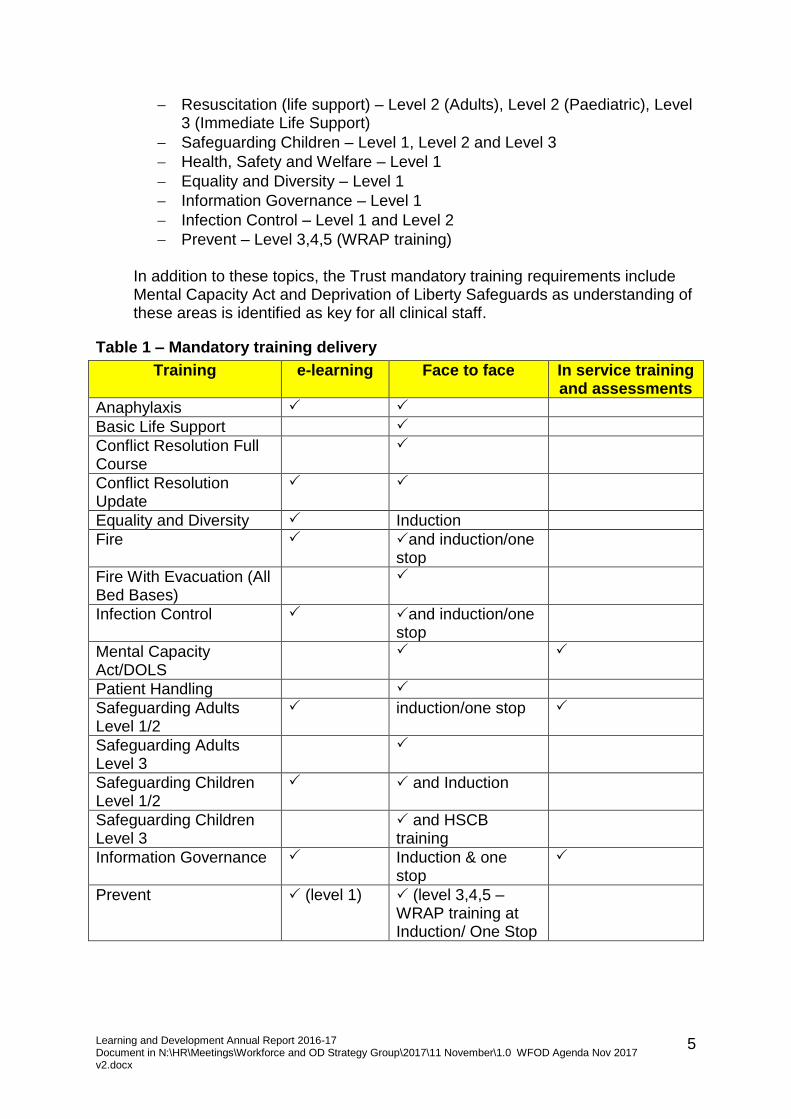
Board: 30 th November 2017 Attachment K0 1 TRUST BOARD Meeting Date: 30 th November 2017 Title: Supporting Papers Available electronically on the website at https://www.hct.nhs.uk/about-us/our-board/meeting-papers/ Executive Lead: Various Author(s): Various For: Noting The Board is requested to note the following supporting papers which are for information only and which are referenced in Executive Directors’ Reports. Lead Agenda Link Title & Category Attachment Clinical Services & Healthcare Governance PW AM B2 (i) B3 (i) Quality Report Q2 Minutes of the Healthcare Governance Committee meeting held on 19 th September 2017 K1 K2 Operations and Performance PB C2 (i) Integrated Board Performance Report (October 2017) K3 Strategy, Resources and Engagement PB DE CH D2 (i) D3 (i) D5 (i) Month 7 Finance Report (October 2017) Learning and Development Annual Report Appendices to the Hertfordshire Health Concordat. App 1 Background App 2 Consultation Principles App 3 HSC Substantial variation guidance App 4 Checklist App 5 Signatories K4 K5 K6
Transcript
Board: 30th November 2017 Attachment K0
1
TRUST BOARD Meeting Date: 30th November 2017 Title: Supporting Papers Available electronically on the website at https://www.hct.nhs.uk/about-us/our-board/meeting-papers/ Executive Lead: Various Author(s): Various For: Noting The Board is requested to note the following supporting papers which are for information only and which are referenced in Executive Directors’ Reports. Lead Agenda
Link Title & Category Attachment
Clinical Services & Healthcare Governance PW AM
B2 (i) B3 (i)
Quality Report Q2 Minutes of the Healthcare Governance Committee meeting held on 19th September 2017
'To maintain and improve the health and wellbeing of the people of Hertfordshire and other areas served by the Trust'
Quality Report
Quarter 2 – 2017/18
Board 30th November 2017 Attachment K1
2
CONTENTS
Achievements ....................................................................................................................................................................... 3 Challenges ............................................................................................................................................................................. 3 Quality Dashboard ................................................................................................................................................................ 4 CQUINs/Quality Priorities ..................................................................................................................................................... 5 Risk Register .......................................................................................................................................................................... 6 Care Quality Commission ...................................................................................................................................................... 6 Quality Assurance Visits ........................................................................................................................................................ 6 Patient Safety Incidents ........................................................................................................................................................ 9 Medication Incidents .......................................................................................................................................................... 10 Serious Incidents and Local Investigations ......................................................................................................................... 11 Safer Care (Safety Thermometer, Falls and Pressure Ulcers) ............................................................................................. 13 Mortality Review Group ..................................................................................................................................................... 15 Medical Revalidation .......................................................................................................................................................... 16 Infection Prevention and Control ....................................................................................................................................... 16 Children and Adult Safeguarding ........................................................................................................................................ 17 Looked After Children and Care Leavers ............................................................................................................................ 19 Whistleblowing / Raising Concerns .................................................................................................................................... 19 Patient Surveys ................................................................................................................................................................... 21 Patient Stories ..................................................................................................................................................................... 21 Friends and Family Test ...................................................................................................................................................... 22 Complaints and Compliments ............................................................................................................................................. 22 2017 Patient Led Assessment of the Care Environment (PLACE) Programme ................................................................... 24 Learning Disabilities ............................................................................................................................................................ 26 Carers .................................................................................................................................................................................. 26 CCG/GP Hotline Enquiries ................................................................................................................................................... 26 NICE Quality Standards and Guidance ................................................................................................................................ 27 Clinical Audit ....................................................................................................................................................................... 28 Medicines Management ..................................................................................................................................................... 32 Public Health Metrics .......................................................................................................................................................... 32 Claims .................................................................................................................................................................................. 36 Coroners’ Inquests .............................................................................................................................................................. 36 Appendix 1: Keeping in Touch visits ................................................................................................................................... 37 Appendix 2: Quality Assurance Visit Action Plan - Antenatal and newborn screening service .......................................... 38 Appendix 3: Safeguarding Children Dashboard Q2 ............................................................................................................ 42 Appendix 4: Safeguarding Adult Dashboard Q2 ................................................................................................................. 43 Appendix 5: Carers – actions to date .................................................................................................................................. 44 Appendix 6: Results of Carers’ survey ................................................................................................................................ 45
Board 30th November 2017 Attachment K1
3
Q2 ACHIEVEMENTS AND CHALLENGES Achievements
Challenges
ACHIEVEMENTS There was a decrease in the percentage of reported patient safety
incidents resulted in harm – 44% in Q2 compared to 57% in Q1 The number of avoidable category 2 to 4 pressure ulcers has reduced HCT’s harm free care rate remains above the national benchmark at 97.85% HCT continues to maintain its Friends and Family Test score of 98% The results of the Patient Led Assessment of the Care Environment (PLACE)
demonstrated that HCT performed above the national average in all domains
Tricia Wren (Deputy Director of Q&G / Deputy Chief Nurse) and Sue Thompson (Named Nurse Safeguarding Children) were both awarded the accolade of Queen’s Nurse
4 out of 5 CQUINs are on trajectory to meet Q2 targets
CHALLENGES There was a small increase in the number of injurious falls in community
hospital wards HCT declared 4 SIs in Q2; these will be investigated through the SI process to
identify learning 1 case of E.coli blood stream infection was reported in Q2; RCA will be
undertaken to identify learning and good practice The quarterly target for 1 CQUIN has been partially met in Q2; a potential
risk relating to the staff health and wellbeing CQUIN has been identified due to current high level of organisational change and will be monitored via the Risk Register
The quarterly targets for 2 Quality Priorities have been partially met in Q2; actions are in place to bring these back on trajectory during Q3 and Q4
Areas for improvement were identified during internal peer review visits; areas identified include lack of staff awareness of policies and processes, and inconsistent practices
Board 30th November 2017 Attachment K1
4
Quality Dashboard
Board 30th November 2017 Attachment K1
5
QUALITY ASSURANCE
CQUINs/Quality Priorities
CQUINs
Title of CQUIN
On trajectory / not on trajectory /
met / not met Q1 Q2
Improving staff health and wellbeing On trajectory On trajectory1 Supporting proactive and safe discharge On trajectory On trajectory Preventing ill health by risky behaviours – alcohol and tobacco
On trajectory Partially met2
Improving the assessment of wounds On trajectory On trajectory Personalised care and support planning On trajectory On trajectory 1 Whilst the staff health and wellbeing CQUIN is currently on trajectory there is a risk that HCT will not meet Part 1 of this CQUIN, which relates to staff giving positive responses to specific questions in the Annual Staff Survey, due to the current high level of organisational change. 2 Whilst there has been an improvement in the number of inpatients screened for tobacco and alcohol use, and given brief intervention advice, the percentage improvement target has not been met in some elements. Targeted work will be undertaken with Ward Managers to ensure that patients are screened and that this is appropriately recorded. This will be monitored monthly by the Clinical Services Manager, and training provided where needed. Quality Priorities
Title of Quality Priority Met / partially met / not met
Q1 Q2 Supporting people with health conditions and disabilities to manage their own care as far as possible
Met (on trajectory) Partially met3
Supporting the population by developing patient-focussed outcomes to improve their health and wellbeing.
Met (on trajectory) Met (on trajectory)
Supporting Integrated Community Team patients with complex needs to be involved in their personalised care planning through the effective use of S1 care plans
Partially met Partially met4
Improving the safety of patients in our care by reducing avoidable pressure damage
Partially met Met (on trajectory)5 3 On trajectory in relation to staff training; however services have still to identify self-management ambassadors that have been trained in health coaching. Work to achieve this is ongoing 4 SystmOne care plan review not yet completed due to ICT service redesign work. All care plans will include a personalised planning component; question relating to personalised care planning added to Patient Experience survey. However, data not yet collated to support this measure; training on SystmOne care plans and associated tools commenced but not yet completed; data collected but not complete due to care plan review work. 5 Overall percentage of avoidable acquired PU is improving against target at 3.06%; number of Category 3 and 4 is higher than target; number of Category 2 is much lower than target; 60% of patients with avoidable PU receiving home care worker support; 20% in residential home care setting; highlight delayed reporting of early PU damage signs by carers to nursing staff
Board 30th November 2017 Attachment K1
6
Risk Register Risks are routinely reviewed at Senior Management team meetings with key risks and their management brought to the attention of the Executive team following Business Unit Performance Reviews. Risk owners review and update their risks at least every month, and the High-Level Risk Register is reviewed by the Executive Group on a monthly basis. At the end of Q2, there are 10 risks on the High Level Risk Register; 8 operational risks and 2 corporate risks. Themes identified are risks relating to staffing levels and vacancy rates, and re-commissioning of specialist services. Care Quality Commission Registration • The current registration status is ‘good’. The Statement of Purpose has been amended to note
transfer of Simpson Ward from WHHT to HCT. CQC Quality Improvement Plan • The action plan has been completed for main review • Assurance checks for each area continue and there is an improvement in consistency in practice;
these are supported by BUPR • The Simpson Ward Improvement Plan has been developed to support safe, effective practice with a
focus upon leadership • SystmOne changes and aligned training of staff has been completed to support electronic patient
records and effective timely clinical decision-making with patients and carers. Quality Assurance Visits External Quality Assurance Visits, internal peer reviews and Keeping in Touch (KiT) visits undertaken by HCT staff, stakeholders and Board members provide vital information about the quality of our services, identify any areas for improvement, and are an opportunity to engage with our staff and patients. Keeping in Touch (KiT) visits • There were 2 KiT visits undertaken in Q2 - to Simpson Ward, Hemel Hempstead and to the Diabetes
Service • During Q3, Non-Executive Board members will be invited to take part in further Quality Assurance
peer review visits, thus there are no planned KIT visits. Main themes: • Follow up to ensure all staff complete HCT induction, expected behaviours, appraisal and leadership • Planned estate works are completed to support effective medicines management • Diabetic triage and referral , IM&T access, clarification for consultant working, noted a supportive
Clinical Manager. A full narrative relating to these visits is attached as Appendix 1.
Board 30th November 2017 Attachment K1
7
Staff engagement events • A ‘Listening To You’ event was held by the Director of HR and Workforce OD at Herts & Essex
Hospital. • An Afternoon Tea event was held, providing support to newly appointed staff Band 6 and above, and
to understand their experience of working within the Trust three months after appointment. External Quality Assurance Visits During Q2, 3 external visits were undertaken in HCT services • Public Health England Screening carried out a quality assurance visit to the Antenatal and Newborn
Screening Service in July, including the Central Midlands South Child Information and health visiting services provided by HCT
• E&N CCG carried out a visit to Herts and Essex Hospital community hospital ward in September • The CQC also carried out a thematic review into the PALMS service (Positive Behaviour, Autism,
Learning Disability and Mental Health Service for children and young people) in September. Areas of good practice
Antenatal and Newborn Screening Service
• A comprehensive risk strategy and risk management policy, which is used to inform service developments and delivery
• Clear internal governance structures and escalation processes • A standard operating procedure detailing sickle cell counselling
competencies for health visitors, which reflects NHS Screening Programme requirements
Herts and Essex Community Hospital Ward
• The unit was calm and organised • High and low level cleaning was good • Patient feedback throughout the unit was positive - caring staff,
OT/physio staff supportive and food good PALMS Service – formal report not yet received
• Initial feedback overwhelmingly positive • Strong, committed, skilled and passionate team
Area requiring improvement identified / actions taken
Antenatal and Newborn Screening Service
• Review of policy and standardisation of operational and communication processes
• Completion of SystmOne and data reconciliation workstreams • Audit of recording and monitoring systems The full QAV Action Plan is attached as Appendix 2
Herts and Essex Community Hospital
No improvement actions were identified
PALMS Service The formal report is awaited. Internal Peer Reviews • The final ICT visit was carried out in July, which was into the Stort Valley ICT team • A visit was carried out on Simpson Ward on 24 August following the transfer of the ward on 1 August
2017 • Five visits were carried out in August and September to the FIRST Team, accompanying staff on visits
to patients’ homes. Areas of good practice
Stort Valley ICT Team • All patients spoken to reported that they had been treated with respect, compassion and dignity
Board 30th November 2017 Attachment K1
8
• Learning from incidents, complaints and feedback is routinely shared across the team
• All staff spoken to were aware of the reporting process for suspected safeguarding issues
Simpson Ward • NEWS observation charts and escalation charts completed appropriately • Call bells answered promptly • Drug storage procedures being followed appropriately
FIRST Team • All patients spoken to on the visits reported that they had been treated in a respectful, caring, discreet way and that the staff visiting them were informed
• All staff spoken to were aware of who to contact if they had any concerns about a patient
Areas requiring improvement identified / actions taken
Stort Valley ICT Team • Not all staff recorded the visit directly onto SystmOne before leaving the patient
• Not all staff were aware of the lone worker policy • Not all staff were aware of the process for booking an interpreter • Not all staff were aware of their service risks • Not all staff felt supported by the management team
Simpson Ward • One patient with an indwelling catheter did not have a catheter passport • Some staff not using personal protective equipment appropriately • Some estates issues relating to the fabric of the building and also some
ward equipment • Room temperature of medicines storage room above temperature – air
conditioning unit fitted but not yet connected • Drug tabards not in use
FIRST Team • Not all staff had attended an induction session • Not all staff were compliant with HCT uniform policy • Not all staff were bare below the elbows • Not all staff had a kit bag for carrying equipment into the patients’ homes
Board 30th November 2017 Attachment K1
9
CONSISTENT AND IMPROVING PATIENT SAFETY
Patient Safety Incidents Incidents During Q2 1243 patient safety incidents were reported.
559 incidents resulted in harm and are broken down as follows:
Q1 Q2 Low harm 692 500 Moderate harm 59 57 Severe harm 0 2 Death *1 0 Total number of incidents resulting in harm
752 (57%) 559 (44%)
Total number of incidents reported
1308 1243
*In Q1, the incident resulting in death occurred in HMP The Mount and was investigated under HCT’s SI process
Themes and trends of all incidents The 10 most-reported types of all incidents reported during Q2 are detailed below:
Equality characteristic group information The percentage of Datix incidents which include equality characteristic group information is outlined below:
399
124 113 93 72 69 57 55 51 42
100% 99.5% 94% 86%
53%
Gender Race Age Disability Religion orbelief
Board 30th November 2017 Attachment K1
10
Central Alert System During Q2 a total of 32 CAS alerts were received within HCT; 23 of these were not applicable to HCT, 6 were applicable to HCT, 3 are awaiting confirmation of applicability, and 2 were cascaded for information only. Q1 Q2 Total number of CAS alerts applicable to HCT
3 6
Number of CAS alerts disseminated, actions completed and alert closed
2 Closed within
timescales 6
Closed within timescales
Number disseminated, actions on going and alert remains open
1 On trajectory to close
within timescales 0
CAS alerts received are detailed by category below:
Medication Incidents
During Q2 there were 111 medication-related incidents reported.
During Q2 two incidents resulted in moderate harm, as follows: • A palliative care patient was discharged from the acute hospital into community with insufficient
pain relief prescribed in SC syringe pump, leading to an increased request for pain relief by patient. The patient had previously been on fentanyl patches but was not discharged with these. Further advice was taken from Hospice palliative care consultant and the syringe pump dose of pain relief was increased.
• An incorrect dose of insulin was administered to a patient, resulting in hospital admission for further
119
11 0 0
111
2 2 0
Total number of medicationincidents
Total number of medicationincidents resulting in low
harm
Total number of medicationincidents resulting in
moderate harm
Total number of medicationincidents resulting in severe
harm
Q1
Q2
14
10
5 3
Medical Devices Estates & Facilities Drug Alerts Patient Safety Alerts
Board 30th November 2017 Attachment K1
11
observation. The patient was well on discharge the following day. Serious Incidents and Local Investigations Serious incidents There were a total of 4 SIs reported in Q2:
SIs are detailed by category below:
Q1 Q2 Slips/trips/falls meeting SI criteria
2 2
Pressure ulcers meeting SI criteria
0 1
Death in custody 1 0 Treatment delay 0 1
On completion, each SI report will be reviewed at the Serious Incident Assurance Panel to provide assurance of evidence of actions taken to address concerns identified and that changes have been embedded in practice. Themes and learning from SIs
1. A patient presented with left knee pain which did not resolve despite continued reassessment of the knee, assessment of the hip joint was not considered for some time, however the patient was eventually diagnosed with a fractured neck of femur 2. A patient had an unwitnessed fall. The Extended Falls Assessment was not completed by therapy staff as expected
1. Patients with non-resolving and undiagnosed pain should have x-rays of the joints above and below the presenting complaint to rule in/out referred pain form undiagnosed fracture. 2. A process will be put in place to ensure that the Extended Falls Assessment template is used by therapy staff when required and records will be spot checked to ensure that this is being completed.
1. A LD patient was not assessed as staff felt he was able to consent to treatment however had not considered his ability to weigh up and understand information. 2. A patient with cognitive impairment did not have a MCA completed when making unwise decisions which may have prompted staff to offer the patient more support.
1. All patients who are admitted to a community hospital will have MCA considered to ensure effective care is delivered. 2. Staff on the unit will have their MCA competencies reassessed and a review of a cohort of patients records to ensure that MCAs are being completed appropriately.
MORSE completion
MORSE score was calculated incorrectly for a patient throughout their stay (2 incidents).
A dip test of the records on the unit will be undertaken to identify poor practice, staff will be identified to review their competencies (2 incidents).
Equality characteristic group information
Local investigations There were a total of 9 locally investigated incidents reported in Q2: Locally investigation incidents are detailed by category below:
Q1 Q2 Information governance 1 0 Safeguarding allegations of neglect
Gender Age Disability Ethnicity/group Religion Sexual orientation
Female 80-84 Long standing health
condition Not stated Not Known Not Recorded
Male 35 - 39 None White British Not Recorded Not Recorded
Male 90+ Not Recorded Indian Not Recorded Heterosexual/Straight
Female 80-84 None White British Not known Heterosexual
4
9
Total
Q1
Q2
Board 30th November 2017 Attachment K1
13
Themes and learning from locally investigated incidents
Theme Commentary Outcomes/Learning Communication with other providers
A patient required non urgent transport at a weekend, due to changes in transport service provision the staff ended up calling a 999 ambulance.
The service manager has ensured that staff have transport service contact details available 24hrs a day.
Holistic care planning
A patient receiving subcutaneous (s/c) fluids did not have their care reviewed by the Doctor prior to a weekend leading to an unclear pathway for the patient over the weekend.
Staff will ensure that any patient on IV or s/c fluids has a medical review prior to a weekend to ensure that the plan of care is in place and clear to all staff.
IG processes A handover sheet was found in the car park with patient details- the process to destroy the sheet at the end of every shift was not followed.
All staff have been reminded to ensure that the processes are followed. Ward Managers will monitor the process to ensure that all staff are following.
Safer Care (Safety Thermometer, Falls and Pressure Ulcers) Safety Thermometer data (HCT average)
97.34% 97.85%
Harm free care in HCT
Safety Thermometer - harm free care
Q1
Q2
National benchmark - 95%
0.81%
1.03%
0.61%
0.20%
1%
1% 1%
0%
New pressure ulcers Falls with harm New catheter-associatedUTIs
New VTEs in a communityhospital
Safety Thermometer - 'new' harms
Q1
Q2
Board 30th November 2017 Attachment K1
14
Falls in community hospitals Four falls were classified as moderate or severe harm; all were sustained at PBCH. Due to the increasing number of falls at PBCH, a deep dive is being undertaken to identify themes and trends. Achievements • Rate of falls per 1000 Occupied Bed Days (OBD): during Q2 HCT reported an average of 6.03 falls per
1000 OBD against a national benchmark of 8.40 falls per 1000 OBD • Rate of injurious falls per 1000 OBD: during Q2 HCT reported an average of 2.34 injurious falls per
1000 OBD against a national benchmark of 2.58 falls per 1000 OBD. Areas of Improvement identified • Partnership working with other trusts: Strengthening the collaboration between HCT, ENHHT and
WHHT; HPFT has been invited to future meetings. Work includes: − sharing lessons from local investigations and /or serious incidents − review of trust leaflets and falls prevention advice to achieve consistency of information − developing a shared understanding of the definition of a fall
• Sensor mat SOP is now in use across the Community Hospitals. Implementation will be evaluated by audit by the end of Q3.
Falls Assessment Compliance • Audit of falls assessment compliance was undertaken of all community hospitals with an identified
falls champion on site during Q2 2017/18 • This demonstrated that on average 63% of patients were identified as being at high risk of falling
and that 76% of those patients had a tailored falls prevention plan in place • Falls Champions will implement actions to ensure falls prevention plans are in place for patients
assessed as being at high risk of falling • Re-audit Q3 2017/18
86
30
3 0
87
37
3 1
Total number offalls in community
hospitals
Total number ofinjurious falls in
communityhospitals
Number of fallscategorised as
resulting inmoderate harm
Number of fallscategorised as
resulting in severeharm
Q1
Q2
Board 30th November 2017 Attachment K1
15
Pressure ulcers There were 408 category 2 to 4 pressure ulcer incidents reported in Q2, representing 33% of all patient safety incidents reported in quarter. Of these, 9 were deemed to be avoidable. Avoidable pressure ulcers Achievements • The overall percentage of avoidable HCT acquired PU remains low at 2.2% of all pressure ulcer
incidents reported • 321 HCT staff from a wide range of disciplines and grades have received All About Pressure Ulcer
training at the bases since April 2017 • 3 RCA themes have been identified: delayed or missing risk and core assessments, discussions and
leading of care worker actions, managing non-concordance effectively. Areas requiring improvement identified / actions taken • Communication with carers by HCT staff to highlight risk and provide care guidance – raising
awareness of care home agreement and the need to guide careworkers • Educating carers to recognise early signs of PU damage and escalate – exploring React to Red
Campaign and contributing to HCPA training programme • Managing non-concordance – an information sheet and guidance has been produced which is being
reviewed by patients • Risk and core assessments to be undertaken as per Trust guidelines – to improve this further at the
base training will be delivered focusing on the 3 RCA themes. Mortality Review Group There were two deaths in HCT inpatient units in Q2. • Both patients were admitted to a HCT inpatient unit for end of life care, therefore the death was
6
0
2
0
Number of expected deaths in quarter Number of unexpected deaths in quarter
Q1
Q2
2
11
1
8
Avoidable category 2 PUs Avoidable category 3 and 4 PUs
Q1
Q2
Board 30th November 2017 Attachment K1
16
expected • A further patient became unwell and was transferred to an emergency unit by paramedics where
the patient sadly died. Although not expected on admission, given the prognosis the patient could have passed away within a 6 to 12 month timeframe.
Medical Revalidation • A further meeting of the HCT Decision Making Group took place in August 2017. Since the last
meeting processes are being embedded • The Medical Revalidation Officer is now in post • The Responsible Officer received input and advice from the group regarding concerns about
individuals and the relevant system issues are also being addressed.
Infection Prevention and Control
Healthcare Associated Infections (HCAI) • One case Of E.coli blood stream infection reported in Q2. No trajectory set. Root cause analysis (RCA)
undertaken to identify learning and good practice • One case of CDI reported in Q2, taking the total to 4 cases notified since April 2017. This exceeds the
monthly trajectory by 1 case. RCA undertaken in all cases and all put forward for appeal. • The CCG commended the Infection Prevention & Control Team on its completion of a robust RCA for
CDI case 4. Outbreaks of HCAI There were no outbreaks of HCAI reported in Q2. Achievements • Standardisation of skin and IV disinfectant products finalised for rollout October 2017 • New IV Standard Operating Procedure formulated • 100% of patient screened for MRSA on admission to community hospitals. Areas requiring improvement identified / actions taken • The Trust is working with the CCG and other providers to improve the assessment and management
of patients with a suspected urinary tract infection (UTI). Assessment tool to be developed into a SystmOne template
• Implementation of the foam mattresses/cushions SOP in community hospitals audited in September
3
0 0
1
0
1
Clostridium difficileinfections (CDI)
MRSA blood streaminfections (BSI)
E.coli blood streaminfections
Q1
Q2
Board 30th November 2017 Attachment K1
17
2017. Children and Adult Safeguarding Safeguarding Children Training and supervision Achievements • The first Safeguarding level 1 and 2 training workbook was cascaded widely throughout HCT in
Quarter 1; this has improved compliance significantly from 94% to 97%. The feedback to this alternative method of training has been positive and will be closely monitored
• Audit on Safeguarding Knowledge at the Leading Lights event in July 2017 resulted in 87% of the safeguarding knowledge quiz questionnaires being completed. The audit indicated that 96% of staff from Children, Adults and Corporate Services were able to answer the questions correctly.
• Sue Thompson (Named Nurse) and Rebecca Reynolds (Safeguarding Children Nurse Specialist) presented at the Hertfordshire Safeguarding Children Board (HSCB) 0 – 25 conference in July, raising awareness of Graded Care Profile, SEND offer and partnership working
• Domestic Abuse re-audit in August indicates a small improvement in compliance with the policy - 79% compliance with the follow-up and risk assessment process of the Domestic Abuse Police Notifications, compared to 62% in January 2017. Continual reminders about the policy are given during safeguarding supervision, training and via the communication platforms. A further re-audit will occur in Q4
• The first audit to ascertain whether the Child Sexual Exploitation (CSE) template was being used correctly was undertaken in August, using Q1 data. There was evidence that the CSE template had been used on 7 young people in Q1. Although this was a very small cohort, it is evidence that the CSE template is being used correctly, with risk assessment and effective action planning. There was evidence of very good practice of liaison and monitoring, particularly to support the young person and support parents and carers
• Safeguarding Manager, Amanda Hampton, was commended for her work in the Multi-agency Safeguarding Hub and her input to ensure effective partnership working at the Leading Lights awards in July
• Sue Thompson was awarded Queens Nurse in July • Rapid Response Poster was displayed at the Queens Nurse Conference in September. Areas requiring improvement / actions taken • Re-examine the Multi-Agency Risk Assessment pathway to enhance partnership working
96%
99%
97% 98%
Percentage of staff who are compliantwith SGC training
Percentage of staff who are compliantwith SGC supervision
Q1
Q2
Trust target - 95%
Board 30th November 2017 Attachment K1
18
• IT re-design for paediatric liaison and audit the process to give assurance that the new model is not posing any increased risk to children attending the A&E department in the west of the county following the decommissioning of the Paediatric Liaison post.
The Safeguarding Children dashboard for Q2 is attached as Appendix 3. Safeguarding Adults Training During Q2 training targets have been achieved as measured against contract standards Achievements • Assisted in the development of the Chaperone Policy • Rolled out additional training to SAFA Champions on Modern Slavery and Self-Neglect • DOLS leaflet developed and distributed to all inpatient units • Themes and trends identified from SAFA Champions supervision sessions • Sharing Lessons in Practice re Learning Disability patients and Care Homes shared via Clinical Matters
to all staff Areas of improvement identified / actions taken • Audit of Not Brought In Policy still required • Polices for PREVENT and Management of Allegations of Abuse by HCT Staff require revision The Safeguarding Adult dashboard for Q2 is attached as Appendix 4.
98% 98%
100%
97%
98%
100%
90%
92%
94%
96%
98%
100%
Percentage of staff who arecompliant with safeguarding
adults training
Percentage of staff who arecompliant with MCA training
Percentage of staff who arecompliant with DoLS training
Q1
Q2
Trust target - 95%
Board 30th November 2017 Attachment K1
19
Looked After Children and Care Leavers
Achievements • HCT LAC GPs completed 98% of Initial Health Assessments within timescale • 100% Out of County Review Health Assessments completed within time scale by Specialist LAC
nurses • 8 LAC Champions from Children’s Universal Services (CUS) identified and trained • Redesign of 0-5 Review Health Assessment (RHA) template for HCT Health Visitors • Delivery of 4 training sessions to foster carers across the County. Positive feedback received • 94% completion of Personal Health Information Plans for all 18 year olds. Areas requiring improvement identified / actions taken • Difficulty in meeting statutory time frames for the RHAs completed by CUS due to amendments
required. CUS and LAC working together to develop tools and templates to improve the quality and meet statutory timeframes
• Information sharing challenges with CAMHS. Information sharing pathway developed, currently awaiting agreement and ratification from HPFT
• Demonstrating positive health outcomes for children and young people. Quality outcome measure currently being sought
• Completion of Personal Health Information Plans for all 18 year olds continues to be a challenge. There is no national guidance or templates. LAC nurses in discussion with other Counties, the Deputy Designated Nurse and Doctor to develop a local template.
Whistleblowing / Raising Concerns
90%
93% 93%
89%
88%
89%
90%
91%
92%
93%
94%
Percentage of all LAC Initial Health Assessmentsreferred to HCT staff completed within agreed
timescales
Percentage of all Review Health Assessments oflooked after children referred to HCT staff
completed with time scales
Q1
Q2
Trust target - 90%
0
1
0
2
Number of whistleblowing events Number of raising concerns events
Q1
Q2
Board 30th November 2017 Attachment K1
20
During Q2: • There was 1 Herts-wide concern raised, no patient safety issues were identified • There was 1concern raised regarding the HVBU System Process, no known patient safety issues
were identified.
Board 30th November 2017 Attachment K1
21
AN OUTSTANDING PATIENT EXPERIENCE Patient Surveys The information below summarises Q2 community hospital inpatient survey results. A snapshot of patient comments received is detailed below: Were you treated with Dignity and Respect?
• The Sister was very inclusive and person centred. As a family we have been very reassured regarding the process. My nan has clearly been well looked after and her well-being has improved since being looked after at this hospital.
• My daughter was recently an inpatient, and from the moment she arrived until she was discharged she was treated with the utmost respect and dignity. NOTHING was too much trouble, if she requested anything it was dealt with in minutes, the physio team were also outstanding, from the cleaners to the most senior staff, they made her stay a pleasant one. And I would like to say on behalf of [daughter] and her family, a very BIG thank you, and to let everyone know that she is getting along fine. Thank you all once again
Overall, how would you rate the quality of care received?
• Very good care, nice staff, very clean ward • Great care from all staff. Lovely ward to be on and very kind staff • Good care on a very well-run ward. Staff very nice, as is the doctor
Areas for improvement identified Two negative responses were received in the Q2 community inpatient survey: • Physio and OT were brilliant, cannot fault them. Problem with Agency Nurses (rudeness) • Timing and communication with family members can be improved. Patient Stories One patient story was shared at Trust Board during Q2 by the Bladder and Bowel service, focusing on
98% 98% 98% 98%
Percentage of patients who told us they weretreated with dignity and respect
Percentage of patients who told us that theoverall quality of care was good or better than
good
Q1
Q2
Board 30th November 2017 Attachment K1
22
work the service carries out with patients’ to help them self-manage to improve their symptoms. Friends and Family Test The FFT score measures the percentage of patients who would recommend Trust services to friends and family if they needed similar care or treatment.
• The services that have underperformed in this area are exception reported in the BUPR. Complaints and Compliments Complaints Q1 Q2 Number of complaints received 38 37 Percentage of complaints acknowledged within agreed timescales
100% 98%
Number of complaints received graded as category 3 2
(both investigated) 0
Number of complaints referred to the Parliamentary and Health Service Ombudsman
0 1
Number of local resolution meetings held 2 1 Trends and themes identified • A total of 37 complaints were received in Q2; all complainants were offered the opportunity to meet
with staff to discuss their concerns in line with Being Open Guidance • One local resolution meeting took place in Q2 • 98% of all complaints were acknowledged within 3 days • 100% of all complaints were responded to within agreed timescales • The total number of complaints received in Q2 was 37 which represents a 3% decrease when
compared with the total number of complaints received in Q1 (38 complaints) • 1 complaint was referred to the Parliamentary and Health Service Ombudsman and is currently
being investigated • 78% of all complaints received were attributed to Adult Services in East and North Hertfordshire and
Herts Valley.
98% 98%
90%
95%
100%
FFT score
Q1Q2
Trust target - 95%
Board 30th November 2017 Attachment K1
23
The majority of complaints were raised against the following services: • The top three issues raised were;
− Standards of care (24% of all complaints received) − Clinical treatment (24% of all complaints received) − Communication (oral) (16% of all complaints received)
Examples of organisational learning and improvement from complaints
Theme Commentary Outcomes/Learning
Missed Visits or Delayed Appointments
A complaint regarding delay in MSK referral process.
• The service recruited a new member of staff to work to resolve the backlog of referrals.
• Staff were reminded the importance of ensuring all correspondence is checked and responded to in a timely manner.
Communication Standards
Concerns were raised regarding poor communication levels within the MSK (Acute Therapies) Service
• All Acute Therapy staff have undergone training to treat all patients and family with dignity and respect.
• Regular clinical team meetings are held to reflect on the importance for good communication to achieve optimum clinical outcomes and maintain a good staff/patient relationships.
Unacceptable waiting times for appointments
A complaint was made regarding the long waiting times for autism assessment.
• The Trust is currently working with the Commissioners to develop a Hertfordshire-wide Autism pathway. Clinical staff are taking an active part in the Clinical Reference Group which has supported the development of the pathway.
Triangulation of patient experience and patient safety information The Patient Safety and Experience Review Group has piloted a tracker to triangulate quality team information. The Patient Safety and Experience Review Group will: • Review Serious Incidents to pick up on any trends or patterns which can then be escalated to Clinical
Effectiveness Group (CEG) • Identify areas of improvement through trend analysis of complaints which can be summarised and
provided to CEG
16% 16%
11%
Community Nursing &Integrated Teams
Community Hospitals Nutrition & Dietetics
Board 30th November 2017 Attachment K1
24
• Share learning with Business Units via team meetings, Trust Clinical publications and Trust reports.
Equality characteristic group information The Patient Experience Team captures evidence to demonstrate equal access to all groups of people who wish to make a complaint in line with the national directives to ensure equality for people in the 9 protected characteristics groups: • The majority of complaints received in Q2 were related to people aged 80 years of age or over (42%).
38% of all complaints received were related to people aged 0-15 years of age which can be explained in part by an increase in complaints received about waiting times for autism assessment in the community paediatric service. As previously detailed the Trust is currently working with commissioners to develop a Hertfordshire wide Autism pathway in an effort to reduce the current waiting times and inappropriate referrals to the service
• Complaints raised by the person affected, i.e. the patient, account for the majority of Q2 and total 54% of all complaints received.
Compliments
Q1 Q2 Number of compliments received 2841 1335
Number of compliments per 1000 patient contacts
3.93 3.08
PALS contacts
Q1 Q2 Number of PALS contacts received 197 100
Percentage of PALS contacts received that were HCT-related
59% (118) 53% (53)
Number of MP enquiries received 6 11 2017 Patient Led Assessment of the Care Environment (PLACE) Programme The PLACE programme of visits was carried out between March and June 2017. The following bed-based units were assessed: • Potters Bar Hospital • Danesbury House Neurological Centre Inpatient Unit • Herts and Essex Hospital • Holywell Neurological Rehabilitation Unit • Langley House Inpatient Unit • Queen Victoria Memorial Hospital • St Peters Ward, Hemel Hempstead Hospital It was agreed with NHS Digital that Runcie Ward, St Albans, would not be assessed due to a consultation that was being carried out during the assessment period.
Board 30th November 2017 Attachment K1
25
New HCT volunteers were recruited in line with national instruction for organisations to identify their own volunteers and reduced involvement from local Healthwatch in this element of the PLACE programme. PLACE results summary:
Domain HCT score -
2017 National average
Better or worse than
national average
HCT score – 2016
comparison
Better or worse than
HCT 2016
Cleanliness 99% 98% 98%
Food/Hydration (ward assessment and organisational assessment combined)
90% 88% 86%
Privacy, Dignity & Wellbeing 86% 84% 81%
Condition, Appearance & Maintenance
95% 93% 93%
Dementia 88% 75% 79%
Disability 89% 78% 80%
• Cleanliness – in comparison with the national average of 98% all HCT bed-based units bar St Peters
Ward (94%) performed above the national average • Food/Hydration – in comparison with the combined national average of 88% all HCT bed-based
units bar Herts & Essex Hospital (87% average) performed above the national average • Privacy, Dignity & Wellbeing – in comparison with the national average of 84%, Holywell, Langley
House and Herts & Essex Hospital performed below the national average • Condition, Appearance & Maintenance – in comparison with the national average of 93%, all HCT
bed-based units bar St Peters Ward (81%) performed below the national average • Dementia – all HCT bed-based units performed above the national average of 75% • Disability – all HCT bed-based units performed above the national average of 75% Next Steps A detailed report will be shared on 21st November 2017 at Healthcare Governance Committee.
0%
20%
40%
60%
80%
100%
Cleanliness Food/Hydration(ward
assessment andorganisational
assessmentcombined)
Privacy, Dignity& Wellbeing
Condition,Appearance &Maintenance
Dementia Disability
HCT score - 2017
National average
HCT score – 2016
Board 30th November 2017 Attachment K1
26
Implementation of an action plan, including areas of improvement, will be led by Clinical Services with support from the Patient Experience Team. Learning Disabilities Q1 Q2 Number of LD patients attending HCT services
339 380
Number of LD patients flagged on S1 (open referrals)
1925 1217
Carers The HCT strategic plan for Carers 2015 to 2018 was reviewed at the Patient Safety & Experience committee in Q2. There are five key themes to be delivered: 1. Identification of carers 2. HCT provides quality support and inclusion for carers 3. HCT duties as an employer 4. HCT duties to demonstrate outcomes for carers 5. HCT duties to engage carers A working group comprised of a manager from the Patient Experience Team, Adult services, Children’s services, Human Resources and the Communication and Engagement team are meeting to ensure the actions continue to progress. A summary of actions taken to date can be found in Appendix 5. The results of a Carers’ Survey undertaken in July 2017 can be found in Appendix 6. CCG/GP Hotline Enquiries
Q1 Q2 Proportion of urgent ENHCCG hotline enquiries responded to within 5 working days
There were no urgent hotline enquiries
received in Q1
There were no urgent hotline enquiries
received in Q1 Proportion of routine ENHCCG hotline enquiries responded to within 20 working days
92% (11 out of 12) 83% (10 out of 12)
The above figures relate to ENHCCG hotline enquiries only as specified in the Quality Schedule 2017/19.
Board 30th November 2017 Attachment K1
27
EXCELLENT CLINICAL EFFECTIVENESS NICE Quality Standards and Guidance The NICE Working Group (NWG) reviewed NICE guidance (NG) and quality standards (QS) released at the end of each month by the NICE. Where the guidance is found to be applicable to HCT commissioned services, action plans are reviewed at the NWG and an update is provided to the Clinical Effectiveness Group (CEG) meeting to provide assurance of clinical compliance of meeting evidenced-based practice standards.
Q2 Assessed Total assessed
Applicable Total applicable Month NG QS NG QS
July 18 2 20 9 2 11
August 22 0 22 10 0 10
September* 21 7 28 * * *
Total 61 9 70 19* 2* 21* *September guidance - awaiting assessment of applicability
NICE Guidance implemented Quality Standard, QS128 Early years: promoting health and well-being in under 5’s • HCT delivers a high standard of care to universal and vulnerable children/families who may need
extra support • HCT has effective links with GP and midwifery services who highlight any concerns identified in the
antenatal period ensuring Health Visitor involvement • An increase in staffing for all teams will enable 5 face to face universal contacts. Quality Standard, QS154 Violent and aggressive behaviours in people with mental health problems • Young people and their families are supported to identify triggers and early warning signs by
educational and support tools (e.g. Arousal Curve, Incredible 5 point scale) • Functional assessments (observations, behavioural recording forms and clinical interviews) identify
triggers and setting events • PALMS collaboratively work out strategies to de-escalate and prevent behaviours. Quality Standard, QS65 Hepatitis B • Health Visitors (HVs) ask mothers about their Hepatitis B status at the Antenatal/New Birth/Transfer
In visit • HVs will also check the SystmOne patient record to see what Hepatitis B status is recorded by Child
Health • Children within Children’s Universal Service already identified as Hepatitis B positive will receive the
full vaccine programme. Quality Standard, QS52 Peripheral arterial disease (PAD)
Board 30th November 2017 Attachment K1
28
• All patients referred to the Leg Ulcer Service receive an holistic assessment which includes PAD • Comorbidities (e.g. diabetes, smoking and weight) as part of the holistic assessment are also
assessed although the service is not commissioned to offer this • Doppler assessments to measure ABPIs (Ankle Brachial Pressure Index) on appropriate patients is
undertaken unless contraindicated. Clinical Guideline, CG147 Peripheral arterial disease: diagnosis and management • The leg ulcer service assesses patients with leg ulceration for reduced blood flow to one or both
lower limbs • The GP is contacted to request a vascular referral at the Acute Trust for a diagnosis of PAD. NICE Guideline, NG59 Low Back Pain and Sciatica in Over 16s: Assessment & Management • The format of back classes has been changed and Staff have been trained across all sites • MSK Service aims to improve people’s quality of life by promoting the most effective forms of care
for low back pain and sciatica. NICE Guideline, NG51, Sepsis: recognition, diagnosis and early management • HCT provide training on management of sepsis as part of 2-day clinical update sessions • The development of Sepsis algorithm guides staff on recognising the signs of Sepsis including the
‘Sepsis Six’ guidance • Sepsis algorithm can be audited as part of the care plan on SystmOne to provide assurance of
appropriate assessment NG19, Diabetic foot problems: prevention and management • East & North Hertfordshire CCG (following funding from NHS England) has commissioned an
increased Diabetes Multi-Disciplinary Foot Clinic • Initially this will be funded for 1 year, and will ensure adherence to NICE guidance by allowing 24
hours access to the Podiatry Team (to be in place by early 2018 - recruitment to extra posts is currently underway).
Clinical Audit Learning from National Clinical Audit Reports National Diabetes Audit, 2015-2016 [Report date: 31 January 2017]. Report 1: Care Processes and Treatment Targets; England and Wales; CEG, August 2017 The audit set out to review prevalence of diabetes and the percentage of diabetes patients who receive the 8 diabetes care processes. The report does not detail specific results for HCT as an organisation as data has been extrapolated for Hertfordshire patients as part of individual Clinical Commissioning Groups (CCGs) and benchmarked against national results. Actions include: • Increasing patient engagement through telephone follow-up with patients who DNA and use of text
messaging for appointment reminders to reduce non-attendance • Piloted Saturday DESMOND Education Clinics. Due to the success of the pilot, HCT will continue to
offer monthly Saturday DESMOND Education Clinics to increase participation. Feedback received in
Board 30th November 2017 Attachment K1
29
Q1/Q2 is very positive, 97% (424/437) of patients are extremely likely/likely to recommend this course to family or friends:
• Improved collaboration between West Hertfordshire Hospitals Trust (WHHT) - the Diabetes Service has been successful in partnering with WHHT to deliver an integrated model for the delivery of care across acute and community sectors
• Diabetes Specialist Nursing (DSN) Team has now undertaken training of Health Care Assistants (HCAs) for administering insulin. Patient feedback as part of the HCA project:
• Participate in the next round of the National Diabetes Audit (2018). National Diabetes Foot Care Audit Report, 2014-2016 14 July 2014 to 8 April 2016. [Report date: 7 March 2017]; England and Wales; CEG, August 2017 The audit aims to see if NICE recommended care structures are in place for the management of diabetic foot disease. The NDFA was launched in July 2014 and is a continuous data collection audit, in which HCT’s Podiatry service has participated for the past three years.
Actions include: • Reviewed SystmOne templates to improve data collection for the national audit. SystmOne template
now incorporates a wound care classification as recommended by NICE Guidance NG19 • All Podiatrists (Band 6 and above) are to complete at least 2 NDFA forms as part of their objectives. • Reviewing referral form and current pathway – due by December 2017 • Commissioning of a Multi-Disciplinary Foot Clinic will ensure adherence to NICE guidance is achieved
for preventing and managing foot problems in adults with diabetes by allowing 24 hours access to the team.
Learning from Local Clinical Audit
The girls always discuss my diabetes with me and even ask me about my diet and my general wellbeing, they seem to be very knowledgeable about my condition” “Great service”
Board 30th November 2017 Attachment K1
30
Nutritional Audit in Community Hospital Settings; CEG, April 2017 The audit demonstrated that, while a number of the key characteristics for the provision of good nutritional care are embedded within the day to day practice of staff working within the Community Hospitals, there were risks identified. There was limited assurance, around correct MUST tool assessment by staff possibly due to low uptake of MUST e-Learning training, leading to inappropriate referral to a dietitian and patients receiving inappropriate Oral Nutritional Supplements (ONS). There is limited guidance following MUST assessment available on SystmOne. Actions include: • Dieticians are providing 15 minutes of face-to-face MUST training on the bed bases • SystmOne template has been reviewed and updated so that the MUST score will trigger a linked
action to provide guidance on the steps to take following MUST assessments (e.g. provide high energy nutrient rich foods, ONS supplements etc.)
• Re-audit in 6 months on the MUST Score and Use of ONS in Q3 once MUST training implemented across all Community Hospitals.
NEWS Risk Assessment Audit; Ward Managers Meeting The audit was undertaken in Q1 across eight Community Hospital Units (as part of HCT quality schedule) demonstrated that NEWS score on deteriorating patients was recorded in a timely way in 89% of inpatients and escalated in 96%. Actions include: • NEWS scores to be reviewed at each handover • Reviewed agency staff checklist to ensure competency and compliance in the use of NEWS • Re-audit in Q3. Audit to Investigate the Adherence of Antimicrobial Prescribing in HCT Community Hospitals; Medicines Management Forum; July 2017 The audit results have shown an improvement in prescribing against HCT formulary guidance, stop/review dates on charts. The level of appropriate recording of antibiotic indication in the notes was low compared to previous audits and this area requires improvement. Not all prescriptions have a stop/review date and indication of antibiotic annotated on the prescription chart. The work carried out by Pharmacy Team will lead to less risk of Clostridium Difficile infection and development of resistance. Actions include: • Quarterly audits carried out all eight community hospital units to monitor improvement and ensure
good standards of practice are maintained • Results of audits are reported to ward managers/teams (including prescribers) on the day of the
audits for immediate action to highlight any issues identified which is likely to have the most impact on prescribing practice
• Antibiotic APP developed in conjunction with both local Hertfordshire Commissioners to provide staff working in the community access to pharmaceutical information allowing them to make appropriate and timely antibiotic choices to treat patients.
Proton Pump Inhibitors (PPI) Audit; Medicines Management Forum; July 2017 The audit was to review PPI prescribing against HCT PPI guidance and was carried out in three Community Hospital Units (Potters Bar, Holywell Inpatients, and Midway Inpatient Unit). The report
Board 30th November 2017 Attachment K1
31
showed that some prescribing of PPI from the acute/GP practices are inappropriate and that this can potentially increase the risk of interactions, adverse effects and clinical risks (including Clostridium difficile, Osteoporosis and Hypomagnesaemia). Actions include: • Share results with prescribers to help increase awareness of the need to assess PPIs in all patients to
determine if they are clinically required/safely stopped • Reissue the HCT PPI guidelines to all inpatient medical and nursing staff highlighting the need to
review PPI prescribing within 72 hours of admission, document the indication on the drug chart/patients’ notes and where relevant document a stop or review date
• Re audit all HCT inpatient units PPI prescribing in April 2018. Pain Audit; Medicines Management Forum; July 2017 This audit was undertaken as part of the quality improvement action plan from CQC, as it was found that the Trust did not have consistent tools to monitor pain. The audit was undertaken across community settings in HCT and ascertained whether pain tools were being used and whether staff were using them effectively to assess and manage pain for patients who expressed pain as a concern. The audit demonstrated that not all services had access to a pain template and where one was available; it was not being fully completed and reviewed. Actions include: • Review national tools and gain permission to use these. Collaborative working with Learning
Disability/Children’s Services and Adults services to ensure standardised pain templates • 4 Pain templates now added on SystmOne (September 2017) and accessible for all services [Abbey
pain scale for cognitive impairment, Entonox pain scale for learning disabilities, Wong-Baker faces for children, Pain Sites for adults]
• Education and training plan in place • Re-audit in 23rd October 2017 to monitor compliance of the use of the new pain tools.
HCT Syringe Pump (McKinley) Audit (St Albans & Harpenden Locality; Clinical Effectiveness Forum; September 2017 The objective of the audit was to assess the key aspects of the revised policy and identify areas of training and support that are needed to ensure staff are competent and confident with this clinical procedure. 88% respondents knew about the HCT policy and where to access it. 92% of respondents knew where to access help and support (from a variety of sources). 71% respondents felt confident about putting up a syringe pump. Actions include: • Training on the revised Syringe Pump Policy • Training on the Individualised Care Plan for the Dying Patient – to ensure that staff understand why
this is used and when to implement it
Feedback from a patient with learning disability in a residential home: “I liked using the pictures to talk about my pain”
Board 30th November 2017 Attachment K1
32
• Ensure all staff have competencies signed – to be included on e-roster. Staff Engagement Session at Leading Lights in July 2017 A clinical audit information session was held at the ‘Leading Lights’ event in July 2017 to promote how clinical audit can be used as a quality improvement tool to enhance patient care. Medicines Management Review of NICE Technology Appraisals • During Q2 NICE published 32 TAs; all of these were reviewed and 7 were found to be applicable to
HCT commissioned services. Antibiotic prescribing audit Community hospitals Point prevalence audit was undertaken in July 2017: • 23 patients were included in the audit; 24 oral or IV antimicrobial preparations were prescribed • 100% of patients were prescribed antimicrobial medication in line with pan-Herts or primary care
guidance or HCT guidelines. Community district nursing teams • Prescribing data is not currently available for Q2 as ePACT prescribing data is provided by CCG;
quarterly reporting of prescribing data is therefore retrospective • During Q1, 121 antibiotic prescriptions were issued by HCT nurses • 6 prescriptions were outside of the HCT/CCG antibiotic prescribing guidelines. Individual prescribers
have been asked to provide their clinical reasoning for prescribing outside of the guidelines and will be followed up by the Pharmacy Team.
MHRA Medicines Related Patient Safety Alerts • During Q2 3 MHRA updates have been received • 2 of the drug updates were applicable to HCT services and have been circulated to services for
review and response. Public Health Metrics Make Every Contact Count (MECC) Training
Q1 Q2 Number of eligible staff 2194 2190 Number of eligible staff who have received MECC training 986 980 Percentage of eligible staff who have received MECC training 45% 45%
Board 30th November 2017 Attachment K1
33
Patient Advice Regarding Alcohol Consumption
Board 30th November 2017 Attachment K1
34
Weight Management
Board 30th November 2017 Attachment K1
35
Smoking status and advice given
Percentage of patients with a smoking status recorded
Adult Specialist Services 89.28%
Children's and Young People's Services 88.29%
East & North Herts ICT 94.45%
Herts Valley ICT 94.51%
Inpatients 50.51%
Percentage of people who smoke
Adult Specialist Services 38.26%
Children's and Young People's Services 10.33%
East & North Herts ICT 2.27%
Herts Valley ICT 6.50%
Inpatients 6.53%
Percentage of smokers given brief intervention advice
Adult Specialist Services 56.74%
Children's and Young People's Services 70.33%
East & North Herts ICT 65.77%
Herts Valley ICT 55.22%
Inpatients 62.5%
Number of smokers referred to HSSS (as reported by HSSS)
Total 51
Board 30th November 2017 Attachment K1
36
LEARNING FROM CLAIMS AND LITIGATION Claims
Clinical negligence claims No new clinical negligence claims have been received in Q2. One clinical negligence claim reported as received in Q1, relating to a prisoner at HMP The Mount, has been closed. This is because the allegations of negligence pre-dated the time that the prisoner arrived at HMP the Mount and HCT is not therefore the liable party. Note: Any new claims reported are claims received and advise of allegations. They do not necessarily confirm that the Trust has admitted liability. In some cases of new claims reported, the Trust may not be the correct defendant and further investigation is underway.
Other claims New Employer‘s Liability
Claims New Third Party Liability Claims Claims closed
1 (Alleged slip in a puddle at a
community hospital resulting in injury to member of staff)
0 0
Trends in claims There are no discernible trends. Claims are few in number, tend to be of low value and are widely spread in terms of services, geography and the nature of claim.
Coroners’ Inquests 1 The Inquest into the death in custody of a prisoner in HMP The Mount, who died in Watford
General Hospital on 26th May 2016 having been found hanging by a ligature on 22nd May 2016 was held in September 2017.
The conclusion of the jury as to death was misadventure. In respect of circumstances the deceased came by his death the jury returned a short narrative: “Misadventure contributed to by the failure of prison and healthcare staff to share pertinent information”. Although the (mandatory) Independent Clinical Review of this incident had made some findings and recommendations the Trust’s own Serious Incident Investigation did not identify any healthcare failings.
The Coroner stated that he would not be issuing a Prevention of Future Death Report (PFD).
2 An Inquest into a death in custody at HMP The Mount in September 2015, originally scheduled to
be held in September 2017, has now been deferred by the Coroner until November 2018. This is on account of witness availability. A number of health care staff are required to give evidence and the Trust is legally represented jointly with HPFT in respect of this Inquest.
Board 30th November 2017 Attachment K1
37
Appendix 1: Keeping in Touch visits
Service Examples of Good Practice Main Themes ( Opportunities / Challenges) Recommended Actions
Diabetes Service • Welcoming professional approach with clients
• Thorough description and explanation of medication aims, how it works- what to be looking for that indicates the medication dose needs to be altered.
• The principles of the impact of carbohydrates on sugar levels and insulin.
• Checking that the client had understood information and checked if any further questions.
• Interface with District Nurses- HCA role working well
• High demand for the service • Appropriateness of referrals • Staffing and access to consultants • Positive feedback about the new team manager-
very approachable and supportive • Clinic access to blood results not always possible. • Future connectivity system one and EMIS • Awaiting update re newly commissioned service
• Link self-management team with team manager to consider how can enhance impact.
• Explore how DSN’s can be given locality profile information and a range of indicators.
• Access to blood results – if a resolution not identified team leader to escalate
Simpson Ward
• Name badges are worn, but require updating to HCT.
• Medicines are securely stored. • The Medirest team were caring and
enthusiastic, ensuring that patients are helped to choose from the menu and have nicely presented meals.
• A new kitchen looks very smart. • Patient bathrooms were in good order
and very clean.
• Visit took place two weeks after HCT took over the running of the ward from WHHT. The most recent CQC rating of the ward was “Inadequate”.
• Staff are progressively transitioning to HCT however a great deal of input is required to develop staff and overcome poor practices and move towards a CQC “Good” level of performance.
• A detailed report has been sent to the acting CEO
Board 30th November 2017 Attachment K1
38
Appendix 2: Quality Assurance Visit Action Plan - Antenatal and newborn screening service
Action not yet initiated
In progress and on target
In progress but not on target
Action completed Not achieved Action deferred
Ref
Item Action Required Lead Due Date
for Completion
Progress/Updates
1. Update the Hertfordshire Community NHS Trust incident policy to reflect the requirements defined in “Managing Safety Incidents in NHS Screening Programmes”
NHSE Priority rating: Standard
Evidence needed: Ratified policies meet requirements described in national guidance.
CS 12 months CS making contact with HCT Quality team to amend.
2. Standardise child health operational processes and communication across the 4 health visiting areas to include a single point of access for Cambridgeshire Community Services NHS Trust, Central and North West London NHS Foundation Trust and Essex Partnership University NHS Foundation Trust
Responsibility - Central Midlands South, Cambridgeshire Community Services NHS Trust Central and North West London NHS Foundation Trust ,Essex Partnership University NHS Foundation Trust and Hertfordshire Community NHS Trust
NHSE Priority rating: Standard
Evidence needed: Standard operating procedure ratified by all organisations.
CS 3 months CS to lead on the standardization of the CHIS processes across CMS CHIS area. ACTION for Hertfordshire CUS is to align resource to a SPOC for antenatal and new births within the re-procurement design.
3. Develop a standard operating procedure for the “bulk upload” of blood spot screening results Responsibility - Central Midlands South Child Health Information
NHSE Priority Rating: Standard
Evidence needed: Standard operating procedures ratified.
CS 6 months SOP ready, training will take place October 2017.
4. Complete project to merge 5 Evidence needed: Central CS/JJ/HCT 12 months Booked for May 2018. Work
Board 30th November 2017 Attachment K1
39
Ref
Item Action Required Lead Due Date
for Completion
Progress/Updates
SystmOne units
NHSE Priority Rating: Standard
Midlands South Child Health Information operate a single child health unit.
COMMS up and risk management to be prepared with communications plan.
5. Complete a data reconciliation exercise for children who are registered with a London GP and resident in Hertfordshire or Bedfordshire to cover the period April to July 2017
NHSE Priority Rating: High
NHS Digital data extract requested Data reconciliation completed Blood spot screening outcome recorded for all children in this cohort.
CS 3 months Both North Hubs contacted; meeting 6/10/17 to plan reconciliation. Running report end October. To put HCT RR. To consider a regular data cleansing programme.
6. Formalise communication processes between the 4 London child health information hubs and Central Midlands South Child Health Information
Responsibility – NHS England (Central Midlands) and (London), Central Midlands South Child Health Information and London hubs
NHSE Priority Rating: High
Standard operating procedures ratified Central Midlands South Child Health Information programme board meeting notes
CS 3 months
7. Include designated contacts for all relevant organisations in the death of a child standard operating procedure
NHSE Priority Rating: Standard
Standard operating procedure includes designated contacts
CS 3 months Complete for sign off by QA. CS to send. October 2017.
8. Standardise the process for notifying Child Health Information of all babies who require hepatitis B vaccine scheduling and follow up serology
Responsibility - Central Midlands South Child Health Information, Bedford Hospital NHS Trust, East and North Hertfordshire NHS Trust, Luton and Dunstable University Hospital NHS Foundation Trust, Milton Keynes University
Standard operating procedure for notification Annual audit of notifications.
CS 6 months Single process is already in place. CMS CHIS regular audits in place to cross reference maternity data. To query with PH Screening Board.
Board 30th November 2017 Attachment K1
40
Ref
Item Action Required Lead Due Date
for Completion
Progress/Updates
Hospital NHS Foundation Trust and West Hertfordshire Hospital NHS Foundation Trust
NHSE Priority Rating: Standard
9. Make sure that all NIPE newborn examination results and screening outcomes are communicated to child health services
Responsibility - Central Midlands South Child Health Information, Bedford Hospital NHS Trust East and North Hertfordshire NHS Trust, Luton and Dunstable University Hospital NHS Foundation Trust, Milton Keynes University Hospital NHS Foundation Trust and West Hertfordshire Hospital NHS Foundation Trust
NHSE Priority Rating: Standard
Audit of NIPE results and screening outcomes on child health information system demonstrates complete data.
CS 12 months NIPE in place Lister/Beds/L & D; MK sending on spreadsheet. WHHT in progress.
10. Implement and monitor a plan to ensure that the newborn blood spot screening avoidable repeat rate is no more than 2% (NB2)
Responsibility –Cambridgeshire Community Services NHS Trust, Essex Partnership University NHS Foundation Trust and Hertfordshire Community NHS Trust
New Priority Rating: Standard
Action plan that is agreed and monitored by antenatal and newborn screening programme board Acceptable level for NB2 reached.
CS/LL 6 months Mechanism in place within HCT; Datix complete with lessons learned. To establish with NNBS Lead HCT Liz Little the current performance.
11. Implement and monitor a plan to ensure that at least 95% of babies have a blood spot screening outcome recorded within 21 days of notification of registration to child health services (NB4) Responsibility – NHS England, Central Midlands South Child Health Information, Cambridgeshire Community Services NHS Trust, Essex
Action plan that is agreed and monitored by antenatal and newborn screening programme board Acceptable level for NB4 reached Screening outcome recorded for all babies
LL 6 months Liz Little to provide an assurance plan about how this is managed & reviewed in HCT.
Board 30th November 2017 Attachment K1
41
Ref
Item Action Required Lead Due Date
for Completion
Progress/Updates
Partnership University NHS Foundation Trust and Hertfordshire Community NHS Trust NHSE Priority Rating: Standard
12. Implement and monitor a plan to ensure that at least 95% of samples are received in the laboratory within 3 working days of sample collection
Responsibility – Cambridgeshire Community Services NHS Trust, Essex Partnership University NHS Foundation Trust, Central and North West London NHS Foundation Trust and Hertfordshire Community NHS Trust
NHSE Priority Rating: Standard
Action plan that is agreed and monitored by antenatal and newborn screening programme board Acceptable level for standard 5 reached
LL 3 months Liz Little to confirm that there is a clear SOP re this & how this is managed. This is monitored by CHIS & is escalated when dates are not within 3 day timescale.
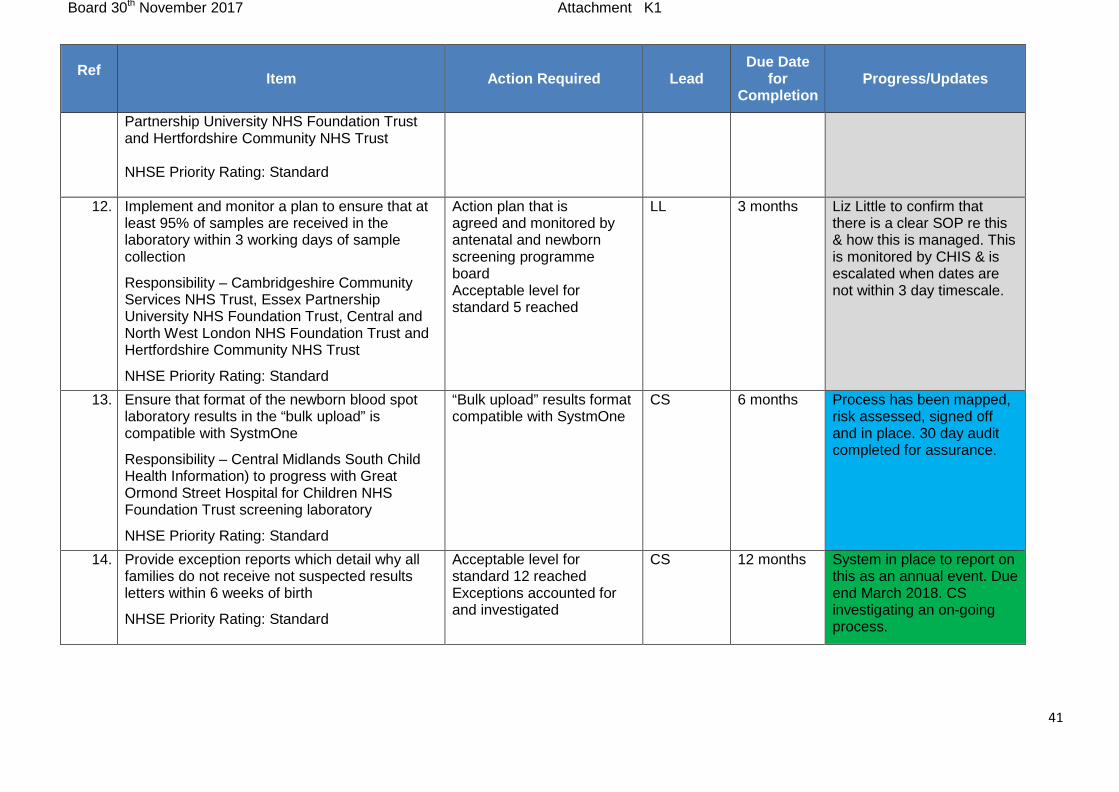
13. Ensure that format of the newborn blood spot laboratory results in the “bulk upload” is compatible with SystmOne
Responsibility – Central Midlands South Child Health Information) to progress with Great Ormond Street Hospital for Children NHS Foundation Trust screening laboratory
NHSE Priority Rating: Standard
“Bulk upload” results format compatible with SystmOne
CS 6 months Process has been mapped, risk assessed, signed off and in place. 30 day audit completed for assurance.
14. Provide exception reports which detail why all families do not receive not suspected results letters within 6 weeks of birth
NHSE Priority Rating: Standard
Acceptable level for standard 12 reached Exceptions accounted for and investigated
CS 12 months System in place to report on this as an annual event. Due end March 2018. CS investigating an on-going process.
Board 30th November 2017 Attachment K1
42
Appendix 3: Safeguarding Children Dashboard Q2
Board 30th November 2017 Attachment K1
43
Appendix 4: Safeguarding Adult Dashboard Q2
Board 30th November 2017 Attachment K1
44
Appendix 5: Carers – actions to date
Objective Action
Identification of carers • Carers recorded on Systm1. The numbers of carers referred are reported quarterly by the Performance and Information team to the Carers Lead.
• Operations staff are proportionately trained to be carer-aware. Training delivered to staff on line or via Carers champion training sessions. Information regarding training included in induction pack.
• Carers champions have put up displays in public areas of ward and clinics
• Staff refer carers to Carers in Herts via an icon on the home page of all HCT computers.
HCT provides quality support and inclusion to carers
• HCT has 63 carer’s champions. The Carers Champions are invited to meet quarterly at a meeting chaired by the HCT Carers Lead
• Activities were organised during national carer’s week in June which included a cake sale raising £100 for Carers in Herts.
• Two members of HCT staff recently completed a 100 mile bike ride to raise funds for additional resources to implement Partnership in Care. This new approach involves extending visiting hours and enabling carers to be more involved in supporting the person they care for during their hospital stay if they wish to be.
HCT duties to engage carers, to learn from and share best practice for carers, to join up engagement processes to minimize duplication for carers.
• In partnership with the Carers lead at East and North Herts NHS Trust (ENHT), a carer’s survey was completed in July 2017.
• In August 2017 carers met with carers leads from ENHT, West Herts Hospital Trust (WHHT), HCT and Carers in Herts to discuss what matters most to carers. Follow up work on the key issues identified, will commence in Q3 involving carers and staff.
• Plans for the implementation of Partnership in Care are in progress. − Staff have completed a survey. − Following meetings with ward staff, patients and carers
in September, it will be piloted on 2 wards − Plan to roll out to all the community hospitals by January
2018.
Board 30th November 2017 Attachment K1
45
Appendix 6: Results of Carers’ survey
Improving Carer Support in East and North Herts NHS Trust and Hertfordshire Community NHS
Trust Ruth Bradford, Engagement Manager and Strategic Lead for Carers in HCT
Jodie Deards, Carers Lead, ENHT The Carers leads at East and North Herts NHS Trust (ENHT) and Hertfordshire Community NHS Trust (HCT) are working together to develop a shared pathway for carers to ensure a smoother transition between acute and community services. Over the past year, the Carers Lead in ENHT has implemented measures to improve the carers experience and involvement. A key action has been to extend visiting hours from 9am to 9pm. Research highlights that the involvement of family and friends in care helps to improve communication, experience and clinical outcomes for patients. Participation in care is increased and patients and their carers stress and anxiety is reduced. Practical measures to support this includes providing carers with a lanyard so they can be easily identified, including carers in the hot drinks round and providing a snack bag. HCT’s strategic plan for carers has included carer identification in the patient’s records, recruiting Carers Champions in each service to provide information and training to new staff and signposting to Carers in Herts. HCT are planning to introduce Partnership in Care by September. This is similar to the model used by ENHT and also involves extending the visiting hours. Carers involved in services provided by ENHT and HCT were asked to complete a short survey. This was circulated to carers via the Carers Champions in HCT and via the Carers lead in ENHT. Carers in Herts shared the survey via social media with their members. The survey There were 22 responses. Carers completing the survey were asked to leave contact details if they wished to be involved in follow up work. A total of 5 carers expressed an interest. The survey asked 4 questions:
1. How do we include you when the person you care for becomes involved in health care services? For example emergency or planned hospital admission or home visiting from the District Nursing service.
− Tick all that apply: − Including you in their initial assessment − Including you in discussion about their care plan − Other (please specify)
2. How would you like to be involved and kept informed whilst the person you care for is receiving their care?
− Tick all that apply − Face to face contact with you − Telephone contact − A message book
Board 30th November 2017 Attachment K1
46
− Other (please specify) 3. How would you like to be involved at the point of discharge either to home or from one service
to another? Tick all that apply: Involvement in discharge planning, Other (Please specify)
4. Thinking about your role as a carer, what is most important to you? Results The pie charts show the responses. A high percentage of carers responded that they would like to be included in the initial assessment and discussion about the care plan. The majority of respondents (86%) would prefer to be kept informed by face to face contact, 50% ticked telephone contact and a small number ticked message book. Other suggestions included email and text.
Responses to the final question about what is most important included, • listening skills • knowing the patient is OK and having information about treatment • advice, guidance, financial advice • patients receive the same information. i.e. we are treated as one • being present during treatment to support emotionally • mental strength and encouragement • being involved and acknowledged.
Next steps A focus group to be held in August with 3 key objectives:
1. Share the survey results 2. Identify the areas that Carers feel require the most focus 3. Develop a clear plan of action to take forward
Develop a shared care pathway for carers for acute and community services Work in partnership with the other NHS organisations in Hertfordshire to develop a shared strategy for Carers.
Board 30th November 2017 Attachment K2
1
Healthcare Governance Committee Tuesday 19 September 2017 2.00 – 17.00
Boardroom, Howard Court
Key Points for the Board and Audit Committee to note: RED
• None
AMBER/RED • Insulin Related Incident analysis • Business Unit Performance Report
AMBER/GREEN
• Herts Non Acute Stranded Patient Review • Risk Strategy Plan update • FIRST Assurance Report • Simpson Ward Update • Quality Report Q1 • Complaints Interim Report • Serious Incident Interim Report • Safe Staffing (July & August 2017) • Pressure Ulcer Q1 • National ambition to reduce Gram Negative blood stream infections 2017-18
GREEN
• Savile Report Compliance
1. Present & Apologies Present:
Anne McPherson Alan Russell Jeff Philips Tricia Wren Dr John Omany Marion Dunstone
AMc AR JP PW JO MD
Non-Executive Director (Chair) Non-Executive Director Non-Executive Director Deputy Director of Quality & Governance and Deputy Chief Nurse Medical Director Director of Operations
In Attendance:
Simon Wan Rosan Rowland Louise Ayres Charlie Cadogan Suleiman Banian Marina Sweatman
SW RR LA CC SB MS
Chief Pharmacist DGM Inpatients Implementation Manager HV ICT Service Manager Head of Risk & Clinical Effectiveness Board Support Officer
Apologies:
David Law Clare Hawkins Debbie Eyitayo
DL CH DE
Chief Executive Deputy CEO, Director of Quality &Chief Nurse Interim Director of HR & OD
Board 30th November 2017 Attachment K2
2
Tracey Westley Linda Sheridan Brenda Griffiths Declan O’Farrell
TW LS BG DOF
Assistant Director Risk & Quality Assurance Non-Executive Director Non-Executive Director (designate) Trust Chair
Item Action Date 1a Introduction and Apologies The chair opened the meeting and observers were welcomed. No
apologies were noted.
2. Declaration of Interests No declarations or conflicts of interest were recorded.
3. Previous Minutes and Tracker Progress
The minutes of meeting on 18th July 2017 were received and accepted as correct. Tracker The completed (blue) and in progress actions (green) were acknowledged. 3 18.7.17 The Hertsmere Locality Operational Review will be built into the mobilisation plan. The timing will be reviewed in November but the feeling is that the most useful time to hold the review would be in February 2018 with external stakeholders and GPs participating. Remove from the tracker.
MS
Feb 18
4. Assurance 4.1 Herts Non Acute Stranded Patient Review A presentation was given on the findings from the Stranded Patient
Review and the progress of the roll out of the Red to Green programme It was noted that: (i) The Red to Green programme is a new initiative to reduce the
length of stay in Community Hospitals and introduce smart rehabilitation.
(ii) The outcomes of the The Emergency Care Improvement Programme (ECIP) non acute stranded patient review in East and North Herts undertaken in June 2017 were presented.
(iii) Raising the profile of discharge planning with patients and families is planned with visual aides to support this process
Challenge, Observations & Questions a) The Red to Green programme requires a data set to give full
assurance and demonstrate a track record of success especially when reporting to Commissioners.
b) A task and finish group will be reviewing the challenges and constraints for areas within HCT gift to address. This may lead to a review of roles to ensure best use of resources and maximise discharge potential.
c) In order to maximise capacity for both health and social care there are a range of system wide changes to be addressed including
Board 30th November 2017 Attachment K2
3
Item Action Date potentially moving towards adult care trusted assessment.
d) The four patient questions to be added to the Keeping in Touch visit prompt sheet.
e) The work undertaken to date was commended. The ongoing work to consider the impact on patients’ lives, not just patient flow.
f) Staff need to be empowered to refuse patients that are inappropriate referrals and an escalation process should be in place to support staff. MD advised that this is an on-going area of focus.
Decisions and Actions 1. The Red to Green programme requires a data set to give full
assurance and demonstrate a track record of success especially when reporting to commissioners.
2. Four patient questions to be added to the Keeping in Touch visit, prompt sheet
3. The findings from the Stranded Patient Review and the progress of the roll out of the Red to Green programme noted
Risk Rating: Green
RR MS/RR
To note To note
4.2 Insulin Related Incidents analysis The Insulin related incidents analysis was received and discussed.
It was noted that: (i) Of the medication incident reports a high level of these related to
insulin however all reported a low level of harm (ii) Trends have been captured and an Insulin Working Group has
been set up to reduce the incidents and to consider new ways of working to include more patient involvement in the administration of their own insulin.
(iii) A “Sharing Lessons” in practice is being developed and will be cascaded to staff.
Challenge, Observations & Questions a) A change in culture is being moved forward to include patient self-
management. b) Pictorial information is useful to clarify information and processes
for staff and patients. c) It was acknowledged that staff have professional accountability to
undertake basic checking of drugs before administration. d) Assurance was provided that the situation has not deteriorated
with HCA’s administering insulin. HCT are comparable with other Trusts. HCT capture the data which others Trusts do not.
e) Medium and long term aims may include tele-medicine or other technological solutions.
Decisions and Actions 1. The Insulin Related Incidents analysis was noted
Board 30th November 2017 Attachment K2
4
Item Action Date Risk Rating: Amber/Red
4.3 Trust Compliance With Recommendations Following Savile Enquiry The Trust compliance with recommendations following the Savile enquiry
was received and discussed. It was noted that: (i) Assurance was provided that the Trust has implemented all
recommendations set out by the Secretary of State following the Savile inquiry (2015).
(ii) A gap analysis review was completed in May 2015 and all recommendations have been implemented.
(iii) Policies and processes have been updated to ensure patients are kept safe while in HCT care.
(iv) Progress and implementation of the recommendations has been monitored via the Safeguarding Children Forum
Decisions and Actions 1. The Savile report was recommended to the Board. The Trust
compliance with recommendations following the Savile enquiry was noted
Risk Rating: Green
4.4 Health & Wellbeing Strategy The revised Health and Well Being Strategy was received and
discussed. It was noted that: (i) The Health and Wellbeing Strategy was presented to the
Committee in July at which further review of the following points was requested in respect of: • Safety • Clinical Effectiveness • Effectiveness outcomes
(ii) Revisions to the Strategy by the Deputy Director of Quality and Governance / Deputy Chief Nurse and the Associate Director Risk and Quality have been incorporated. The main changes are: • Inclusion of an additional outcome: ‘people will receive
safe and effective care from trained and skilled professionals’
• Additional narrative on Quality Priorities
(iii) The content of the strategy has also been updated to reflect the ongoing redesign work in Herts Valleys (HV). The Director of Service Development and Partnerships has confirmed that the HV redesign work does not materially alter the content of the strategy.
Challenge, Observations & Questions
Board 30th November 2017 Attachment K2
5
Item Action Date
a) The revised Strategy reads very well and flows well, current developments have informed the revision.
Decisions and Actions
1. The revised Health & Wellbeing Strategy was approved and recommended to the Board for approval.
Risk Rating: Green .
4.5 Risk Strategy Plan update The Risk Strategy Plan update was received and discussed
It was noted that: (i) The year 2016-17 has been a maintenance and consolidation
year due to capacity within the risk and assurance team. The team is now up to strength.
(ii) The risk plan is revised in line with the revision of the Risk Strategy and will be presented in November.
(iii) ISO 9000 scope for accreditation, has been placed on hold in light of risk team capacity, current wider environmental and commissioning landscape. Following review at the Audit Committee the Executive Team have been asked to make a decision re “on hold” or “no longer pursue”.
Challenge, Observations & Questions a) Feedback from a recent staff event showed that they are aware of
the incident reporting system and the risk register. b) It was acknowledged that work is ongoing to review the risk
register further together with the risk reporting culture.
Decisions and Actions
1. Risk Strategy Plan update was noted
Risk Rating: Amber/Green
4.6 First Assurance Report The FIRST assurance report was received and discussed.
It was noted that: (i) This is a new service which has involved working closely with
partners. (ii) This model could provide significant efficiencies in the system. (iii) All safeguarding concerns regarding agency staff have been
investigated, none of the 5 concerns raised were upheld. The police were notified in one case and have confirmed they are not investigating further.
(iv) A rota of Quality Assurance Visits is planned during August/September. Initial findings have been positive and have
Board 30th November 2017 Attachment K2
6
Item Action Date highlighted good infection control, positive verbal feedback from service users re care being offered. Further consideration to be given to ensure care is quickly arranged for new patients especially at weekends.
(v) FIRST response, progress, demand and activity in respect of Delayed Transfer of Care (DTOC) were highlighted.
(vi) KPI achievements were highlighted. (vii) Progress is being made with WHHT to agree stable funding which
will allow recruitment into HCT contracts, and drive efficiency, resilience and quality.
(viii) Data was provided on the CQuIN and hospital re admissions.
Challenge, Observations & Questions a) Thanks were recorded for the excellent work in setting up and
continually improving this new service which takes patients out of hospital to be assessed at home for health and social care needs. It is a credit to CC and the team.
b) Good assurance was provided that patient safety is paramount and a regular assurance visit program is in place.
c) The challenges in relation to social care provision and funding were discussed and solutions are being sought to ensure patient flow.
d) Every effort should be made when the opportunity arises to retain the excellent staff currently in place and train to HCT standard.
e) A process needs to be developed to understand the reason for hospital re admission and lessons learned used to avoid future re admission and improve the patient experience.
f) Other opportunities to expand this service further across the county to make a difference are being scoped.
g) The virtues of this service and future expansion and funding requirements for winter provision to be addressed and planned with the Commissioners, System Resilience Group (SRG) and A&E delivery board and STP.
Decisions and Actions 1. Scope and request potential contribution from the winter pressures
funding for expansion of the FIRST service. 2. FIRST assurance report was noted
Risk Rating: Amber/Green
CH/MD
To note
4.7 Mortality Policy The Mortality Policy was received and discussed
It was noted that: (i) This policy takes into account information from other Community
Trusts. (ii) Community Hospital Medical Directors and Mortality leads are
working together to developed a common approach to a Standard Operating Procedure (SOP) which aligns with the policy.
Board 30th November 2017 Attachment K2
7
Item Action Date (iii) The NHSI deadlines are being worked toward on both the policy
and the data set.
Challenge, Observations & Questions a) The policy is first class. b) Queries were raised with regard to HCT ward manager’s capability
to accurately complete the after death checklist, this is to be considered further.
c) It was confirmed that if any issues become apparent beyond the community care responsibility these will be escalated to the Medical Director in his role as Responsible Officer to refer on appropriately.
Decisions and Actions
1. Mortality Policy was approved
Risk Rating: Not applicable
4.8 Simpson Ward CQC plan The Simpson Ward CQC plan was received and discussed
It was noted that: (i) The improvement plan advised actions that have been put in place
to successfully integrate Simpson Ward from WHHT into HCT, and to take forward quality improvements.
(ii) Assurance was provided that quality improvements are in line with CQC domains to ensure delivery of a “Good” rating.
(iii) Clinical professional lead Nurse has been appointed.
Challenge, Observations & Questions a) Reasonable progress has been made in a relatively short period of
time since handover of this ward to HCT. It was acknowledged that it will take time to turnaround and a number of environmental issues are within WHHT gift to address.
b) Recent NED visit experience and observations were shared. Areas that need to be addressed were highlighted. Confirmation and assurance was given that every effort is being made to bring this ward up to HCT standards which includes supporting the staff with the cultural change required, however this will take time. The plans are for completion by early 2018 prior to CQC visit with regular updates to HGC to monitor progress.
c) More targets around the compassionate care element and the staffing establishment status to be included in the improvement plan.
d) It was acknowledged that enhanced social care is required, this is underway.
e) The risk of additional potential pressure during the winter period was highlighted. RR advised that all referrals will be managed via the bed bureau, they will gate keep the flow.
f) Clarification was given on the timeline for transfer of equipment
Board 30th November 2017 Attachment K2
8
Item Action Date and assets and the challenges in respect of the installation of Wi-Fi.
Decisions and Actions
1. More targets around the compassionate care element and the
staffing establishment status to be included in the improvement plan
2. Simpson Ward update was noted
Risk Rating: Amber/Green
TW
To note
4.9 End of Life Final Internal Audit Report The End of Life Final Internal Audit Report was received and discussed.
It was noted that: (i) This audit report has been reviewed by the Audit Committee. An
amber risk rating was issued, giving reasonable assurance that the controls in place to manage this risk are suitably designed and consistently applied.
(ii) One medium priority management action was agreed to ensure that the Palliative Care Dashboard is being used effectively and captures all appropriate data.
(iii) The planned Operational Review will review and test the progress made on the auditor recommendations.
Challenge, Observations & Questions a) It was suggested that progress has been made, however this
continues to be a work in progress that dovetails with the work on the Strategic Delivery Plan. On an ongoing basis progress will be monitored by the Strategy Implementation Steering Group.
b) The operational review attendees to receive the Steering Group minutes from the previous two meetings and the internal audit for background information prior to the review on 9th October.
c) HGC were content with the approach that was taken by the internal auditors.
Decisions and Actions
1. End of Life Final internal Audit Report was noted
Risk Rating: Not applicable
4.10 Quality Report Q1 The Quality Report Q1 was received and discussed.
It was noted that: (i) The full quality report has been revised in response to previous
comment. Highlighted achievements and risks were outlined and a revised quality dashboard was included.
Board 30th November 2017 Attachment K2
9
Item Action Date (ii) Each section has been revised to reflect KPIs supported by an
exception report. (iii) Appendices provide a highlight and further additional information
providing outcome of assurance visits and HCT contractual arrangements.
(iv) Achievements: • 97.34% of patients received harm free care whilst in the care
of HCT • 27% reduction in the number of falls in community hospitals • 2 avoidable category 2 pressure ulcers reported compared to
6 in Q4 2016/17 • 0 cases of MRSA or E.coli bloodstream infections attributable
to HCT • 4 CQUINs and 2 Quality Priorities on trajectory or met in
quarter • 0 unexpected deaths reported • 98% of patients would recommend HCT services to Friends
and Family (v) Challenges
• 11 avoidable category 3 or 4 pressure ulcers, 4 above the Quality Priority quarterly trajectory of 7
• 3 cases of C.difficile reported; RCA demonstrated no lapse in care in 2 cases
• 3 serious incidents declared, compared to 2 in Q4 2016/17 • 1 CQUIN and 2 Quality Priorities not on trajectory or partially
met in quarter; work is underway to bring these on track for Q2 • Keeping in touch visits demonstrate recruitment and retention
continues to be a challenge; HR working with staff to mitigate staff loss and ensure patient safety
(vi) The red areas on the dash board were discussed.
Challenge, Observations & Questions a) There has been a focused drive to increase the percentage of
harm free care, the resultant 97.3% is substantially above the national average and is worthy of note.
b) It was felt that the narrative around the unexpected death of a prisoner needs to be reviewed to ensure that it is appropriate.
Decisions and Actions
1. The Quality Report Q1 gives reasonable assurance and was
noted
Risk Rating: Amber/Green
4.10a Complaints update The Complaints mid Q2 update covering July and August 2017 was
received and discussed. It was noted that: (i) 30 complaints have been received from 1st July – 31st August
Board 30th November 2017 Attachment K2
10
Item Action Date 2017.
(ii) There have been no referrals to the Parliamentary and Health Service Ombudsman (PHSO) to date.
(iii) There has been one category 3 complaint to date. (iv) Four complaints have been re-opened for further investigation. (v) An overview of the category 3 and re-opened complaints was
provided. Challenge, Observations & Questions a) In respect of the complaint and underlying incident Ref 1487
further clarification was requested on the appropriateness of using mugs to serve soup and the temperature of the contents. This will be investigated further.
b) The themes and hotspots were discussed included missed visits and waiting times for PALMs. PSEG are reviewing missed visits further and work is on-going to look at different ways to report the reasons for these.
Decisions and Actions
1. Complaints mid Q2 update was noted
Risk Rating: Amber/ Green
4.10b Serious Incident (SI) Mid Q2 update The Serious Incident mid Q2 update covering the period July and August
2017 was received and discussed. It was noted that: (i) Three serious incidents were reported
• One fall • One pressure ulcer meeting SI criteria • One treatment delay causing significant harm
(ii) All investigations are underway in line with policy. (iii) A summary of learning, outcomes and actions identified to
improve practice and delivery of safe and effective patient care will be cascaded to staff.
Challenge, Observations & Questions a) A query was raised regarding any potential imported SIs from
Simpson Ward prior to the transfer from WHHT to HCT. This will be followed up.
b) The risk rating was discussed and changed to Amber/ Green as the information to hand at present does not support a Green rating this may change following further investigation and subject to further assurance being provided.
Decisions and Actions 1. Serious Incident Mid Q2 update was noted
Board 30th November 2017 Attachment K2
11
Item Action Date Risk Rating: Amber/Green
4.10c Safe Staffing mid Q2 Summary The Safe Staffing mid Q2 summary for July – August 2017 was received
and discussed. It was noted that: (i) The report includes safe staffing data and exception reports for
July and August. The main issue is the vacancy rate at Herts & Essex Hospital (HEH), a great deal of focussed work is underway to address this and retain existing staff.
(ii) The sickness rates appear high but it was confirmed that these have reduced in August although not available prior to the production of the report.
(iii) The August sickness, vacancy and pressure ulcer data is not yet available.
(iv) Full analysis of Q2 data will be provided to the November meeting.
(v) Deep dives are being undertaken for reported red areas. Challenge, Observations & Questions a) The feedback from the recent Director of HR Listening event held
at HEH was positive. The leadership has changed; this appears to be helping with the cultural change.
b) It was acknowledged that Essex as a whole has recruitment issues. HCT is working with Princess Alexandra Hospital (PAH) to develop a more structured approach to recruitment.
c) Overall staffing position in the West improved with staff moving from closed wards at St Albans.
d) There is currently no visibility regarding the safe staffing for the ICT teams. It was agreed that this would be presented quarterly to this meeting starting in November including dashboards and explanatory narrative. The changes in Herts Valleys ICT from 2nd November may well have a significant impact. A new dashboard with a wider view of indicators is being developed; this will be reviewed by the Executive team regularly through this period of change.
Decisions and Actions 1. Quarterly reports for ICT safe staffing including dashboards and
explanatory narrative. 2. Safe Staffing mid Q2 summary was noted
Risk Rating: Amber/Green
PW
14.11.17
4.11 Pressure Ulcer Q1
The Pressure Ulcer (PU) Q1 report was received and discussed. It was noted that:
Board 30th November 2017 Attachment K2
12
Item Action Date (i) There is a downward trend in the total numbers of pressure ulcers
reported. (ii) There is a reduction in avoidable category 2 pressure ulcers;
although there has been an increase in avoidable category 3 and 4 pressure ulcers.
(iii) A summary of assurance, actions and recommendations to support the Trusts aim to reduce avoidable pressure ulcers was presented.
(iv) A great deal of work is underway to further improve this position including prevention information for patients/ carers.
(v) Benchmarking data is good. (vi) Further analysis has shown that a significant number of reported
PUs (10 out of the 13) are patients in receipt of Homecare or in residential care establishments. This information has been shared with the CCG.
Challenge, Observations & Questions a) The report is well written and very clear. b) It was suggested that the reporting of PUs could be reviewed to
potentially specify where PU was acquired as with the Cdiff reporting and track the progress/ deterioration from the point at which HCT became involved.
c) Missing from the report is the clinical background for the patients which could have an impact on healing. It was reported that this work is underway.
Decisions and Actions 1. Reporting to be reviewed and amended to specify where PU was
acquired and progress since HCT intervention. 2. Pressure Ulcer Q1 report was noted
Risk Rating: Amber/Green
PW/CP
Nov 17
4.12 PLACE update
The PLACE update report was received and discussed. It was noted that: (i) Overall HCT has performed above the national average in all
assessment areas. (ii) HCT has improved scores when compared with the results for
2016. (iii) Some of the community units scored slightly below the national
target in one or more of the six areas of assessment and these will be reviewed.
(iv) A more detailed report will be provided in Q2.
Challenge, Observations & Questions a) Congratulations to all involved for this achievement. b) The issues identified around food will be reviewed further; it was
acknowledged that some of these areas are not within HCT gift.
Board 30th November 2017 Attachment K2
13
Item Action Date Decisions and Actions 1. PLACE report was noted
Risk Rating: Amber/ Green
4.13 High Level Risk Register
High Level Risk Register as at 21st August 2017 was received and discussed. It was noted that: (i) There are10 risks currently on the register (ii) One risk (Ref 319) has been de-escalated and the remaining ten
risks have not changed since the last report. (iii) There is one emergent risk (Ref 486) which is aligned to the
Inpatient units budget overspend. Challenge, Observations & Questions a) The new format provides the information in a much clearer way
and shows the outstanding actions and updates. b) Clarification was given on the outstanding skin health issue that
has remained open for more than one year. This will be addressed by the Customer Service Transformation which will provide much better resilience. Skin Health risks have been escalated within the business unit; these are being reviewed to fully understand the scoring.
c) The Executive team is asked to review the small specialist services with limited resilience and under pressure for a variety of reasons despite mitigation. To decide the way forward and to advise the Board.
d) The Executive team to decide on how the HLRR will be reported to the Board moving forward. It was suggested that a highlight version goes to the Public board to ensure transparency.
Decisions and Actions 1. Executive to review the limited resilience for the small specialist
services, decide the way forward and advise the Board accordingly.
2. Executive to review and decide how the HLRR is reported to the Board
3. The High Level Risk Register was noted Risk Rating: Not Applicable
CH MD/JO
Nov 17 Sep 17
4.14 Business Unit Performance Reviews
Board 30th November 2017 Attachment K2
14
Item Action Date The BUPR were received and discussed:
The main messages from the September 2017 BUPRs are: (i) Adults
• Activity underperformance o HVCCG future commissioning of specialist services o Skin Health o Prison o Diabetes o MediPi
Beds
o Overspend o Medical Staffing model and cover o DTOCs o HEH Staffing
ICT
o ICT Therapy waiting times – improving with backlog clearance o Working establishment & impact of increased sickness and
turnover - HV, North Herts and ULV o FIRST – Contracting and quality issues o MIU – Peaks in activity
(ii) Children’s
o Nascot Lawn – Maintaining service until 31st
Jan 2018 o Medical equipment Beds o Access to Dental within the Prison o School funding HVCCG o PALMS o Waiting times Health Visiting
Autistic Spectrum Disorder Community Paediatrics Children’s OT
Challenge, Observations & Questions a) The changes in the report summaries were well received. b) The BUPR reports correlate and corroborate risks identified in a
variety of reports to HGC along with assurance on actions being taken to mitigate the risks identified
Decisions and Actions 1. BUPRs were noted.
Risk Rating: Amber/Red
4.15 Clinical Quality Review Minutes
Board 30th November 2017 Attachment K2
15
Item Action Date The Clinic Quality Review minutes from the meeting on 11th July 2017
were received and accepted. Decision and Actions
1. The Clinical Quality Review minutes were accepted
5.0 Patient Safety & Experience 5.1 Patient Safety & Experience Group Assurance Report and Minutes
The Patient Safety & Experience Group Chair’s Assurance Report and the minutes for the meeting held on 17th August 2017 were received. It was noted that: RED
• TPP/SystmOne: Concerns regarding children transferring to HCT services with no access to records continues. SystmOne lead for HCT is working with NHS Digital, NHSE and ICO. Risk recorded on corporate risk register.
AMBER / RED
• Paediatric Liaison: Concerns regarding implementation of digital solution at WHHT. System unable to recognise time of presentation, duplicate admissions etc. Acute staff lack capacity to review data. Risks identified by the group and escalated to Designated Nurse, who will present a paper to HSCB in September 2017. HV continues to cover the service until final solution agreed.
• The Q1 medication report highlights that the number of incidents relating to insulin remains high. There is limited assurance that these incidents are investigated as robustly as they should be, or that the Management of Medication Errors is being followed. Working group formed to review process for local investigation, lessons learnt and closure of insulin-related incidents and provide assurance.
• Concerns were raised regarding reasons for missed ICT visits, including staff not reporting sickness absence in accordance with policy and poor connectivity leading to staff not completing patient records or checking tasks throughout the day. Actions agreed include staff communication around professional responsibilities and procedure for reporting sickness absence, and escalation of connectivity issues through OSMT.
AMBER / GREEN
• Three cases of CDI have been reported in year to date; none of the cases are linked and all have undergone RCA and it has been agreed will go to appeal as no lapses in care were identified.
• A reduction in the number of medication related incidents resulting in harm was noted.
GREEN
• A positive increase in the number of referrals received by Carer’s in Herts was noted.
Board 30th November 2017 Attachment K2
16
Item Action Date • The streamlined version of the Q1 Quality Report was noted. • The meeting noted an improvement in the harm free care rate
measured on the Safety Thermometer. • The Q1 inpatient falls report demonstrated a reduction in the
number of falls reported, with HCT being the fourth lowest reporter benchmarked against other trusts.
• The Patient Experience Forum will provide opportunity for external scrutiny of complaints and responses; representatives from Healthwatch and Carers in Herts will also be undertaking pieces of work on behalf of HCT.
OTHER POINTS TO NOTE
• The meeting supported the proposed HCT ENHCCG wound dressing project. SW to clarify budget responsibilities.
• Three policies were approved • The Safeguarding Children Section 11 demonstrated progressive
and innovative service developments undertaken and good practice delivered by the safeguarding team.
Challenge, Observations & Questions
a) It was acknowledged that the TTP/ SystmOne issues need a national response from NHS digital, NHSE and the ICO.
b) Ways of cascading the positive outcomes from the children’s safeguarding report to support the upcoming tender to be investigated.
Decisions and Actions 1. Ways of cascading the positive outcomes from the children’s
safeguarding report to support the upcoming tender to be investigated.
2. The Chair’s assurance report and minutes of the meeting held on 17th August 2017 were noted.
Risk Rating: Not applicable
PW
To note
5.2 Infection Prevention and Control Forum Assurance Report and Minutes
The Infection Prevention and Control Forum Assurance Report and minutes for the meeting held on 19th July 2017 were received. RED
• Water Safety – Discussions on going between HCT and HPFT regarding a shared approach following joint working around estates. Accountability to be discussed and established.
AMBER/RED
• Antibiotic Audit – concerns regarding “stop dates” for antibiotic and patient notes being accurate. Realistic trajectory targets to be set to measure improvement.
Board 30th November 2017 Attachment K2
17
Item Action Date AMBER/GREEN
• Infection Prevention and Control Training – downward trend noted through Q1. Additional training sessions have been arranged. Concerns regarding accuracy of BI portal. Team managers to be encouraged to escalate inaccuracies noted.
GREEN
• Flu Vaccination Campaign – Early planning and recruiting of flu champions. Improved methods of logging vaccination uptake to be considered. Further information on fridge space and vaccine storage to be obtained.
Challenge, Observations & Questions a) It was acknowledged that the information is slightly historic. b) Evidence and information from Australia’s experience with flu
could be used to support HCT’s flu vaccination campaign. c) No high level risks were noted
Decisions and Actions 1. The Chair’s assurance report and minutes of the meeting held on
19th July 2017 were noted.
Risk Rating: Not applicable
5.3 National Ambition to reduce Gram-Negative Blood Stream Infections 2017-18
The National Ambition to reduce Gram-Negative Blood Stream Infections 2017-18 was received and discussed It was noted that: (i) Gram-negative blood stream infections have increased by a fifth in
the last five years (NHS I, 2017). Evidence shows that these may have contributed to approximately 5,500 NHS patient deaths in 2015.
(ii) The Department of Health has set an ambitious target to reduce incidence by 50% across the system by 2021.
(iii) The local health economy has to work together to achieve this aim. An overview of the current work in place to support the initiative was given.
(iv) The reported cases in HCT Community Hospitals are low, four reported in 2015/16, one in 2016/17 and zero to date in 2017/18.
Challenge, Observations & Questions
a) It was suggested that consideration be given to including the E coli
infection data in the IBPR.
Decisions and Actions 1. Consider the inclusion of the E coli data in the IBPR moving
forward.
PW
To note
Board 30th November 2017 Attachment K2
18
Item Action Date 2. The National Ambition to reduce Gram-Negative Blood Stream
Infections 2017-18 report was noted
Risk Rating: Amber/Green
6.0 Clinical Effectiveness 6.1
Medical Revalidation Decision Making Group Terms of Reference were received and discussed. It was noted that: (i) These have been revised in line with previous feedback and
ensure that all groups are included. (ii) This group is also used for Medical Management.
Decisions and Actions 1. The Medical Revalidation Decision Making Group Terms of
Reference were reviewed and approved. Risk Rating: Not Applicable.
6.2 Medical Revalidation Decision Making Group - Committee Chair’s Assurance Report
The Committee Chair’s Assurance Report for the MRDMG meeting held on 10th August 2017 was received. It was noted that: RED
No SIs or never events involving doctors to report since the last meeting. However, the GMC had stated that following a review of the case involving the Skin Health doctor, they concluded there was no clinical case to answer. There will be a local investigation into the governance of this individual’s appointment process. The status of the individual is being reviewed.
AMBER\RED Employment processes for Doctors have been put in place. Due to lack of information there remains a lack of assurance that Doctors are competent and fit to practice. An internal audit is underway to review all medical staff currently employed and within the employment process to ensure that appraisals and qualifications are up to date and the appointment governance process has been adhered to.
Decisions and Actions 1. The Medical Revalidation Decision Making Group assurance report was noted. Risk Rating: Not Applicable
Board 30th November 2017 Attachment K2
19
Item Action Date
6.3 Clinical Effectiveness Group Chair’s Assurance Report and Minutes from the Meeting held on 7th August 2017.
The Clinical Effectiveness Group Chair’s Assurance Report and Minutes from the Meeting held on 7th August 2017 were received. It was noted that: RED
• Assurance regarding end of life training in bed-based units had not been received. A progress update will be sought from the Head of Learning & Development.
AMBER / RED
• NICE guidance and Quality Standards have been implemented; however there is limited assurance of the clinical outcomes after the implementation of NICE guidance. A prioritisation of audit of continued compliance with NICE guidance will be undertaken.
• A recent record keeping audit only provided limited assurance around the safety and completeness of clinical records in HCT services as the audit was designed to comply with IG Toolkit requirements and did not cover all aspects of record keeping. The committee supports a fuller, more focussed Trust-wide record keeping audit based on triangulation of information from SIs, complaints and review of deaths, with dip testing of any areas of non-return.
AMBER / GREEN
• The results of the IG Toolkit record keeping audit provided some assurance within the scope of the audit.
GREEN
• Policies, SOPs, guidelines and PGDs were noted and approved with some minor changes to some of the documents recommended.
OTHER POINTS TO NOTE
The national audits discussed at previous meeting provided limited assurance as there were no findings or recommendations specific to HCT arising from either audit. However it was noted that actions are being taken at local level to provide assurance regarding the quality and safety of service delivery.
Challenge, Observations & Questions
a) It was confirmed that in addition to the internal audit programme
and IG toolkit there is a programme of dip testing for record keeping. It is apparent that this information is not being used to triangulate upwards, to provide the organisational assurance and learning. This was discussed further in the BUPR meeting and links are to be investigated to align both information streams to provide assurance. The Quality leads and internal audit are liaising to pull this together.
Board 30th November 2017 Attachment K2
20
Item Action Date Decisions and Actions 1. Triangulation of internal audit and dip test result to provide
organisational assurance and share lessons learned. 2. Clinical Effectiveness Group Chair’s Assurance Report and
Minutes from the Meeting were noted Risk Rating: Not applicable
JO
To note
7. Key Items for Noting
None
8. Key Items For Escalation or Further Action
The small specialist service resilience to be reviewed by the Executive team.
9. Supporting Papers
The following supporting papers were received for information: SP1 Item 4.10 Quality Report Quarter1- full report
10. Date of Next Meeting(s)
Assurance meetings: 21 Nov 2017 2.00 – 5.00 Boardroom, Howard Court 16 Jan 2018 2.00 – 5.00 Boardroom, Howard Court 20 March 2018 2.00 – 5.00 Boardroom, Howard Court Operational Reviews Health Visiting and School Nursing 22nd September from 2.00 pm Boardroom, Howard Court, Welwyn Garden City AL7 1BW Palliative and End of Life Care to assess compliance against the CQC action plan on the 9
th October 2017
A provisional date for February 2018 has been set to look at the improved ways of delivering quality care being introduced by Integrated Community Teams.
11. Meeting Summary – Informal Feedback From Observers
None
HCT INTEGRATED BOARD PERFORMANCE
REPORT October 2017
1
HCT IBPR Final October 2017
Board 30th November 2017 Attachment K3
Section
1 Trust Scorecard
2 Key Messages
3 Quality KPIs
4 Performance KPIs Inc. National & Local indicators
5 Learning & Development KPIs
6 Workforce & Finance KPIs
Appendix 1. Safe Staffing Report
2
3
Indicator
2017/18
Target /
Threshold
Current period
performance
Current
Period
RAG
YTD RAG
Trend from
previous
month
Trend over time
HCT
Benchmarking
Rank
Trusts
Participating
TRUST SCORECARD 17/18
G G
6
10
15
(Overall Turnover)
4
18
17
16
17
14
16
(Overall
Turnover)
17Absence Rate 3.6% 3.90% A A
Underlying Staff turnover (Voluntary resignations excluding retirements, redundancy and the end of
FTCs) A �12% 14.6% A
�
�
�% posts vacant
(vacant WTE/budgeted WTE).10% 10.40% A A
Workforce &
Finance
% of staff who have received an appraisal in the last 12 months 90% 89.0%
�
A A
% of staff completing Information Governance training (Rolling Year) 95% 87.4% A A
�
�
% of all clinical and medical relevant staff (all clinical staff including staff in supervisory roles
requiring a clinical registration) will undertake
Level 2 safeguarding adults
90% 92.3% G G
97.0% G G �
L & D
% staff who have undertaken mandatory training 90.0% 89.3% A A �
% of staff who have undertaken level 1 / 2 safeguarding adults training every 3 years 90% 97.3%
% of eligible staff trained at appropriated level of safeguarding children in accordance with IC
document Level 1, Level 2, Level 395%
10
Patient waiting list (including Consultant & Non-consultant led services) 92.0% 96.5% G
�All data entered on S1 within 24 hours of contact >=90% 87.7% A A
G �
Community Hospitals - % of NHS (health) bed days lost due to delayed transfers of care
5%
for health delays
4% by Mar 18
Total 16.9%
(Health 11.1%
HCS 5.7%
Both 0.1%)
R R �
Perform
ance
Community Hospitals - Average length of stay in HCT community hospital - ALL Stroke (Rehab
Pathway)42 Days
G RCommunity Hospitals - Average length of stay in HCT community hospital - Non Stroke (Rehab
Pathway)21 days 21.8
No of avoidable category 2 pressure ulcers acquired in HCT care
30% reduction
on baseline from
2016/2017
0 G G
37.5 �
�
G G
98% 1
�
8For information 12 �
0 G
5 14
Quality
% of patients receiving harm free care (New Harms only) Compliant �
G G �
C.difficile cases occurring post 3 days following admission into HCT bed based facilities (i.e.
acquired in our facility)
Friends and Family test 90%
Full Year 6
monthly
trajectory
1 - Sep
�G
98.2% G G
Number of complaints received in month
Scorecard Key Messages Quality KPIsPerformance
KPIsL&D KPIs
Workforce & Finance KPIs
Appendices
October 2017 Key Messages
Performance highlights
• 98% of patients receiving harm free care (new harms).
• No C.diff cases reported in October
• Stroke and Non-stroke LOS within rehab pathway thresholds.
• 1 and 2.5 year health reviews now back on target.
• 96.5% of patients waiting within 18 weeks for their initial appointment.
• Childrens safeguarding training levels above target.
Areas for Board review
• Two avoidable Category 3 Pressure ulcers reported in October
• DTOC rate above the 5% threshold with 11.1% health delays recorded in October.
• Trust below target of 90% for data entry within 24 hours of contact with 87.0% recorded.
• HCT above national target for health visiting caseloads.
• Nursing P2 and Therapies P2 and P3 not achieved in October.
• Staff Mandatory training figures below target with 89% in October
• Underlying Staff turnover over threshold and remained at 14.6% recorded in October.
• Absence rate increased to 3.90% in October.
Scorecard Key Messages Quality KPIsPerformance
KPIsL&D KPIs
Workforce & Finance KPIs
Appendices
4
5
Ref Indicator
Quality - Clinical Governance
Q22 Number of inpatient falls resulting in moderate or more severe harm (Quarterly) For information
Q20 Percentage of inpatient deaths compared to all discharges (Quarterly) For information
Q18 No of avoidable category 2 pressure ulcers acquired in HCT care
30% reduction on
baseline from
2016/17
0 G G
Q21 Number of inpatient falls by 1000 OBD (Quarterly) For information
Q19 No of avoidable category 3 or 4 pressure ulcers acquired in HCT care 0 2 R R �
�
G G
2017/18
Target /
Threshold
Current
period
performance
Current
Period
RAG
YTD RAG
Trend
from
previous
month
Trend over time
�Q1 % of patients receiving harm free care (New Harms only) Compliant 98.2%
�
�
�9
Q8
GG
Q13 Number of patient-related incidents reported in month For information 397
Q12 The number of SI's that remain open to HCT For information
Reduction in the prevalence of CAUTI, based on safety thermometer data 1% 0.18% G G
100% G
�
Q10The percentage of SIs that have 60-day RCA and action plans completed and
submitted to commissioner within 60 days. Reported monthly
Monthly
90% �G
Q9The number of Serious Incidents reported in month to the Commissioner against the
SI policyFor information 4
Q6 % of relevant patients screened for MRSA (excluding respite patients).Monthly
95% �100.0% G G
�
�
Q4 C.diff cases rates per 1000 occupied bed days For information 0.00
Q5 Compliance with Hand hygiene in all Community Hospitals will be > 95% 95% 99.3% G G
0 G
�
Q3C.difficile cases occurring post 3 days following admission into HCT bed based
facilities (i.e. acquired in our facility)
Full Year 6
Monthly trajectory
0 - Oct
Q2 Number of Avoidable MRSA bacteraemia cases in year for HCT 0 0
�G
Scorecard Key Messages Quality KPIsPerformance
KPIsL&D KPIs
Workforce & Finance KPIs
Appendices
6
Ref Indicator
2017/18
Target /
Threshold
Current
period
performance
Current
Period
RAG
YTD RAG
Trend
from
previous
month
Trend over time
Q24 Number of clinical negligence claims closed in the quarter (Quarterly) For information
Q23 Number of clinical negligence claims received in quarter (Quarterly)6
YTD
�
Q26 Number of complaints received in month For information �
Q27 Proportion of complaints resolved within timescale agreed with complainant 80%
Monthly100% G
12
G
Quality - Patient Experience
Q25 Friends and Family test >95%
G
�
Q28 Number of PALS enquiries (for HCT services) reported monthly For information �
Q29 Number of compliments received Quarterly (Quarterly) For information 1335
HCT were over the 5% threshold after recording 11.1% health delays in October. This is an increase of 2.3 days from previous month. The units with
the biggest delays were Herts & Essex (9.4%) for East and North and St Peters (24.7%) for Herts Valley. These two units combined for 226 bed days
out of the 607 days lost in October which equates to 37%. The most common reasons for delay in October were Domiciliary (129 days) and Continuing
health care Assessment (182 days). When looking at reasons beyond HCT control, i.e. Patient choice or self-funding care for Residential/Nursing
Home and Homecare, the health delays improved to 7%.
Actions in place to support patient flow and achievement of improved DTOC position:
• Weekly Teleconferences with all system partners to agree total number of community DTOC and next actions to discharge. (Daily in Herts Valley
with CCG and Herts County Council)
• Additional weekly internal HCT conference call with Exec representation for each bed based unit
• Daily call from bed bureau to each unit to review delayed patients or patients approaching EDD to ensure expected actions are completed on time
• The new structure of the Adults Business Unit inpatients portfolio is now in place with all leadership posts recruited to
• All therapy leads and ward managers have objectives built into appraisal to reflect the Red to Green programme
Ongoing work-streams
• Red 2 Green has been relaunched at Herts and Essex Hospital in Sept 2017
• Review of internal professional standards for inpatient units
• Task and finish groups now established around top 3 constraints i.e. CHC, therapy & patient choice.
(P10) Non-Stroke ALOS
HCT were over the ALOS thresholds for Non-stroke patients in October. HCT recorded an ALOS of 29 days for non-stroke patients which was an
increase of a day on previous month. Eight patients stayed 80 days or more and of these patients, two stayed over 100 days. These patient were only
able to rehab for 98 days combined due to health. The overall length of stay improved to 21 days under the rehab pathway.
P13) Estimated discharge date (EDD) achievement
The majority of non-met EDD are linked with delayed transfers of care issues with 52% of patients achieving their estimated discharge date. This is a
decrease of 3% from previous month. When patients who did not have a delayed transfer of care are excluded, 71% of patients were discharged on or
before their EDD. This is being escalated to the locality managers of each hospital unit and EDD processes are currently being reviewed.
Scorecard Key Messages Quality KPIsPerformance
KPIsL&D KPIs
Workforce & Finance KPIs
Appendices
11
12
(P16) Health Visiting - Average caseload size
Caseload figures improved to 403. 10 of 15 HV teams successfully recruiting to 5% over budgeted caseload to cope with natural turnover. Hemel
Hempstead & Garston team are having the most difficulty despite offering a Golden Handshake initiative for Hemel. Budgeted Caseload will reduce to
398 approx. by end October without taking into account actual caseload which includes adjusted figures for mat leaves and Long term sickness , 80%
of management time for Team Leads and 20% education time Community Practice Teachers. Recruitment and greater skill mix of Nursery Nurses
continues. Exception reporting on all amber and red KPI’s in place with robust recovery plans to achieve green by end November 17.
(P31, P32) Smoking advice & intervention
HCT are meeting the thresholds for recording smoking status, however referrals to Hertfordshire Stop Smoking Service are still under performing and
this is currently being reviewed and monitored with HCC for 17/18.
(P37-P42) Urgent Nursing and Therapy referral priorities
Significant work is underway to manage the increasing demand for the service. Clinic type approaches have been introduced to improve through put
into the service, staff are being utilised to support areas with increased demand including Watford. The therapy service is now fully recruited Work is
ongoing as part of the redesign programme to ensure that robust and efficient triage and referral allocation processes are implemented. Internal
monitoring of all breaches is reviewed three times weekly. Significant progress has been made in addressing the historic therapy waiting list which is
positively impacting upon the number of breaches within the service.
(P43) All data entered on S1 within 24 hours of contact
Currently HCT are recording 87% of contacts within 24 hours and this is a small decrease from last month. There is a focus to improve the efficiency
of recording and this will be escalated to the Business Units who have access to the information at staff level. The recording improves to 90% at 48
hours of contact.
Scorecard Key Messages Quality KPIsPerformance
KPIsL&D KPIs
Workforce & Finance KPIs
Appendices
13
Ref Indicator
2017/18
Target /
Threshold
Current
period
performance
Current
Period
RAG
YTD RAG
Trend from
previous
month
Trend over time
�
�
A
A
A
�
�
�
A A
A A
�
G
�G
�
�
G
A A
G
G
G
G
G
�
�
�
G
�
�
L4 Infection control 90% 86.5% A
L6% of eligible staff trained at appropriated level of safeguarding children
in accordance with IC document Level 1, Level 2, Level 395% 97.0% G G
L5 Basic life support 90% 89.8%
G
L1 % staff who have undertaken mandatory training 90% 89.3%
L3 Patient moving and handling 90% 87.5% A
A
L8% of staff who have undertaken level 1 /2 safeguarding adults training at
induction95% 95.6% G G
G
90% 92.3%
L9% of staff who have undertaken level 1 / 2 safeguarding adults training
every 3 years90% 97.3%
L7% of eligible staff who have undertaken safeguarding children
supervision appropriate to their role (Quarterly)95%
L14 % of staff completing Information Governance training (Rolling Year) 95% 87.4%
L13 % of relevant staff who have undertaken PREVENT training 90% 90.5%
L12 % of relevant staff who have undertaken MCA training 95% 97.8%
L2% of eligible staff who have received mandatory fire training in the last
12 months90% 89.2%
L11 Staff undertaken DOLS training in previous 3 years 95% 99.3%
L10% of all clinical and medical relevant staff (all clinical staff including staff
in supervisory roles requiring a clinical registration) will undertake Level
2 safeguarding adults
�
L16 Equality & Diversity Training 90% 94.9% G G �
L15 Conflict resolution training 90% 94.0% G G
Learning & Development
Scorecard Key Messages Quality KPIsPerformance
KPIsL&D KPIs
Workforce & Finance KPIs
Appendices
L&D EXCEPTION REPORT (16 KPIs RAG RATED) 0 7 8
ACTION
(L1) % Staff who have undertaken mandatory training
Overall staff mandatory training levels dropped to 89% and under the 90% target due to a slight drop in numbers across key training areas for October.
(L2, L3, L4, L5) Patient Moving & handling, Infection control and Infection control
Patient Moving and Handling and basic life support training increased steadily in October and are within 3% of target. Infection control training also
improved, however fire training dropped slightly but is still within 1% of target.
(L14) % of staff completing Information Governance training (Rolling Year)
IG training was achieved for 2016-17 and is currently at 87.4% for October. Questionnaire currently being reviewed and refresher reminders sent – the IG
group has asked managers to ensure that all staff have completed their 17/18 training by 31/12/17.
Appraisal rates increased to 89% in October and just 2% under the 90% target. Appraisal rates are increasing as the management cascade to all staff
continues. Monitoring and regular training continues.
(W7) % Posts Vacant
The Trust’s vacancy rate has fallen in October 2017 to 10.4% against a 10% target. This is in part due to a reduction of 30 wte budgeted establishment in
the adult community teams in Herts Valley, which is being implemented through taking out vacancies and reallocating staff across the patch. The
remaining vacancies in these services, which had been on hold for this redeployment, can now be recruited to. Recent work to improve recruitment has
included distributing 500 posters to Community Centres, libraries, supermarkets etc. across Hertfordshire. Four job fairs have been attended in the last two
months and the Trust has also continued to increase its social media presence
(W10) Underlying Staff turnover
Staff turnover rates are currently at 14.62% for underlying turnover and 23.16% for total turnover (which includes TUPE transfers out). Under the NHSI
Nurse Retention Programme, the Trust’s current priority is a 90 Day Improvement Programme in Herts and Essex Hospital, including running focus groups
talking to staff about retention issues. A wider retention workshop for all nurses is taking place on 4th December and the introduction of a nursing careers
clinic is being explored. The stretch target is to reduce nursing turnover from 21.8% to 17% by August 2018
(W12) Absence Rate
In-month sickness absence for October has increased back to above the 3.6% target at 3.9%. Both Business Units are progressing work to reduce
absence rates, with the Adult Business Unit sending letters out to all staff benchmarking and rag rating their individual sickness, whilst the Children’s and
young person’s Business Unit is focusing on raising the skills of managers to address absence. This is in additional to the wider Trust Health and
Wellbeing programme and staff flu campaign.
(W14) Retained Surplus
An adjustment was requested to the retained earnings position in quarter one, relating to the transfer of the Parkway property to NHS Property Services.
The transfer was reflected as a £1,206k deficit which is adjusted back in the performance against the control total resulting in zero impact to the Trust for
the property transfer. As a result the Trust is reporting a deficit position year to date of £1,113k which is £1,204k behind plan.
(W15) Aged Debtors
Overall debt has increased by £938k during October 2017 to an overall total of £2,462k. The increase is due to a number of more recently raised invoices
within the 0-30 and 31-60 days categories remaining unpaid.
Capital expenditure is £787k at the end of month 7 which is below the Trust's submitted plan for 2017-18. Expenditure to date relates mainly to schemes
which have continued from 2016-17 together with the current year's IT equipment replacement programme.
Safe Staffing Community Hospital Dashboard 17-18Oct-17
Day Night
Target
Staffing Quality data
19
Safe Staffing Exception Report
Staffing Levels
Langley House: Additional Health care assistant hours for patient requiring one to one care overnight throughout the month. St Peters Ward had two
specials through-out the night and day
Vacancy rates
Herts & Essex Hospital reported 4.78 WTE Band 5 vacancies as at 10th October. Additional budget has been identified for Simpson ward from 1st
October. Recruitment is currently underway
Bank & Agency use
Herts & Essex Hospital continues to have high levels of agency use to cover vacancies. Langley House reported a high number of complex patients on
the ward during October (36 patients deemed at high risk of falling due to age and frailty, and 20 patients deemed as having other complex needs)
Moderate/Severe falls
One patient at Potters Bar hospital had a fall resulting in a fracture neck of femur (severe harm); however it is unlikely that this fall will meet Serious
incidence criteria as all preventative measures had been put into place
.
Serious Incidents
One Serious Incident was raised regarding safeguarding concerns reported by the patient’s family to Adult Care Services regarding care delivered whilst
at Langley House. This incident will be fully investigated through the SI investigation process
Scorecard Key Messages Quality KPIsPerformance
KPIsL&D KPIs
Workforce & Finance KPIs
Appendices
- 1 -
Board 30th November 2017 Attachment K4
FINANCE REPORT TO THE STRATEGY AND RESOURCES COMMITTEE
Title: Month 7 Finance Report (October 2017)
Sponsoring Director: Director of Finance
Author(s): Finance Department
Purpose: The purpose of the report is to provide the Board with HCT’s financial position as at Month 7 – 2017/18.
Action required by the Board:
The Board is asked to note the Trust’s financial position as at 31st October 2017.
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP Appendices SOF Glossary
- 2 -
Finance Strategy & Resources Report October 2017 (Month 7)
Contents
Section Title
1 Director of Finance Message
2 Clinical Income
3 Pay Expenditure
4 Non Pay Expenditure
5 Cost Improvement Programme (CIP)
6 Statement of Financial Position
- Cash Flow Statement
- Capital Expenditure
- Aged Receivables
- Better Payments Practice Code (BPPC) Performance
7 Single Oversight Framework (SOF)
8 Glossary
Finance Strategy & Resources Report October 2017 (Month 7)
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
- 3 -
Finance Strategy & Resources Report October 2017 (Month 7)
1 Director of Finance Message
The Trust performance against the control total is £2K ahead of
plan in month 7 and £5K ahead of plan year to date.
The Trust performance against the control total is £2K ahead of plan in month 7, and £5K ahead of plan year to date. As a result of this, the Trust's single oversight risk ratingis maintained at a 1.
An adjustment was requested to our retained earnings position in quarter one, relating to the transfer of the Parkway property to NHS Property Services. The transfer wasreflected as a £1,206K deficit which is adjusted back in the performance against the control total resulting in zero impact to the Trust for the property transfer.
Due to the above the Trust is reporting a year to date deficit position of £1,113K which is £1,204K behind plan.
Year to date the Trust had a favourable position relating to
Revenue from Patient Care Activities of £334K.
Revenue from Patient Care Activity is ahead of plan as at month 7 by £334K due to additional income (non block related) and £538K adverse in month due to a budgetvirement relating to SACH beds income. The additional income year to date is offset against additional expenditure incurred. Clinical income mainly consists of block incomeand therefore only small deviations from budget are expected to materialise during the year.
The income position includes £412K as at month 7 for the planned recognition of the Sustainability and Transformation Fund (STF) allocation.
The year to date CIP delivery for the Trust as at month 7 is
£3,028K as per plan.
At the end of month 7, the Trust had delivered £3,028K of CIPs against a plan of £3,028K. Of the CIP savings delivered to date, £1,587K has been delivered non-recurrently and £1,440K recurrently. The slippage against the recurrent plan is mainly due to central CIP schemes including the SLA renegotiation and Customer Service Transformation projects.
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
- 4 -
Table 1: Income and Expenditure Summary
Finance Strategy & Resources Report October 2017 (Month 7)
INCOME & EXPENDITURE SUMMARY Budget Actual Variance Budget Actual Variance Budget Forecast Variance£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Income 12,291 11,761 (530) 82,466 82,857 390 140,294 141,475 1,181
Add back a l l I&E Impairments/ (reversa ls ) 0 0 0 0 0 0 177 177 0Remove capi ta l donations/grants I&E impact 4 4 0 28 31 3 48 51 3Add back ga ins/ (losses ) from transfers by absorption 0 0 0 0 1,206 1,206 0 1,206 1,206
Control Total 66 68 2 119 124 5 1,972 1,975 3
In Month Year to Date Forecast
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
- 5 -
Table 2: Income and Expenditure Performance
The Trust has planned to realise a benefit of £958K in M12 due to the sale of two properties. The sale of the two properties was agreed in the Capital Plan in December 2016.
- 6 -
Finance Strategy & Resources Report October 2017 (Month 7)
Table 3: Performance against Budget by Business Units
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
Business Units Budget Actual Variance Key Driver of Movement Budget Actual Variance Key Driver of Movement Budget Actual Variance Key Driver of Movement£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Core Adult Services (5,579) (5,369) 210Low spend on pay due to non recurrent vacancies and funding for 1-1 care.
(39,944) (39,077) 866
Low spend on pay due to non recurrent vacancies, reduction in agency spend and funding for 1-1 care.
(67,822) (66,991) 831
Low spend on pay due to vacancies and anticipated reduction temporary staffing. Forecast includes winter pressure costs.
Children's Services (2,401) (2,373) 28Low spend on pay due to non recurrent vacancies.
(17,024) (16,792) 232Low spend on pay due to non recurrent vacancies.
(29,049) (28,953) 95
Favourable variance due to non recurrent vacancies partly offset by an increase in recruitment for Health Visitors.
Corporate Services (2,051) (2,205) (154)
£83K CIP slippage for CST & SLAs. £50K Additional funding to be issued centrally to realign cost pressures.
(14,189) (14,834) (646)£583K CIP slippage for CST & SLAs. Additional funding to be issued centrally to realign cost pressures.
(23,089) (25,062) (1,972)
£745K additional funding to be issued centrally to realign cost pressures. £600K Increased management consultancy and interim staff spend to support Trust tender submissions£500K CIP slippage for the CST scheme£150K Finance system change costs.
Other Income 10,651 10,542 (108)£66K CQUIN underperformance and NCA income below plan.
75,102 74,950 (152)£66K CQUIN underperformance and NCA income below plan.
128,122 127,580 (542)
£229K CQUIN underperformance. £250k Income reduction due to Rapid Response Service overhead and £50k due to the loss of the MSK service. NCA underperformance, partly offset by increased MIU activity within the Business Units.
(870) 439 1,310Release of Trust Contingency Reserves.
Other Adjustments (468) (437) 31 Small variance on depreciation (3,203) (4,272) (1,069)
£1.2M Parkway transfer to NHSPS offset in the adjusted position, partly offset by the underspend variance on depreciation.
(5,545) (6,472) (927)
£1.2M Parkway transfer to NHSPS offset in the adjusted position, partly offset by the underspend variance on depreciation.
Net Surplus/(Deficit)
62 64 2 91 (1,113) (1,204) 1,747 541 (1,206)
*Other income includes block, NCA's and Education Funding**Other adjustments includes PDC, Depreciation, amortisation, Finance costs, PDC Dividend, Transfer of Property
In Month Year to Date Year End Forecast
- 7 -
Finance Strategy & Resources Report October 2017 (Month 7)
Table 4: Analysis of Continuing Risks and Opportunities to Trust's Financial Position
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
Risk No.Risk/Opportunity Identification Process
RAG Rating/Risk
Score
Financial Value£'000
Risk Assessed Value £'000
Basis for Financial AssessmentExec Lead
Actions to Mitigate
1Planned sale of properties does not deliver expected savings.
Capital Plan 5 (958) (192)Expected savings calculated by Financial Accountant and Head of Estates as per the Estates Strategic Plan
PBMaintaining and reporting progress in line with the Estates Strategic Plan
2Cost Improvement Plans - Customer Service Transformation
CIP Tracker 25 (500) (500) CIP Project Plan MD
Close monitoring of project milestones against the plan, bringing action due dates forward where possible.
3Cost Improvement Plans - Renegotiate E&NH Trust Service Level Agreement
CIP Tracker 16 (500) (320) CIP Project Plan MDOngoing discussions are taking place with the Trust.
4 100% of CQUIN targets are not achieved. CQUIN Tracker 16 (467) (299) Quarterly reporting CH Quarterly monitoring of all schemes
5Loss of overhead for Rapid Response Service Decommissioning in October 2017
SLR 12 (500) (240) Business Modelling PB
Ongoing discussions are taking place with Commissioners and NHSI regarding recovery of the loss in contribution.
Green 1-3Amber-Green 4-7Amber 8-13Amber-Red 14-17Red 18-25
The Trust is currently forecasting a surplus of £541K. When adjusting for the transfer of the Parkway property to NHSPS and depreciation on donated assets the forecast surplus is £1,975K.Current risks and opportunities to the Trust 's forecast outturn position are detailed below:
- 8 -
Finance Strategy & Resources Report October 2017 (Month 7)
Table 5: Income Performance
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
2 Clinical Income (Patient Care Activity)
The trust had a year to date favourable position relating to
Revenue from Patient Care Activities of £334K.
The Trust had a year to date favourable position relating to Revenue from Patient Care Activities of £334K and £538K adverse in month. The year to date favourable position includes £394K for estates recharges continuingover-performance in PALMS, Hertfordshire School Nursing and ICT. The income is partly offset by under performance against plan within Homefirst, ESD, Children's SLT and E&N Physio and OT. Furthermore, the Block Income for both CCG's was impacted by the reduction of their services commencing in October 2017 such as TB Service and Rapid Response.
The in month position is mainly due to a budget virement relating to SACH funding and CQUIN underperformance of £64K.
The income position includes £412K income year to date for the planned recognition of the Sustainability and Transformation Fund (STF) allocation.
The forecast out-turn position for the Trust's Patient Care Activity is a favourable variance of £1,036K which includes £700K for estates recharges and £500K additional Local Authority income for School Nursing and PALMs.The additional income is partly reduced by the reduction in services for the MSK and Rapid Response £343K, CQUIN under-performance of £229k for HV and E&NH CCG, slippage on income for Children's SLT £255K, Homefirst£278K, NCA £150K and PACE £230K.
INCOME PERFORMANCE Budget Actual Variance Budget Actual Variance Budget Forecast Variance£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Education, Tra ining and Research 62 62 1 431 425 (7) 712 725 13STF Income 92 92 0 412 412 0 916 916 0Other Cash Revenue 57 64 7 392 455 62 666 798 132Total Other Operating Revenue 211 218 8 1,236 1,291 56 2,294 2,439 145
TOTAL EBITDA Income 12,291 11,761 (530) 82,466 82,857 390 140,294 141,475 1,181
Investment Revenue 3 3 1 18 18 0 31 32 0
Total Income 12,294 11,764 (529) 82,485 82,875 390 140,325 141,506 1,181
In Month Year to Date Forecast
- 9 -
Finance Strategy & Resources Report October 2017 (Month 7)
Table 6: Pay Cost by Business Unit
Table 7: Bank & Agency by Division
The Trust agency spend is below the NHSI Agency Ceiling threshold by £176K in month and above the threshold by £128K year to date. The Medical Agency spend breached the NHSI threshold by £47K YTD due to pressures within Community Medical Staffing. In line with the above recruitment plans, the year-end trust agency spend is forecasted to be £8,642K, which is below the £8,710 target by £68K. Furthermore, the medical agency spend is forecasted to be £836K, which is above the £811K target by £25K.
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
3 Pay Expenditure
The pay position as at month 7 is £765K
favourable and £1,104K favourable year to date.
The Trust posted a pay expenditure underspend of £765K in month 7 and £1,104K underspend year to date. The pay underspend reflects a reduction in the temporary spend run-rate as a result of theclosure of SACH beds, funding drawn from reserves towards specialising 1:1 care, non-recurrent vacancies in ICT's and continuing vacancies predominately within School Nursing, Health Visiting, Dental,Continuing Care Carers, Nascot Lawn, Physio and SLT.
The Trust had an under-establishment of 270 wte in month 7 of which 187 wte was covered by temporary Bank and Agency staff. Monthly detailed reviews are taking place at cost centre level toensure the agency spend is reduced compared to the year to date run rate as well as the 16-17 spend.
The forecast out-turn position for the Trust's pay position is an overspend of £351K. The forecast has been updated to reflect commissioning changes to the MSK, Rapid Response Service and additional Simpson Ward running costs, which is also reflected in the income position. The bank and agency forecast is expected to increase further due to the additional capacity required for the Simpson wardwhich is partly offset against the full recruitment of Health Visitors and Nursery Nurses from October 2017 and adjustments for non recurrent spend during April to July 2017.
Finance Strategy & Resources Report October 2017 (Month 7)
Table 12: Non Pay Analysis
* This includes: Management Consultancy, Mental Health Contracts, Patient Transport/Ambulance Services, Pharmacy Contracts, Recharge - Estates, SLA, Recharge - Procurement, Substance Abuse Contracts, and Training - Other Training Staff.
** This includes: Computer Maintenance, Hire of Premises, Lease Cars, Miscellaneous Expenses, Mobile Phone Costs, Operational Services, Postage - Franking Costs, Telephone Costs.
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
4 Non Pay Expenditure
Non-pay recorded a £204K overspend in month 7 and a
£1,577K overspend year to date.
The Trust has delivered an unfavourable non-pay expenditure variance of £204K in month 7 and £1,577K year to date. The overspend year to date includes £956K spend for Establishment includes slippageagainst plan for central CIP schemes and contingency cost pressures. Premises is overspend by £645K which includes rental offset by income, SLA and Building Repairs and Maintenance costs pressures.Furthermore, the overspend of £254K year to date within Clinical Supplies and Services is driven by increased unit price costs for continence products, volume increases in radiology diagnostic testing andissuing prescriptions as well as higher purchases of equipment, appliances and instruments. The favourable variance within other non pay includes the release of the Bad Debts provision.
The forecast out-turn unfavourable variance of £1,764K includes, £600K spend within other non pay for increased management consultancy and interim staff spend to support Trust tender submissions, £150Ktowards system costs, £700K expenditure which is offset by CCG income within estates and £500K slippage on the CST CIP scheme. Pressures continue within the clinical supplies at £465K as described above and Business Units are working with Budget Holders in order to minimise this spend going forwards.
In Month £'000 Year to Date £'000 Forecast (£'000)
- 13 -
Finance Strategy & Resources Report October 2017 (Month 7)
Finance Strategy & Resources Report October 2017 (Month 7)
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
5 CIP
At the end of month 7, the Trust had delivered £3,028K of CIPs against a plan of £3,028K. Of the CIP savings delivered to date, £1,587 has been delivered non-recurrently and £1,440K recurrently. The slippage against the recurrent plan is mainly due to central CIP schemes including the SLA renegotiation and Customer Service Transformation projects which has been recovered via vacancy underspends within the various Business Units. Business Units are working closely with the Project Management Office to closely manage deviations from plan and over recover CIPs in future months.
The year to date CIP delivery for the Trust as at month 7 is £3,208k as per
plan.
Table 13: CIP by Programme Table 16: Cumulative CIP Performance
Plan Actual Variance Plan Actual Variance Plan Actual Variance
In Month Actual £'000 Year to Date £'000 Forecast Year End Achievement £'000
In Month £'000 Year to Date £'000 Forecast Year End Achievement £'000
In Month £'000 Year to Date £'000 Forecast Year End Achievement £'000
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
- 14 -
Table 17: Statement of Financial Position
Finance Strategy & Resources Report October 2017 (Month 7)
6 Statement of Financial Position
Statement of Financial Position Opening Balance Closing Balance Forecast£000's £000's £000's
NON-CURRENT ASSETS:
Intangible Assets 595 455 357
Property, Plant and Equipment 60,087 57,616 63,036TOTAL Non Current Assets 60,682 58,462 63,393CURRENT ASSETS:
Trade and Other Receivables: NHS 5,405 4,377 2,126The settlement of a number of outstanding prior year invoices has reduced NHS receivables.
Trade and Other Receivables: Non NHS 1,204 1,669 474This is due to prepayments as at the year end most of the invoices are finished and the new ones come in early in next year (e.g. system one invoice received in May 17)
Cash and Cash Equivalents: GBS/NLF 18,772 21,068 21,644Cash and Cash Equivalents: Other 1 5 0TOTAL Current Assets 25,382 27,119 24,244CURRENT LIABILITIESTrade and Other Payables: Capital (336) (31) (298) The fall in capital payables refIects the reduced capital programme in the first half of 2017-18.
Trade and Other Payables: Non Capital (13,601) (14,040) (13,758) The increase is mainly due to increased accruals for NHS property services as no invoices received
Borrowings (176) (176) (176)
Provisions (144) (101) (245) Provisions relating to redundancy and CQUIN have been utilised.
Other Liabilities: Deferred Income (1,405) (2,057) (1,244) The movement reflects normal quarterly invoices deferral.
Total Current Liabilities (15,662) (16,405) (15,721)TOTAL ASSETS LESS CURRENT LIABILITIES 70,402 69,176 71,916NON-CURRENT LIABILITIES:Borrowings (2,532) (2,444) (2,356) The first scheuled loan repayment was made in September.Provisions (1,031) (1,009) (653) Unwinding of the discount.Total Non-Current Liabilities (3,563) (3,453) (3,009)TOTAL NET ASSETS EMPLOYED 66,839 65,723 68,907
Financed by:Public Dividend Capital 1,131 1,131 1,131Revaluation Reserve 17,221 17,193 18,996 The transfer of the balance for Parkway to the Income and Expenditure Reserve.Other Reserves 4,946 4,947 4,947Income and Expenditure Reserve 43,541 42,452 43,833 The movement on the Income and Expenditure Reserve relates to the operating position for
September 2017 less the transfer of the Revaluation Reserve balance for Parkway.
TOTAL TAXPAYERS' AND OTHERS' EQUITY 66,839 65,723 68,907
Non Current Assets have reduced in value due to the transfer of Parkway to NHS Property Services and the disposal of IT equipment; additionally the depreciation charge is currently greater than expenditure from the capital programme for 2017-18.
Cash balances have increased as a result of the settlement of prior year receivables and reduced capital activity up to month 7
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
- 15 -
Table 18: Cash Flow Statement
Finance Strategy & Resources Report October 2017 (Month 7)
Cashflow StatementPlan Actual Variance
£'000 £'000 £'000
Operating Surplus/(Deficit) 1,124 1,150 26Depreciation and Amortisation 2,101 2,057 (44)Impairments and Reversals 0 0 0Operating Cashflow before working capital 3,225 3,207 (18)
Movements in working capital(Increase)/Decrease in Trade and Other Receivables 815 4 (811)Increase/(Decrease) in Trade and Other Payables 551 1,260 709Increase/(Decrease) in Movement in Provisions (8) (44) (36)Net Cash Flows from working capital 1,358 1,221 (137)
Net Cash Inflow/(Outflow) from Operating Activities 4,583 4,428 (155)
Interest Received 18 18 0(Payments) for Property, Plant and Equipment (4,194) (1,092) 3,102(Payments) for Intangible Assets 0 0 0Proceeds from sales of PPE and investment property 0 84 84Net Cash Inflow/(Outflow) from Investing Activities (4,176) (990) 3,102
Loans from Department of Health - repaid (88) (88) 0Interest Paid (28) (29) (1)Dividend (Paid)/Refunded (874) (1,020) (146)Net Cash Inflow/(Outflow) from Financing Activities (990) (1,137) (147)
NET INCREASE/(DECREASE) IN CASH AND CASH EQUIVALENTS (583) 2,300 2,799
Cash and Cash Equivalents at Beginning of the Period 17,061 18,773 1,712
Cash and Cash Equivalents at the end of the period 16,478 21,073 4,511
Plan Actual VarianceLiquidity Ratio (days) 17 28 11
Year to Date
Year to Date
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
- 16 -
Table 19: Capital Expenditure
Finance Strategy & Resources Report October 2017 (Month 7)
Capital Expenditure by Programme
Plan Actual Variance Plan Forecast Variance£000's £000's £000's £000's £000's £000's
• The Trust can add the net book value of disposals from the Fixed Asset Register within year to the capital programme but for reporting purposes this is deducted to arrive at the agreed Capital Resource Limit of £4,633k. In 2017-18 to date HCT has disposals of £136k which means that the Trust is able to spend £4,769k on capital schemes.
• Capital expenditure is £787k at the end of month 7 which is below the Trust's submitted plan for 2017-18. Expenditure to date relates mainly to schemes which have continued from 2016-17 together with the current year's IT equipment replacement programme.
• Planned expenditure reflects the capital plan for 2017-18 as submitted to NHSI. This plan included additional investment above the level of forecast depreciation; NHSI has now approved additional expenditure of £1,134k bringing the current capital resource limit to a total of £4,633k.
• At the Capital Investment Group at the end of October 2017 new schemes were approved which are expected to have finished by the end of March 2017.
• We still have £707k unallocated at this time as we need to account for amendments on the budgets of the existing schemes.
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
Finance Strategy & Resources Report October 2017 (Month 7)
NHS CCGs 428 886 84 75 1,473 60%
431 309 0 58 798 32%57 33 0 101 191 8%
916 1,228 84 235 2,462 100%
Percentage of total debt 37% 50% 3% 10% 100%-140 1,156 -55 -23 938
Overall debt has increased by £938k during October 2017 to an overall total of £2,462k. The increase is due to a number of more recently raised invoices within the 0-30 and 31-60 days categories remaining unpaid. These include charges relating to Rapid Response, Simpson Ward, First Service and Additional capacity; there are no known issues to delay payment so full settlement is expected. The level of debt over 90 days has decreased to £235k with the proportion of this category of debt to overall debt also decreasing from 17% to 10%. Debt within this category relates to a small number of outstanding issues which are being actively pursued for resolution. The main items are invoices raised to local authorities in respect of GUM activity, to Cambridgeshire & Peterborough CCG relating to rent increases invoiced by NHS Property Services and Hertsmere Borough Council relating to the Elstree redevelopment project. Residual debt with Royal Free NHS FT has reduced to £42k.
% Total Debt
NHS OtherNon NHS Total
Movement in Month £000
Debtor Type 0-30 Days £000's31-60 Days
£000's61-90 Days
£000's> 90 Days £000's Total Debt £000's
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
- 18 -
Table 23: BPPC Performance
Table 24: Cash Performance and Rolling Projection
Finance Strategy & Resources Report October 2017 (Month 7)
April May June July Aug Sept Oct Nov Dec Jan Feb MarTarget 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%% Volume 94% 91% 92% 92% 93% 92% 92%% Value 98% 76% 82% 84% 85% 87% 89%Monthly
April May June July Aug Sept Oct Nov Dec Jan Feb MarTarget 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%% Volume 94% 88% 94% 94% 94% 91% 92%% Value 98% 64% 99% 96% 95% 97% 99%
The Trust follows up those authorisers who are holding up payment of invoices, addresses any training isues and identifies any invoices on hold for unjustifiable reasons.
The BPPC performance in month for volume has increased from 91% to 92% while the cumulative performance has remained constant at 92%. Performance for value has improved during September from 97% to 99% and that has improved cumulative performance from 87% to 89%.
The cash balance of £21,073k at the end of October 2017 is above the planned figure for the year. This is mainly due to the delay in finalising the capital programme, the majority of which is now scheduled for the latter part of the financial year. It is anticipated that cash outlay will increase over plan in the next few months with the forecast cash balance for the end of the year being in line with the plan. The liquidity ratio has remained above the plan at 28 days. This is due to current working capital balances and operating expenses being more favourable than originally forecast.
£7,000
£9,000
£11,000
£13,000
£15,000
£17,000
£19,000
£21,000
£23,000
Apr 17 May 17 Jun 17 Jul 17 Aug 17 Sep 17 Oct 17 Nov 17 Dec 17 Jan 18 Feb 18 Mar 18
Cash Performance and Rolling Projection
Plan Actual Forecast
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
- 19 -
Table 25: Single Oversight Risk Rating
Finance Strategy & Resources Report October 2017 (Month 7)
7 Single Oversight Framework (SOF)The Single Oversight Framework
Risk Rating for the Trust is 1. The Single Oversight Framework Risk Rating (SOF) is the NHS Improvement’s approach, to overseeing NHS providers. The SOF assesses the financial performance of providers via the “Use of Resources Metrics (UOR)” comprising the following five metrics:
• Liquidity Ratio• Capital Servicing Capacity• I&E Margin• I&E Distance from Plan• Agency
The overall metric is calculated by attaching a 20% weighting to each category.
The Single oversight risk rating for the Trust as at month 7 has been maintained at 1. The Trust is forecasting to achieve the year end control total and risk rating of 1 as perthe plan.
Plan Actual Variance Plan Actual Variance
Capital service cover rating 1 1 1 1Liquidity rating 1 1 1 1I&E margin rating 2 2 1 1Distance from financial plan 1 2Agency rating 1 2 1 1
Overall Rating 1 1
YTD Forecast
Contents DoF Message Clinical Income Pay Non Pay CIP SOFP SOF Appendices Glossary
- 20 -
DoLs - Deprivation of Liberty Safeguarding
CQUIN - Commissioning for Quality and Innovation
IDAT - Integrated Discharge and Admissions Team
CCG - Clinical Commissioning Group
MEN C - Meningococcal C
PALMS - Positive Behaviour Autism Learning Disability and Mental Health Service
NHSI - National Health Service Improvement
CIP - Cost Improvement Programme
OT - Occupational Therapy
PT - Physio Therapy
CAPEX - Capital Expenditure Programme
ICT - Integrated Community Teams
BUPR - Business Unit Performance Review
ENHT - East and North Herts Trust
FP10 - Community Prescription
BPPC - Better Payment Practice Code
SACH - St Alban's Community Hospital
LEARNING AND DEVELOPMENT ANNUAL REPORT 2016-17
Learning and Development Department Howard Court
14 Tewin Road Welwyn Garden City
AL7 1 BW
Board 30th November 2017 Attachment K5
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
2
CONTENTS
1 Introduction .............................................................................................................. 3 2 The Team ................................................................................................................ 3
3. Details of monitoring against frameworks ................................................................ 4 3.1 Induction .......................................................................................................... 4 3.2 Local Induction ................................................................................................ 4 3.3 Statutory and Mandatory Training ................................................................... 4 Table 1 – Mandatory training delivery ........................................................................ 5
3.4 Essential and Regulatory Training ................................................................... 6 3.5 Mandatory Training Compliance ...................................................................... 6 Table 2 – Mandatory training Compliance by Business Unit ...................................... 6 3.6 Delivery against Learning and Development Plan ........................................... 6 3.7 Mandatory Training Costs ............................................................................... 7
Table 3 – Spend on Mandatory Training Provision 2016-17 ...................................... 7
4 Delivery against the Learning and Development Plan ............................................. 7 5 Regulatory Requirements –Quality Commission (CQC), Quality and CQUINs........ 8
6 Quality Control of Training Provision ....................................................................... 8 7 Learning and Development Agreement ................................................................... 9
Table 4: Mentors at 31 3 17 ..................................................................................... 10
8 Management and Leadership ................................................................................ 11 9 Development of Band 1-4 staff ................................................................................... 13
Administrative Learning and Support Needs ............................................................ 13
10 Non-Medical Prescribing ........................................................................................... 14 13 University Modules and Short Courses..................................................................... 14 14 External Training ...................................................................................................... 16
15 Internal Clinical Training ........................................................................................... 16
16 Key Skills Training .................................................................................................... 18 17 E-learning ................................................................................................................. 18 18 Supporting IT competence ........................................................................................ 18 19 Appraisal ................................................................................................................... 18
21 Conclusion ................................................................................................................ 19 22 Challenges for 2017-18 ............................................................................................ 19
Table 5 – Clinical Training at Regional Universities ................................................. 15 Table 6 - External spend .......................................................................................... 16 Table 7 - Internal training ......................................................................................... 16 APPENDICES
Appendix 2 – Mandatory Training Planned vs. Places Provided ………………..20
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
3
1 Introduction
2016-17 has been a busy year for the Learning and Development Team. Resources have been maintained but demands for training continue to increase. Our key achievements for 2016/17 were:
We maintained mandatory training compliance across the year with an average compliance of 92% across the year. A highlight is that 95% of Trust staff have received Prevent Training, the highest in Hertfordshire
We introduced a ‘2 day Clinical Development Programme’ to enable nurses in Adult Services to receive an annual update of clinical skills such as Diabetes, Continence and Syringe Driver in a ‘One Stop’ format
We worked with the Transformation Team to create bespoke e-learning for HCT staff on User Self-Management for roll-out in 2017/18
We launched our Leaders Forum for all staff that identify themselves as leaders; to complement our Senior Leaders Forum and enable the Senior Management Team to engage directly with our Leaders
We joined the Trainee Nursing Associates Fast Follower programme with 4 Health Care Assistants gaining places on the programme.
Our first Learning and Development Apprentice achieved her Level 2 Apprenticeship in Business Administration. She has gone on to a higher level apprenticeship with another service in the Trust
We reviewed the Induction programme, shortening it and making it more flexible. We estimate that this has freed up 200 days of staff time each year
We supported the recruitment of the first 10 directly employed apprentices for the Trust including an apprentice within the Learning and Development Team. A further 34 staff members enrolled on an apprenticeship programme
2 The Team
At the end of the year, headcount for the department stands at 15 people, made up of 12.80 wte as follows
Head of Learning and Development 1.00 Head of Leadership and Management Development 0.60
Education Leads 3.80
Learning and Development Coordinators 3.0
Senior Learning and Development Administrators 2.37
Learning and Development Administrator 1.0
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
4
Apprentice 1.0
There has been an increase in establish with additional resource for leadership, including a new post ‘Head of Leadership and Management Development’ and support for pre-reg students (funded via NMET funds)
3. Details of monitoring against frameworks
3.1 Induction
Corporate Induction runs monthly at Robertson House only as we no longer have access to multiple sites. New employees are required to attend within 3 months of joining with most line managers booking staff on the programme before staff join the Trust. Average time to Induction is 8 weeks. 400 new starters received I induction checklists and 470 bookings were made for each day of Induction Reporting is completed monthly and a 98% average monthly compliance was achieved across the year against a target of 98%. 5 staff were overdue of Induction at year end. A new structure for Corporate Induction was implemented in September 2016 to build flexibility for staff that had already completed (or transferred compliance for) mandatory training. It included focussing Day 2 of Safeguarding Adults and Children and removing Day 3 and it is estimated that this will release 200 days of new starter time back into practice. The Trust implemented the automated IAT process in September 2016. This includes the transfer of mandatory training compliance from previous employers for Trust starters (and onwards from the Trust), thus reducing time to induction. This has started slowly as most staff continue to complete full induction but it is anticipated that, as this process becomes better known, further gains can be made. 50 new starters brought competences with them, against the 400 staff recruited
3.2 Local Induction
The Local induction checklist is updated and agreed by the Health and Safety committee as required. Competency frameworks are sent to new nursing and clinical support staff in ICT Teams and Bed Bases. 400 Checklists were sent to new starters in 2016-17, as significant reduction in the 600 sent the previous year.
3.3 Statutory and Mandatory Training
All statutory and mandatory training continues to be aligned to the Core Skills Training Framework (CSTF) against the following standards;
Fire – Level 1
Conflict Resolution
Patient Moving and Handling – Level 1 and Level 2
Safeguarding Adults – Level 1 and Level 2
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
Safeguarding Children – Level 1, Level 2 and Level 3
Health, Safety and Welfare – Level 1
Equality and Diversity – Level 1
Information Governance – Level 1
Infection Control – Level 1 and Level 2
Prevent – Level 3,4,5 (WRAP training)
In addition to these topics, the Trust mandatory training requirements include Mental Capacity Act and Deprivation of Liberty Safeguards as understanding of these areas is identified as key for all clinical staff.
Table 1 – Mandatory training delivery
Training e-learning Face to face In service training and assessments
Anaphylaxis
Basic Life Support
Conflict Resolution Full Course
Conflict Resolution Update
Equality and Diversity Induction
Fire and induction/one stop
Fire With Evacuation (All Bed Bases)
Infection Control and induction/one stop
Mental Capacity Act/DOLS
Patient Handling
Safeguarding Adults Level 1/2
induction/one stop
Safeguarding Adults Level 3
Safeguarding Children Level 1/2
and Induction
Safeguarding Children Level 3
and HSCB training
Information Governance Induction & one stop
Prevent (level 1) (level 3,4,5 – WRAP training at Induction/ One Stop
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
6
3.4 Essential and Regulatory Training
The Essential and Regulatory Training Framework identifies training required by specific groups of staff including clinical programmes such as mentorship update and Anaphylaxis. We will work in 2017/18 to increase the range of essential training requirements to include more clinical topics and to include these onto BI reporting.
3.5 Mandatory Training Compliance
Compliance has been maintained across the year with an average compliance of 92%
Table 2 – Mandatory training Compliance by Business Unit
Business Unit Compliance at 31.3.17
Children and Young People 94%
Corporate 97%
Adult Services 90%
Overall Compliance 92%
Refreshers are now generated automatically from the BI system advising staff of training that is due in the next 3 months, as well as training that is overdue Details of compliance by topic can be viewed in Appendix 1.
3.6 Delivery against Learning and Development Plan
Appendix 2 shows training planned against provided. Differences in booked and attended show the level of cancellation/DNA. Higher levels of provision than planned reflect additional provision to assist services to achieve compliance.
93% 93%
92%
91% 91%
90%
90%
91%
92%
90%
90%
92%
91%
90%
87%
88%
89%
90%
91%
92%
93%
94%
Apr-16
May-16
Jun-16
Jul-16
Aug-16
Sep-16
Oct-16
Nov-16
Dec-16
Jan-17
Feb-17
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
7
3.7 Mandatory Training Costs
Table 3 – Spend on Mandatory Training Provision 2016-17
Training Spend 16/17 Spend 15/16
BLS/ILS/Anaphylaxis £52,437.50
£47,047.50
Conflict Resolution £16,345.00
£18,485.00
Fire £1,113.00
£3,923.50
Patient Handling £44,190.40
£49,916.55
First Aid £1,146.00
£1,945.00
Misc. £1,600.00 £977
TOTAL
£116,831.90
£127,242.05
The reductions in training costs reflect the exceptional costs in 15/16 of remedial training to bring up mandatory training compliance. Resuscitation costs increased to reflect the changes to competence requirements to include AED
4 Delivery against the Learning and Development Plan
4.1 Learning and Development – Support for Trust Strategy
Additional resource for leadership was made available this year reflecting the Trust commitment to Leadership Development and supporting the Effective Leadership component of Effective Teams
E-learning (812 User Self-Management and Patient Activation) has been developed to support the Self-Management workstream. This will be launched in June 2017
4.2 Training Needs Analysis (TNA)
The TNA data comes from several sources – external requirements at national, regional and local level, as well as those identified internally by the organisation, service, team and individual. The TNA process has been further developed to improve returns and accuracy. Managers were asked about individual requirements for external training, clinical modules and apprenticeship programmes, whilst Clinical Quality Leads completed the TNA for the large scale clinical training required by services. The result has achieved a more accurate reflection of requirements.
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
8
5 Regulatory Requirements –Quality Commission (CQC), Quality and CQUINs
Mandatory training – see above o Following an update of Resuscitation Council Guidance for
community and inpatient units the requirements for training were updated
Registered nurses in Bed Bases are completing Immediate Life Support
All other clinical staff in Adult Services receive information on using a Defibrillator.
o The End of Life Cquin focussed on staff confidence to have difficult
conversations and this was delivered by the Macmillan Education Team
Quality Priorities for 16/17 included o Increase the number of new nurses joining the trust trained to be
competent to deliver insulin medication. The target of 80% was not met (increase from 24-54% over the year). Difficulties with recruitment within the Diabetes Team reduced capacity to deliver training so this training was commissioned from the University of Hertfordshire. In addition to the training for Health Care Assistants was provided by the University of Hertfordshire. This priority identified training for new staff; update training was also provided at the Clinical Update days
o Increase the number of staff in Community hospitals, Integrated
Community Teams and children’s services trained and assessed as competent to deliver intravenous (IV) therapy – 62% received an annual update against a target of 70%. The requirements for update training are currently under review by the Intravenous Therapy Group.
6 Quality Control of Training Provision
6.1 Contracts Resuscitation Training was tendered this year based on the new Resuscitation Council requirements. The tender was awarded again to ECG Ltd.
6.2 Evaluation Survey Monkey has been used throughout the year to support evaluation of programmes. This has improved the quality of the reporting enabling quantitative reporting on the quality of the training. Pre/post confidence measures have been included enabling demonstration of the immediate impact. Most evaluation is completed on paper and entered by the Learning and Development team. An impact evaluation of Health Coaching Training was completed online giving positive feedback.
6.4 Equity of Access
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
9
The increase in e-learning reduces the requirements for individuals to travel across the county to complete training. Disability requirements are tailored to individual need.
6.5 Reporting A regular programme of reporting is in place
IBPR reporting to the Board compliance in Appraisal, Fire, Safeguarding Adults- (at Induction, all staff and level C for safeguarding champions), Mental Capacity Act Training, Infection Control, Information Governance, Patient Moving and Handling, Prevent, Resuscitation, Equality and Diversity. Safeguarding Children compliance information is also provided to the quality team for inclusion.
Business Unit Performance Reporting – Appraisal, Fire, Moving and Handling, Resuscitation, Conflict Resolution, Infection Control Information Governance, Equality and Diversity, MCA, Safeguarding Adults (at Induction, all staff and level C for safeguarding champions), Prevent, Safeguarding children at relevant level, with exception reporting of services below 50% compliance.
4 monthly and annual reporting to the Workforce and OD committee – all items on the statutory and mandatory training framework and delivery against the Leadership plan.
IBPR and BUPR reports are generated automatically by the BI system giving consistency across relevant templates. ‘Mandatory Training by Employee’ continues to be the most requested report in the BI portal, with 2 other training reports in the top 10 of BI reports.
7 Learning and Development Agreement
The Learning and Development agreement, between Health Education East of England and HCT, identifies the responsibilities of the Trust to provide high quality practice placements for SHA commissioned students in return to access to CPD funding and Deanery funding for medical staff.
7.1 Annual Monitoring The Annual QIPF process to consider the quality of placements and education provided by the Trust took place in February 2017. This included a peer review process between HCT and HPFT which enabled the Trust to recognise its own good practice and learn from colleague. The final report RAG rated the Trust as 6 Green Ratings, 1 Amber Green Rating, 1 Amber rating, 0 Red Ratings. This compares to the previous year when Trust had 2 Green, 3 Amber and 1 Red Rating. This improvement in the ratings given to the Trust is a result of delivery of a comprehensive action plan, including
Raising the profile of pre-registration activity with the Board and Executive – including via Workforce and OD and Learning and Development reports, engagement with Professional Clinical Leaders Group and other professional fora.
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
10
Significantly increasing the proportion of Nursing Mentors that meet the requirements of the NMC, without which it is not possible to accept students. Addition of Mentorship and Mentorship Triennial Review to the BI reporting system and including the figures in mandatory training reporting
Students being given nebula login to enable access to local information
Rollout of smartcards to students in bed bases to enable access to SystmOne
Provision of login details to the Trust intranet for all students to enable access to policies and student communications
Increased engagement with AHP services hosting students and development of Clinical Facilitators Register to mirror that of Nursing Mentors Register
Providing funds from NMET funds to support services to provide excellent clinical placements. This funding has been used to purchase resources, backfill for development activities and training for staff members.
The feedback report from Health Education England highlighted particularly the excellent feedback from students on the quality of placements they receive within the Trust The new Health Education England Quality Framework is being implemented in 2017/18.
7.2 Pre-registration Students Over 500 Pre –registration students were supported across the trust during 2016/17 for a total of 3300 weeks. This includes pre-registration students on nursing, physiotherapy, speech and language therapy, occupational therapy and dietetics as well as the Trust’s own staff completing specialist practice programmes. Student days are held at Potters Bar for all students on placement in the Trust with talks from practitioners on their specialist area. This also provides students with an opportunity to discuss any issues they may have in placement. This is an ideal opportunity to engage with students about employment within the Trust and HR have been included in the programmes to offer this.
Table 4: Mentors at 31 3 17
Meets both update and TR requirements 169 58%
Meets TR requirements only 27 9%
Meets update but not TR requirements 68 24%
Does not meet update nor TR requirement 25 9%
Grand Total 316 100%
More than 95% of staff meet the requirement of Triennial Review and 84% for Annual updates. The Nursing and Midwifery Council will be consulting in 2016/17 on the structures and processes for supporting student nurses in
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
11
practice. This is likely to impact on the current requirements for mentorship training and triennial review.
8 Management and Leadership
The Effective Leadership project was initiated as part of the Effective Teams Transformation stream. Progress against milestones reported into PMO and the Workforce and Organisational Development Strategy Steering Group as part of the assurance process. The project consists of 3 strands: leadership capability, leadership development and Talent management. In order to deliver the project and respond to increasing OD demands, a whole time Education Lead post was recruited to support the Head of Leadership and Management Development.
The Healthcare Leadership 360° tool assessing leadership competence against a set of standards has been carried out in Adults SMT and children’s SMT. Each manager received individual feedback on performance and then group feedback on team performance. Development plans were put in place. Plans for using the tool on the next tier of managers have been agreed.
A range of internal and external leadership and management programmes were delivered throughout the year against the plan.
The Senior Management Development programme was refreshed and the audience extended to include Deputy General Managers and Heads of Service. Topics were agreed in co-design with the facilitators NHS Elect with the aim of developing cohesive and capable leadership.
The Open Leadership Masterclass supported by internal experts and NHS Elect were delivered monthly covering a range of leadership and management topics.
The contract for externally facilitated Action learning sets was retendered and the provision increased to enable more managers to access the support. They are attended by 60 service managers and Heads of Service. The basic unit of action learning is a set of participants who learn with and from each other by working on real problems and engaging in group reflection on their experiences. Action Learning Sets continue to consider opportunities for innovation, and the impact of wider NHS changes (the “bigger picture”) to reflect the strategic roles of set members.
44 team leaders and first line managers completed HCT’s Making a Difference-Foundations in Management and Leadership programme undertaking modules, change projects, patient observations, Belbin profiling, shadowing, action learning and LF 360°.
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
12
The 4th Supervising and Leading for Success programme for band 4/5 staff was attended by 20 staff. This programme continues to be positively evaluated and we will look at how this can be funded via the Apprenticeship Levy going forwards.
Leadership interventions were identified, delivered and evaluated as the organisation and business needs were identified for example workshops on MBTI, Belbin, root cause analysis, team building facilitation, mobile working and appraisal.
To understand the role of a clinical leader, the Edward Jenner Leadership Academy Self-directed e-Learning programmes were promoted to all staff. It included 6 modules based on the National NHS Healthcare Leadership Framework.
The quarterly Senior Leaders Forum continued to build a collaborative effective senior leadership team focussing on key organisational priorities and developments. These were well attended and evaluated. And included external partner perspectives.
The Leaders Forum became established and is running twice each year. It ensures that key messages continue to be cascaded and is attended by approximately 100 leaders and managers at each event. The concept of Glimpses of Brilliance (GOBs) continues to be used across the Trust to highlight good practice.
The Annual Leaders Conference was attended by over 130 leaders in HCT with inspirational key note speakers helping us celebrate our successes. Gavin Oates inspired us and challenged us to make a difference by channelling our inner “Mary Poppins or Mr Banks”
A number of staff accessed the Leadership Academy programmes which provided accredited qualifications in management and Leadership
A local franchised model for delivering the Leadership Academy Mary Seacole programme was implemented with internal facilitators trained and system partners working together to coordinate and deliver the programme to our staff at a significantly reduced cost.
Support was provided to the NHS Management Graduate training schemes by providing orientation experiences. Whilst we achieved accreditation to host a strategic placement trainee no trainees came to us for placement. This was due to demand of placements exceeding trainee’s available and geographical challenges.
HCT agreed a 2 year SLA with the local authority to host HCC graduate trainees, supporting the business function of operational business units.
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
13
System working with STP partners has progressed with the locality OD events; Mary Seacole project and work on the Hemel Hub, however resourcing of these remain an issue.
9 Development of Band 1-4 staff
Funding has been received from the Workforce Partnership to support the development of apprenticeships and Band 1-4 staff in HCT
Administrative Learning and Support Needs
The Admin Development Group have been very active during 2016/17 and achievements include:
Administration Conference 140 administrative staff from across the Trust attended the first Administration Conference. They heard Keynote Speaker Neil Moses exhort them to “Unleash the tiger within and unmask your potential”. Overall, participants gave the day an 85% confidence to apply their learning from the day. In view of the excellent feedback and demand from staff that were unable to attend; a further conference will be held in winter 2017
A dedicated Admin Forum page is now on the intranet
A bank of Administrative Objectives were developed and are available via AT-Performance for appraisers and staff to use.
Apprenticeships
The Trust has engaged in the use of NVQs/Apprenticeships since 2015. The aim is to have well trained staff with the skills to do the job and qualifications recognising their knowledge, abilities and skills. Apprenticeships will provide career progression routes initially for non-registered clinical workforce and the administration team supporting HCT whilst meeting the standards required of the Trust e.g. CQC and NHS contract requirements; Talent for Care and Widening Participation etc.
Following recruitment of a replacement Education Lead, a review of responsibilities has increased the resources within the team being used to support Apprenticeships and to prepare for the implementation of the Apprenticeship Levy.
HCT are currently using the following Apprenticeships:-
Business Administration
Medical Administration
Customer Services
Health and Social Care
Allied Health Professional Support Worker
Project Management
Assistant Practitioner
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
14
Table 5: Apprenticeship Starters
Year Nos
2015 – 2016 44
2016 - 2017 40
An Apprenticeship Plan has been developed for implementation during 2017-2020 and it is anticipated that this will lead to a significant increase in the numbers of apprenticeships started by Trust staff. We will use the opportunities within our Apprenticeship Plan to market HCT as an excellent employer of choice and obtain value for money from the Apprenticeship Levy funds.
Care Certificate
Changes to Apprenticeships means the new standards for the Healthcare Support Worker Apprenticeship at Level 2 will include the Care Certificate and the Trusts Healthcare Competencies. 54 new staff members completed their Care Certificate during 2016/17
New Developments
The Trust will work with Bedfordshire University to help develop new standards for Health Visitors Apprenticeship.
We are currently gauging interest in a number of new Higher Level Apprenticeships which will become available in 2018 e.g. Podiatry, OT and Physio. The aim is to create a high quality Apprenticeship Career Progression Pathways, whilst preparing the Trusts staff for the challenge of increasing demands on Community Services.
10 Non-Medical Prescribing
11 members of staff from HCT are currently undertaking the V300 Non-Medical Prescribing Programme (extended) and three the V150 (nurse formulary) at the University of Herts. The Specialist Practice (District Nursing) programme has been amended to provide the V300 programme at the request of the Trust, instead of the V150 programme required for the qualification. 190 places were taken on CPD updates and medicines management programmes A ‘user group’ has been created in AT-learning which identifies all Independent Prescribers and allow monitoring of their CPD completion.
13 University Modules and Short Courses
Clinical modules and skills courses were commissioned from University of Hertfordshire and University of Bedfordshire to a total of approximately £160 000. This was a significant reduction from the £290 000 received the previous year. The table below shows activity at the regional universities – it can be noted that
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
15
most is spent on short courses with a particular focus on diabetes and intravenous therapy. Additional funds were provided by the Workforce Partnership to support Specialist Community Practice – District Nursing, Health Visiting, School Nursing and Community Children’s Nursing
Table 6 – Clinical Training at Regional Universities
Activity name No attended
UoH Diabetes (short course) 122
UoH Intravenous Therapy (Full Day) 78
UoH Intravenous Therapy Update 165
UoH Intravenous Cannulation and Phlebotomy 104
UoH Intravenous Champions Day 3
Other short courses
ARU Clinical Supervision in Care Practice 40
UoH Acupuncture Update 15
UoH Assessment and management of respiratory patients in the community 14
UoH Childhood Immunisation and Vaccination 1
UoH Dementia Champions 7
UoH Knee Masterclass (short course) 15
UoH Managing Back Pain in the Community 6
UoH Movement and Posture for HCA's 4
UoH Musculoskeletal Pathologies for HCAs 9
Modules
UoB Advancing Healthcare Practice: Concepts and Principles Level 7 1
UoB Evidence Based Healthcare Practice 1
UoB History Taking and Assessment Skills Level 6 8
UoH Advanced Decision Making in Health and Social Care 1
UoH CPAD 1 and CPAD 5 4
UOH Non-Medical Prescribing V150 (Module) 3
UoH Non-Medical Prescribing (Nurses) (Module) 11
UoH Preparation for Mentorship (Module) 15
UoH Leg Ulcer Management - A Competency Based Course 1
UoH Minor Illness Autonomous Practice 1
Specialist Practice
UoH Specialist Community Nursing BSc Hons (Children's Community Nursing) 2
UoH Specialist Community Nursing BSc Hons (District Nursing) 6
UoH Specialist Community Nursing BSc Hons (School Nursing) - part time 3
No out of region funds were made available from the Workforce Partnership to fund training not available at local universities such that all external training was funded directly by the Trust.
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
16
14 External Training
Money was allocated and in agreement with the relevant GM to ensure that the funds were spent in ways that linked to BU priorities.
Table 7 - External spend
Business Unit Amount
CYP £ 13,659.00
adults £ 8,731.50
corporate £ 9,113.80
consultants £ 6,366.00
Grand Total £ 37,870.30
Leadership Development
£ 39,022.00
15 Internal Clinical Training
4000 face to face training places were provided in 2016/17. There has been some changes in courses with the most participants reflecting the high priority given in 2016/17 to palliative care, health coaching and UNICEF breastfeeding training. The clinical 2 day update programme began in October 2016 and numbers attending this training are planned to increase in 2017/18
Table 8 - Internal training
Activity name No attended
Palliative Care Advance Care Planning Workshop 475
Carers working with 334
Mentorship Update 295
Induction Dementia Training 277
HV Developmental dysplasia of hip (DDH) 254
HV Programme UNICEF Breastfeeding and relationship building UPDATE 196
Health Coaching x 2 Days 135
Mentorship - Triennial Review 108
Palliative Care - EOL Champions 105
School Nurse Development Day 99
Clinical 2 Day Update programme 90
Nursing Revalidation Information and Guidance 82
Continence Programme Urinary Catheterisation & Principles of Care 74
Looked After Children Health Assessment training for Health Visitors 61
Syringe Driver Training (New Staff) 58
Meridian Training Programme 55
Medication management workshop 54
Continence (New Starter) 53
Palliative Care & EoL Care (Allied Health professionals) 53
School Nurse Sustain Steps to Excellence 53
School Nurse Immunisation Update 52
Palliative Care Day 1 and 2 (x 2 Days New starters) 49
Pressure Ulcer Programme for HCA's 49
Wound Care (New Starters) 47
Leg Ulcer Programme - Part 1 & Part 2 (2 day programme) 46
Injection Technique Training 45
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
17
Prescribing CPD Forums 44
School Nurse - Nasal Flu 43
Wound Care Education Programme for Health Care Assistants and Therapists 41
Long Term Conditions (New starter) 40
Care Certificate Induction Day for HCA's 38
ICT Clinical Effectiveness Programme 37
Wound Care Management Programme for Qualified Staff 36
Prescribing Update 34
Solihull training for School Nurses (Both days must be attended) 32
LMWH training for HCA's ( Heparin) 31
Syringe Driver (Pump) Training Device Users update (McKinley T34) 31
Palliative Care Dementia and EOL Care 30
Falls Prevention 28
Tongue Tie Training 28
Looked After Children Health Assessment training for School Nurses 27
Phlebotomy (Venepuncture) 26
Carbs Awareness Training 25
Mental Health First Aid Lite 25
HV Programme - Family Partnership Model Supervision facilitators Training 22
Palliative Emergencies 22
Health Coaching Update 20
HV Programme - Solihull (2 days both dates to be attended) 19
Leg Ulcer Skills Enhancement Update for Experienced Practitioners 18
HV Programme UNICEF training for HVAs and Reception staff only 17
HV Programme - ASQ communication day 16
New Immunisers Course 16
Health Visitor Clinical Day 15
MaPPS training 13
Top to Toe 13
Balance Rehabilitation 12
Falls Champions Training 12
Gluing and Wound Care 12
Pressure Ulcer Awareness Briefing 12
User Self-management Kick Off 11
HV Preceptorship training 10
Jaundice Training 10
Pulmonary Rehabilitation 10
Wound Care & Assessment (CQUIN) 10
Blood Glucose Monitoring Programme (NOVA) 8
Diabetes Update for School Nursing 8
Sickle Cell Update for School Nursing 8
Management of Respiratory Conditions in Childhood 6
Leg Ulcer In-Service Training (6 Modules) 5
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
18
16 Key Skills Training
Appraisal skills for new appraisers continues as the most attended course with demand for Pre-retirement and e-roster training increasing
Table 9 – Key Skills Training
Activity name No attended
Appraiser Training (New Appraisers) 121
E-Rostering Training 79
Pre-Retirement Course 41
DEC Full Training (suitable for newly appointed DECs) 37
Appraisal for Appraisees - preparing for your Appraisal 23
Developing Resilience within the NHS 23
TRAC Training 21
Workplace Health Champion Training 11
AT-Performance Practical Training 8
Loggist Training 8
First Aid at Work 7
NHSP/E-Roster Training 7
17 E-learning
5000 e-learning modules were completed in 2016-17 (a reduction of 30% on 2015-16). This drop can be accounted for by larger numbers of staff completing training with a 3 year refresher period during 2015-16; these are not required to complete modules again in 2016/17.
18 Supporting IT competence
The Trust has been without an IT trainer because of the retirement of the previous post holder. The Trust is rolling out the NHS IT training portal which provides online interactive training on windows packages, including the capability of the Trust to develop bespoke e-learning. The Portal includes very short video clips to demonstrate particular functions and links to these are highlighted on the Trust Intranet site.
19 Appraisal
Appraisal rates have fluctuated between 86 and 91% during the year, with an average month end compliance of 88% and year end figure of 88.4%. The Trust continues to not meet the target of 90% but average compliance has risen by 4% since 15-16. The requirement for staff to have an appraisal to achieve incremental progression has had an impact but less than anticipated. The 2016 staff survey identified a significant improvement in the quality of appraisal experience for staff members. Training of appraisers continues and appears to be impacting on this measure. The training also focusses on the use of the Service Plan as the source of objectives.
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
19
21 Conclusion
Mandatory Training has continued to be top of the agenda for Learning and Development this year but clinical competence is becoming more important and responding to this can be seen in the increasing clinical programmes. The Team continues to work to ensure that the training provided meets the requirements of all staff groups – the volume of training in all areas continues to increase.
22 Challenges for 2017-18
The Workforce and OD delivery plan for 2017-18 identifies the following deliverables relevant to Learning and Development
Objective 2016/17 deliverables
When Achieved (Qtr. 17/18)
Build individual and organisational capability through Learning and Development
Support delivery of mandatory training compliance Q4
Deliver training programmes to support the CQUINs Q4
Work with system partners to implement the Apprenticeship Levy
Q4
Develop and deliver development programmes to equip staff for new service models under the Trust Strategy and STP Plan
Q4
Support excellent clinical placements for pre- Q4
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
20
registration students
Retain and attract a talented workforce through Model Employment Practices
Review the recording and reporting system for appraisal and identify alternative options
Q4
Provide workforce support to the bids for Bedfordshire Community Services and Hertfordshire Children’s Services
Q4
Support implementation of the customer services transformation
Q4
Become a high performance organisation through excellent Leadership and Talent Management
Deliver 2017/18 Board Development Programme Q4
Implement leadership interventions to develop effective teams
Q4
Roll out the Healthcare Leadership model 360 Q4
Identify and develop opportunities for system wide leadership development
Q4
Develop system of talent management at leadership level
Q4
The following will also impact: A removal of funding from Health Education England, particularly with respect
funds at University of Hertfordshire will impact on the opportunities available to staff members who are unable to access specialist training at local universities
The new HEE Quality Framework Review will require a review of current student placement quality against these new standards.
Ongoing requirements for Leadership and Management Development, particularly with respect to Effective Teams and support for the roll out of the Adult and Children Delivery Models
An increase in demand for system wide OD interventions without identified additional resourcing
Delivery of the User Self Management CQUIN and quality priorities with roll out of e-learning and face to face training
Plans to raise managers’ awareness to expect mandatory training competences from previous employers to reduce training required at Induction
Implement processes to use the Apprenticeship Levy to support staff development and ensure all funds are spent
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
21
Development of an alternative appraisal recording system and support for roll-out of Employee Self Service
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
22
Appendix 1 – Mandatory training compliance
Indicator
frequency 2015-16 performance
2016-17 target
2016-17 performance
RAG Status
level 1/2 safeguarding adults training at induction
Once 92% 98% 99% G
level 1/2 safeguarding adults training every 3 years
3 years 98% 90% 98% G
level 1/2 safeguarding adults training to Trust targets
1 year/ 3years 90% 90% 88% A
level 3 safeguarding adults training
Once 93% 90% 95% G
% of relevant staff who have undertaken MCA training (Annual audit) reported Quarterly
3 years
91% 90% 98% G
fire training Annual
95% 90% 92% G
Patient moving and handling
Annual 87% 90% 88% A
BLS annual 90% 90% 88% A
infection control Annual / 3
years 90% 90% 89% A
Conflict resolution 3 years 94% 90% 92% G
Information governance Annual 96% 95% 96% G
PREVENT Once 95% 95% 95% G
Equality and Diversity 3 years 96% 90% 95% G
Safeguarding Children - level 1
3 years 93% 95% 92% A
Safeguarding Children - level 2
3 years 94% 95% 93% A
Safeguarding Children - level 3
15 months
95% 95% 92% A
Safeguarding Children - level 4
15 months 100% 95% 100% G
Overall Compliance 93% 90% 92% G
% of staff who have received an appraisal in the last 12 months
85% 90% 88% A
Learning and Development Annual Report 2016-17 Document in N:\HR\Meetings\Workforce and OD Strategy Group\2017\11 November\1.0 WFOD Agenda Nov 2017 v2.docx
23
Appendix 2 – Mandatory Training Planned vs. Places Provided
Session Title
Anticipated yearly
requirement
Places Provided
Places booked Places
Attended
Basic Life Support, immediate life support and anaphylaxis
2150 2800 2350 2070
Conflict Resolution
400 560 500 450
Conflict Resolution update
600 300 250 200 plus e-learning
Fire 1500 face to face /e-learning
300 places Fire
Evacuation face-to-face places for bed bases
870 fire update face
to face places
570 fire
evacuation
e-learning
470 e-learning 850 fire updates
450 with evacuation
470 e-learning 700
fire updates 400 with
evacuation
Patient moving and handling
1370 230 new patient
handlers 1450
updates
216 new patient handlers
1200 updates
183 new patient handlers
1050 updates 39 p
odiatry
Board 30th November 2017 Attachment K6 Appendix 1
1
HERTFORDSHIRE COUNTY COUNCIL (HCC) HEALTH SCRUTINY COMMITTEE (HSC) BACKGROUND TO NHS CONSULTATION & HCC CONCORDAT
1. INTRODUCTION 1.1. It is the role of HCC to hold the local NHS to local democratic account. However,
the relationship between HCC’s Health Scrutiny Committee (HSC) and its health partners is only one of the many that operate at different levels across the two sectors. The Health & Wellbeing Board (HWB) will influence the strategic direction for commissioning services that relate to the health and wellbeing of the population. HCC and health staff work closely together to ensure that their commissioning strategies are aligned and that patients’ experience of moving between health and social care services are as seamless as possible.
2. Legislative background
2.1. The law gives powers to local authorities (other than districts in two-tier areas) to
consider issues affecting the health of local people and to call the NHS and private providers whose services are funded by the NHS to account on behalf of local communities.1 The primary aims of health overview and scrutiny is to ensure that: • health services reflect the views and aspirations of local communities • all sections of local communities have equal access to services • all sections of local communities have an equal chance of a successful
outcome from services.2 2.2. The regulations specifically require NHS bodies to consult on any proposals for
“substantial variations or developments” of health services. HSC does not have powers to enforce any of the recommendations it makes to the NHS or private providers, either as a result of carrying out a scrutiny review, or in responding to a consultation. It can only hope to influence decisions by the evidence it brings forward and to ensure that consultation by the NHS has been of a high quality. The final decision on how NHS services are run and developed remains with NHS Boards. In Hertfordshire HSC and NHS bodies have agreed an approach to monitoring the implementation of recommendations through the OSC Review of Recommendations Topic Group.
1 Health and Social Care Act 2001, National Health Service Act 2006 (section 244) as amended by Health and Social Care Act 2012; Local Authority (Public Health, Health and Wellbeing Boards and Health Scrutiny) Regulations 2013 2 Centre for Public Scrutiny, Substantial Variations and Developments of Health Services: a Guide, 2005.
Board 30th November 2017 Attachment K6 Appendix 1
2
2.3. In addition to the creation of duties relating to local authority scrutiny, legislation requires the NHS to involve and consult the public widely on what it does.3 Clinical Commissioning Groups (CCGs), NHS Trusts and NHS Foundation Trusts must involve and consult people who receive or who may receive health services on:
• the planning of the provision of those services, • the development and consideration of proposals for changes in the way
those services are provided, and • decisions affecting the operation of those services
3. Hertfordshire County Council Health Scrutiny Committee (HSC) 3.1 HSC has been carrying out its scrutiny powers since 2002. The statutory health
scrutiny powers, following changes made by the Health and Social Care Act 2012, now rest with HCC, but they will continue to be exercised on behalf of HCC by HSC. HSC includes representation from all the districts/boroughs in Hertfordshire. All districts/boroughs, and HCC’s executive , continue to provide an executive response to NHS consultation proposals and service developments.
3.2 HSC is aware that the NHS in Hertfordshire has also been developing the ways it
involves and consults patients and the public and HSC wishes to encourage these developments, at the same time recognising the finite resources available. HSC aims to ensure that it has a comprehensive overview of NHS developments and an opportunity to contribute to improving the health of the people of Hertfordshire. It wishes to support new developments designed to improve health services, as long as it is assured that good and comprehensive involvement and consultation with patients and the public is happening. HSC believes that the best way for it to scrutinise the activities of the NHS locally is to act as a challenging critical friend.
3.3 HSC expects to be informed of proposed substantial variations in services, as is
required by law. However, HSC would not wish – and indeed would not have the capacity - to carry out detailed scrutiny in relation to the content of all new NHS proposals or existing services. This does not preclude HSC from undertaking scrutiny on specific issues it deems necessary. It is very important, therefore, that HSC can be satisfied that adequate, appropriate and effective consultation and involvement of patients and the public has takes place as a matter of course.
3 National Health Service Act 2006 (section 242) as amended by the Health and Social Care Act 2012.
Board 30th November 2017 Attachment K6 Appendix 1
3
3.4 HSC understands that consultations are not referenda and that NHS Boards must weigh up a number of factors in making decisions about changes in services. HSC and the NHS signatories to this Concordat agree that the views of patients and the local population are an important factor which must play and be seen to play a role in those decisions.
4. The Concordat between Health & HCC 4.1. HCC, acting through HSC, and the NHS signatories of this Concordat have agreed
to develop a Concordat on the way in which patients and the public in Hertfordshire are informed, consulted and involved in decision-making by the NHS. The purpose of this Concordat is: • to create an explicit consensus between HSC and the NHS in Hertfordshire
about the principles that should underlie good consultation of patients and the public
• to enable HSC to prioritise its scrutiny activity and to maintain the role of critical friend referred to above
• to assist patients and the public, including HealthWatch Hertfordshire (HWH), to understand the principles on which consultation with them is carried out by the NHS.
4.2. The guiding assumption is that, only where there is clear evidence that a
consultation process has failed to comply with the principles of the Concordat in a way which has materially affected the process or outcome will there be a need for detailed and formal scrutiny review by HSC. Such principles and assessment of compliance with them could never be wholly scientific, since they require a degree of judgement about whether their spirit has been fulfilled, and an understanding of local circumstances. However, it is hoped that they will provide a public benchmark to assist patients, the public, and NHS bodies themselves as well as HSC to plan patient and public involvement and consultation and to evaluate the adequacy and effectiveness of consultations.
4.3. It is accepted that both providers and commissioners have a statutory duty to
“involve and consult”; however, the lead organisation in respect of public consultation is the commissioning body. This body is expected to lead the contact with HSC.
4.4. Each signatory shall notify HCC’s Scrutiny Officer of the name and contact details
for a lead officer within their organisation who shall act as the principle point of contact for all matters in relation to this concordat. Any amendments to the name, role or contact details of a lead officer shall also be notifed accordingly.
5. Status of the Concordat, Amendments, Withdrawal and Successor Bodies
5.1. The Concordat is not a legally binding contract or agreement. However, the
signatory organisations voluntarily subscribe to its provisions. Agreeing the
Board 30th November 2017 Attachment K6 Appendix 1
4
Concordat shall be approved by each organisation in accordance with its Constitutional requirements. HCC’s Head of Scrutiny shall maintain a definitive current version of the Concordat.
5.2. Significant amendments which impact on the substance of the Concordat or any of its provisions will continue to be revised and agreed by health and HSC. Amendment will only be made with the agreement of all signatories. Minor amendments (including e.g. changes of organisation name or post titles) shall not require agreement.
5.3. Any signatory may withdraw from the Concordat by giving three months notice in
writing to HCC’s Head of Scrutiny. Withdrawal from the Concordat does not exempt an organisation from the fulfilment of its statutory duties in respect of consultation.
5.4. An organisation shall automatically cease to be a signatory to this concordat in the
event of it ceasing to exist as a statutory body. The Concordat does not bind successor organisations but any successor organisation shall be invited and encouraged to become a signatory. Notification in writing to HCC’s Head of Scrutinyl shall constitute an organisation becoming a signatory for this purpose, subject to their having complied with paragraph 12.1 above.
5.5. The establishment of HWH requires inclusion within any Concordat arrangements.
Where a member of the public, a representative organisation of the HWH or a member of HSC believes that consultation has not been carried out according to the spirit of the principles in the Concordat they may submit evidence to HSC as to why they consider the Concordat has not been complied with. In such instances HSC will either as a whole, or appoint a sub-group of it members to assess the process of consultation against the principles in the Concordat and decide, on this basis, whether further scrutiny is necessary. Appendix 4 to the Concordat provides a checklist of questions to assist any assessment of whether consultations have followed the principles of the Concordat.
5.6. The Concordat draws on the relevant legislation (referred to in footnotes) and the
experience of HSC and the NHS in developing and overseeing good practice on consultation and involvement at a practical level. In addition, the Concordat has drawn on principles outlined in the following documents:
• Hertfordshire County Council’s Have Your Say principles for consultation • Consultation Principles 2016 • The Independent Reconfiguration Panel’s best practice guidance. • NHS Constitution • Health & Social Care Act 2012 • Care Act 2014
Consultation Principles 2016
A. Consultations should be clear and concise Use plain English and avoid acronyms. Be clear what questions you are asking and limit the number of questions to those that are necessary. Make them easy to understand and easy to answer. Avoid lengthy documents when possible and consider merging those on related topics.
B. Consultations should have a purpose Do not consult for the sake of it. Ask departmental lawyers whether you have a legal duty to consult. Take consultation responses into account when taking policy forward. Consult about policies or implementation plans when the development of the policies or plans is at a formative stage. Do not ask questions about issues on which you already have a final view.
C. Consultations should be informative Give enough information to ensure that those consulted understand the issues and can give informed responses. Include validated assessments of the costs and benefits of the options being considered when possible; this might be required where proposals have an impact on business or the voluntary sector.
D. Consultations are only part of a process of engagement Consider whether informal iterative consultation is appropriate, using new digital tools and open, collaborative approaches. Consultation is not just about formal documents and responses. It is an on-going process.
E. Consultations should last for a proportionate amount of time Judge the length of the consultation on the basis of legal advice and taking into account the nature and impact of the proposal. Consulting for too long will unnecessarily delay policy development. Consulting too quickly will not give enough time for consideration and will reduce the quality of responses.
F. Consultations should be targeted Consider the full range of people, business and voluntary bodies affected by the policy, and whether representative groups exist. Consider targeting specific groups if appropriate. Ensure they are aware of the consultation and can access it. Consider how to tailor consultation to the needs and preferences of particular groups, such as older people, younger people or people with disabilities that may not respond to traditional consultation methods.
G. Consultations should take account of the groups being consulted Consult stakeholders in a way that suits them. Charities may need more time to respond than businesses, for example. When the consultation spans all or part of a holiday period, consider how this may affect consultation and take appropriate mitigating action.
H. Consultations should be agreed before publication Seek collective agreement before publishing a written consultation, particularly when consulting on new policy proposals. Consultations should be published on gov.uk.
I. Consultation should facilitate scrutiny
Karen Humm
Text Box
Consultation Principles; Guidance Cabinet Office
Publish any response on the same page on gov.uk as the original consultation, and ensure it is clear when the government has responded to the consultation. Explain the responses that have been received from consultees and how these have informed the policy. State how many responses have been received.
J. Government responses to consultations should be published in a timely fashion Publish responses within 12 weeks of the consultation or provide an explanation why this is not possible. Where consultation concerns a statutory instrument publish responses before or at the same time as the instrument is laid, except in exceptional circumstances. Allow appropriate time between closing the consultation and implementing policy or legislation.
K. Consultation exercises should not generally be launched during local or national election periods. If exceptional circumstances make a consultation absolutely essential (for example, for safeguarding public health), departments should seek advice from the Propriety and Ethics team in the Cabinet Office.
This document does not have legal force and is subject to statutory and other legal requirements.
1. Department of Health guidance (2014), good practice as recorded by the Centre for Public Scrutiny (CfPS 2005) and Section 10.6.3 of Local Authority Scrutiny regulations recommend that the following are taken into account when considering whether a development, proposed change or variation is ‘substantial’:
• Changes in accessibility of services • The impact of the proposal on the wider community and other services
(including economic impact, transport and regeneration) • The degree to which patients are affected • Changes to service models and methods of service delivery NHS e.g.
moving a particular service into a community setting from an acute hospital setting
2. Section 242 of the NHS Act places a statutory duty on the NHS to engage
and involve the public and service users in: • Planning the provision of services • The development and consideration of proposals to change the
provision of those services • Decisions affecting the operation of services.
To assist in transparency a template for detailing service changes that can be shared with HSC is in Appendix 3a.
APPENDIX 4
1
Checklist to ascertain if consultations have followed the Concordat, Consultation Principles, NHS Constitution & best practice Reflecting the 4 Tests, consultation should provide evidence of
• Strong public and patient engagement. • Consistency with current and prospective need for patient choice. • Clear, clinical evidence base. • Support for proposals from commissioners.
1. What efforts has the health body made from an early stage to inform
relevant stakeholders that a proposal is being formulated? 2. What evidence is there of patient and public involvement and/or
consultation in the development of the proposal? 3. If the proposal is clearly a substantial variation in services and not
subject to formal public consultation, how will the health body ensure stakeholder input?
4. If there is doubt about whether the proposal constitutes a substantial
variation have the Head of Scrutiny and the Health Scrutiny Committee (HSC) been asked for their views?
5. In the case of proposals that will not lead to substantial variations in
services, is the timescale for consultation realistic and acceptable? 6. Have those being consulted been made aware of the objectives of the
consultation? Have options been put forward in good faith? Has it been made clear which options are still “on the table” and which have been ruled out and the reasons given in sufficient depth to justify their exclusion?
7. Have the right people been consulted: key stakeholders, user groups
and individuals with an interest and those likely to be affected? Has consultation sought to elicit responses from a representative cross-section and a geographical spread (where appropriate) of views? Has the health consulting body encouraged people to give their views and enabled the voices of seldom-heard people and minorities to be heard?
8. Has consultation taken the right forms appropriate to the subject matter
and to those being consulted? Have responses to consultation been captured, recorded and reported appropriately? Have consultees been made aware of how they can complain about the consultation process, if they wish?
APPENDIX 4
2
9. Is the language of any consultation documents and events accessible, user-friendly and jargon free? Has any publicity made clear what the overall implications of any proposed changes will be?
10. Has analysis of consultation responses used fair and objective methods?
Has the methodology for analysing consultation responses been recorded in any report of consultation, where appropriate? Where possible, has a demographic and geographic breakdown of responses been provided in any final report? Is any final report available to relevant Boards, HSC and the public and is anonymised raw data from consultation available on request?
11. Have any decisions made after a consultation period given due weight
and attention to consultation responses and made it clear how they have influenced the decision(s)? How will feedback be given, where possible, to those consulted? Where a decision goes against a large body of opinion of those consulted, or against the view of those who will be most affected, have reasons been given for this?
APPENDIX 5
1
Signatories The signatories below have signed on behalf of their organisation and have done so in agreement with the principles outlined in the Concordat 2017.
1. Signed………………………………………… Date………………. Print Name and Post Title…………………………………….................... (Hertfordshire County Council which will act through its Health Scrutiny Committee)
2. Signed………………………………………… Date………………. Print Name and Post Title…………………………………….................... (Hertfordshire Partnership University NHS Foundation Trust)
3. Signed………………………………………… Date………………. Print Name and Post Title…………………………………….................... (East & North Hertfordshire NHS Trust)
4. Signed………………………………………… Date………………. Print Name and Post Title…………………………………….................... (West Hertfordshire Hospitals NHS Trust)
5. Signed………………………………………… Date………………. Print Name and Post Title…………………………………….................... (East of England Ambulance Service NHS Trust)
6. Signed………………………………………… Date………………. Print Name and Post Title…………………………………….................... (Hertfordshire Community NHS Trust)
7. Signed………………………………………… Date………………. Print Name and Post Title……………………………………….................. (Herts Valleys Clinical Commissioning Group)
8. Signed………………………………………… Date………………. Print Name and Post Title……………………………………….................. (East & North Herts Clinical Commissioning Group)
9. Signed………………………………………… Date………………. Print Name and Post Title……………………………………….................. (Cambridge & Peterborough Clinical Commissioning Group)
10. Signed………………………………………… Date………………. Print Name and Post Title……………………………………................... (Princess Alexandra Hospital, Harlow)
11. Signed………………………………………… Date………………. Print Name and Post Title…………………………………….................... (Healthwatch Hertfordshire)