28
Diabetic Dyslipidaemia BY ن الرحيم الرحم بسمKHALED EL SAYED EL HADIDY Professor of Internal Medicine Beni Sueif University Consultant of Endocrinology & Diabetes
| Date post: | 10-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | ueda2015 |
| View: | 25 times |
| Download: | 0 times |

Diabetic Dyslipidaemia BY
بسم هللا الرحمن الرحيم
KHALED EL SAYED EL HADIDY
Professor of Internal Medicine
Beni Sueif University
Consultant of Endocrinology & Diabetes

Is it only the LDL Goals that can solve the
problem of Diabetic Dyslipidaemia?
Agenda
Lipid Pathophysiolog in T2DM.
Dyslipidemia as a CAD. Risk Factor.
Neglected Area in Diabetic Dyslipidaemia .
ADA Standards of Medical Care in Diabetes (2013).
Antilipidemic drugs.
Take Home message.

• Apo A-1
• SD LDL
HDL
Apo A-1
(CETP)
(LACT)
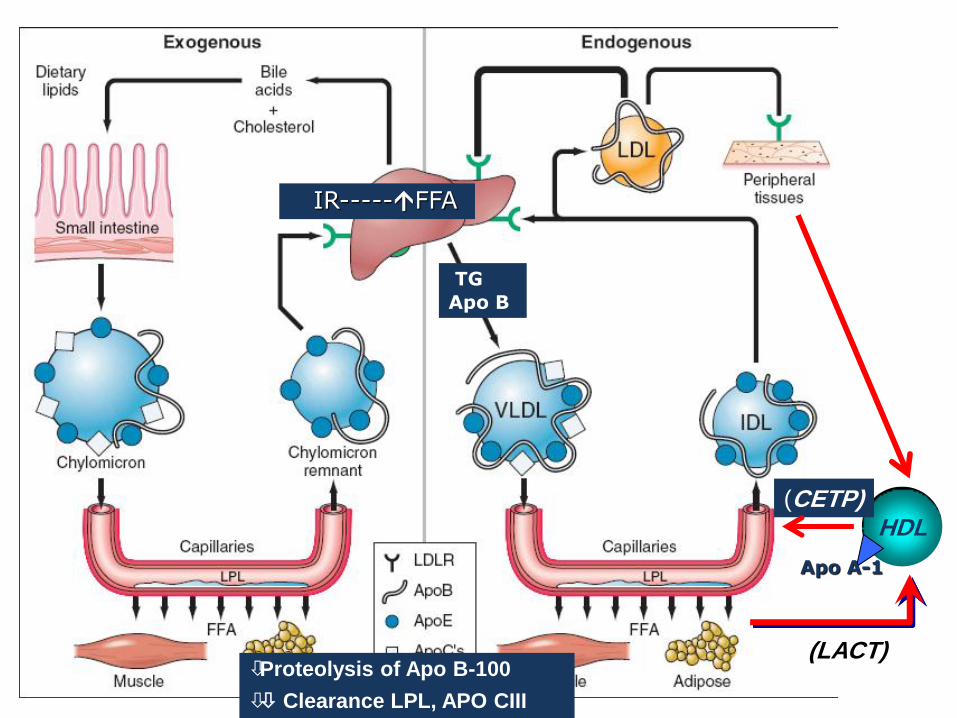
IR-----FFA
TG
Apo B
Proteolysis of Apo B-100
Clearance LPL, APO CIII
HDL (CETP)
(LACT)
Apo A-1

IR-----FFA
TG
Apo B
Proteolysis of Apo B-100
Clearance LPL, APO CIII
SD
LDL
HDL (CETP)
(LACT)
Apo A-1
(CETP)

• Apo A-1
• SD LDL
HDL
Apo A-1
(CETP)
(LACT) Proteolysis of Apo B-100
Clearance LPL, APO CIII
TG
Apo B
IR-----FFA
SD
LDL
↑ Non–HDL
= Total C – HDL-C (all atherogenic lipids)
(CETP)

Agenda
• Lipid Pathophysiolog in T2DM.
• Dyslipidemia as a CAD. Risk Factor.
• Neglected Area in Diabetic Dyslipidaemia .
• ADA Standards of Medical Care in Diabetes (2013).
• Antilipidemic drugs.
• Take Home message.

(Aso. CHD) most common cause
of morbidity and mortality in type 2 DM.
( Aso. accounts for about 80% of all mortality).
(75% due to CHD & 25% due to cerebral or PVD).
`(CARDS): multicentre randomised placebo-controlled trial. Lancet 2004;364:685-696. 2Third Report of the NCEP Expert Panel on Detection, Evaluation, and Treatment of
High Blood Cholesterol in Adults (ATP III). Circulation. 2002;106:3143-3421.
(NCEP) (ATP) III : patients with diabetes should be
regarded as having CHD risk equivalent to that of patients with
known CHD.
European guidelines : risk of developing an MI is the
same for diabetic patients as it is for nondiabetic patients with a
prior MI.
Therefore, the same aggressive lipid treatment goals
should be applied to both diabetic and CHD patients,
even if the diabetic have no evidence of existing CHD.

CAD. Risk Factors

Agenda
• Lipid Pathophysiolog in T2DM.
• Dyslipidemia as a CAD. Risk Factor.
• Neglected Area in Diabetic Dyslipidaemia .
• ADA Standards of Medical Care in Diabetes (2013).
• Antilipidemic drugs.
• Take Home message.

Non–HDL-C Superior to LDL-C in Predicting CHD Risk
Liu J, et al. Am J Cardiol. 2006;98:1363-1368.
0
0.5
1
1.5
2
2.5
LDL - C mg/dL
Non–HDL-C, mg/dL
Rela
tive C
HD
Ris
k
<130 130-159 ≥160
≥190
160-189 <160
The Framingham Study
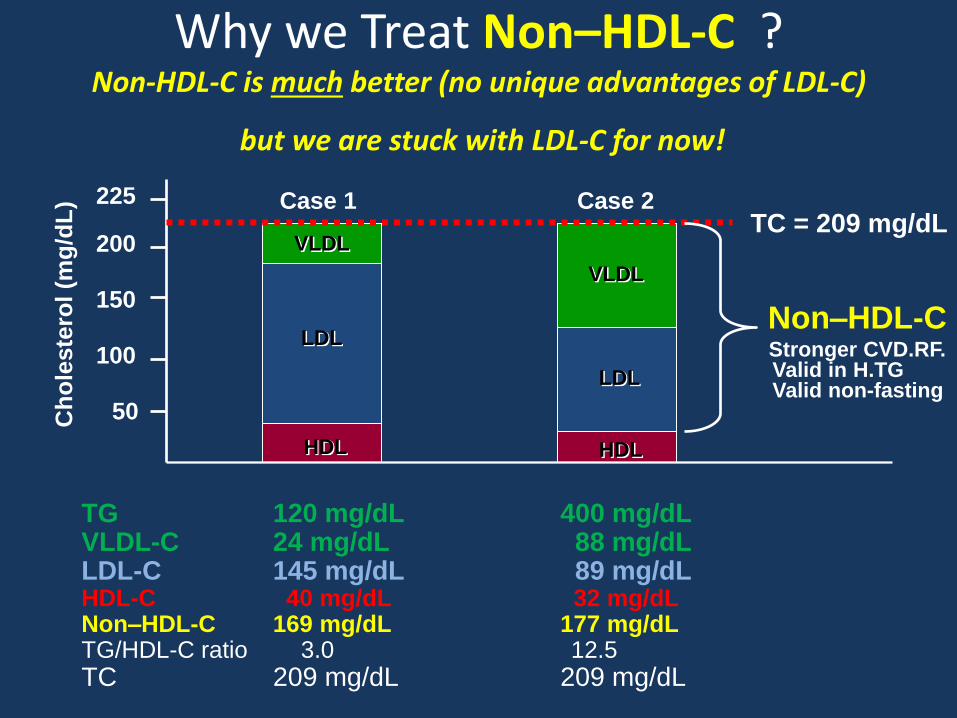
Why we Treat Non–HDL-C ? Non-HDL-C is much better (no unique advantages of LDL-C)
but we are stuck with LDL-C for now!
TG 120 mg/dL 400 mg/dL VLDL-C 24 mg/dL 88 mg/dL LDL-C 145 mg/dL 89 mg/dL HDL-C 40 mg/dL 32 mg/dL Non–HDL-C 169 mg/dL 177 mg/dL TG/HDL-C ratio 3.0 12.5
TC 209 mg/dL 209 mg/dL
Ch
ole
ste
rol
(mg
/dL
) Case 1 Case 2
50
100
150
200
225
TC = 209 mg/dL
HDL HDL
LDL
LDL
VLDL
VLDL
Non–HDL-C Stronger CVD.RF. Valid in H.TG Valid non-fasting

<147
>147
<116 >116 <142 >142
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
Re
lati
ve
Ris
k o
f C
AD
Small, Dense LDL May Predict CAD
Better than LDL-C, Apo B, and TG
St-Pierre AC, et al. Circulation. 2001;104:2295-2299.
LDL-C (mg/dL)
Apolipoprotein B (mg/dL)
Triglycerides (mg/dL)
39.6%
<39.6%
Small, dense
LDL (<255 Å)
4.0
p<0.001
(N=35)
1.0 (N=35)
6.5
p<0.001
(N=50)
6.5
p=0.13
(N=15)
3.9
p<0.001
(N=27)
1.0 (N=9)
5.9
p<0.001
(N=58)
2.0
p=0.12
(N=14) 1.0
(N=12)
3.3
p<0.001
(N=20) 1.9
p=0.15
(N=11)
5.6
p<0.001
(N=65)
>147 LDL-C
130 mg/dL
LDL-C
130 mg/dL

Elevated Triglycerides Increase the Risk of CHD at All Levels of HDL-C
17.2
4.36.7
7.9
6.1
3.1 3.71.15.7
2.2 1.3 1.0
0
4
8
12
16
20
Od
ds R
ati
o f
or
Pre
matu
re C
AD
<30 30-39 40-49 50+
<200
200-299
>300
HDL-C, mg/dL
Triglycerides,
mg/dL
Hopkins PN, et al. J Am Coll Cardiol. 2005;45:1003-1012.

Agenda
• Lipid Pathophysiolog in T2DM.
• Dyslipidemia as a CAD. Risk Factor.
• Neglected Area in Diabetic Dyslipidaemia .
• ADA Standards of Medical Care in Diabetes (2013).
• Antilipidemic drugs.
• Take Home message.

Standards of Medical Care in Diabetes—2013 Dyslipidemia/Lipid Management (1)
Screening
• Most: measure fasting lipid. / y. (B)
• low-risk lipid values: (LDLc <100 , HDLc >50 , and TG <150) (mg/dL)
measure fasting lipid. / 2 y. (E)
ADA. VI. Prevention, Management of Complications. Diabetes Care 2013;36(suppl 1):S31.

Standards of Medical Care in Diabetes—2013 Dyslipidemia/Lipid Management (2)
Treatment recommendations
lifestyle modification (A)
– Reduction of saturated fat, trans fat, cholesterol intake.
– Increased n-3 fatty acids, viscous fiber, plant stanols/sterols.
– Reduction of Weight. (if indicated)
– Increased physical activity.
ADA. VI. Prevention, Management of Complications. Diabetes Care 2013;36(suppl 1):S31.

Standards of Medical Care in Diabetes—2013 Dyslipidemia/Lipid Management (3)
Treatment recommendations Statin therapy
• should + lifestyle .
(( regardless of baseline lipid levels)).
– with overt CVD. (A) – without CVD > 40 y. + 1 or >1 other CVD. RF. (A)
• Consider + lifestyle.
– with lower risk (e.g., without overt CVD, < 40 years of age). (C) * LDLc remains >100 mg/dL. * Multiple CVD. RF.
ADA. VI. Prevention, Management of Complications. Diabetes Care 2013;36(suppl 1):S31.

Standards of Medical Care in Diabetes—2013 Dyslipidemia/Lipid Management (4)
Treatment recommendations
• Combination therapy has been shown not to provide additional cardiovascular benefit above statin therapy alone and is not generally recommended (A)
• Statin therapy is contraindicated in pregnancy (B)
ADA. VI. Prevention, Management of Complications. Diabetes Care 2013;36(suppl 1):S31.

Standards of Medical Care in Diabetes—2013 Dyslipidemia/Lipid Management (2013)
Treatment (LDLc cholesterol) goals
• without overt CVD
– < 100 mg/dL (2.6 mmol/L) (B)
• with overt CVD
– < 70 mg/dL (1.8 mmol/L), (using a high dose of a statin, is an option ) (B)
ADA. VI. Prevention, Management of Complications. Diabetes Care 2013;36(suppl 1):S31.
If targets not reached on maximal tolerated statin therapy Alternative goal: reduce
LDLc ~30–40% from baseline (B)
TG < 150 mg/dL (1.7 mmol/L),
HDLc > 40 mg/dL (1.0 mmol/L) in men and
> 50 mg/dL (1.3 mmol/L) in women, are desirable (C)

ADA/ACC 2008 Consensus Statement: Goals
Brunzell JD, et al. Diabetes Care. 2008;31:811-822.
Whenever TG > 200 mg/dL
LDL-C
Non–HDL-C = Total C – HDL-C
Apo B
Highest-Risk Patients
• Known CVD
• Diabetes plus ≥1 additional major
CVD risk factora
<70 mg/dL <100 mg/dL <80 mg/dL
High-Risk Patients
• No diabetes or known CVD but
≥2 major CVD risk factorsa
• Diabetes but no other major
CVD risk factorsa
<100 mg/dL <130 mg/dL <90 mg/dL
““Very High” 1ry Objective: TG reduction
• TG ≥500 mg/dL 2nd Objective: LDL-C and non–HDL-C reduction

Recommendations for lipid analysis as
treatment target in the prevention of CVD
Every 40
mg/dL
reduction in
LDL-C is
associated
with
corresponding
22%
reduction in
CVD
mortality and
morbidity
LDL-C
remains the
primary
target of
therapy
ESC - 2011

Mechanisms of action of lipid-lowering drugs
CETP Inhibitors
FDA approved supplement
Omega 3 Fish oil
LDL size
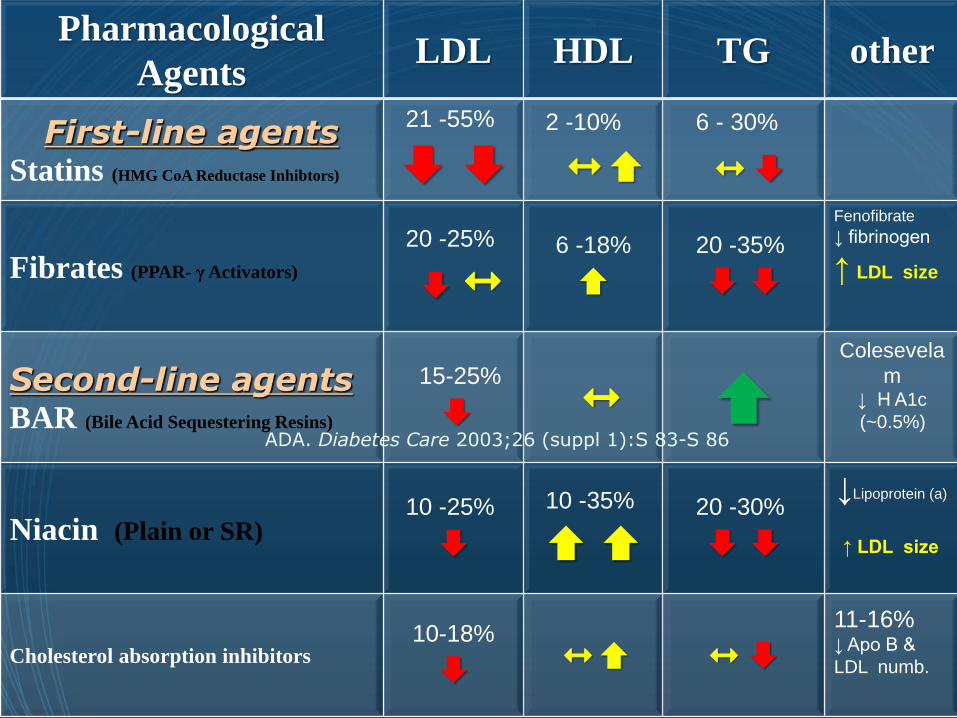
Pharmacological
Agents LDL HDL TG other
First-line agents Statins (HMG CoA Reductase Inhibtors)
21 -55%
2 -10%
6 - 30%
Fibrates (PPAR- γ Activators)
20 -25%
6 -18%
20 -35%
Fenofibrate
↓ fibrinogen
↑ LDL size
Second-line agents BAR (Bile Acid Sequestering Resins)
15-25%
Colesevela
m ↓ H A1c
(~0.5%)
Niacin (Plain or SR) 10 -25%
10 -35%
20 -30%
↓Lipoprotein (a)
↑ LDL size
Cholesterol absorption inhibitors 10-18%
11-16% ↓ Apo B &
LDL numb.
ADA. Diabetes Care 2003;26 (suppl 1):S 83-S 86
Take home message.


THANK YOU

















