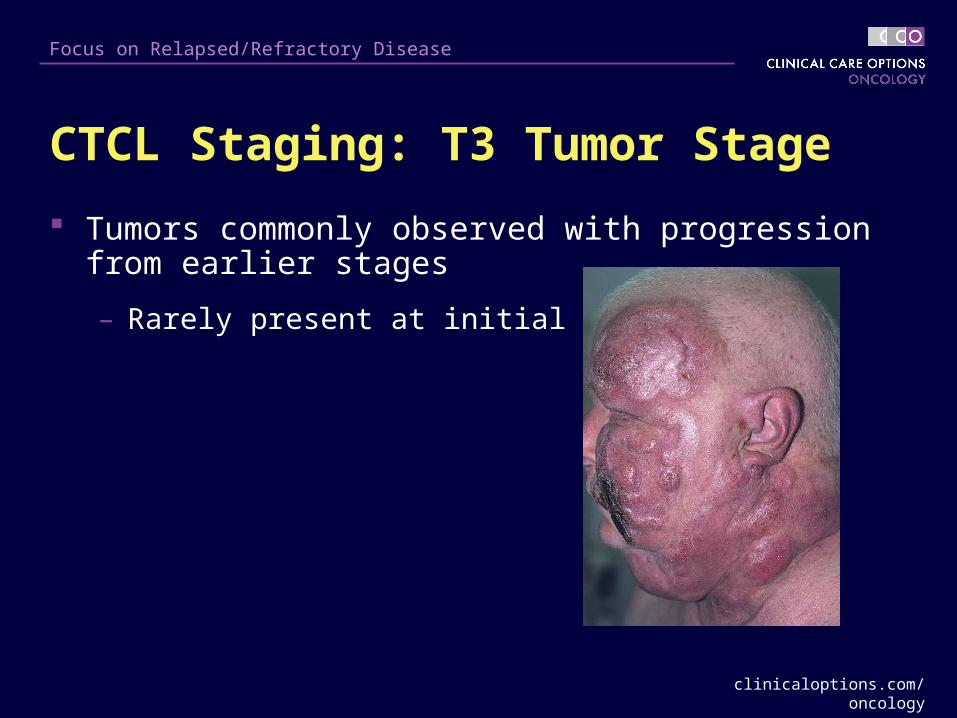
CTCL Staging: T3 Tumor Stage
Tumors commonly observed with progression from earlier stages
– Rarely present at initial diagnosis
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
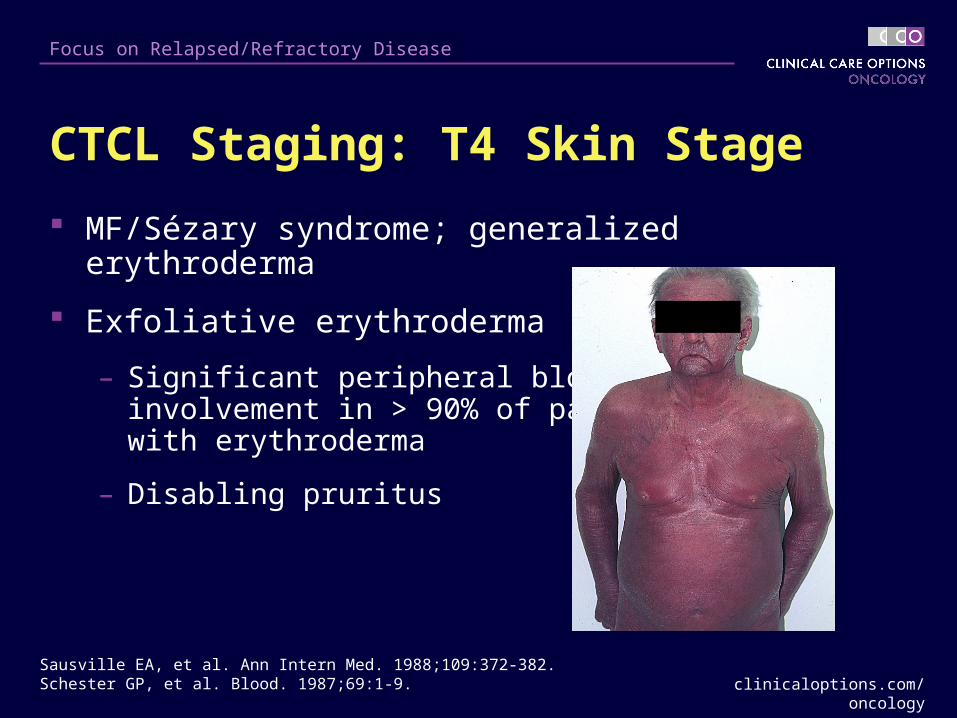
CTCL Staging: T4 Skin Stage
MF/Sézary syndrome; generalized erythroderma
Exfoliative erythroderma
– Significant peripheral blood involvement in > 90% of patients with erythroderma
– Disabling pruritus
Sausville EA, et al. Ann Intern Med. 1988;109:372-382.Schester GP, et al. Blood. 1987;69:1-9.

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
CTCL Staging: T4 Skin Stage (continued) Poor prognostic features
– PAS-positive cytoplasmic inclusions
– CD4 positive, CD7 negative phenotype
– Large circulating Sézary cells

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Staging of CTCL: LN Path stages
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
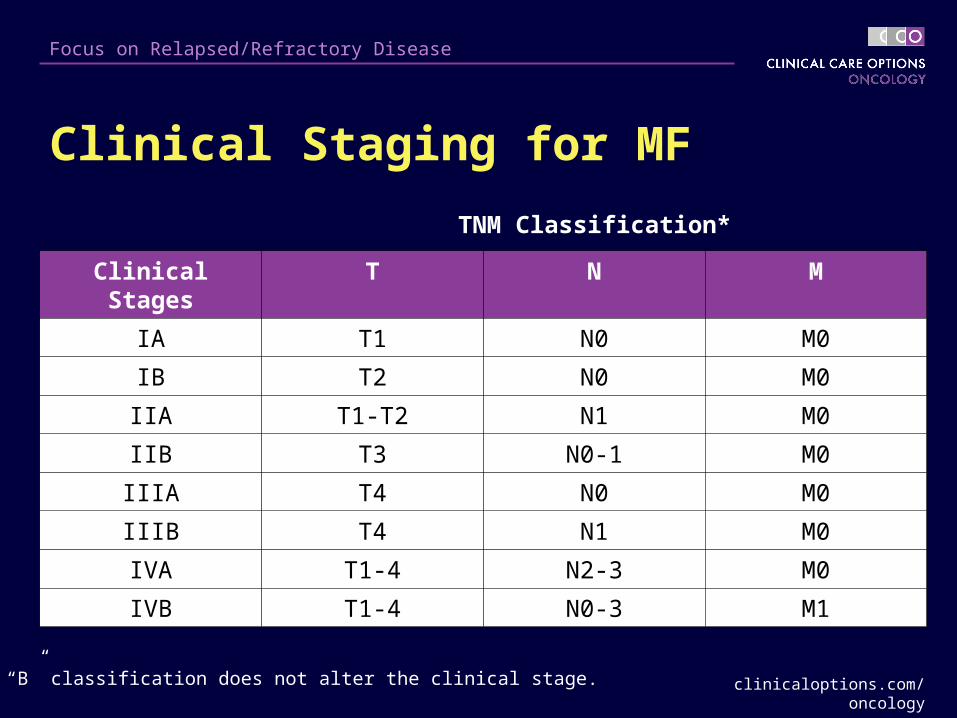
Clinical Staging for MF
Clinical Stages T N M
IA T1 N0 M0
IB T2 N0 M0
IIA T1-T2 N1 M0
IIB T3 N0-1 M0
IIIA T4 N0 M0
IIIB T4 N1 M0
IVA T1-4 N2-3 M0
IVB T1-4 N0-3 M1
* The “B” classification does not alter the clinical stage.
TNM Classification*
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
CTCL: Survival By Stage
Survival for CTCL patient varies according to stage
Little overlap in survival between stages
– Stage IA: no median survival, similar to general population
– Stage IB: 5-year survival ~ 85%
Poor survival in advanced disease
– Median survival for patients with stage IV CTCL: ~ 2.5 years
Kim, Y. H. et al. Arch Dermatol 2003;139:857-866

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
MF Histopathology
Surface antigen immunophenotyping
– Classic antigenic profile: CD4+, CD8-, CD26-, CD45RO+
– Variable presence or loss of pan T-cell markers CD5 and/or CD7
Early-stage lesions characterized by
– Infiltrating “reactive” CD8+ T-lymphocytes
– Cutaneous dendritic cells (lost upon disease progression)
T-cell gene rearrangement testing to confirm clonality
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
MF: Recommended Staging Studies
Routine clinical evaluations should include:
– History and physical examination
– Complete blood count with differential
– Examination of blood smear for quantification of atypical lymphocytes (Sézary cells)
– Comprehensive chemistry panel
– Lactate dehydrogenase (LDH)
– Lymph node biopsy if clinically apparent nodes present
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
MF: Other Staging Studies
Other studies performed in special circumstances or for clinical trials
Bone marrow aspirate/biopsy
– Involvement in patients with advanced disease rarely changes treatment recommendation
Imaging Studies (CT scans)
– Generally of modest utility and rarely positive in early T1 or T2 disease
– Reserved for patients with Sézary syndrome or for quantifying disease stage in patients with tumor stage and palpable adenopathy
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Differential Diagnosis of MF
It is important to distinguish between MF and other T-cell disorders involving the skin
– CD30+ cutaneous large T-cell lymphoma
– CD30- cutaneous large T-cell lymphoma
– Peripheral T-cell lymphoma (unspecified)
– Lymphomatoid papulosis
– Subcutaneous panniculitis-like T-cell lymphoma
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
WHO/EORTC Classification of Primary CTCL
Willemze R, et al. Blood. 2005;105:3768-3785.
CTCL, NK-cell Lymphomas
MF/MF variants and subtypes
Folliculotropic MF Pagetoid reticulosis Granulomatous slack skin
Sézary syndrome
Adult T-cell leukemia/lymphoma
Primary cutaneous CD30+ lymphoproliferative disorders Primary cutaneous anaplastic large cell lymphoma Lymphomatoid papulosis
Subcutaneous panniculitis-like T-cell lymphoma
Extranodal NK/T-cell lymphoma, nasal type
Primary cutaneous peripheral T-cell lymphoma, unspecified Primary cutaneous aggressive epidemiotropic CD8+ T-cell lymphoma (provisional) Cutaneous γ/δ T-cell lymphoma (provisional) Primary cutaneous CD4+ small/medium-sized pleomorphic T-cell lymphoma (provisional)
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Pathogenesis of MFSkin homing T cells

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Membrane Proteins of the Malignant T Cell
CD3 and T-cell receptor
CD4 (TH 2 subtype)
CD45RO (Memory T Cell)
CLA (Cutaneous Lymphoid Antigen)
LFA-1
CD26 (-)/(+)
CD25 (+)/(-)CD7 (-)/(+)
CCR4
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
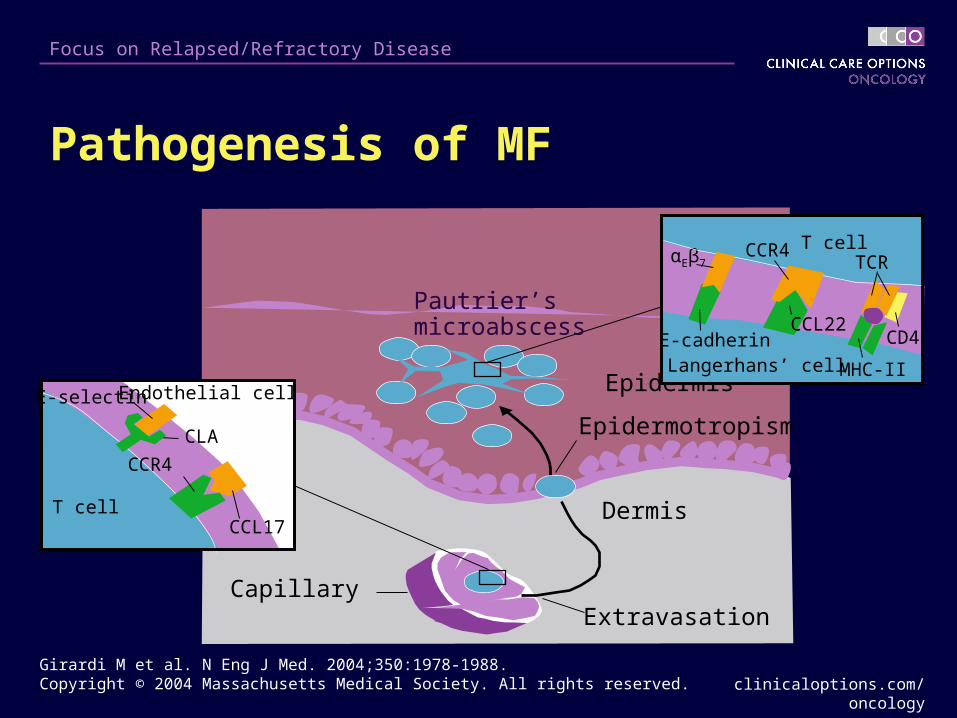
Pathogenesis of MF
Girardi M et al. N Eng J Med. 2004;350:1978-1988. Copyright © 2004 Massachusetts Medical Society. All rights reserved.
Epidermotropism
CapillaryExtravasation
Epidermis
Pautrier’s microabscess
Dermis
CLA
CCL17
Endothelial cell
CCR4
E-selectin
T cell
T cell
Langerhans’ cell
TCRαEβ7CCR4
MHC-II
CCL22CD4E-cadherin

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
CTCL: Prognostic Groups
Low-risk group (most favorable): TNM stages IA, IB, IIA.
– Survival: ~ 12 years
Intermediate risk group: TNM stages IIB, III, IVA with grade LN3 lymph node histopathology
– Survival: ~ 2-3 years
High-risk group (least favorable): TNM stage IVB, IVA with grade 2 years LN4 lymph node histopathology
– Survival: ~ < 2 years
Foss FM, Sausville EA. Hematol Oncol Clin North Am. 1995;9:1011-1019.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
CTCL: Skin-Directed Therapy
Topical steroids
Topical nitrogen mustard (NM)
– Mechlorethamine
Topical bexarotene gel
Topical carmustine
Phototherapy
– NBUVB
– PUVA
Radiotherapy
– Total skin EBRT
– Localized EBRT
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
CTCL: Systemic Therapy
Tretinoin capsules
Bexarotene capsules
Acitretin capsules
Methotrexate
Prednisone/chlorambucil
Interferon
Extracorporeal photochemotherapy
Other biologic modifiers
Denileukin diftitox
Combination chemotherapy

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
CTCL Treatment Algorithm
Stage IA Stage IB, IIA Stage IIB Stage III Stage IVA, B
Denileukin Diftitox
Electron Beam
Photopheresis ± IFN ± Bex
Photopheresis
UVB
Topical corticosteroids (Class I)
Bexarotene gel
PUVA (± IFN or ± Retinoid)
Nitrogen Mustard
Bexarotene capsules
Chemotherapy or AlloSCT
Chemotherapy or AlloSCT

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
CTCL: Topical Therapies

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Topical Nitrogen Mustard for MF
Mechanism of action: DNA alkylation, possible delayed type hypersensitivity (TH1) response
Aqueous or ointment base, applied to skin once daily
– Continue for 2-3 months after CR (longer maintenance does not decrease relapse rate)
Efficacy in patch/plaque stage MF
– T1 (n = 107) OR 93%; CR 65%; 5-year relapse free rate, 52%
– T2 (n = 88) OR 72%; CR 34%; 5-year relapse free rate, 19%
Kim YH. Dermatol Ther. 2003;16:288-298.Kim YH, et al. Arch Dermatol. 2003;139:165-173.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Topical Nitrogen Mustard for MF
Adverse effects
– Irritant dermatitis < 25% (ointment)
– Allergic contact dermatitis < 66% (aqueous), < 10% (ointment)
– No systemic absorption
– Possible slight increase in nonmelanoma skin cancers
Kim YH. Dermatol Ther. 2003;16:288-298.Kim YH, et al. Arch Dermatol. 2003;139:165-173.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Topical Bexarotene for MF
Mechanism of action: Specific retinoid X receptor ligand that influences critical pathways for cell proliferation, differentiation, and apoptosis
Formulation: 1% gel, applied to affected skin, 1-2 cm margins
– Applied every other day first week, once daily second week, up to 4 times daily as tolerated
Adverse effects
– Irritant “retinoid” dermatitis, 70%– Intervene with dose reduction, mildly potent topical steroids
Zhang C, Duvic M. Dermatol Ther. 2003;16:322-330.Kempf W, et al. Hematol Oncol Clin N Am. 2003;17:1405-1419.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
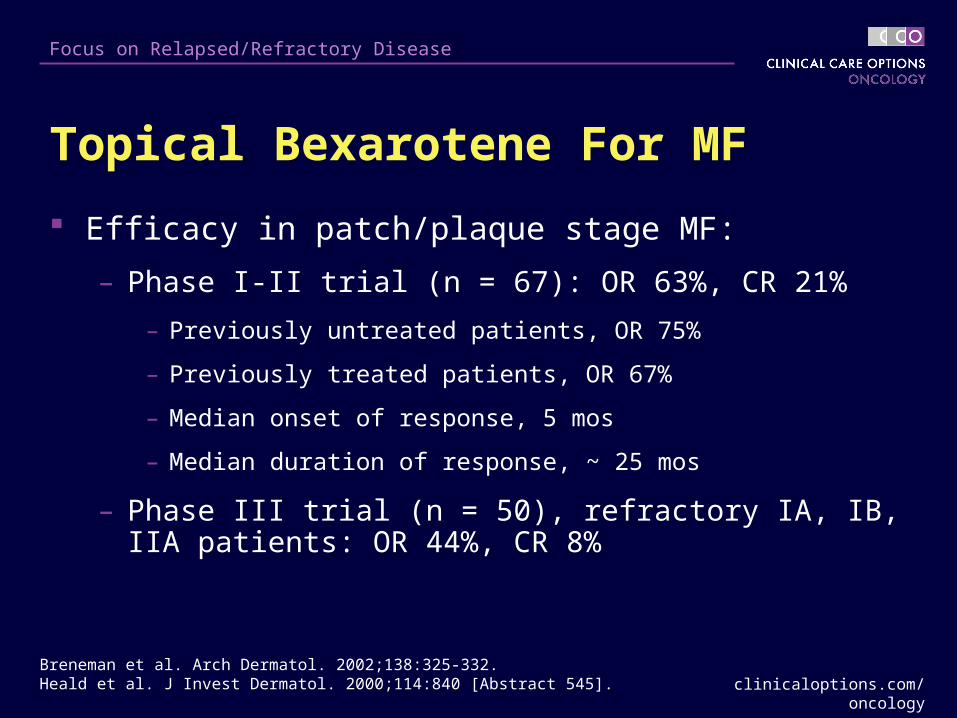
Topical Bexarotene For MF
Efficacy in patch/plaque stage MF:
– Phase I-II trial (n = 67): OR 63%, CR 21%
– Previously untreated patients, OR 75%
– Previously treated patients, OR 67%
– Median onset of response, 5 mos
– Median duration of response, ~ 25 mos
– Phase III trial (n = 50), refractory IA, IB, IIA patients: OR 44%, CR 8%
Breneman et al. Arch Dermatol. 2002;138:325-332.Heald et al. J Invest Dermatol. 2000;114:840 [Abstract 545].

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Phototherapy for MF
Mechanism of action: induction of T-cell apoptosis, possibly Langerhans’ cell apoptosis
– Wide-band UVB (WBUVB)
– Narrow-band UVB (NBUVB)
– Psoralens + UVA = PUVA
Baron ED, Stevens SR. Dermatol Ther. 2003;16:303-310.
UVAUVB
290 nm 320 nm 400 nm
Narrow-band UVB311 nm
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
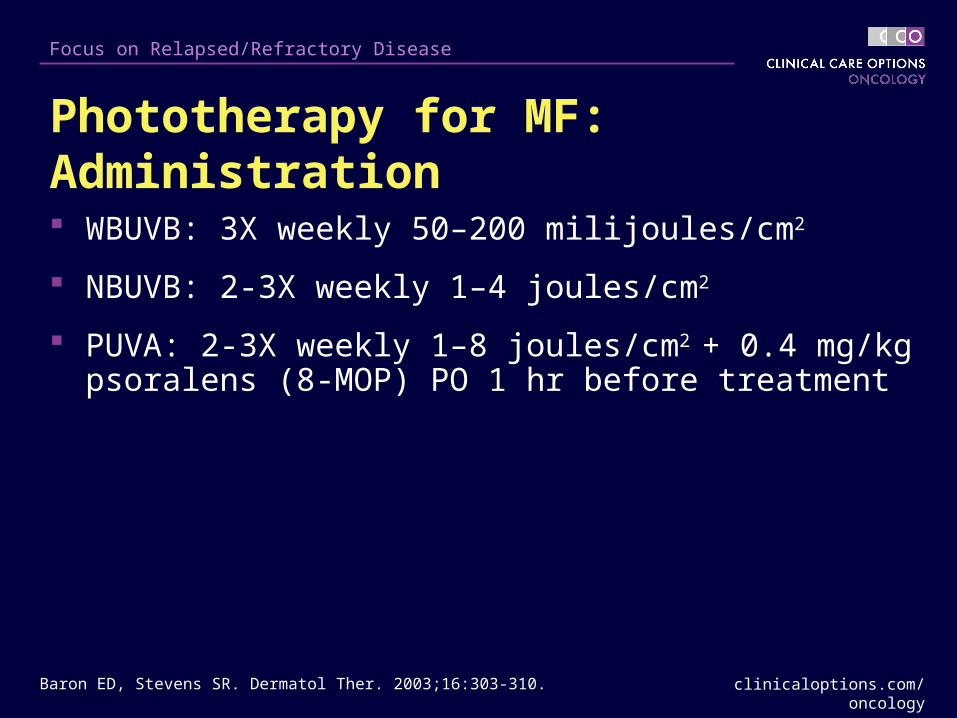
Phototherapy for MF: Administration
WBUVB: 3X weekly 50–200 milijoules/cm2
NBUVB: 2-3X weekly 1–4 joules/cm2
PUVA: 2-3X weekly 1–8 joules/cm2 + 0.4 mg/kg psoralens (8-MOP) PO 1 hr before treatment
Baron ED, Stevens SR. Dermatol Ther. 2003;16:303-310.

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
PUVA in MF
Efficacy
– IA: 54/60 (90% CR), 31% relapse
– IB: 88/116 (76% CR), 56% relapse
– IIA: 7/9 (78% CR), 71% relapse
– III: 11/18 (61% CR), ~ 100% relapse
Adverse Effects
– Phototoxic sunburn reactions
– Nausea from ingested psoralens
– Increased risk SCC > BCC (8% to 10% with PUVA)
– Increased risk of melanoma (seen in psoriasis pts treated with PUVA 15 years after first exposure)
Baron ED, Stevens SR. Dermatol Ther. 2003;16:303-310.Herrmann JJ, et al. J Am Acad Dermatol. 1995;33:234-242.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
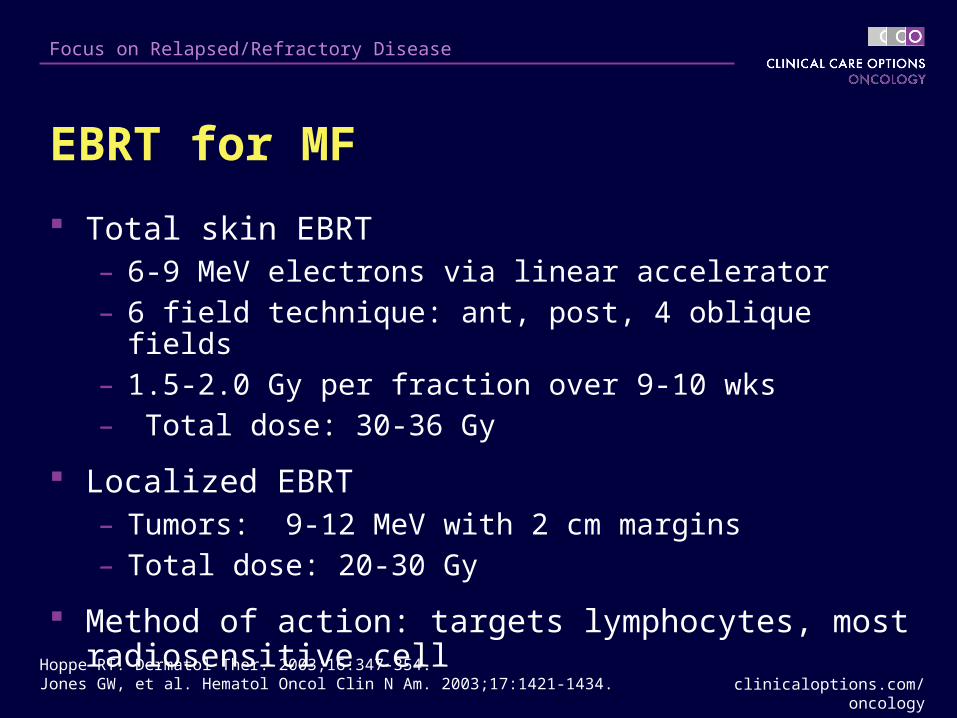
EBRT for MF
Total skin EBRT– 6-9 MeV electrons via linear accelerator– 6 field technique: ant, post, 4 oblique fields– 1.5-2.0 Gy per fraction over 9-10 wks– Total dose: 30-36 Gy
Localized EBRT– Tumors: 9-12 MeV with 2 cm margins– Total dose: 20-30 Gy
Method of action: targets lymphocytes, most radiosensitive cell
Hoppe RT. Dermatol Ther. 2003;16:347-354.Jones GW, et al. Hematol Oncol Clin N Am. 2003;17:1421-1434.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
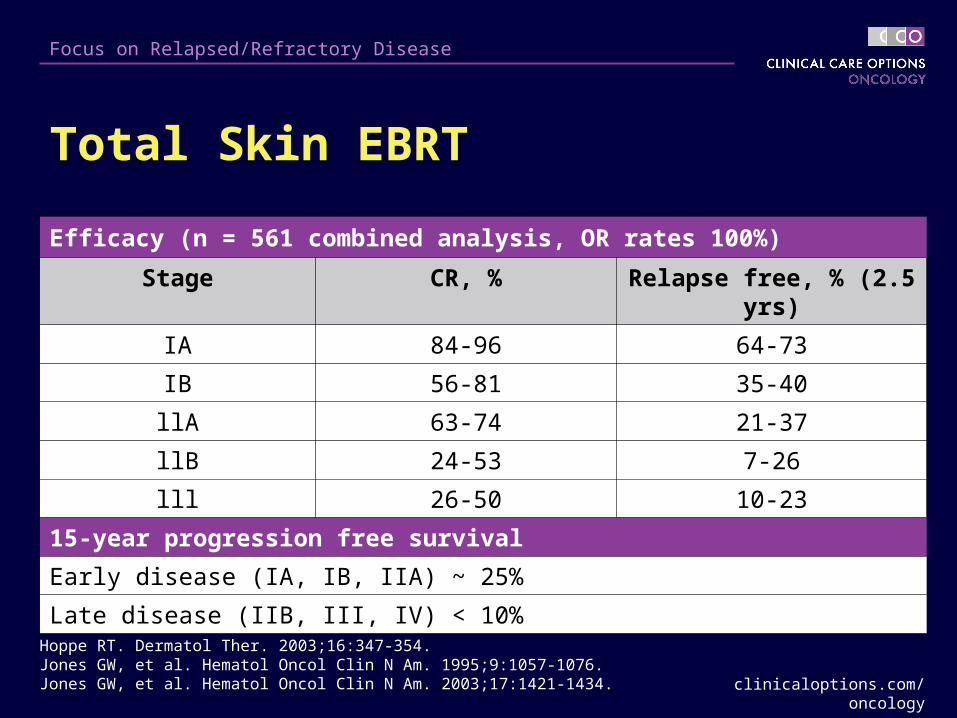
Total Skin EBRT
Hoppe RT. Dermatol Ther. 2003;16:347-354.Jones GW, et al. Hematol Oncol Clin N Am. 1995;9:1057-1076.Jones GW, et al. Hematol Oncol Clin N Am. 2003;17:1421-1434.
Efficacy (n = 561 combined analysis, OR rates 100%)
Stage CR, % Relapse free, % (2.5 yrs)
IA 84-96 64-73
IB 56-81 35-40
llA 63-74 21-37
llB 24-53 7-26
lll 26-50 10-23
15-year progression free survival
Early disease (IA, IB, IIA) ~ 25%
Late disease (IIB, III, IV) < 10%
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Total Skin EBRT
Adverse effects
– Acute skin effects: burning erythema, edema
– Chronic skin effects: xerosis, superficial atrophy, telangiectasia, dyspigmentation
– Alopecia, loss of nails (usually regrow)
– Heat intolerance due to the suppression of sweat gland production (usual duration, 6-12 mos)
– Increased SCC and BCC
– Other therapies may play a role
Hoppe RT. Dermatol Ther. 2003;16:347-354Jones GW, et al. Hematol Oncol Clin N Am. 2003;17:1421-1434.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
CTCL: Systemic Therapies

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Oral Retinoids for MF/Sézary Syndrome Specific retinoid receptor ligands that influence critical
pathways for cell proliferation, differentiation, and apoptosis
Retinoid Daily Dose
Acitretin 25-50 mg/d
Bexarotene* 300 mg/m2 BSA/day
Isotretinoin 1 mg/kg/d
* FDA-approved for CTCL in December 1999
Zhang C, Duvic M. Dermatol Ther. 2003;16:322-330.Kempf W, et al. Hematol Oncol Clin N Am. 2003;17:1405-1419.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
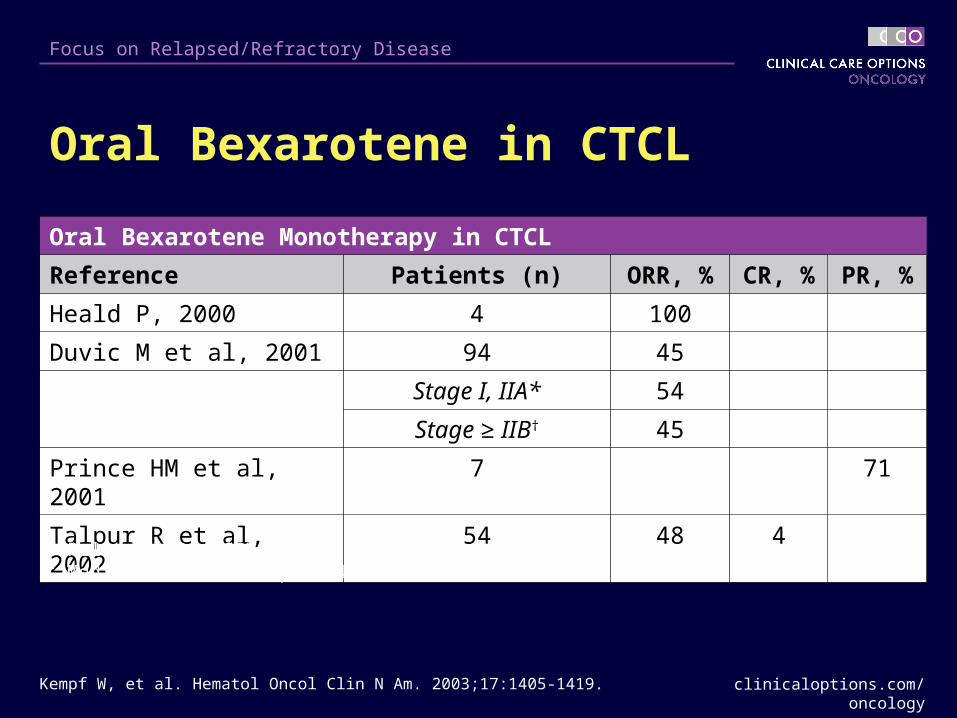
Oral Bexarotene in CTCL
Oral Bexarotene Monotherapy in CTCL
Reference Patients (n) ORR, % CR, % PR, %
Heald P, 2000 4 100
Duvic M et al, 2001 94 45
Stage I, IIA* 54
Stage ≥ IIB† 45
Prince HM et al, 2001 7 71
Talpur R et al, 2002 54 48 4
* Relapse rate: 28%† Median time to relapse: 43 weeks
Kempf W, et al. Hematol Oncol Clin N Am. 2003;17:1405-1419.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
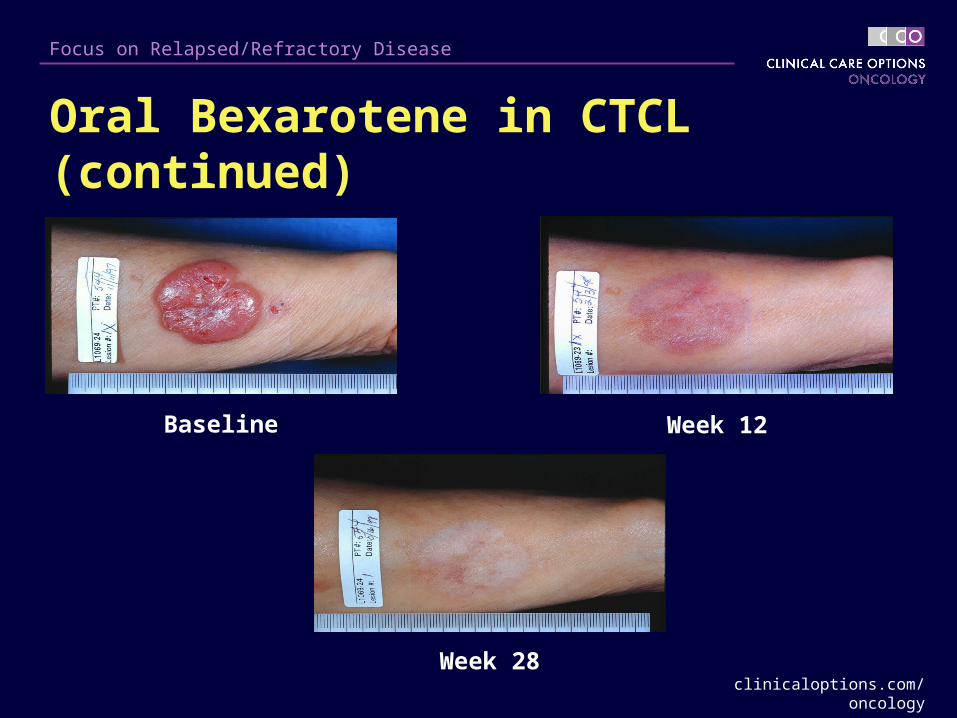
Oral Bexarotene in CTCL (continued)
Baseline Week 12
Week 28

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Oral Bexarotene for MF/Sézary Syndrome Adverse effects: hyperlipidemia (> 80%): usually requires
treatment with lipid lowering agent
– Triglyceride level of 700-900 mg/dL in patients on treatment warrants therapy interruption for 5-7 days
– Addition of lipid-lowering agent; resume therapy at half initial dose, monitor triglycerides once weekly thereafter
– Initiation of lipid-lowering agent recommended 1 week before starting oral bexarotene
– Diet: reduction of fat/sugar intake
– Initiating with low-dose bexarotene feasible in some patients (eg, those with diabetes)
Zhang C, Duvic M. Dermatol Ther. 2003;16:322-330.Kempf W, et al. Hematol Oncol Clin N Am. 2003;17:1405-1419.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Oral Bexarotene for MF/Sézary Syndrome Other adverse effects:
– Leukopenia (11%)
– Central hypothyroidism (30% to > 70%): may require thyroid supplementation
– Gemfibrozil contraindicated
Zhang C, Duvic M. Dermatol Ther. 2003;16:322-330.Kempf W, et al. Hematol Oncol Clin N Am. 2003;17:1405-1419.

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Stage IV Disease/Sézary Syndrome

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Sézary Syndrome
Characterized by erythroderma, circulating Sézary cells, adenopathy
– Secondary characteristics: alopecia, onychodystrophy, palmar/plantar keratoderma
EORTC suggests: TCRR (+) peripheral blood, CD4/CD8 > 10 for diagnosis of Sézary syndrome.
Prognosis poor: median survival, < 20-36 mos
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
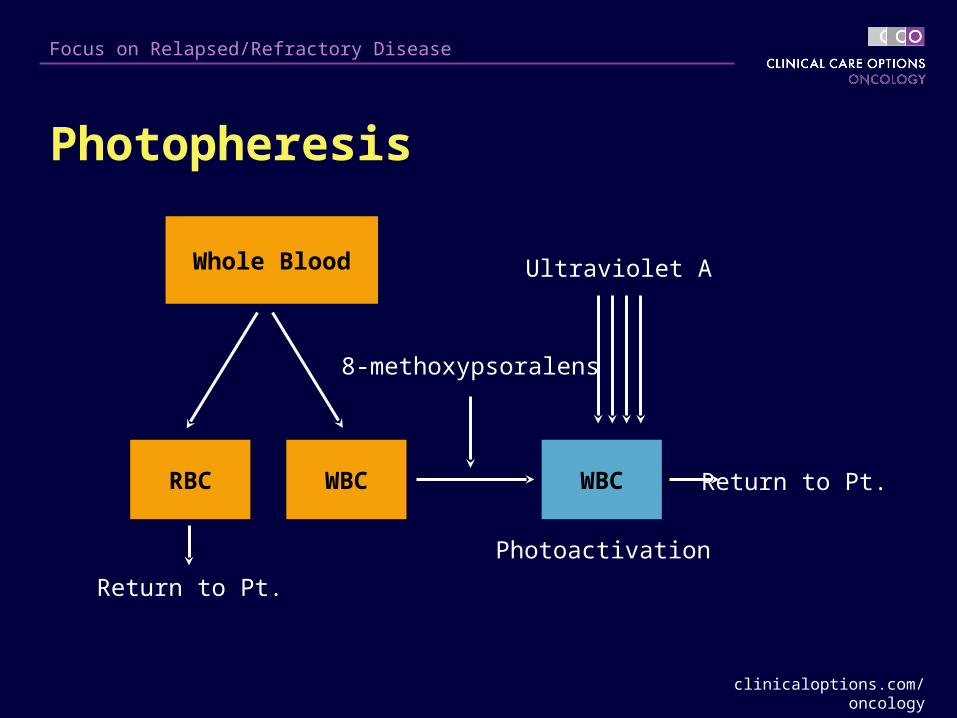
Photopheresis
Whole Blood
RBC WBC WBC
8-methoxypsoralens
Ultraviolet A
Photoactivation
Return to Pt.
Return to Pt.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Photopheresis for MF/Sézary Syndrome CTCL protocol: one 3-hour treatment on 2 consecutive
days, every 4 weeks
Proposed mechanism of action
– Induces apoptosis of lymphocytes
– Converts monocytes to immature dendritic cells
– Dendritic cells engulf lymphocytes and present tumor antigen to cytotoxic T cells
Zic JA. Dermatol Ther. 2003;16:337-346.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
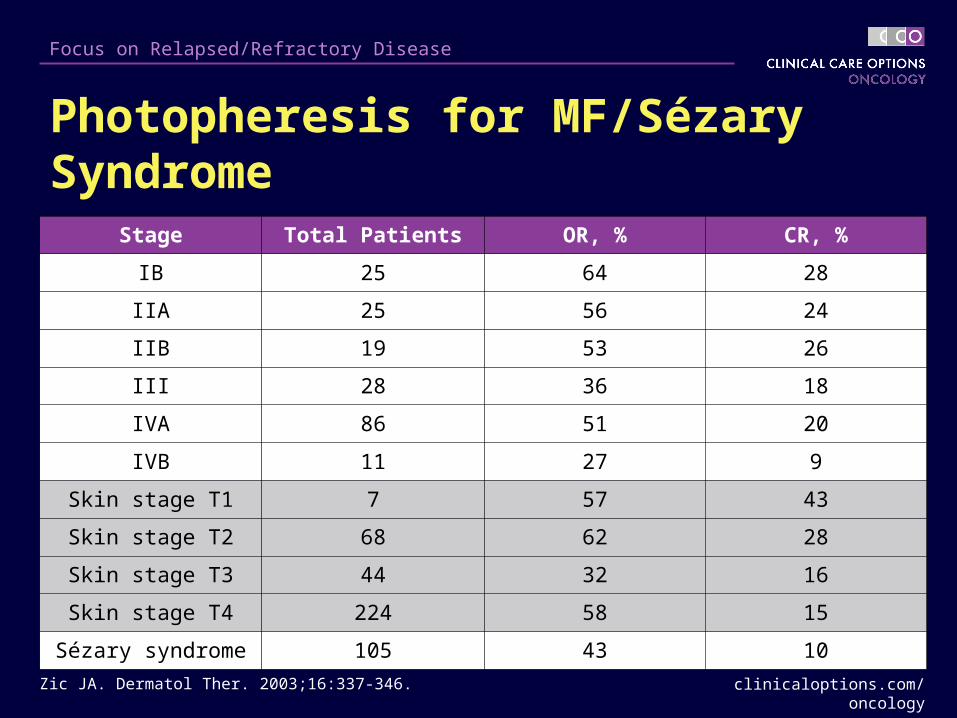
Photopheresis for MF/Sézary Syndrome
Stage Total Patients OR, % CR, %
IB 25 64 28
IIA 25 56 24
IIB 19 53 26
III 28 36 18
IVA 86 51 20
IVB 11 27 9
Skin stage T1 7 57 43
Skin stage T2 68 62 28
Skin stage T3 44 32 16
Skin stage T4 224 58 15
Sézary syndrome 105 43 10
Zic JA. Dermatol Ther. 2003;16:337-346.
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Denileukin Diftitox for CTCL
Diphtheria toxin fragments A and B linked to interleukin-2
– Approximately 50% CTCL tumor cells express interleukin-2 receptor
Pivotal study (N = 71) in pretreated patients, most with stage IIB-IVB disease (63%)
– 30% overall response
– Median duration of response, 4 mos
Olsen E, et al. J Clin Oncol. 2001;19:376-388.

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Denileukin Diftitox for CTCL: Adverse Events
Olsen E, et al. J Clin Oncol. 2001;19:376-388.Foss FM et al. Clin Lymphoma. 2001;4:298-302.
Acute hypersensitivity reactions (69%): acute; hypotension, SOB, rash, chest pain
– Pretreatment with steroids may improve tolerability, maintain response
Vascular leak syndrome (27%): delayed;hypotension, edema, hypoalbuminemia
Infections (48%)
Lymphopenia (34%)
clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Chemotherapy for CTCL
Modest response, reserved for relapsed or refractory disease
Duration of response < 6 mos
Some agents show notable activity:
– Deoxycoformycin
– Gemcitabine: phase II trial (N = 32) untreated CTCL, 7 (22%) CR, 17 (53%) PR
– Pegylated liposomal doxorubicin: retrospective analysis (N = 34) CTCL patients,15 CR (DFS 13.3 mo), 15 PR
Kuzel TM. Dermatol Ther. 2003;16:355-361.Pichardo DA, et al. Leuk Lymphoma. 2004;45:1755-1765.Marchi E, et al. Cancer. 2005;104:2437-2441.Wollina U, et al. Cancer. 2003;98:993-1001.

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Allogeneic Peripheral Stem Cell Transplant for CTCLReference Patients
(age, yrs)Conditioning
RegimenGVHD
prophylaxisOutcome
Soligo 2003
N = 3 (51-60) Fludarabine, TBI CSA, MMF 3 CR: 18 and 24 mo, 1 dead
d+73
Molina 2003, 2005
N = 8 (21-59) Fludar/Melph n = 4Cyclophos/TBI n = 3Cyclophos/Busulfan
CSA n = 8MTX n = 4MMF n = 6
8 CR: 6 alive (33-106 mo), 2 dead (sepsis)
Guitart 2002
N = 3 (27-39) Cyclophos/Mesna, TBI
CSA, steroid, +/- MMF
3 CR: 15, 52, 60 mo
Masood 2002
N = 1 (37) Cyclophos, TBI MTX, CSA CR: 24 mo
Koeppel 1994
N = 1 (21) Cyclophos, TBI MTX, CSA, steroid
CR: 72 mo
Pichardo DA, et al. Leuk Lymphoma. 2004;45:1755-1765.

clinicaloptions.com/oncology
Focus on Relapsed/Refractory Disease
Summary of Therapies for CTCL
Skin-directed therapies: highly effective in the early stages of MF
– Relapses common
The challenge: develop systemic targeted therapies with minimal adverse effects capable of inducing meaningful remissions
Current therapeutic goal: do no harm, prevent disease progression
Comparison trials needed to prioritize systemic therapy

















