222 Cancer Control October 2011, Vol. 18, No. 4 tation. UCB is now used in a growing number of trans- plant centers worldwide for the treatment of metabolic and deposit diseases, bone marrow failure syndromes, hemoglobinopathies, and malignancies. As the number of UCB transplant procedures has increased, a growing body of evidence has demonstrated that this alternative source of HSCs could, at least in part, close the gap in finding a donor for patients who require a potentially curative allo- geneic transplant but lack a suitable related or unrelated adult donor. The use of UCB is standard practice in pe- diatrics and has become an expanding practice in adults for the treatment of malignant diseases. The advantages of UCB transplantation include rapid availability, low risk of infection transmission, absence of donor risk, and the relatively lower risk of graft-vs-host disease (GVHD) with From the Blood and Marrow Transplant Program and Division of Hematology, Oncology and Transplantation at the University of Minnesota, Minneapolis, Minnesota. Submitted February 8, 2011; accepted May 3, 2011. Address correspondence to Claudio G. Brunstein, MD, PhD, De- partment of Medicine, University of Minnesota, Mayo Mail Code 480, 420 Delaware Street, SE, Minneapolis, MN 55455. E-mail: [email protected]No significant relationship exists between the author and the com- panies/organizations whose products or services may be refer- enced in this article. Gene Elling. St. Lucia. Photograph. Umbilical cord blood transplantation is a useful treatment in several types of hematologic malignancies. Umbilical Cord Blood Transplantation for the Treatment of Hematologic Malignancies Claudio G. Brunstein, MD, PhD Background: The use of unrelated umbilical cord blood (UCB) has grown as an allogeneic source of hematopoietic cells for transplantation of patients with hematologic malignancies. As the number of UCB transplantation procedures has grown, an increasing number of publications have focused on disease-specific outcomes. Methods: This review focuses on the outcome data following UCB transplantation in subsets of hematologic malignancies in which experience with this graft source is greater. Results: Registry and single-institution reports regarding the outcomes of children and adults with acute leukemias after UCB transplantation include many patients, while data on the clinical outcomes of other leukemias are limited due in part to the small number of patients with these diseases. UCB is now routinely used as a source of hematopoietic stem cells (HSCs) in pediatric allogeneic transplantation when a suitable sibling donor is not available. Data also support the use of UCB as an alternative source of HSC for transplantation of patients with hematologic malignancies who lack a more conventional donor. Current data also support UCB for patients who require an allograft in the setting of prospective clinical trials. Conclusions: Along with safety and feasibility in UCB transplantation, continued study is needed that focuses on issues such as accelerating engraftment, extending access, ensuring quality, and examining outcomes in specific subgroups of patients. Introduction Over the last decade we have seen a significant increase in the use of umbilical cord blood (UCB) as a source of hematopoietic stem cells (HSCs) for allogeneic transplan-
Transcript
222 Cancer Control October 2011, Vol. 18, No. 4
tation. UCB is now used in a growing number of trans-plant centers worldwide for the treatment of metabolic and deposit diseases, bone marrow failure syndromes, hemoglobinopathies, and malignancies. As the number of UCB transplant procedures has increased, a growing body of evidence has demonstrated that this alternative source of HSCs could, at least in part, close the gap in fi nding a donor for patients who require a potentially curative allo-geneic transplant but lack a suitable related or unrelated adult donor. The use of UCB is standard practice in pe-diatrics and has become an expanding practice in adults for the treatment of malignant diseases. The advantages of UCB transplantation include rapid availability, low risk of infection transmission, absence of donor risk, and the relatively lower risk of graft-vs-host disease (GVHD) with
From the Blood and Marrow Transplant Program and Division of Hematology, Oncology and Transplantation at the University of Minnesota, Minneapolis, Minnesota.
Submitted February 8, 2011; accepted May 3, 2011.
Address correspondence to Claudio G. Brunstein, MD, PhD, De-partment of Medicine, University of Minnesota, Mayo Mail Code 480, 420 Delaware Street, SE, Minneapolis, MN 55455. E-mail: [email protected]
No signifi cant relationship exists between the author and the com-panies/organizations whose products or services may be refer-enced in this article.
Gene Elling. St. Lucia. Photograph.
Umbilical cord blood transplantation
is a useful treatment in several types
of hematologic malignancies.
Umbilical Cord Blood Transplantation for the Treatment of Hematologic Malignancies
Claudio G. Brunstein, MD, PhD
Background: The use of unrelated umbilical cord blood (UCB) has grown as an allogeneic source of hematopoietic cells for transplantation of patients with hematologic malignancies. As the number of UCB transplantation procedures has grown, an increasing number of publications have focused on disease-specifi c outcomes.Methods: This review focuses on the outcome data following UCB transplantation in subsets of hematologic malignancies in which experience with this graft source is greater.Results: Registry and single-institution reports regarding the outcomes of children and adults with acute leukemias after UCB transplantation include many patients, while data on the clinical outcomes of other leukemias are limited due in part to the small number of patients with these diseases. UCB is now routinely used as a source of hematopoietic stem cells (HSCs) in pediatric allogeneic transplantation when a suitable sibling donor is not available. Data also support the use of UCB as an alternative source of HSC for transplantation of patients with hematologic malignancies who lack a more conventional donor. Current data also support UCB for patients who require an allograft in the setting of prospective clinical trials.Conclusions: Along with safety and feasibility in UCB transplantation, continued study is needed that focuses on issues such as accelerating engraftment, extending access, ensuring quality, and examining outcomes in specifi c subgroups of patients.
IntroductionOver the last decade we have seen a signifi cant increase in the use of umbilical cord blood (UCB) as a source of hematopoietic stem cells (HSCs) for allogeneic transplan-
October 2011, Vol. 18, No. 4 Cancer Control 223
preserved graft-vs-malignancy effects. The disadvantages of UCB transplantation are the limited cell dose, delayed engraftment, and lack of additional immune cells if donor lymphocytes are needed. Controversial issues include, but are not limited to, immune reconstitution and risk of infections. While advances have improved results with UCB transplantation, outcomes with matched unrelated transplants have also improved. Determining the optimal source requires further study and is beyond the scope of this manuscript.
The fi eld of UCB transplantation has advanced from investigating its safety and feasibility to addressing more specifi c issues such as accelerating engraftment, extend-ing access, ensuring quality and, importantly, examining outcomes in specifi c subgroups of patients. This review focuses on our current knowledge about disease-specifi c outcomes with UCB transplantation.
LeukemiaLeukemia is currently the disease subset in which the largest amount of data is available regarding UCB trans-plantation, in particular acute leukemia. Registry and single-institution reports on the outcomes of both chil-dren and adults with acute leukemias after UCB trans-plantation include hundreds of patients. However, data on the clinical outcomes of other leukemias are limited due in part to the small number of patients with these diseases. Although most series on the outcomes of hema-tologic malignancies after UCB transplantation include a small number of patients with chronic myeloid leukemia (CML), myelodysplastic syndrome (MDS), and other my-eloproliferative disease, only a few reports address the specifi c outcomes associated with these diseases.
Acute Leukemia in ChildrenEarly reports of UCB transplantation tended to refl ect the outcomes of pediatric patients, with acute leukemia representing 30% to 50% of patients in most series.1-9 These initial series consisted mostly of pediatric patients, mainly because the cell dose available from a single UCB unit was not suffi cient for use with larger adolescent and adult patients.
Data on outcomes of children with acute leukemia fi rst became available in the late 1990s. Table 1 summa-rizes these outcomes from selected publications of the treatment of children with acute leukemia.7,10-18 These are mostly manuscripts that describe comparisons to other HSC sources. Acute leukemia patients were re-ported to have engraftment rates of about 80%, with treatment-related mortality (TRM) rates of 44%, relapse rates of approximately 40%, and event-free survival rates at 2 years of 30% to 40%.10,13 More recently, data on the treatment of acute leukemia from the Cord Blood Trans-plantation Study (COBLT) were reported.16,18 The data on infants and young children with acute leukemia showed rates of neutrophil engraftment of only 60%, relapse of
31%, and a probability of survival at 1 year of 47%.16 In a more recent report from COBLT on children with hema-tologic malignancies, 84% of whom had acute leukemia, the cumulative incidence of neutrophil engraftment was 80%, the relapse rate at 2 years was 20%, and the 2-year survival rate was 50%.18 In this later study, children who received better HLA-matched grafts achieved better sur-vival. These studies, however, included mostly patients treated in the 1990s, a time period in which the standard cell dose was lower and UCB grafts with up to 3 HLA mismatches were used more frequently. Moreover, the methodology of HLA typing changed, making it diffi cult to compare older reports with more recent series. The fi rst studies comparing UCB to unrelated adult donor (URD) bone marrow showed promising results with similar to slightly inferior outcomes after UCB transplan-tation.11,12,14 A registry-based landmark analysis by the Center for International Blood and Marrow Transplant Research (CIBMTR) compared UCB to the gold standard of 7–8/8 allele-matched URD bone marrow grafts.17 This study of recently treated patients again showed delayed neutrophil engraftment even though patients received UCB grafts that were selected based on modern standards of cell dosage for UCB graft selection. Interestingly, 4 of 6 HLA-matched UCB grafts had a higher TRM but a lower relapse risk, while 5–6/6 HLA-matched UCB grafts had a lower TRM and higher relapse risk. In contrast to prior studies comparing UCB to URD, this study showed that 6 of 6 HLA-matched UCB grafts had superior leukemia-free survival, compared to less well-matched UCB grafts and to URD grafts (Fig 1).17
Thus, considering the substantial body of evidence and experience of UCB transplantation for the treatment of acute leukemia in children, UCB is now routinely used as a source of HSC in pediatric allogeneic transplantation when a suitable sibling donor is not available.
Acute Leukemia in AdultsThe feasibility of UCB transplant in adults with acute leu-kemia was initially established by a large registry-based study of 68 patients (34 adults with acute leukemia)6 and by the adult cohort of COBLT, which included mostly acute leukemia patients.19 These early studies demon-strated that engraftment was poor in the small number of long-term survivors due in part to the nature of the study population, which consisted of many heavily pretreated patients with high-risk disease.
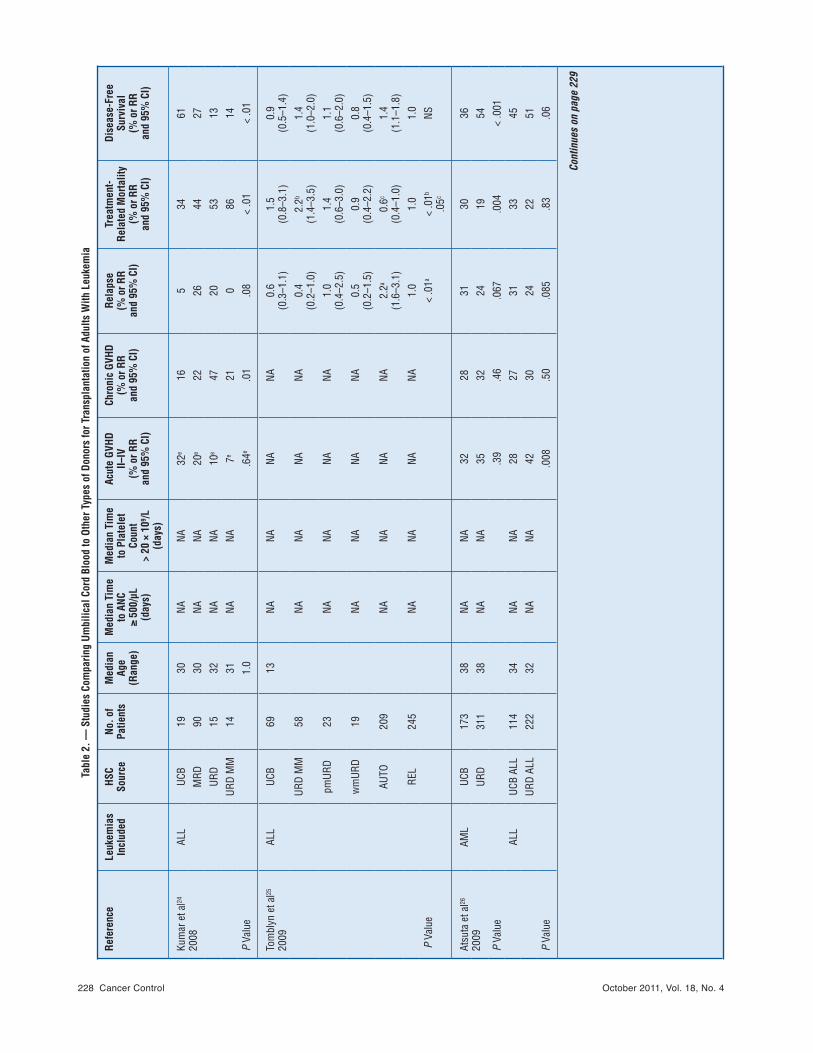
More recently, studies comparing the outcomes of adults with leukemia who received either UCB or adult donor HSC sources have become available (Table 2).20-28 Two landmark papers in particular advanced the fi eld of UCB transplantation in adults.20,21 These studies com-pared the outcomes of adults with leukemia undergoing transplantation with UCB or unrelated donor bone mar-row after myeloablative conditioning. In these studies, analysis of HLA-A and -B typing at the antigen level and
224 Cancer Control October 2011, Vol. 18, No. 4
Tabl
e 1.
— U
mbi
lical
Cor
d Bl
ood
Tran
spla
ntat
ion
for C
hild
ren
With
Leu
kem
iaa
Refe
renc
eHS
C So
urce
No. o
f Pa
tient
sNo
. of
Patie
nts
With
Le
ukem
ia
Med
ian
Age
(yrs
)
Neut
roph
ilEn
graf
tmen
t(%
)
Plat
elet
Engr
aftm
ent
(%)
Acut
e GV
HDII–
IV(%
or R
Ran
d 95
% C
I)
Chro
nic
GVHD
(% o
r RR
and
95%
CI)
Rela
pse
(% o
r RR
and
95%
CI)
Trea
tmen
t-Rel
ated
Mor
talit
y(%
or m
edia
n da
ys
to A
NC ≥
500
/µL)
Surv
ival
or
Dise
ase-
Free
Su
rviv
al(%
or R
Ran
d 95
% C
I)
Loca
telli
et a
l10
1999
UCB
unre
late
d60
605.
533
7837
2840
44 d
ays
42 a
t 1 y
r
UCB
rela
ted
4242
5.5
2785
4113
42
Bark
er e
t al11
2001
UCB
2617
4.5
8872
425
NA27
at 1
00 d
ays
53 a
t 2 y
rs
URD
mar
row
2617
4.7
9676
3520
15 a
t 100
day
s41
at 2
yrs
P Va
lue
NS.8
0.1
2.3
5.4
0UR
D31
125.
885
8436
7NA
23 a
t 100
day
s52
at 2
yrs
URD
TCD
mar
row
3112
6.8
9084
3513
16 a
t 100
day
s56
at 2
yrs
P Va
lue
NS>
.80
.32
.60
> .8
0
Roch
a et
al12
2001
UCB
9999
680
9033
2538
39 a
t 100
day
s35
at 2
ys
URD
mar
row
262
262
8.0
9685
5646
3919
at 1
00 d
ays
49 a
t 2 y
rs
URD
TCD
mar
row
180
180
8.0
9085
3412
4714
at 1
00 d
ays
41 a
t 2 y
rs
P Va
lue
.000
4NA
NA<
.001
< .0
01NA
UCB
< .0
1TC
D .1
9UC
B .5
5TC
D .0
7
Wag
ner e
t al7
2002
UCB
102
637
8865
at
180
days
3910
ALL:
high
risk
43
stan
dard
risk
10 AM
L:hi
gh ri
sk 4
7st
anda
rd ri
sk1
of 4
pat
ient
s
30 a
t 1 y
r58
at 1
yr,
70 a
t 1 y
r if
dose
> 1
.7 ×
10
5 CD3
4+/k
g,
60 a
t 2 y
rs
(non
mal
igna
nt
dise
ase)
, 38
at 2
yrs
(m
alig
nant
dis
ease
)
Mic
hel e
t al13
2003
UCB
9595
4.8
2658
3515
2920
day
s49
at 2
yrs
Cont
inue
s on
pag
e 22
5
October 2011, Vol. 18, No. 4 Cancer Control 225
Tabl
e 1.
— U
mbi
lical
Cor
d Bl
ood
Tran
spla
ntat
ion
for C
hild
ren
With
Leu
kem
iaa
Refe
renc
eHS
C So
urce
No. o
f Pa
tient
sNo
. of
Patie
nts
With
Le
ukem
ia
Med
ian
Age
(yrs
)
Neut
roph
ilEn
graf
tmen
t(%
)
Plat
elet
Engr
aftm
ent
(%)
Acut
e GV
HDII–
IV(%
or R
Ran
d 95
% C
I)
Chro
nic
GVHD
(% o
r RR
and
95%
CI)
Rela
pse
(% o
r RR
and
95%
CI)
Trea
tmen
t-Rel
ated
Mor
talit
y(%
or m
edia
n da
ys
to A
NC ≥
500
/µL)
Surv
ival
or
Dise
ase-
Free
Su
rviv
al(%
or R
Ran
d 95
% C
I)
Jaco
bsoh
n et
al14
2004
UCB
2626
688
7719
3315
1961
at 3
yrs
URD
mar
row
2323
4.4
9696
2240
2513
60 a
t 3 y
rs
P Va
lue
.000
4<
.001
< .0
01.8
3.6
6.7
2.7
1.7
2
Gluc
kman
et a
l15
2004
UCB
550
503
9.4
7643
at
60 d
ays
3626
2634
30 a
t 3 y
rs
Wal
l et a
l16
2005
UCB
3838
1.6
(infa
nt)
CINC
59
KM 6
9CI
NC 5
3KM
82
CINC
41
KM 4
4CI
NC 2
6KM
33
CINC
31
KM 4
614
of 3
2 pa
tient
s47
at 1
yr
Eape
n et
al17
2007
bUR
D m
arro
w11
611
6<
1697
851.
01.
01.
01.
01.
0
URD
mar
row
HLA
mis
mat
ched
166
166
< 16
9774
1.51
(1
.08–
2.13
)1.
62
(1.0
8–2.
45)
0.77
(0
.51–
1.16
)1.
42
(0.8
7–2.
32)
0.99
(0
.73–
1.36
)
UCB
503
503
< 16
6/
685
790.
45
(0.2
2–0.
96)
0.76
(0
.35–
1.64
)0.
8
(0.3
5–1.
32)
0.26
(0
.06–
1.09
)0.
54
(0.3
0–0.
97)
5/
6high
8064
0.92
(0
.63–
1.34
)0.
60
(0.3
5–1.
02)
0.67
(0
.43–
1.02
)1.
48
(0.8
9–2.
46)
0.94
(0
.68–
1.31
)
5/6lo
w59
430.
76
(0.4
3–1.
34)
0.98
(0
.43–
2.22
)0.
72
(0.3
5–1.
51)
1.88
(1
.01–
3.47
)1.
12
(0.7
1–1.
75)
4/
676
470.
92
(0.6
6–1.
30)
0.72
(0
.45–
1.14
)0.
54
(0.3
6–0.
83)
2.31
(1
.47–
3.62
)1.
17
(0.8
7–1.
57)
Kurtz
berg
et a
l18
2008
UCB
191
180
7.7
8050
at
180
days
4220
2017
at 1
00 d
ays
57 a
t 1 y
r
a Unl
ess
othe
rwis
e sp
ecifi
ed, c
linic
al o
utco
mes
des
crib
ed a
re fo
r the
who
le c
ohor
t.b 6
/6 =
HLA
-mat
ched
UCB
, 5/6
high
= 1
-locu
s HL
A-m
ism
atch
ed U
CB w
ith h
igh
cell
dose
, 5/6
low =
1-lo
cus
HLA-
mis
mat
ched
UCB
with
low
cel
l dos
e, 4
/6 =
2-lo
ci H
LA-m
ism
atch
ed U
CB.
Resu
lts fo
r acu
te a
nd c
hron
ic G
VHD,
TRM
, rel
apse
, and
tim
e to
trea
tmen
t fai
lure
(sho
wn
in th
e su
rviv
al c
olum
n) a
re re
lativ
e ris
ks u
sing
the
alle
le-m
atch
ed u
nrel
ated
mar
row
gro
ups
as th
e re
fere
nce
(RR
1.0)
.HS
C =
hem
atop
oiet
ic s
tem
cel
ls,
GVHD
= g
raft-
vs-h
ost d
isea
se, U
CB =
um
bilic
al c
ord
bloo
d, U
RD =
unr
elat
ed v
olun
teer
don
or, R
EL =
rela
ted,
TCD
= T
-cel
l dep
lete
d, A
LL =
acu
te ly
mph
obla
stic
leuk
emia
, AM
L =
acut
e m
yelo
id le
ukem
ia, C
INC
= cu
mul
ativ
e in
cide
nce,
KM
= K
apla
n-M
eier
, NS
= no
t sig
nifi c
ant,
NA =
not
ava
ilabl
e.
226 Cancer Control October 2011, Vol. 18, No. 4
DRB1 at the allele level was performed, and leukemia-free survival was similar for recipients of UCB and unrelated donor bone marrow. Despite some methodological dif-ferences, these studies reported that leukemia-free sur-vival for UCB was similar to mismatched URD and similar to slightly inferior to matched URD. These studies set the stage for an increase in the utilization of UCB as a source of HSC for adult transplantation worldwide. More recently, two additional registry-based studies revisited the issue of the effi cacy of UCB relative to URD grafts.26,27 A study from the Japan Cord Blood Bank Network and the Japan Marrow Donor Program examined the out-comes of patients with acute myeloid leukemia (AML) and acute lymphoblastic leukemia (ALL) who received 4–6/6 HLA-matched UCB grafts to 8/8 allele-matched URD bone marrow.26 Both ALL and AML patients were found to have signifi cantly lower rates of neutrophil engraftment. Relapse rates were similar for both graft sources. Notably, while outcomes for ALL patients were similar for both graft sources, UCB recipients with AML had a higher rate of TRM and a lower rate of leukemia-free survival compared to bone marrow transplantation (Table 2). The authors attributed these fi ndings not only to delayed engraftment after UCB transplantation but also to the relative risk of acute and chronic GVHD among bone marrow recipients. A collaboration between the CIBMTR and Eurocord registries led to an updated study in adult patients with leukemia comparing UCB to URD grafts.27 In contrast to prior registry studies, this analysis compared the outcomes of 4–6/6 HLA-matched UCB grafts with a cryopreserved nucleated cell dose of ≥ 2.5
× 107/kg to 7–8/8 allele-matched URD grafts from bone marrow and/or peripheral blood. While TRM was higher among recipients of UCB, the leukemia-free survival was similar for all graft types, thus further supporting the utilization of UCB as an alternative source of HSC for patients with low-risk and high-risk leukemia (Fig 2) with no HLA-matched unrelated donor. Single institutions have also compared UCB with adult donor stem cell sources in cohorts that largely consisted of patients with leukemia.22-26 Takahashi et al22 studied 113 patients with hematologic malignancies (70% with acute leukemia) who received either 3–6/6 HLA-matched UCB or 5–6/6 HLA-matched URD grafts. In contrast to registry-based studies, they observed a lower risk of TRM and better disease-free survival after UCB transplantation. Another report by Takahashi et al23 compared 171 patients with hematologic malignancies (70% with acute leukemia) who received either UCB or related donor grafts (pe-ripheral blood and bone marrow). While the incidence of severe acute and extensive chronic GVHD was lower in recipients of UCB grafts, the incidences of grade II–IV GVHD, TRM, relapse, and disease-free survival were simi-lar for both HSC sources.
As the number of adults receiving UCB transplanta-tion is still relatively small, most series have not provided outcomes for specifi c leukemia subtypes. Reports on the outcomes of patients with AML are promising, with fac-tors that infl uence these outcomes ranging from graft selection to disease stage at transplantation.29-31 Ooi et al29 reported on 18 patients with de novo AML who received single UCB grafts after myeloablative condition-
Fig 1. — Leukemia-free survival of children with acute leukemia after myeloablative single umbilical cord blood or unrelated donor bone marrow transplantation. From Eapen M, Rubinstein P, Zhang MJ, et al. Outcomes of transplantation of unrelated donor umbilical cord blood and bone marrow in children with acute leukaemia: a comparison study. Lancet. 2007;369(9577):1947-1954. Reproduced with permission from Elsevier.
October 2011, Vol. 18, No. 4 Cancer Control 227
Tabl
e 2.
— S
tudi
es C
ompa
ring
Umbi
lical
Cor
d Bl
ood
to O
ther
Typ
es o
f Don
ors
for T
rans
plan
tatio
n of
Adu
lts W
ith L
euke
mia
Refe
renc
eLe
ukem
ias
Incl
uded
HSC
Sour
ceNo
. of
Patie
nts
Med
ian
Age
(Ran
ge)
Med
ian
Tim
e to
ANC
≥
500/
µL(d
ays)
Med
ian
Tim
e to
Pla
tele
t Co
unt
> 20
× 1
09 /L(d
ays)
Acut
e GV
HD
II–IV
(% o
r RR
and
95%
CI)
Chro
nic
GVHD
(% o
r RR
and
95%
CI)
Rela
pse
(% o
r RR
and
95%
CI)
Trea
tmen
t-Re
late
d M
orta
lity
(% o
r RR
and
95%
CI)
Dise
ase-
Free
Su
rviv
al(%
or R
R an
d 95
% C
I)
Laug
hlin
et a
l20
2004
AML
ALL
MDS
UCB
150
(16–
60)d
2760
0.81
a
(0.5
9–1.
10)
0.66
b
(0.4
4–0.
99
1.62
(1.0
8–2.
42)
1.12
(0.6
3–2.
02)
0.73
(0.4
6–1.
14)
0.85
(0.4
3–1.
70)
1.89
(1
.45–
2.48
) 0.
99
(0.7
0–1.
40)
1.48
(1
.18–
1.86
) 0.
94
(0.6
9–1.
28)
URD
mar
row
367
(16–
60)d
2029
1.0a
1.0a
1.0a
1.0a
1.0a
URD
MM
mar
row
83(1
6–60
)d18
291.
0b1.
0b1.
0b1.
0b1.
0b
P V
alue
< .0
01<
.001
.17a
.04b
.02a
.69b
.16a
.65b
< .0
01a
.96b
.001
a
.69b
Roch
a et
al21
2004
AML
ALL
UCB
9825
(15–
55)
26NA
0.57
(0.3
7–0.
87)
0.64
(0.3
7–1.
1)1.
02(0
.63–
1.65
)1.
13(0
.78–
1.64
)0.
95(0
.72–
1.25
)
URD
mar
row
584
32(1
5–59
)19
NA1.
01.
01.
01.
01.
0
P Va
lue
.001
NA.0
1.1
1.9
3.5
0.7
0
Taka
hash
i et a
l22
2004
AML
ALL
MDS
CML
UCB
6836
(16–
53)
2240
0.61
(0.3
7–1.
01)
0.60
(0.2
8–1.
28)
0.75
(0.1
6–3.
56)
0.32
(0.1
2–0.
86)
0.27
(0.1
4–0.
51)
URD
mar
row
4526
(16–
50)
1825
1.0
1.0
1.0
1.0
1.0
P Va
lue
.01
.01
.05
.18
.73
.02
< .0
1
Taka
hash
i et a
l23
2007
AML
ALL
MDS
CML
UCB
9238
2240
1.09
(0.7
1–1.
68)
0.49
(0.2
9–0.
85)
0.72
(0.4
4–1.
25)
0.49
(0.1
9–1.
24)
0.74
(0.4
4–1.
25)
REL
7140
1722
.51.
01.
01.
01.
01.
0
P Va
lue
.83
< .0
1<
.01
.69
.01
.26
.13
.26
Cont
inue
s on
pag
e 22
8
228 Cancer Control October 2011, Vol. 18, No. 4
Tabl
e 2.
— S
tudi
es C
ompa
ring
Umbi
lical
Cor
d Bl
ood
to O
ther
Typ
es o
f Don
ors
for T
rans
plan
tatio
n of
Adu
lts W
ith L
euke
mia
Refe
renc
eLe
ukem
ias
Incl
uded
HSC
Sour
ceNo
. of
Patie
nts
Med
ian
Age
(Ran
ge)
Med
ian
Tim
e to
ANC
≥
500/
µL(d
ays)
Med
ian
Tim
e to
Pla
tele
t Co
unt
> 20
× 1
09 /L(d
ays)
Acut
e GV
HD
II–IV
(% o
r RR
and
95%
CI)
Chro
nic
GVHD
(% o
r RR
and
95%
CI)
Rela
pse
(% o
r RR
and
95%
CI)
Trea
tmen
t-Re
late
d M
orta
lity
(% o
r RR
and
95%
CI)
Dise
ase-
Free
Su
rviv
al(%
or R
R an
d 95
% C
I)
Kum
ar e
t al24
2008
ALL
UCB
1930
NANA
32e
165
3461
MRD
9030
NANA
20e
2226
4427
URD
1532
NANA
10e
4720
5313
URD
MM
1431
NANA
7e21
086
14P
Valu
e1.
0.6
4e.0
1.0
8<
.01
< .0
1
Tom
blyn
et a
l25
2009
ALL
UCB
6913
NANA
NANA
0.6
(0.3
–1.1
)1.
5(0
.8–3
.1)
0.9
(0.5
–1.4
)UR
D M
M58
NANA
NANA
0.4
(0.2
–1.0
)2.
2b
(1.4
–3.5
)1.
4(1
.0–2
.0)
pmUR
D23
NANA
NANA
1.0
(0.4
–2.5
)1.
4(0
.6–3
.0)
1.1
(0.6
–2.0
)w
mUR
D19
NANA
NANA
0.5
(0.2
–1.5
)0.
9(0
.4–2
.2)
0.8
(0.4
–1.5
)AU
TO20
9NA
NANA
NA2.
2a
(1.6
–3.1
)0.
6c
(0.4
–1.0
)1.
4(1
.1–1
.8)
REL
245
NANA
NANA
1.0
1.0
1.0
P V
alue
< .0
1a<
.01b
.05c
NS
Atsu
ta e
t al26
2009
AML
UCB
173
38NA
NA32
2831
3036
URD
311
38NA
NA35
3224
1954
P Va
lue
.39
.46
.067
.004
< .0
01AL
LUC
B AL
L11
434
NANA
2827
3133
45UR
D AL
L22
232
NANA
4230
2422
51P
Valu
e.0
08.5
0.0
85.8
3.0
6
Cont
inue
s on
pag
e 22
9
October 2011, Vol. 18, No. 4 Cancer Control 229
Tabl
e 2.
— S
tudi
es C
ompa
ring
Umbi
lical
Cor
d Bl
ood
to O
ther
Typ
es o
f Don
ors
for T
rans
plan
tatio
n of
Adu
lts W
ith L
euke
mia
Refe
renc
eLe
ukem
ias
Incl
uded
HSC
Sour
ceNo
. of
Patie
nts
Med
ian
Age
(Ran
ge)
Med
ian
Tim
e to
ANC
≥
500/
µL(d
ays)
Med
ian
Tim
e to
Pla
tele
t Co
unt
> 20
× 1
09 /L(d
ays)
Acut
e GV
HD
II–IV
(% o
r RR
and
95%
CI)
Chro
nic
GVHD
(% o
r RR
and
95%
CI)
Rela
pse
(% o
r RR
and
95%
CI)
Trea
tmen
t-Re
late
d M
orta
lity
(% o
r RR
and
95%
CI)
Dise
ase-
Free
Su
rviv
al(%
or R
R an
d 95
% C
I)
Eape
n et
al27
2010
AML
ALL
UCB
165
2824
52NA
NANA
NANA
URD
mar
row
332
3919
280.
78
(0.5
6–1.
08)
0.63
(0.4
4–0.
90)
0.85
(0.5
9–1.
20)
1.69
(1.1
9–2.
39)
1.15
(0.9
0–1.
47)
URD
mar
row
MM
140
0.59
(0.4
1–0.
86)
0.59
(0.3
9–0.
90)
0.84
(0.5
5–1.
28)
1.06
(0.7
2–1.
58)
0.93
(0.6
9–1.
24)
URD
PB63
233
1419
0.57
(0.4
2–0.
77)
0.38
(0.2
7–0.
53)
0.85
(0.6
1–1.
17)
1.62
(1.1
8–2.
23)
1.12
(0.8
9–1.
39)
URD
PB
MM
256
0.49
(0.3
5–0.
68)
0.46
(0.3
2–0.
67)
0.91
(0.6
7–1.
32)
0.95
(0.6
8–1.
34)
0.91
(0.7
1–1.
17)
P Va
lue
< .0
001
< .0
001
NA.0
01<
.000
1.8
6<
.000
1.0
9
Brun
stei
n et
al28
2010
AML
ALL
MDS
CML
dUCB
128
2526
531.
01.
01.
01.
01.
0M
RD20
440
1620
1.08
(0.8
2–1.
43)
1.58
a
(1.0
3–2.
43)
3.67
a
(2.1
4–6.
27)
0.31
a (0
.18–
0.53
)1.
09(0
.80–
1.49
)UR
D15
231
1921
1.83
a
(1.3
6–2.
47)
1.71
b
(1.1
2–2.
63)
3.05
a
(2.1
4–6.
27)
0.61
(0.3
3–1.
15)
0.85
(0.6
1–1.
20)
URD
MM
5231
18.5
212.
35a
(1.5
2–3.
63)
2.07
b
(1.1
9–3.
60)
2.50
a
(1.2
3–5.
07)
0.38
a
(0.2
4–0.
59)
1.12
(0.7
3–1.
73)
P Va
lue
< .0
1<
.01
< .0
1<
.01
.03a
.01b
< .0
1<
.01
NS
a Ind
icat
es re
latio
n be
twee
n pe
rcen
tage
or R
R re
sults
in th
e sp
ecifi
c ta
ble
colu
mn
and
the
P va
lues
for t
hat c
olum
n w
ithin
the
sam
e st
udy.
b RR
appl
ies
to c
ompa
rison
bet
wee
n UC
B co
mpa
red
to m
atch
ed U
RD.
c RR
appl
ies
to c
ompa
rison
bet
wee
n UC
B co
mpa
red
to m
ism
atch
ed U
RD.
d Age
repo
rted
by in
terv
als
of 1
6–20
, 21–
30, 3
1–40
, 41–
50, a
nd 5
1–60
. No
med
ian
avai
labl
e.e R
efer
s to
gra
de II
I–IV
acu
te G
VHD.
Dat
a on
gra
de II
–IV
wer
e no
t ava
ilabl
e.HS
C =
hem
atop
oiet
ic s
tem
cel
l, AN
C =
abso
lute
neu
troph
il co
unt,
GVHD
= g
raft-
vs-h
ost d
isea
se, A
ML
= ac
ute
mye
loid
leuk
emia
, ALL
= a
cute
lym
phob
last
ic le
ukem
ia, M
DS =
mye
lody
spla
stic
syn
drom
e,
UCB
= um
bilic
al c
ord
bloo
d, U
RD =
unr
elat
ed d
onor
, URD
MM
= H
LA-m
ism
atch
ed u
nrel
ated
don
or, C
ML
= ch
roni
c m
yelo
id le
ukem
ia, R
EL =
rela
ted
dono
r with
no
refe
renc
e to
HLA
-mat
chin
g, M
RD =
mat
ched
un
rela
ted
dono
rs, p
mUR
D =
parti
ally
HLA
-mat
ched
unr
elat
ed d
onor
, wm
URD
= w
ell H
LA-m
atch
ed u
nrel
ated
don
or, A
UTO
= au
tolo
gous
don
or, d
UCB
= do
uble
um
bilic
al c
ord
bloo
d, C
I = c
onfi d
ence
inte
rval
, NS
= n
ot s
igni
fi can
t.
230 Cancer Control October 2011, Vol. 18, No. 4
ing. Seventeen of the 18 patients achieved neutrophil recovery, and 16 achieved sustained platelet recovery. Half of the 6 patients died of AML relapse. One patient died of treatment-related causes. At the time of the re-port, 14 patients were alive and disease-free, resulting in a disease-free survival rate of 77% at 2 years. In a more recent report, Sanz et al30 evaluated 49 adults with AML treated with myeloablative UCB transplantation. In this study, UCB selection took into consideration both the nucleated and CD34+ cell doses. The cumulative inci-dence rates of neutrophil and platelet engraftment were 96% and 73%, respectively. The incidence of TRM was 39%, with a relapse rate of 19% at 2 years. The overall leukemia-free survival rate in this cohort was 37% at 4
years, which was infl uenced by the infused nucleated cell dose. A preliminary study describing the outcomes of AML after reduced-intensity conditioning was presented at the 2006 American Society of Hematology meeting.31 This study included patients with high-risk AML who received either a 4–6/6 HLA-matched UCB graft (n = 43) or an HLA-matched sibling peripheral blood stem cell (PBSC) graft (n = 21). Most of the UCB grafts (n = 28) consisted of two UCB units. In this limited number of patients, the proportion of engraftment was not signifi -cantly lower after UCB (88% vs 100%, P = .10). When comparing UCB and PBSC recipients, there were similar incidence rates of TRM at 1 year (28% vs 38%, P = .43) and relapse rates at 2 years (35% vs 35%, P = .72), resulting
Fig 2. — Leukemia-free survival of adults with acute leukemia after myeloablative transplantation comparing single umbilical cord blood to unrelated donor 7–8/8 allele level HLA-matched bone marrow and peripheral blood with low- (A) and high-risk disease (B). PBPC = peripheral blood progenitor cells, UCB = umbilical cord blood. From Eapen M, Rocha V, Sanz G, et al. Effect of graft source on unrelated donor haemopoietic stem-cell transplantation in adults with acute leukaemia: a retrospective analysis. Lancet Oncol. 2010;11(7):653-660. Reproduced with permission from Elsevier.
A
B
8/8 matched bone marrowNumber at Risk
7/8 matched bone marrow8/8 matched PBPC7/8 matched PBPC
4/6–6/6 matched UCB
246106452166123
17769
3168977
13946
2206647
9935
1434530
82
Months
Leu
kem
ia-F
ree
Su
rviv
al (
%)
100
80
50
40
20
0
90
70
60
30
10
Bone marrow matchedBone marrow mismatchedPBPC matchedPBPC mismatchedUCB
Bone marrow matchedBone marrow mismatchedPBPC matchedPBPC mismatchedUCB
0 6 12 18 24
311123624
8/8 matched bone marrowNumber at Risk
7/8 matched bone marrow8/8 matched PBPC7/8 matched PBPC
4/6–6/6 matched UCB
8634
1809042
3112633417
175
391910
133
1912
9
10
Leu
kem
ia-F
ree
Su
rviv
al (
%)
100
80
50
40
20
0
90
70
60
30
10
Months0 6 12 18 24
314
86
October 2011, Vol. 18, No. 4 Cancer Control 231
in similar survival rates at 2 years (31% vs 32%, P = .62). In multivariate analysis, only the disease-risk group was associated with an increased relative risk (RR) of relapse (RR = 2.9, 95% confi dence interval [CI], 1.3–6.2, P < .01) and death (RR = 2.6, 95% CI, 1.1–5.5, P = .02). Inves-tigators at the University of Minnesota compared the outcomes of UCB to other graft sources after myeloabla-tive conditioning for the treatment of ALL.24,25 Signifi cant differences were reported among the stem cell sources regarding year of transplantation, time from diagnosis to transplantation and, as expected, cell doses infused. The worst outcomes were observed after autologous transplantation25 and mismatched URD graft.24,25 While other graft sources including UCB had similar leukemia-free survival, other factors that were predictors of poorer outcome were advanced disease (≥ CR3), white blood cell count ≥ 30 × 109/L at diagnosis, a cytomegalovirus seropositive recipient or donor, and ≥ 2 induction cycles to achieve a complete response. In patients transplanted in CR1–2, independent predictors of poorer outcomes were older age, white blood cell count ≥ 30 × 109/L at diagnosis, and mismatched URD graft.
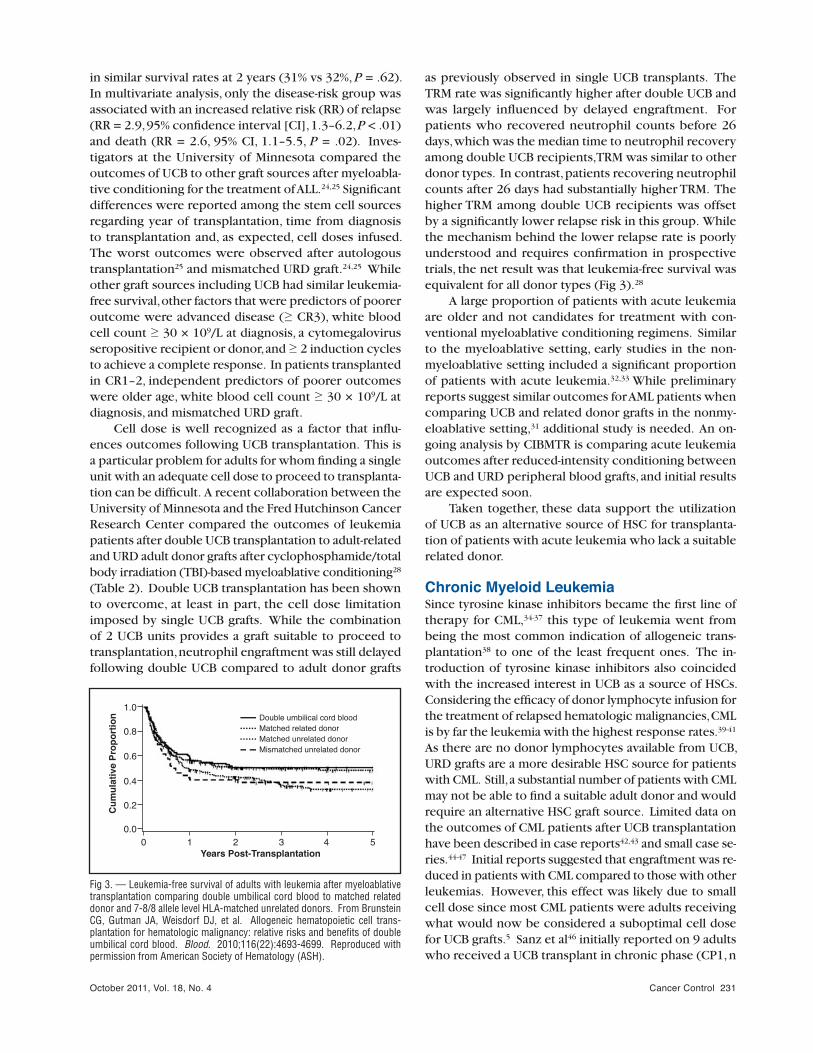
Cell dose is well recognized as a factor that infl u-ences outcomes following UCB transplantation. This is a particular problem for adults for whom fi nding a single unit with an adequate cell dose to proceed to transplanta-tion can be diffi cult. A recent collaboration between the University of Minnesota and the Fred Hutchinson Cancer Research Center compared the outcomes of leukemia patients after double UCB transplantation to adult-related and URD adult donor grafts after cyclophosphamide/total body irradiation (TBI)-based myeloablative conditioning28 (Table 2). Double UCB transplantation has been shown to overcome, at least in part, the cell dose limitation imposed by single UCB grafts. While the combination of 2 UCB units provides a graft suitable to proceed to transplantation, neutrophil engraftment was still delayed following double UCB compared to adult donor grafts
as previously observed in single UCB transplants. The TRM rate was signifi cantly higher after double UCB and was largely infl uenced by delayed engraftment. For patients who recovered neutrophil counts before 26 days, which was the median time to neutrophil recovery among double UCB recipients, TRM was similar to other donor types. In contrast, patients recovering neutrophil counts after 26 days had substantially higher TRM. The higher TRM among double UCB recipients was offset by a signifi cantly lower relapse risk in this group. While the mechanism behind the lower relapse rate is poorly understood and requires confi rmation in prospective trials, the net result was that leukemia-free survival was equivalent for all donor types (Fig 3).28
A large proportion of patients with acute leukemia are older and not candidates for treatment with con-ventional myeloablative conditioning regimens. Similar to the myeloablative setting, early studies in the non-myeloablative setting included a signifi cant proportion of patients with acute leukemia.32,33 While preliminary reports suggest similar outcomes for AML patients when comparing UCB and related donor grafts in the nonmy-eloablative setting,31 additional study is needed. An on-going analysis by CIBMTR is comparing acute leukemia outcomes after reduced-intensity conditioning between UCB and URD peripheral blood grafts, and initial results are expected soon.
Taken together, these data support the utilization of UCB as an alternative source of HSC for transplanta-tion of patients with acute leukemia who lack a suitable related donor.
Chronic Myeloid LeukemiaSince tyrosine kinase inhibitors became the fi rst line of therapy for CML,34-37 this type of leukemia went from being the most common indication of allogeneic trans-plantation38 to one of the least frequent ones. The in-troduction of tyrosine kinase inhibitors also coincided with the increased interest in UCB as a source of HSCs. Considering the effi cacy of donor lymphocyte infusion for the treatment of relapsed hematologic malignancies, CML is by far the leukemia with the highest response rates.39-41 As there are no donor lymphocytes available from UCB, URD grafts are a more desirable HSC source for patients with CML. Still, a substantial number of patients with CML may not be able to fi nd a suitable adult donor and would require an alternative HSC graft source. Limited data on the outcomes of CML patients after UCB transplantation have been described in case reports42,43 and small case se-ries.44-47 Initial reports suggested that engraftment was re-duced in patients with CML compared to those with other leukemias. However, this effect was likely due to small cell dose since most CML patients were adults receiving what would now be considered a suboptimal cell dose for UCB grafts.5 Sanz et al46 initially reported on 9 adults who received a UCB transplant in chronic phase (CP1, n
Years Post-Transplantation
Cu
mu
lati
ve P
rop
ort
ion
1.0
0.0
0.2
0.6
0.8
0.4
0 1 2 3 4 5
Double umbilical cord blood
Mismatched unrelated donorMatched unrelated donorMatched related donor
Fig 3. — Leukemia-free survival of adults with leukemia after myeloablative transplantation comparing double umbilical cord blood to matched related donor and 7-8/8 allele level HLA-matched unrelated donors. From Brunstein CG, Gutman JA, Weisdorf DJ, et al. Allogeneic hematopoietic cell trans-plantation for hematologic malignancy: relative risks and benefi ts of double umbilical cord blood. Blood. 2010;116(22):4693-4699. Reproduced with permission from American Society of Hematology (ASH).
232 Cancer Control October 2011, Vol. 18, No. 4
= 5; CP2, n = 1), accelerated phase (n = 1) or blast crisis (n = 2). All had failed more conventional treatments and autologous transplantation (n = 3) and lacked a suitable unrelated or related donor. Patients were conditioned with a myeloablative regimen using a combination of thiotepa, busulfan, cyclophosphamide or fl udarabine, and antithymocyte globulin (ATG). Four of the 9 patients, all transplanted in chronic phase, had prolonged remissions. This group recently updated their experience, reporting outcomes for 26 patients who received the same condi-tioning regimen.47 Most patients were in chronic phase (CP1, n = 7; CP2, n = 11). All patients in accelerated phase or blast crisis died of transplant-related causes. For the whole cohort, the disease-free survival rate at 8 years was 41% for all patients and 59% for only chronic phase patients. In another report, 20 patients with CML (CP1, n = 6; accelerated phase, n = 14) received UCB transplants after myeloablative (n = 12) or nonmyeloablative (n = 8) conditioning.45 With the exception of time to neutrophil engraftment, which was longer for myeloablation (21 vs 13 days), both conditioning regimens resulted in similar rates of acute GVHD, TRM, relapse, and survival. Notably, the relapse rate was approximately 10% and the overall survival rate was 50%. Although a large proportion of patients were transplanted with advanced disease, relapse rates were low, suggesting a potent graft-vs-leukemia ef-fect of UCB in CML.5,44-47
Myelodysplastic SyndromeMDS is a relatively uncommon hematologic malignancy, and the only potentially curative therapy for MDS is allo-geneic HSC transplantation. Ooi et al48 initially reported on 13 adults with MDS and AML secondary to MDS who received single UCB grafts after myeloablative condition-ing. Notably, neutrophil recovery occurred in 12 of 13 patients, with 10 patients being alive and disease-free at the time of their report. In an update of this cohort that included 33 patients, they continue to observe a high incidence of neutrophil engraftment (90%), low TRM (14%), low relapse risk (16%), and an encouraging event-free survival rate at 5 years of 70%.49 A Eurocord study of 171 adult recipients of UCB transplants, includ-ing 16 patients (9%) with MDS, reported a 30% relapse rate.44 An analysis of a larger number of MDS patients should be available soon. A report from the University of Minnesota50 described the outcomes of 84 adults with MDS undergoing myeloablative (62%) and nonmyeloabla-tive (38%) transplantation, of whom 26 patients (31%) received UCB grafts. Although engraftment was delayed after UCB transplant, the cumulative incidence of engraft-ment did not signifi cantly differ from other donor types. Relapse and disease-free survival rates were similar across donor types. The main determinant of outcome seemed to be the percentage of blasts at the time of transplanta-tion, in which patients with < 5% blasts had a lower risk of relapse (16% vs 35%, P = .06) and a better disease-free
survival at 5 years (42% vs 19%, P = .12). Investigators at Duke University recently published a pediatric series involving 23 patients with MDS who received 4–6/6 HLA-matched UCB grafts and TBI-based myeloablative conditioning. Outcomes for this cohort were comparable to previous studies, with a neutrophil engraftment rate of 80%, a relapse risk of 13%, a TRM rate of 27%, and an event-free survival rate at 3 years of 61%. Taken together, these limited data suggest that MDS patients who lack a suitable, more conventional donor can be considered for UCB transplantation, preferably in prospective studies.
Lymphoid MalignanciesUCB has recently been evaluated for the treatment of lymphomas and multiple myeloma. Although data on multiple myeloma are limited to a few cases in larger series or case reports,51-55 several studies on patients with lymphomas treated with UCB transplantation sug-gest that UCB may be a valuable alternative for patients with this diagnosis who require an allogeneic transplant (Table 3).56-61 Yuji et al56 reported the outcomes of 20 patients with Hodgkin and non-Hodgkin lymphomas after reduced-intensity conditioning and UCB transplanta-tion. The conditioning regimen consisted of fl udarabine, melphalan, and 4 Gy of TBI. Although 8 patients died of transplant-related causes, 15 achieved primary neutro-phil recovery and 10 were alive and progression-free at the time of the report. An updated analysis by this same group on 110 patients with low-, intermediate-, and high-grade lymphoma/leukemia was presented at a meeting of the American Society of Hematology.58 The conditioning regimen was the same except that the TBI dose was 0–8 Gy. The higher dose of TBI was given to patients with high-grade disease. Notably, one-third of patients had an Eastern Cooperative Oncology Group (ECOG) performance score ≥ 3. This ECOG score was a primary infl uence on outcomes, as seen in a PFS rate of 23% at 3 years, a TRM rate of 42%, and a relapse rate of 29%. Patients with high-grade lymphoma/leukemia who received higher TBI doses had a better PFS. In-terestingly, in the subgroup of patients with mature lymphoid malignancies (n = 84), low levels of lactate dehydrogenase (LDH) was the only independent predic-tor of a better PFS. Eurocord reported the results of a study that included patients with lymphoid malignancies who received UCB transplant after reduced-intensity conditioning (n = 64) or myeloablative conditioning (n = 36).60 Neutrophil recovery was achieved in 84% of patients, with a slightly shorter interval to recovery for recipients of reduced-intensity conditioning (17 days vs 22 days) and a higher engraftment rate for patients who received a conditioning regimen that included TBI and a higher CD34+ cell dose but did not receive antilympho-cyte globulin/ATG (ALG/ATG). The TRM rate was 28% at 1 year and the relapse/progression rate was 35% at 2 years. The PFS rate was 36% at 2 years and was better
October 2011, Vol. 18, No. 4 Cancer Control 233
Tabl
e 3.
— U
mbi
lical
Cor
d Bl
ood
Tran
spla
ntat
ion
for A
dults
With
Lym
phoi
d M
alig
nanc
ies
Refe
renc
eLy
mph
oid
Mal
igna
ncie
sIn
clud
ed
HSC
Sour
ceNo
. of
Patie
nts
Med
ian
Age
(yrs
)
Med
ian
Tim
e to
AN
C >
500/
µL(d
ays)
Med
ian
Tim
e to
Pl
atel
et C
ount
>
20 ×
109 /L
(day
s)
Acut
e GV
HDII–
IV(%
)
Chro
nic
GVHD
(%)
Rela
pse/
Prog
ress
ion
(%)
Trea
tmen
t-Re
late
d M
orta
lity
(%)
PFS
(%)
Yuji
et a
l56
2005
NHL
HLUC
B20
4720
308
of 1
52
of 1
1NA
4150
Maj
hail
et a
l57
2006
HLUC
BRE
L9 12
28 4210 7
NA NA67 58
11 33NA NA
22 2525 20
P Va
lue
.02
.70
.24
.88
.67
Wak
e et
al58
2008
NHL
HL MM
ATL
LBL
UCB
2653
19NA
4238
2942
23 a
t 3 y
rs
Brun
stei
n et
al59
2009
NHL
HL CLL
UCB
6546
846
5719
4215
34 a
t 3 y
rsCu
rren
t PFS
:49
at 3
yrs
Rodr
igue
s et
al60
2009
NHL
HL CLL
UCB
104
4117
NA24
1935
2836
at 2
yrs
Rodr
igue
s et
al61
2009
NHL
HL CLL
UCB
URD
75 284
44 48NA NA
NA NA33 31
37 4838 35
28 3034
at 2
yrs
34 a
t 2 y
rs
P Va
lue
NS.0
5NS
NSNS
HSC
= he
mat
opoi
etic
ste
m c
ell,
ANC
= ab
solu
te n
eutro
phil
coun
t, GV
HD =
gra
ft-vs
-hos
t dis
ease
, PFS
= p
rogr
essi
on-fr
ee s
urvi
val,
NHL
= no
n-Ho
dgki
n ly
mph
oma,
HL
= Ho
dgki
n ly
mph
oma,
UCB
= u
mbi
lical
cor
d bl
ood,
NA
= no
t ava
ilabl
e, R
EL =
rela
ted
dono
r, M
M =
mul
tiple
mye
lom
a, A
TL =
acu
te T
-cel
l leu
kem
ia/ly
mph
oma,
LBL
= ly
mph
obla
stic
lym
phom
a, C
LL =
chr
onic
lym
phoc
ytic
leuk
emia
, URD
= u
nrel
ated
don
or,
NS =
not
sig
nifi c
ant.
234 Cancer Control October 2011, Vol. 18, No. 4
for patients with chemotherapy-sensitive disease who received a higher nucleated cell dose and a conditioning regimen that included low-dose TBI.
Intermediate- and low-grade lymphoid malignancies are more frequently diagnosed in older patients, and often patients have received an autologous transplant by the time they are referred for allogeneic transplantation. Thus, the number of reduced-intensity conditioning UCB trans-plantations for lymphomas is likely to be greater than that of myeloablative conditioning transplantation as many institutions would consider recipients of prior autologous transplantation heavily pretreated to withstand a second myeloablation. A study of 65 adults with high-, intermedi-ate-, and low-grade lymphoid malignancies with a median of 4 previous treatments was reported by the University of Minnesota (Table 3).59 All patients received a condition-ing regimen consisting of cyclophosphamide, fl udarabine, and 2 Gy of TBI. Median time to neutrophil recovery was only 8 days. A large proportion (86%) received double UCB grafts, resulting in 57% of patients developing grade II–IV acute GVHD. TRM was relatively low (15%), the relapse/progression rate was 42%, and the PFS rate was 34%. However, of 26 patients who had disease relapse/progression, 15 patients, of whom 9 achieved a complete response, had immunosuppression removed or received some form of additional antilymphoma therapy, which generally included rituximab. Thus, the current PFS rate was 49% and the overall survival rate was 55%. Patients with low-grade disease had a particularly improved cur-rent PFS rate of 68% (Fig 4).59 Preliminary data from the same institution suggested that outcomes of Hodgkin lymphoma patients are similar, regardless of whether they receive a UCB or related-donor graft (Table 3).56 More recently, the Eurocord presented a study comparing the outcomes of lymphoid malignancy patients after 4–6/6 HLA-matched UCB transplantation (n = 75) or 6/6 or 8/8
HLA-matched peripheral blood URD (n = 284) transplan-tation in the setting of reduced-intensity conditioning.61 As part of the conditioning regimen, it was more common for UCB patients to receive TBI and for URD patients to receive ATG/ALG or alemtuzumab. Neutrophil engraft-ment was higher after URD transplantation (98% vs 85%, P < .0001). Acute GVHD, TRM, and relapse risks were similar between the two groups, but there was slightly less chronic GVHD after UCB transplantation (37% vs 48%, P = .05). The PFS at 2 years was 34%, the same for both UCB and URD. A fi nal analysis based on this presentation should be available soon.
While the outcomes of UCB transplantation need to be evaluated in larger numbers of patients with specifi c subtypes of lymphoid malignancy, current data support the utilization of UCB for patients who require an al-lograft in the setting of prospective clinical trials.
ConclusionsSupported by a rapidly growing body of evidence dem-onstrating the safety and effi cacy of UCB transplantation, this HSC source has been used more frequently for the treatment of patients with hematologic malignancies. After an initially limited utilization among adults in con-trast to routine utilization in children who lack a suitable sibling donor, UCB transplantation for older and larger patients is also increasing. Factors that specifi cally con-tributed to the expanded use of UCB in adults include, but are not limited to, results of outcomes utilizing a higher minimum nucleated cell dose to select grafts that yielded results similar to other donor types, the utilization of double UCB grafts for adult patients who do not have a single unit large enough to proceed to transplantation, and the use of reduced-intensity conditioning regimens in UCB transplantation.
The fi eld of UCB transplantation is still relatively young, and several areas of this fi eld require additional research to further improve outcomes. One example is the reduced rate and cumulative incidence of engraft-ment in UCB recipients that could potentially impact the risk of TRM. Efforts in improving engraftment are ongoing and include expanding the inventory of high-quality UCB units, utilizing double UCB grafts,28 coadmin-istering third-party CD34+ progenitors,62 improving ex vivo expansion,63 activating homing receptors (such as CXCR4),64 and utilizing intra-bone marrow injection.65,66 Others have been investigating how to reduce the risk of GVHD and potentially improve immune reconstitu-tion and reduce the risk of infections.67 As with unre-lated donor transplantation, outcomes in specifi c patient subgroups could also be improved by refi ning donor selection such as considering killer immunoglobulin-like receptor (KIR) ligand matching.68,69 The results of ongoing multicenter prospective clinical trials in both Europe and the United States will improve understanding of the indications and applicability of double UCB grafts
Months Post-UCBT
Cu
mu
lati
ve P
rop
ort
ion
0.0
0 12 24 36
0.2
0.4
0.6
0.8
1.0follicular lymphoma/CLL
large-cell/mantle-cell lymphoma
Hodgkin lymphoma
Fig 4. — Current progression-free survival of patients with lymphoid malignancies after reduced-intensity umbilical cord blood transplantation. Brunstein CG, Cantero S, Cao Q, et al. Promising progression-free survival for patients low and intermediate grade lymphoid malignancies after nonmye-loablative umbilical cord blood transplantation. Biol Blood Marrow Transplant. 2009;15(2):214-222. Reproduced with permission from Elsevier.
October 2011, Vol. 18, No. 4 Cancer Control 235
(eg, CTN-0501) and reduced-intensity conditioning (eg, CTN-0604) UCB transplantation.
Appreciation is expressed to Michael J. Franklin, MS, of the University of Minnesota for assistance in editing and to Carol Taubert for assistance in preparing this manuscript.
References 1. Wagner JE, Kernan NA, Steinbuch M, et al. Allogeneic sibling umbil-ical-cord-blood transplantation in children with malignant and non-malignant disease. Lancet. 1995;346(8969):214-219. 2. Wagner JE, Rosenthal J, Sweetman R, et al. Successful transplanta-tion of HLA-matched and HLA-mismatched umbilical cord blood from unre-lated donors: analysis of engraftment and acute graft-versus-host disease. Blood. 1996;88(3):795-802. 3. Kurtzberg J, Graham M, Casey J, et al. The use of umbilical cord blood in mismatched related and unrelated hemopoietic stem cell transplan-tation. Blood Cells. 1994;20(2-3):275-283; discussion 284. 4. Gluckman E, Rocha V, Boyer-Chammard A, et al. Outcome of cord-blood transplantation from related and unrelated donors. Eurocord Trans-plant Group and the European Blood and Marrow Transplantation Group. N Engl J Med. 1997;337(6):373-381. 5. Rubinstein P, Carrier C, Scaradavou A, et al. Outcomes among 562 recipients of placental-blood transplants from unrelated donors. N Engl J Med. 1998;339(22):1565-1577. 6. Laughlin MJ, Barker J, Bambach B, et al. Hematopoietic engraft-ment and survival in adult recipients of umbilical-cord blood from unrelated donors. N Engl J Med. 2001;344(24):1815-1822. 7. Wagner JE, Barker JN, De For TE, et al. Transplantation of unrelated donor umbilical cord blood in 102 patients with malignant and nonmalignant diseases: infl uence of CD34 cell dose and HLA disparity on treatment-relat-ed mortality and survival. Blood. 2002;100(5):1611-1618. 8. Ohnuma K, Isoyama K, Ikuta K, et al. Cord blood transplantation from HLA-mismatched unrelated donors as a treatment for children with hae-matological malignancies. Br J Haematol. 2001;112(4):981-987. 9. Isoyama K, Ohnuma K, Kato K, et al. Cord blood transplantation from unrelated donors: a preliminary report from the Japanese Cord Blood Bank Network. Leuk Lymphoma. 2003;44(3):429-438. 10. Locatelli F, Rocha V, Chastang C, et al. Factors associated with outcome after cord blood transplantation in children with acute leukemia. Blood. 1999;93(11):3662-3671. 11. Barker JN, Davies SM, De For T, et al. Survival after transplanta-tion of unrelated donor umbilical cord blood is comparable to that of hu-man leukocyte antigen-matched unrelated donor bone marrow: results of a matched-pair analysis. Blood. 2001;97(10):2957-2961. 12. Rocha V, Cornish J, Sievers EL, et al. Comparison of outcomes of unrelated bone marrow and umbilical cord blood transplants in children with acute leukemia. Blood. 2001;97(10):2962-2971. 13. Michel G, Rocha V, Chevret S, et al. Unrelated cord blood transplan-tation for childhood acute myeloid leukemia: a Eurocord Group analysis. Blood. 2003;102(13):4290-4297. 14. Jacobsohn DA, Hewlett B, Ranalli M, et al. Outcomes of unrelated cord blood transplants and allogeneic-related hematopoietic stem cell trans-plants in children with high-risk acute lymphocytic leukemia. Bone Marrow Transplant. 2004;34(10):901-907. 15. Gluckman E, Rocha V, Arcese W, et al. Factors associated with out-comes of unrelated cord blood transplant: guidelines for donor choice. Exp Hematol. 2004;32(4):397-407. 16. Wall DA, Carter SL, Kernan NA, et al. Busulfan/melphalan/antithy-mocyte globulin followed by unrelated donor cord blood transplantation for treatment of infant leukemia and leukemia in young children: the Cord Blood Transplantation study (COBLT) experience. Biol Blood Marrow Transplant. 2005;11(8):637-646. 17. Eapen M, Rubinstein P, Zhang MJ, et al. Outcomes of transplanta-tion of unrelated donor umbilical cord blood and bone marrow in children with acute leukaemia: a comparison study. Lancet. 2007;369(9577):1947-1954. 18. Kurtzberg J, Prasad VK, Carter SL, et al. Results of the Cord Blood Transplantation Study (COBLT): clinical outcomes of unrelated donor um-bilical cord blood transplantation in pediatric patients with hematologic ma-lignancies. Blood. 2008;112(10):4318-4327. 19. Cornetta K, Laughlin M, Carter S, et al. Umbilical cord blood trans-plantation in adults: Results of the prospective cord blood transplantation (COBLT). Biol Blood Marrow Transplant. 2005;11(2):149-160. 20. Laughlin MJ, Eapen M, Rubinstein P, et al. Outcomes after trans-plantation of cord blood or bone marrow from unrelated donors in adults with leukemia. N Engl J Med. 2004;351(22):2265-2275. 21. Rocha V, Labopin M, Sanz G, et al. Transplants of umbilical-cord
blood or bone marrow from unrelated donors in adults with acute leukemia. N Engl J Med. 2004;351(22):2276-2285. 22. Takahashi S, Iseki T, Ooi J, et al. Single-institute comparative analysis of unrelated bone marrow transplantation and cord blood transplantation for adult patients with hematologic malignancies. Blood. 2004;104(12):3813-3820. 23. Takahashi S, Ooi J, Tomonari A, et al. Comparative single-institute analysis of cord blood transplantation from unrelated donors with bone mar-row or peripheral blood stem-cell transplants from related donors in adult patients with hematologic malignancies after myeloablative conditioning regimen. Blood. 2007;109(3):1322-1330. 24. Kumar P, De For TE, Brunstein C, et al. Allogeneic hematopoietic stem cell transplantation in adult acute lymphocytic leukemia: impact of donor source on survival. Biol Blood Marrow Transplant. 2008;14(12):1394-1400. 25. Tomblyn MB, Arora M, Baker KS, et al. Myeloablative hematopoi-etic cell transplantation for acute lymphoblastic leukemia: analysis of graft sources and long-term outcome. J Clin Oncol. 2009;27(22):3634-3641. 26. Atsuta Y, Suzuki R, Nagamura-Inoue T, et al. Disease-specifi c analyses of unrelated cord blood transplantation compared with unrelated bone marrow transplantation in adult patients with acute leukemia. Blood. 2009;113(8):1631-1638. 27. Eapen M, Rocha V, Sanz G, et al. Effect of graft source on unrelated donor haemopoietic stem-cell transplantation in adults with acute leukaemia: a retrospective analysis. Lancet Oncol. 2010;11(7):653-660. 28. Brunstein CG, Gutman JA, Weisdorf DJ, et al. Allogeneic hemato-poietic cell transplantation for hematological malignancy: relative risks and benefi ts of double umbilical cord blood. Blood. 2010;116(22):4693-4699. 29. Ooi J, Iseki T, Takahashi S, et al. Unrelated cord blood transplantation for adult patients with de novo acute myeloid leukemia. Blood. 2004;103(2):489-491. 30. Sanz J, Sanz MA, Saavedra S, et al. Cord blood transplantation from unrelated donors in adults with high-risk acute myeloid leukemia. Biol Blood Marrow Transplant. 2010;16(1):86-94. 31. Brunstein CG, Setubal D, Tomblyn M, et al. Umbilical cord blood transplant after reduced intensity conditioning provides outcomes compa-rable HLA-matched siblings for patients with high risk and advanced acute myeloid leukemia. Blood. 2006;108(11):606. Abstract. 32. Ballen KK, Spitzer TR, Yeap BY, et al. Double unrelated reduced-intensity umbilical cord blood transplantation in adults. Biol Blood Marrow Transplant. 2007;13(1):82-89. 33. Brunstein CG, Barker JN, Weisdorf DJ, et al. Umbilical cord blood transplantation after nonmyeloablative conditioning: impact on transplanta-tion outcomes in 110 adults with hematologic disease. Blood. 2007;110(8):3064-3070. 34. Druker BJ, Sawyers CL, Kantarjian H, et al. Activity of a specifi c inhibitor of the BCR-ABL tyrosine kinase in the blast crisis of chronic myeloid leukemia and acute lymphoblastic leukemia with the Philadelphia chromo-some. N Engl J Med. 2001;344(14):1038-1042. 35. Druker BJ, Talpaz M, Resta DJ, et al. Effi cacy and safety of a specifi c inhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemia. N Engl J Med. 2001;344(14):1031-1037. 36. Kantarjian H, Shah NP, Hochhaus A, et al. Dasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 362(24):2260-2270. 37. Saglio G, Kim DW, Issaragrisil S, et al. Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N Engl J Med. 2010;362(24): 2251-2259. 38. McGlave PB, Shu XO, Wen W, et al. Unrelated donor marrow trans-plantation for chronic myelogenous leukemia: 9 years’ experience of the national marrow donor program. Blood. 2000;95(7):2219-2225. 39. Chiorean EG, De For TE, Weisdorf DJ, et al. Donor chimerism does not predict response to donor lymphocyte infusion for relapsed chronic my-elogenous leukemia after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2004;10(3):171-177. 40. Dazzi F, Szydlo RM, Craddock C, et al. Comparison of single-dose and escalating-dose regimens of donor lymphocyte infusion for relapse after allografting for chronic myeloid leukemia. Blood. 2000;95(1):67-71. 41. Guglielmi C, Arcese W, Dazzi F, et al. Donor lymphocyte infusion for relapsed chronic myelogenous leukemia: prognostic relevance of the initial cell dose. Blood. 2002;100(2):397-405. 42. Maschan AA, Skorobogatova EV, Samotchatova EV, et al. A suc-cessful cord blood transplant in a child with second accelerated phase chronic myeloid leukemia following lymphoid blast crisis. Bone Marrow Transplant. 2000;25(2):213-215. 43. Pecora AL, Stiff P, Jennis A, et al. Prompt and durable engraftment in two older adult patients with high risk chronic myelogenous leukemia (CML) using ex vivo expanded and unmanipulated unrelated umbilical cord blood. Bone Marrow Transplant. 2000;25(7):797-799. 44. Arcese W, Rocha V, Labopin M, et al. Unrelated cord blood trans-plants in adults with hematologic malignancies. Haematologica. 2006;91(2): 223-230. 45. Brunstein CB, Setubal D, De For T, et al. Umbilical cord blood trans-plantation for adult patients with chronic myeloid leukemia. Biol Blood Mar-row Transplant. 2007;13(2 suppl):84.
236 Cancer Control October 2011, Vol. 18, No. 4
46. Sanz GF, Saavedra S, Jiménez C, et al. Unrelated donor cord blood transplantation in adults with chronic myelogenous leukemia: results in nine patients from a single institution. Bone Marrow Transplant. 2001;27(7):693-701. 47. Sanz J, Montesinos P, Saavedra S, et al. Single-unit umbilical cord blood transplantation from unrelated donors in adult patients with chronic myelogenous leukemia. Biol Blood Marrow Transplant. 2010;16(11):1589-1595. 48. Ooi J, Iseki T, Takahashi S, et al. Unrelated cord blood transplan-tation for adult patients with advanced myelodysplastic syndrome. Blood. 2003;101(12):4711-4713. 49. Sato A, Ooi J, Takahashi S, et al. Unrelated cord blood transplanta-tion after myeloablative conditioning in adults with advanced myelodysplas-tic syndromes. Bone Marrow Transplant. 2011;46(2):257-261. 50. Warlick ED, Cioc A, De For T, et al. Allogeneic stem cell transplanta-tion for adults with myelodysplastic syndromes: importance of pretransplant disease burden. Biol Blood Marrow Transplant. 2009;15(1):30-38. 51. Ando T, Yujiri T, Tominaga T, et al. Autografting followed by a re-duced-intensity conditioning unrelated donor cord blood transplantation for a patient with refractory multiple myeloma: successful engraftment with mini-mal toxicity. Eur J Haematol. 2005;74(2):175-179. 52. Kasahara I, Nishio M, Yamamoto S, et al. Cord blood transplanta-tion with a reduced-intensity conditioning regimen for patients with relapsed aggressive multiple myeloma after cytoreduction with bortezomib. Int J He-matol. 2009;90(3):413-415. 53. Miura Y, Azuma T, Kusumi E, et al. Graft-versus-myeloma effects in reduced-intensity cord blood transplantation. Int J Hematol. 2007;86(5):463-465. 54. Toubai T, Hirate D, Shono Y, et al. Chimerism and T-cell receptor repertoire analysis after unrelated cord blood transplantation with a reduced-intensity conditioning regimen following autologous stem cell transplantation for multiple myeloma. Int J Lab Hematol. 2008;30(1):75-81. 55. Yamada T, Tomonari A, Takahashi S, et al. Unrelated cord blood trans-plantation with a reduced-intensity conditioning regimen following autologous transplantation for multiple myeloma. Int J Hematol. 2004;80(4):377-380. 56. Yuji K, Miyakoshi S, Kato D, et al. Reduced-intensity unrelated cord blood transplantation for patients with advanced malignant lymphoma. Biol Blood Marrow Transplant. 2005;11(4):314-318. 57. Majhail NS, Weisdorf DJ, Wagner JE, et al. Comparable results of umbilical cord blood and HLA-matched sibling donor hematopoietic stem cell transplantation after reduced-intensity preparative regimen for advanced Hodgkin lymphoma. Blood. 2006;107(9):3804-3807. 58. Wake A, Uchida N, Ishiwata K, et al. Single institute analysis of re-duced intensity cord blood transplantation from unrelated donors for adults with advanced lymphoid malignancies. Blood (ASH Annual Meeting Ab-stracts). 2008;112:1963. Abstract. 59. Brunstein CG, Cantero S, Cao Q, et al. Promising progression-free survival for patients low and intermediate grade lymphoid malignancies after nonmyeloablative umbilical cord blood transplantation. Biol Blood Marrow Transplant. 2009;15(2):214-222. 60. Rodrigues CA, Sanz G, Brunstein CG, et al. Analysis of risk fac-tors for outcomes after unrelated cord blood transplantation in adults with lymphoid malignancies: a study by the Eurocord-Netcord and Lymphoma Working Party of the European Group for Blood and Marrow Transplantation. J Clin Oncol. 2009;27(2):256-263. 61. Rodrigues CA, Canals C, Brunstein C, et al. Comparison of out-comes after unrelated cord blood transplantation and matched unrelated donor RIC transplantation for lymphoid malignancies: a Eurocord-Netcord Group/Lymphoma Working Party and Chronic Leukemia Working Party of the European Group for Blood and Marrow Transplantation Study. Blood (ASH Annual Meeting Abstracts). 2009;114:663. 62. Fernández MN, Regidor C, Cabrera R, et al. Unrelated umbilical cord blood transplants in adults: early recovery of neutrophils by supportive co-transplantation of a low number of highly purifi ed peripheral blood CD34+ cells from an HLA-haploidentical donor. Exp Hematol. 2003;31(6):535-544. 63. Delaney C, Heimfeld S, Brashem-Stein C, et al. Notch-mediated expansion of human cord blood progenitor cells capable of rapid myeloid reconstitution. Nat Med. 2010;16(2):232-236. 64. Ratajczak MZ, Reca R, Wysoczynski M, et al. Modulation of the SDF-1-CXCR4 axis by the third complement component (C3)--implications for traffi cking of CXCR4+ stem cells. Exp Hematol. 2006;34(8):986-995. 65. Brunstein CG, Barker JN, Weisdorf DJ, et al. Intra-BM injection to enhance engraftment after myeloablative umbilical cord blood transplan-tation with two partially HLA-matched units. Bone Marrow Transplant. 2009;43(12):935-940. 66. Frassoni F, Gualandi F, Podestà M, et al. Direct intrabone transplant of unrelated cord-blood cells in acute leukaemia: a phase I/II study. Lancet Oncol. 2008;9(9):831-839. 67. Brunstein CG, Miller JS, Cao Q, et al. Infusion of ex vivo expanded T regulatory cells in adults transplanted with umbilical cord blood: safety profi le and detection kinetics. Blood. 2011;117(3):1061-1070. 68. Brunstein CG, Wagner JE, Weisdorf DJ, et al. Negative effect of KIR alloreactivity in recipients of umbilical cord blood transplant depends on transplantation conditioning intensity. Blood. 2009;113(22):5628-5634.
69. Willemze R, Rodrigues CA, Labopin M, et al. KIR-ligand incompatibil-ity in the graft-versus-host direction improves outcomes after umbilical cord blood transplantation for acute leukemia. Leukemia. 2009;23(3):492-500.