Friedman et al. An end result of study of twenty-four cases. J Bone Joint Surg [Am] 34:893-900, 1952 39. Douglas J: Resection of the head of the ulna for anterior displacement accompanying unreduced Colles’ fracture. Ann Surg 60:388-9, 1914 40. Boyd HB, StoneMM: Resection of the distal end of the ulna. J Bone Joint Surg26:313-21, 1944 41. Swanson AB: Implant arthroplastyfor disabilities of the distal radioulnar joint. Use of a silicone rubber capping implant followingresection of the ulnar head. Orthop Clin North Am 4:373-82, 1973 42. Berg E: Indication for and results with Swanson distal ulnar prosthesis. SouthMed.J 69:858-61, 1976 Ulnar deficiency Twenty-nine patients with 34 ulnardeficient limbswere studied; the average follow-up was 7.7 years. Topermitearly determination of prognosisand decisions regarding treatment, four subtypes of this condition have been identified. Progressive ulnardeviation of the wrist was not observed in any case, andthe fibrocartilaginous ulnaranlage wasresected only to correct fixed deformities of the wrist. The most useful operation washumeral or radial osteotomy to correct the hand on flank deformity.A group of patients who were optimally treated with prosthetic fitting is discussed. (J HAND SURG 11A:822..9, 1986.) Jeffrey K. Miller, M.D., Steven M. Wenner, M.D., and Leon M. Kruger, M.D., Boston and Springfield, Mass. Longitudinal deficiency of the ulna, corn- plete or partial, is a rare affection of the upperlimbs; radial deficiency occurs ten times more frequently. Ul- nar deficiency did not occur in Entin’s I series of 61 cases of upper limb deficiency, or in the series of Henkel and Willert 2 of 557 malformedupper limbs) Accord- ing!y, most series of patients with ulnar deficiencyhave be6n relatively small. 3t° Several different classification systems based pri- marily on’ radiographic features have been proposed. Kummel defined three types on the basis of the radio- graphic appearanceof the elbow joint as follows: type A, normal appearing joint; type B, radiohumeral syn- ostosis; type C, dislocated radial head. Ogden and associates 4 proposed a system based upon the degree of ulna visible radiologically. Each of these systerns From the Shriners Hospital for Crippled Children, Springfield Unit, 516 Carew St., Springfield, Mass. Received for publication July12, 1985; accepted in revised form March 14, 1986. Reprint requests: Steven M. Wenner, M.D., 39Mulberry St., Spring- field, MA 01105. adequately classifies the deformities, yet they are not useful in making clinical decisions regarding prognosis and treatment. We present a classification system on the basis of our long-term follow-up of a large number (29)~f patients with longitudinal deficiencyof the ulna. This system is useful for formulating a prognosis and planning treatment in this condition. Materials and methods Twenty-nine patients with 34 ulnar deficient limbs were studied. Multiple clinical and radiographic fea- tures were retrospectively reviewed to determine the influence of each one, and the combinations of different ones, on the overall prognosis and on the clinical de- cision makingprocess. The patients were seen at the Shriners Hospital, Springfield Unit, over a 30-year period between 1954 and 1984. Follow-upaveraged 7.7 years, with a range of 2 months to 16 years, 8 months.In 19 cases the left side only was affected, in five cases the fight side only was affected, and five cases were bilateral. There were 18 male patients and 11 female patients. There was no familyhistory of a similar deformity in any of the cases. 822 THE JOURNAL OF HAND SURGERY
Transcript
Friedman et al.
An end result of study of twenty-four cases. J Bone JointSurg [Am] 34:893-900, 1952
39. Douglas J: Resection of the head of the ulna for anteriordisplacement accompanying unreduced Colles’ fracture.Ann Surg 60:388-9, 1914
40. Boyd HB, Stone MM: Resection of the distal end of theulna. J Bone Joint Surg 26:313-21, 1944
41. Swanson AB: Implant arthroplasty for disabilities of thedistal radioulnar joint. Use of a silicone rubber cappingimplant following resection of the ulnar head. OrthopClin North Am 4:373-82, 1973
42. Berg E: Indication for and results with Swanson distalulnar prosthesis. South Med.J 69:858-61, 1976
Ulnar deficiency
Twenty-nine patients with 34 ulnar deficient limbs were studied; the average follow-up was 7.7years. To permit early determination of prognosis and decisions regarding treatment, foursubtypes of this condition have been identified. Progressive ulnar deviation of the wrist was notobserved in any case, and the fibrocartilaginous ulnar anlage was resected only to correct fixeddeformities of the wrist. The most useful operation was humeral or radial osteotomy to correctthe hand on flank deformity. A group of patients who were optimally treated with prostheticfitting is discussed. (J HAND SURG 11A:822..9, 1986.)
Jeffrey K. Miller, M.D., Steven M. Wenner, M.D., and Leon M. Kruger, M.D.,Boston and Springfield, Mass.
Longitudinal deficiency of the ulna, corn-
plete or partial, is a rare affection of the upper limbs;radial deficiency occurs ten times more frequently. Ul-nar deficiency did not occur in Entin’sI series of 61cases of upper limb deficiency, or in the series of Henkeland Willert 2 of 557 malformed upper limbs) Accord-ing!y, most series of patients with ulnar deficiency havebe6n relatively small.3t°
Several different classification systems based pri-marily on’ radiographic features have been proposed.Kummel defined three types on the basis of the radio-graphic appearance of the elbow joint as follows: typeA, normal appearing joint; type B, radiohumeral syn-ostosis; type C, dislocated radial head. Ogden andassociates4 proposed a system based upon the degreeof ulna visible radiologically. Each of these systerns
From the Shriners Hospital for Crippled Children, Springfield Unit,516 Carew St., Springfield, Mass.
Received for publication July 12, 1985; accepted in revised formMarch 14, 1986.
Reprint requests: Steven M. Wenner, M.D., 39 Mulberry St., Spring-field, MA 01105.
adequately classifies the deformities, yet they are notuseful in making clinical decisions regarding prognosisand treatment. We present a classification system onthe basis of our long-term follow-up of a large number(29)~f patients with longitudinal deficiency of the ulna.This system is useful for formulating a prognosis andplanning treatment in this condition.
Materials and methods
Twenty-nine patients with 34 ulnar deficient limbswere studied. Multiple clinical and radiographic fea-tures were retrospectively reviewed to determine theinfluence of each one, and the combinations of differentones, on the overall prognosis and on the clinical de-cision making process.
The patients were seen at the Shriners Hospital,Springfield Unit, over a 30-year period between 1954and 1984. Follow-up averaged 7.7 years, with a rangeof 2 months to 16 years, 8 months. In 19 cases the leftside only was affected, in five cases the fight side onlywas affected, and five cases were bilateral. There were18 male patients and 11 female patients. There was nofamily history of a similar deformity in any of the cases.
822 THE JOURNAL OF HAND SURGERY
November 1986 Ulnar deficiency 823
Fig. 2. A typical type A deformity with dislocated radial head
oand a bowed radius.
Fig. 1. Type A deformity. Elbow motion was from 80 to120°, and from neutral to 10° of pronation.
Classification of elbow and forearm deformities
The limbs showed four distinct subtypes by radio-graphic and clinical examinations. They are as follows: ,
Type A. (14 limbs) Type a has a dislocated radial "
head, with a variable degree of bowing of the radius.Ossification of the ulna is delayed in most cases, but "progress’ive ossification is seen in serial x-ray films.Most patients lack normal elbow flexion/extension and
¯
forearm pronation/supination. The elbow has a variablerange of motion, but it tends to rest in an average offorty ° of flexion. No patient has a cubital web. Thelimited range of motion does not prove to be a majorfunctional deficit. With compensatory shoulder motion,all patients can adequately position their hand in space.Elbow instability is not a complaint in any of thesepatients (Figs. 1 and 2).
Type B. (3 limbs) In Type B deformity the radialhead is dislocated, there is complete and persisting ab-sence of the ulna, and there is cubital webbing. Theaverage elbow flexion deformity measured 125° and allwere greater than 110°. All three of these patients hadlimited ability to position and use the hand in front of Fig. 3. Type B deformity. Note the characteristic cubital web.
824 Miller, Wenner, and KrugerThe Journal of
HAND SURGERY
Fig. 5. Type C deformity. Note the radiohumeral synostosisand mildly bowed radius.
Fig. 4. The elbow of the patient in Fig. 3. Nearing skeletalmaturity, the features include complete absence of the ulna,dislocated radial head, and marked flexion of the forearmsegment.
the body because of the flexed elbow. These patientsuse their ulnar deficient limbs to help perform tasksabout the head and chest only (Figs. 3 and 4).
Type C. (14 limbs) Type C patients have a radio-humeral synostosis, with a variable amount of ulna. As
¯ with type A patients, ossification of the ulna is delayed,but it always eventually appears. The angle betweenthe humerus and radius is variable, measuring between15° and 100° in our patients. The radius is bowed, butin no case did the bowing progress with time (Fig. 5).
The "hand on flank" deformity was present in nineof fourteen limbs. This deformity consists of a hyper-pronated forearm, bowing of the radius, and flexionand rotation of the elbow so that the hand faces pos-teriorly and tends to lie on the flank or buttock at rest(Fig. 6, A). To place the hand in a functional positionin front of the plane of the body, the patient externally
rotates at the shoulder (Fig. 6, B).Type D. (3 limbs) Type D deformity shows a radio-
humeral synostosis, with a straight radius and an ulnaof near normal length but of markedly diminished di-ameter. The forearm is in neutral rotation. The elbowis at an average of 45° of flexion. With the straight
radius, no patient exhibits the "hand on flank" defor-mity. These patients function well, and they can easilyposition the hand in front of the body without excessiveexternal rotation at the shoulder (Fig. 7).
Associated deformities
Wrist. The wrist was ulnarly deviated to a significantdegree in 14 of the 34 cases. The ulnar deviation wasnot progressive in any of the cases.
Hand. A three-digit hand was the most commonpattern seen. Nineteen of the 34 cases (56%) showedthis variation (Table I).
The thumb was absent in 7 cases, hypoplastic in 7cases, and of normal size in 20 cases. It was frequ~iatlyof normal size but had no opposition power. In thesecases the first webspace was contracted.
Syndactyly, always simple, was present in 13 of thehands. The most frequently observed hand anomaly wasfixed flexion deformity of the interphalangeal joints.This was present in 23 of the cases.
Shoulder. There were four cases of ipsilateral shoul-der instability. These patients could either subluxate ordislocate their shoulders. In two instances this occurredwhile the patient maneuvered the hand into a functionalposition (cases 19 and 23). The dislocations were easilyreduced by the patients and all patients were asymp-tomatic.
Miscellaneous. Nineteen of the 29 patients hadanomalies remote from the ulnar deficient limbs. Eigh-teen had additional musculoskeletal anomalies--fivewith toe syndactyly, three with contralateral above el-
Vol. 11A, No. 6November 1986 Ulnar deficiency 825
Fig. 6. A more severely involved type C deformity. A, View from behind patient shows the "handon flank" deformity at rest. B, Frontal view of same patient preparing to bring the hand into afunctional position by external rotation and abduction of the shoulder.
bow amputations, three with bilateral fibular deficiency,two with bilateral proximal focal femoral deficiency,four with scoliosis, and three with adactylia of other-wise normal limbs. Also represented were congenitaldislocations of the hip, congenital coxa vara, congen-itally short femur, torticollis, and two patients withabsence of the ipsilateral pectoralis major. The centralnervous system was involved in one case of Sturge-Weber syndrome, and in one case of grand mal seizures.Also present was one case each of hypospadius, bi-cornuate uterus, branchial cyst, and congenital dia-phragmatic hernia.
Nonoperative treatments. Most patients were eval-uated at an early age. They were started on a programof passive stretching of the ulnarly deviated wrist andnight splinting of the wrist. The patients were encour-aged to perform two-handed activities and to use theirdeficient limbs as much as possible. Two patients withtype B deformity were fitted with above elbow typeprostheses over the flexed elbow. One patient wore theprosthesis full time, with greatly improved overall func-tion (case 17). The other patient rejected his prosthesisafter being fit with it at age ten (case 16).
Operative treatment of elbow and forearm defor-mities. Of the twenty type A, B, and D limbs, onlyone patient was treated surgically for the elbow or fore-arm deformity. This procedure was an attempted releaseof a cubital web; the operation was unsuccessful (case15). The type A patients had enough mobility of theelbow and forearm to position the hand in front of the
Fig. 7. The features of type D deformity. Note the radio-humeral synostosis, the straight radius, and the diminutiveulna.
body. Type D patients, because of the straight forearmand despite the fixed elbow, could position their handsadequately with compensatory shoulder motion.
Of the fourteen type C limbs, five had a total of eight
826 Miller, Wenner, and KrugerThe Journal of
HAND SURGERY
Table I
Patient Type Extremity Digits Follow-up
1 A L 4 3 mo2 A L 3 7 mo3 A R 3 2 yr
4 A R 3 10 yr, 3 moD L 4
5 A R 3 2 yr
6 A L 2 2 yr, I0 mo
7 A L I 15 yr
8 A L 2 16 yr
9 A L 3 2 yr, 6 mo10 A L 5 2 yr, 6 mo
11 A L12 A L
3 1 yr, 11 mo3 14 yr, 3 mo
3 11 yr, 2 mo31 2 mo3 14 yr, 9 mo
2 1 yr, 9 mo
13 A RD L
14 A L15 B R
16 B L
Operations~prostheses
NoneSyndactyly releaseRelease constriction band at wrist
NoneNoneNone
Syndactyly release, rotational os-teotomy of radial digit
NoneNoneBE prosthesisRelease of cubital web, rotational
osteotomy ulnar metacarpalNone
Associated anomalies
Camptodactyly;-Sturge-Weber syndromeHypospadius; syndactyly of toesLeft hypoplastic humerus, dislocated el-
bow, adactylia 4th, 5th fingers; bilat-eral absent 5th rays of feet; bilateralgenu valgus
Syndactyly, left 2nd + 3rd, 4th + 5thtoes; 1%" leg length discrepancy
Congenital short femur, left, syndactylyleft 4th + 5th toes; left congenital BEamputation
Absent right 5th ray
Right congenital AE amputation; bilateralPFFD with fibular deficiency
Left congenital coxa vara; left clubfoot;bilateral genu valgus
Infantile idiopathic scoliosisSyndactyly left 2nd through 5th toesAbsent left pectoralis major; bilateral pes
planusIdiopathic scoliosisBilateral PFFD; Right congenital AE am-
putation; Right equinovalgus foot
Idiopathic scoliosis
NoneAbsense of right pectoralis major
Left CDH
osteotomies of the humerus or radius to correct rota-tiQnal and/or angular deformity. These osteotomieswere done because the combination of the three factors(fixed pronation of the forearm, flexion of the radiuson the humerus, bowing of the radius) produced the"hand on flank" deformity. Often the deformity was
not completely corrected with one osteotomy. One pa-tient had three osteotomies, another two, and two ofthe remaining three patients are scheduled to have asecond osteotomy. The results of these osteotomieswere considered good by the patients and their families,
both in terms of function and appearance. Postopera-tively, the limb rested in a more natural appearing po-sition, with the hand in front of the coronal plane ofthe body.
Technique of humeral osteotomy. If the involvedhand rests on the flank or on the buttock, the patier~tshould be considered a candidate for the osteotomy.
The objective of the operation is to place the hand infront of the trunk, with the forearm held in midrotation.Approximately 60° of elbow flexion is sought.
Radiographs are evaluated (1) to confirm the presenceof elbow and/or forearm synostosis and (2) to determine
the optimal site for osteotomy. --The patient is placed in a supine position on the
operating table. A lateral incision is used and the os-teotomy site is exposed subperiosteally. Marks are madeon the bone to verify its preosteotomy orientation. Aclosing wedge osteotomy is done, with its base placedanteriorly and medially (on the basis of the resting po-sition of the limb) and the apex posteriorly and laterally.If necessary, an added segment of bone (0.5 cm to 1.0
cm) can be removed to lessen the tension on the softtissues. The fragments are fixed with crossed wires.The incision is closed, and a cast is applied to the limb.
Because it is difficult to achieve the desired position
Vol. llA, No. 6November 1986
Ulnar deficiency 827
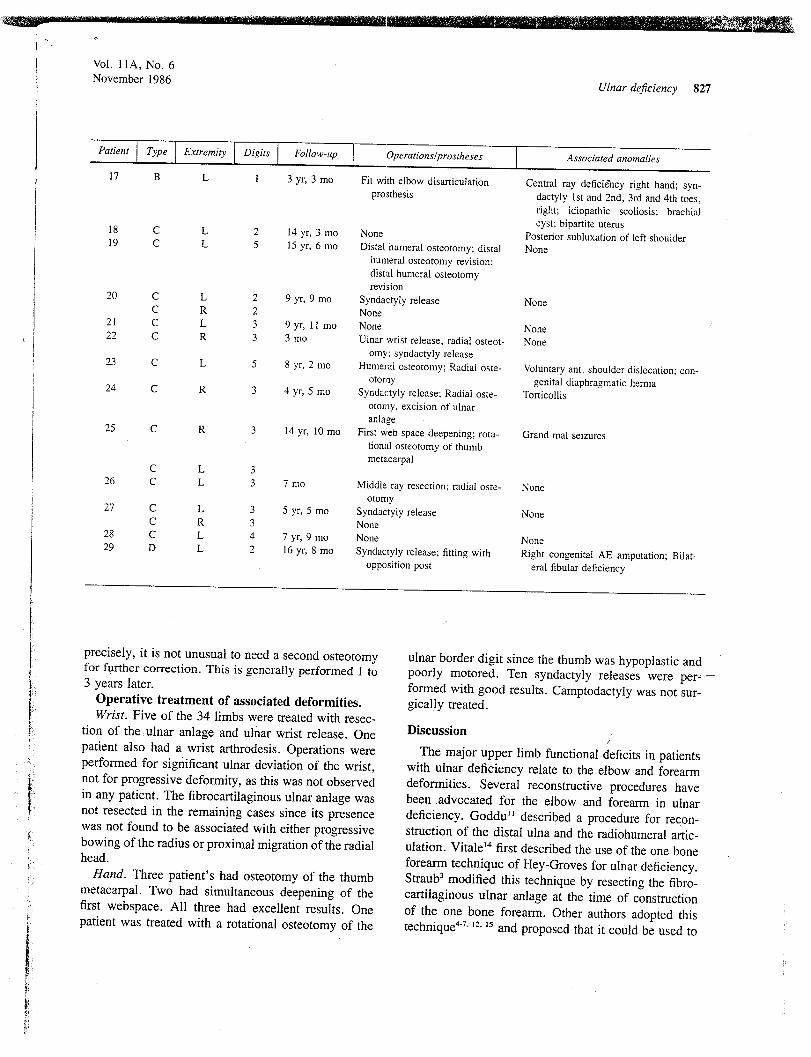
Patient Type Extremity Digits Follow-up Operations~prostheses Associated anomalies
17 B L 1 3 yr, 3 mo Fit with elbow disarticulation Central ray deficiency right hand; synoprosthesis dactyly 1st and 2nd, 3rd and 4th toes,
right; idiopathic scoliosis; brachialcyst; bipartite uterus18 C L 2 14 yr, 3 mo None Posterior subluxation of left shoulder19 C L 5 15 yr, 6 mo Distal humeral osteotomy; distal None
20 C L 2 9 yr, 9 mo Syndactyly release NoneC R 2 None
21 C L 3 9 yr, 11 mo None None22 C R 3 3 mo Ulnar wrist release, radial osteot- Noneomy; syndactyly release
23 C L 5 8 yr, 2 mo Humeral osteotomy; Radial oste- Voluntary ant. shoulder dislocation; con-otomy genital diaphragmatic hernia24 C R 3 4 yr, 5 mo Syndactyly release; Radiat oste- Torticollisotomy, excision of ulnaranlage
First web space deepening; rota-tional osteotomy of thumbmetacarpal
25 C R 3 14 yr, 10 mo Grand real seizures
c L 326 C L 3 7 mo Middle ray resection: radial oste- None
otomy27 C L 3 5 yr, 5 mo Syndactyly release NoneC R 3 None28 C L 4 7 yr, 9 mo None None29 D L 2 16 yr, 8 mo Syndactyly release: fitting with Right congenital AE amputation; Bilat-
opposition post eral fibular deficiency
precisely, it is not unusual to need a second osteotomyfor further correction. This is generally performed I to3 years later.
Operative treatment of associated deformities.Wrist. Five of the 34 limbs were treated with resec-
tion of the,ulnar anlage and ulnar wrist release. Onepatient also had a wrist arthrodesis. Operations wereperformed for significant ulnar deviation of the wrist,not for progressive deformity, as this was not observedin any patient. The fibrocartilaginous ulnar anlage wasnot resected in the remaining cases since its presencewas not found to be associated with either progressive
bowing of the radius or proximal migration of the radialhead.
Hand. Three patient’s had osteotomy of the thumbmetacarpal. Two had simultaneous deepening of thefirst webspace. All three had excellent results. Onepatient was treated with a rotational osteotomy of the
ulnar border digit since the thumb was hypoplastic andpoorly motored. Ten syndactyly releases were per---formed with good results. Camptodactyly was not sur-gically treated.
Discussion
The major upper limb functional deficits in patientswith ulnar deficiency relate to the elbow and forearmdeformities. Several reconstructive procedures havebeen .advocated for the elbow and forearm in ulnardeficiency. Goddu’~ described a procedure for recon-struction of the distal ulna and the radiohumeral artic-
ulation. Vitale~4 first described the use of the one boneforearm technique of Hey-Groves for ulnar deficiency.Straub3 modified this technique by resecting the fibro-cartilaginous ulnar anlage at the time of constructionof the one bone forearm. Other authors adopted this
technique4-7, ~2. ~5 and proposed that it could be used to
828 Miller, Wenner, and KrugerThe Journal of
HAND SURGERY
provide stability to the forearm and to correct a supi-nation deformity. Laurin and Farmer~3 and Blair andassociates9 observed good function in their patientswithout this procedure and did not recommend it. Wechose not to construct a one bone forearm in any ofour type A patients (who would be candidates for suchprocedure according to the above authors) for two rea-sons. First, progressive forearm shortening caused bythe dislocated radial head being driven proximally didnot occur. Second, many of our type A patients retaineda useful arc of forearm rotation, as Blair noted in hispatients. Such motion would be eliminated by the onebone forearm operation.
Frantz and O’Rahilly 8 recommended above elbowprosthetic fitting for patients with ulnar deficiency andan acutely flexed elbow with a cubitat web. Their resultswith release of the cubital web were poor. These," pa-tients would be classified as type B in our system. Ourexperience with these patients has been similar, withone unsuccessful attempt at release of a cubital web,and one successful above elbow prosthesis wearer. Fit-ting a prosthesis over a sensate limb requires early ac-ceptance by the patient and family. This explains whyone patient rejected the prosthesis when first fitted withit at age ten.
It is essential that type C patients be differentiatedfrom type D patients. The former may require correctiveosteotomies if the combined position of the elbow, fore-arm, and wrist is such to yield the "hand on flank"deformity. The type D patients should not require anoperation other than for their hands. The two types canbe distinguished at an early age, and it is helpfill tooffer this prognostic information to the parents.
The fibrocartilaginous ulnar anlage has been de-::scribed as the anatomic structure responsible for pro-gressive bowing of the radius, dislocation or synostosisof the radiohumeral joint, ulnar subluxation of the wrist,and loss of longitudinal growth of the radius.4’ 6.7.14. 15Ogden and colleagues4 recommended treatment by earlyresection to prevent these problems, and they reportedimprovement in the bowing of the radius after this pro-cedure. However, Broudy and Smith5 did not note in-creasing ulnar deviation of the wrist or late dislocationof the radial head in their series of 26 cases. We didnot observe any of the previous problems in 29 limbsthat did not have the ulnar anlage resected. We found
¯ this procedure useful to correct the ulnarly deviatedwrist. We do not recommend its use to prevent pro-gressive bowing of the radius, late radial head dislo-cation, or loss of longitudinal growth of the radius.
The hand deformities are best.treated in the usual
manner. The most useful procedures were rotationalosteotomy of a border digit and syndactyly release. Thehigh incidence of flexion deformities of the interpha-langeal joints has not been previously reported.
Atrophy and weakness about the shoulder girdle havebeen noted by others. Our description of four patientswith shoulder instability is a previously unreported find-ing. This represents another feature of the generalizedlimb bud defect. The finding is of clinical significanceif the patient is dislocating the shoulder in order to putthe hand into a functional position. This can be treated,as was done in two of our patients, through correctiveosteotomies to put the hand in a position of func-tion, while allowing the shoulder to remain in neutralposition.
Our series of patients had a very. high percentage ofassociated anomalies. This may be because of our statusas a referral center for limb deficient children and tothe special interest in this problem of the senior author(L. M. K.).
Conclusions
1. We believe this system for the classification ofulnar deficiency is useful for predicting prognosis andplanning treatment in a given case.
Type A. Dislocated radial head with bowed ra-dius. These patients do not require osteotomy to po-sition the hand in front of the body. One bone forearmconstruction is not necessary since progression of theradial bow, elbow instability, and loss of forearm lengthcaused by the dislocation have not been observed." Type B. Dislocated radial head, straight radius, cub-
ital web with flexed elbow.Function is improved by early fitting with an above
elbow type prosthesis. Release of the web is not_suc-cessful.
Type C. Radiohumeral synostosis with bowed ra-dius, variable presence of ulna.
Patients in this group, with more severe combinationsof deformities, will benefit from radial or humeral os-teotomy to position the hand in front of the body.
Type D. Radiohumeral synostosis with straight ra-dius, diminutive ulna.
These patients are easily identified at birth and shouldrequire no treatment for their elbow and forearm de-formities.
2. Resection of the fibrocartilaginous ulnar anlagewas useful only to correct fixed ulnar deviation at thewrist.
3. A new association is described--shoulder insta-bility in the patient with ulnar deficiency.
Vol. 1 tA, No. 6November 1986 Ulnar deficiency
REFERENCES
1. Entin MA: Reconstruction of congenital abnormalities ofthe upper extremities. J Bone Joint Surg [Am] 41:681,1959
10. Straub LR: Congenital absence of the radius and ulna. JBone Joint Surg [Am] 54:907, 1972
11. Goddu LA: Reconstruction of elbow and bone graft ofrudimentary ulna. N Engl J Med 202:i"142, 1930
12. Spinner M, Freundlich BD, Abeles ED: Management ofmoderate longitudinal arrest of development of the ulna.Clin Ortho 69:199, 1970
13. Laurin CA, Farmer AW: Congenital absence of ulna. CanJ Surg 2:204, 1959
14. Vitale CC: Reconstructive surgery for defects in the shaftof the ulna in children. J Bone Joint Surg [Am] 34:804,1952
15. Watson HK, Bohne WH: The role of the fibrous band inulnar deficient extremities. J Bone Joint Surg [Am]53:816, 1971
16. Kelilian H: Congenital deformities of the hand and fore-arm. Philadelphia, 1974, WB Saunders Co. pp 866-90
17. Tooms RE: The amputee. In Lovell WW, Winter RB,editors: Pediatric orthopedics. Philadelphia. 1978, JBLippincott Co, pp 1024-6
Brachymetacarpia and brachyphalangia
The x-ray features of 325 patients, with shortening of the metacarpals and/or phalanges wereanalyzed. Most patients with congenital hand anomalies (syndactyly, cleft hand, etc.) had shortened middle phalanx of the small finger only; however, some patients also had a shortenedmiddle phalanx of the index finger. The patients with brachymesophalangia of two and five raysalso had a tendency to have shortened middle phalanges of the index and small fingers. Some
patients’ anomalies, such as shortening of the middle phalanges in both the index and smallfingers, did not adequately fit Bell’s classification. The patients who had shortened metacarpalssometimes also had shortened middle and distal phalanges and a shortened metatarsus. Com-binations of shortened phalanges and/or metacarpals were so numerous that it was impossibleto fit them into any simple classification. (J HAND SURG 11A:829-36, 1986.)
Takayuki Miura, M,D., Shuhei Torii, M.D., and Ryogo Nakamura, M.D.,
Nagoya, Japan
Shortening of the metacarpal and phalan-
geal bones (brachydactyly) may be found in various
From the Department of Orthopaedic Surgery, School of Medicine,Nagoya University, Nagoya, Japan.
Received for publication Nov. 1 I, 1985; accepted in revised formMarch 28, 1986.
Reprint requests: Takayuki Miura, Department of Orthopaedic Sur-gery, School of Medicine, Nagoya University, 65 Tsurumacho,Showaku, Nagoya, Japan. 466.
congenital hand anomalies, such as syndactyly, clefthand, symbrachydactyly, and some malformation syn-dromes.~-~ However, an isolated brachymetacarpia orbrachyphalangia is occasionally seen and brachy-mesophalangia 5 (shortening in the middle phalanx ofthe small finger) is frequently found in persons ofJapanese origin. 2- ~
When shortening is limited to one phalanx of one ortwo digits there is no functional disturbance and, mor-