1 Complications of Urinary Complications of Urinary Diversion Diversion Jennifer L. Dodson, M.D. Jennifer L. Dodson, M.D. Department of Urology Department of Urology Johns Hopkins University Johns Hopkins University Types of Diversion Types of Diversion Conduit Diversions Conduit Diversions Ileal conduit Ileal conduit Colon conduit Colon conduit Continent Diversions Continent Diversions Continent catheterizable reservoir Continent catheterizable reservoir Continent rectal pouch Continent rectal pouch
Transcript
1
Complications of Urinary Complications of Urinary DiversionDiversion
Jennifer L. Dodson, M.D.Jennifer L. Dodson, M.D.Department of UrologyDepartment of Urology
Technically simplestTechnically simplestSegment of choiceSegment of choice
Colon Conduit:Colon Conduit:Transverse or sigmoidTransverse or sigmoidUsed when ileum not appropriate (eg: concomitant colon resectioUsed when ileum not appropriate (eg: concomitant colon resection, n, abdominal radiation, short bowel syndrome, IBD)abdominal radiation, short bowel syndrome, IBD)
Conduit necrosis:Conduit necrosis:Acute ischemia to bowel segmentAcute ischemia to bowel segmentUrgent reUrgent re--explorationexploration
Conduit ischemia:Conduit ischemia:Stomal stenosis or strictureStomal stenosis or stricture
Conduit elongation:Conduit elongation:Distal obstruction at fascia or stomaDistal obstruction at fascia or stoma
Prevention:Prevention:Attention to blood supply of segmentAttention to blood supply of segmentPeriodic imaging postPeriodic imaging post--operativelyoperatively
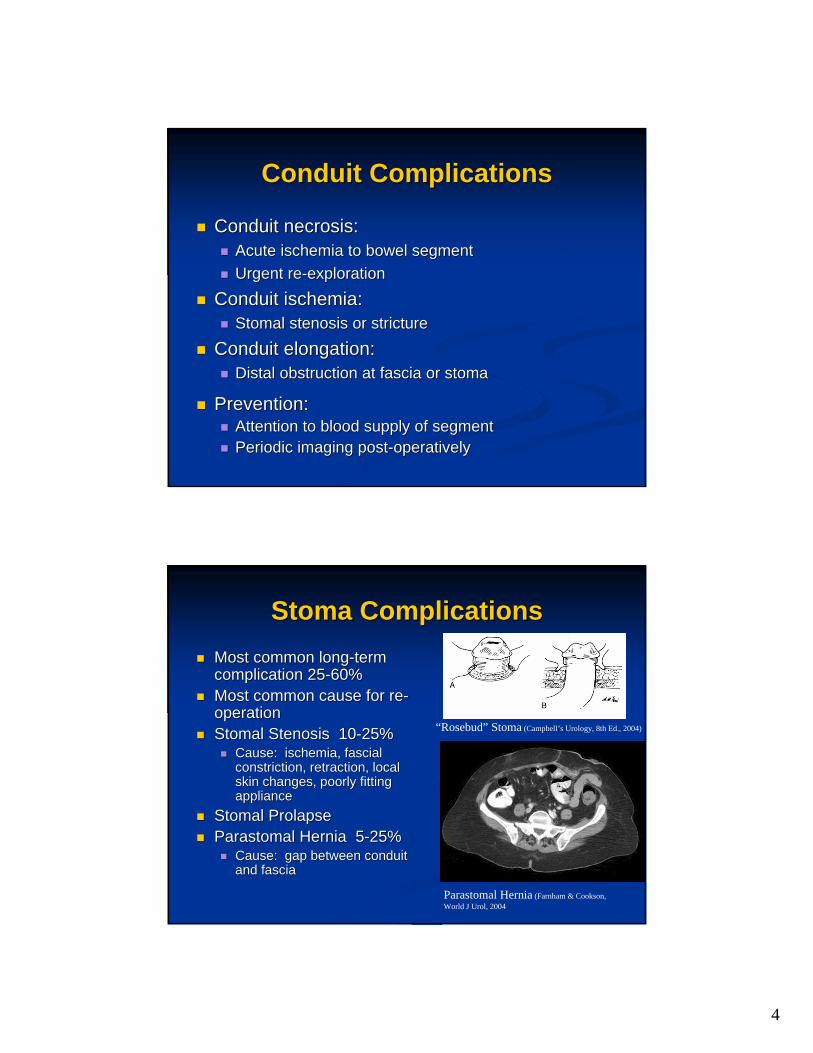
Stoma ComplicationsStoma ComplicationsMost common longMost common long--term term complication 25complication 25--60%60%Most common cause for reMost common cause for re--operationoperationStomal Stenosis 10Stomal Stenosis 10--25%25%
Difficulty catheterizing 3Difficulty catheterizing 3--18%18%Cause: stomal stenosis or tortuosity of channelCause: stomal stenosis or tortuosity of channelHighest incidence in tunneled appendixHighest incidence in tunneled appendixPrevention: in the OR, by stabilizing the channel, Prevention: in the OR, by stabilizing the channel, avoiding kinking, tension, or ischemiaavoiding kinking, tension, or ischemiaTreatment: dilation vs stomal revision with VTreatment: dilation vs stomal revision with V--flapflap
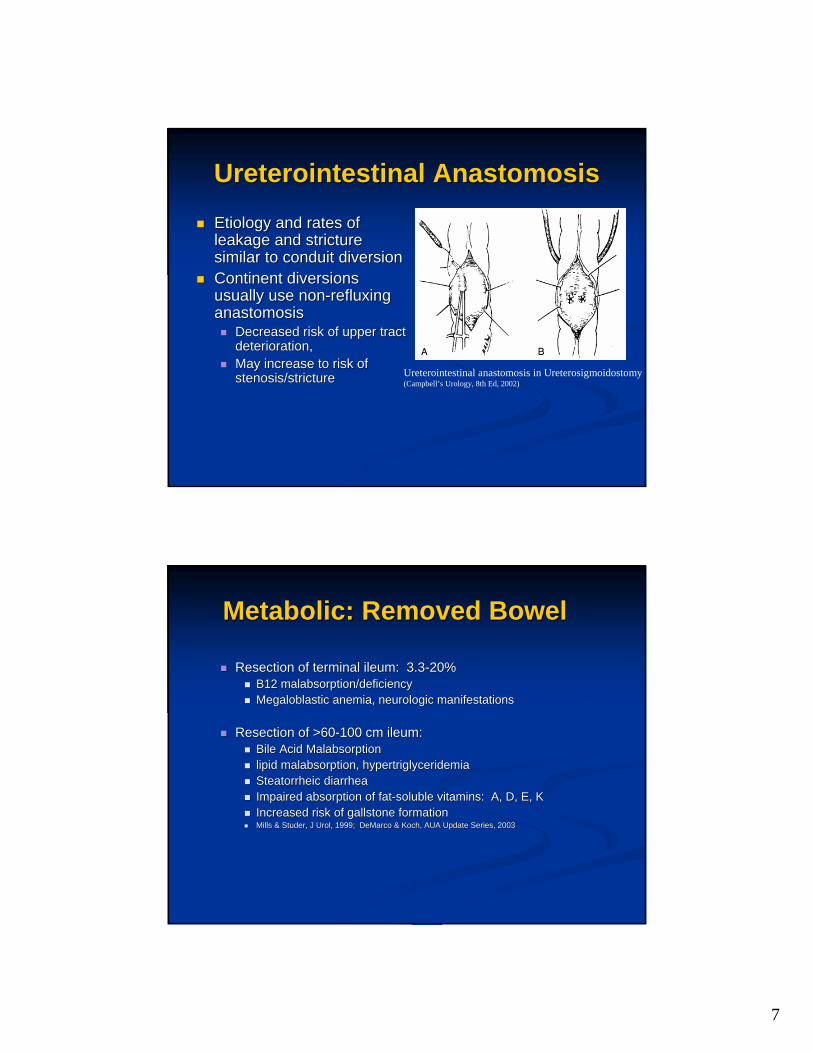
Etiology and rates of Etiology and rates of leakage and stricture leakage and stricture similar to conduit diversionsimilar to conduit diversionContinent diversions Continent diversions usually use nonusually use non--refluxing refluxing anastomosisanastomosis
Decreased risk of upper tract Decreased risk of upper tract deterioration, deterioration, May increase to risk of May increase to risk of stenosis/stricturestenosis/stricture Ureterointestinal anastomosis in Ureterosigmoidostomy
(Campbell’s Urology, 8th Ed, 2002)
Metabolic: Removed BowelMetabolic: Removed Bowel
Resection of terminal ileum: 3.3Resection of terminal ileum: 3.3--20%20%B12 malabsorption/deficiencyB12 malabsorption/deficiencyMegaloblastic anemia, neurologic manifestationsMegaloblastic anemia, neurologic manifestations
Resection of >60Resection of >60--100 cm ileum: 100 cm ileum: Bile Acid MalabsorptionBile Acid Malabsorptionlipid malabsorption, hypertriglyceridemialipid malabsorption, hypertriglyceridemiaSteatorrheic diarrheaSteatorrheic diarrheaImpaired absorption of fatImpaired absorption of fat--soluble vitamins: A, D, E, Ksoluble vitamins: A, D, E, KIncreased risk of gallstone formationIncreased risk of gallstone formationMills & Studer, J Urol, 1999; DeMarco & Koch, AUA Update SeriesMills & Studer, J Urol, 1999; DeMarco & Koch, AUA Update Series, 2003, 2003
8
MalabsorptionMalabsorption
Metabolic: Removed BowelMetabolic: Removed Bowel
Resection of ileocecal valve: Resection of ileocecal valve: Decreased transit timeDecreased transit timeIncreased wet weight of stoolIncreased wet weight of stooldiarrheadiarrhea
Resection of colon segment:Resection of colon segment:Right colon important for storage of stoolRight colon important for storage of stool
Bone demineralizationBone demineralizationAcidosisAcidosis
carbonate and phosphate released from bone to carbonate and phosphate released from bone to buffer hydrogen ionsbuffer hydrogen ionsAcidosis inhibits production of 1, 25Acidosis inhibits production of 1, 25--dihydroxycholecalciferoldihydroxycholecalciferolAcidosis activates osteoclast activityAcidosis activates osteoclast activityIncreased excretion of calcium in urine Increased excretion of calcium in urine
RicketsRicketsOsteomalaciaOsteomalacia
10
Stone DiseaseStone Disease
Upper tract stones: Upper tract stones: Metabolic etiologyMetabolic etiologyChronic dehydration, concentrated urineChronic dehydration, concentrated urineIf large ileal resection, risk of enteric hyperoxaluria with calIf large ileal resection, risk of enteric hyperoxaluria with calcium cium oxalate stone formationoxalate stone formationHypocitraturiaHypocitraturiaHypercalciuria due to metabolic acidosis Hypercalciuria due to metabolic acidosis
Cancer riskCancer risk
Ureterosigmoidostomy:Ureterosigmoidostomy:> 200 cases of secondary malignancy reported> 200 cases of secondary malignancy reportedAge 25Age 25--30 yo: 47730 yo: 477--fold increased riskfold increased riskAge 55Age 55--60 yo: 860 yo: 8--fold increased risk over general populationfold increased risk over general populationHistology: adenoma, adenocarcinomaHistology: adenoma, adenocarcinomaFollowFollow--up starting between 3up starting between 3--5 years post5 years post--op with yearly op with yearly endoscopy, ultrasoundendoscopy, ultrasound
Austen & Kalble, J Urol, 2004
11
Cancer riskCancer risk
Conduit and continent diversions:Conduit and continent diversions:Variable histologyVariable histology
Austen & Kalble, J Urol, 2004
Compliance & Access to Care Compliance & Access to Care
CathetersCathetersLubricationLubricationIrrigation and frequent catheterizationIrrigation and frequent catheterizationFollowFollow--upup
12
Potential Research QuestionsPotential Research Questions
Which is better in this context: Which is better in this context: Conduit, Conduit, rectal reservoir, or rectal reservoir, or catheterizable reservoir?catheterizable reservoir?
Major issues:Major issues:Complications: short and longComplications: short and long--termtermCosts: FollowCosts: Follow--up and consumablesup and consumablesCultural acceptance of different diversionsCultural acceptance of different diversions
References:References:
Austen, M., Kalble, T.: Secondary malignancies in different forAusten, M., Kalble, T.: Secondary malignancies in different forms of ms of urinary diversion using isolated gut. J Urol., 172: 831, 2004.urinary diversion using isolated gut. J Urol., 172: 831, 2004.DeMarco, R.T., and Koch, M.O.: Metabolic complications of DeMarco, R.T., and Koch, M.O.: Metabolic complications of continent urinary diversion. AUA Update Series, 15, XXII, 2003.continent urinary diversion. AUA Update Series, 15, XXII, 2003.Farnham, S.B. and Cookson, M.S.: Surgical complications of Farnham, S.B. and Cookson, M.S.: Surgical complications of urinary diversion. World J Urol, 22: 157, 2004urinary diversion. World J Urol, 22: 157, 2004Mills, R.D., and Studer, U.E.: Metabolic consequences of continMills, R.D., and Studer, U.E.: Metabolic consequences of continent ent urinary diversion. J Urol., 161: 1057, 1999.urinary diversion. J Urol., 161: 1057, 1999.Nagi, G., Dublin, N., McClinton, S., NNagi, G., Dublin, N., McClinton, S., N’’Dow, J.M.O., Neal, D.E., Dow, J.M.O., Neal, D.E., Pickard, R., Yong, S.M.: Urinary diversion and bladder Pickard, R., Yong, S.M.: Urinary diversion and bladder reconstruction/replacement using intestinal segments for intractreconstruction/replacement using intestinal segments for intractable able incontinence or following cystectomy. The Cochrane Collaboratioincontinence or following cystectomy. The Cochrane Collaboration, n, Issue 3, 2005.Issue 3, 2005.